PERSONAGGI FAMOSI CON IBD - Giacomo Trallori · TERAPIA DELLA COLITE ULCEROSA ... PERSONAGGI FAMOSI...
37
12/04/2012 1 Malattie Infiammatorie Croniche Intestinali: TERAPIA DELLA COLITE ULCEROSA Giacomo Trallori Venerdi 23 e Sabato 24 Marzo 2012 Firenze PERSONAGGI FAMOSI CON PERSONAGGI FAMOSI CON IBD IBD
Transcript of PERSONAGGI FAMOSI CON IBD - Giacomo Trallori · TERAPIA DELLA COLITE ULCEROSA ... PERSONAGGI FAMOSI...
12/04/2012
1
Malattie Infiammatorie Croniche Intestinali:TERAPIA DELLA COLITE ULCEROSA
Giacomo Trallori Venerdi 23 e Sabato 24 Marzo 2012
Firenze
PERSONAGGI FAMOSI CON PERSONAGGI FAMOSI CON IBDIBD
12/04/2012
2
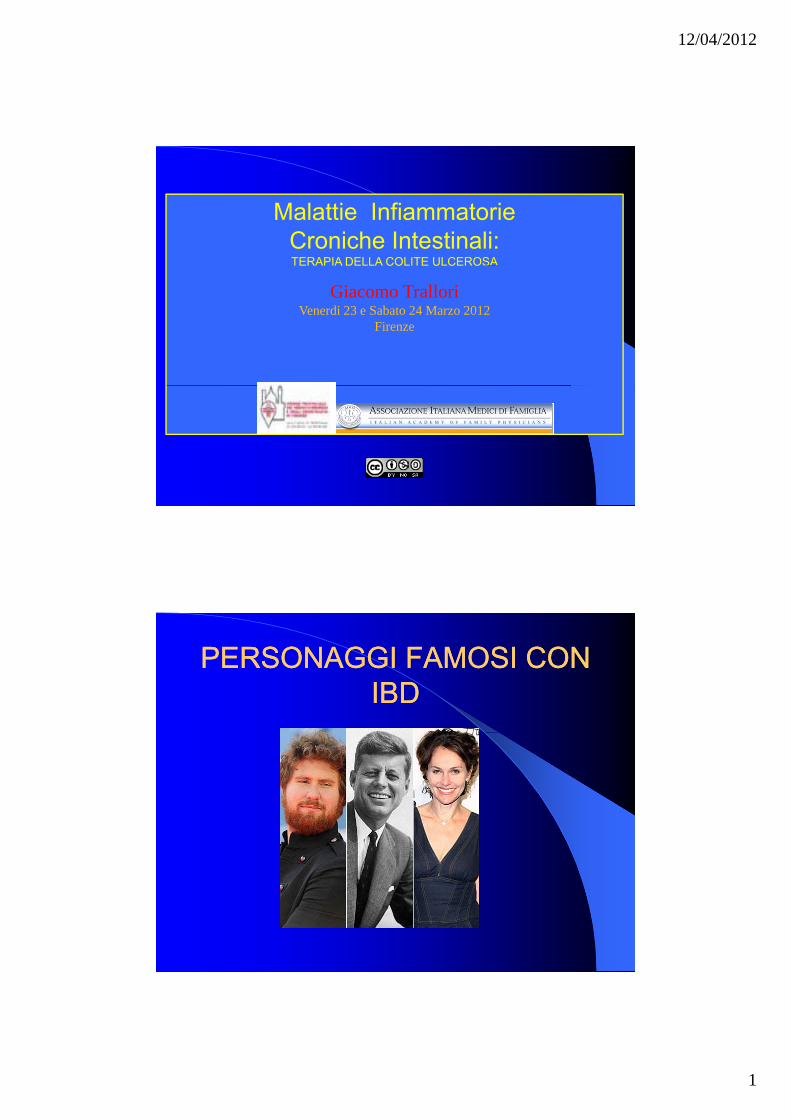
Current PharmacotherapyCurrent Pharmacotherapy
Because no cure for UC has been foundBecause no cure for UC has been found, treatment of the disease consists of long-term pharmacotherapyDirected at controlling the symptoms of the diseaseThe ultimate goal is to achieve remission and avoid surgery
Traditional Approach To Traditional Approach To Therapy For Ulcerative ColitisTherapy For Ulcerative Colitis
12/04/2012
3
La terapia medica della La terapia medica della M.R.G.E.M.R.G.E.
Giacomo Trallori MDGiacomo Trallori MDGiacomo Trallori, MDGiacomo Trallori, MDAzienda Ospedaliera Azienda Ospedaliera CareggiCareggiFirenzeFirenze
Costi studio 2004Costi studio 2004
12/04/2012
4
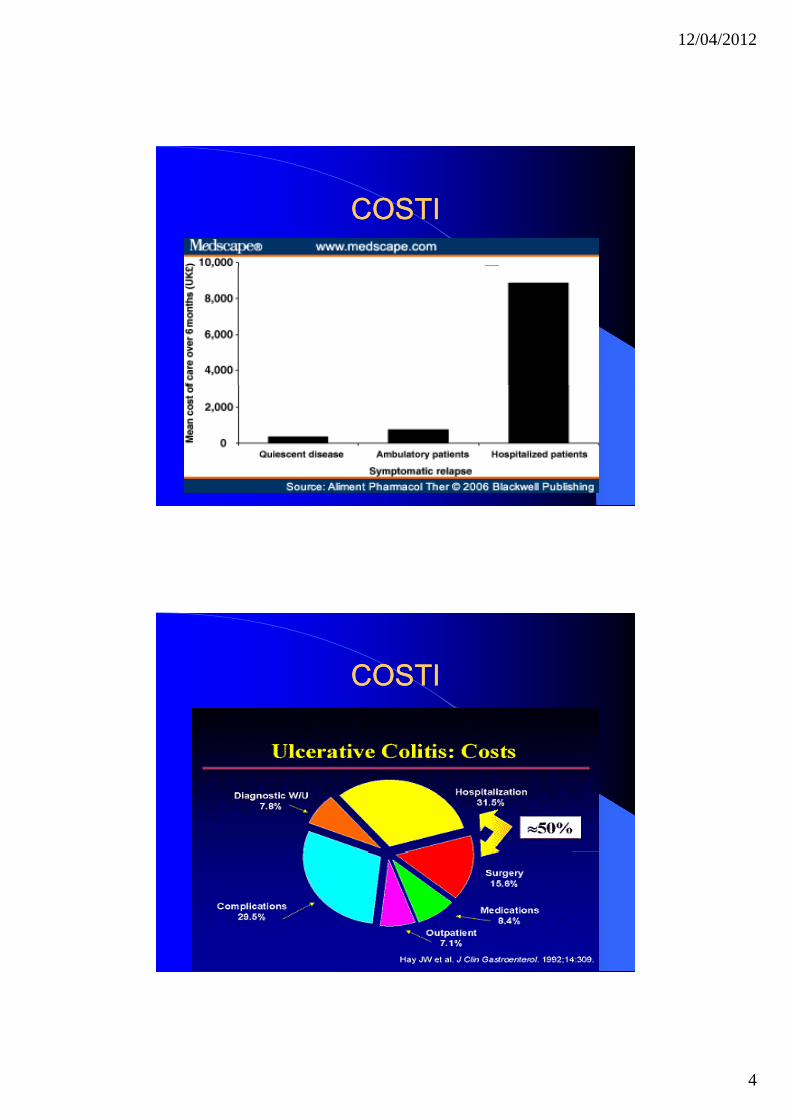
COSTICOSTI
COSTICOSTI
12/04/2012
5
SulfasalazineSulfasalazine
Became available in the 1940’s when SvatzBecame available in the 1940 s when Svatz et al discovered that sulfasalazine, originally used to treat RA, was also noted to reduce colonic mucosal inflammation and bloody diarrhea
SulfasalazineSulfasalazine
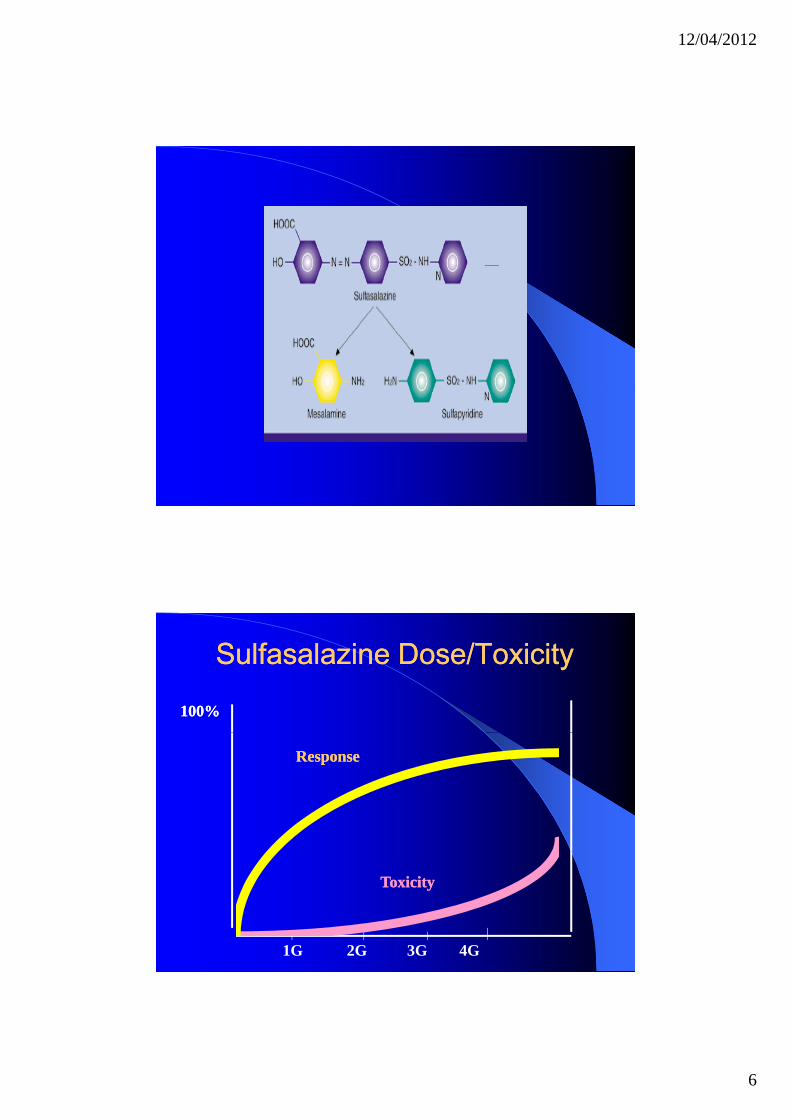
Is indicated for the treatment of mild toIs indicated for the treatment of mild to moderate UC, as adjunctive therapy in severe cases, and for prolongation of remissionIt is a prodrug comprised of mesalamine and sulfapyridine joined by a diazo bondand sulfapyridine joined by a diazo bondAbout 1/3 of the dose is absorbed in the small intestine
12/04/2012
6
Sulfasalazine Dose/ToxicitySulfasalazine Dose/Toxicity
100%100%
ResponseResponse
1G 2G 3G 4G
ToxicityToxicity
12/04/2012
7
SulfasalazineSulfasalazine
Adverse events of sulfasalazine are of twoAdverse events of sulfasalazine are of two types: dose-related or hypersensitivityThe first group includes nausea, vomiting, abdominal discomfort, anorexia, and headache.Less common include hemolytic anemia, reticulocytosis, and methemoglobinemia
SulfasalazineSulfasalazine
The second group are non dose dependentThe second group are non-dose dependent They include exfoliative dermatitis, aplastic anemia, hepatitis, pancreatitis, pneumonitis, autoimmune hemolysis, pericarditis, nephrotic syndrome, and severe exacerbation of symptoms of colitis
12/04/2012
8
SulfaSulfa--Free Oral MesalamineFree Oral Mesalamine
Studies have shown that mesalamine is theStudies have shown that mesalamine is the principal therapeutically active component of sulfasalazine, while sulfapyridine is the carrierRecognition that sulfapyridine is associated with dose-related adverse events led to efforts to develop sulfa-free productsdevelop sulfa free productsThese include Asacol (mesalamine), Dipentum (olsalazine), Pentasa (mesalamine), and Colazal (balsalazide)
Asacol (mesalamine)Asacol (mesalamine)
Asacol tablets were introduced to the US in 1992Asacol tablets were introduced to the US in 1992Unlike sulfasalazine, olsalazine, and balsalazine, Asacol is not a prodrug It contains a core of 400 mg of mesalamine coated with a pH-sensitive acrylic polymer call Eudragit-S which delays release of mesalamine until the
bl h i f H f 7 btablet reaches an environment of pH of 7 or aboveThe coating typically dissolves in the terminal ileum or colon
12/04/2012
9
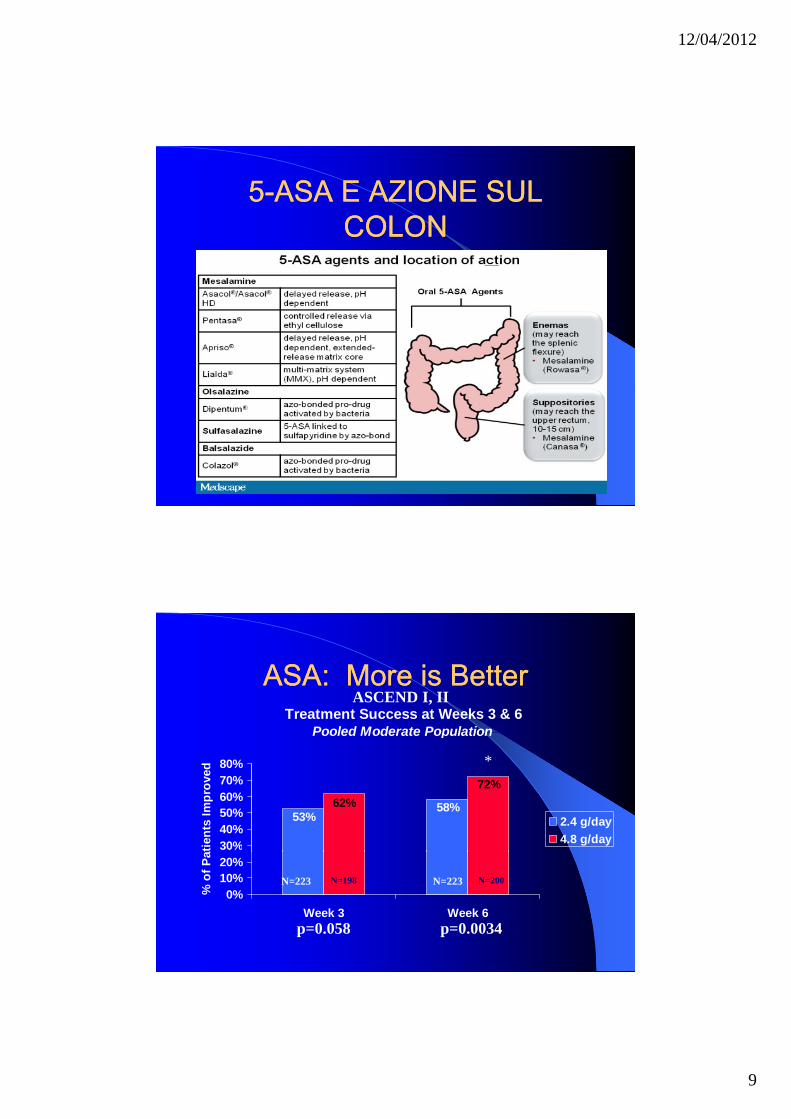
55--ASA E AZIONE SUL ASA E AZIONE SUL COLONCOLON
ASA: More is BetterASA: More is BetterTreatment Success at Weeks 3 & 6
Pooled Moderate Population
ASCEND I, II
Pooled Moderate Population
58%53%
72%62%
30%40%50%60%70%80%
atie
nts
Impr
oved
2.4 g/day4.8 g/day
*
0%10%20%
Week 3 Week 6
% o
f Pa
p=0.0034p=0.058
N=223 N=223N=198 N=200
12/04/2012
10
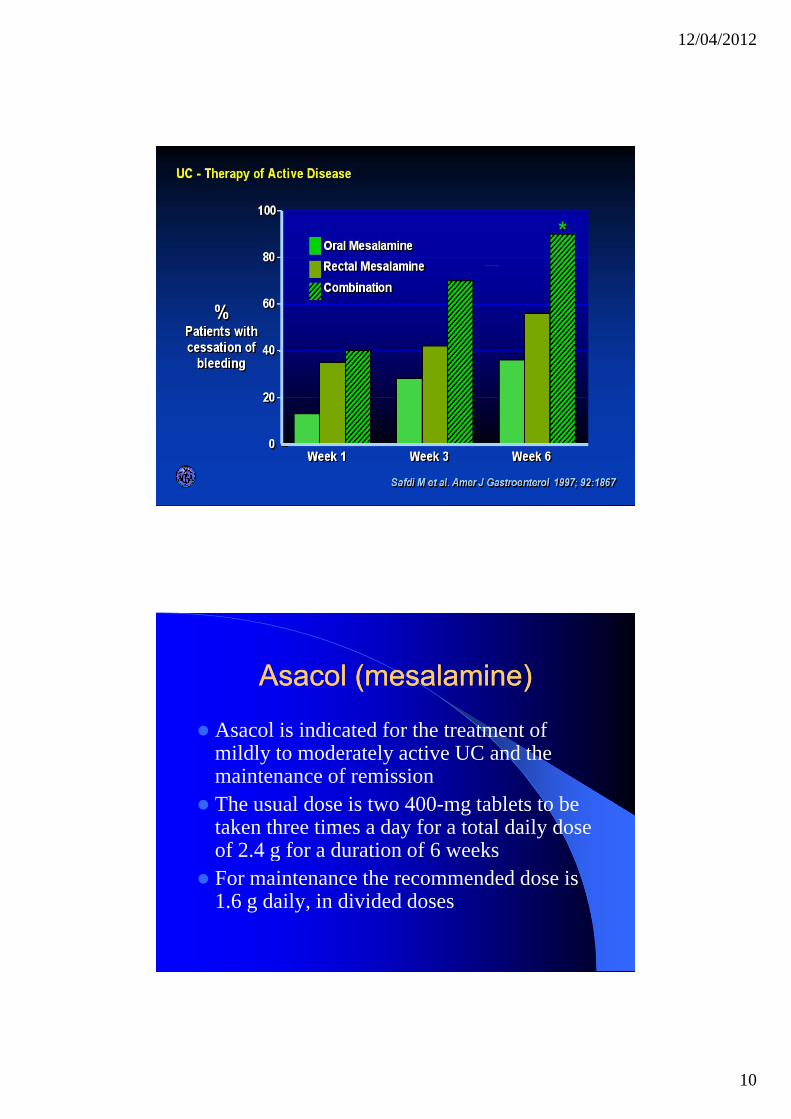
Asacol (mesalamine)Asacol (mesalamine)
Asacol is indicated for the treatment ofAsacol is indicated for the treatment of mildly to moderately active UC and the maintenance of remission The usual dose is two 400-mg tablets to be taken three times a day for a total daily dose of 2 4 g for a duration of 6 weeksof 2.4 g for a duration of 6 weeksFor maintenance the recommended dose is 1.6 g daily, in divided doses
12/04/2012
11
Pentasa (mesalamine)Pentasa (mesalamine)
Pentasa has been marketed in the US since 1993Pentasa has been marketed in the US since 1993Pentasa is also not a prodrugUnlike Asacol, the delivery system is made up of mesalamine microspheresIt is moisture activated, thus the capsules di i t t i th t h di i t ll ddisintegrate in the stomach, dispersing controlled-release microspheres into the small bowel and throughout the rest of the colon
Pentasa (mesalamine)Pentasa (mesalamine)
Pentasa is indicated for the induction ofPentasa is indicated for the induction of remission and for the treatment of mildly to moderately active UCThe recommended dose is four 250-mg capsules four times a day for a total daily dose of 4 0 gdose of 4.0 gTreatment duration is up to 8 weeksIs not indicated for maintenance UC
12/04/2012
12
Dipentum (olsalazine)Dipentum (olsalazine)
Dipentum was introduced to the US in 1990Dipentum was introduced to the US in 1990 and contains 250-mg of olsalazine sodiumIt is a prodrug consisting of two molecules of mesalamine joined by a diazo bond which is cleaved by bacterial action in the colon
Dipentum (olsalazine)Dipentum (olsalazine)
Dipentum is indicated for maintenance ofDipentum is indicated for maintenance of remission of UC in patients intolerant to sulfasalazineThe usual dose is two 250-mg capsules twice a day for a total daily dose of 1.0 gDipentum is not indicated for the treatment of acute ulcerative colitis
12/04/2012
13
Colazal (balsalazide)Colazal (balsalazide)
Colazal was introduced to the US in 2000Colazal was introduced to the US in 2000 and contains 750-mg of balsalazide sodiumIt is a prodrug and is delivered intact to the colon where it is cleaved by bacterial azoreduction to release mesalamine70% of patients intolerant of sulfasalazine are able to tolerate balsalazide
Colazal (balsalazide)Colazal (balsalazide)
The recommended dose of 6 75 g/dayThe recommended dose of 6.75 g/day contains 2.4 g of mesalamineIt is indicated for the treatment of mildly to moderately active ulcerative colitisThe safety and effectiveness of Colazal y Cbeyond 12 weeks has not been establishedIs not indicated for the maintenance of UC
12/04/2012
14
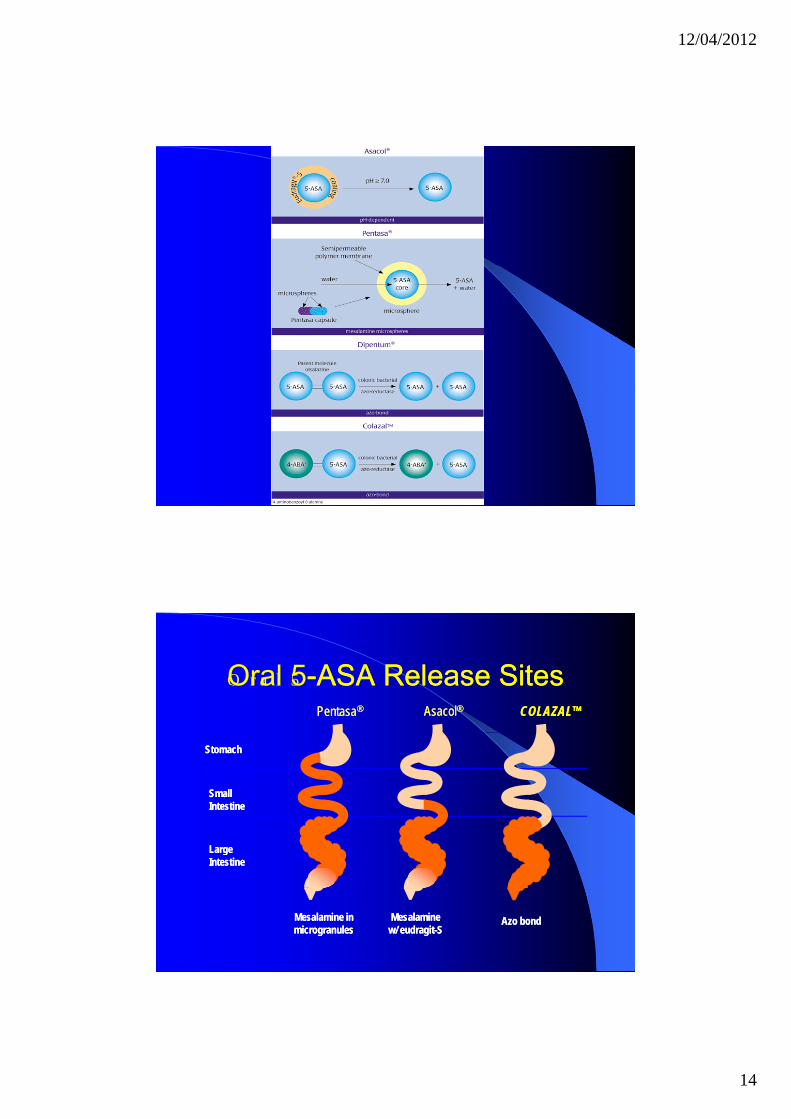
O r a l 5Oral 5--ASA Release SitesASA Release SitesCOLAZAL™COLAZAL™Pentasa® Pentasa® Asacol®Asacol®
StomachStomach
Small IntestineSmall Intestine
Large Large Large IntestineLarge Intestine
Azo bondAzo bondMesalamine in microgranulesMesalamine in microgranules
Mesalaminew/ eudragit-SMesalamine
w/ eudragit-S
12/04/2012
15
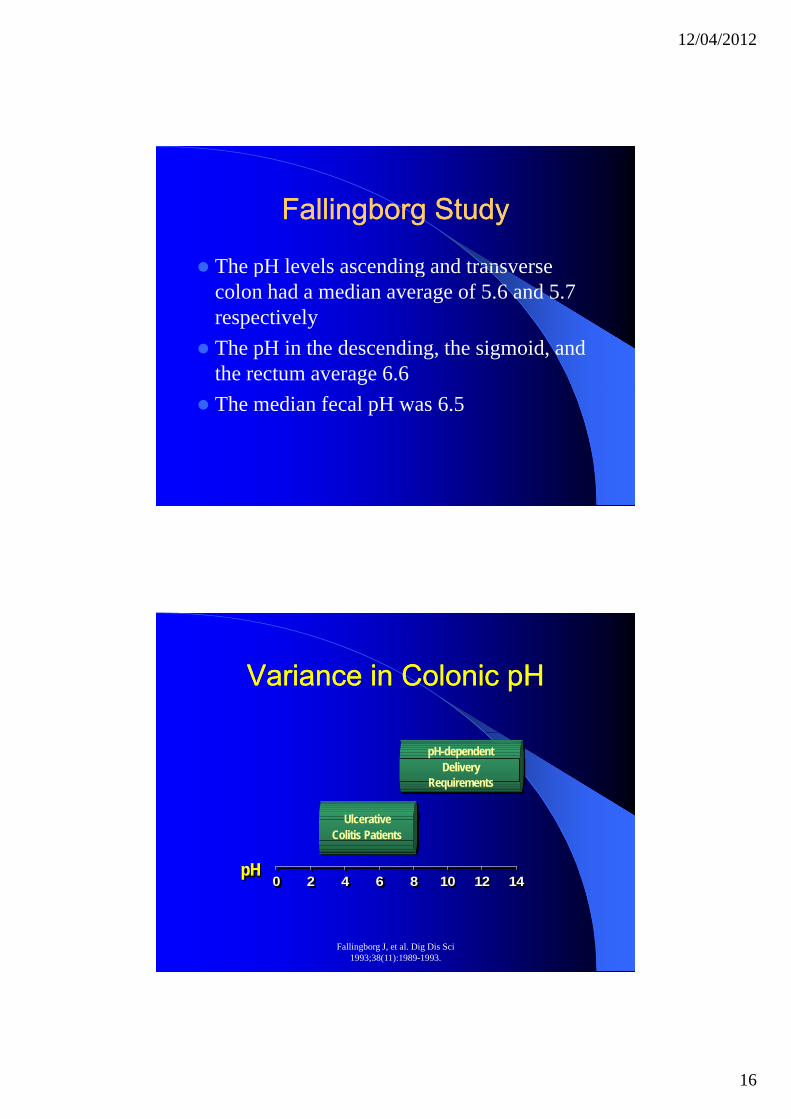
Fallingborg StudyFallingborg Study
pH of the gut lumen was measured in 39pH of the gut lumen was measured in 39 people with UC using a pH-sensitive, radiotransmitting capsuleThe location of the capsule was determined by X-rayThe pH was 5.7 in the cecum, but rose to 6.6 in the rectum
Fallingborg StudyFallingborg Study
The low pH in the cecum is thought to beThe low pH in the cecum is thought to be caused by bacterial fermentation of non-absorbed carbohydratesIn 17 of the subjects, the pH decreased by 0.1-0.8 units while leaving the terminal ileum and entering the cecumileum and entering the cecumIn the cecum the pH dropped between 0.5-2.5 pH units to a median value of 5.7
12/04/2012
16
Fallingborg StudyFallingborg Study
The pH levels ascending and transverseThe pH levels ascending and transverse colon had a median average of 5.6 and 5.7 respectivelyThe pH in the descending, the sigmoid, and the rectum average 6.6The median fecal pH was 6.5
Variance in Colonic pHVariance in Colonic pH
Ulcerative Colitis Patients
pH-dependent Delivery
Requirements
Fallingborg J, et al. Dig Dis Sci 1993;38(11):1989-1993.
0 2 4 6 8 10 12 14pH
12/04/2012
17
SteroidsSteroids
Corticosteroids such as prednisoneCorticosteroids, such as prednisone, methylprednisolone, and budesonide have been used to reduce inflammation in patients who do not respond to 5-ASA medsCan be given orally, intravenously, an enema or suppositoryenema, or suppositorySee improvement within daysAre a short term control of flare-up
SteroidsSteroids
Long term use increase likelihood of side effectsLong term use increase likelihood of side effects– Weight gain– Acne– Facial hair– HTN– OsteoporosisOsteoporosis– Diabetes– Mood swings– Risk of infection
12/04/2012
18
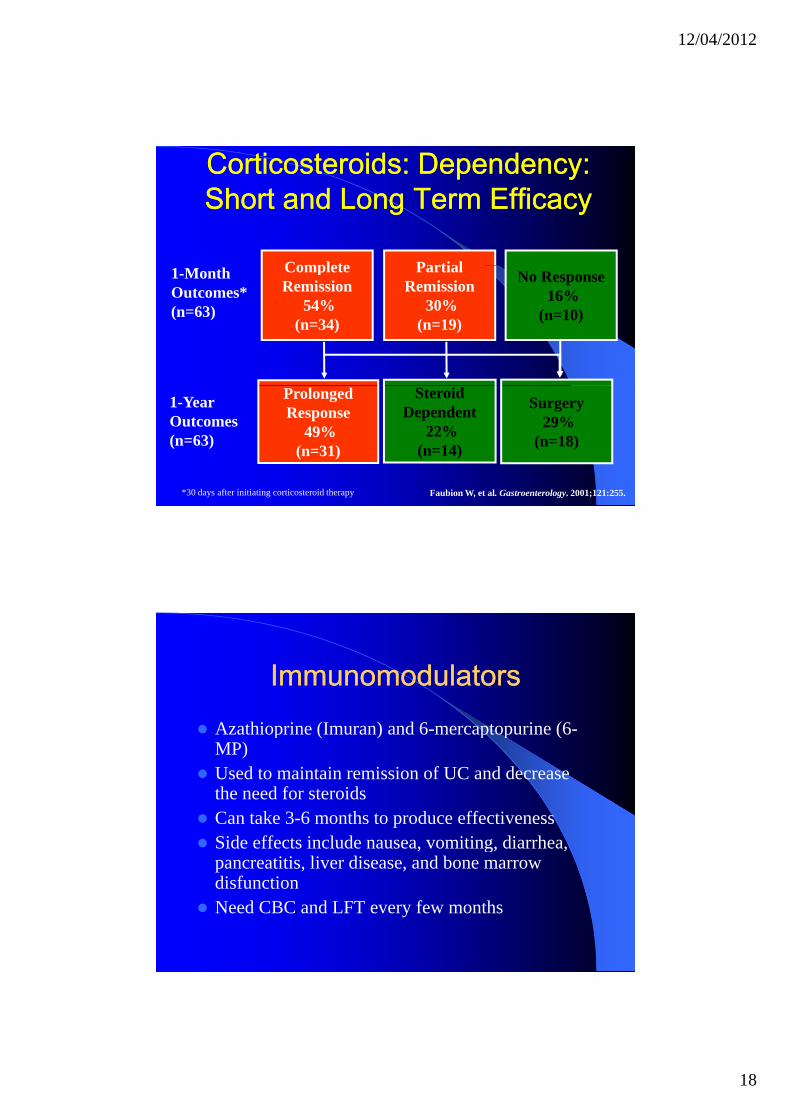
Corticosteroids: Dependency: Corticosteroids: Dependency: Short and Long Term EfficacyShort and Long Term Efficacy
Complete Partial1-Month Outcomes*(n=63)
Complete Remission
54%(n=34)
Partial Remission
30%(n=19)
No Response 16%
(n=10)
*30 days after initiating corticosteroid therapy Faubion W, et al. Gastroenterology. 2001;121:255.
1-YearOutcomes(n=63)
Steroid Dependent
22%(n=14)
Prolonged Response
49%(n=31)
Surgery 29%
(n=18)
ImmunomodulatorsImmunomodulators
Azathioprine (Imuran) and 6-mercaptopurine (6-Azathioprine (Imuran) and 6 mercaptopurine (6MP)Used to maintain remission of UC and decrease the need for steroidsCan take 3-6 months to produce effectivenessSide effects include nausea, vomiting, diarrhea, gpancreatitis, liver disease, and bone marrow disfunctionNeed CBC and LFT every few months
12/04/2012
19
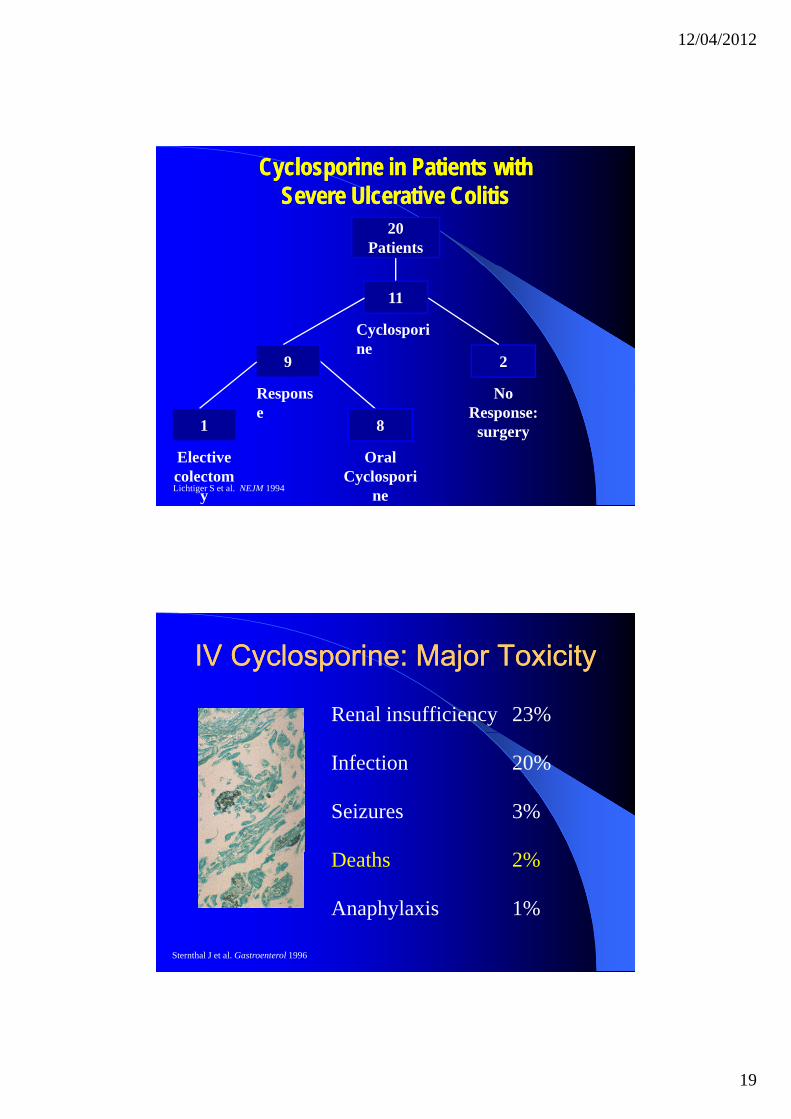
20Patients
Cyclosporine in Patients withCyclosporine in Patients withSevere Ulcerative ColitisSevere Ulcerative Colitis
29
11
Cyclosporine
81
No Response:
surgery
Response
Elective colectom
y
Oral Cyclospori
neLichtiger S et al. NEJM 1994
IV Cyclosporine: Major ToxicityIV Cyclosporine: Major Toxicity
Renal insufficiency 23%
Infection 20%
Seizures 3%
hDeaths 2%
Anaphylaxis 1%
Sternthal J et al. Gastroenterol 1996
12/04/2012
20
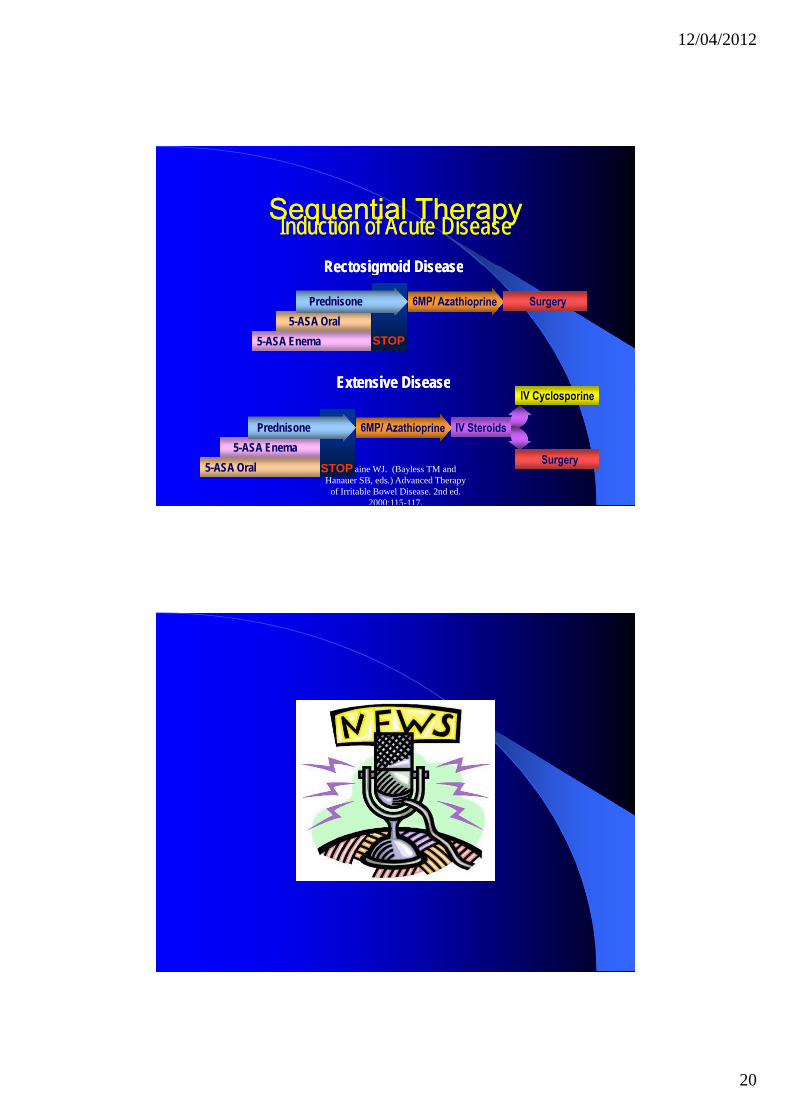
Sequential TherapySequential Therapy
Rectosigmoid DiseaseRectosigmoid Disease
Induction of Acute DiseaseInduction of Acute Disease
STOP5-ASA Enema5-ASA Oral
Prednisone
Rectosigmoid DiseaseRectosigmoid Disease
Extensive DiseaseExtensive Disease
Tremaine WJ. (Bayless TM and Hanauer SB, eds.) Advanced Therapy
of Irritable Bowel Disease. 2nd ed. 2000:115-117.
STOP5-ASA Enema
5-ASA Oral
Prednisone
Extensive DiseaseExtensive Disease

12/04/2012
21
UTILIZZO ANTIUTILIZZO ANTI--TNFTNF
New Therapy for Treatment of New Therapy for Treatment of UCUC
Tumor necrosis factor-alpha is a chemicalTumor necrosis factor-alpha is a chemical produced by the bodyIt is responsible for recruiting immune cells to different tissue where they cause inflammation, swelling, pain, warmth, and erythemaHigh concentrations of TNF have been found in aHigh concentrations of TNF have been found in a variety of infections and inflammatory diseases such as UC
12/04/2012
22
Remicade (infliximab) to Treat Remicade (infliximab) to Treat Ulcerative ColitisUlcerative Colitis
Remicade is an anti TNF drugRemicade is an anti-TNF drugRemicade is a monoclonal antibody that is formed by combining portions of human and murine antibody moleculesIt targets and neutralizes TNF, thus g ,decreasing the inflammatory response
Remicade (infliximab) to Treat Remicade (infliximab) to Treat Ulcerative ColitisUlcerative Colitis
In a retrospective study by Sands et al 16 patientsIn a retrospective study by Sands et al, 16 patients with severe UC received a single 5-mg/kg infusion of remicadeClinical, endoscopic, and histological improvements were observed in 88% (14/16) of patients after initial treatmentpatients after initial treatment5 months later, 38% (6/16) of the patients received a second infusion to maintain remission
12/04/2012
23
Remicade (infliximab) to Treat Remicade (infliximab) to Treat Ulcerative ColitisUlcerative Colitis
Surgery was avoided in 6/7 patients whoSurgery was avoided in 6/7 patients who were previous surgical candidatesClinical remission was maintained in 14/16 patients for at least six months and in 4/16 for at least ten monthsMost of the patients were completely withdrawn from corticosteroid therapy
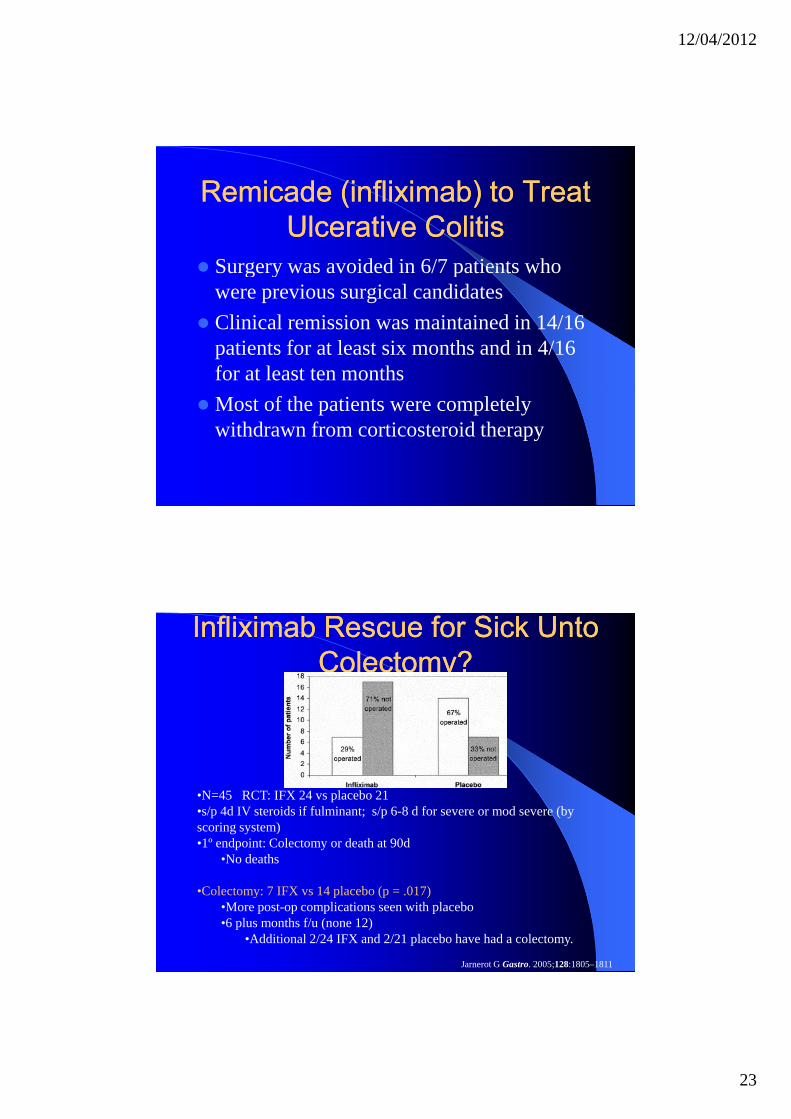
InfliximabInfliximab Rescue for Sick Unto Rescue for Sick Unto ColectomyColectomy??
•N=45 RCT: IFX 24 vs placebo 21•s/p 4d IV steroids if fulminant; s/p 6-8 d for severe or mod severe (by scoring system)•1º endpoint: Colectomy or death at 90d
•No deaths
•Colectomy: 7 IFX vs 14 placebo (p = .017)•More post-op complications seen with placebo•6 plus months f/u (none 12)
•Additional 2/24 IFX and 2/21 placebo have had a colectomy.
Jarnerot G Gastro. 2005;128:1805–1811
12/04/2012
24
Remicade (infliximab) to Treat Remicade (infliximab) to Treat Ulcerative ColitisUlcerative Colitis
In a second study 11 patients with severeIn a second study, 11 patients with severe UC were randomized to either receive a single infusion of remicade or a placeboOf the 8 patients receiving the remicade, 4 experienced a clinical response at 2 weeksOf the 3 patients receiving the placebo, all 3 experienced no response
Remicade (infliximab) to Treat Remicade (infliximab) to Treat Ulcerative ColitisUlcerative Colitis
Some of the most common symptoms as with anySome of the most common symptoms, as with any drug, are headaches, nausea, vomiting, URI, dizziness, and rashesMore serious complications include TB, pneumonia, sepsis, herpes zoster, leukemia, and lymphomalymphomaAdditionally, some people were noted to become ANA and anti-double-stranded DNA positive
12/04/2012
25
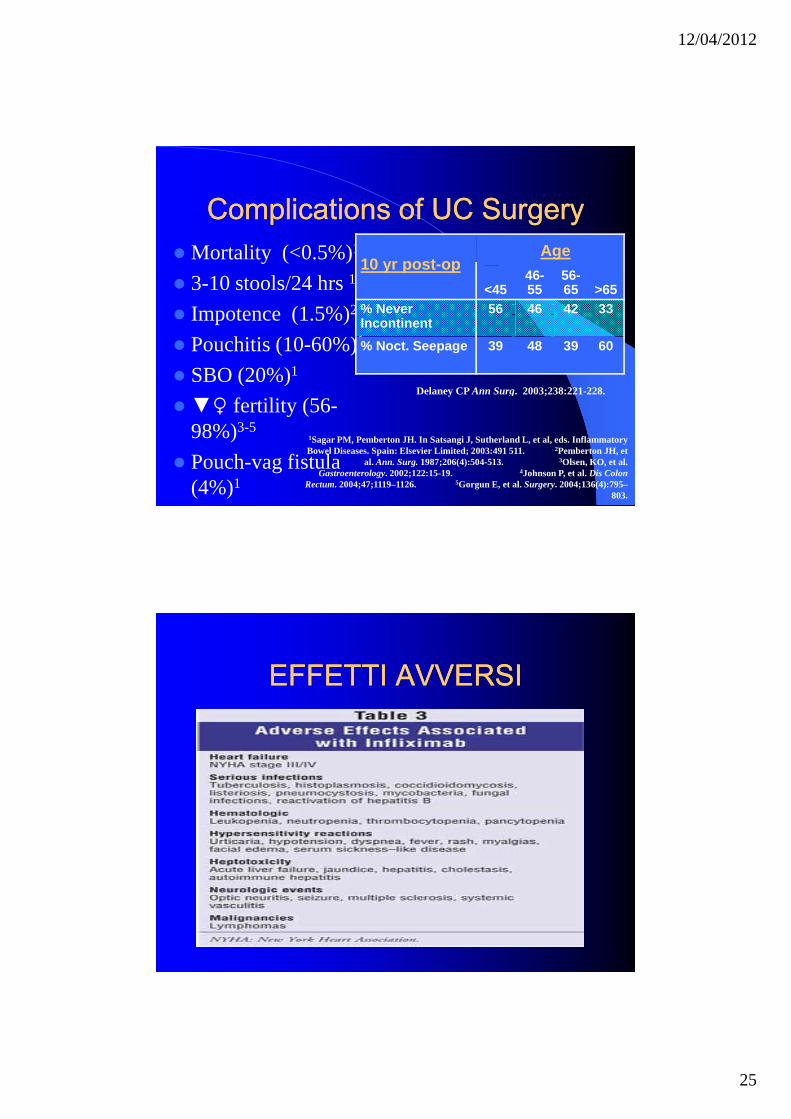
Complications of UC SurgeryComplications of UC SurgeryMortality (<0.5%)1
10 yr post-opAge
3-10 stools/24 hrs 1
Impotence (1.5%)2
Pouchitis (10-60%)1
SBO (20%)1
10 yr post-op<45
46-55
56-65 >65
% Never Incontinent
56 46 42 33
% Noct. Seepage 39 48 39 60
( )▼♀ fertility (56-98%)3-5
Pouch-vag fistula (4%)1
1Sagar PM, Pemberton JH. In Satsangi J, Sutherland L, et al, eds. Inflammatory Bowel Diseases. Spain: Elsevier Limited; 2003:491 511. 2Pemberton JH, et
al. Ann. Surg. 1987;206(4):504-513. 3Olsen, KO, et al. Gastroenterology. 2002;122:15-19. 4Johnson P, et al. Dis Colon
Rectum. 2004;47;1119–1126. 5Gorgun E, et al. Surgery. 2004;136(4):795–803.
Delaney CP Ann Surg. 2003;238:221-228.
EFFETTI AVVERSIEFFETTI AVVERSI
12/04/2012
26
Anti Anti -- TNFTNF
AntiAnti-- TNFTNF
12/04/2012
27
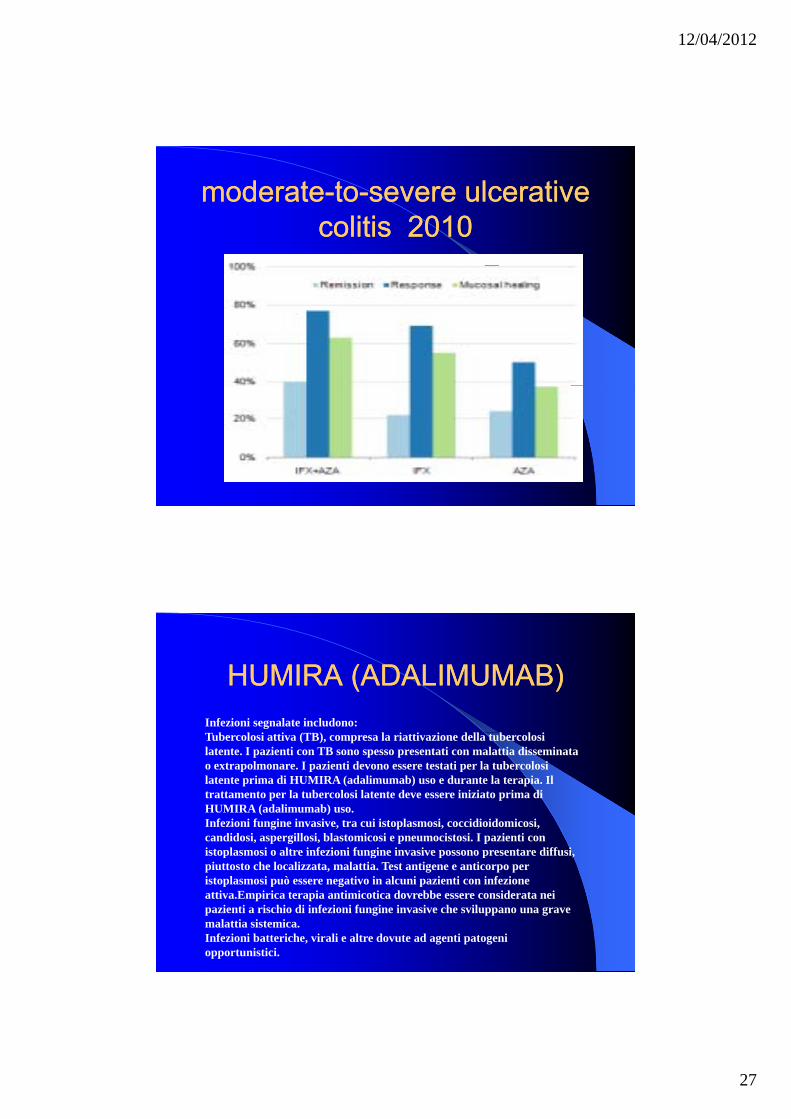
moderatemoderate--toto--severesevere ulcerative ulcerative colitiscolitis 20102010
HUMIRA (ADALIMUMAB)HUMIRA (ADALIMUMAB)Infezioni segnalate includono:Tubercolosi attiva (TB), compresa la riattivazione della tubercolosi latente. I pazienti con TB sono spesso presentati con malattia disseminata o extrapolmonare. I pazienti devono essere testati per la tubercolosi latente prima di HUMIRA (adalimumab) uso e durante la terapia. Il trattamento per la tubercolosi latente deve essere iniziato prima di HUMIRA (adalimumab) uso.Infezioni fungine invasive, tra cui istoplasmosi, coccidioidomicosi, candidosi, aspergillosi, blastomicosi e pneumocistosi. I pazienti con istoplasmosi o altre infezioni fungine invasive possono presentare diffusiistoplasmosi o altre infezioni fungine invasive possono presentare diffusi, piuttosto che localizzata, malattia. Test antigene e anticorpo per istoplasmosi può essere negativo in alcuni pazienti con infezione attiva.Empirica terapia antimicotica dovrebbe essere considerata nei pazienti a rischio di infezioni fungine invasive che sviluppano una grave malattia sistemica.Infezioni batteriche, virali e altre dovute ad agenti patogeni opportunistici.
12/04/2012
28
IBD Drugs in Pregnancy IBD Drugs in Pregnancy
5-ASAs and corticosteroids low risk for use during d b f di
gpregnancy and breast-feedingImmunosuppressants– AZA/6-MP appear low risk during pregnancy– Methotrexate contraindicated
Antibiotics– Ampicillin and cephalosporins are low risk– Ciprofloxacin and metronidazole should be avoided for
longterm uselongterm useBiologics: – Anti-TNF agents low risk. Infliximab and likely
adalimumab cross placenta in third trimester
Natural RemediesNatural Remedies
www copingwithcolitiswww.copingwithcolitisSeasilver: 100% plant-based nutritional supplement 1-STARCat’s Claw: Helps normalize the balance of beneficial microbes and reverse conditions of intestinal inflammation 5-STAR
12/04/2012
29
12/04/2012
30
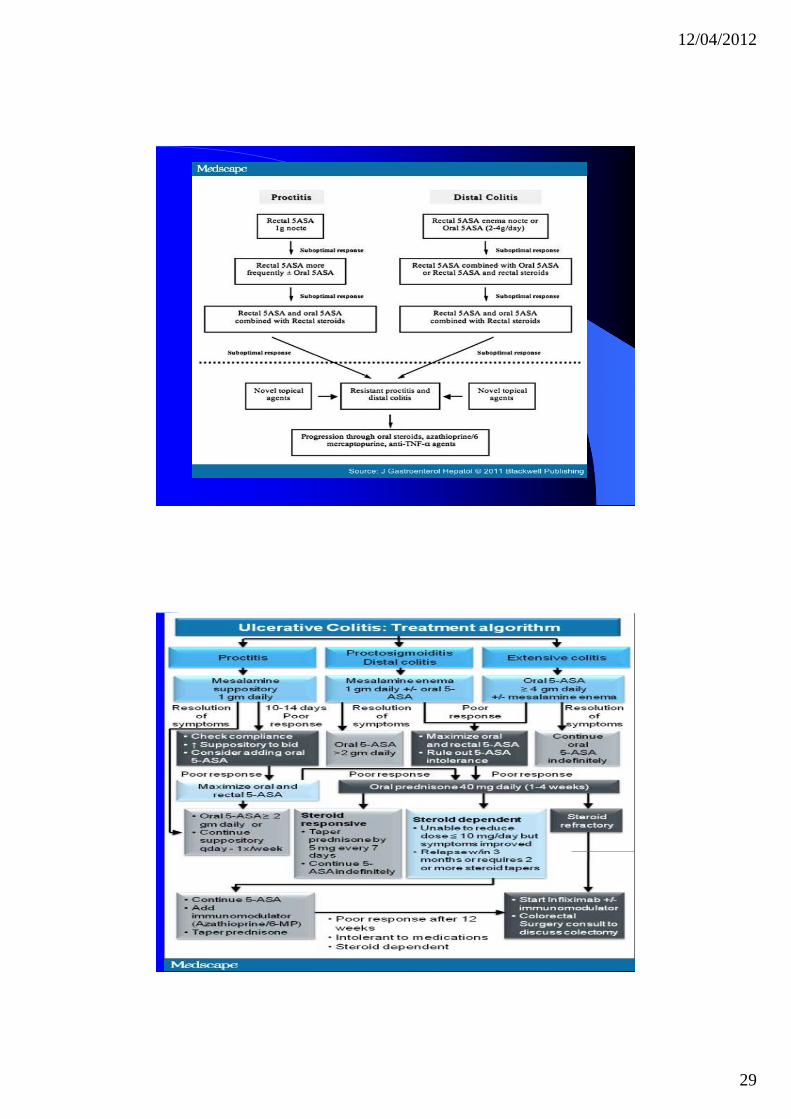
Ulcerative Colitis: Mild to ModerateUlcerative Colitis: Mild to ModerateAcute flare
Exclude entericpathogen
Extensive
Oral 5-ASA
Responseadequate
Responseinadequate
MaintainResponse adequate Consider
Consider rectal therapy(5-ASA and/or steroid)
Patient willing totake rectal therapy
Patient unwilling to take rectal
therapy
L sided
Maintainoral 5-ASA
adequate Considerincreased dose
Responseinadequate
Oral steroidResponse inadequate
Oral 5-ASA Response inadequate
Responseadequate
Maintain
Ulcerative Colitis: Moderate to SevereUlcerative Colitis: Moderate to Severe
Moderate
Inadequate response ConsideInadequate response
Severe
Oral steroid
Taper
Successfu
Adequate response
Unsuccessful
IV Steroid
6MP/AZA
Succes
Response
Failure
rCyA
No response
Inflixim
No response
l
Maintain on
5-ASA and observe
s
Maintain6-MP/AZA
Colectomy
InfliximabResponse
Maintaininfliximab
12/04/2012
31
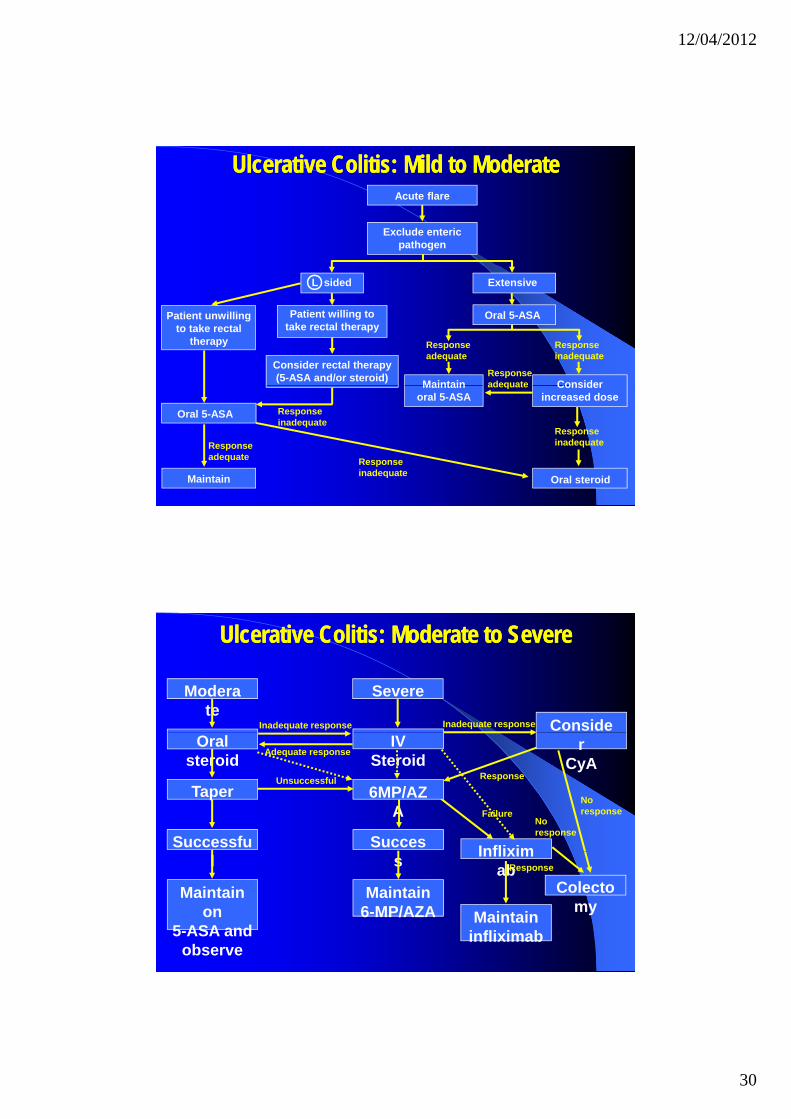
Final PointsFinal PointsThere is no “one size fits all” to IBD therapy– Therapy and decision making are tailored to the py g
individualAlgorithms are based upon available evidence– Evidence is in constant flux
Success of algorithms depends upon optimization of each step of therapy andoptimization of each step of therapy and considerable judgment about each outcome– Skillful application of medical therapy makes all the
difference in outcomes
THERAPY ULCERATIVE THERAPY ULCERATIVE COLITISCOLITIS
12/04/2012
32
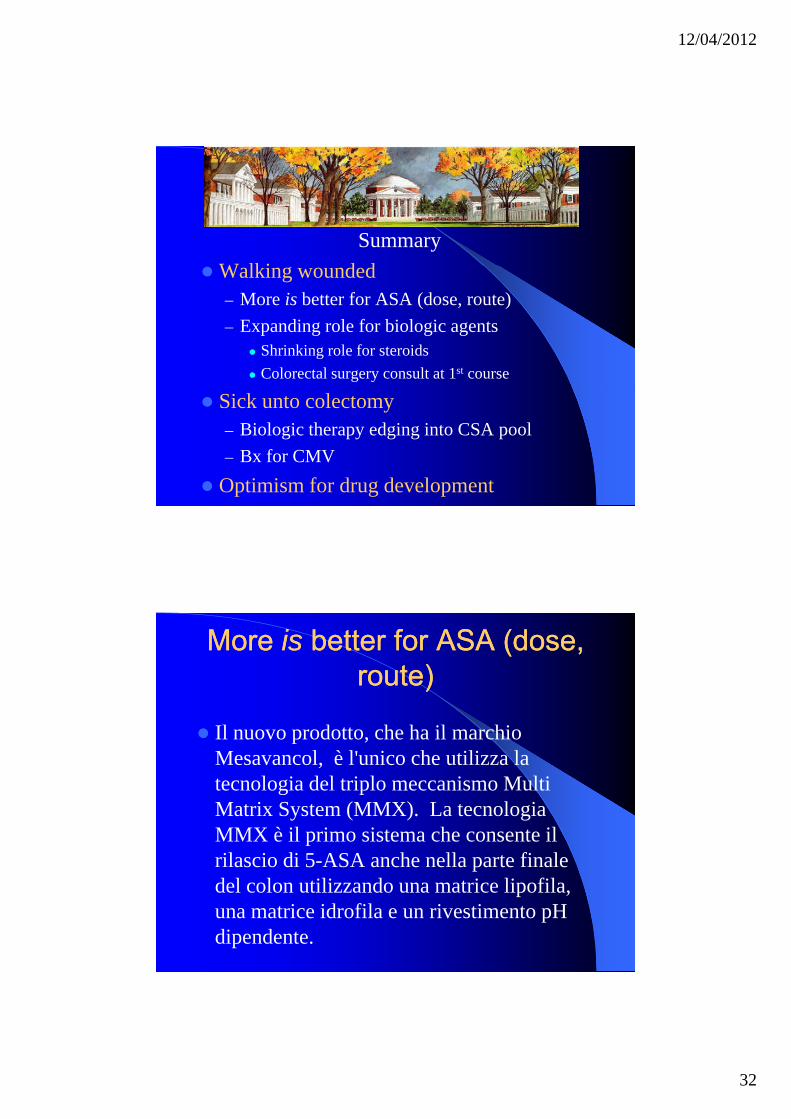
SummaryW lki d dWalking wounded– More is better for ASA (dose, route)– Expanding role for biologic agents
Shrinking role for steroidsColorectal surgery consult at 1st course
Sick unto colectomy– Biologic therapy edging into CSA pool– Bx for CMV
Optimism for drug development
More More isis better for ASA (dose, better for ASA (dose, route)route)
Il nuovo prodotto che ha il marchioIl nuovo prodotto, che ha il marchio Mesavancol, è l'unico che utilizza la tecnologia del triplo meccanismo Multi Matrix System (MMX). La tecnologia MMX è il primo sistema che consente il rilascio di 5-ASA anche nella parte finale del colon utilizzando una matrice lipofila, una matrice idrofila e un rivestimento pH dipendente.
12/04/2012
33
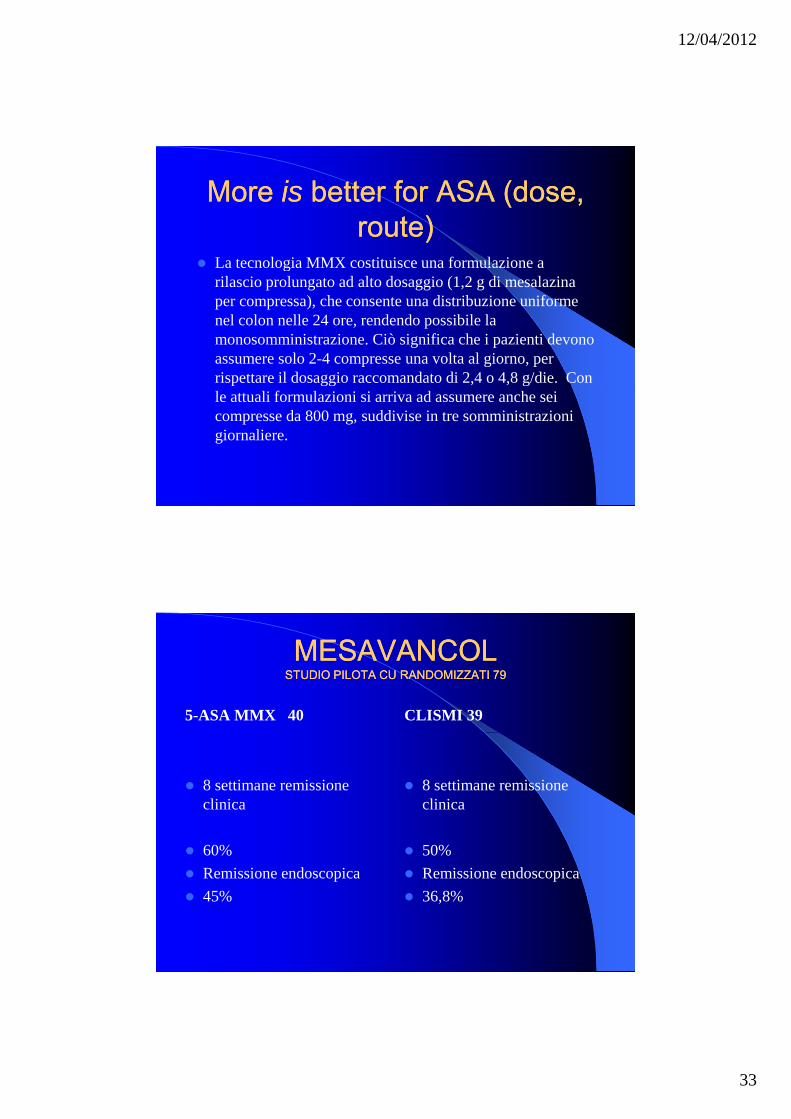
More More isis better for ASA (dose, better for ASA (dose, route)route)
La tecnologia MMX costituisce una formulazione aLa tecnologia MMX costituisce una formulazione a rilascio prolungato ad alto dosaggio (1,2 g di mesalazina per compressa), che consente una distribuzione uniforme nel colon nelle 24 ore, rendendo possibile la monosomministrazione. Ciò significa che i pazienti devono assumere solo 2-4 compresse una volta al giorno, per rispettare il dosaggio raccomandato di 2,4 o 4,8 g/die. Con p gg gle attuali formulazioni si arriva ad assumere anche sei compresse da 800 mg, suddivise in tre somministrazioni giornaliere.
MESAVANCOLMESAVANCOLSTUDIO PILOTA CU RANDOMIZZATI 79STUDIO PILOTA CU RANDOMIZZATI 79
5-ASA MMX 40 CLISMI 39
8 settimane remissione clinica
60%
8 settimane remissione clinica
50%60%Remissione endoscopica45%
50%Remissione endoscopica36,8%
12/04/2012
34
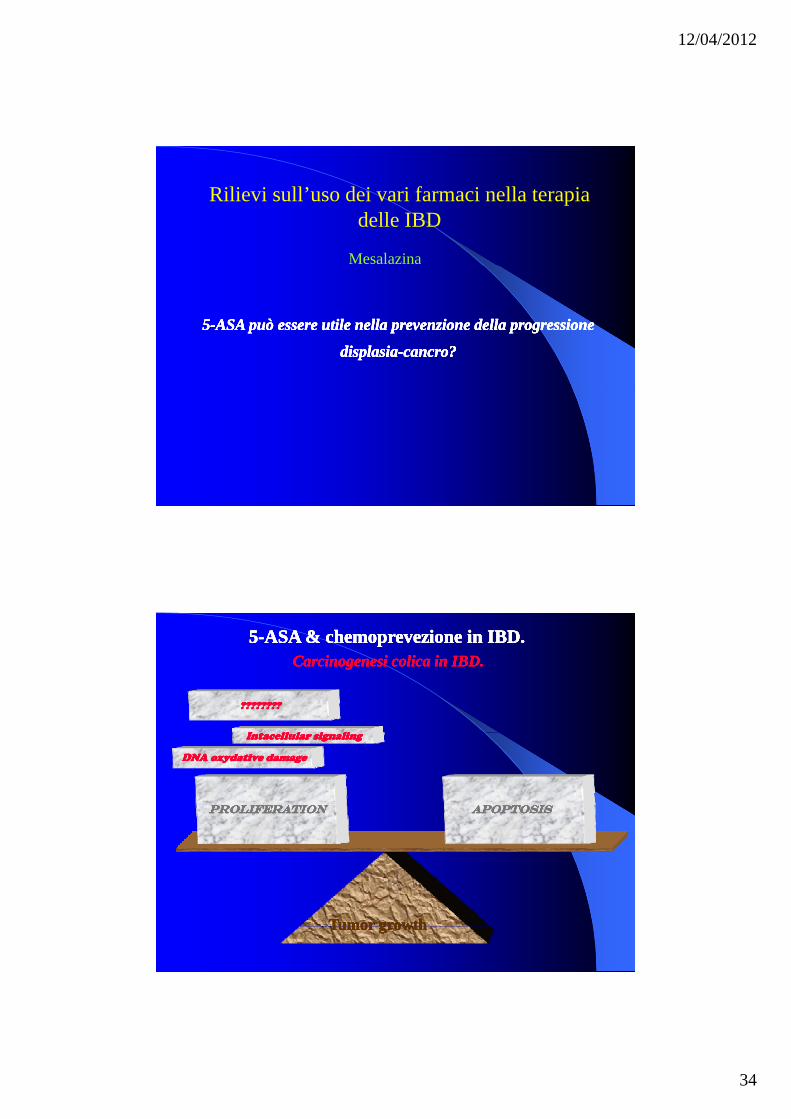
Rilievi sull’uso dei vari farmaci nella terapia delle IBD
Mesalazina
55--ASA può essere utile nella prevenzione della progressione ASA può essere utile nella prevenzione della progressione
displasiadisplasia--cancro?cancro?
55--ASA può essere utile nella prevenzione della progressione ASA può essere utile nella prevenzione della progressione
displasiadisplasia--cancro?cancro?
I ll l i liI ll l i liI ll l i liI ll l i li
????????????????????????????????
55--ASA & chemoprevezione in IBD.ASA & chemoprevezione in IBD.Carcinogenesi colica in IBD.Carcinogenesi colica in IBD.
55--ASA & chemoprevezione in IBD.ASA & chemoprevezione in IBD.Carcinogenesi colica in IBD.Carcinogenesi colica in IBD.
DNA oxydative damageDNA oxydative damageDNA oxydative damageDNA oxydative damage
Intacellular signalingIntacellular signalingIntacellular signalingIntacellular signaling
ProliferationProliferationProliferationProliferation ApoptosisApoptosisApoptosisApoptosis
Tumor growthTumor growthTumor growthTumor growth
12/04/2012
35
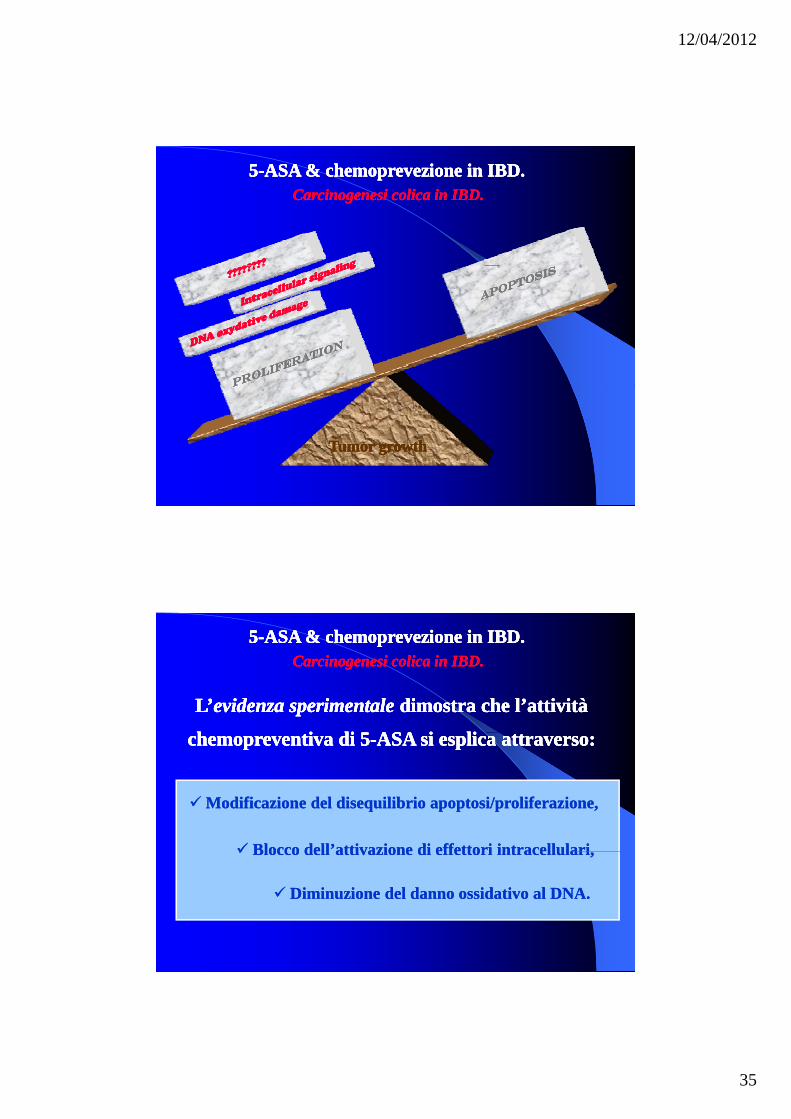
55--ASA & chemoprevezione in IBD.ASA & chemoprevezione in IBD.Carcinogenesi colica in IBD.Carcinogenesi colica in IBD.
55--ASA & chemoprevezione in IBD.ASA & chemoprevezione in IBD.Carcinogenesi colica in IBD.Carcinogenesi colica in IBD.
Tumor growthTumor growthTumor growthTumor growth
L’L’evidenzaevidenza sperimentalesperimentale dimostra che l’attività dimostra che l’attività
h i di 5h i di 5 ASA i liASA i li
L’L’evidenzaevidenza sperimentalesperimentale dimostra che l’attività dimostra che l’attività
h i di 5h i di 5 ASA i liASA i li
55--ASA & chemoprevezione in IBD.ASA & chemoprevezione in IBD.Carcinogenesi colica in IBD.Carcinogenesi colica in IBD.
55--ASA & chemoprevezione in IBD.ASA & chemoprevezione in IBD.Carcinogenesi colica in IBD.Carcinogenesi colica in IBD.
chemopreventiva di 5chemopreventiva di 5--ASA si esplica attraverso:ASA si esplica attraverso:chemopreventiva di 5chemopreventiva di 5--ASA si esplica attraverso:ASA si esplica attraverso:
Modificazione del disequilibrio apoptosi/proliferazione,Modificazione del disequilibrio apoptosi/proliferazione,
Blocco dell’attivazione di effettori intracellulariBlocco dell’attivazione di effettori intracellulariBlocco dell attivazione di effettori intracellulari,Blocco dell attivazione di effettori intracellulari,
Diminuzione del danno ossidativo al DNA.Diminuzione del danno ossidativo al DNA.
12/04/2012
36
ANCORA ANCORA 0 0 MINUTI !!!MINUTI !!!
Questions?Questions?
12/04/2012
37
GRAZIE !!!GRAZIE !!!