
PERCUTANEOUS TRANSHEPATIC BILIARY DRAINAGE IN A...
5
Archives of the Balkan Medical Union Copyright © 2017 Balkan Medical Union vol. 52, no. 2, pp. 225-229 June 2017 RÉSUMÉ Drainage biliaire transhépatique chez un patient avec sténose maligne et anatomie altérée- rapport de cas Introduction. Nous présentons le cas d’un patient de 72 ans admis à notre hôpital avec une jaunisse intense. Présentation du cas. Cinq mois auparavant, il avait subi une intervention chirurgicale digestive palliative pour un carcinome massif du processus unciné du pan- créas, qui obstruait la lumière duodénale, mais sans obstruction biliaire, donc une dérivation digestive avait été effectuée. La CPRE n’était pas une option due à l’obstruction maligne duodénale. Par conséquent, nous avons décidé d’insérer un tube de drainage bili- aire par voie transhépatique percutanée en utilisant l’échographie et le guidage radiologique. Initialement, l’évolution était favorable avec une baisse de la bili- rubine de moitié. Deux semaines plus tard, le patient revient à notre hôpital avec le tube biliaire partielle- ment migré à l’extérieur et avec fuite du péricathéter . Avant de récupérer le drainage biliaire percutané, nous ABSTRACT Introduction. We present the case of a 72-year-old pa- tient admitted to our hospital with intense jaundice. Case presentation. Five months previously, he had undergone palliative digestive surgical intervention for massive carcinoma of the uncinate process of the pancreas, which obstructed the duodenal lumen but without biliary obstruction, so a digestive derivation had been performed. The endoscopic retrograde chol- angiopancreatography (ERCP) was not an option due to the duodenal malignant obstruction. Therefore, we decided to insert a biliary drainage tube via percutane- ous transhepatic route using ultrasound and radiologi- cal guidance. Initially, the evolution was favorable with a bilirubin drop by half. Two weeks later, the patient returns to our hospital with the biliary tube partially migrated outside and with pericatheter leakage. Before retrieving the percutaneous biliary drainage we insert- ed under X-rays a guidewire which was well placed in the distal duodenum. Afterwards, we extracted the biliary drainage over the guidewire, advanced over CASE REPORT PERCUTANEOUS TRANSHEPATIC BILIARY DRAINAGE IN A PATIENT WITH MALIGNANT STENOSIS AND ALTERED ANATOMY Gabriel Constantinescu 1,2 , Oana Plotogea 2 , Vasile Șandru 2 , Radu Țincu 1,3 , Alexandru Chiotoroiu 4 , Dragoș Ene 1,4 , Bogdan Popa 1,5 , Mădălina Ilie 1,2 1 University of Medicine and Pharmacy “Carol Davila“, Bucharest, Romania 2 Gastroenterology Department, Clinical Emergency Hospital of Bucharest, Romania 3 Intensive Care and Toxicology Department, Clinical Emergency Hospital of Bucharest, Romania 4 General Surgery Department, Clinical Emergency Hospital of Bucharest, Romania 5 Radiology Department, Clinical Emergency Hospital of Bucharest, Romania Corresponding author: Dr. Mădălina Ilie Clinical Emergency Hospital of Bucharest, 8 Calea Floreasca, Bucharest, Romania e-mail: [email protected] Conflicts of interests: none
Transcript of PERCUTANEOUS TRANSHEPATIC BILIARY DRAINAGE IN A...

Archives of the Balkan Medical UnionCopyright © 2017 Balkan Medical Union
vol. 52, no. 2, pp. 225-229June 2017
RÉSUMÉ
Drainage biliaire transhépatique chez un patient avec sténose maligne et anatomie altérée- rapport de cas
Introduction. Nous présentons le cas d’un patient de 72 ans admis à notre hôpital avec une jaunisse intense. Présentation du cas. Cinq mois auparavant, il avait subi une intervention chirurgicale digestive palliative pour un carcinome massif du processus unciné du pan-créas, qui obstruait la lumière duodénale, mais sans obstruction biliaire, donc une dérivation digestive avait été effectuée. La CPRE n’était pas une option due à l’obstruction maligne duodénale. Par conséquent, nous avons décidé d’insérer un tube de drainage bili-aire par voie transhépatique percutanée en utilisant l’échographie et le guidage radiologique. Initialement, l’évolution était favorable avec une baisse de la bili-rubine de moitié. Deux semaines plus tard, le patient revient à notre hôpital avec le tube biliaire partielle-ment migré à l’extérieur et avec fuite du péricathéter . Avant de récupérer le drainage biliaire percutané, nous
ABSTRACT
Introduction. We present the case of a 72-year-old pa-tient admitted to our hospital with intense jaundice.Case presentation. Five months previously, he had undergone palliative digestive surgical intervention for massive carcinoma of the uncinate process of the pancreas, which obstructed the duodenal lumen but without biliary obstruction, so a digestive derivation had been performed. The endoscopic retrograde chol-angiopancreatography (ERCP) was not an option due to the duodenal malignant obstruction. Therefore, we decided to insert a biliary drainage tube via percutane-ous transhepatic route using ultrasound and radiologi-cal guidance. Initially, the evolution was favorable with a bilirubin drop by half. Two weeks later, the patient returns to our hospital with the biliary tube partially migrated outside and with pericatheter leakage. Before retrieving the percutaneous biliary drainage we insert-ed under X-rays a guidewire which was well placed in the distal duodenum. Afterwards, we extracted the biliary drainage over the guidewire, advanced over
CASE REPORT
PERCUTANEOUS TRANSHEPATIC BILIARY DRAINAGE IN A PATIENT WITH MALIGNANT STENOSIS AND ALTERED ANATOMY
Gabriel Constantinescu1,2, Oana Plotogea2, Vasile Șandru2, Radu Țincu1,3, Alexandru Chiotoroiu4, Dragoș Ene1,4, Bogdan Popa1,5, Mădălina Ilie1,2
1 University of Medicine and Pharmacy “Carol Davila“, Bucharest, Romania2 Gastroenterology Department, Clinical Emergency Hospital of Bucharest, Romania3 Intensive Care and Toxicology Department, Clinical Emergency Hospital of Bucharest, Romania4 General Surgery Department, Clinical Emergency Hospital of Bucharest, Romania5 Radiology Department, Clinical Emergency Hospital of Bucharest, Romania
Corresponding author: Dr. Mădălina Ilie
Clinical Emergency Hospital of Bucharest, 8 Calea Floreasca, Bucharest, Romania
e-mail: [email protected]
Conflicts of interests: none

Percutaneous transhepatic biliary drainage in a patient with malignant stenosis… – CONSTANTINESCU et al
226 / vol. 52, no. 2
INTRODUCTION
Over the past decades, biliary interventions have evolved and increased in prevalence and utility. Current percutaneous biliary interventions include percutaneous transhepatic cholangiography (PTC), biliary drainage and percutaneous cholecystostomy.
Percutaneous Transhepatic Biliary Drainage (PTBD) is indicated in patients with non-operative lesions, when endoscopic stenting using endoscopic retrograde cholangio-pancreatography (ERCP) is im-possible due to malignant duodenal infiltration, or because of modified postoperative anatomy of the digestive tract, complications or severe general state of the patient. In these patients, PTBD plays an im-portant role in treatment. The procedure brings a decrease in plasma bilirubin level, as well as improve-ment in life quality by relieving symptoms associated with jaundice, thus optimizing the clinical state of patient, allowing for resection or palliative radio or chemotherapy1,2.
CASE PRESENTATION
A 72-year-old man presented to our hospital with intense jaundice, dark urine, and light-colored stools. Regarding his disease history, we must mention that he had been operated, 5 months earlier, for massive carcinoma of the uncinate process of the pancreas. At that time, the patient presented important weight loss, vomiting, and abdominal pain, but had no jaun-dice. The computed tomography showed pancreatic tumor complicated with total stenosis of the second duodenum. The approach was a palliative interven-tion. Surgeons created a posterior transmesocolic
gastrojejunostomy and Braun s anastomosis in or-der to restore digestive transit. Five months later, at presentation, laboratory findings showed cholestasis (bilirubin level – 16 mg/dl), hepatic cytolysis, positive inflammatory tests (erythrocyte sedimentation rate – 50 mm/h and positive C reactive protein), moderate anemia. We performed esophago-gastro-duodenosco-py, which revealed total stenosis of the duodenum because of tumoral invasion and gastrojejunostomy but we could not pass the stenosis, so papilla was unreachable. The ultrasound examination showed dilated intra- and extrahepatic bile ducts (Figure 1, Figure 2) and hypoechoic pancreatic mass with im-precise delimitation (Figure 3).
Taking into account that an ERCP procedure was not an option, we decided to drain the bile by percutaneous methods, using ultrasound and fluoro-scopic guidance. Regarding the management, we started by administering broad spectrum antibiotics before the procedure. Afterward, the patient received intravenous conscious sedation (Midazolam). We in-jected Lidocaine 1% for local anesthesia. Then, we inserted a Chiba needle under ultrasound guidance and accessed the intrahepatic bile duct of the left lobe. The contrast was injected to opacify the intra-hepatic bile ducts. The percutaneous cholangiogram showed dilated bile ducts in both left and right lobe and also a 14 mm common bile duct with distal stric-ture on the last 2 cm. Under fluoroscopic guidance, we placed a guidewire. The stricture could not be overcame, so we inserted an 8Fr bougie in order to dilate it. Finally, an 8Frx35cm biliary drainage cath-eter was inserted and bile stasis was externalized. The tube was sutured to the skin.
the guidewire a biliary dilator and injected contrast to confirm position. Bile drainage was subsequently obtained by percutaneous placement of fully covered self-expandable metal stent (SEMS).Conclusions. The particularity of the case is the fact that biliary drainage can be difficult to obtain when the anatomy has been modified. In these cases, per-cutaneous drainage under ultrasound guidance repre-sents an alternative to ERCP, when the duodenum is obstructed and the papillary access is impossible.
Keywords: percutaneous biliary drainage, ultrasound, radiologic guidance.
avons inséré sous rayons X un fil de guidage bien placé dans le duodénum distal. Ensuite, nous avons extrait le drainage biliaire sur le fil guide, avancé sur le fil guide un dilatateur biliaire et injecté la substance de contraste pour confirmer la position. Le drainage bili-aire a ensuite été obtenu par emplacement percutané d’un stent métallique auto-expansible entièrement re-couvert (SEMS).Conclusions. La particularité du cas est le fait que le drainage biliaire peut être difficile à obtenir lorsque l’anatomie a été modifiée. Dans ces cas, le drainage percutané sous échographie représente une alterna-tive à la cholangio-pancréatographie endoscopique ré-trograde (CPRE), lorsque le duodénum est obstrué et l’accès papillaire est impossible.
Mots-clés: drainage biliaire percutané, échographie, guidage radiologique.
Archives of the Balkan Medical Union
June 2017 / 227
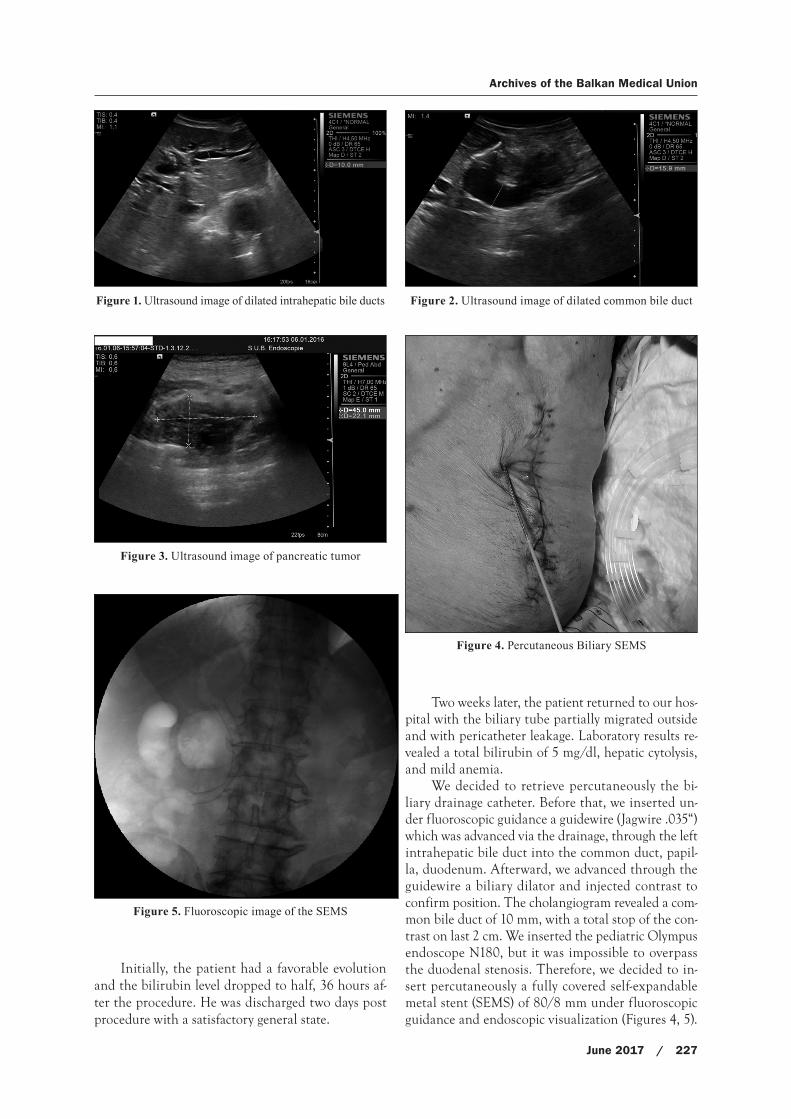
Initially, the patient had a favorable evolution and the bilirubin level dropped to half, 36 hours af-ter the procedure. He was discharged two days post procedure with a satisfactory general state.
Two weeks later, the patient returned to our hos-pital with the biliary tube partially migrated outside and with pericatheter leakage. Laboratory results re-vealed a total bilirubin of 5 mg/dl, hepatic cytolysis, and mild anemia.
We decided to retrieve percutaneously the bi-liary drainage catheter. Before that, we inserted un-der fluoroscopic guidance a guidewire (Jagwire .035“) which was advanced via the drainage, through the left intrahepatic bile duct into the common duct, papil-la, duodenum. Afterward, we advanced through the guidewire a biliary dilator and injected contrast to confirm position. The cholangiogram revealed a com-mon bile duct of 10 mm, with a total stop of the con-trast on last 2 cm. We inserted the pediatric Olympus endoscope N180, but it was impossible to overpass the duodenal stenosis. Therefore, we decided to in-sert percutaneously a fully covered self-expandable metal stent (SEMS) of 80/8 mm under fluoroscopic guidance and endoscopic visualization (Figures 4, 5).
Figure 1. Ultrasound image of dilated intrahepatic bile ducts
Figure 3. Ultrasound image of pancreatic tumor
Figure 5. Fluoroscopic image of the SEMS
Figure 4. Percutaneous Biliary SEMS
Figure 2. Ultrasound image of dilated common bile duct

Percutaneous transhepatic biliary drainage in a patient with malignant stenosis… – CONSTANTINESCU et al
228 / vol. 52, no. 2
We successfully deployed the stent through the pa-pilla in the duodenum, the final position being con-firmed by injecting contrast via a biliary dilator.
After the procedure, we repeated the ultra-sound which confirmed the correct position of the stent (Figure 6) and also the presence of significant aerobilia, demonstrating the biliary drainage into the duodenum (Figure 7).
Two days later, the patient was discharged with satisfactory general state and a bilirubin level of 2 mg/dl.
This case highlights the need of ultrasound guidance combined with radiological guidance in performing PTBD in a patient with modified diges-tive anatomy.
DISCUSSIONS
In a patient with obstructive jaundice caused by biliary malignant stenosis, palliation is usually achieved by endoscopic insertion of an endoprosthe-sis for internal bile drainage. Endoscopic treatment can be difficult or impossible after duodenal malig-nant obstruction or after surgery when the normal anatomy has been changed. In these patients, per-cutaneous methods can be used to achieve adequate bile drainage3.
We presented from our practical experience the case of a patient with obstructive jaundice due to pancreatic carcinoma. One particularity of this case report is that the patient had altered anatomy which made impossible the drainage by using clas-sical me thods. The alternative would have been the surgical approach, with more immediate risks. So, we performed PTBD using ultrasound and radiological guidance. Another particularity could be the paucity of reports regarding this approach if we take into con-sideration that ERCP and biliary stenting fails in only
5–10% of patients with malignant biliary obstruction because papilla is inaccessible4.
Percutaneous Transhepatic Biliary Drainage (PTBD) was introduced in the 1960s. It is most often performed using a hybrid approach with ultrasound and radiological guidance. PTBD can provide biliary drainage in three ways. The simplest of these is exter-nal drainage through a percutaneous tube which exits the skin. The method is typically used when a tight stricture cannot be traversed with a guidewire. The second technique involves inserting a directional cath-eter through the percutaneous sheath and advancing it through the biliary obstruction. The internal-external catheter allows bile to drain externally and/or internal-ly. The third technique establishes internal drainage by percutaneous placement of a plastic or self-expandable metal stent across the biliary stricture5,6.
Indications for percutaneous biliary drainage include relief of obstructive jaundice, cholangitis, brachytherapy access for malignant lesions, failed en-doscopic biliary drainage or surgically altered anato-my which usually precludes endoscopy6,7.
Studies2,8,9 have shown that PTBD prolongs life of the incurably ill, but is burdened with a large num-ber of complications and inconveniences in further treatment. The complication rate can be important, and depends on the patient status and diagnosis. Patients with cholangitis, stones, coagulopathies, proximal or malignant obstruction, will have higher complication rates10. Complications may occur during the procedure (intrahepatic bile ducts perforation, hemobilia, extrahepatic bile ducts perforation) or af-ter the procedure (drain dislocation, hemobilia, peri-tonitis, sepsis, biliary fistula, fluid accumulation)1.
Several authors have suggested that complica-tions related to internal/external tubes as a result of inadequate bile flow and tube dislodgment (sep-sis and hemorrhage) can be minimized by placing a
Figure 6. SEMS image in pancreatic head Figure 7. Aerobilia post SEMS insertion

Archives of the Balkan Medical Union
June 2017 / 229
self-retaining tube of at least 10 Fr through the am-pulla or anastomosis10. Moreover, PTBD should not be performed on patients with non-dilated bile ducts, because of high risk of complications11.
In our case, the post-procedure complication was drain dislocation, which also appeared in other stud-ies12. After this complication, we decided to retrieve the drain and insert percutaneously a fully covered self-expandable metal stent. Relieving bile ducts ten-sion with subsequent bile supply to the alimentary tract caused immediate improvement in the patient’s general condition.
Endoscopic ultrasound (EUS)-guided biliary drainage (EUS-BD) is a recently developed alternative to PTBD for patients in whom ERCP is not an op-tion13. Also known as ESCP (endosonographic chol-angiopancreatography), it combines EUS and ERCP techniques, to obtain biliary of pancreatic drainage.
The complexity of ESCP, with a significant learn-ing curve and the potential for complications and tech-nical failure, makes it very inaccessible even though in the last decade has started to replace PTBD14.
CONCLUSIONS
Jaundice secondary to malignant bile duct ob-struction is commonly treated by endoscopic inser-tion of an endoprosthesis. If the endoscopic pro-cedure is unsuccessful or cannot be performed, percutaneous drainage using a hybrid ultrasound and radiological guidance technique by inserting either a biliary drainage or a metallic expandable stent is a generally accepted alternative, in selected patients.
REFERENCES
1. Knap D, Orlecka N, Judka R et al. Biliary duct obstruction treatment with aid of percutaneous transhepatic biliary drainage. Alexandria Journal of Medicine 2016; 52:185–191.
2. Ciesielczyk B, Murawa D. Percutaneous drainage of biliary ducts. Rep Pract Oncol Radiother 2004;9:69-72.
3. Cwikiel W. Percutaneous management of occluded biliary duct endoprostheses. Acta Radiologica 2000 (41): 338–342.
4. Bapaye A, Dubale N, Aher A. Comparison of endosonogra-phy-guided vs. percutaneous biliary stenting when papilla is inaccessible for ERCP. United European Gastroenterol J. 2013; 1(4): 285–293.
5. Katz MHG, Ahmad SA. Multimodality management of bor-derline resectable pancreatic cancer. Endoscopic and per-cutaneous biliary drainage procedures: role in preoperative management, diagnosis and palliation. Springer 2016:50-70.
6. Nedelcu C, Ilie M, Șandru V, et al. Percutaneous transhe-patic cholangio-drainage and biliary stent placement – a ren-dez-vous procedure in a patient with Billroth II anastomosis, Filodritto ISI proceedings, 2016.
7. Brant WE, Helms CA. Fundamentals of Diagnostic Radiology. Lippincott Williams & Wilkins-4th Edition 2012; 24:666-668.
8. Gazzaniga GM, Faggioni A, Bondanzi G, Bagardo C, Filauro M. Percutaneus transhepatic biliary drainage – twelve years experience. Hepatogastroenterology 1991;38:154-59.
9. Malangoni MA, Mc Coy M, Richardson JD, Flint LM. Effective palliation of malignant biliary duct obstruction. Ann Surg 1985;201:554-59.
10. Saad WEA, Wallace MJ, Wojak JC, Kundu S, Cardella JF. Quality improvement guidelines for percutaneous transhe-patic cholangiography, biliary drainage, and percutaneous cholecystostomy. J Vasc Interv Radiol 2010; 21:789 –795.
11. Cozzi G, Severini A, Civelli E, et al. Percutaneous transhe-patic biliary drainage in the management of postsurgical biliary leaks in patients with nondilated intrahepatic bile ducts. Cardiovasc Intervent Radiol. 2006;29(3):380–8.
12. Robson PC, Heffernan N, Gonen M, et al. Prospective study of outcomes after percutaneous biliary drainage for malig-nant biliary obstruction. Ann Surg Oncol 2010;17:2303–11.
13. Hara K, Yamao K, Mizuno N et al. Endoscopic ultrasonog-raphy-guided biliary drainage: Who, when, which, and how? World J Gastroenterol 2016; 22(3): 1297–1303.
14. Perez-Miranda M., Barclay R., Kahaleh M. Endoscopic ultra-sonography – guided endoscopic retrograde cholangiopan-creatography (ERCP) – therapeutic and advanced ERCP. Gastrointest Endoscopy Clin N Am 2012; 22: 491-509.


















