
Percutaneous Transluminal Carotid Angioplasty and ... · 646 Percutaneous Transluminal Carotid...
3
646 Percutaneous Transluminal Carotid Angioplasty and Detachable Balloon Embolization in Fibromuscular Dysplasia Arthur B. Dublin,1 Harold A. Baltaxe,1 and Cully A. Cobb 1112 Fibromuscular dysplasia (FMD), a vascular disease of un- known etiology, most often affects the renal arteries (85% of cases) of young females [1]. However, this disease may also produce areas of stenosis at the C1-C2 vertebral level in the internal carotid artery (ICA) [1, 2]. Lesions producing symp- toms have been managed by bougie dilatation, surgical end- arterectomy, excision and artery reconstruction, patch angio- plasty, and endarterectomy with balloon dilatation [3-5]. Our case is the second reported by us, the seventh known pub- lished instance of FMD treated by percutaneous transluminal angioplasty (PTA), and the first patient with FMD treated by detachable balloon embolization. Case Report A 47-year-old woman developed left retroorbital headaches, which gradually increased in severity over a 3 month period. Physical examination revealed intermittent mild hypertension, a left Horner syndrome with intact sweating, possible hypalgesia in the distribution of the left cranial nerve VI , and bilateral carotid bruits. A computed tomographic (CT) scan of the brain was normal. Cerebral angiography demonstrated severe FMD of both ICAs and an aneurysm of the left ICA just caudal to the skull base (fig. 1). Because of the risk of hemorrhage or thrombus embolization from this aneurysm and the difficulty and danger of surgical treatment, an invasive neuroradiologic procedure was elected. A 5 French cerebral catheter (Cook, Bloomington, IN) was intro- duced into the proximal right ICA (caudal to the FMD) via a 6.5/8.5 French femoral arterial sheath (Cook). Blood pressure was 135/100 mm Hg . Using a 260 cm (0.035 inch) guide wire, the original catheter was removed, and a 5 French GrOntzig catheter (Cook) was intro- duced with a balloon 4 mm in inflated diameter and 2 cm in length. The tip of the GrOntzig catheter was placed cephalad to the region of FMD, and a blood pressure of 100/90 mm Hg was recorded (fig. 2) . Five thousand units of heparin was infused rapidly through the catheter. The balloon was then inflated three times (30 sec each instance) in the area of cephalad FMD. After this procedure, the pressure gradient was abolished (blood pressure, 145/105 mm Hg) (fig. 2) . The catheter was then withdrawn, and the remaining seg- ments of FMD were similarly dilated. However, few postdilatation angiographic changes were noted (figs. 1A and 1 B). A mild apraxia Received October 20, 1983; accepted after revision February 29, 1984. of the left hand was observed immediately after angioplasty, but this deficit began to resolve over the next hour. Next, the angioplasty catheter was removed, and a 5 French cerebral catheter (which was used as a marker device) was placed within the proximal left common carotid artery. Via a left femoral arterial puncture, a 4.8 French nondetachable balloon catheter (Cook) was introduced through a 9 French thin-wall catheter (Becton-Dick- inson, Rutherford, NJ). Continuous infusion of heparinized saline (10 U/ml solution) through the 9 French thin-wall catheter, and around the 4.8 French nondetachable balloon catheter, was maintained dur- ing the next occlusion procedure. The balloon was inflated in the left proximal ICA. and total occlusion of this vessel was confirmed by the 5 French marker catheter. The patient tolerated this procedure well for 10 min; therefore, nitroprusside was administered intravenously to lower the mean systolic blood pressure to 70 mm Hg to accentuate the neurologic effects of hypotension on the left carotid occlusion (6). Despite some expression of light-headedness by the patient, no objective neurologic deficits were observed over the next 5 min. Aspiration of blood from the 9 French thin-wall catheter was accom- plished during balloon deflation and removal. A 1.8 mm (non inflated diameter) detachable occluder balloon (Heyer-Shulte, Goleta CAl mounted on a 2/4 French coaxial catheter system was introduced through the 9 French catheter. The balloon was placed in the precavernous segment of the left ICA, inflated with 0.25 ml of 210 mg iodine/ml metrizamide, and then detached by traction (fig. 3). A second balloon could not be placed cephalad to the aneurysm due to the lack of blood flow and the numerous FMD webs. Two more detachable balloons were placed in the cervical carotid artery, thus effectively trapping the aneurysm (fig. 3). During the conclusion of the procedure, a digital arterial angiogram of the abdominal aorta revealed a 95% FMD stenosis of the right renal artery. This was not treated. The patient was free of headaches and well 3 months after the procedure, with no evidence of neurologic deficit, left carotid pulse, or bruit. Skull films showed no significant interval change in the position of the detachable balloons. Discussion FMD has five basic histologic patterns. Medial fibroplasia usually produces the aneurysmal leSions, while regions of stenosis are frequently associated with medial fibromuscular 1 Department of Diagnostic Radiology, University of California, Davis Medical Center, 4301 X St., Room 214, Sacramento, CA 95817. Address reprint requests to A. B. Dublin. 2 Department of Neurological Surgery, University of California, Davis Medical Center, Sacramento, CA 95817. AJNR 5:646-648, September/October 1984 0195-6108/84/0505- 0646 $00.00 (tJ American Roentgen Ray Society
Transcript of Percutaneous Transluminal Carotid Angioplasty and ... · 646 Percutaneous Transluminal Carotid...
646
Percutaneous Transluminal Carotid Angioplasty and Detachable Balloon Embolization in Fibromuscular Dysplasia Arthur B. Dublin ,1 Harold A. Baltaxe,1 and Cully A. Cobb 1112
Fibromuscular dysplasia (FMD), a vascular disease of unknown etiology, most often affects the renal arteries (85% of cases) of young females [1] . However, this disease may also produce areas of stenosis at the C1-C2 vertebral level in the internal carotid artery (ICA) [1, 2]. Lesions producing symptoms have been managed by bougie dilatation, surgical endarterectomy, excision and artery reconstruction, patch angioplasty, and endarterectomy with balloon dilatation [3-5]. Our case is the second reported by us, the seventh known published instance of FMD treated by percutaneous transluminal angioplasty (PTA), and the first patient with FMD treated by detachable balloon embolization.
Case Report
A 47-year-old woman developed left retroorbital headaches, which gradually increased in severity over a 3 month period. Physical examination revealed intermittent mild hypertension, a left Horner syndrome with intact sweating , possible hypalgesia in the distribution of the left cranial nerve VI , and bilateral carotid bruits. A computed tomographic (CT) scan of the brain was normal. Cerebral angiography demonstrated severe FMD of both ICAs and an aneurysm of the left ICA just caudal to the skull base (fig . 1). Because of the risk of hemorrhage or thrombus embolization from this aneurysm and the difficulty and danger of surgical treatment, an invasive neuroradiologic procedure was elected.
A 5 French cerebral catheter (Cook, Bloomington, IN) was introduced into the proximal right ICA (caudal to the FMD) via a 6.5/8.5 French femoral arterial sheath (Cook). Blood pressure was 135/100 mm Hg. Using a 260 cm (0.035 inch) guide wire, the original catheter was removed, and a 5 French GrOntzig catheter (Cook) was introduced with a balloon 4 mm in inflated diameter and 2 cm in length. The tip of the GrOntzig catheter was placed cephalad to the region of FMD, and a blood pressure of 100/90 mm Hg was recorded (fig . 2). Five thousand units of heparin was infused rapidly through the catheter. The balloon was then inflated three times (30 sec each instance) in the area of cephalad FMD. After this procedure, the pressure gradient was abolished (blood pressure, 145/105 mm Hg) (fig. 2). The catheter was then withdrawn, and the remaining segments of FMD were similarly dilated. However, few postdilatation angiographic changes were noted (figs. 1 A and 1 B). A mild apraxia
Received October 20, 1983; accepted after revision February 29, 1984.
of the left hand was observed immediately after angioplasty, but this deficit began to resolve over the next hour.
Next, the angioplasty catheter was removed, and a 5 French cerebral catheter (which was used as a marker device) was placed within the proximal left common carotid artery. Via a left femoral arterial puncture, a 4.8 French nondetachable balloon catheter (Cook) was introduced through a 9 French thin-wall catheter (Becton-Dickinson, Rutherford, NJ). Continuous infusion of heparinized saline (10 U/ml solution) through the 9 French thin-wall catheter, and around the 4.8 French nondetachable balloon catheter, was maintained during the next occlusion procedure. The balloon was inflated in the left proximal ICA. and total occlusion of this vessel was confirmed by the 5 French marker catheter. The patient tolerated this procedure well for 10 min; therefore, nitroprusside was administered intravenously to lower the mean systolic blood pressure to 70 mm Hg to accentuate the neurologic effects of hypotension on the left carotid occlusion (6). Despite some expression of light-headedness by the patient, no objective neurologic deficits were observed over the next 5 min. Aspiration of blood from the 9 French thin-wall catheter was accomplished during balloon deflation and removal.
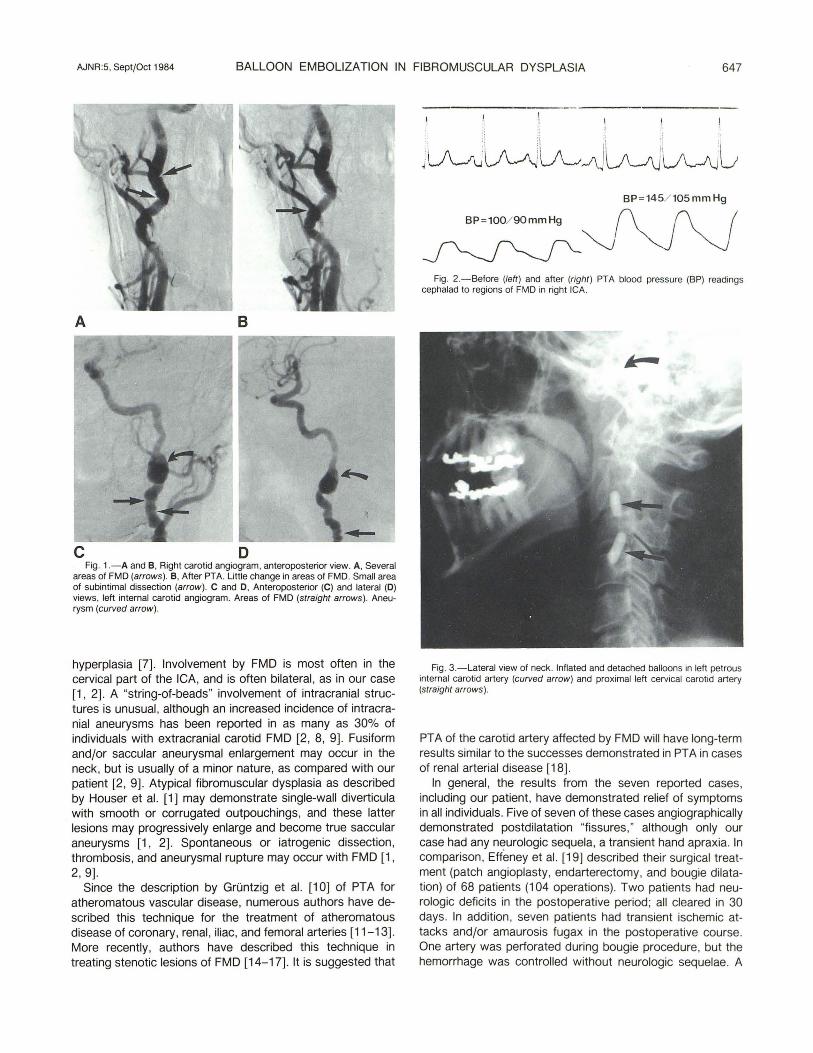
A 1.8 mm (non inflated diameter) detachable occluder balloon (Heyer-Shulte, Goleta CAl mounted on a 2/4 French coaxial catheter system was introduced through the 9 French catheter. The balloon was placed in the precavernous segment of the left ICA, inflated with 0.25 ml of 210 mg iodine/ml metrizamide, and then detached by traction (fig. 3). A second balloon could not be placed cephalad to the aneurysm due to the lack of blood flow and the numerous FMD webs. Two more detachable balloons were placed in the cervical carotid artery, thus effectively trapping the aneurysm (fig . 3). During the conclusion of the procedure, a digital arterial angiogram of the abdominal aorta revealed a 95% FMD stenosis of the right renal artery. This was not treated .
The patient was free of headaches and well 3 months after the procedure, with no evidence of neurologic deficit, left carotid pulse, or bruit. Skull films showed no significant interval change in the position of the detachable balloons.
Discussion
FMD has five basic histologic patterns. Medial fibroplasia usually produces the aneurysmal leSions, while regions of stenosis are frequently associated with medial fibromuscular
1 Department of Diagnostic Radiology, University of California, Davis Medical Center, 4301 X St. , Room 214, Sacramento, CA 95817. Address reprint requests to A. B. Dublin.
2 Department of Neurological Surgery, University of California, Davis Medical Center, Sacramento, CA 95817.
AJNR 5:646-648, September/October 1984 0195-6108/84/0505- 0646 $00.00 (tJ American Roentgen Ray Society
AJNR:5, Sept/Oct 1984 BALLOON EMBOLIZATION IN FIBROMUSCULAR DYSPLASIA 647
A B
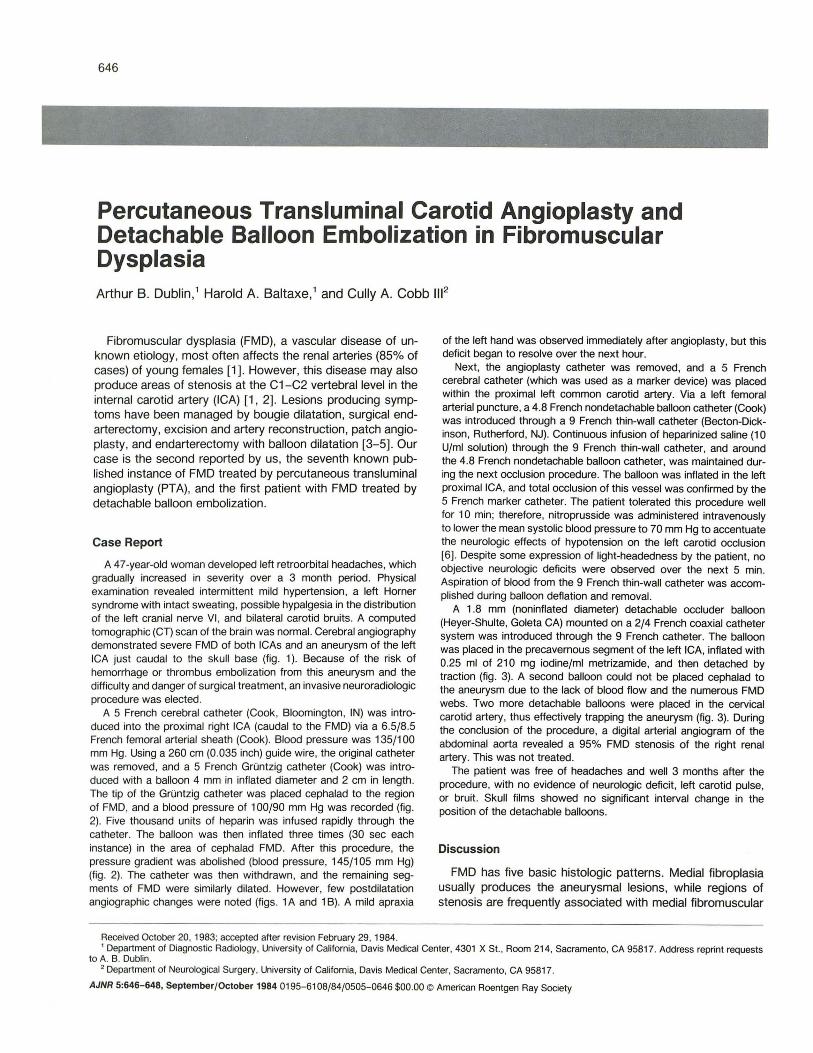
c D Fig. 1.-A and B, Right carotid angiogram, anteroposterior view. A, Several
areas of FMD (arrows) . B, After PTA. Little change in areas of FMD. Small area of subintimal dissection (arrow). C and 0 , Anteroposterior (C) and lateral (0) views, left internal carotid angiogram. Areas of FMD (straight arrows). Aneurysm (curved arrow) .
hyperplasia [7] . Involvement by FMD is most often in the cervical part of the ICA, and is often bilateral , as in our case [1, 2]. A "string-of-beads" involvement of intracranial structures is unusual, although an increased incidence of intracranial aneurysms has been reported in as many as 30% of individuals with extracranial carotid FMD [2, 8, 9] . Fusiform and/or saccular aneurysmal enlargement may occur in the neck, but is usually of a minor nature, as compared with our patient [2, 9]. Atypical fibromuscular dysplasia as described by Houser et al. [1] may demonstrate single-wall diverticula with smooth or corrugated outpouchings, and these latter lesions may progressively enlarge and become true saccular aneurysms [1, 2]. Spontaneous or iatrogenic dissection, thrombosis, and aneurysmal rupture may occur with FMD [1, 2, 9] .
Since the description by Gruntzig et al. [10] of PTA for atheromatous vascular disease, numerous authors have described this technique for the treatment of atheromatous disease of coronary, renal, iliac, and femoral arteries [11-13]. More recently, authors have described this technique in treating stenotic lesions of FMD [14-17]. It is suggested that
BP =145/ 105mmHg
~~~ Fig. 2.- Before (left) and after (right) PTA blood pressure (BP) readings
cephalad to regions of FMD in right ICA.
Fig. 3.- Lateral view of neck. Inflated and detached balloons in left petrous internal carotid artery (curved arrow) and proximal left cervical carotid artery (straight arrows) .
PTA of the carotid artery affected by FMD will have long-term results similar to the successes demonstrated in PTA in cases of renal arterial disease [18].
In general, the results from the seven reported cases , including our patient, have demonstrated relief of symptoms in all individuals. Five of seven of these cases angiographically demonstrated postdilatation "fissures, " although only our case had any neurologic sequela, a transient hand apraxia. In comparison, Effemey et al. [19] described their surgical treatment (patch angioplasty, endarterectomy, and bougie dilatation) of 68 patients (104 operations). Two patients had neurologic deficits in the postoperative period; all cleared in 30 days. In addition, seven patients had transient ischemic attacks and/or amaurosis fugax in the postoperative course. One artery was perforated during bougie procedure, but the hemorrhage was controlled without neurologic sequelae. A

648 DUBLIN ET AL. AJNR:5, Sept/Oct 1984
comparison randomized study of open surgical techniques and PTA of FMD is suggested.
The use of detachable balloon techniques has been described in a variety of pathologic entities, including carotidcavernous sinus fistulas , intracranial aneurysms, and arterial laceration [20-22]. Carotid sacrifice by detachable balloon embolization is an alternative to surgical exploration, particularly in those cases in which the aneurysm is surgically inaccessible [20] .
In conclusion, PTA offers several advantages to surgical procedures for FMD. These advantages include the ability to treat multiple areas of FMD from a single transfemoral puncture site, continuous fluoroscopic control of the procedure, the lack of a large incision site, an awake patient with local anesthetic control , and no suture material in the artery that might conceivably produce turbulent flow and possible subsequent thrombus formation . Balloon sacrifice of the carotid artery offers an alternative to the surgical treatment of aneurysmal dilatation of the carotid artery, which may be associated with this disease.
REFERENCES
1. Houser OW, Baker HL Jr, Sandok BA, Holley KE. Cephalic arterial fibromuscular dysplasia . Radiology 1971 ;101 : 605- 611
2. Osborn AG, Anderson RE. Angiographic spectrum of cervical and intracranial fibromuscular dysplasia. Stroke 1977; 8 : 617 - 626
3. Balaji MR , De Weese JA. Fibromuscular dysplasia of the internal carotid artery. Its occurrence with acute stroke and its surgical reversal. Arch Surg 1980;115 :984- 986
4. Morris GC Jr, Lechter A, De Bakey ME. Surgical treatment of fibromuscular disease of the carotid arteries. Arch Surg 1968;96 : 636-643
5. Perry MO. Fibromuscular disease of the carotid artery. Surg GynecolObstet 1972;134 :57- 60
6. Youmans JR . Cerebral blood flow in clinical problems. In: Youmans JR. Neurological surgery. Philadelphia: Saunders, 1982 : 786- 845
7. McCormack LJ , Poutasse EF, Meaney TF, Noto TJ, Dustan HP. A pathologic-arteriographic correlation of renal arterial disease.
Am Heart J 1966;72: 188-198 8. Sandok BA, Houser OW, Baker HL, Holley KE. Fibromuscular
dysplasia. Arch Neuro/1971;24 :462- 466 9. Taveras JM, Wood EH. Diagnostic neuroradiology. Baltimore:
Williams & Wilkins, 1976 :850-857 10. Gruntzig A, Myler R, Stertzer S, Kaltenbach M, Turino M. Coro
nary percutaneous transluminal angioplasty: preliminary results. Circulation 1978;58[SuppI2} :11-56
11 . Gruntzig A, Vetter W, Meier B, Kuhlmann , U, Lutolf U, Siegenthaler W. Treatment of renovascular hypertension with percutaneous transluminal dilatation of a renal artery stenosis. Lancet 1978;1 :801-802
12. Motarjeme A, Keifer JW, Zuska AJ . Percutaneous transluminal angioplasty of brachiocephalic arteries . AJNR 1982;3 : 169-174, AJR 1982;138: 457 -462
13. Motarjeme A, Keifer JW, Zuska AJ . Percutaneous transluminal angioplasty of the deep femoral artery. Radiology 1980; 135 :613-617
14. Mullan S, Duda EE, Patronas NJ. Some examples of balloon technology in neurosurgery. J Neurosurg 1980;52 :321-329
15. Hasso AN, Bird CR, Zinke DE, Thompson JR. Fibromuscular dysplasia of the internal carotid artery: percutaneous transluminal angioplasty. AJNR 1981;2 :175- 180, AJR 1981 ;136 :955-960
16. Belim A, Veselci M, Vanek I, Weiss K, Peregrin J. Percutaneous transluminal angioplasty. Cardiovasc Intervent Radial 1982 ; 5:79-81
17. Dublin AB, Baltaze HA, Cobb CA III. Percutaneous transluminal carotid angioplasty in fibromuscular dysplasia. Case report. J Neurosurg 1983;59 : 162- 165
18. Saddekin S, Sniderman KW, Hilton S, Sos TA. Percutaneous transluminal angioplasty of non atherosclerotic lesions. AJR 1980;135:975-982
19. Effeney OJ, Ehrenfield WK, Stoney RJ , Wylie E. Fibromuscular dysplasia of the internal carotid artery. World J Surg 1979;3 : 179-185
20. Berenstein A, Kricheff II , Ransohoff J. Carotid-cavernous fistulas: intraarterial treatment. AJNR 1980;1 :449-457
21 . Debrun G, Lacour P, Vinuela F, Fox A, Drake CG, Caron JP. Treatment of 54 traumatic carotid-cavernous fistulas. J Neurosurg 1981;55 :678-692
22. Mehringer CM , Hieshima GB, Grinnell VS, et al. Therapeutic embolization for vascular trauma of the head and neck. AJNR 1983;4 :137-142


















