Peptide Blocking of PD-1/PD-L1 Interaction for Cancer ... · PD-L1 is expressed on many types of...
12
Research Article Peptide Blocking of PD-1/PD-L1 Interaction for Cancer Immunotherapy Chunlin Li 1,2 , Nengpan Zhang 1 , Jundong Zhou 3 , Chen Ding 1,4 , Yaqing Jin 1,2 , Xueyuan Cui 1,5 , Kefeng Pu 1 , and Yimin Zhu 1 Abstract Immunotherapy has become a promising alternative therapeu- tic approach for cancer patients. Interruption of immune check- points, such as CTLA-4 and PD-1, has been verified to be a successful means for cancer therapy in clinical trials. mAb target- ing PD-L1 has been approved to treat urothelial carcinoma, non– small cell lung cancer, or Merkel cell carcinoma by the FDA. However, the high cost of the antibody can limit its application. In our study, targeting PD-L1 peptide (TPP-1), which specifically binds to PD-L1 with high affinity, was identified through bacterial surface display methods. Using a T-cell activation assay and mixed lymphocyte reaction, TPP-1 was verified to interfere with the interaction of PD-1/PD-L1. To examine the inhibitory effect of TPP-1 on tumor growth in vivo, a xenograft mouse model using H460 cells was established. The growth rate of tumor masses in TPP-1 or PD-L1 antibody–treated mice was 56% or 71% lower than that in control peptide–treated mice, respectively, indi- cating that TPP-1 inhibits, or at least retards, tumor growth. IHC of the tumors showed that IFNg and granzyme B expres- sion increased in the TPP-1 or PD-L1 antibody–treated groups, indicating that TPP-1 attenuates the inhibitory effect of PD-L1 on T cells and that T cells may get reactivated. On the basis of our data, TPP-1 peptide could work as an alternative to antibodies for tumor immunotherapy. Cancer Immunol Res; 6(2); 178–88. Ó2017 AACR. Introduction To become fully activated, T cells need to receive antigen- independent costimulatory signals through the corresponding receptors. However, coinhibitory receptors are also expressed on T cells to regulate their activation, tolerance, and immunopathol- ogy, thereby balancing the immune system (1). Cytotoxic T lymphocyte–associated protein 4 (CTLA-4, CD152; ref. 2) is a critical inhibitory receptor expressed on cytotoxic T lymphocyte cells and acts as an important brake in the regulation of cell-cycle progression. Ipilimumab, an mAb targeting CTLA-4, was the first immunotherapeutic antibody drug approved by the FDA in 2011 (3) for the treatment of advanced melanoma. Although cancer immunotherapy with anti–CTLA-4 has achieved modest success in clinical practice in the past several years, data collected from both animal experiments and clinical trials indicate a potential risk of autoimmunity or other severe adverse events related to anti–CTLA-4 administration (3, 4). Programmed cell death 1 (PD-1, CD279) and programmed cell death ligand 1 (PD-L1, B7-H1, CD274) are recognized as promising targets for cancer immunotherapy (2, 4). Preliminary clinical findings of the mAbs targeting PD-1/PD-L1 show equivalent antitumor activity but moderate side effects compared with targeting CTLA-4 (5, 6). B7-1 (CD80) and B7-2 (CD86), the ligands of CTLA-4, are expressed on antigen-present- ing cells (APC). Blockade of CTLA-4 primarily activates T cells in secondary lymphoid organs (4, 7) and, therefore, has a systemic impact that is not confined to the tumor microenvironment (TME) only, which may explain why mAbs targeting the CTLA- 4 pathway can induce severe autoimmune disease or other adverse events. PD-L1 is expressed on many types of cancers (8–10), and its high expression in tumor cells or presence in TME can be indic- ative of tumor-infiltrating lymphocytes (11). Blockade of PD-1/ PD-L1 can strengthen the function of effector T cells and increase their production of cytokines through reactivation (1, 12). It mainly has local and regional influence on the immune system, although some systemic side effects can occur. Compared with CTLA-4 antibody, which can have severe systemic side effects, the blockade of PD-1/PD-L1 pathway could be viewed as relatively safer than that of CTLA-4 (4). Therefore, the application of drugs targeting PD-1/PD-L1 immune checkpoint could be a more promising approach for the cancer immunotherapy. Three PD-L1 mAbs, atezolizumab, durvalumab (MEDI4736), and avelumab (13–15), have been approved by the FDA. Although the anti- bodies have made great progress in cancer treatment, their appli- cation in patients is still limited due to high production costs and immunogenicity. Specific binding peptides have the advantage of much lower production cost and amenability to chemical synthesis. Peptide therapeutics, such as the GLP-1 peptide (approved by the FDA for the treatment of type II diabetes), have gained wide application in the clinic (16). Peptides targeting cancer cells, cytokines, and 1 CAS Key Laboratory of Nano-Bio Interface, Suzhou Institute of Nano-Tech and Nano-Bionics, Chinese Academy of Sciences, Suzhou, China. 2 University of Chinese Academy of Sciences, Beijing, China. 3 Nanjing Medical University, Affiliated Suzhou Hospital, Department Radio Oncology, Suzhou, China. 4 China Pharmaceutical University, Nanjing, China. 5 Shanghai University, Shanghai, China. Note: Supplementary data for this article are available at Cancer Immunology Research Online (http://cancerimmunolres.aacrjournals.org/). Corresponding Author: Yimin Zhu, Suzhou Institute of Nano-Tech and Nano- Bionics, 398 Ruoshui Road, Suzhou Industrial Park, Suzhou 215123, China. Phone: 8605-12628-72618; Fax: 8605-12628-72553; E-mail: [email protected] doi: 10.1158/2326-6066.CIR-17-0035 Ó2017 American Association for Cancer Research. Cancer Immunology Research Cancer Immunol Res; 6(2) February 2018 178 on May 19, 2020. © 2018 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from Published OnlineFirst December 7, 2017; DOI: 10.1158/2326-6066.CIR-17-0035
Transcript of Peptide Blocking of PD-1/PD-L1 Interaction for Cancer ... · PD-L1 is expressed on many types of...

Research Article
Peptide Blocking of PD-1/PD-L1 Interaction forCancer ImmunotherapyChunlin Li1,2, Nengpan Zhang1, Jundong Zhou3, Chen Ding1,4, Yaqing Jin1,2,Xueyuan Cui1,5, Kefeng Pu1, and Yimin Zhu1
Abstract
Immunotherapy has become a promising alternative therapeu-tic approach for cancer patients. Interruption of immune check-points, such as CTLA-4 and PD-1, has been verified to be asuccessful means for cancer therapy in clinical trials. mAb target-ing PD-L1 has been approved to treat urothelial carcinoma, non–small cell lung cancer, or Merkel cell carcinoma by the FDA.However, the high cost of the antibody can limit its application.In our study, targeting PD-L1 peptide (TPP-1), which specificallybinds to PD-L1with high affinity, was identified through bacterialsurface displaymethods. Using a T-cell activation assay andmixedlymphocyte reaction, TPP-1 was verified to interfere with theinteraction of PD-1/PD-L1. To examine the inhibitory effect of
TPP-1 on tumor growth in vivo, a xenograft mouse model usingH460 cells was established. The growth rate of tumor masses inTPP-1 or PD-L1 antibody–treated mice was 56% or 71% lowerthan that in control peptide–treated mice, respectively, indi-cating that TPP-1 inhibits, or at least retards, tumor growth.IHC of the tumors showed that IFNg and granzyme B expres-sion increased in the TPP-1 or PD-L1 antibody–treated groups,indicating that TPP-1 attenuates the inhibitory effect of PD-L1on T cells and that T cells may get reactivated. On the basis ofour data, TPP-1 peptide couldwork as an alternative to antibodiesfor tumor immunotherapy. Cancer Immunol Res; 6(2); 178–88.�2017 AACR.
IntroductionTo become fully activated, T cells need to receive antigen-
independent costimulatory signals through the correspondingreceptors. However, coinhibitory receptors are also expressed onT cells to regulate their activation, tolerance, and immunopathol-ogy, thereby balancing the immune system (1). Cytotoxic Tlymphocyte–associated protein 4 (CTLA-4, CD152; ref. 2) is acritical inhibitory receptor expressed on cytotoxic T lymphocytecells and acts as an important brake in the regulation of cell-cycleprogression. Ipilimumab, an mAb targeting CTLA-4, was the firstimmunotherapeutic antibody drug approved by the FDA in 2011(3) for the treatment of advanced melanoma. Although cancerimmunotherapy with anti–CTLA-4 has achieved modest successin clinical practice in the past several years, data collected fromboth animal experiments and clinical trials indicate a potentialrisk of autoimmunity or other severe adverse events related toanti–CTLA-4 administration (3, 4). Programmed cell death 1(PD-1, CD279) and programmed cell death ligand 1 (PD-L1,
B7-H1, CD274) are recognized as promising targets for cancerimmunotherapy (2, 4).
Preliminary clinical findings of themAbs targeting PD-1/PD-L1show equivalent antitumor activity but moderate side effectscompared with targeting CTLA-4 (5, 6). B7-1 (CD80) and B7-2(CD86), the ligands of CTLA-4, are expressed on antigen-present-ing cells (APC). Blockade of CTLA-4 primarily activates T cells insecondary lymphoid organs (4, 7) and, therefore, has a systemicimpact that is not confined to the tumor microenvironment(TME) only, which may explain why mAbs targeting the CTLA-4pathway can induce severe autoimmunedisease or other adverseevents.
PD-L1 is expressed on many types of cancers (8–10), and itshigh expression in tumor cells or presence in TME can be indic-ative of tumor-infiltrating lymphocytes (11). Blockade of PD-1/PD-L1 can strengthen the function of effector T cells and increasetheir production of cytokines through reactivation (1, 12). Itmainly has local and regional influence on the immune system,although some systemic side effects can occur. Compared withCTLA-4 antibody, which can have severe systemic side effects, theblockade of PD-1/PD-L1 pathway could be viewed as relativelysafer than that of CTLA-4 (4). Therefore, the application of drugstargeting PD-1/PD-L1 immune checkpoint could be a morepromising approach for the cancer immunotherapy. Three PD-L1mAbs, atezolizumab, durvalumab (MEDI4736), and avelumab(13–15), have been approved by the FDA. Although the anti-bodies have made great progress in cancer treatment, their appli-cation in patients is still limited due to high production costs andimmunogenicity.
Specific binding peptides have the advantage of much lowerproduction cost and amenability to chemical synthesis. Peptidetherapeutics, such as the GLP-1 peptide (approved by the FDA forthe treatment of type II diabetes), have gainedwide application inthe clinic (16). Peptides targeting cancer cells, cytokines, and
1CAS Key Laboratory of Nano-Bio Interface, Suzhou Institute of Nano-Tech andNano-Bionics, Chinese Academy of Sciences, Suzhou, China. 2University ofChinese Academy of Sciences, Beijing, China. 3Nanjing Medical University,Affiliated Suzhou Hospital, Department Radio Oncology, Suzhou, China. 4ChinaPharmaceutical University, Nanjing, China. 5Shanghai University, Shanghai,China.
Note: Supplementary data for this article are available at Cancer ImmunologyResearch Online (http://cancerimmunolres.aacrjournals.org/).
Corresponding Author: Yimin Zhu, Suzhou Institute of Nano-Tech and Nano-Bionics, 398 Ruoshui Road, Suzhou Industrial Park, Suzhou 215123, China. Phone:8605-12628-72618; Fax: 8605-12628-72553; E-mail: [email protected]
doi: 10.1158/2326-6066.CIR-17-0035
�2017 American Association for Cancer Research.
CancerImmunologyResearch
Cancer Immunol Res; 6(2) February 2018178
on May 19, 2020. © 2018 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst December 7, 2017; DOI: 10.1158/2326-6066.CIR-17-0035

membrane receptors have been investigated for the diagnosis andtreatments of cancers (17–19). It has also been demonstrated thatshielding the critical region of peptides by glycosylation or PEGconjugation is effective at reducing immunogenicity (20–22).Peptides with low molecular weights have the ability of goodtissue penetration comparedwith antibodies. Because of their lowmolecular weight, peptides could be delivered into the core oftumor masses (23). In this report, bacterial surface display meth-ods (24) were used to screen a PD-L1–targeting peptide with highaffinity and specificity. In vitro and in vivo experiments showed thatone of PD-L1–binding peptides could interfere with PD-1/PD-L1biological function and, therefore, could be applied as a potentialdrug for tumor immunotherapy.
Materials and MethodsReagents and cell culture
Recombinant human PD-L1 (cat. #10084-H08H), PD-L2(cat. #10292-H08H), GM-CSF (cat. #10015-HNAY), IL4 (cat.#11846-HNAE), IL2 (cat. #11848-HNAY1), bFGF (cat. #10014-HNAE), and recombinant mouse PD-L1 (cat. #50010-M08H)were purchased from Sino Biological Inc. Anti-human PD-L1(cat. #557924, clone MIH1), anti-human PD-1 (cat. #557946,clone MIH4), and anti-human CD4 (cat. # 561841, clone RPA-T4) were purchased from BD Biosciences. Dynabeads MyOneStreptavidin C1 magnetic beads (cat. #65002), Biotin-XXMicroscale Protein Labeling and Detection Kit (cat. #B30756),streptavidin PE (SAPE) conjugates (cat. #S-866), DynaMag-Spin Magnet (cat. #12320D), Dynabeads human T-activatorCD3/CD28 (cat. #11131D), and Ham's F-12K medium (cat.#21127030) were obtained from Thermo Fisher Scientific.Human serum (cat. #ZX101-1) was bought from BeijingZoman Biotechnology Co., Ltd. RPMI1640 medium (cat.#SN30809.01), IMDM (cat. #SH30228.01), penicillin/strepto-mycin solution (cat. #SV30082.01), and FBS (cat.#SV30087.02) were purchased from HyClone. Histopaque-1077 was bought from Sigma Aldrich. BSA V (cat. #A8020)was obtained from Solarbio. Purified functional-grade anti-human CD3 (cat. #16-0039-81) was obtained fromeBioscience. Anti-IFNg (cat. #BA0952) was obtained fromBOSTER. Anti-granzyme B (GZMB; cat. #13588-1-AP) wasobtained from Proteintech. The human IFNg ELISA Kit (cat.#70-EK1802) was bought from Multisciences. Vita-Orange cellviability reagent (cat. #B34302) was bought from Biotool. ThePD-L1 antibody, durvalumab, was a gift from Dingfu Biotarget(12, 25).
The human lung cancer cell line H460 was maintained inRPMI1640 medium and authenticated by short tandem repeattyping method. The human breast cancer cell line MDB-MB-435was obtained from the Chinese Academy of Sciences cell bank.The human breast cancer cell line MDB-MB-231 was kindlyprovided by Professor Guangli Suo (Suzhou Institute of Nano-tech and Nano-Bionics, CAS, Suzhou, China). MDB-MB-231 andMDA-MB-435 were cultured in DMEM medium. CHO-K1 over-expressing PD-L1 (CHO-K1/PD-L1) and its parent cell line,CHO-K1, and the plasmid of plvx-puro/luciferase were kindlyprovided by Icartab Biomed of Suzhou and were maintained inF-12K medium. The media were all supplemented with 10% FBSand 1% penicillin/streptomycin, and all cultured at 37�C, 5%CO2. All cells lines were tested to be free from mycoplasmacontamination by a mycoplasma genus-specific PCR.
Screening of binding peptides to PD-L1 from a random displaylibrary
A random bacterial surface display library was kindly providedby Professor Patrick S. Daugherty (University of California, SantaBarbara, Santa Barbara, CA). Peptides with 15 randomized aminoacid sequences were displayed at the N-terminus of enhancedcircularly permuted OmpX (eCPX), an outer membrane pro-tein of Escherichia coli. These bacteria express the peptideand eCPX simultaneously under the control of the araBADpromoter (24), and the library size consisted of 5 � 108 clones.PD-L1 was biotinylated and binding (the quantity of biotin)was detected according to the protocol for the Biotin-XXMicroscale Protein Labeling Kit with FluoReporter BiotinQuantitation Assay Kit.
Isolation of peptide–bacteria complexes was performed aspreviously reported with some modification (26). Briefly, thelibrary size was reduced by magnetic-activated cell sorting(MACS) with 40 nmol/L biotinylated PD-L1. After MACS, thenew library was grown further, and the library size was estimated.MACSwas repeated until the library sizewas smaller than 1� 107,and then FACS was performed using a FACS Aria II (BectonDickinson). The concentration range of PD-L1 that we used forscreeningwas from40 to 10nmol/L. The incubation duration andtemperature for the peptide library with biotinylated PD-L1 was45 minutes at 4�C. Following PD-L1 incubation, SAPE (finalconcentration, 5 nmol/L) was added and incubated for 30 min-utes. The bacteria with higher fluorescence intensity were sortedby flow cytometry and cultured in LB medium overnight for thenext screening round. To improve specificity, 1% (v/v) humanserumwas added in the last three to five rounds. Once the bindingrate andmean fluorescence intensity stopped increasing after twoconsecutive rounds, the bacterial cloneswere collected and sent toGENEWIN Inc. for DNA sequencing.
Construction of the focused libraryThe focused library with the format X5CWCWRX5 on the
N-terminus of eCPX was constructed by using degenerate codeNVS oligonucleotides (27, 28) as the forward primer. Construc-tion of the focused bacterial display peptide library was per-formed as described previously (29). In short, the procedureinvolved preparing the vector and the insert DNA segment,performing test ligations, producing electro-competent E.coli cells(MC1061), transforming the ligation, and counting the librarysize. Ten clones from LB agar plates were randomly selected andwere sequenced to evaluate the quality. Focused library screeningprocedures were performed as already described in the methods.Starting concentration of PD-L1 was 10 nmol/L, and 3% (v/v)human serum was added in the following screening.
Binding property analysis of peptides displayed on bacterialsurfaces
The binding properties of clones to PD-L1 were comparedunder four conditions: (i) at the concentration of 2 nmol/L;(ii) at different concentrations ranging from 0.2 to 4.8 nmol/L;(iii) undergoing rigid washing or normal washing procedures;and (iv)with the additionof BSA, IL4, IFNg , or bFGF. Thebacterialclones undergoing "rigid washing" were suspended in PBS (pH7.4) and incubated at 4�C for 5 minutes, whereas the clonesundergoing "normal washing" were suspended only in PBS. Thebinding ability of clones under the above conditions was mea-sured by flow cytometry.
Effect of PD-L1–Targeting Peptide on Cancer Immunotherapy
www.aacrjournals.org Cancer Immunol Res; 6(2) February 2018 179
on May 19, 2020. © 2018 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst December 7, 2017; DOI: 10.1158/2326-6066.CIR-17-0035

Measuring the KD value of TPP-1 to PD-L1TPP-1 (TPP-1: SGQYASYHCWCWRDPGRSGGSK) was synthe-
sized at GL Biochem Ltd, and the N-termini of the peptideswere labeled with FITC. A scrambled TPP-1 peptide namedSPP-1 (SPP-1: SGQGYRWDSYRWHPSCACGGSK) was designedand synthesized and served as a control (26).
The affinity constant (KD) and kinetics (ka and kd) of TPP-1peptide binding to PD-L1 were determined by surface plasmonresonance (SPR, BiacoreT200). PD-L1 was immobilized on thesurface of a XanTex sensor chip. The remaining reactive sites wereclosed by 1 mol/L ethanolamine at the flow rate of 10 mL/minutefor 7minutes. TPP-1was dissolved anddilutedwithHEPES buffer(HBS, pH 7.4). Peptide concentrations were 0.625, 1.25, 2.5, 5.0,and 10.0 mg/mL. Each sample was injected at a flow rate of 25mL/minute for about 15 minutes. KD, ka, and kd were calculatedby BiacoreT200 Evaluation Software, version 2.0.
Examination of binding specificity of the soluble peptidesThe binding specificity of TPP-1 to PD-L1 was examined with
both a fluorescence-based ELISA and cell-based analyses. Forfluorescence-based ELISA analysis, fluorescence plates (Costar)were coated with 100 mL (1 mg/mL) of human PD-L1 (hPD-L1),human PD-L2 (hPD-L2), mouse PD-L1 (mPD-L1), or BSA in PBS(pH 7.4) overnight at 4�C. Plates were then blocked with 1% BSAin PBST (PBS with 0.05% Tween 20) for 1 hour at room temper-ature. After washing twice with PBST, the peptides (20 mmol/L)were added into each well and incubated for another 1.5 hours atroom temperature. Afterward, the plates were washed three timeswith PBST. The relative fluorescence intensity of each well wasdetermined by Cytation 3 (BioTek) using 488 nm excitation and515 nm emission wavelengths.
Cell-based analysis was performed on both attached anddetached cells by flow cytometry and fluorescence microscopy,respectively. CHO-K1, CHO-K1/PD-L1, MDA-MB-231, andMDA-MB-435 cells were detachedwith 0.25% trypsin and dilutedto a final concentration of 1� 106 cells/mL. Afterward, cells wereincubated with 4 mmol/L FITC-labeled peptides or PD-L1 anti-body (BD Biosciences) for 40 minutes on an inversion shaker at4�C, and then, each tubewaswashedwith PBS twice and analyzedwith a flow cytometer.
For thefluorescencemicroscopy, CHO-K1 andCHO-K1/PD-L1were seeded in a 12-well plate (2� 105 cells/well). At 70% to 80%confluency, cells were washed with PBS twice, followed by block-ing with 1% BSA for 10 minutes. FITC-labeled peptides wereadded at a final concentration of 10 mmol/L and incubated for 30minutes at room temperature. Afterward, cells were washed withPBS twice and fixed with 4% paraformaldehyde. Cell nuclei werestained with Hoechst 33342 (2 mg/mL; Sigma Aldrich) for 10minutes and then washed with PBS twice. Cells were visualizedunder a fluorescent microscope (Nikon Ti).
Ligand inhibition assayExamination of the interference of TPP-1 peptides on the
binding of PD-L1 to PD-1 or durvalumab was performed witha fluorescence-based ELISA and cell-based analyses. For fluores-cence-based ELISA analysis, each well of a 96-well plate wasprecoated with 100 mL (1 mg/mL) PD-L1 in PBS overnight at 4�C.On the second day, the plate was blocked with 1% BSA in PBST,and then 100 nmol/L biotinylated PD-1 or durvalumab withFITC- labeled TPP-1 (at the final concentration of 40, 20, 10, 5, or2.5 mmol/L) was added into each well and incubated at room
temperature for 1.5 hours. After being washed twice with PBST,the relative FITC fluorescence intensity was determined by Cyta-tion 3 (488 nm excitation and 515 nm emission). For thedetection of the biotinylated PD-1 or durvalumab signals, SAPE(at the final concentration of 5 nmol/L) was added into wells andincubated for 30 minutes at room temperature. After beingwashed twice with PBST, the relative PE fluorescence intensitywas determined by Cytation 3 (488 nm excitation and 575 nmemission). Cell-based analysis was performed with a flow cyt-ometer. CHO-K1/PD-L1 cells were incubated with TPP-1 peptide(at the final concentration of 40, 20, 10, or 0 mmol/L) plus 100nmol/L biotinylated PD-1 or durvalumab for 60 minutes on aninversion shaker at 4�C. SAPE (5 nmol/L) was added after beingwashed twice with PBS and then incubated for another 30minutes. Samples were analyzed by flow cytometry.
T-cell activation assayHuman peripheral blood mononuclear cells (PBMC) were
isolated from the blood of a healthy donor by the histopaque-1077 as per the manufacturer's instructions. CD4þ T cells wereisolated from PBMCs using FACS, and the sorting efficiency wasdetected by a CD4-APC antibody. To generate CD4þ T-cell blasts,cells were adjusted to 5 � 105 cells/mL in IMDM with 10% FBSand IL2 (20 ng/mL), followed by the addition of human T-activator CD3/CD28 beads (bead-to-cell ratio was 1:1). Freshmedium was added every other day, and cells were harvested andfrozen at day 7 for later use.
For each test well in the 96-well plate, 100 mL anti-human CD3(1 mg/mL) was added into each well and incubated at 4�Covernight. On the second day, the antibody solution was aspi-rated out, and wells were washed with 200 mL PBS twice. After-wards, 100 mL PD-L1 at the final concentration of 0.1 mg/mL wasadded into the wells, and plates were held in the 37�C incubatorfor 3 hours, followed by washing with PBS twice. Next, durvalu-mab and peptides (TPP-1 or SPP-1) at various concentrationswere added into the corresponding wells, and the plates wereincubated at 37�C for 1 hour followed by two washes with PBS.Finally, CD4þ T cells (at the concentration of 5� 104 cells/well in150 mL medium) were added, followed by the centrifugation at1,000 rpm for 2 minutes. Cells were incubated in a humidincubator with 5% CO2 at 37�C for 3 days. Culture supernatantswere collected, and the quantitation of IFNg was detected usingthe human IFNg ELISA Kit. T-cell proliferation rate was evaluatedby the Vita-Orange cell viability reagent (has greater linear rela-tionship between cell number andOD450 value, according to thereagent instructions).
Mixed lymphocyte reactionFresh PBMCs were cultured in IMDM at 37�C for 2 hours and
washed twice with PBS after removing the supernatant. Theremaining cells were cultured in IMDM plus 10% FBS, GM-CSF(25 ng/mL), and IL4 (50 ng/mL). Fresh mediumwas added every3 days.Onday 6, TNFa (50 ng/mL)was added to induce dendriticcells (DC) for 24 hours. PD-L1 expression was detected by flowcytometry. Mature DCs were frozen for later use.
Before mixed lymphocyte reactions (MLR), DCs were treatedwith mitomycin C (MMC, 100 mg/mL) for 2 hours. The frozenCD4þT cellswere thawed and cultivated overnight. About 1�105
cells were seeded in each well with a DC:T ratio of 1:10 in 200 mLIMDM plus 10% FBS. IFNg in supernatants and cell proliferationwas quantified at day 3.
Li et al.
Cancer Immunol Res; 6(2) February 2018 Cancer Immunology Research180
on May 19, 2020. © 2018 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst December 7, 2017; DOI: 10.1158/2326-6066.CIR-17-0035

In vivo studiesFive- to 6-week-old female Balb/c nudemice (SLAC Laboratory
Animal) were used in this experiment to evaluate antitumoractivity in vivo, and mice were housed in environmentally con-trolled, specific pathogen-free conditions. All animal studies wereapproved by a local Ethics Committee for Animal Experiments.
The FITC-conjugated TPP-1 peptides (4 mg/kg) were injectedsubcutaneously, and the relative FITC fluorescence intensity wasmeasured by the IVIS Lumina II system (PerkinElmer) at timepoints of 0, 6, 12, 24, 48, and 72 hours. The half-life of the peptidein subcutaneous tissue was calculated to determine and assess thepeptide dosing interval.
The H460 cells were transfected with the plvx-puro/luciferaselentiviral vector, followedby selectionwithpuromycin (1mg/mL),and clones with stable expression were established throughmonoclonal cultivation. Human PBMCs were enriched and acti-vated as described above. On the fifth day, PBMCs were addedinto the plates of luciferase-expressing H460 cells (H460-luc),which were treated with mitomycin C, followed by coculturinganother 3 days. H460-luc cells (2 � 106), along with 5 � 105
PBMCs in 0.1 mL PBS, were injected subcutaneously into theflank of the mice. TPP-1 (2 or 4 mg/kg), SPP-1 (4 mg/kg), and
durvalumab (0.1 mg/kg) were injected subcutaneously of eachgroup every other day eight times. The group injected with onlytumor cells, followed by treating with TPP-1 (4 mg/kg), wasappointed as control. The tumor volumes were measured withcalipers in two dimensions (tumor volumes ¼ 1/2 � a � b2, a isthe length and b is the width). The tumor mass was evaluated bymeasuring the bioluminescence with the IVIS Lumina II system(PerkinElmer) every week for a total of five times. All the micewere killed on day 40, and the tumor tissues were collected. Theexpression human IFNg and GZMB in tumor tissues of eachgroup were determined by IHC with corresponding antibodies.Digital pictures were taken by a Zeiss Scope A1, and thepercentage of immuno-positive stained area was assessed usinga digital image analyzing software (ImageJ, http://rsb.info.nih.gov/ij/; ref. 30).
Structure prediction andmodel construction of TPP-1 to PD-L1The three-dimensional model of TPP-1 was predicted through
the local meta-threading server LOMETS (31), and the bindingmodel complex of TPP-1 to PD-L1was described by ZDOCK (32).The Vector NTI-3D Molecular Viewer software (Thermo FisherScientific) was used to visualize the complex of TPP-1 and PD-L1.
SAPE
SAPE
Antigen
PD-L1
PD-L1–binding
PD-L1–binding
PD-L1–binding
PD-1
Peptides
peptides
Biotin
Incu
batio
nIn
duce
d by
arab
inos
e
Waste
FACS
Construction of thefocused libraryBacteria library
displaying peptide
Sequencing& analysis
Amplification
Sequencing &synthesis
Cytokines
Bacterial library
Bacteria
PD-L1
PD-L1 Biotin
TCR MHC Cytokines
bacteria
PD-1
TCR MHC
PD-L1
APCs or
APCs or
tumor cell
tumor cell
T cells
A
B
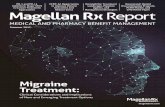
Figure 1.
A and B, Schematic description of the PD-L1–binding peptides screening procedure (A) and mechanisms of how PD-L1–binding peptides activate PD-L1–mediatedinhibition of T cells (B). TCR: T-cell receptor.
Effect of PD-L1–Targeting Peptide on Cancer Immunotherapy
www.aacrjournals.org Cancer Immunol Res; 6(2) February 2018 181
on May 19, 2020. © 2018 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst December 7, 2017; DOI: 10.1158/2326-6066.CIR-17-0035

Statistical analysisAll the data were expressed as means � SEM. Histograms and
line charts were generated by GraphPad Prism 6.0. t tests wereused to determine the P values. A P value <0.05 was considered tobe statistically significant.
ResultsIdentification of the PD-L1–binding peptides from a randomlibrary
A random bacterial surface display library was used to screenand identify the PD-L1–binding peptides. MACS and FACS wereused to enrich the binding peptide for PD-L1 (screening proce-dures shown in Fig. 1A). After one cycle of MACS, the library sizewas about 5 � 106 peptides, and FACS was then used forscreening. After eight cycles of FACS, the percentage of bacteriain the sorting gate increased from 2.1% (40 nmol/L PD-L1) to54.1% (10 nmol/L PD-L1 with 1% human serum; Fig. 2A). Fortybacterial clones were randomly selected for sequencing, and ninedifferent peptide sequences were obtained. The sequences werealigned using Vector NTI software (Fig. 2B), and the consensussequence "CWCWR" was detected using WebLogo 3.3 (Fig. 2C).The soluble peptides of the CWCWR sequence were synthesized,and the binding specificity was tested by flow cytometry withMDA-MB-231 andMDA-MB-435 (Supplementary Fig. S1), whichhad high and low PD-L1 expression, respectively. The results
indicated that the specificity of the consensus sequence neededto be improved.
Identification of peptides with high affinity and specificityTo improve the affinity and specificity of the PD-L1–binding
peptides, a focused library with the format X5CWCWRX5 wasconstructed into pBAD33-eCPX (Supplementary Fig. S2A). Thelibrary size was about 5 � 107 (count of clones on the LB agarplates). The sequencing results (Supplementary Fig. S2B) indi-cated that the quality of this library met requirements andcould be used for the following screening. After one cycle ofMACS and 13 cycles of FACS, the mean fluorescence intensity ofPE-A increased from 31 (10 nmol/L PD-L1) to 1,287 (2 nmol/LPD-L1 with 3% human serum; Fig. 2D). A total of 20 cloneswere selected, and seven different peptide sequences wereobtained (Fig. 2E). No obvious consensus sequence wasidentified.
Binding properties of peptides displayed on the bacterialsurface
The binding properties of peptides displayed on the surface ofbacteria were preliminarily analyzed by flow cytometry. With 2nmol/L PD-L1, clone 1 and clone 3 showed significantly higherbinding ability than clone 2 and random library clones (Supple-mentary Fig. S3A). With the increasing of PD-L1 concentrationfrom 0.2 to 4.8 nmol/L, the binding properties of clone 1 and
Figure 2.
PD-L1–binding peptides were obtained with bacterial surface display methods. A, PD-L1–binding peptides were enriched from the random library with onecycle of MACS and eight cycles of FACS. B, Sequence alignment of the binding peptides from the random library using the Vector NTI software. C, Consensussequence predicted by WebLogo 3.3 and CWCWR was regarded as the consensus sequence. D, PD-L1–binding peptides were enriched from the focusedlibrary with one cycle of MACS and 13 cycles of FACS. E, The sequences of PD-L1–binding peptides screened from the focused library.
Li et al.
Cancer Immunol Res; 6(2) February 2018 Cancer Immunology Research182
on May 19, 2020. © 2018 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst December 7, 2017; DOI: 10.1158/2326-6066.CIR-17-0035

clone 3 showed the same trend (Supplementary Fig. S3B). Bindingabilities of clone 1 and clone 3 both declined significantly whenundergoing the rigid washing procedure after incubation withPD-L1 (Supplementary Fig. S3C). The decline extent of both clone1 and clone3was similar. The additions of BSA, IL4, IFNg , or bFGFinto corresponding incubation systems did not influence thebinding ability (Supplementary Fig. S3D). All these results show
that clone 1 and clone 3 were better than clone 2 in bindingaffinity and specificity, with no significant differences betweenthemselves.
TPP-1 binds specifically to PD-L1 with high affinityThe peptides of clone 1 and clone 3 were synthesized, and
solubility tests indicated that clone 3 was easier to dissolve in the
Figure 3.
The physiochemical properties of TPP-1peptide. A, The binding affinity of TPP-1peptide to PD-L1 examined by an SPRmethod. B, The binding specificity ofTPP-1 to hPD-L1, hPD-L2, mPD-L1, andBSA analyzed by fluorescence-basedELISA (n ¼ 5). C, The binding ability ofTPP-1 to CHO-K1 (dotted) and CHO-K1/PD-L1 (solid) determined by flowcytometry (n ¼ 3). D, The changes influorescence signals of TPP-1-FITC (solidlines) and PD-1-PE (dotted lines) with theincreased concentration of peptideanalyzed by fluorescence-based ELISA(n¼ 3). E, PD-1–binding capacity to CHO-K1/PD-L1 cells in the presence of differentconcentrations of TPP-1 peptides wasanalyzed by flow cytometry (n ¼ 3). F,Changes in fluorescent signals of TPP-1-FITC (solid lines) and durvalumab-PE(dotted lines) with increasingconcentrations of peptide analyzed byfluorescence-based ELISA (n ¼ 3). G,Durvalumab-binding capacity to CHO-K1/PD-L1 cells in the presence of differentconcentrations of TPP-1 peptides wasanalyzed by flowcytometry (n¼ 3). Data,mean � SEM; � , P < 0.05; �� , P < 0.01,unpaired t test.
Effect of PD-L1–Targeting Peptide on Cancer Immunotherapy
www.aacrjournals.org Cancer Immunol Res; 6(2) February 2018 183
on May 19, 2020. © 2018 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst December 7, 2017; DOI: 10.1158/2326-6066.CIR-17-0035

sterile water than clone 1, and thus, clone 3 was chosen for thefollowing experiments and named as TPP-1 (targeting PD-L1peptide 1). A scrambled TPP-1 peptide (SPP-1) was used as acontrol based on ELISA results (Supplementary Fig. S4).
TheKD, ka, and kdof thebindingbetweenTPP-1 andPD-L1weredetermined by the SPR method (Fig. 3A). According to ourpreliminary data, the single mode was used to determine theaffinity and kinetics. Five different concentrations of TPP-1 weretested, and the KD value was 9.467 � 10–8 mol/L (3.022 � 10–4
Ms–1 for ka and 3,192 s–1 for kd).hPD-L2 and mPD-L1 had the most similar amino acid
sequences to PD-L1 as described in previous reports (33, 34), aswell as similar spatial structure. TheELISA results (Fig. 3B) showedthat TPP-1 had no cross-reactivity to mPD-L1 and hPD-L2, indi-cating its specificity to PD-L1.
To evaluate the binding specificity in a more physiologicenvironment, the binding ability of TPP-1 to CHO-K1/PD-L1cells was examined by flow cytometry and fluorescence micros-copy. The expression of PD-L1 in CHO-K1/PD-L1, MDA-MB-231, and MDA-MB-435 was measured by flow cytometry (Sup-plementary Fig. S5A). Compared with MDA-MB-435, CHO-K1/PD-L1, and MDA-MB-231 cell lines had higher PD-L1 expres-sion. TPP-1 had higher binding to CHO-K1/PD-L1 and MDA-MB-231 cells (Fig. 3C; Supplementary Fig. S5B). In contrast,for MDA-MB-435 cells (expression of PD-L1 is relatively low),TPP-1 had low binding (Supplementary Fig. S5B). TPP-1 pep-tide at higher concentrations had comparable staining withPD-L1 mAbs. Similar results were seen for CHO-K1 cells usingfluorescence microscopy (Supplementary Fig. S6). Together,these results confirm that TPP-1 can not only bind specificallyto free PD-L1 but also to cells that expressed PD-L1 on their cellmembrane.
TPP-1 can block the interaction of PD-1 and PD-L1In the ligand inhibition assay, the interference of TPP-1
peptides on the binding of PD-L1 to PD-1 or durvalumab wasinvestigated either using fluorescence-based ELISAs or cell-based analysis. The ELISA results showed that the TPP-1 peptidecould effectively bind to PD-L1, even in the presence of PD-1 ordurvalumab (solid lines of Fig. 3D and F). The fluorescencesignals of PD-1–PE were decreased with the increased concen-tration of TPP-1 peptide. However, the fluorescent signals of
durvalumab-PE did not change significantly (dotted linesof Fig. 3D and F). From these results, we assumed that TPP-1at the tested concentrations did not block durvalumab (100nmol/L) but could interfere the interaction between PD-1 (100nmol/L) and PD-L1. However, our results did not make clearwhether the binding site of TPP-1 to PD-L1 was overlappedwith that of durvalumab. It has been shown that the bindingsite of durvalumab to PD-L1 is highly overlapped with that ofPD-1 (35). Considering the relative lower affinity of TPP-1 toPD-L1, we hypothesized that for TPP-1 to block PD-1/PD-L1interaction, the binding site of TPP-1 to PD-L1 would need tobe overlapped with that of PD-1. Our hypothesis was validatedby flow cytometry (Fig. 3E and G). As the concentration of TPP-1 was increased, the PD-1–binding capacity toward CHO-K1/PD-L1 was decreased. Durvalumab did not show the sametrend.
TPP-1 reverses PD-L1–mediated inhibition of T-cell activationT-cell activation assays were performed to determine whether
TPP-1 could block PD-L1 in culture and, thereby, activate theCD4þ T cells. IFNg production and cell proliferation wereevaluated. In the presence of CD3 antibody, T cells releasedmore IFNg and proliferated significantly, which was reversed bythe addition of PD-L1 at an ED50 of about 5 to 10 mg/mL(Supplementary Fig. S7A), and TPP-1 peptide alone or TPP-1plus PD-L1 did not activate T cells without anti-CD3 (Supple-mentary Fig. S7B). When an antagonist was added, the releaseof IFNg and proliferation was seen, with durvalumab blockingPD-L1 at 68 nmol/L. Similarly, at a TPP-1 concentration of 20mmol/L, both IFNg release (Fig. 4A) and T-cell proliferation(Supplementary Fig. S7C) increased significantly by compari-son, confirming that PD-L1 can block the function and T cell–activating ability of TPP-1.
MLRs were conducted to confirm the activity of TPP-1 in amore physiologic environment, as shown in the schematicillustration (Fig. 1B). Matured DCs had a 16-fold higher PD-L1 expression compared with the control (Supplementary Fig.S8A). CD4þ T cells were activated by CD3/CD28 antibody andIL2. At a TPP-1 concentration of 20 mmol/L, IFNg release wassignificantly higher than control and SPP-1 (Fig. 4B), and all thegroups showed similar outcomes for proliferation (Supplemen-tary Fig. S8B).
1,000
800
600
400
200
0
600
400
200
0
IFN
g (pg
/mL)
IFN
g (pg
/mL)
ControlDurvalumab (68 nmol/L)
Durvalumab(68 nmol/L)
TPP-1 (4 mmol/L)TPP-1 (20 mmol/L)SPP-1 (20 mmol/L)
CD3
PD-L1(10 mg/mL)
(mmol/L)
(mmol/L)
TPP-1
SPP-1
4 20
20
– + +
+ +
+
+ + +
+ + + +
– –
––
–
– – – – – –
– – – –
– – – –
A B
Figure 4.
TPP-1 reactivated T-cell functionverified by T-cell activation assays(A; n ¼ 3) and MLR assay (B; n ¼ 5).The extent of T-cell activation waspositively correlated to the amount ofIFNg production. Data, mean � SEM;� , P < 0.05, unpaired t test.
Li et al.
Cancer Immunol Res; 6(2) February 2018 Cancer Immunology Research184
on May 19, 2020. © 2018 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst December 7, 2017; DOI: 10.1158/2326-6066.CIR-17-0035

07 14
Time (days)
21 28 35
70
5
10
15
Tum
or
volu
me
(mm
3 ;×1
02 )
12 17 22 27 32 0
GZMB IFNg
GZMBIFNg
10
20
Are
a (1
00%
) 30
40
Time (days)
2
4
Tota
l flu
x (p
/s;×
1011
)
64 mg/kg SPP-1
4 mg/kg TPP-1
2 mg/kg TPP-1
0.1 mg/kg Durvalumab
Control
4 mg/kg SPP-14 mg/kg SPP-1
4 mg/kg TPP-1
4 mg/kg TPP-1
2 mg/kg TPP-1
2 mg/kg TPP-1
0.1 mg/kg Durvalumab
0.1 mg/kg Durvalumab
Control
Control
4 mg/kg SPP-1
4 mg/kg TPP-1
2 mg/kg TPP-1
0.1 mg/kg Durvalumab
Control
A
B
C
E
D
Figure 5.
TPP-1 inhibited the tumor growth in a tumor xenograft model via reactivating T-cell function. A, Representative bioluminescence images of tumor-bearingmice for each group (n ¼ 5) on day 21. B, Total bioluminescent signal (p/s) changes for each group at day 7, 14, 21, 28, and 35. C, Tumor volume (mm3) changesmeasured on day 7, 12, 17, 22, 27, and 28. D, Representative images of IFNg and GZMB immunostaining on tumor tissues for each group. Scale bars, 200 mm.Magnification, �40. E, Quantification of IFNg and GZMB expression (n ¼ 5); data, mean � SEM; � , P < 0.05; �� , P < 0.01, one unpaired t test per row.
Effect of PD-L1–Targeting Peptide on Cancer Immunotherapy
www.aacrjournals.org Cancer Immunol Res; 6(2) February 2018 185
on May 19, 2020. © 2018 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst December 7, 2017; DOI: 10.1158/2326-6066.CIR-17-0035

TPP-1 inhibits human tumor growth via a T-cell–dependentmechanism
The in vivo activities of TPP-1 were evaluated in a xenograftmouse model. The H460-luc cell line had high expression ofluciferase and PD-L1 (Supplementary Fig. S9). A mixture of cells,which contained previously activated PBMCs and H460-luc cellsat a ratio of 1:4, were subcutaneously injected into mice, andpeptides were injected every other day based on the half-life of thepeptide in subcutaneous tissue (Supplementary Fig. S10). Therepresentative bioluminescence images of tumor-bearingmice foreach group are shown in Fig. 5A. The total radiance (p/s) (Fig. 5B)and tumor volumes (Fig. 5C) of each group were recorded. Theseresults confirm that durvalumab and TPP-1 can inhibit tumorgrowth (compared with SPP-1 and control) in this xenograftmouse model. The growth rate in TPP-1- or durvalumab-treatedmice was 56% or 71% lower than that in control peptide–treatedmice, respectively. When administered in the absence of T cells(control group), TPP-1 had no effect on the growth of the H460-luc tumors (Fig. 5).
To further verify that the inhibitory effects of TPP-1 on tumorgrowth were mediated by the reactivation of T cells, the expres-sion of IFNg and GZMB in tumor tissues was examined. When Tcells are activated, cytokines, such as IFNg and GZMB, will besecreted to the TME to initiate killing of tumor cells. The resultsfrom IHC (Fig. 5D and E) showed that the expression of IFNgand GZMB increased significantly in the durvalumab and TPP-1groups compared with those in control and SPP-1 groups,which indicated that our peptide inhibited tumor growth byreactivating T cells through blocking the interaction betweenPD-1 and PD-L1.
Prediction of possible binding sites of TPP-1 to PD-L1The secondary structure of TPP-1 was composed of a random
coil and beta-sheet predicted by LOMETS (Supplementary Fig.S11A). The binding model of TPP-1 to PD-L1 (PDB ID of PD-L1:3BIS) was predicted by ZDOCK (Supplementary Fig. S11B). Thebinding position of PD-1 (light sea green) to PD-L1 (space fillmodel in dark khaki) is shown in Supplementary Fig. S11C. Theseresults, combined with the ligand inhibition assay, indicate thatthe binding site of TPP-1 may be close to the PD-1- and PD-L1–binding pocket.
DiscussionThe interference of PD-1/PD-L1 interaction has yielded
impressive progress in the immunotherapy of cancers. In thisreport, PD-L1–targeting peptides were identified with bacterialsurface display methods through random library and focusedlibrary screening, sequentially. The binding property of a can-didate peptide named TPP-1 was investigated. The resultsshowed that TPP-1 could bind specifically to PD-L1 with highaffinity and block PD-1/PD-L1 interaction. TPP-1 lead to thereactivation of the T cells in in vitro and in vivo assays, whichindicates that TPP-1 could work as inhibitory candidate forPD-L1 to treat cancers.
The KD value is an important parameter to evaluate thebinding affinity of two molecules. The KD value of PD-L1 withits natural binding ligand, PD-1, is about 500 nmol/L (34). Inour study, the KD value of PD-L1 with TPP-1 peptide is about 95nmol/L (around five times less than that with PD-1), meaningthat the affinity between TPP-1 and PD-L1 is higher than that
between PD-1 and PD-L1. The binding site of TPP-1 to PD-L1 isclose to the interactive site of PD-1 and PD-L1 (36) predicted byZDOCK software, which may indicate that TPP-1 could inter-fere with the binding ability of PD-1 to PD-L1 and potentiallyact as blockade molecule.
A xenograft mouse model was used to evaluate the ability ofTPP-1 to reactivate T cell–mediated tumor cell killing. Thebioluminescence signal and tumor volumes were assessed toevaluate the antitumor activity of TPP-1 mediated by thereactivation of T cells. Around 4 weeks after inoculation ofpreviously activated T cells with H460-luc cells, the biolumi-nescence signals and tumor volumes in all five groupsincreased significantly compared with those in the first 3weeks. However, there existed significant differences amongthe groups. The volume of tumors and the bioluminescentsignals of tumor masses in durvalumab and TPP-1 groups didnot increase as fast as those in control and SPP-1 groups. Thismay indicate that T cells were reactivated and had cytotoxiceffects on cancer cells. To test our speculation, the expressionof IFNg and GZMB was examined by IHC. IFNg and GZMB arebiomarkers of T-cell activation and are believed to be producedby CD4þ Th type I cells or CD8þ cytotoxic lymphocytes (37).Expression of these two cytokines in our study could representthe activation extent of T cells in vivo. The expression of IFNgand GZMB increased in durvalumab and TPP-1 (4 mg/kg) incomparison with control and SPP-1 groups, which couldexplain why tumor growth was inhibited by the activation ofT cells. However, we also noticed that after 4 weeks, tumorsseemed to recover from inhibitory effects, and the speed oftumor growth rose (Fig. 5B and C). A reason this occurredmight be due to H460 cell lines having high expression ofPD-L1, which could be stimulated by inflammatory factors(especially IFNg) in the TME (38), which would help tumorcells escape from host immune recognition (39, 40). Mono-therapy targeting only one immune checkpoint, such as CTLA-4, PD-1/PD-L1, was not effective at this stage, which is con-sistent with other researchers' conclusions (12). The combina-tory therapy of our peptides with drugs targeting checkpointsor other treatments (41, 42), such as traditional chemotherapyor radiotherapy, may be a better choice.
Peptides are emerging as an attractive area of therapeuticagents because as potential drugs, they have many advantages,such as low molecular weight, low price, facile synthesis, and soon. In our study, we also showed that our TPP-1 peptide athigher concentrations had comparable effects on inhibitingtumor growth as durvalumab. Although some peptide drugshave been approved for clinical use, like goserelin for breastcancer and prostate cancer (43, 44) and exenatide for type IIdiabetes (45), challenges still exist in the development andwide application of peptide drugs. Peptides used orally are easyto be digested in the stomach, but after they pass the stomach,hydrophilic peptides are difficult to be absorbed by the intes-tine. If peptide drugs are directly injected intravenously, fastrenal clearance, as well as enzymatic degradation in plasma,may occur. However, many attempts have achieved great prog-ress. Researchers have conjugated Fc domains to peptides toavoid enzymatic digestion and designed nanocarriers for pep-tide delivery to prolong their circulation time (46, 47). With theappearance and development of new techniques, we believedthat challenges for the development of peptide drugs can beovercome, and peptides as drugs would be widely used.
Li et al.
Cancer Immunol Res; 6(2) February 2018 Cancer Immunology Research186
on May 19, 2020. © 2018 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst December 7, 2017; DOI: 10.1158/2326-6066.CIR-17-0035

Taken together, we have shown that TPP-1 peptide can specif-ically interact with PD-L1 and block PD-1/PD-L1 interaction. Ithas the potential as a substitution for antibodies in cancerimmunotherapy. Peptides with high affinity and specificity maybe effective candidates for targeting therapy once the properdelivery systems have been established.
Disclosure of Potential Conflicts of InterestNo potential conflicts of interest were disclosed.
Authors' ContributionsConception and design: C. Li, Y. ZhuDevelopment of methodology: C. Li, Y. ZhuAcquisition of data (provided animals, acquired and managed patients,provided facilities, etc.): C. Li, C. Ding, X. CuiAnalysis and interpretation of data (e.g., statistical analysis, biostatistics,computational analysis): C. Li, Y. Zhu
Writing, review, and/or revision of the manuscript: C. Li, Y. Jin, K. Pu, Y. ZhuAdministrative, technical, or material support (i.e., reporting or organizingdata, constructing databases): C. Li, N. Zhang, J. Zhou, Y. ZhuStudy supervision: C. Li, Y. Zhu
AcknowledgmentsThis work was funded by the National Natural Science Foundation of China
(no. 81171451, 81372361, 81602552), Natural Science Foundation of Jiangsuprovince (no. BE2015647), and Science and Technology Bureau of Suzhou(no. SS201649).
The costs of publication of this articlewere defrayed inpart by the payment ofpage charges. This article must therefore be hereby marked advertisement inaccordance with 18 U.S.C. Section 1734 solely to indicate this fact.
Received January 22, 2017; revised July 17, 2017; accepted November 30,2017; published OnlineFirst December 7, 2017.
References1. Keir ME, Butte MJ, Freeman GJ, Sharpel AH. PD-1 and its ligands in
tolerance and immunity. Annu Rev Immunol 2008;26:677–704.2. Pardoll DM. The blockade of immune checkpoints in cancer immuno-
therapy. Nat Rev Cancer 2012;12:252–64.3. Hodi FS,O'Day SJ,McDermott DF,Weber RW, Sosman JA,Haanen JB, et al.
Improved survivalwith ipilimumab in patients withmetastaticmelanoma.N Engl J Med 2010;363:711–23.
4. Topalian SL, Taube JM, Anders RA, Pardoll DM. Mechanism-driven bio-markers to guide immune checkpoint blockade in cancer therapy. Nat RevCancer 2016;16:275–87.
5. Topalian SL, Sznol M, McDermott DF, Kluger HM, Carvajal RD, SharfmanWH, et al. Survival, durable tumor remission, and long-term safety inpatients with advanced melanoma receiving nivolumab. J Clin Oncol2014;32:1020–30.
6. Garon EB, Rizvi NA, Hui RN, Leighl N, Balmanoukian AS, Eder JP, et al.Pembrolizumab for the treatment of non-small-cell lung cancer. N Engl JMed 2015;372:2018–28.
7. Topalian SL, Drake CG, Pardoll DM. Immune checkpoint blockade: acommon denominator approach to cancer therapy. Cancer Cell 2015;27:450–61.
8. Konishi J, Yamazaki K, Azuma M, Kinoshita I, Dosaka-Akita H, NishimuraM. B7-h1 expression onnon-small cell lung cancer cells and its relationshipwith tumor-infiltrating lymphocytes and their PD-1 expression. Clin Can-cer Res 2004;10:5094–100.
9. ThompsonRH,GilletttMD,Cheville JC, LohseCM,DongHD,WebsterWS,et al. Costimulatory B7-H1 in renal cell carcinoma patients: indicator oftumor aggressiveness and potential therapeutic target. Proc Natl Acad SciUSA 2004;101:17174–9.
10. Hino R, Kabashima K, Kato Y, Yagi H, Nakamura M, Honjo T, et al. Tumorcell expression of programmed cell death-1 ligand 1 is a prognostic factorfor malignant melanoma. Cancer 2010;116:1757–66.
11. Thompson RH, Kuntz SM, Leibovich BC, Dong HD, Lohse CM, WebsterWS, et al. Tumor B7-H1 is associated with poor prognosis in renal cellcarcinoma patients with long-term follow-up. Cancer Res 2006;66:3381–5.
12. Stewart R, Morrow M, Hammond SA, Mulgrew K, Marcus D, Poon E, et al.Identification and characterization ofMEDI4736, an antagonistic anti-PD-L1 monoclonal antibody. Cancer Immunol Res 2015;3:1052–62.
13. Rosenberg JE, Hoffman-Censits J, Powles T, van der Heijden MS, Balar AV,Necchi A, et al. Atezolizumab in patients with locally advanced andmetastatic urothelial carcinoma who have progressed following treatmentwith platinum-based chemotherapy: a single-arm, multicentre, phase 2trial. Lancet 2016;387:1909–20.
14. Syed YY. Durvalumab: first global approval. Drugs 2017;77:1369–76.15. KaufmanHL, Russell J, HamidO, Bhatia S, Terheyden P, D'Angelo SP, et al.
Avelumab in patients with chemotherapy-refractory metastatic Merkel cellcarcinoma: a multicentre, single-group, open-label, phase 2 trial. LancetOncol 2016;17:1374–85.
16. De Block CEM, Van Gaal LF. GLP-1 receptor agonists for type 2 diabetes.Lancet 2009;374:4–6.
17. Corti A, Curnis F, Rossoni G, Marcucci F, Gregorc V. Peptide-mediatedtargeting of cytokines to tumor vasculature: the NGR-hTNF example.Biodrugs 2013;27:591–603.
18. Saha A, Mohapatra S, Kurkute P, Jana B, Sarkar J, Mondal P, et al. Targeteddelivery of a novel peptide-docetaxel conjugate to MCF-7 cells throughneuropilin-1 receptor: reduced toxicity and enhanced efficacy of docetaxel.RSC Adv 2015;5:92596–601.
19. Chang HN, Liu BY, Qi YK, Zhou Y, Chen YP, Pan KM, et al. Blocking of thePD-1/PD-L1 interaction by a D-peptide antagonist for cancer immuno-therapy. Angew Chem Int Ed Engl 2015;54:11760–4.
20. Nelson AL, Dhimolea E, Reichert JM. Development trends for humanmonoclonal antibody therapeutics. Nat Rev Drug Discov 2010;9:767–74.
21. Henninot A, Collins JC, Nuss JM. The current state of peptide drugdiscovery: back to the future? J Med Chem 2017 Aug 11. [Epub ahead ofprint].
22. Li W, Joshi MD, Singhania S, Ramsey KH, Murthy AK. Peptide vaccine:progress and challenges. Vaccines 2014;2:515–36.
23. Behr TM, Gotthardt M, Barth A, B�eh�e M. Imaging tumors with peptide-based radioligands. Q J Nucl Med 2001;45:189–200.
24. Rice JJ, Daugherty PS. Directed evolution of a biterminal bacterial displayscaffold enhances the display of diverse peptides. Protein Eng Des Sel2008;21:435–42.
25. Luan Y, Chai D, Peng J, Ma S, Wang M, Ma H, et al. A fully humanmonoclonal antibody targeting PD-L1 with potent anti-tumor activity. IntImmunopharmacol 2016;31:248–56.
26. Chen LS, Li CL, Zhu YM. The HGF inhibitory peptide HGP-1 displayspromising in vitro and in vivo efficacy for targeted cancer therapy. Onco-target 2015;6:30088–101.
27. Ballew JT, Murray JA, Collin P, Maki M, Kagnoff MF, Kaukinen K, et al.Antibody biomarker discovery through in vitro directed evolution ofconsensus recognition epitopes. Proc Natl Acad Sci USA 2013;10:1–6.
28. Pu KF, Yuan LH, Chen LS,Wang AX, Zhou X, ZhangHL, et al. Identificationof VEGFR2-binding peptides using high throughput bacterial displaymethods and functional assessment. Current Cancer Drug Targets 2015;15:158–70.
29. Getz JA, Schoep TD, Daugherty PS. Peptide discovery using bacterialdisplay and flow cytometry. Methods Enzymol 2012;503:75–97.
30. Kaemmer D, Bozkurt A, Otto J, Junge K, Klink C, Weis J, et al. Evaluation oftissue components in the peripheral nervous system using Sirius redstaining and immunohistochemistry: a comparative study (human, pig,rat). J Neurosci Methods 2010;190:112–6.
31. Wu ST, Zhang Y. LOMETS: a local meta-threading-server for proteinstructure prediction. Nucleic Acids Res 2007;35:3375–82.
32. Pierce BG,Wiehe K, HwangH, KimBH, Vreven T,Weng ZP. ZDOCK server:interactive docking prediction of protein-protein complexes and symmet-ric multimers. Bioinformatics 2014;30:1771–3.
Effect of PD-L1–Targeting Peptide on Cancer Immunotherapy
www.aacrjournals.org Cancer Immunol Res; 6(2) February 2018 187
on May 19, 2020. © 2018 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst December 7, 2017; DOI: 10.1158/2326-6066.CIR-17-0035

33. Freeman GJ, Long AJ, Iwai Y, Bourque K, Chernova T, Nishimura H, et al.Engagement of the PD-1 immunoinhibitory receptor by a novel B7 familymember leads to negative regulation of lymphocyte activation. J Exp Med2000;192:1027–34.
34. Butte MJ, Keir ME, Phamduy TB, Sharpe AH, Freeman GJ. Programmeddeath-1 ligand 1 interacts specificallywith the B7-1 costimulatorymoleculeto inhibit T cell responses. Immunity 2007;27:111–22.
35. Lee HT, Lee JY, Lim H, Lee SH, Moon YJ, Pyo HJ, et al. Molecularmechanism of PD-1/PD-L1 blockade via anti-PD-L1 antibodies atezolizu-mab and durvalumab. Sci Rep 2017;7:1–12.
36. LinDYW, TanakaY, IwasakiM,Gittis AG, SuHP,Mikami B, et al. The PD-1/PD-L1 complex resembles the antigen-binding Fv domains of antibodiesand T cell receptors. Proc Natl Acad Sci USA 2008;105:3011–6.
37. Schroder K, Hertzog PJ, Ravasi T, Hume DA. Interferon-gamma: an over-view of signals, mechanisms and functions. J Leukoc Biol 2004;75:163–89.
38. Abiko K, Matsumura N, Hamanishi J, Horikawa N, Murakami R, Yama-guchi K, et al. IFN-gamma from lymphocytes induces PD-L1 expressionandpromotes progressionof ovarian cancer. Br JCancer 2015;112:1501–9.
39. Wimberly H, Brown JR, Schalper K, Haack H, SilverMR, Nixon C, et al. PD-L1 expression correlates with tumor-infiltrating lymphocytes and responseto neoadjuvant chemotherapy in breast cancer. Cancer Immunol Res2015;3:326–32.
40. Nakanishi J, Wada Y, Matsumoto K, Azuma M, Kikuchi K, Ueda S. Over-expression of B7-H1 (PD-L1) significantly associates with tumor grade and
postoperative prognosis in human urothelial cancers. Cancer ImmunolImmunother 2007;56:1173–82.
41. Duraiswamy J, Kaluza KM, Freeman GJ, Coukos G. Dual blockade of PD-1and CTLA-4 combined with tumor vaccine effectively restores T-cell rejec-tion function in tumors. Cancer Res 2013;73:3591–603.
42. Deng LF, Liang H, Burnette B, Beckett M, Darga T, Weichselbaum RR, et al.Irradiation and anti-PD-L1 treatment synergistically promote antitumorimmunity in mice. J Clin Invest 2014;124:687–95.
43. Bolla M, Gonzalez D, Warde P, Dubois JB, Mirimanoff RO, Storme G,et al. Improved survival in patients with locally advanced prostatecancer treated with radiotherapy and goserelin. N Engl J Med 1997;337:295–300.
44. Liu XY, Qu HL, Cao WH, Wang Y, Ma ZL, Li FN, et al. Efficacy ofcombined therapy of goserelin and letrozole on very young womenwith advanced breast cancer as first-line endocrine therapy. Endocr J2013;60:819–28.
45. Drucker DJ, Nauck MA. The incretin system: glucagon-like peptide-1receptor agonists and dipeptidyl peptidase-4 inhibitors in type 2 diabetes.Lancet 2006;368:1696–705.
46. Sato AK, Viswanathan M, Kent RB, Wood CR. Therapeutic peptides:technological advances driving peptides into development. Curr OpinBiotechnol 2006;17:638–42.
47. Werle M, Makhlof A, Takeuchi H. Carbopol-lectin conjugate coated lipo-somes for oral peptide delivery. Chem Pharm Bull 2010;58:432–4.
Cancer Immunol Res; 6(2) February 2018 Cancer Immunology Research188
Li et al.
on May 19, 2020. © 2018 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst December 7, 2017; DOI: 10.1158/2326-6066.CIR-17-0035

2018;6:178-188. Published OnlineFirst December 7, 2017.Cancer Immunol Res Chunlin Li, Nengpan Zhang, Jundong Zhou, et al. ImmunotherapyPeptide Blocking of PD-1/PD-L1 Interaction for Cancer
Updated version
10.1158/2326-6066.CIR-17-0035doi:
Access the most recent version of this article at:
Material
Supplementary
http://cancerimmunolres.aacrjournals.org/content/suppl/2017/12/07/2326-6066.CIR-17-0035.DC1
Access the most recent supplemental material at:
Cited articles
http://cancerimmunolres.aacrjournals.org/content/6/2/178.full#ref-list-1
This article cites 46 articles, 9 of which you can access for free at:
Citing articles
http://cancerimmunolres.aacrjournals.org/content/6/2/178.full#related-urls
This article has been cited by 1 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerimmunolres.aacrjournals.org/content/6/2/178To request permission to re-use all or part of this article, use this link
on May 19, 2020. © 2018 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst December 7, 2017; DOI: 10.1158/2326-6066.CIR-17-0035