Perinatal Opioid Use: Understanding and Aligning Response ......Dorothy J. Mandell, PhD Population...
21
Perinatal Opioid Use: Understanding and Aligning Response between Systems Dorothy J. Mandell, PhD Population Health University of Texas System & University of Texas Health Science Center, Tyler
Transcript of Perinatal Opioid Use: Understanding and Aligning Response ......Dorothy J. Mandell, PhD Population...

Perinatal Opioid Use: Understanding and Aligning Response between SystemsDorothy J. Mandell, PhDPopulation Health University of Texas System & University of Texas Health Science Center, Tyler

Population Health, UT System Administration
• Dorothy Mandell, PhD• Matthew Myers, MPH
• Christopher Greeley, MD• Beth van Horne, DrPH• Nancy Correa, MPH• Rachael Keefe, MD• Yen Hoang Nong, MPH• Meredith Vinez, MPP• Suratha Elango, MD
The Team
Baylor College of Medicine, Public Health Pediatrics

Background – NAS & Infant Drug Exposure
• Neonatal Abstinence Syndrome (NAS):• A clinical diagnosis stemming from a collection of withdrawal
symptoms expressed by a newborn• Seizures, cardiac issues, gastric issues, temperature instability, hyper-
irritability, high-pitch uncontrollable cry• Primarily associated with prenatal opioid exposure • Not all infants exposed to drugs are diagnosed with NAS
• Drug Exposed: • Texas most prevalent drug of threat: Methamphetamines• Poly-drug exposures

The rising tide
• The rate of infants affected by drugs in utero has doubled since the mid 2000’s
• About 35% of prenatal drug exposure cases have a NAS diagnosis
5.86
6.927.54
7.878.33
8.70 8.939.41
0.00
2.00
4.00
6.00
8.00
10.00
2009 2010 2011 2012 2013 2014 2015 2016
Rat
e p
er 1
,000
Liv
e B
irth
s
Prenatal Drug Exposure: Hospital Data Estimates
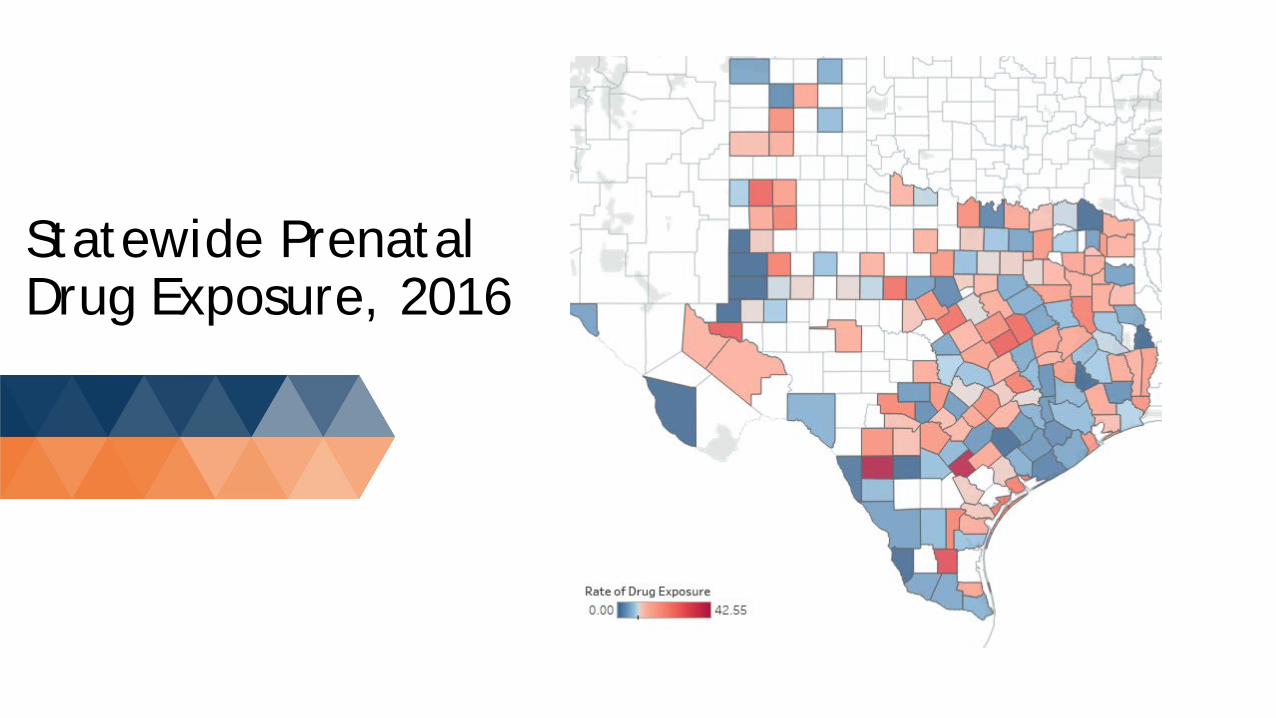
Statewide Prenatal Drug Exposure, 2016

Differences by County, 2016
• No county has more NAS cases and more prenatal drug exposure cases than Bexar County
• 26.8% of all NAS cases in Texas were in Bexar County
• 11% of prenatal drug exposure without withdraw cases in Texas were in Bexar County
• 8% of all births are in Bexar County• 47% of prenatal drug exposures
have a diagnosis of NAS in Bexar county
County Prenataldrug exposure rate
NAS All prenatal drug exposure
Bexar 18.75 235 491Dallas 10.50 114 424Tarrant 9.58 73 256Harris 6.53 75 475Travis 9.64 33 149Nueces 14.92 28 71

Toll of Prenatal Drug Exposure (2015)
Non Drug Exposed
Drug Exposed w/o Withdraw
NAS
Low birth weight 6.1% 28.8% 19.1%Length of Stay 3.3 days 9.6 days 21.9 daysMedicaid 48.3% 69.8% 70.5%Average cost $3,680 $15,890 $32,910
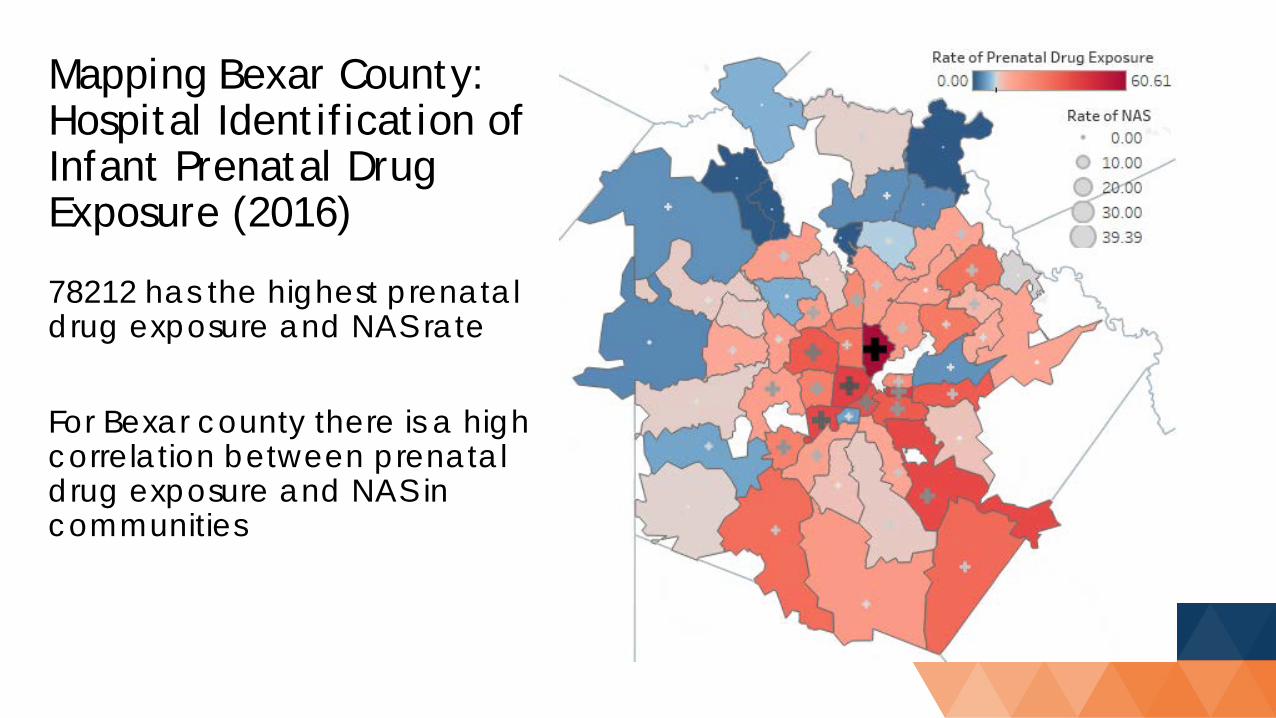
Mapping Bexar County: Hospital Identification of Infant Prenatal Drug Exposure (2016)
78212 has the highest prenatal drug exposure and NAS rate
For Bexar county there is a high correlation between prenatal drug exposure and NAS in communities

Infancy, CPS, and Substance Use
• ~2.5% of all infants in Texas become involved with CPS• Half of these become involved in first 2 weeks• Drug exposure likely cause of vast majority of these cases
• FY16, 38.5% of the ~167k completed investigations were drug related*
• FY17, 90 of the 172 (52%) child fatalities caused by abuse or neglect involved a parent or caregiver actively using a substance and/or under the influence.
• 11 of the 172 (6%) fatalities, the child had a documented history of prenatal drug or alcohol exposure

Goal: To build a cross-sector collaboratives in San Antonio and Houston, with partners from all impacted sectors, to reduce the conflict and confusion arising during the response to perinatal opioid use and improve outcomes for mothers and their children.Through collaboration, we will: • Identify and understand the roles and mission of each sector• Identify gaps and/or misalignment in response and services• Conduct readiness and implementation assessment with key
stakeholders• Generate pathways (e.g., policy recommendations) to fill the gaps
and create alignment• Create new connections and build trust and collaboration between
agencies
Aligning Response between Systems: Project goals and approach

Gaps in response and services: San Antonio Network
GAPS: Obstetrics & PediatricsEmergency Medicine

Generate recommendations to fill the gaps and create alignment
Houston San AntonioMeeting 1: Introduction 12 20
Law Enforcement/Justice 3 14Healthcare 2 1Treatment 6 1
CPS 0 2State 0 0
Community 1 0Research 0 2
Meeting 2: Journey Mapping 14 19Law Enforcement/Justice 4 5
Healthcare 4 3Treatment 4 1
CPS 1 2State 1 1
Community 0 3Research 0 4
Meeting 1Goal: introduce project, vet themes from interviews, share and discuss across sectors
Meeting 2 & 3Goal: go through journey mapping process using 2 true stories from women in recovery, share and discuss across sectors

Overall/General Schools and communities provide more
support for at-risk kids/families. Better identification and support services
Public campaign to decrease stigma and increase awareness of disease and services
Targeted outreach in places women go regularly (gas stations, grocery stores, corner stores…) to know services exist, where to go,
All sectors trained on addiction and services
Recovery coach/case manager to follow through ENTIRE process, engagement at all touchpoints, and beyond to sustain recovery
Early warning system to monitor spikes and identify locations for needed outreach
Justice System Addiction addressed throughout incarceration
using best practices (men, women, and pregnant women)
Linked into supportive community services upon release
Specialized courts and probation officers used to fullest extent
Sealing/expunging criminal records so that minor offenses are not impeding on employment
Pre & Post natal Comprehensive use of SBIRT in OB offices
(including screening for IPV, depression/anxiety, substance use).
OB office with integrated social work to address additional needs (food insecurity, trauma, etc)
Done with compassion and understanding. Education and referrals using warm hand-off
Birth control/family planning discussed during prenatal visits and given at delivery
Safety planning and CPS preparation prior to birth
Medical coverage (including treatment) continues for mom to address ALL of her mental and physical health needs (healthy mom=healthy baby)
Warm and supportive delivery/postpartum care experience
Hospitals able to care for women in active treatment (MAT)
Treatment/Recovery Treatment options are available to fit needs Treatment facilities support pregnant mom,
partners, and other children Pregnant women and partners are prioritized
for treatment Comprehensive, integrated care delivered
onsite to treat whole person Safety planning and CPS preparation prior to
transitioning Linked into supportive community services prior
to transitioning Safe and sober housing with support services
available to help sustain recovery
Child welfare and prevention Support services engaging with women early in
pregnancy Specialized CPS workers and CPS liaisons to
coordinate with other sectors Clear expectations and process outlined to
assist other sectors preparing mom/ensuring child safety
Ideas for the Ideal Future State by Touchpoint

Screening Issues•Substance use screening/testing protocols are not always written down. Much is left up to the discretion of the provider causing inconsistencies and screening/testing to appears to be “arbitrary”•Overall feeling is that medical providers are not always identifying women who need intervention•Strong opinions both for and against universal drug testing during pregnancy and at delivery•Medical staff have had limited training on opioid addiction and MAT
Source: Children and Family Futures

SBIRT: Screening, Brief Intervention, and Referral to Treatment
• SBIRT is an early intervention approach that targets those with nondependent substance use to provide effective strategies for intervention prior to the need for more extensive or specialized treatment
• Overview of SBIRT:• https://www.integration.samhsa.gov/clinical-practice/sbirt
• Example toolkit for implementing:• http://www.masbirt.org/sites/www.masbirt.org/files/documents/
toolkit.pdf

Clinical Guides
https://www.store.samhsa.gov/product/Clinical-Guidance-for-Treating-Pregnant-and-Parenting-Women-With-Opioid-Use-Disorder-and-Their-Infants/SMA18-5054
All Sectors Trained on Addiction and Services
• ... negative attitudes of health professionals towards patients with substance use disorders are common and contribute to suboptimal health care for these patients.

All Sectors Trained on Addiction and Services
• Every door is the right door to treatment• Everyone is a touchpoint for identification• Everyone should have knowledge for treatment referral

Data Sharing: Early warning system
• Rapid ascertainment of overdoses & reversals
• Where should community outreach be targeted
• Rapid shift in resources
Opioid Involved Deaths of Women of Childbearing Age
MAT Clinics

Texas Compared to the Nation
• As of 2015, Texas has the lowest rates of NAS and pre-natal drug exposure without withdraw
• The gift of time: Identify, Coordinate, & Prevent
• But not much time: Seizures of Fentanyl increasing
• https://www.dshs.texas.gov/mch/Obstetric-Care-for-Women-with-Opioid-Use-Disorder-Bundle.aspx17.0
8.4
9.1
5.1
9.4
20.1
3.7
2.5
6.9
4.5
8.1
10.9
7.2
12.9
11.0
10.8
16.0
8.8
6.7
13.2
10.4
10.8
0.0 5.0 10.0 15.0 20.0
New England
Middle Atlantic
East North Central
West North Central
South Atlantic
East South Central
West South Central
Texas
Mountian
Pacific
National Average
Drug Exposed NAS