PERIPHERAL REGIONAL BLOCKS - Allegheny … · · 2017-05-22• Peripheral regional blocks can be...
124
PERIPHERAL REGIONAL BLOCKS by Mike DeBroeck, DNP, CRNA
Transcript of PERIPHERAL REGIONAL BLOCKS - Allegheny … · · 2017-05-22• Peripheral regional blocks can be...
PERIPHERAL REGIONAL BLOCKS
by
Mike DeBroeck, DNP, CRNA
Why am I bothering with
this topic at all?
Do CRNAs REALLY
even do peripheral
regional anesthetics?

YES!!!!!!!

TOPICS
• GENERAL INFO
• SUCCESS RATES
• COMPLICATIONS
• LA CHOICE
• SPECIFIC BLOCKS

General Information
How do we use them?
• Peripheral regional blocks can be used as
primary or adjunct anesthesia for virtually
any surgery to the upper or lower
extremities.
• They are also useful for airway
management, abdominal surgeries,
maxilla-facial/cranial surgeries, neck
surgeries, eye surgeries, and plastics
procedures.

KEYS TO
SUCCESS…
KNOW THE
PHYSICAL
ANATOMY!!!!
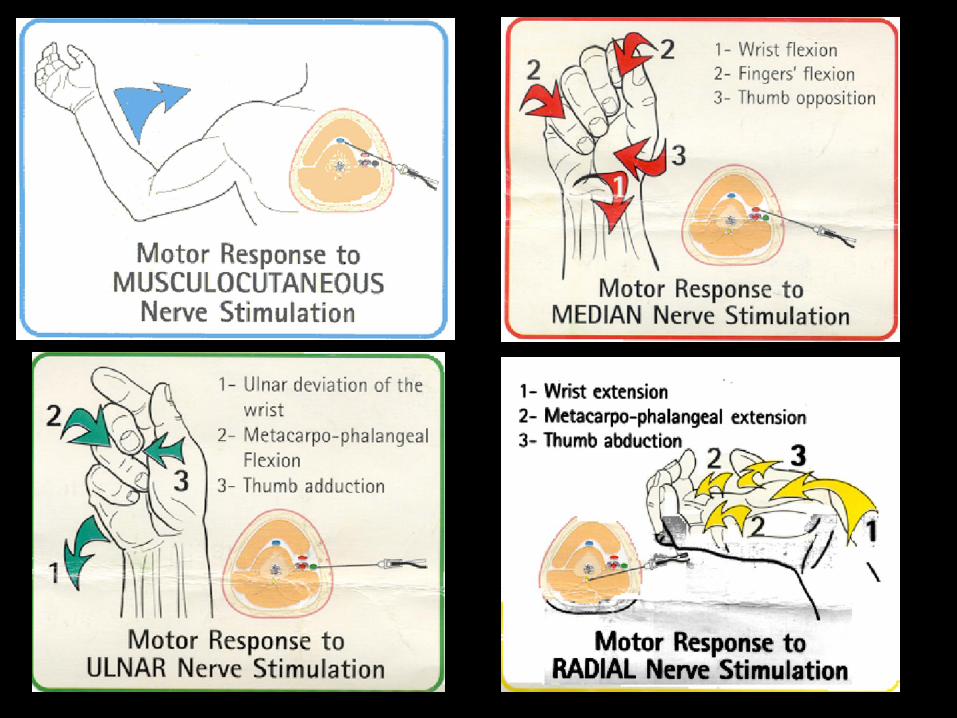
KNOW THE
SENSORY/MOTOR
INNERVATIONS!!!

GET COMFORTABLE WITH
ULTRASOUND
LEARN HOW TO USE A
NERVE STIMULATING
NEEDLE PROPERLY

MANAGE TIME

EDUCATE SURGEONS
EDUCATE THE STAFF

EDUCATE PATIENTS

SUCCESS RATES
SO, HOW GOOD ARE
THEY, REALLY?

SUCCESS RATES FOR MOST
SINGLE SHOT BLOCKS, WHEN
PERFORMED WITH THE PROPER
TECHNIQUE, EQUIPMENT, AND
TRAINING WILL RUN INTO THE
90% RANGE.
INDWELLING DEVICES HAVE A
SLIGHTLY LOWER SUCCESS RATE.
INDIVIDUAL SUCCESS
RATES TEND TO PARALLEL
PROPER USE OF
EQUIPMENT, PROPER
TECHNIQUE, AND
ADEQUACY OF TRAINING

COMPLICATIONS
• Local anesthetic systemic toxicity– Intravascular injection
– Choice of LA
• Neurotoxicity/Nerve injury– Intraneuronal injection
• Patchy block
• Block failure

SO WHY DON’T WE USE
THEM MORE?

WE’RE TOO LATE
PUTTING THEM IN.
THIS IS A FUNCTION OF SCHEDULING
WE DON’T WAIT LONG
ENOUGH FOR THEM TO SET
UP
THIS, TOO, IS MOSTLY A FUNCTION OF
SCHEDULING
WE’RE TOO SLOW
PERFORMING THE
PROCEDURES
This is a function of training and experience
”THE WAY YOU PRACTICE IS THE WAY YOU
PLAY”
LOCAL ANESTHETIC
CHOICE
PICK THE RIGHT DRUG FOR
THE RIGHT OUTCOME.
What are you trying to
accomplish?
• Quick onset?
• Long duration?
• Differential blockade?
• Adjunct to general or neuraxial
anesthesia?
• Post-op pain control?
• Sole anesthetic?
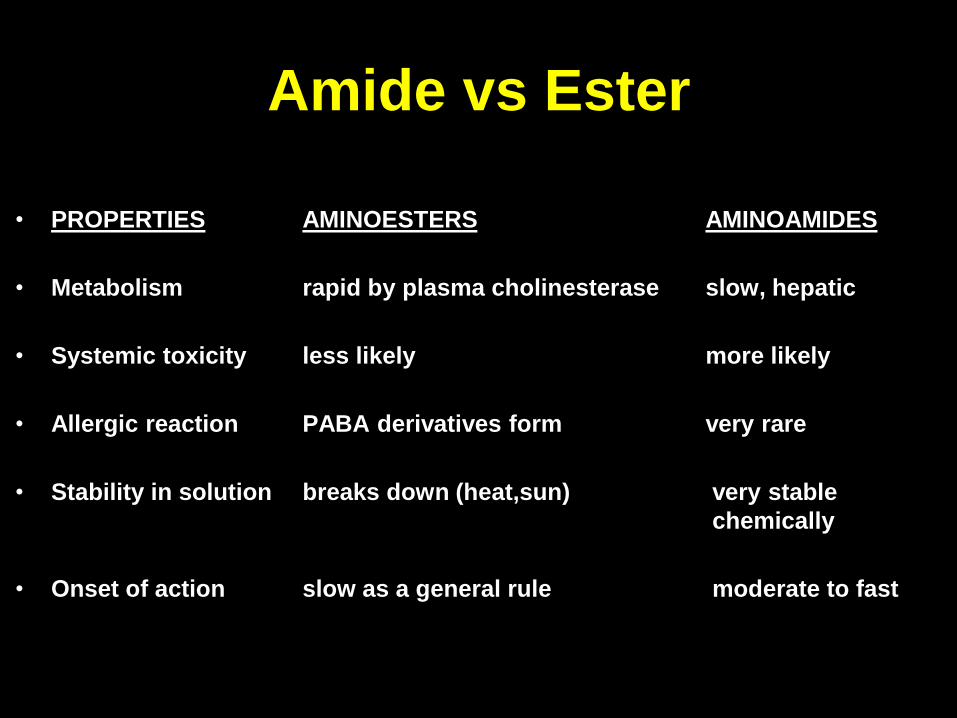
Amide vs Ester
• PROPERTIES AMINOESTERS AMINOAMIDES
• Metabolism rapid by plasma cholinesterase slow, hepatic
• Systemic toxicity less likely more likely
• Allergic reaction PABA derivatives form very rare
• Stability in solution breaks down (heat,sun) very stable
chemically
• Onset of action slow as a general rule moderate to fast
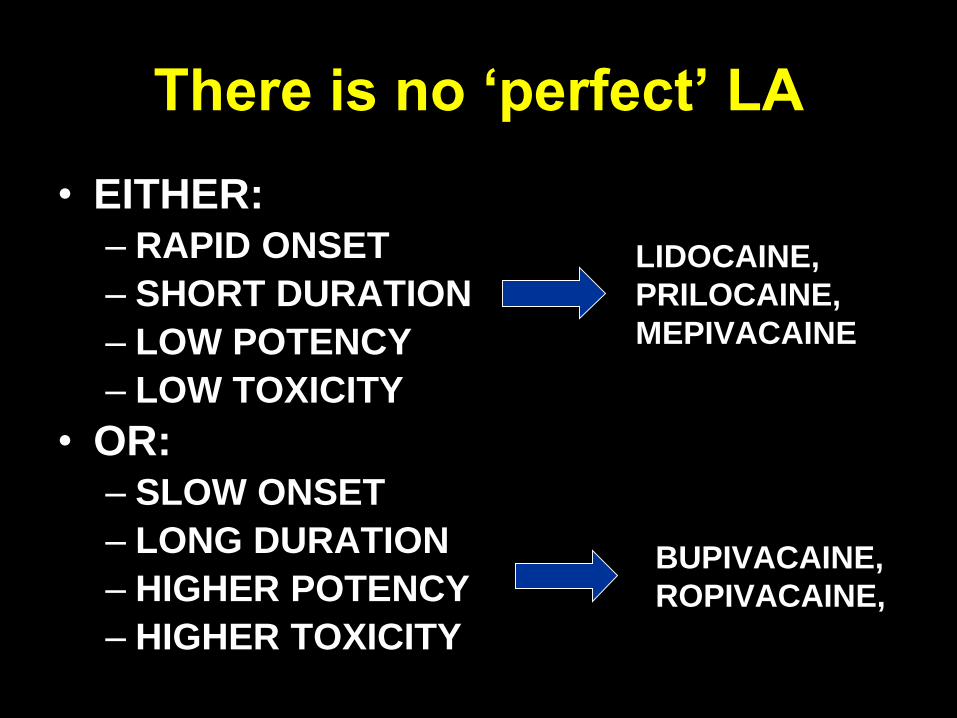
There is no ‘perfect’ LA
• EITHER:– RAPID ONSET
– SHORT DURATION
– LOW POTENCY
– LOW TOXICITY
• OR: – SLOW ONSET
– LONG DURATION
– HIGHER POTENCY
– HIGHER TOXICITY
LIDOCAINE,
PRILOCAINE,
MEPIVACAINE
BUPIVACAINE,
ROPIVACAINE,

Without epi with epi
Amide LA Max
Dosage/Concentration/Procedure
Recommendations
ADJUNCTS
• Epinephrine – 5 mcg/ml
• Clonidine - ∝2-adrenoceptor agonist***
– 100 mcg = 100 extra minutes
– More just gets more side effect
• Dexmedetomidine -- 0.75mcg – 1mcg/kg
– Faster onset, longer duration
• Dexamethasone – 1-2 mg vs 8-10 mg?
– Longer duration but neural toxicity?
BLOCKS
•BRACHIAL PLEXUS
•FEMORAL NERVE
•SCIATIC NERVE
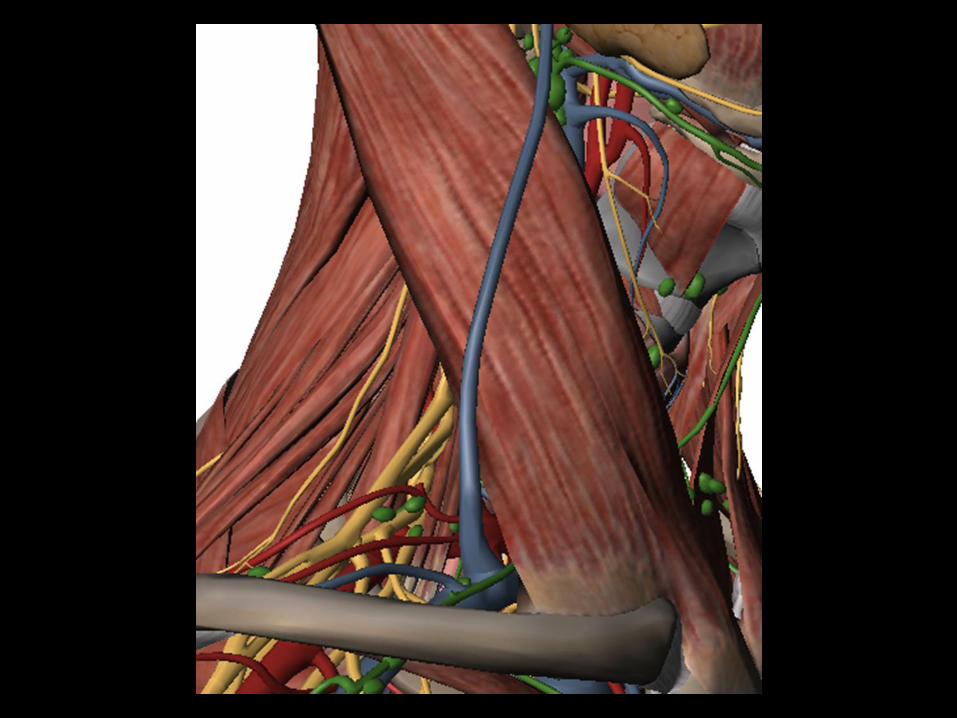
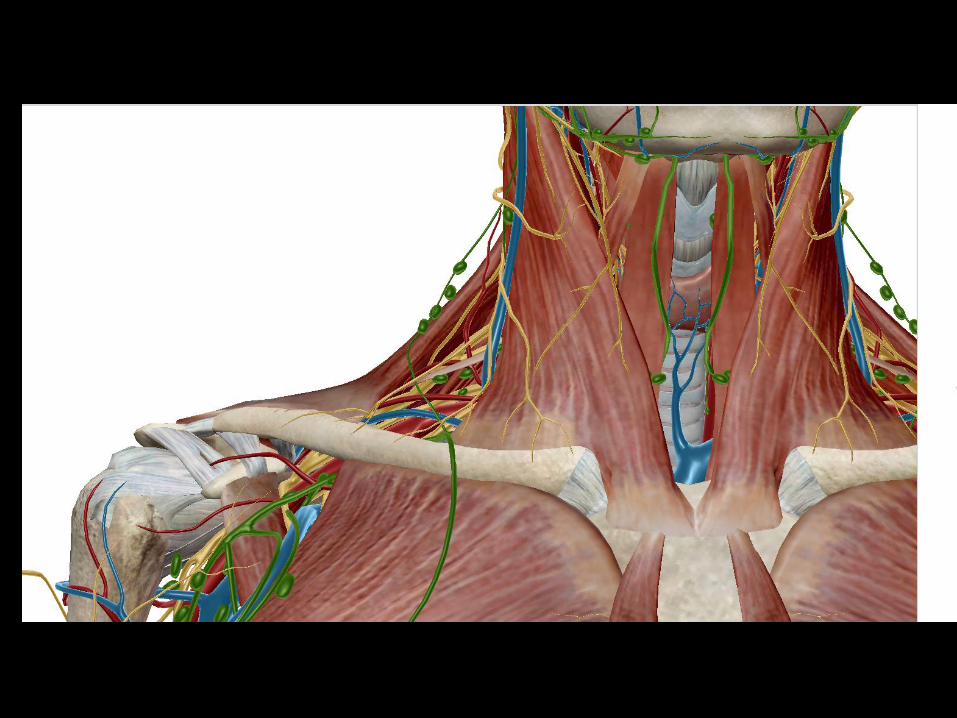
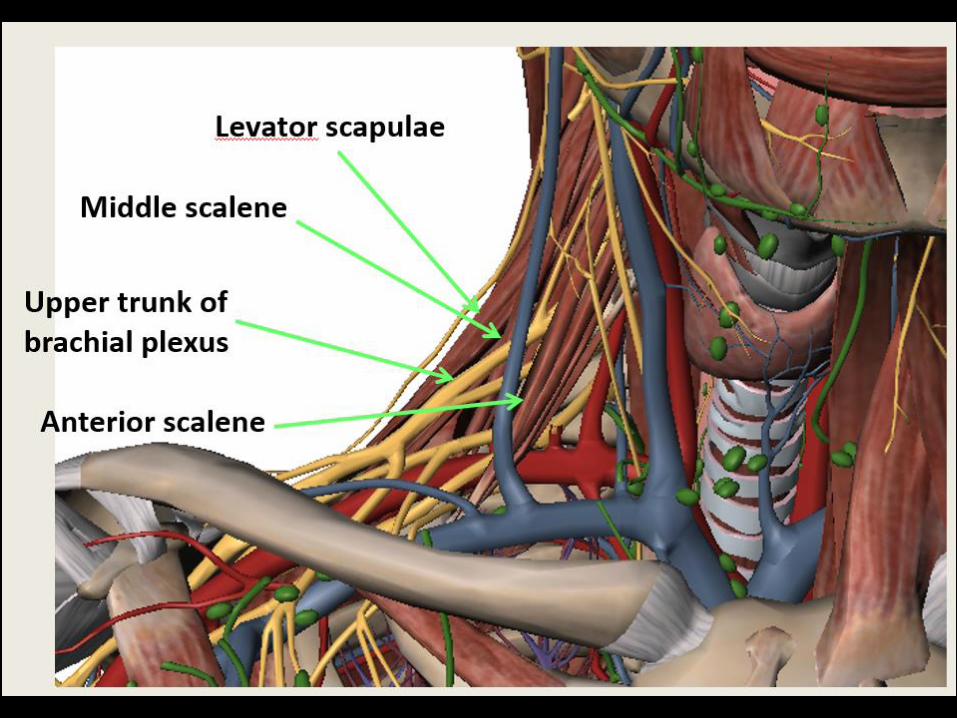
BRACHIAL PLEXUS
BLOCKS
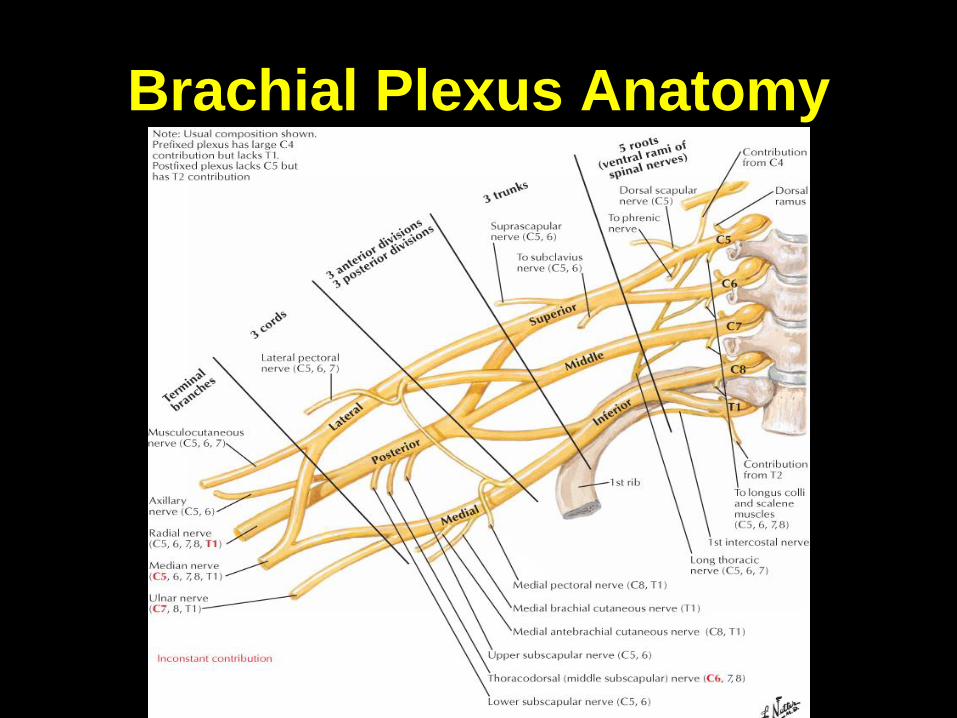
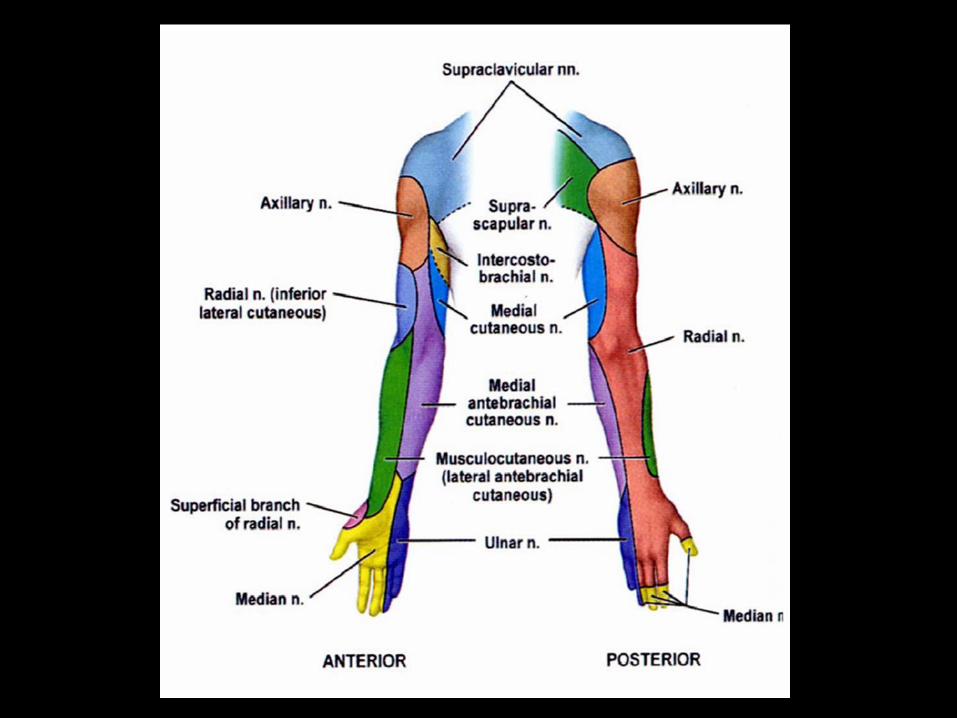
Brachial Plexus Anatomy

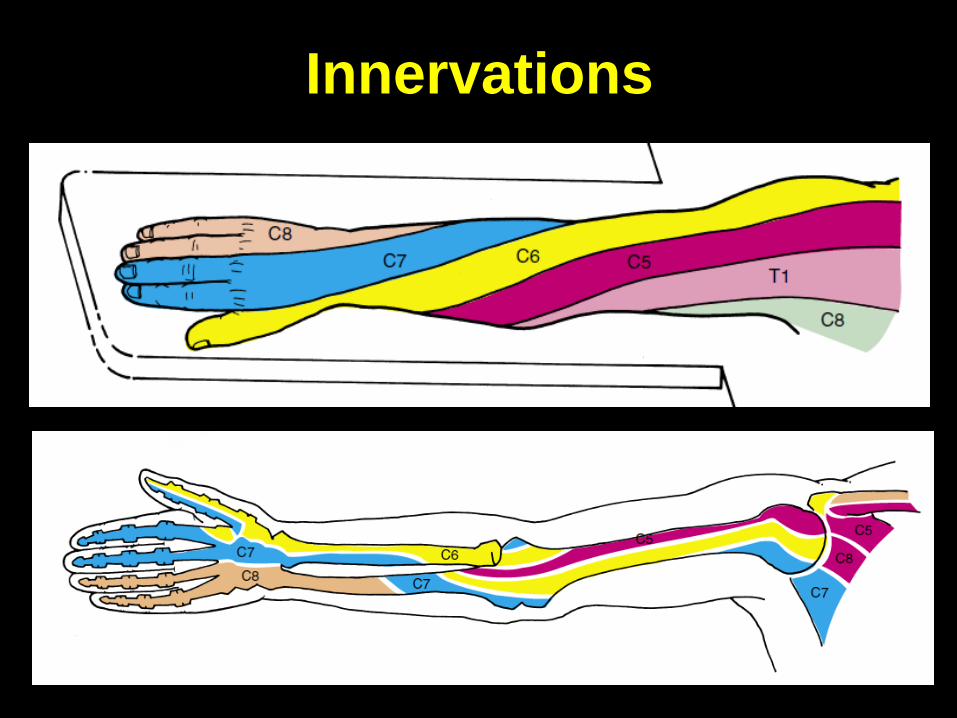
Innervations
Block Choices
• Interscalene
–High
–Low
• Supraclavicular
• Infraclavicular
• Axillary
• Mid-humeral/rescue blocks
• Wrist

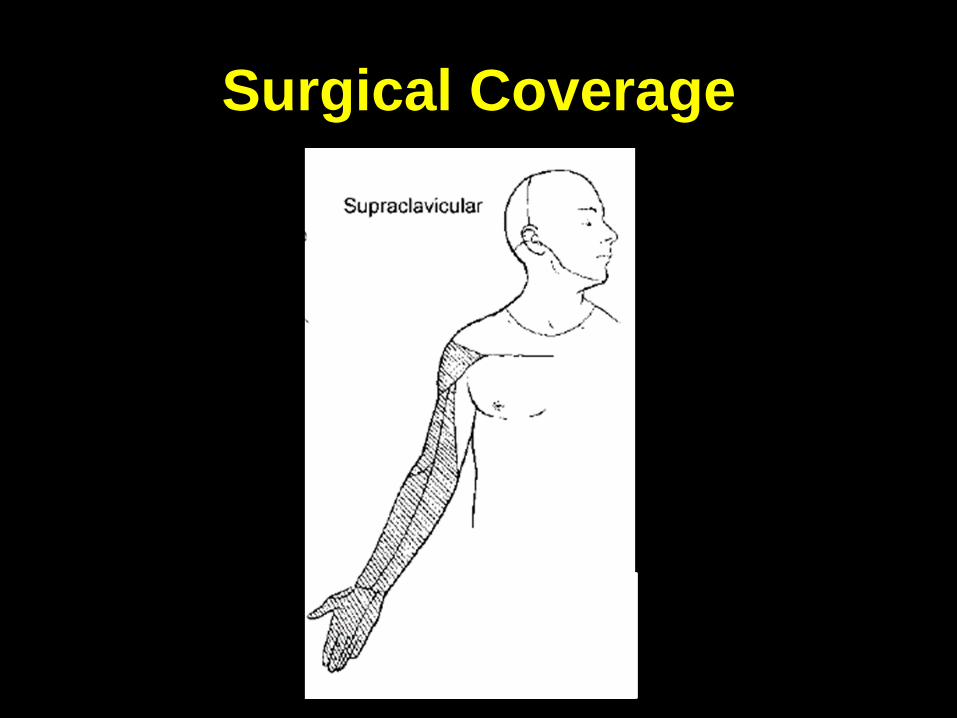
Interscalene


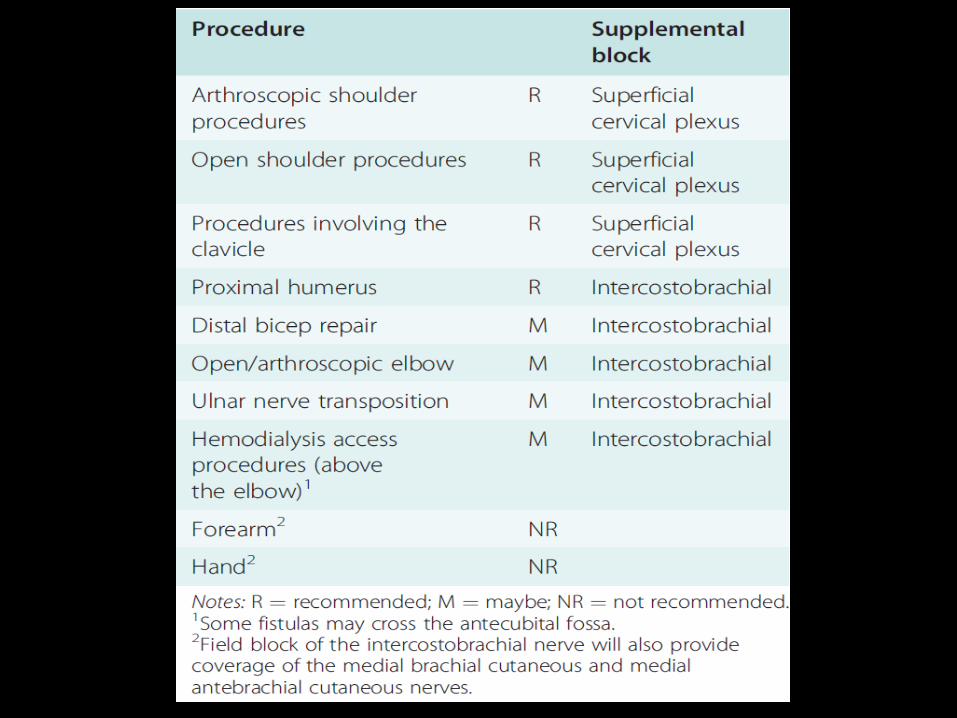
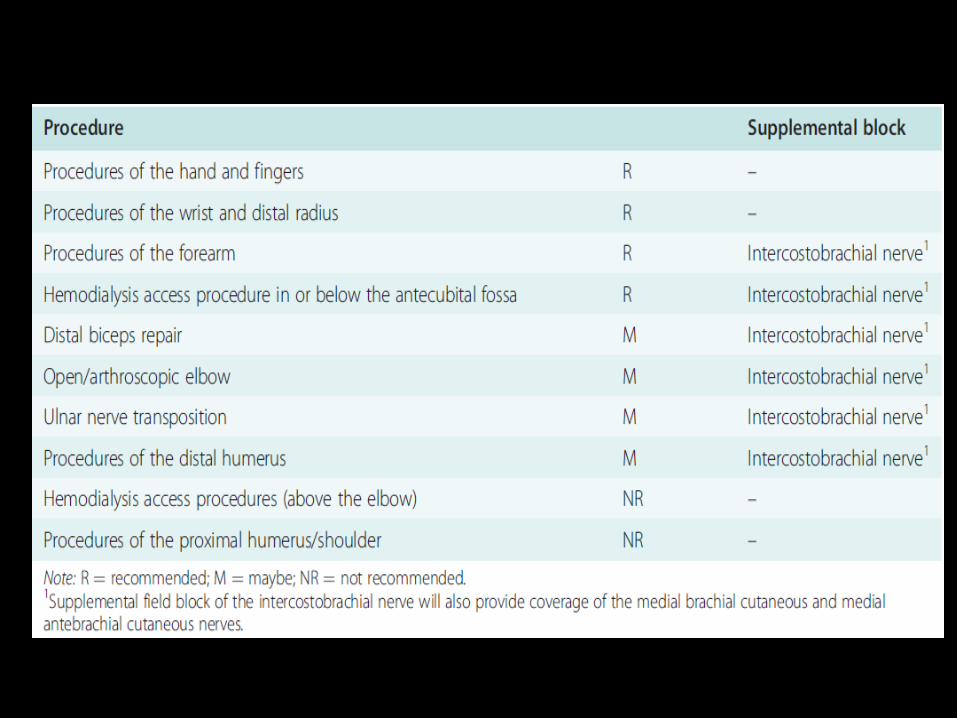
Surgical Coverage
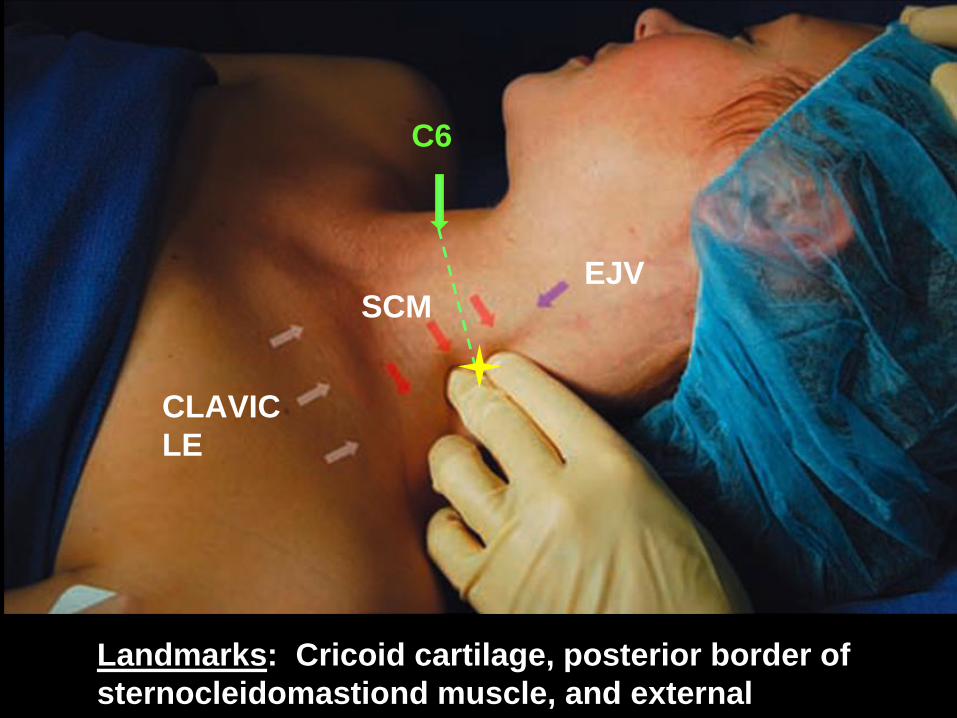
Landmarks: Cricoid cartilage, posterior border of
sternocleidomastiond muscle, and external
jugular vein
C6
EJVSCM
CLAVIC
LE
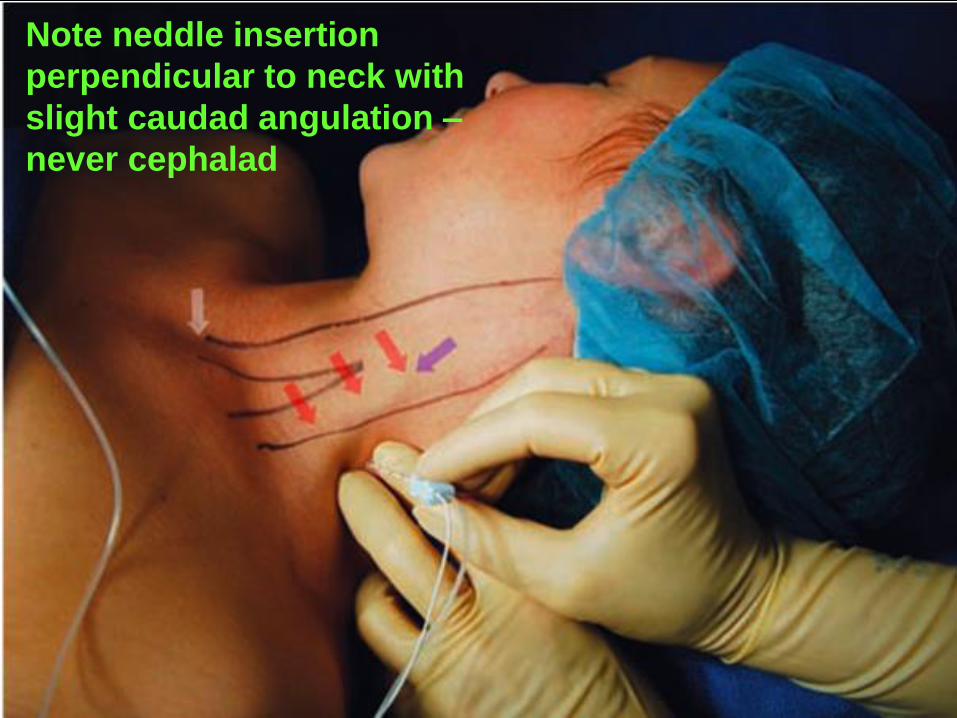
Note neddle insertion
perpendicular to neck with
slight caudad angulation –
never cephalad
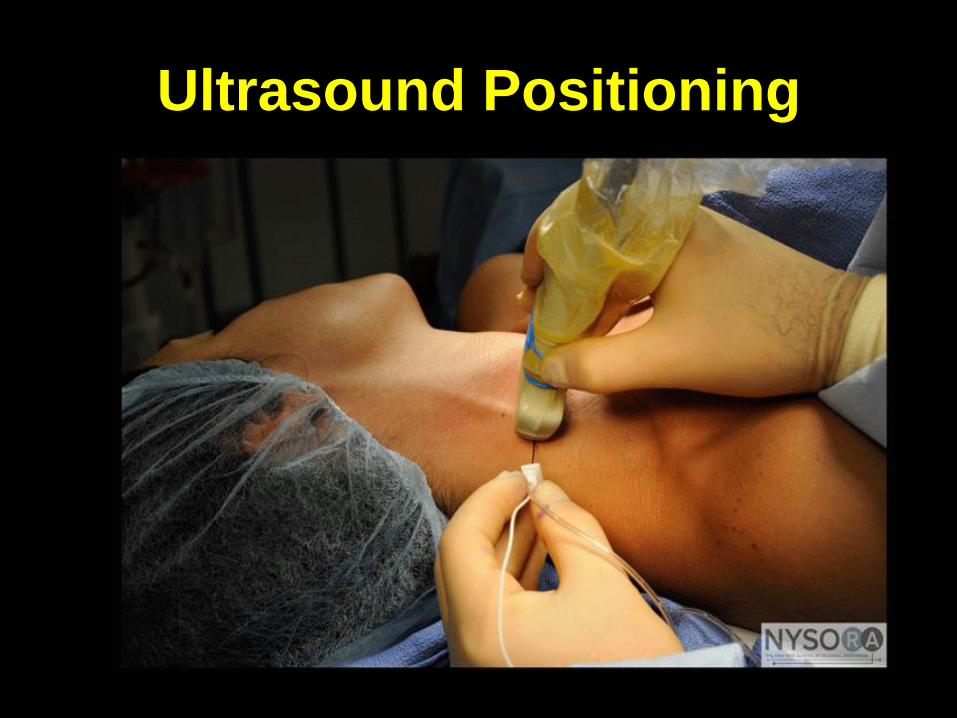
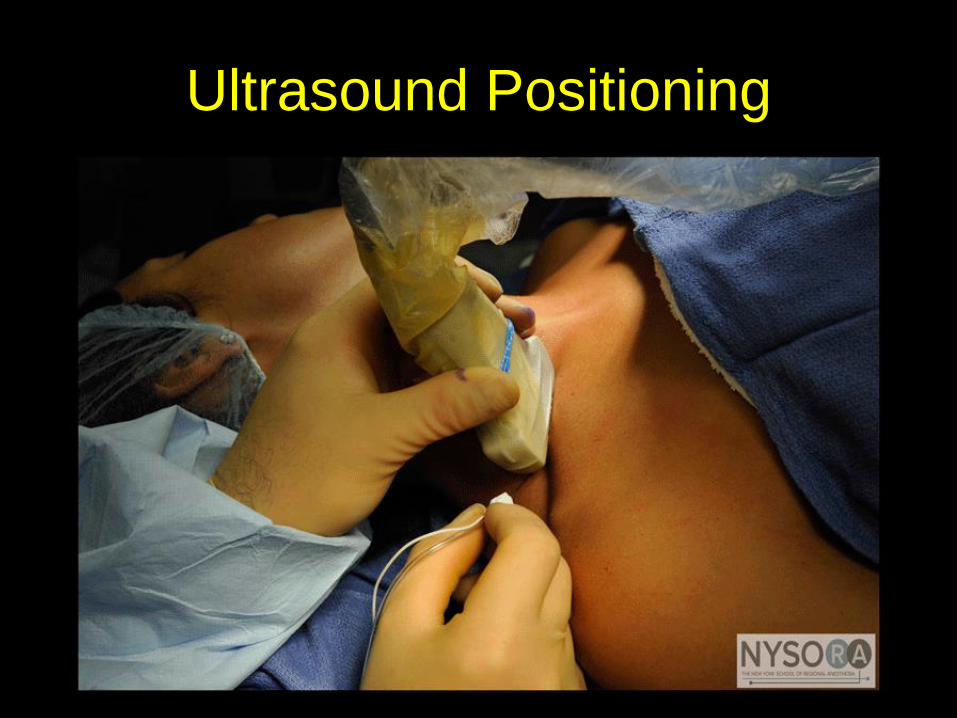
Ultrasound Positioning

Supraclavicular


Surgical Coverage
Surgical Coverage

Ultrasound Positioning

Infraclavicular
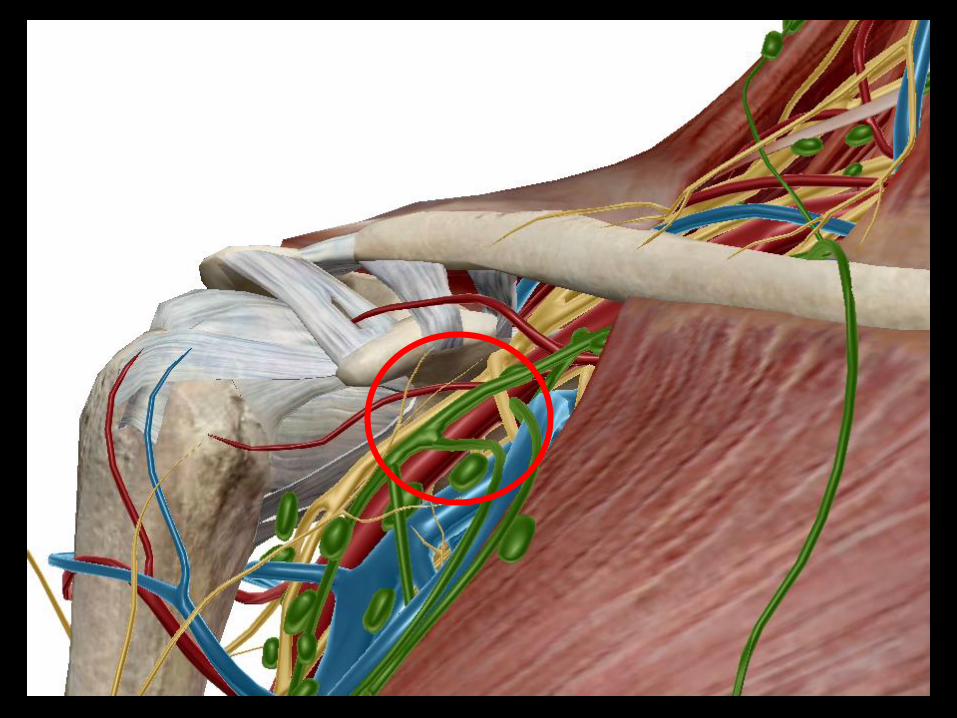

Surgical Coverage

Ultrasound Placement
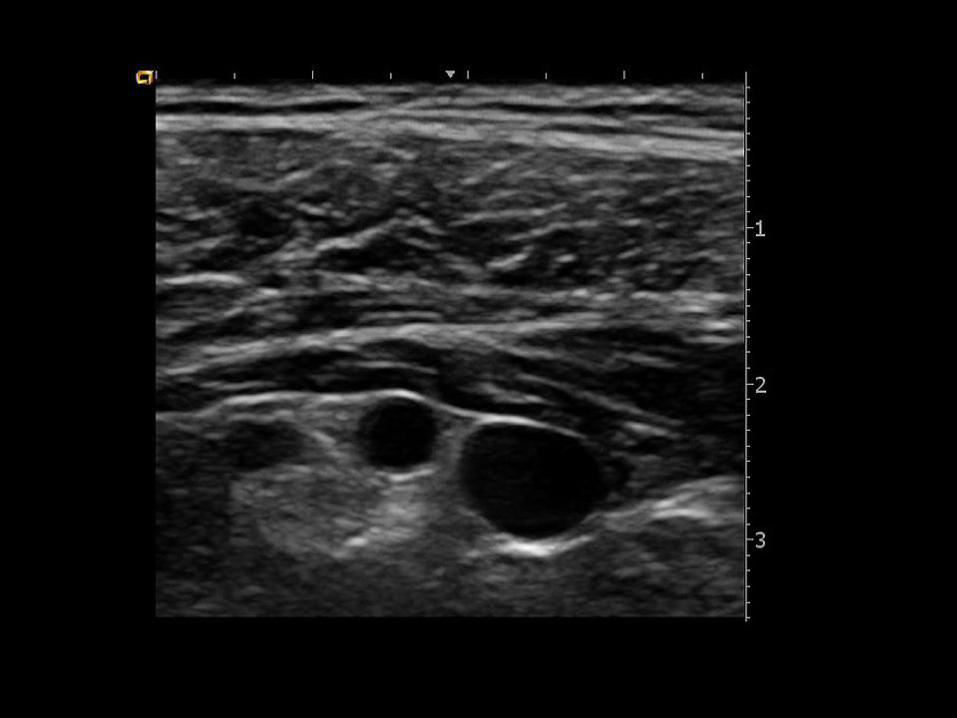
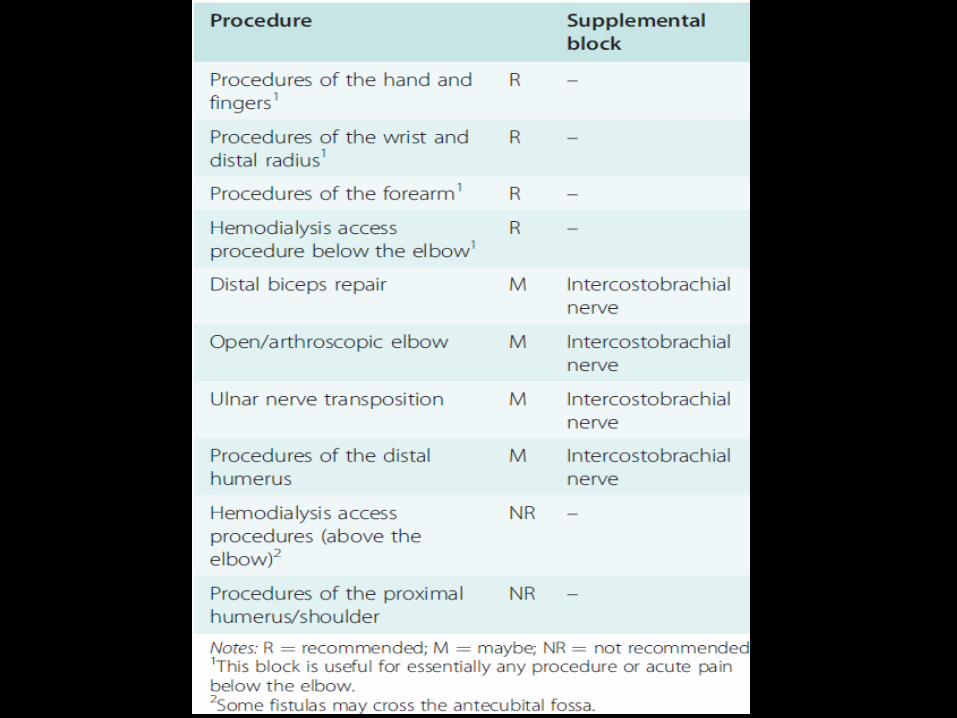
Axillary
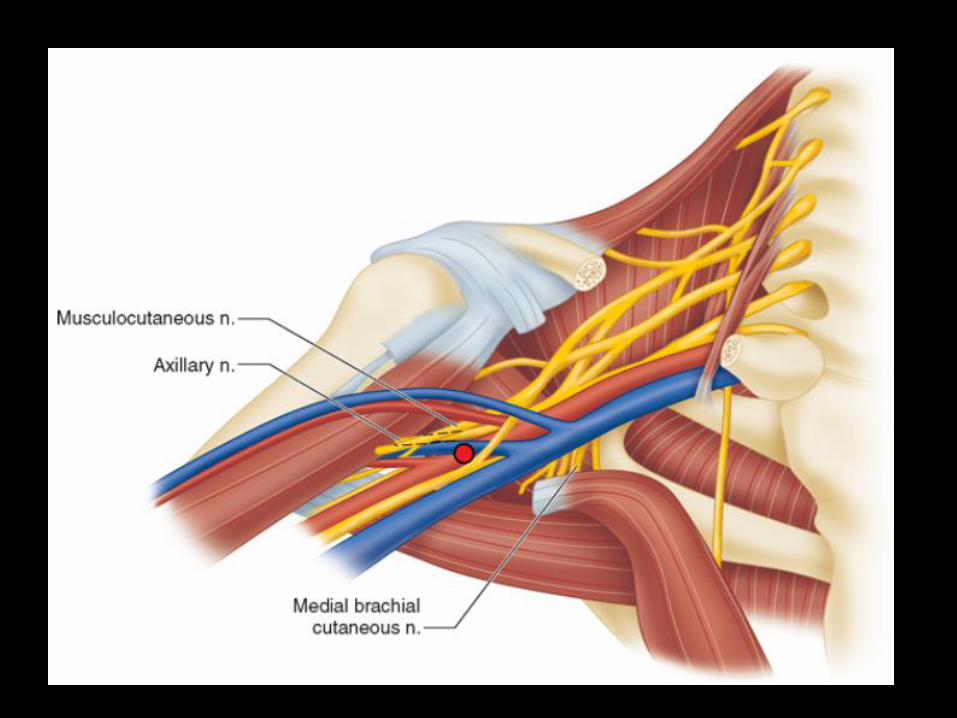


Surgical Coverage
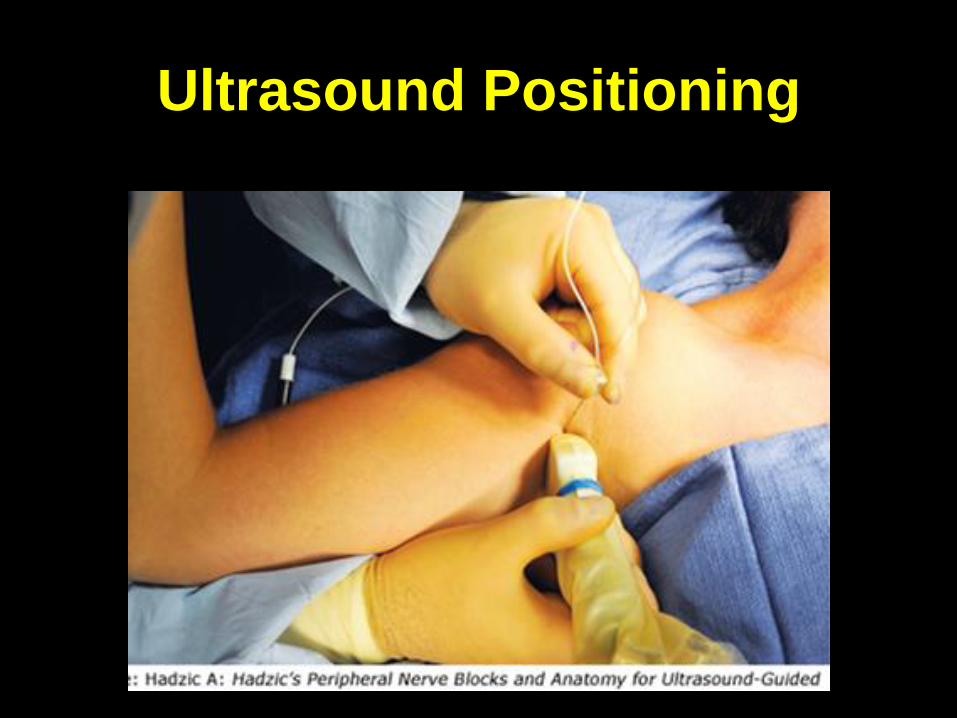
Ultrasound Positioning


Midhumeral/Rescue
Blocks

Midhumeral (Upper 3rd) View
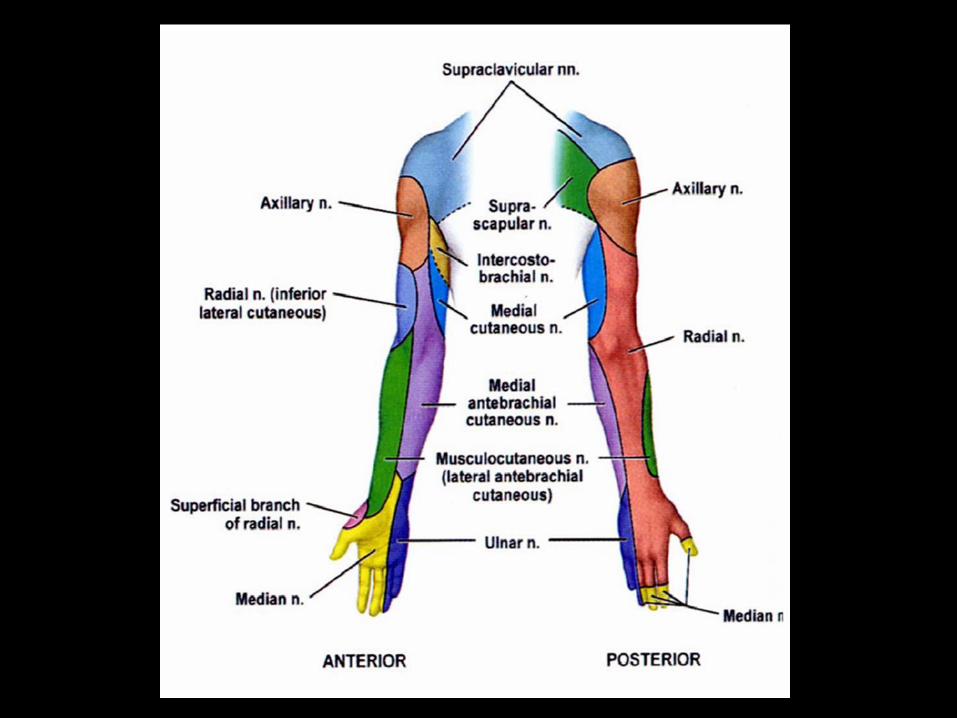

3 Often Needed Supplementals
All blocked at axilla with single generous SC injection.
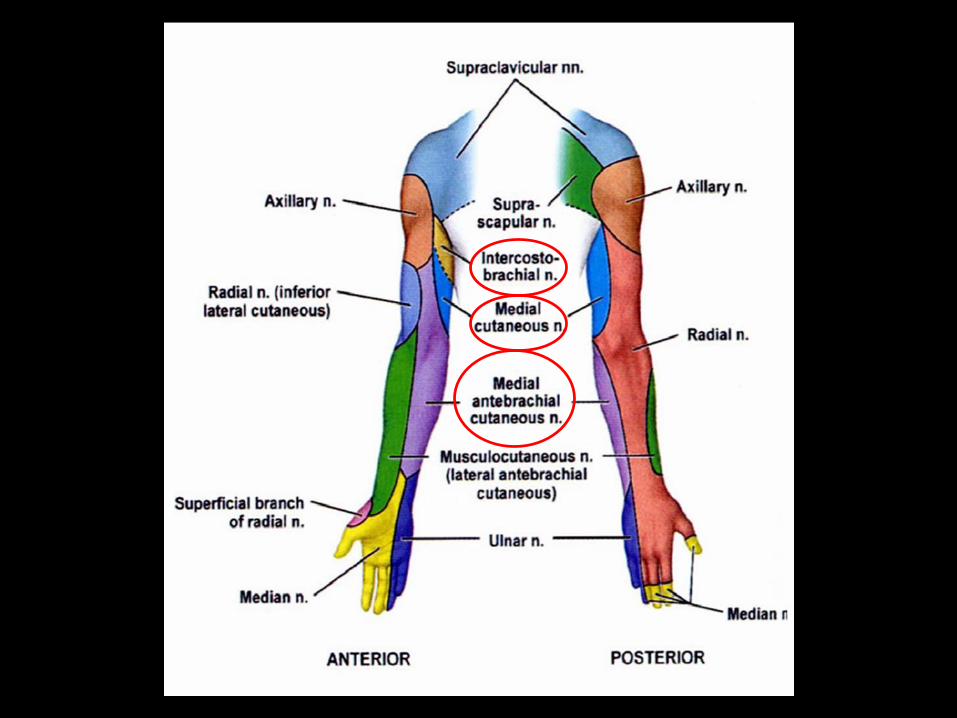

Intercostobrachial Nerve Block
Lower Extremity Blocks
• Lumbar Plexus Block
• Femoral/3 in 1 Block
• Adductor Canal Block
• Saphenous Nerve Block
• Sciatic Nerve Block
• Popliteal Block
• Ankle Block
• Mayo Block


Femoral Nerve Block
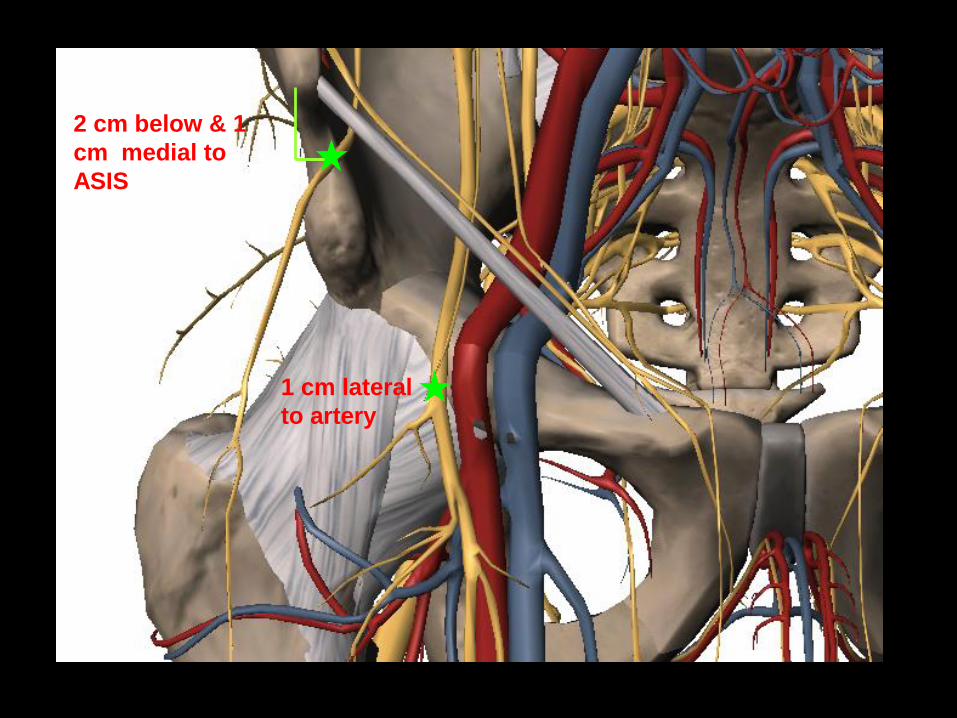
1 cm lateral
to artery
2 cm below & 1
cm medial to
ASIS
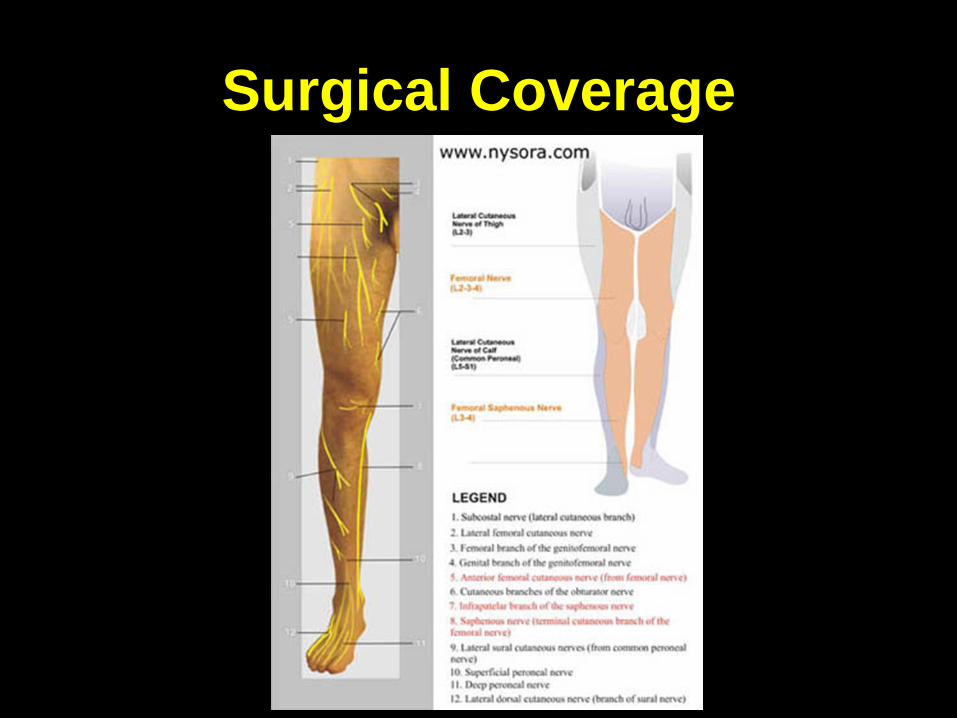
Surgical Coverage

Patella elevates with Stimulation

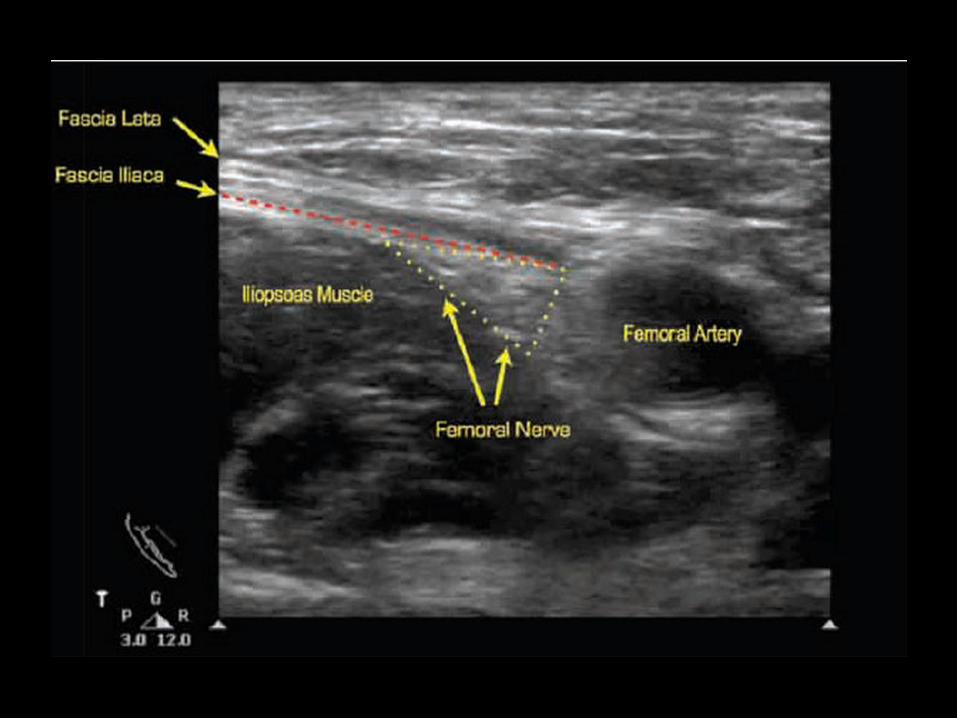
Ultrasound Positioning

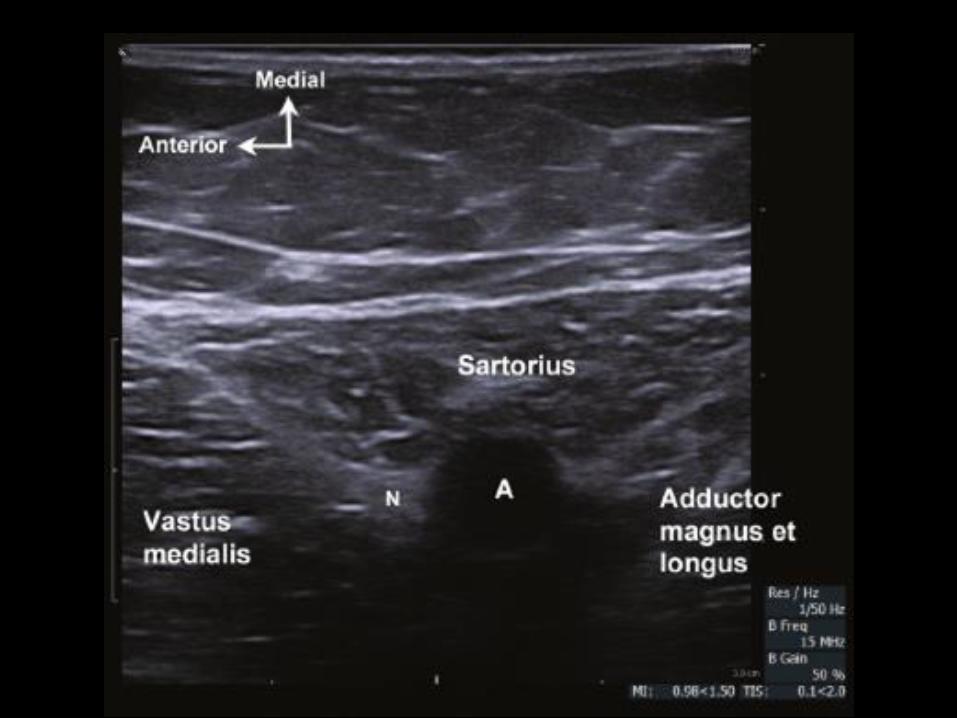
Adductor Canal Block



Ultrasound Positioning

Sciatic Nerve Block





Classic Position and
Landmarks

3cm
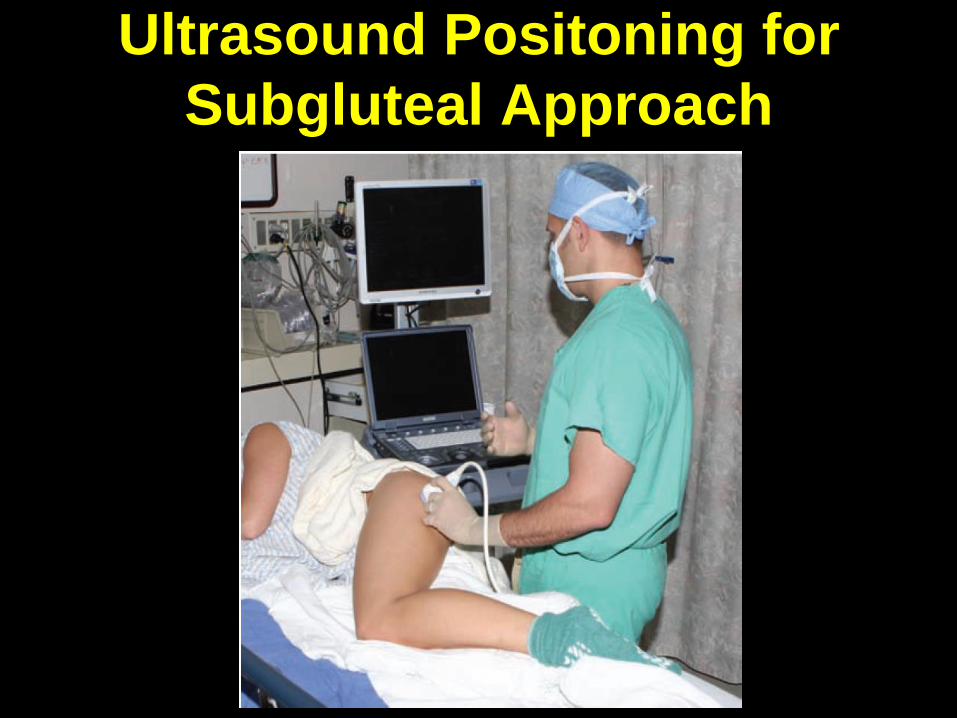
Ultrasound Positoning for
Subgluteal Approach
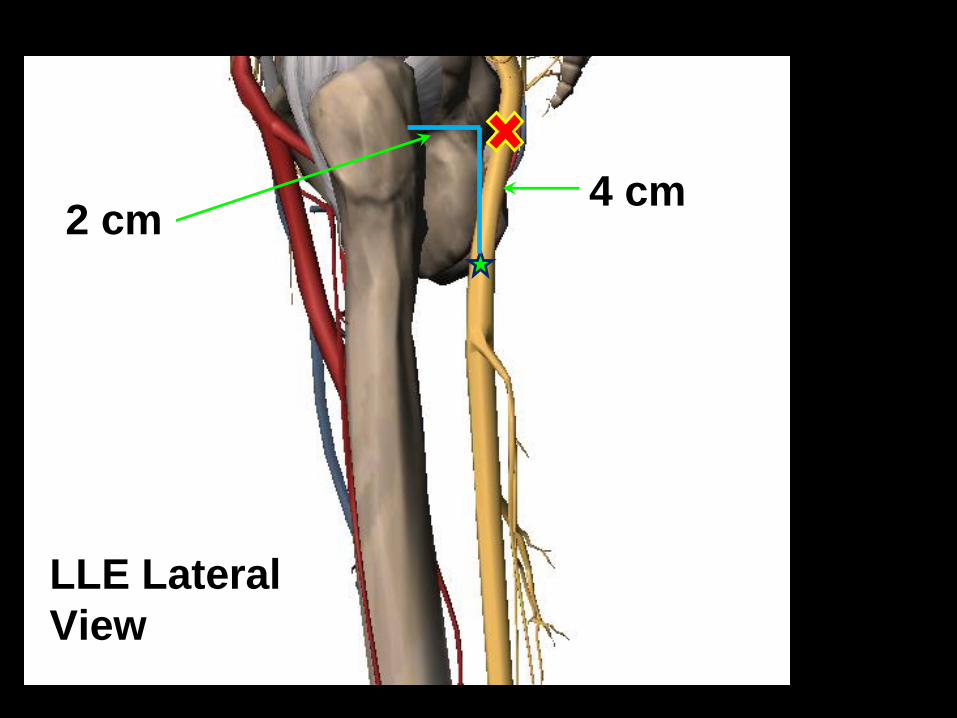
LLE Lateral
View
4 cm2 cm


Popliteal Nerve Block


Landmarks

Ultrasound Positioning


Alternate Positioning

So…what’s the take away?

OUR PRACTICE WORLD IS
CHANGING!
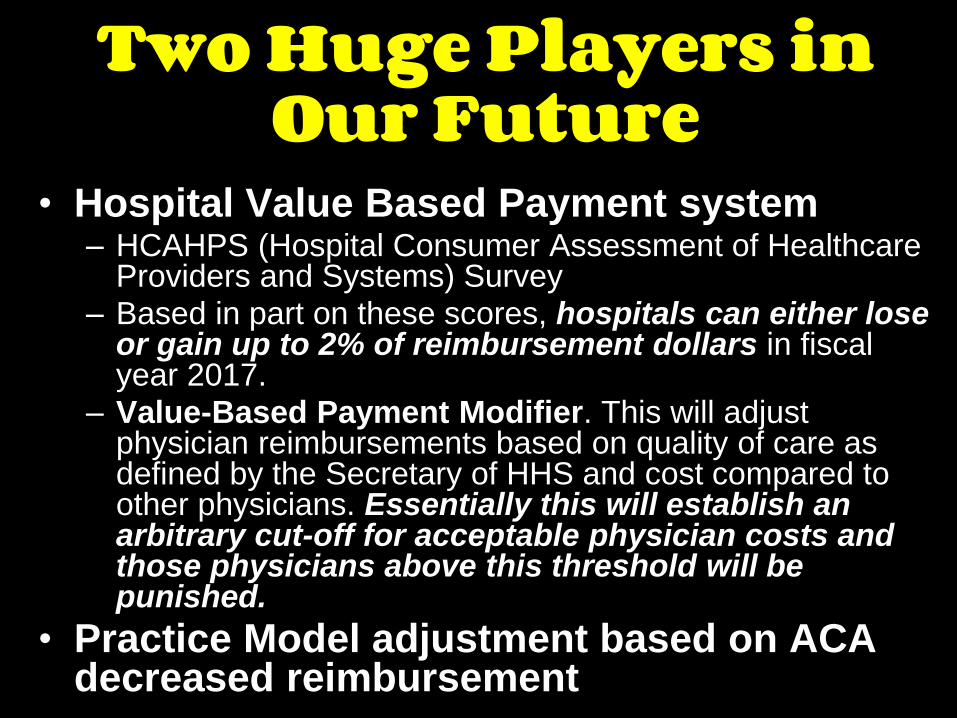
Two Huge Players in Our Future
• Hospital Value Based Payment system– HCAHPS (Hospital Consumer Assessment of Healthcare
Providers and Systems) Survey – Based in part on these scores, hospitals can either lose
or gain up to 2% of reimbursement dollars in fiscal year 2017.
– Value-Based Payment Modifier. This will adjust physician reimbursements based on quality of care as defined by the Secretary of HHS and cost compared to other physicians. Essentially this will establish an arbitrary cut-off for acceptable physician costs and those physicians above this threshold will be punished.
• Practice Model adjustment based on ACA decreased reimbursement
What does that mean for us?
• All anesthesia providers need to be efficient as well
as proficient
– Potentially less physicians and MDAs as regulatory
burden increases and salaries and job satisfaction
decrease
• CRNAs will need to step up and provide care to
their full scope of practice even in non-rural,
non-military environments
– This will mean gaining or re-acquiring skills for many
practicing CRNAs
– Schools will need to be more aggressive in training
SRNA for the future job market.
So how does that translate for me as a provider right now?
New Skill Sets….• Ultrasound proficiency is now a
must.
• Basic peripheral regional block skills are a must.
• Greater use of peripheral regional blocks for improved patient satisfaction.
• Non-traditional roles for value added services to hospitals/patients
Things we’ve kind of always done…
• Interscalene block• Femoral nerve block• Lumbar plexus block• Sciatic nerve block—Labat• Ankle block• Wrist block• Spinals• Epidurals

Things we’re going to need to master…
• All of the previous blocks using US
• Supraclavicular and Infraclavicular blocks under
US guidance
• Multiple variations of sciatic blocks—lateral,
anterior, popliteal—under US guidance
• Adductor canal block under US guidance
• Suprascapular nerve blocks under US guidance
• Better isolation of particular nerves for blockade
so as to preserve as much function as possible
for earlier/faster discharge and greater pain
control
New Trends…and yes, they alluse ultrasound
• Transversus abdominus plane (TAP) block
– Mid axillary and subcostal
• Rectus sheath block
• Paravertebral block
• Pectoral nerve (interfascial plane) block
(PECS I and II)
• Fascia iliaca block
• Ilioinguinal block
• Greater occipital nerve block
Down the road…..• Exparel to replace catheters???
• Better collaboration with surgeons on
exactly where they will be operating and
what postop expectations are
• Change the way we do blocks with an eye for
efficiency– Block room
– Block team
– Equipment/Drugs standardization
– Simple pain service interventions even at small places
• Stop the madness of ‘room air general’ on
top of blocks unless absolutely necessary.
Peripheral regional blocks
ARE our job, but to do them
you have to properly trained,
properly equipped and have
the cooperation of both the
patients and the surgeons.
QUESTIONS?