Prostate Cancer Hospitals India | Prostate Cancer Surgeon in India
Upload
europa-uomo-epadCategory
view
578download
0
Personalized medicine in prostate cancer care
D.Jacqmin
EAU Board Member
EAPM Treasurer
1
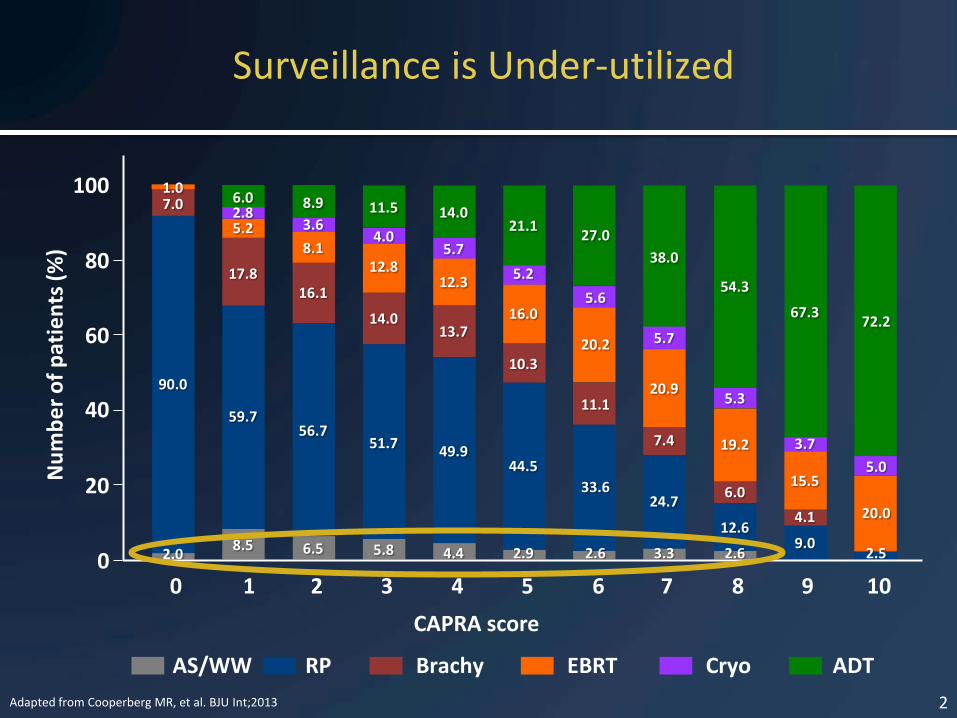
Surveillance is Under-utilized
Adapted from Cooperberg MR, et al. BJU Int;2013
Nu
mb
er
of
pat
ien
ts (
%)
CAPRA score
100
80
60
40
20
0 0 2 3 4 5 6 7 8 9 10 1
AS/WW RP Brachy EBRT Cryo ADT
8.5 2.0 6.5 5.8 4.4 2.9 2.6 3.3
24.7 33.6
44.5 49.9
51.7 56.7
59.7
90.0
16.1 17.8
7.0
11.1
10.3
13.7 14.0
1.0
5.2 2.8 6.0
8.1
3.6
8.9
12.8
4.0
11.5
12.3
5.7
14.0
16.0
5.2
21.1
20.2
5.6
27.0
2.6 2.5 9.0
4.1
15.5
3.7
20.0
5.0
12.6
6.0
19.2
5.3
72.2 67.3
54.3
7.4
20.9
5.7
38.0
2

Clear Need and Opportunity to Improve Prostate Cancer Management
• Significant driver of over treatment is limited accuracy of low
risk classification based on measures available today
• Despite low (3%) risk of disease progression1 and modest treatment benefit2, >90%3 of low risk men will receive immediate treatment
1. Boorjian SA, et al. Urol Oncol 2008; 2. Wilt TJ, et al. N Engl J Med. 2012; 3. Cooperberg MR et al. J Clin Oncol 2010; 4. Otis W. Brawley, MD, American Cancer Society
3
“We desperately need the ability to predict which patient has a localized cancer that is going to metastasize and cause suffering
and death, and which patient has a cancer that is destined to stay in the patient's prostate for the remainder of his life.”
-American Cancer Society4
Prostate cancer care
• How to have a more personalized approach ?
• What’s new ?
• Genomic tests
– Oncotype DX prostate cancer test
– Prolaris test
– Decipher test
4

ONCOTYPE DX PROSTATE CANCER TEST
5

The Oncotype DX® Prostate Cancer Assay
• WHAT is the test? – A tumor gene expression assay which produces a Genomic Prostate Score
(GPS) to help guide initial treatment decisions at the time of biopsy
• WHO is the test for? – Newly diagnosed men with low to low-intermediate risk prostate cancer
(GS 3+3, low volume 3+4)
• WHY do the test? – To improve risk stratification by incorporating individual underlying tumor
biology
– To identify appropriate patients for Active Surveillance (AS) or immediate treatment
6

Oncotype DX® GPS Provides More Accurate and Individualized Risk Assessment at Time of Biopsy
• Developed to address tumor heterogeneity and biopsy under-sampling
• Based on multiple biologic pathways predictive of aggressive prostate cancer
• Optimized technology for very small amounts of tumor from needle biopsies
• Independently validated in contemporary low and low-intermediate risk patients
7
1. Klein et. al. ASCO GU 2011; 2. Klein et. al. ASCO 2012; 3. Cooperberg et. al. AUA 2013
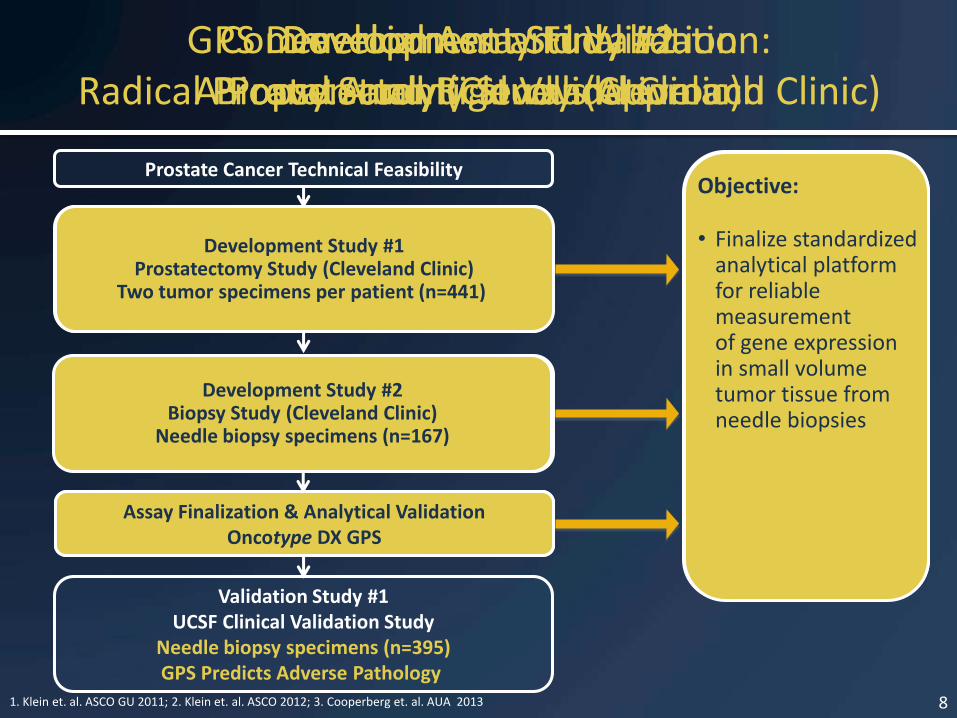
Validation Study #1 UCSF Clinical Validation Study
Needle biopsy specimens (n=395) GPS Predicts Adverse Pathology
Development Study #1 Prostatectomy Study (Cleveland Clinic)
Two tumor foci per patient (n=441) 1º endpoint: Clinical Recurrence
2º endpoints: PCSS, BCR, Adverse Pathology at RP
Prostate Cancer Technical Feasibility
Assay Finalization & Analytical Validation Oncotype DX GPS
Development Study #2 Biopsy Study (Cleveland Clinic)
Needle biopsy specimens (n=167)
Development Study #1 Radical Prostatectomy Study (Cleveland Clinic)
8
Objectives:
• Identify genes associated with clinical recurrence (local recurrence or distant metastases) accounting for tumor heterogeneity
• Additional endpoints included PCSS, biochemical recurrence, and adverse pathology at RP
Development Study #1 Prostatectomy Study (Cleveland Clinic)
Two tumor specimens per patient (n=441)
Development Study #2 Biopsy Study (Cleveland Clinic)
Needle biopsy specimens (n=167)
Assay Finalization & Analytical Validation Oncotype DX GPS
Development Study #2 Biopsy Study (Cleveland Clinic) Commercial Assay Finalization
and Analytical Validation
Objectives:
• To confirm that genes robust to heterogeneity are predictive when assessed in biopsy specimens
• Likelihood of adverse pathology (high grade or non-organ confined disease) at prostatectomy
Objective:
• Finalize standardized analytical platform for reliable measurement of gene expression in small volume tumor tissue from needle biopsies
GPS Development and Validation: A Proven and Rigorous Approach

GPS Incorporates Multiple Biologic Pathways Predictive of Prostate Cancer Aggressiveness
9
Stromal Response BGN
COL1A1 SFRP4
Proliferation TPX2
Androgen Signaling FAM13C
KLK2 AZGP1
SRD5A2
Cellular Organization
FLNC GSN
TPM2 GSTM2
The combination of multiple pathways
is more predictive than
any single pathway
Genes Associated with Better Outcome
Genes Associated with Worse Outcome
ARF1 ATP5E CLTC
GPS1 PGK1
Reference Genes

Development Study #2 Biopsy Study (Cleveland Clinic)
Needle biopsy specimens (n=167)
Objectives:
• To validate GPS as a predictor of adverse pathology in a contemporary early-stage patient cohort
• To determine whether GPS adds independent predictive information beyond standard clinical and pathologic data
Independent Clinical Validation Study of the 17-Gene Oncotype DX® GPS
Validation Study #1 UCSF Clinical Validation Study
Needle biopsy specimens (n=395)
Development Study #1 Prostatectomy Study (Cleveland Clinic)
Two tumor specimens per patient (n=441)
Prostate Cancer Technical Feasibility
Assay Finalization & Analytical Validation Oncotype DX GPS
1. Klein et. al. ASCO GU 2011; 2. Klein et. al. ASCO 2012; 3. Cooperberg et. al. AUA 2013 10

Validation Study Focused on Men Who Were Potential Candidates for Active Surveillance
UCSF Database 1997-2011 Consented RP patients meeting
active surveillance criteria at diagnosis Low/Intermediate risk biopsy
GS 3+3 and low volume 3+4 (fewer than 4 positive cores) Eligible Population
n = 412
17 (4%) Excluded for insufficient RNA quality
Final Evaluable Population n = 395
11 Cooperberg et al, AUA 2013

Combining Biologic & Clinical Information Refines Risk Stratification for Individual Patients
VERY LOW RISK LOW RISK INTERMEDIATE RISK
More Individualized Biologic and Clinical Risk Assessment
Likelihood of Favorable Pathology 100% 30%
Population-Based Clinical Risk Assessment
VERY LOW RISK
LOW RISK INTERMEDIATE RISK
GPS=8 84%
GPS=51 57%
10% (N=37) 49% (N=191) 41% (N=160)
44% (N=169) 31% (N=119)
12
GPS=25 75%
UCSF Validation Study NCCN Risk Classification
• 10% Very Low-risk • 49% Low-risk • 41% Intermediate Risk
GPS Provides Biologic Risk Information
GPS
• Adds more accurate risk assessment by combining biological and clinical risk factors
• Predicted which patients have risk consistent with their NCCN clinical risk group
26% (N=100)
• 35% of men in the NCCN Low-risk group had more indolent biology and likelihood of favorable pathology consistent with Very Low-risk
• 10% of men in the NCCN Low-risk group had more aggressive biology and likelihood of favorable pathology consistent with Intermediate risk
• Identified patients in the NCCN Very Low-risk group who had more aggressive biology, with likelihood of favorable pathology consistent with Low and Intermediate risk disease
• Identified patients with Intermediate risk who had more indolent biology, predicted to be consistent with Low-risk disease
• Enables more accurate identification of a larger population of patients who can more confidently choose active surveillance
• Precisely identifies a patient’s tumor biology and refines the population-based clinical risk assessment with a more personalized risk assessment
Cooperberg et al, AUA 2013
13
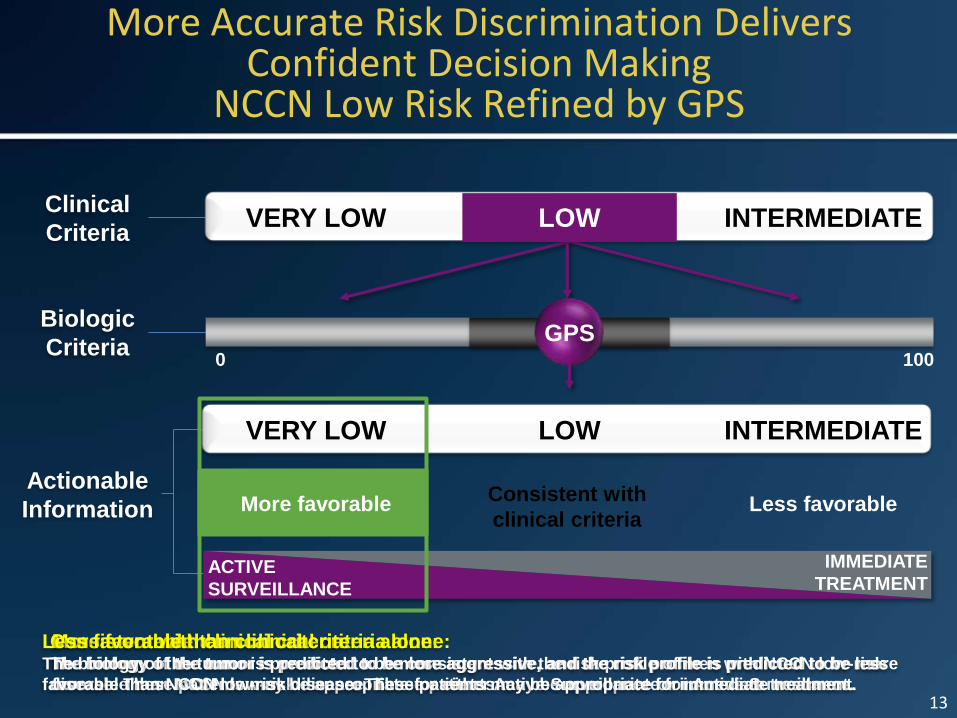
Actionable
Information
Biologic
Criteria
Clinical
Criteria VERY LOW INTERMEDIATE
VERY LOW INTERMEDIATE
ACTIVE
SURVEILLANCE
IMMEDIATE
TREATMENT
GPS
More favorable Consistent with
clinical criteria Less favorable
More favorable than clinical criteria alone: The biology of the tumor is predicted to be less aggressive, and the risk profile is predicted to be more
favorable than NCCN low-risk disease. These patients may be appropriate for Active Surveillance.
Consistent with clinical criteria: The biology of the tumor is predicted to be consistent with the risk profile of men with NCCN low-risk
disease. These patients may be appropriate for either Active Surveillance or immediate treatment.
Less favorable than clinical criteria alone: The biology of the tumor is predicted to be more aggressive, and the risk profile is predicted to be less
favorable than NCCN low-risk disease. These patients may be appropriate for immediate treatment.
0 100
LOW
LOW
More Accurate Risk Discrimination Delivers Confident Decision Making
NCCN Low Risk Refined by GPS
13

PROLARIS TEST
14
Prolaris test
• Studied on biopsies or RP specimens
• 31 cell cycle progression genes (cell proliferation)
• 15 housekeeper genes
• CCP score
15

Prolaris test
• Cell progression genes :
– FOXM1, CDC20, CDKN3, CDC2, KIF11, KIA0101, NUSAP1, CENPF, ASPM, BUB1B, RRM2, DLGAP5, BIRC5, KIF20A, PLK1, T0-P2A, TK1, PBK, ASF1B, C18orf24, RAD54L, PTTG1, CDCA3, MCM10, PRC1, DTL, CEP55, RAD51, CENPM, CDCA8, ORC6L
• Housekeeping genes (reference) :
– RPL38, UBA52, PSMC1, RPL4, RPL37, RPS29, SLC25A3, CLTC, TXNL1, PSMA1, RPL8, MMADHC, RPL13A, LOC723658, PPP2CA, MRFAP1
16

CCP score 10 years CSS
• 0 = risk of NCCN classification
• + 1 means risk x 2
• - 1 means lower risk than NCCN classification
17
Cuzick et al.Lancet Oncol.:2011;12;245-255.
Cooperberg et al.:J.C.Oncol.2013;31;1428-1434.

Positive prostate biopsy
Low Risk
Low Prolaris Score
Active Surveillance
High Prolaris Score
Single Modality Treatment
Intermediate Risk
Low Prolaris Score
Active Surveillance
High Prolaris Score
Multimodality Treatment
High Risk
Low Prolaris Score
Single Modality Treatment
High Prolaris Score
Multimodality Treatment
18
DECIPHER TEST
19

Decipher Prostate Cancer Test
• Predicts probability of metastasis after surgery
• Performed on Radical Prostatectomy specimen
• Validated retrospectively in US on 2000 patients
• Based on 22 RNA biomarkers associated with aggressive prostate cancer
20
Decipher Prostate Cancer test
• Validation study :
– 545 patients operated between 87-01 with high Gleason score, extra-prostatic extension, seminal vesicle invasion or N+
– 192 progressive disease, 353 controls
– Confirmed by 3 other studies from Mayo and CC
21
Erho et al:PLoSone2013;8;e66855.
Klein et al.:Eur.Urol.2015;67;778-786.
Karnes et al.:J.Urol.2013;190;2047-2053.
Den et al.:Int.J.Radiat.Oncol.Biol.Phys.2014;89;1038-1046

Decipher Prostate Cancer Test
• RNA biomarkers :
– LASP1, IQGAP3, NFIB, S1PR4, THBS2, ANO7, PCDH7, MYBPC1, EPPK1, TSBP, PBX1, NUSAP1, ZWILCH, UBE2C, CAMK2N1, RABGAP1, PCAT-32, GLYATL1P4/PCAT-80, TNFRSF19
• Select patients who may benefit from adjuvant treatment after surgery
22

Conclusion
• Genomic tests will help to tailored treatment for Prostate Cancer Patients
• Oncotype DX Prostate Cancer Test : Will help to select Patients candidates for Active Surveillance
• Prolaris test : Will impact the follow-up of patients at risk
• Decipher test : Will detect candidates for early adjuvant treatment in high risk group
• Clinical criteria combined with genomic tests will improve the personalization of treatment in Prostate Cancer Patients
23