Peroperative grading of pyuloric stenosis: A long term clinical and radiolgoical follow-up of...
4
Br. J. Surg. Vol. 65 (1978) 157-160 Peroperative grading of pyloric stenosis : a long term clinical and radiological follow-up of patients with severe pyloric stenosis treated by highly selective vagotomy and dilatation of the stricture PETER DELANEY* Highly selective vagotomy (HSV) is now an accepted form of surgery for uncomplicated duodenal ulcer. Highly selective vagotomy and dilatation has been successfully used in some cases of pyloric stenosis, but many would regard severe pyloric stenosis as a contra- indication to this procedure. Eleven patients with severe pyloric stenosis, measured objectively at operation, have been treated by HSV and dilatation of the stenosis and reviewedfor periods of up to 3 years. The clinical results, immediate and long term, were good in all cases. Barium studies and histo- pathological findings were slower to return to normal. With intensive preoperative preparation to restore the tone of the dilated gastric muscle and gentle, controlled dilatation of the stricture, HSV in these patients should be as satisfactory as in those patients with uncomplicated duodenal ulcer. HIGHLY selective vagotomy (HSV) is now an accepted operation for the treatment of uncomplicated duodenal ulcer. However, the role of this operation in the management of pyloric stenosis is not so clear cut. Although HSV and dilatation has been used success- fully in treating mild and moderate cases of pyloric stenosis (McMahon et a]., 1976), severe stenosis would still be regarded by many as a contraindication to this form of management. This paper presents the results of a 3-year clinical and radiological follow-up of 11 patients with severe, advanced pyloric stenosis secondary to chronic duodenal ulcer who were treated by HSV and dilata- tion of the stenosis. Patients and methods SUMMARY The diagnosis of severe pyloric stenosis was made only when the following three criteria were fulfilled: 1. Clinical: typical copious vomiting and significant weight loss, with or without visible peristalsis and succussion splash. 2. Radiological: large volume of resting gastric juice, big, dilated stomach and marked delay in emptying. 3. Peroperative grading: stricture less than 9 mm in diameter. Details of the patients are set out in Table I. The outstanding symptom was severe vomiting, which was responsible for most of the patients seeking hospital admission. Constant, severe pain was also a prominent feature. As expected, the average age was older and the duration of symptoms longer than in patients with uncomplicated ulcers presenting for elective surgery. The patients were managed initially by nasogastric suction, saline gastric lavage and intravenous fluids for 5-8 days before surgery. Four were severely dehydrated and had hypochloraemic alkalosis and one had clinical tetany. All the patients had severe pyloric stenosis by the radiological standards of Kreel and Ellis (1965). Each patient had a gastro- scopy performed. The stenosis was not adequately visualized in most cases as it was distal to the pyloric sphincter which was deformed and markedly narrowed in all patients. No gastric ulcers were seen but gastric biopsies showed a severe degree of gastritis in each case. Operation was performed only when the patient’s metabolic condition had been stabilized and the grossly dilated stomach had recovered its muscle tone. Surgery When the duodenal ulcer had been confirmed, the stricture was evaluated through a gastrotomy which was made at least lOcm from the pylorus towards the greater curve of the stomach. The diameter of the stricture was measured using Bakes’ dilators and then gradually dilated to size 14 Bakes’ (1 1 mm). Thereafter it was a simple, atraumatic procedure to complete the dilatation digitally up to the distal interphalangeal joint of the index finger (15 mm). In no case was the duodenum perforated during this procedure. The gastrotomy was then closed using two layers of 2/0 chromic catgut. Highly selective vagotomy The neurectomy is started by introducing the left index finger through the lesser omentum on the outer side of the nerve of Latarjet and then passing it behind the nerve (Fig. I). This finger in the lesser sac can be brought forward between the lesser curve of the stomach and the nerve of Latarjet, and commencing dissection on to this finger greatly facilitates entry into the lesser sac. The gastrocolic omentum need not be opened. The lesser curve of the stomach does not seem to be much affected by the gastric hypertrophy in pyloric stenosis and the resection is started about the same distance from the pylorus as in uncomplicated duodenal ulcer. The neurectomy is started by taking the proximal limb of the ‘Crow’s foot’. The lesser curve is reperitonealized with 2/0 chromic catgut as the dissection proceeds and these sutures can be held long to provide gentle traction on the lesser curve of stomach, thereby making dissection of the neurovascular bundles much simpler (Fig. 2). Routine clearance of the lower 5 cm of the oesophagus and the posterior aspect of the fundus and body of the stomach complete the neurectomy. The phreno-oesophageal ligament is repaired with linen thread and the nasogastric tube is removed. Patients start oral fluids on waking. Results Clinical Early postoperative progress was satisfactory and the patients’ ability to retain liquids and then solid foods was reflected by weight gains in all. The longest follow-up was 38 months and the average 18 months. Because of the duration and severity of the preoperative symptoms, these patients were particularly satisfied with their results. There were no cases of bile vomiting, dumping or diarrhoea and there have been no recurrent ulcers to date. Appetite and weight soon returned to normal. Radiological X-ray changes did not keep pace with the immediate improvement in symptoms. Repeat barium meal examinations were done at 3, 6 and 12 months. While a marked improvement in the size of the stomach and the rate of gastric emptying was seen in the earlier * Department of Surgery, Trinity College, Dublin, Ireland.
-
Upload
peter-delaney -
Category
Documents
-
view
217 -
download
0
Transcript of Peroperative grading of pyuloric stenosis: A long term clinical and radiolgoical follow-up of...

Br. J. Surg. Vol. 65 (1978) 157-160
Peroperative grading of pyloric stenosis : a long term clinical and radiological follow-up of patients with severe pyloric stenosis treated by highly selective vagotomy and dilatation of the stricture P E T E R D E L A N E Y *
Highly selective vagotomy (HSV) is now an accepted form of surgery for uncomplicated duodenal ulcer. Highly selective vagotomy and dilatation has been successfully used in some cases of pyloric stenosis, but many would regard severe pyloric stenosis as a contra- indication to this procedure.
Eleven patients with severe pyloric stenosis, measured objectively at operation, have been treated by HSV and dilatation of the stenosis and reviewed for periods of up to 3 years. The clinical results, immediate and long term, were good in all cases. Barium studies and histo- pathological findings were slower to return to normal.
With intensive preoperative preparation to restore the tone of the dilated gastric muscle and gentle, controlled dilatation of the stricture, HSV in these patients should be as satisfactory as in those patients with uncomplicated duodenal ulcer.
HIGHLY selective vagotomy (HSV) is now an accepted operation for the treatment of uncomplicated duodenal ulcer. However, the role of this operation in the management of pyloric stenosis is not so clear cut. Although HSV and dilatation has been used success- fully in treating mild and moderate cases of pyloric stenosis (McMahon et a]., 1976), severe stenosis would still be regarded by many as a contraindication to this form of management.
This paper presents the results of a 3-year clinical and radiological follow-up of 11 patients with severe, advanced pyloric stenosis secondary to chronic duodenal ulcer who were treated by HSV and dilata- tion of the stenosis.
Patients and methods
SUMMARY
The diagnosis of severe pyloric stenosis was made only when the following three criteria were fulfilled:
1. Clinical: typical copious vomiting and significant weight loss, with or without visible peristalsis and succussion splash.
2. Radiological: large volume of resting gastric juice, big, dilated stomach and marked delay in emptying.
3. Peroperative grading: stricture less than 9 mm in diameter. Details of the patients are set out in Table I. The outstanding
symptom was severe vomiting, which was responsible for most of the patients seeking hospital admission. Constant, severe pain was also a prominent feature. As expected, the average age was older and the duration of symptoms longer than in patients with uncomplicated ulcers presenting for elective surgery. The patients were managed initially by nasogastric suction, saline gastric lavage and intravenous fluids for 5-8 days before surgery. Four were severely dehydrated and had hypochloraemic alkalosis and one had clinical tetany. All the patients had severe pyloric stenosis by the radiological standards of Kreel and Ellis (1965). Each patient had a gastro- scopy performed. The stenosis was not adequately visualized in most cases as it was distal to the pyloric sphincter which was deformed and markedly narrowed in all patients. No gastric ulcers were seen but gastric biopsies showed a severe degree of gastritis in each case.
Operation was performed only when the patient’s metabolic condition had been stabilized and the grossly dilated stomach had recovered its muscle tone.
Surgery When the duodenal ulcer had been confirmed, the stricture was evaluated through a gastrotomy which was made at least lOcm from the pylorus towards the greater curve of the stomach. The diameter of the stricture was measured using Bakes’ dilators and then gradually dilated to size 14 Bakes’ (1 1 mm). Thereafter it was a simple, atraumatic procedure to complete the dilatation digitally up to the distal interphalangeal joint of the index finger (15 mm). In no case was the duodenum perforated during this procedure. The gastrotomy was then closed using two layers of 2/0 chromic catgut.
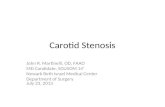
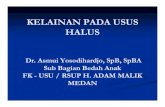
Highly selective vagotomy The neurectomy is started by introducing the left index finger through the lesser omentum on the outer side of the nerve of Latarjet and then passing it behind the nerve (Fig. I). This finger in the lesser sac can be brought forward between the lesser curve of the stomach and the nerve of Latarjet, and commencing dissection on to this finger greatly facilitates entry into the lesser sac. The gastrocolic omentum need not be opened. The lesser curve of the stomach does not seem to be much affected by the gastric hypertrophy in pyloric stenosis and the resection is started about the same distance from the pylorus as in uncomplicated duodenal ulcer. The neurectomy is started by taking the proximal limb of the ‘Crow’s foot’. The lesser curve is reperitonealized with 2/0 chromic catgut as the dissection proceeds and these sutures can be held long to provide gentle traction on the lesser curve of stomach, thereby making dissection of the neurovascular bundles much simpler (Fig. 2). Routine clearance of the lower 5 cm of the oesophagus and the posterior aspect of the fundus and body of the stomach complete the neurectomy. The phreno-oesophageal ligament is repaired with linen thread and the nasogastric tube is removed. Patients start oral fluids on waking.
Results Clinical Early postoperative progress was satisfactory and the patients’ ability to retain liquids and then solid foods was reflected by weight gains in all.
The longest follow-up was 38 months and the average 18 months. Because of the duration and severity of the preoperative symptoms, these patients were particularly satisfied with their results. There were no cases of bile vomiting, dumping or diarrhoea and there have been no recurrent ulcers to date. Appetite and weight soon returned to normal.
Radio logical X-ray changes did not keep pace with the immediate improvement in symptoms. Repeat barium meal examinations were done at 3, 6 and 12 months. While a marked improvement in the size of the stomach and the rate of gastric emptying was seen in the earlier
* Department of Surgery, Trinity College, Dublin, Ireland.

158 Peter Delaney
Table 1: PATIENTS WITH SEVERE PYLORlC STENOSlS: CLINICAL, RADIOLOGICAL, ENDOSCOPIC AND OPERATIVE FINDINGS
Peroperative assessment of
Duration of diameter of Age symptoms Weight Past Barium Endoscopy stricture
Sex (yr) (yr) V VP SS loss (kg) history studies findings (mm) M
M
F
M
M
F
M
M
M
F
M
58
35
48
53
58
55
41
60
43
60
54
22
6
8
20
23
13
18
15
19
13
27
++ ++ ++ ++ ++ ++ ++ ++ ++ ++ ++
10
7
6
12
13
5
10
7
8
7
10
Perforation
- Perforation
Perforation
Perforation
Perforation
Perforation
- -
-
-
PS, gross dilatation
PS, dilated stomach
PS, dilated stomach
PS, gross dilatation
PS, gross dilatation
PS, gross dilatation
PS, dilated stomach
PS, huge stomach
PS, dilated stomach
PS, gross dilatation
PS, gross dilatation
Tiny pylorus, severe gastritis
Small pylorus, gastritis
Small pylorus, gastritis
‘Pin hole’ pylorus, gastritis
Tiny pylorus, gastritis
Small pylorus, gastritis
Small pylorus, gastritis
Small pylorus, gastritis
Tiny pylorus, gastritis
Tiny pylorus, gastritis
Tiny pylorus, gastritis
5
5
5
5
5
5
5
7
9
8
8
V, Vomiting; VP, visible peristalsis; SS, succussion splash; PS, pyloric stenosis.
Fig. 1. The gastrotomy has been closed. The index finger in the lesser sac is brought forward between the nerve of Latarjet and the lesser curve. The dissection is started at this point.
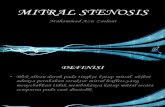
studies (3 and 6 months), it was not until 12 months that the films showed a complete reversal to normal. At this stage the stomach had regained a normal size and, on screening, gastric emptying and the move- ments of the antrum and pyloroduodenal canal were normal (Fig. 3).
Endoscopy Endoscopy was repeated at 3 and 6 months after surgery. No ulcers were seen, although slight duodenal deformity persisted. Gastric biopsy at 3 months in each case showed a moderate gastritis which con- tinued to improve but was still in evidence at 6 months and was classified then as mild.
Fig. 2. As the neurectomy proceeds, the lesser curve is reperitonealized with 2/0 chromic catgut. These sutures are held long to apply traction to the stomach. This makes dissection of the neurovascular bundles much easier.
While the follow-up is short in relation to recurrent ulcer, it is quite adequate in relation to recurrent stenosis. It is more than likely that if the stricture were to recur, it would do so quickly and certainly within the first 6 months (Johnston et al., 1973).
Discussion The evolution of surgery in the management of duodenal ulcer has reached yet another stage. Eleven years ago, Ellis said that ‘although vagotomy combined with gastric drainage is now a well-established procedure in the surgical treatment of duodenal ulcer, it has been suggested by a number of authorities that it is contraindicated in those cases which are complicated

Peroperative grading of pyloric stenosis 159
Q b
by pyloric stenosis’ (Ellis et al., 1966). He went on to state that the results in his series were uniformly good and recommended truncal vagotomy and drainage as the surgical treatment of choice for pyloric stenosis. Today, HSV could be substituted for truncal vagotomy and drainage in the above passage. The high incidence of complications such as diarrhoea, dumping and bile vomiting after gastric surgery is due to the destruction or bypass of the gastric emptying mechanism. Highly selective vagotomy, by preserving this mechanism, is associated with a much lower incidence of those complications. The results of 7-year follow-up of HSV in uncomplicated duodenal ulcer suggest that the incidence of recurrent ulcer is not likely to be any higher than with truncal vagotomy and drainage, and HSV is now accepted as a satisfactory method of treating duodenal ulcer.
Although there have been reports on the use of HSV and dilatation in varying degrees of pyloric stenosis (McMahon et al., 1976), there is still doubt about the use of this method in severe pyloric stenosis.
It is widely appreciated now that pyloric stenosis is in fact a duodenal stenosis and occurs just distal to the pyloric sphincter. In the majority of cases, the tightest part of the stricture occurs within 1 cm of the pylorus, which itself is normally about 15 mm in diameter (Kirk, 1970).
The earlier stages of pyloric stenosis, secondary to chronic duodenal ulcer, are characterized by gradual and massive hypertrophy of the gastric musculature. This increasingly powerful emptying unit is capable of overcoming the progressive stenosis for a long time, this being the compensated phase of pyloric stenosis. Later on, when the stenosis inevitably becomes too tight, the stomach begins to dilate. This, the decom- pensated phase of pyloric stenosis, gives rise to the classic clinical picture of late pyloric stenosis.
The superior results of HSV in treating uncompli- cated duodenal ulcer are due to the preservation of the normal emptying mechanism of the stomach. In severe
C
Fig. 3. Barium studies on the same patient. a, Preoperative 2-h film showing a huge, dilated stomach with gross delay in emptying. b, Twelve months postoperatively there is a normal stomach with no delay in emptying and c, normal filling and emptying of the pyloroduodenal channel. There is no ulcer.
pyloric stenosis it would be most illogical to destroy this emptying unit, which has become even bigger and more powerful than normal.
If HSV and dilatation is to be adopted as an acceptable operation for severe pyloric stenosis, the following points must be borne in mind:

160 Peter Delaney
1. The preoperative work-up of these patients will become vital. Sufficient time must be spent on naso- gastric suction and gastric lavage to allow the stomach to recover its tone before surgery. Otherwise, the post- operative period will be complicated by prolonged gastric atony which will eventually require a drainage procedure.
2. The degree of stenosis may become critical in deciding which cases are suitable for this procedure, and a satisfactory method of objectively measuring the diameter of the stricture is required. The Bakes’ dilators seem admirably suited to this task. They are malleable and can be shaped to ‘fit’ the pyloro- duodenal canal. Because of their shape, it is easier to ‘feel’ the stenosis and to appreciate when the stricture has been passed. This lessens the chance of duodenal rupture which may occur with digital dilatation alone and occurred in 25 per cent of cases in a recent series (McMahon et al., 1976). However, in these cases, the tear was easily repaired and was not associated with any increased morbidity.
The technique of duodenoplasty with HSV in the management of severe pyloric stenosis is attractive. In his series, Kennedy was able to carry out a duodeno- plasty of 2-6cm in length without destroying the sphincter because the stenosis was sufficiently distal in the duodenum to allow this (Kennedy, 1976). In this present series, however, the tightest part of the stricture was so close to the pylorus that duodenoplasty would not have been possible.
Results to date of HSV and dilatation in the management of severe pyloric stenosis are promising.
A clinical trial, randomized and prospective, is now needed to establish whether this method is superior in these cases to the more widely accepted procedure of truncal vagotomy and drainage. These patients would benefit from preservation of the emptying mechanism of the stomach just as much as those patients who have duodenal ulcer without stenosis.
References ELLIS H., STARER F., VENABLES c. et al. (1966) Clinical and
radiological study of vagotomy and gastric drainage in the treatment of pyloric stenosis due to duodenal ulcer. Gut 7, 671-676.
JOHNSTON D., LYNDON P. J., SMITH R. B. et al. (1973) Highly selective vagotomy without a drainage procedure in the treatment of haemorrhage, perforation, and pyloric stenosis due to peptic ulcer. Br. J . Surg. 60, 790-797.
KENNEDY T. (1976) Duodenoplasty with proximal gastric vagotomy. Ann. R . Coll. Surg. Engl. 58, 144-146.
KIRK R. M. (1970) The size of the pyloro-duodenal canal: its relation to the cause and treatment of peptic ulcer. Proc. R . SOC. Med. 63,944-946.
KREEL L. and ELLIS H. (1965) Pyloric stenosis in adults: a clinical and radiological study of 100 consecutive patients. Gut 6, 253-261.
MCMAHON M. J., GREENALL M. J. , JOHNSTON D. et al. (1976) Highly selective vagotomy plus dilatation of the stenosis compared with truncal vagotomy and drainage in the treatment of pyloric stenosis secondary to duodenal ulcer. Gut 17, 471-476.
Paper accepted 12.10.1977.