Pepper Ischaemic mitral regurgitation V2 - Struttura … · Ischaemic mitral regurgitation...
87
Ischaemic mitral regurgitation aetiology and size of the problem John Pepper ERICE MONDAY 13 TH May 2013
Transcript of Pepper Ischaemic mitral regurgitation V2 - Struttura … · Ischaemic mitral regurgitation...
Ischaemic mitral regurgitation aetiology and size of the problem
John Pepper
ERICE
MONDAY 13TH May 2013
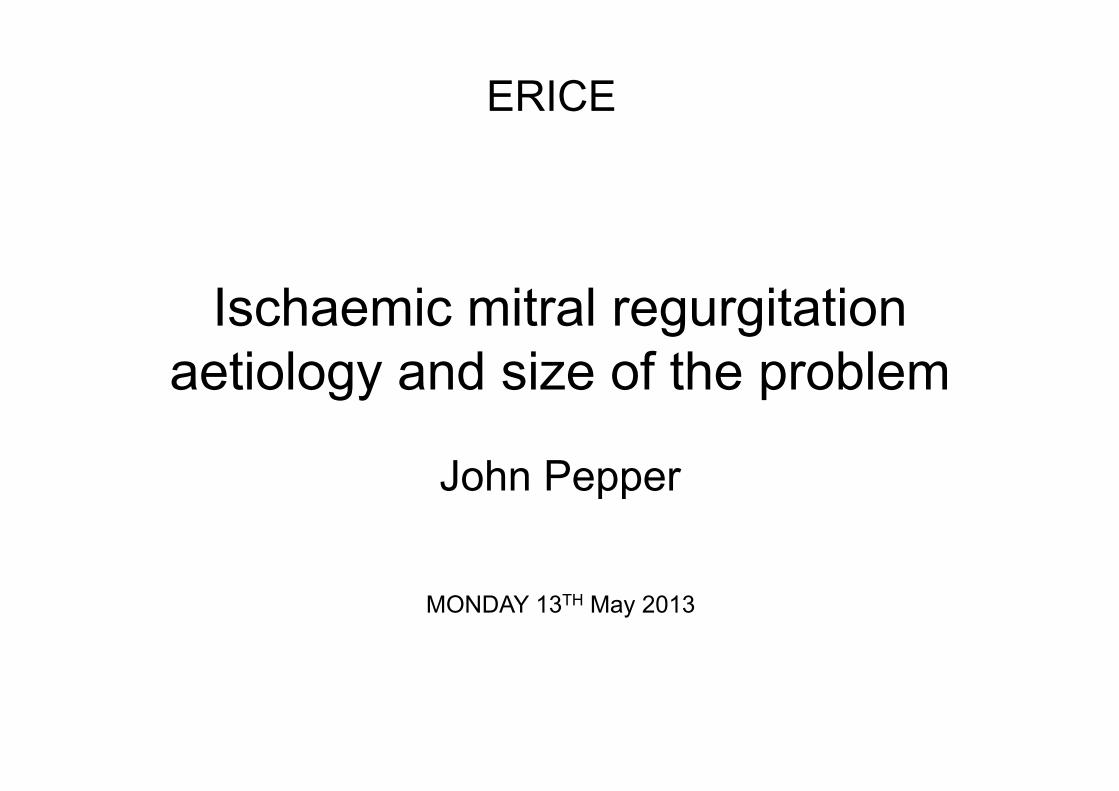
Functional Ischaemic MR Pathophysiology
Functional Ischaemic MR
• Prevalence: 20% of patients after MI. • 200,000 MI/year in the U.K. • 40,000 new cases a year in the U.K. • 2x risk of severe heart failure within 3
years. • 2x risk of death within 3 years.
Functional Ischaemic MR Unresolved questions
• Does correcting moderate FIMR improve outcome?
Ø Cardiac function
Ø Cardiac reverse remodelling
Ø Functional capacity
Ø Quality of life
Ø Survival
Mitral Valve Annuloplasty plus CABG versus CABG alone
in moderate Func9onal Ischemic Mitral Regurgita9on: final results of the Randomized
Ischemic Mitral Evalua9on (RIME) Trial K. M. John Chan,1,2 Prakash P. Punjabi,1,3 Marcus D. Flather,2,4
Riccardo Wage,2 Karen Symmonds,2 Isabelle Roussin,2 Shelley Rahman-Haley,2 Dudley J. Pennell,1,2 Philip J. Kilner,1,2 Gilles D. Dreyfus,1,2,5
John R. Pepper,1,2 on behalf of the RIME Investigators
National Heart & Lung Institute, Imperial College London1, London, U.K.; Royal Brompton & Harefield NHS Foundation Trust2, London, U.K.; Imperial
College Healthcare NHS Trust3, London, U.K.; Norwich Medical School, University of East Anglia4, Norwich, U.K.; Cardiothoracic Centre of Monaco5,
Monte Carlo, Monaco.
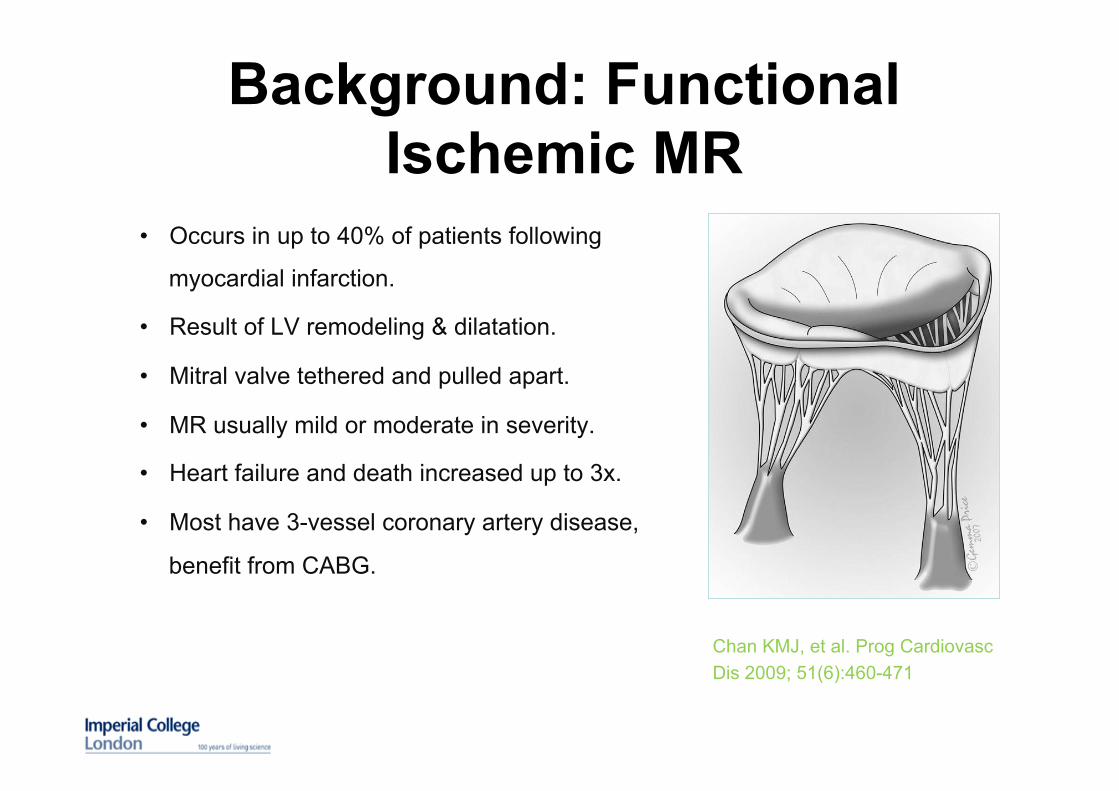
Background: Functional Ischemic MR
• Occurs in up to 40% of patients following
myocardial infarction.
• Result of LV remodeling & dilatation.
• Mitral valve tethered and pulled apart.
• MR usually mild or moderate in severity.
• Heart failure and death increased up to 3x.
• Most have 3-vessel coronary artery disease,
benefit from CABG.
Chan KMJ, et al. Prog Cardiovasc Dis 2009; 51(6):460-471
• Persistent increased risk of heart failure and death (up to 1.5x)
with coronary artery revascularization alone.
• Efficacy of adding mitral valve repair to CABG uncertain: reduction
in MR severity reported in observational, non-randomized studies,
but no improvement in functional capacity, heart failure or survival.
• Significant recurrence rates of MR reported in studies due to
suboptimal surgical techniques (use of flexible annuloplasty
bands, inadequate downsizing, incomplete coronary
revascularization).
Background: Functional Ischemic MR
• Single blinded randomized controlled trial: 7
centers.
• Randomization into two groups (1:1 ratio):
• Group 1: CABG only § Complete coronary artery revascularization. § Pedicled left internal mammary artery grafted
to the LAD.
• Group 2: CABG + Mitral Valve Repair § Complete rigid or semi-rigid mitral
annuloplasty ring used. § Carpentier-McCarthy-Adams IMR ETlogix ring
recommended. § Sized by measurement of anterior mitral valve
leaflet. § Downsized by 2 sizes if alternative complete
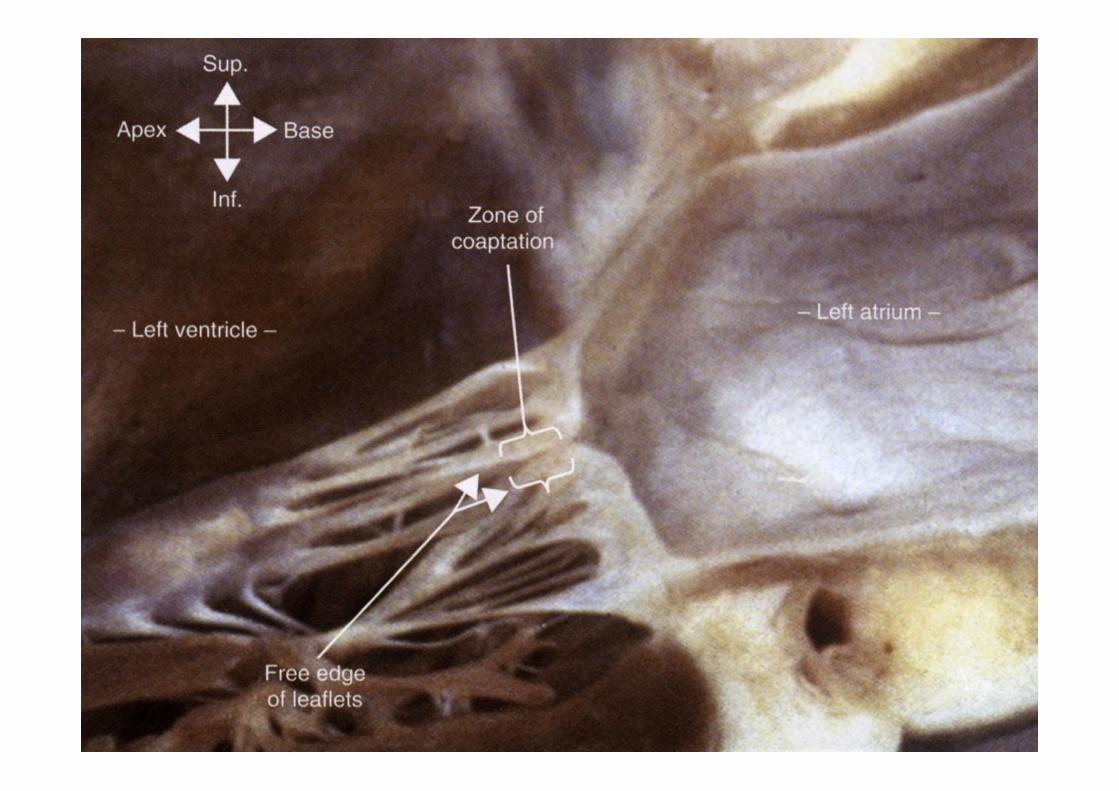
ring used. § Aim: coaptation length of at least 8 mm
between the anterior and posterior mitral valve leaflets with no more than trace MR.
Methods: Study design
• Inclusion criteria § Patients referred for elective CABG. § Moderate functional ischemic MR as defined by the
AHA/ACC/ASE criteria measured at rest or peak exercise by echocardiography:
§ Effective Regurgitant Orifice Area (EROA) 0.20–0.39 cm2
§ Regurgitant Volume 30-59 ml/beat
o Regurgitant Fraction 30-49%
o Vena Contracta Width 0.3-0.69 cm
Methods: Eligibility
Main Exclusion criteria § Severe LV dysfunction: EF < 30%.
§ Structural abnormalities of the mitral valve (including papillary
muscle rupture).
§ Significant aortic valve disease.
§ Previous or active endocarditis.
§ Significant co-morbidities: severe renal, liver or respiratory
impairment.
§ NYHA class IV, unstable angina, acute pulmonary edema,
cardiogenic shock.
§ Previous cardiac surgery.
• Primary hypothesis
§ Adding mitral valve annuloplasty to CABG in patients with
moderate functional ischemic MR improves functional capacity.
• Secondary hypothesis
§ Adding mitral valve annuloplasty to CABG in patients with
moderate functional ischemic MR improves LV reverse
remodelling, MR severity, and BNP levels.
Methods: Hypothesis
Methods: Endpoints
• Primary endpoint (one year):
§ Functional capacity (Peak oxygen consumption)
• Secondary endpoints (one year):
§ LV reverse remodeling (LVESVI)
§ Mitral regurgitation (MR volume)
§ BNP levels.
Methods: Statistics • Power calculations
§ Using 90% power, α = 0.05, and S.D. = 3.5, 82 patients required
to detect difference of ≥ 2.5 ml/kg/min in primary endpoint, peak
VO2.
§ Two planned interim analysis performed.
§ Benefit demonstrated for CABG + MVR group, (P=0.008 for
primary endpoint).
§ Recruitment stopped after results of second interim analysis (73
patients randomised).
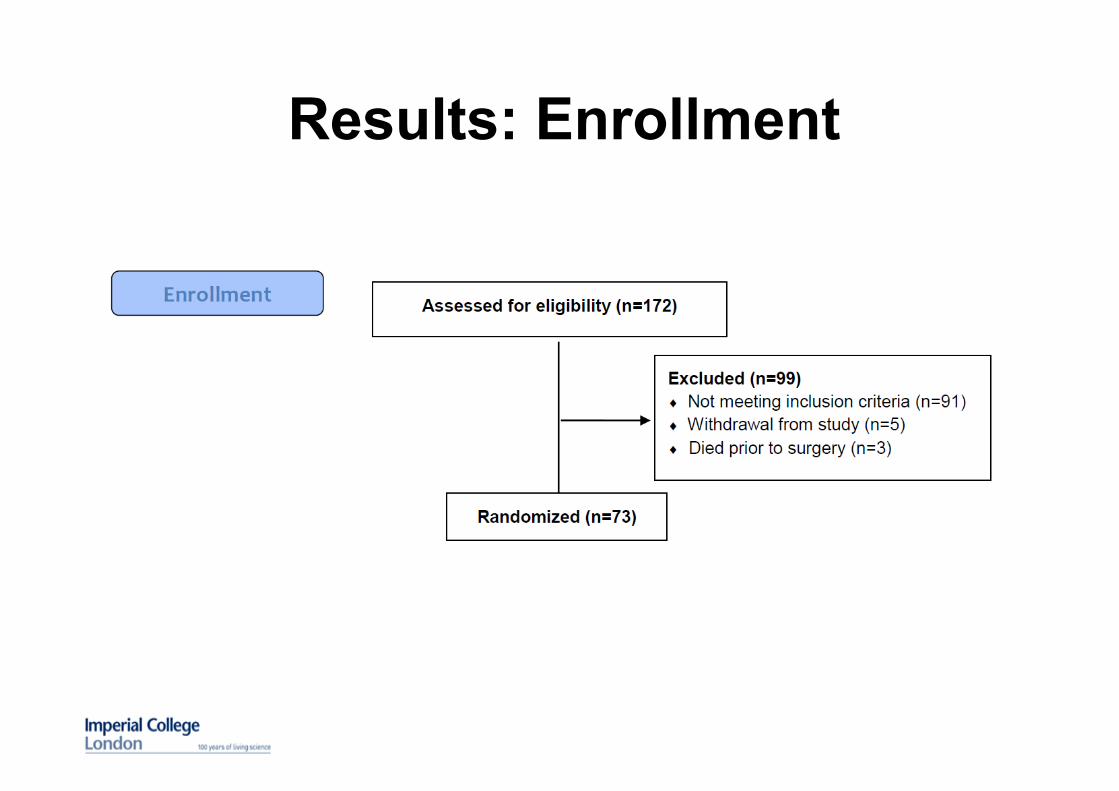
Results: Enrollment
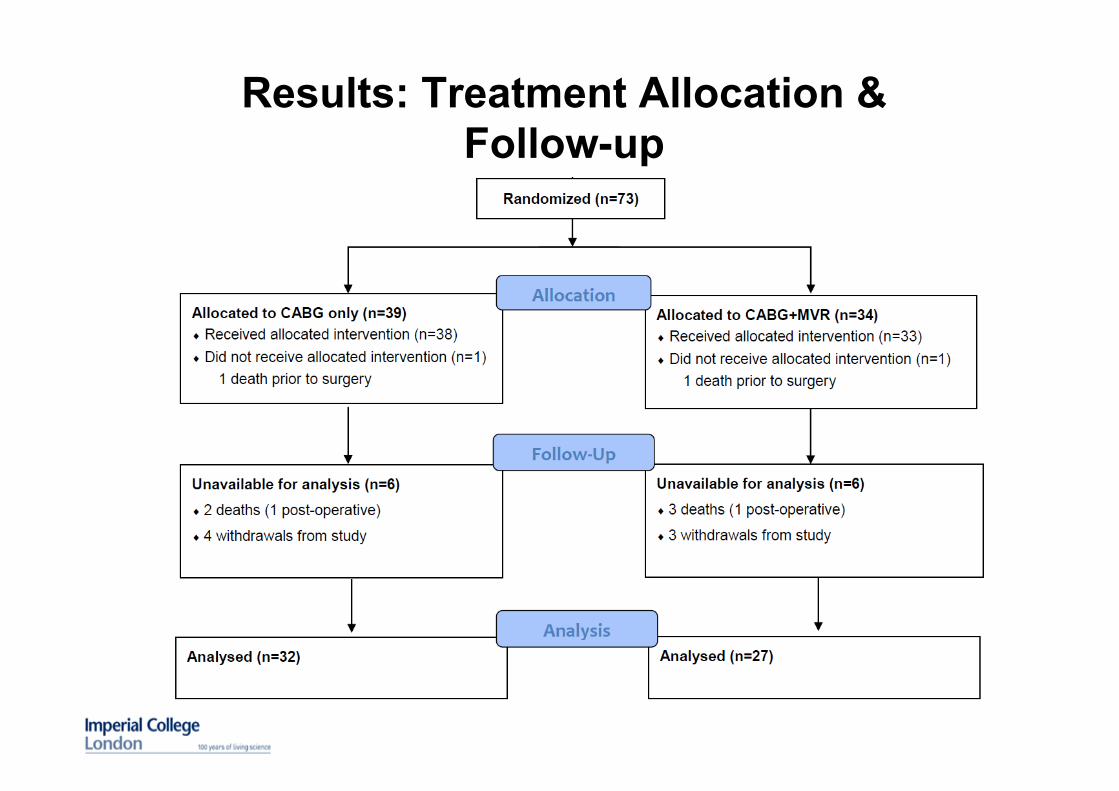
Results: Treatment Allocation & Follow-up
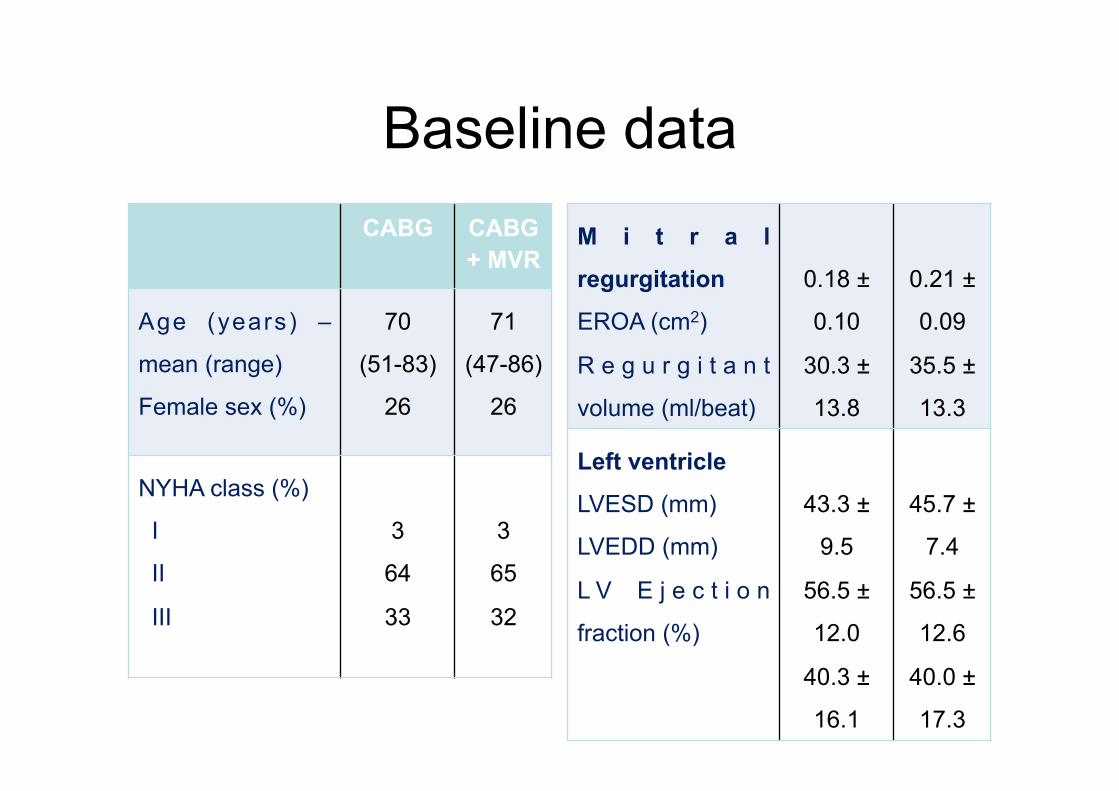
Baseline data M i t r a l
regurgitation
EROA (cm2)
R e g u r g i t a n t
volume (ml/beat)
0.18 ±
0.10
30.3 ±
13.8
0.21 ±
0.09
35.5 ±
13.3
Left ventricle
LVESD (mm)
LVEDD (mm)
L V E j e c t i o n
fraction (%)
43.3 ±
9.5
56.5 ±
12.0
40.3 ±
16.1
45.7 ±
7.4
56.5 ±
12.6
40.0 ±
17.3
CABG CABG + MVR
Age (years) –
mean (range)
Female sex (%)
70
(51-83)
26
71
(47-86)
26
NYHA class (%)
I
II
III
3
64
33
3
65
32
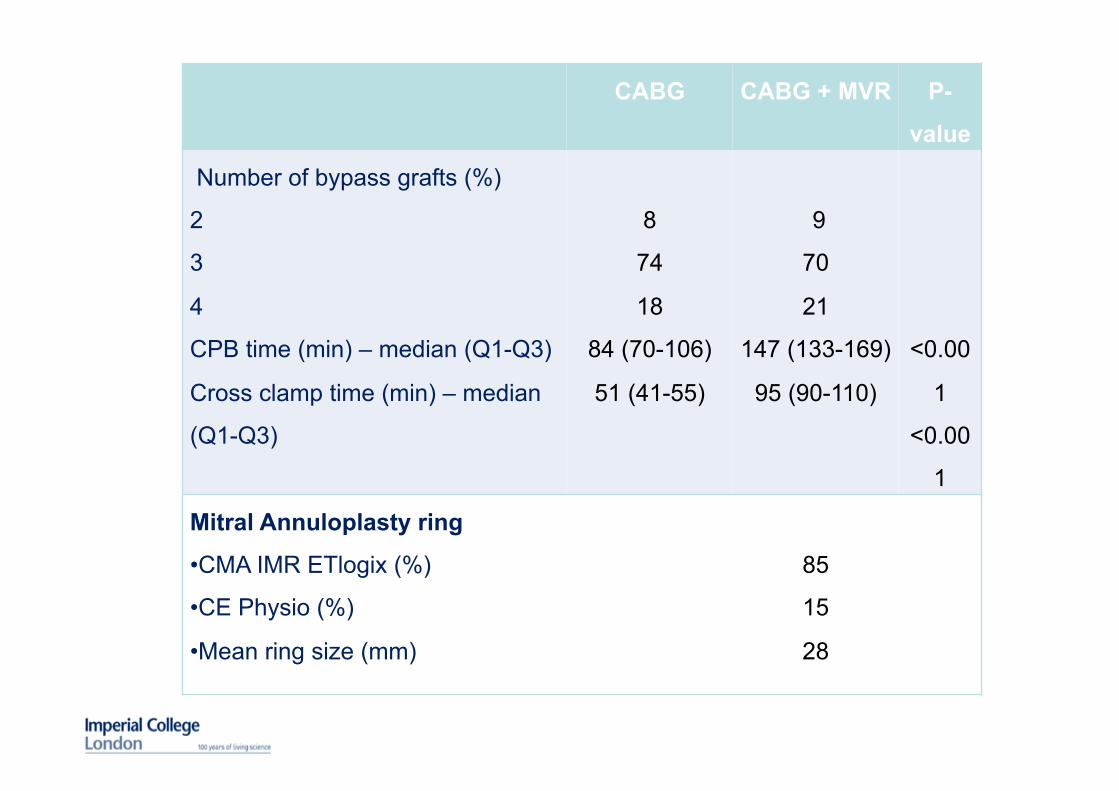
CABG CABG + MVR P-
value
Number of bypass grafts (%)
2
3
4
CPB time (min) – median (Q1-Q3)
Cross clamp time (min) – median
(Q1-Q3)
8
74
18
84 (70-106)
51 (41-55)
9
70
21
147 (133-169)
95 (90-110)
<0.00
1
<0.00
1
Mitral Annuloplasty ring
• CMA IMR ETlogix (%)
• CE Physio (%)
• Mean ring size (mm)
85
15
28
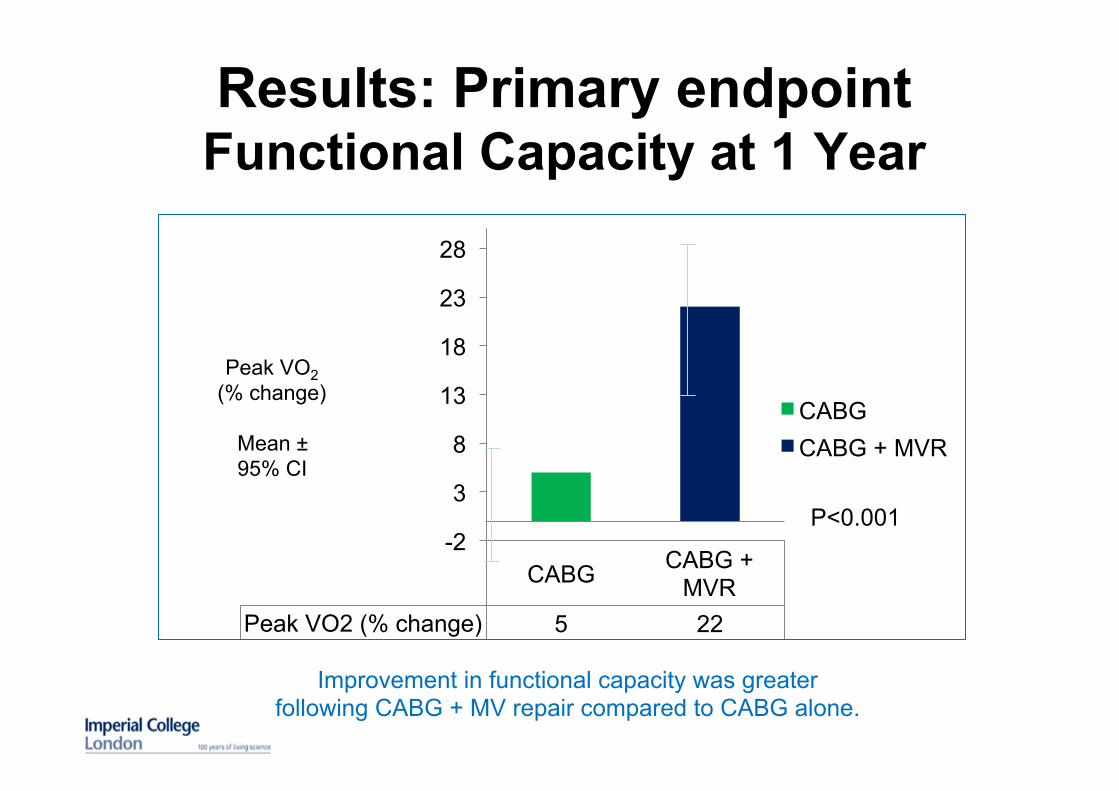
Results: Primary endpoint Functional Capacity at 1 Year
Improvement in functional capacity was greater following CABG + MV repair compared to CABG alone.
CABG CABG + MVR
Peak VO2 (% change) 5 22
-2
3
8
13
18
23
28
CABG CABG + MVR
P<0.001
Peak VO2 (% change)
Mean ± 95% CI
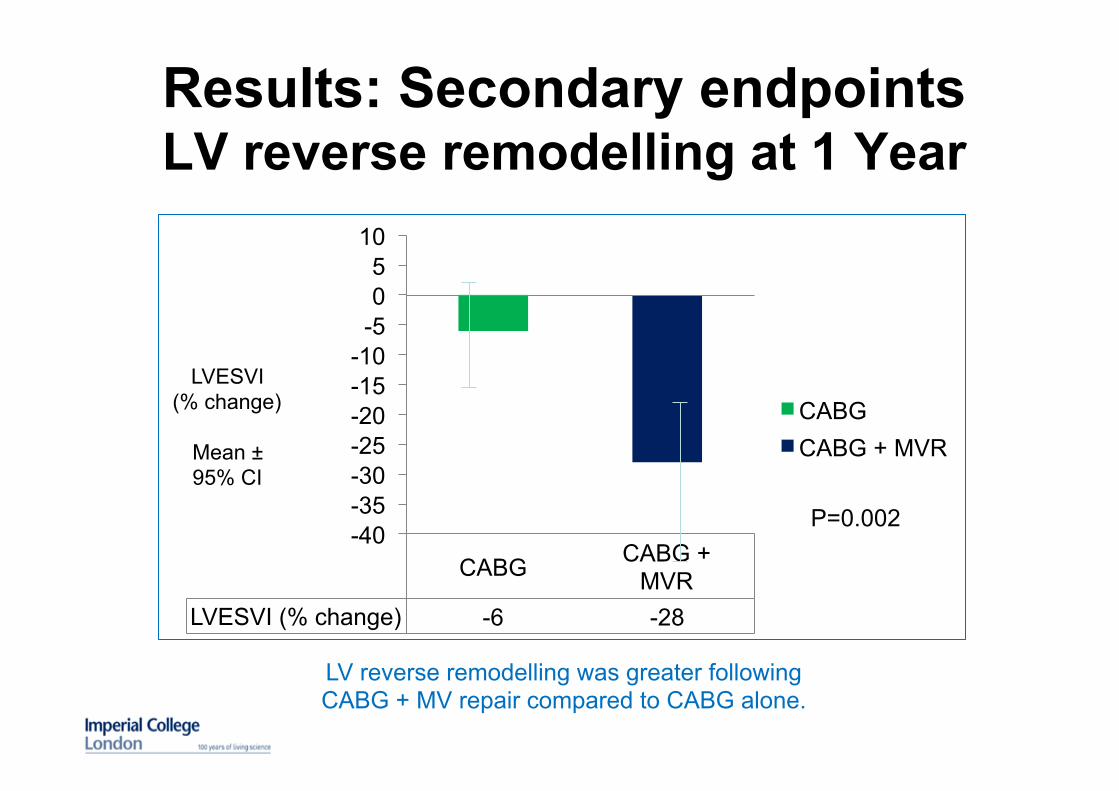
Results: Secondary endpoints LV reverse remodelling at 1 Year
LV reverse remodelling was greater following CABG + MV repair compared to CABG alone.
CABG CABG + MVR
LVESVI (% change) -6 -28
-40 -35 -30 -25 -20 -15 -10
-5 0 5
10
CABG CABG + MVR
LVESVI (% change)
Mean ± 95% CI
P=0.002
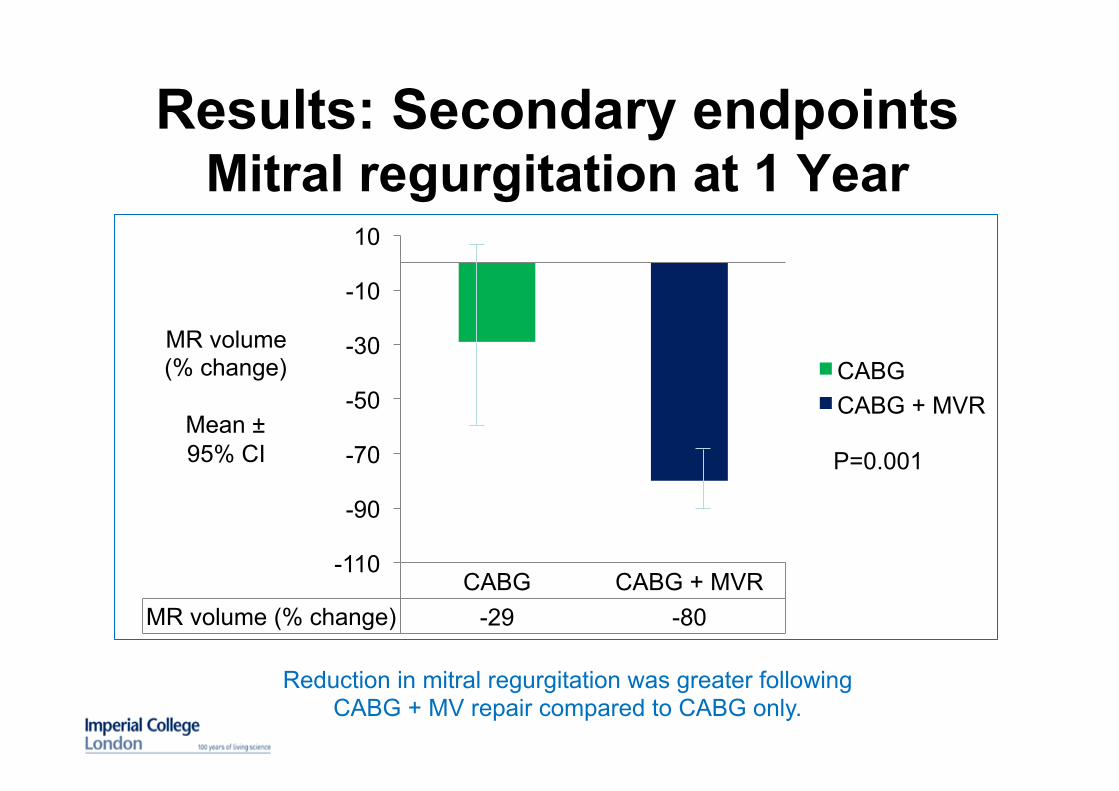
Results: Secondary endpoints Mitral regurgitation at 1 Year
Reduction in mitral regurgitation was greater following CABG + MV repair compared to CABG only.
CABG CABG + MVR MR volume (% change) -29 -80
-110
-90
-70
-50
-30
-10
10
CABG CABG + MVR
MR volume (% change)
Mean ± 95% CI
P=0.001
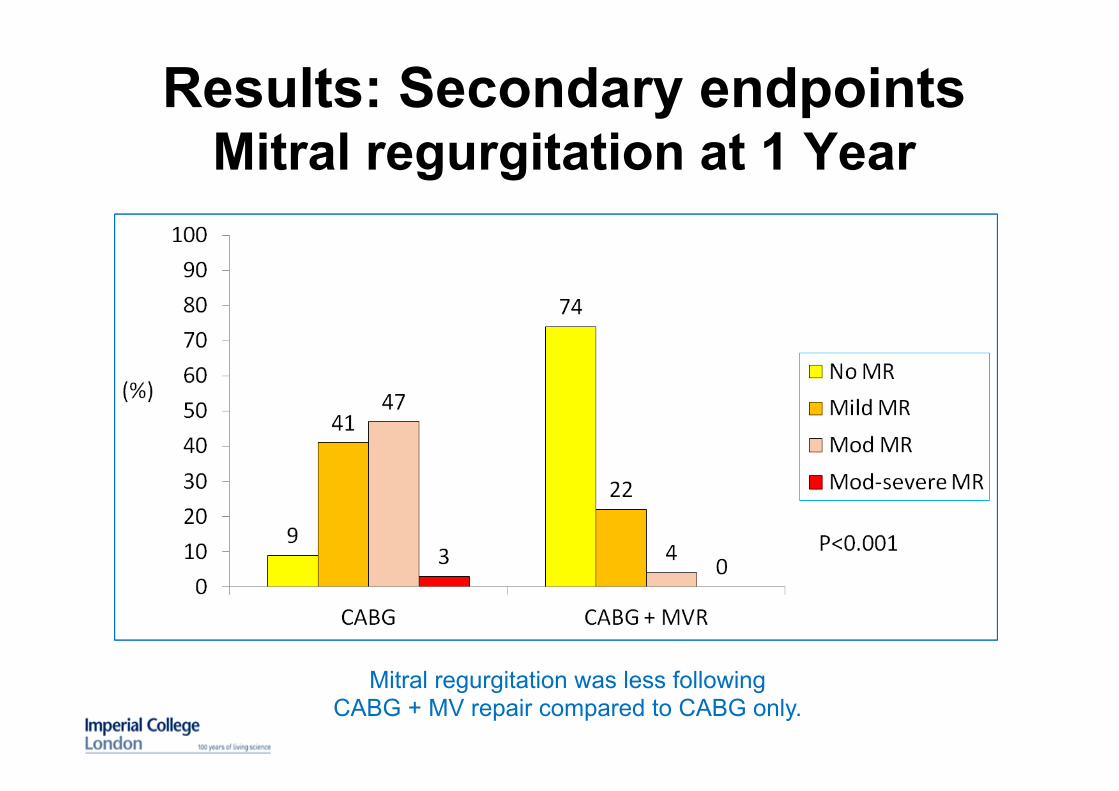
Results: Secondary endpoints Mitral regurgitation at 1 Year
Mitral regurgitation was less following CABG + MV repair compared to CABG only.
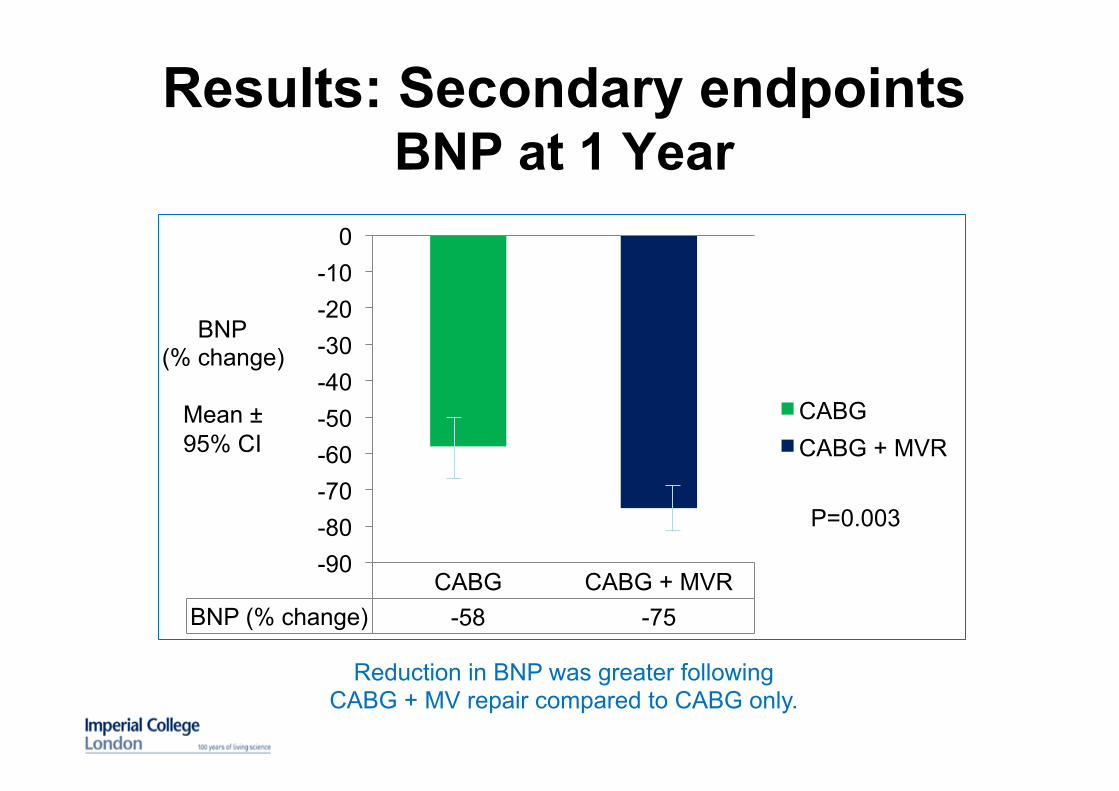
Results: Secondary endpoints BNP at 1 Year
Reduction in BNP was greater following CABG + MV repair compared to CABG only.
CABG CABG + MVR BNP (% change) -58 -75
-90 -80 -70 -60 -50 -40 -30 -20 -10
0
CABG CABG + MVR
BNP (% change)
Mean ± 95% CI
P=0.003
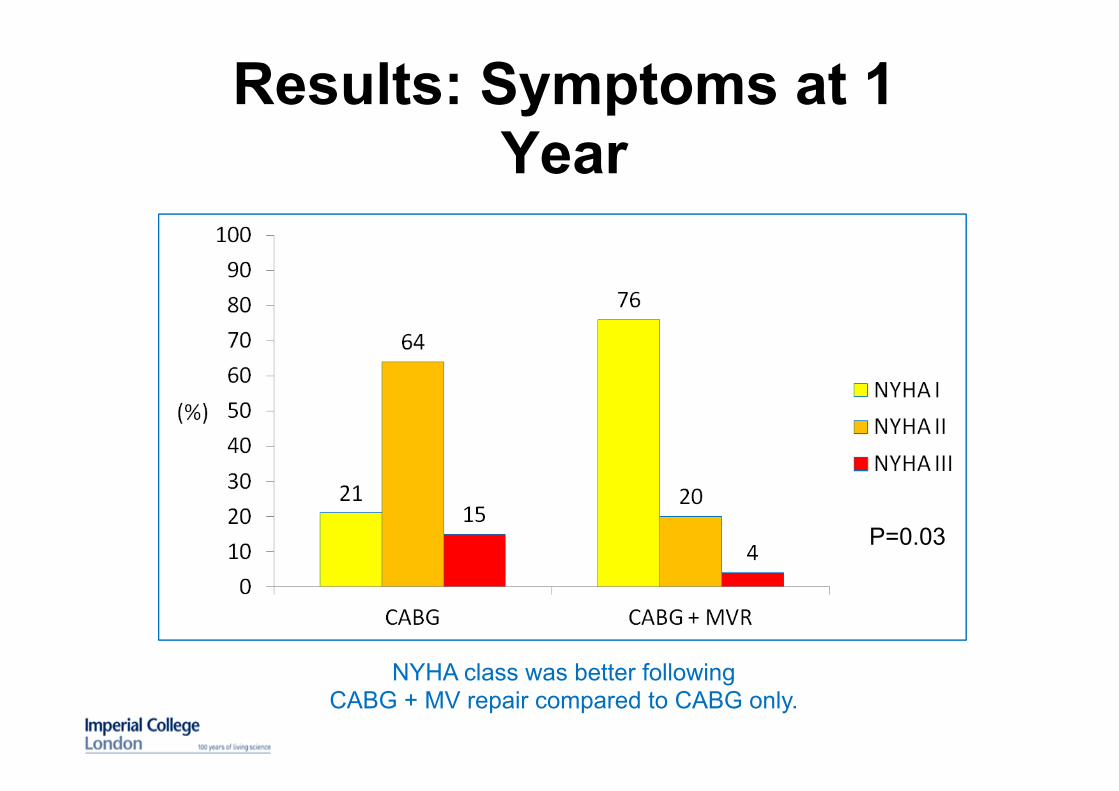
Results: Symptoms at 1 Year
NYHA class was better following CABG + MV repair compared to CABG only.
P=0.03
Limitations
• Study stopped early for benefit after review of
interim results.
• Single (not double) blinded study.
• Endpoints determined at one year; longer follow-
up necessary.
• Study not designed and not powered to evaluate
clinical events and survival.
Conclusions • Compared to CABG alone, addition of MV annuloplasty to CABG in patients with moderate functional ischemic MR improves:
§ Functional capacity and symptoms § LV reverse remodelling § Mitral regurgitation § BNP levels
• The impact of these benefits on longer term clinical outcomes remain to be defined.
• CABG plus MV annuloplasty required longer operation times, increased intubation and hospital stay duration, and blood transfusion.
• Concomitant CABG plus MV annuloplasty should be considered in patients with moderate functional ischemic MR.
Acknowledgement Funders: U.K. Department of Health, Na4onal Ins4tute of Health Research (NIHR), Bri4sh Heart Founda4on, Bri4sh Medical Associa4on, NIHR Biomedical Research Unit of the Royal Brompton & Harefield NHS Founda4on Trust and Imperial College London. Sponsor: Imperial College London. Par9cipa9ng centres: Royal Brompton Hospital, Harefield Hospital, Hammersmith Hospital, Blackpool Victoria Hospital, Bristol Royal Infirmary, Glenfield Hospital Leicester, Heart Hospital, Medical University of Silesia Poland. Principal Inves9gators: John Pepper, Marcus Flather, K M John Chan, Prakash Punjabi, Gilles
Dreyfus, Mohammed Amrani, Augus4ne Tang, George Asimakopoulos, Tom Sypt, John Yap, Andrzej Bochenek.
Echo, CMR and Peak VO2 Core Labs: Isabelle Roussin, Shelley Rahman-‐Haley, Riccardo Wage,
Karen Symmonds, Philip Kilner, Dudley Pennell, David Firmin, Robert Bougard, Stephanie Bayne, Wayne Arthur.
Co-‐ordinators: Belinda Lees, Tollene Riley, Jemyrr Gavino, Sarah Isbell, Shu Fang Wang, CharloVe Waterhouse, Emma Brennan, Lukasz Krzych, Elaine Logtens, Pradeep Narayan.
RIME Trial Primary Hypothesis
Mitral annuloplasty in addition to CABG improves functional capacity compared to CABG alone, in patients with moderate functional ischaemic mitral regurgitation.
RIME Trial Secondary Hypothesis
1. In patients with moderate functional ischaemic mitral regurgitation, mitral annuloplasty in addition to CABG:
• Improves quality of life
• Improves cardiac function
RIME Trial Secondary Hypothesis
2. In patients with moderate functional ischaemic mitral regurgitation, the outcome of CABG alone can be predicted by:
• Stress echo and stress MRI
• Myocardial viability
• Completeness of revascularisation
RIME Trial
Open, prospective randomised controlled trial with blinded comparison of outcomes. 100 patients: 50 CABG alone.
50 CABG + mitral annuloplasty
RIME Trial Inclusion criteria
• Patients referred for CABG with significant RCA or Cx stenoses. • Moderate MR without leaflet prolapse (ERO 20-‐40 mm2)
RIME Trial Exclusion criteria
• Severe LV dysfunction (EF < 30%)
• Significant aortic valve disease
• Atrial fibrillation or non sinus rhythm
• Significant co-‐morbidities (creatinine > 160, INR > 2.0, bilirubin > 40, FEV1:FVC ratio < 0.6) • NYHA IV, unstable angina, acute LVF, cardiogenic shock
• Structural abnormalities of the mitral valve
• Associated conditions significantly increasing risk of surgery
RIME Trial Recruitment
SCREENING
Review angiogram and clinical notes of all patients referred for CABG
MR on clinical examination, previous echo or LV angiogram
Request echo
Moderate functional MR Meets inclusion & exclusion criteria. Discuss at MDT.
Patient invited to take part in study. Written informed consent obtained.
RIME Trial Recruitment
BASELINE INVESTIGATIONS Echo
Peak oxygen consumption test Post-exercise echo
EQ-5D questionnaire Serum BNP CMR scan
RANDOMISATION 50 patients: CABG only
50 patients: CABG + Mitral Annuloplasty
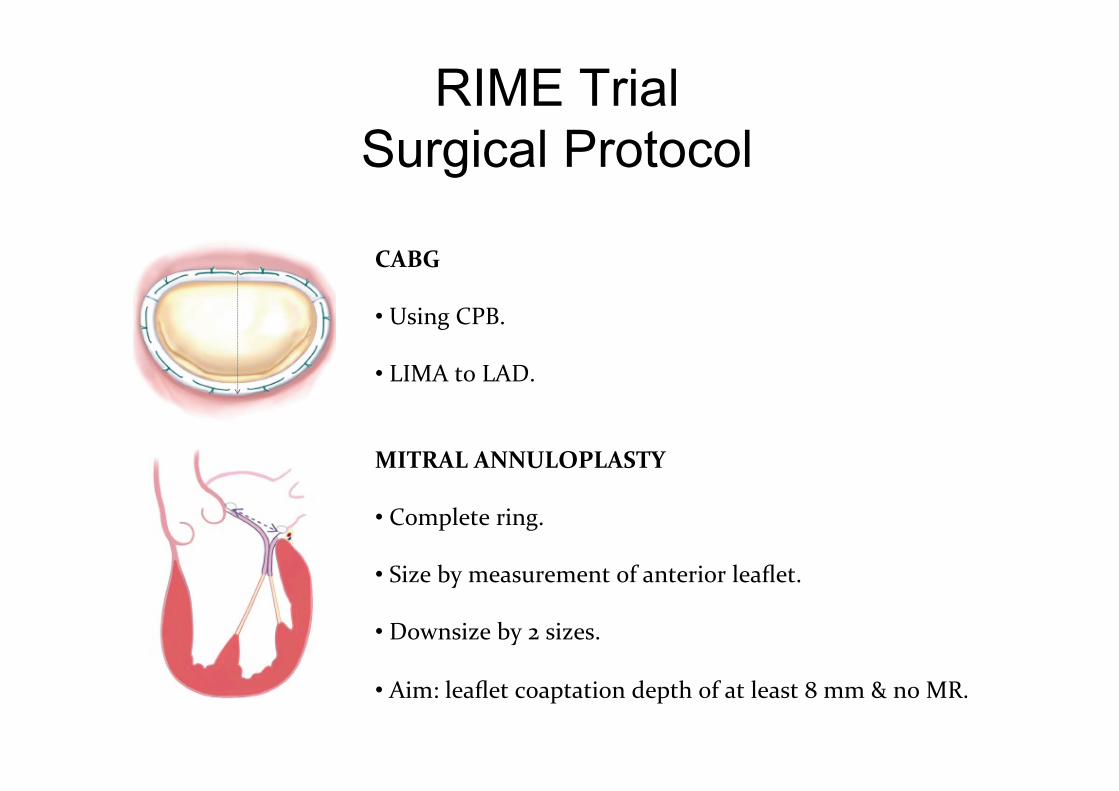
RIME Trial Surgical Protocol
CABG • Using CPB.
• LIMA to LAD.
MITRAL ANNULOPLASTY • Complete ring.
• Size by measurement of anterior leaflet.
• Downsize by 2 sizes.
• Aim: leaflet coaptation depth of at least 8 mm & no MR.
CONCLUSION
• Ischaemic MR is poorly understood • MRI may help • Molecular imaging may help to understand
the remodelling process • Decision making can be difficult.
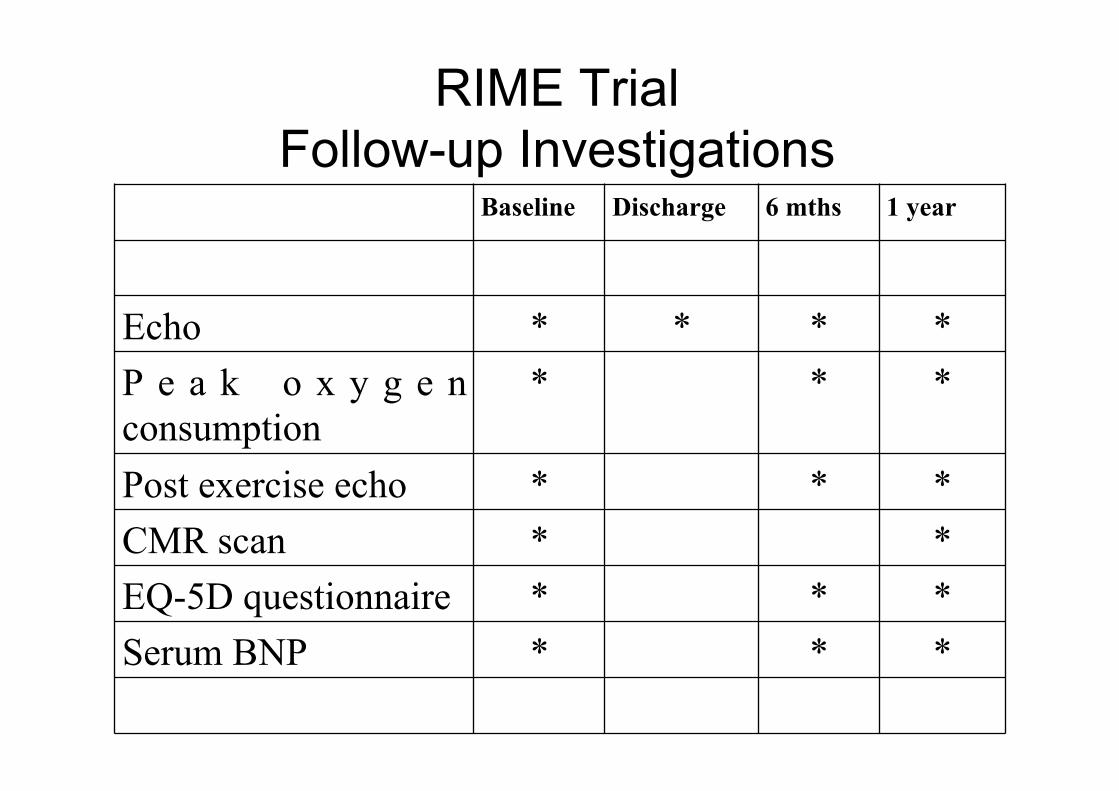
RIME Trial Follow-up Investigations
Baseline Discharge 6 mths 1 year
Echo * * * * P e a k o x y g e n consumption
* * *
Post exercise echo * * * CMR scan * * EQ-5D questionnaire * * * Serum BNP * * *
RIME Trial End points
Primary end point • Functional capacity at 1 year determined by peak oxygen consumption.
Secondary end points • Health-Related Quality of Life at 1 year determined by EQ-5D questionnaire. • Global and regional LV function at 1 year as determined by CMR. • MR grade at 1 year as determined by echo. • Serum BNP levels at 1 year.
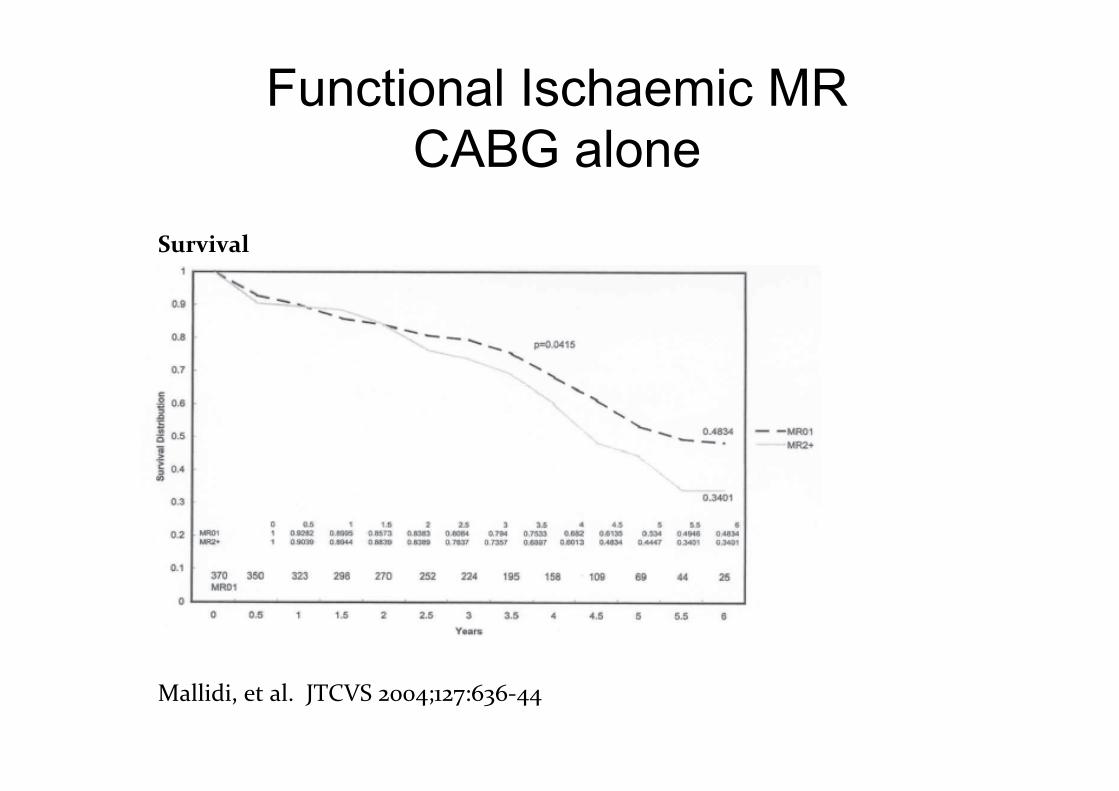
Functional Ischaemic MR CABG alone
Mallidi, et al. JTCVS 2004;127:636-‐44
Survival
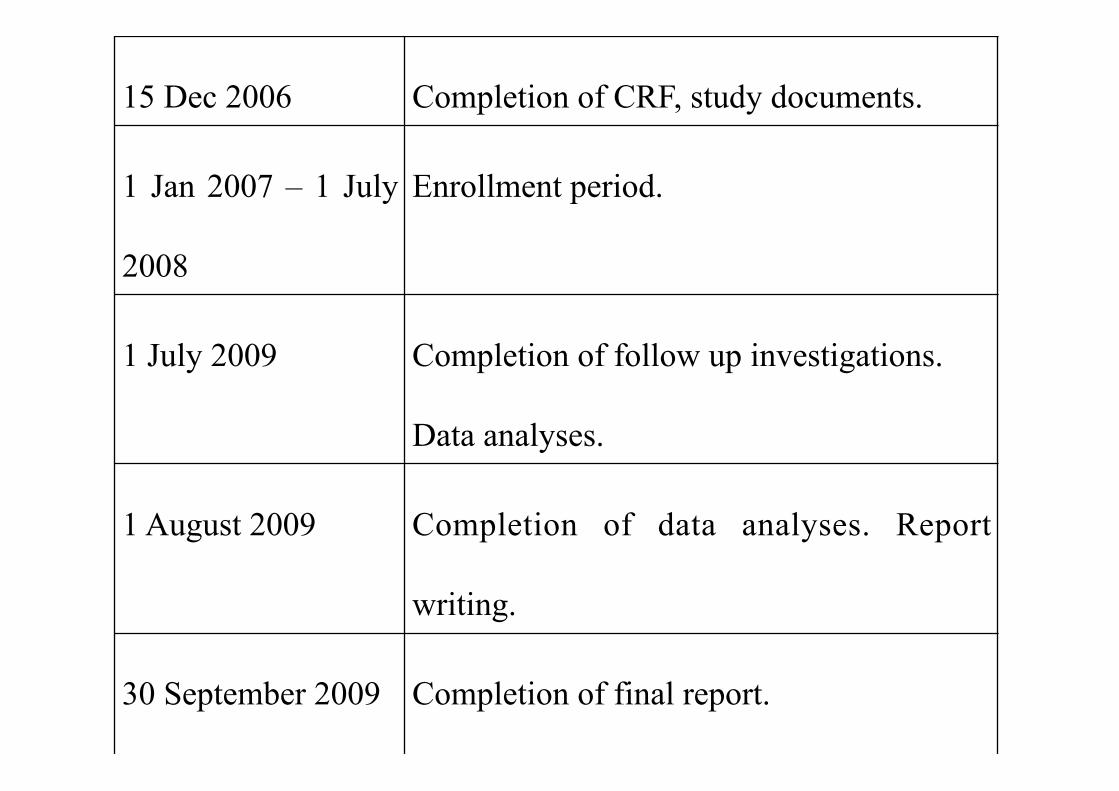
15 Dec 2006 Completion of CRF, study documents.
1 Jan 2007 – 1 July
2008
Enrollment period.
1 July 2009 Completion of follow up investigations.
Data analyses.
1 August 2009 Completion of data analyses. Report
writing.
30 September 2009 Completion of final report.
RIME Trial Investigators
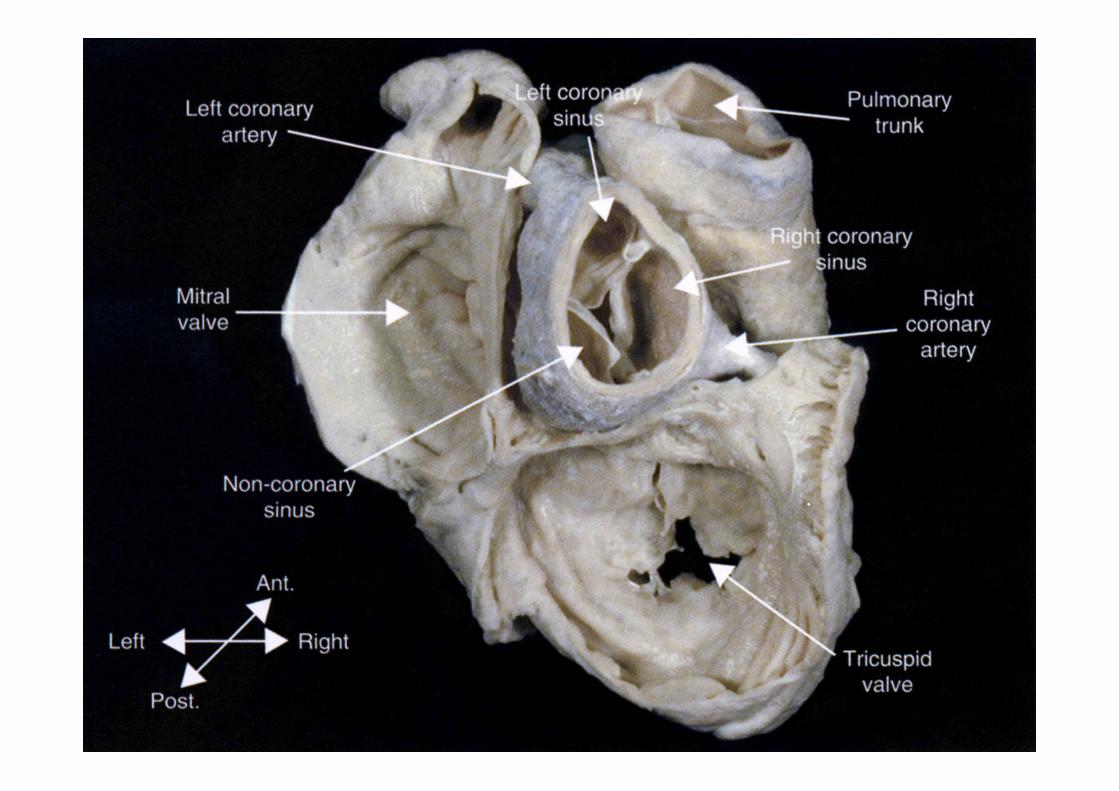
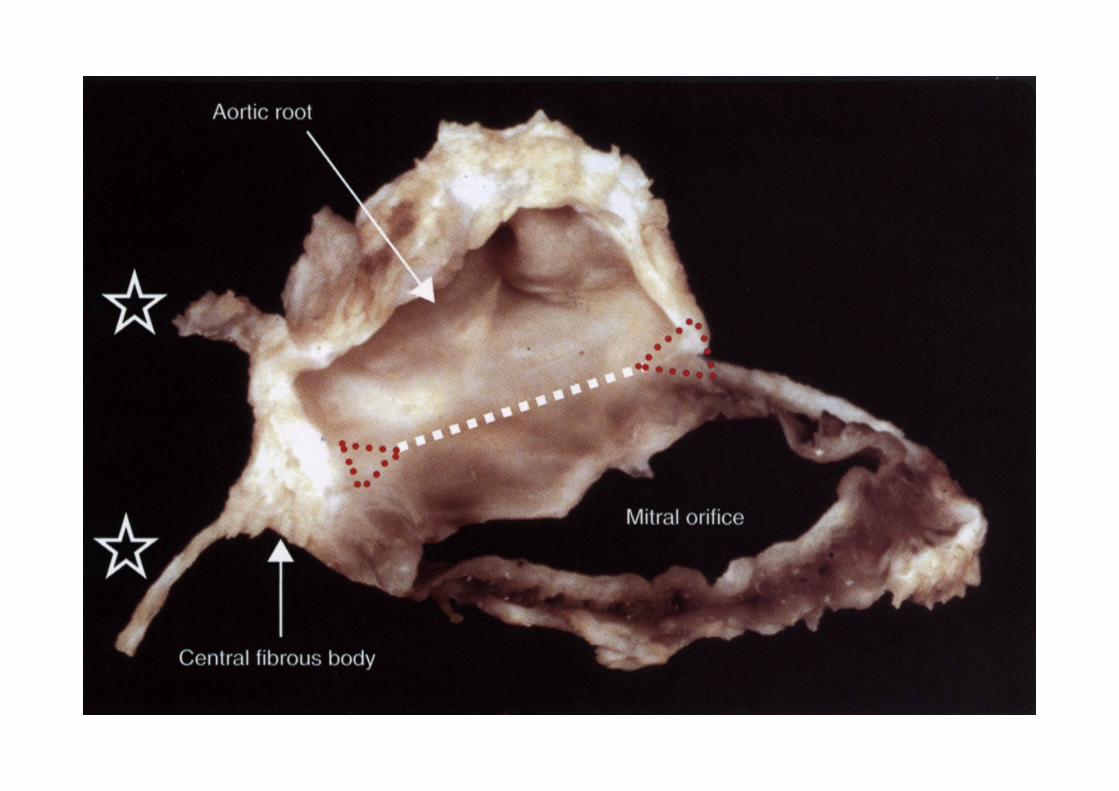
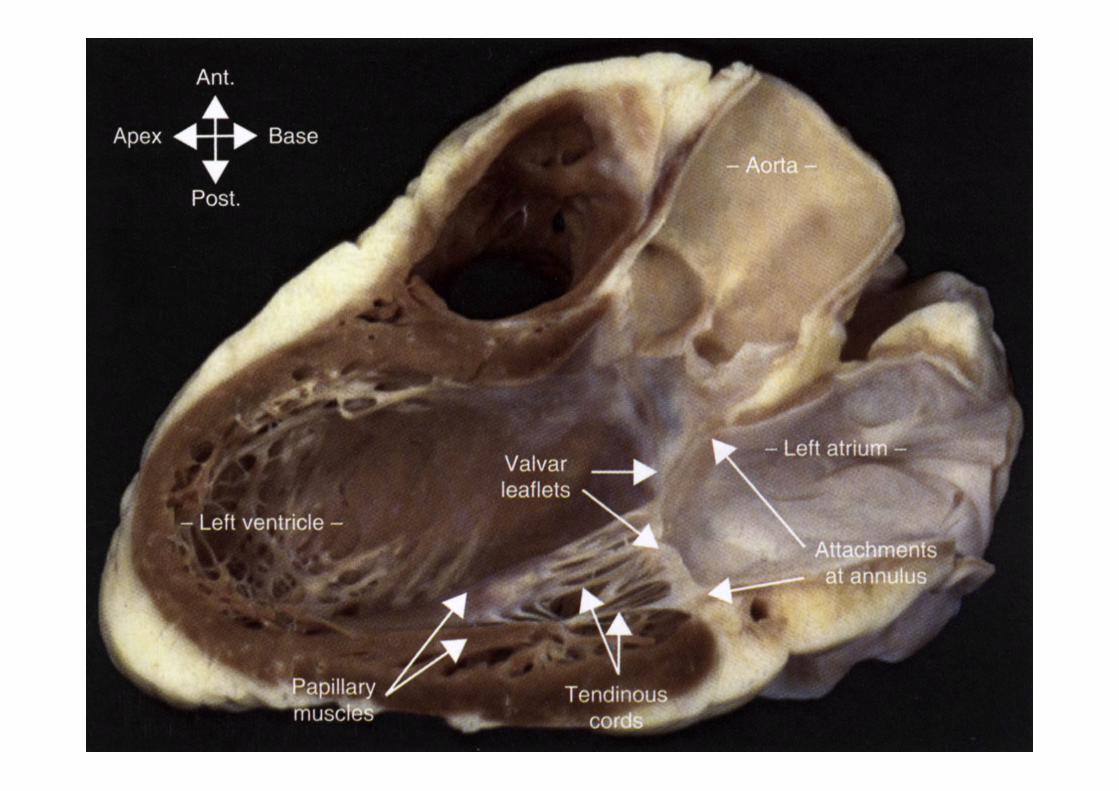
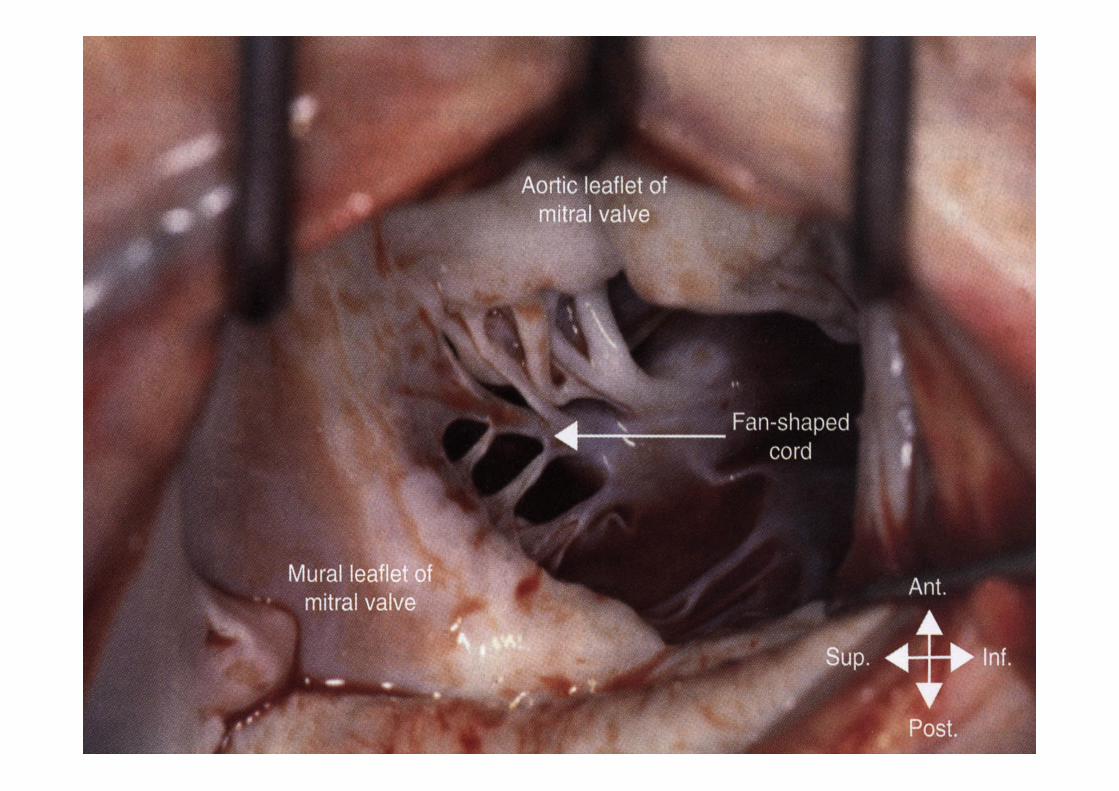
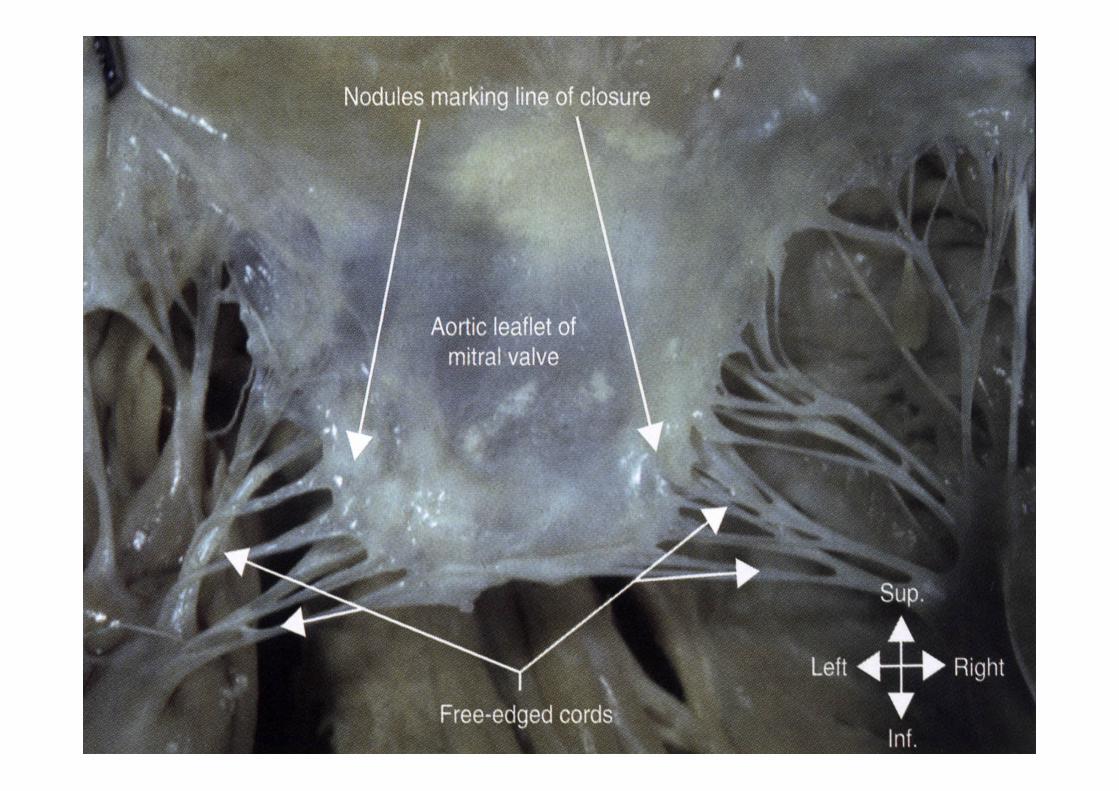
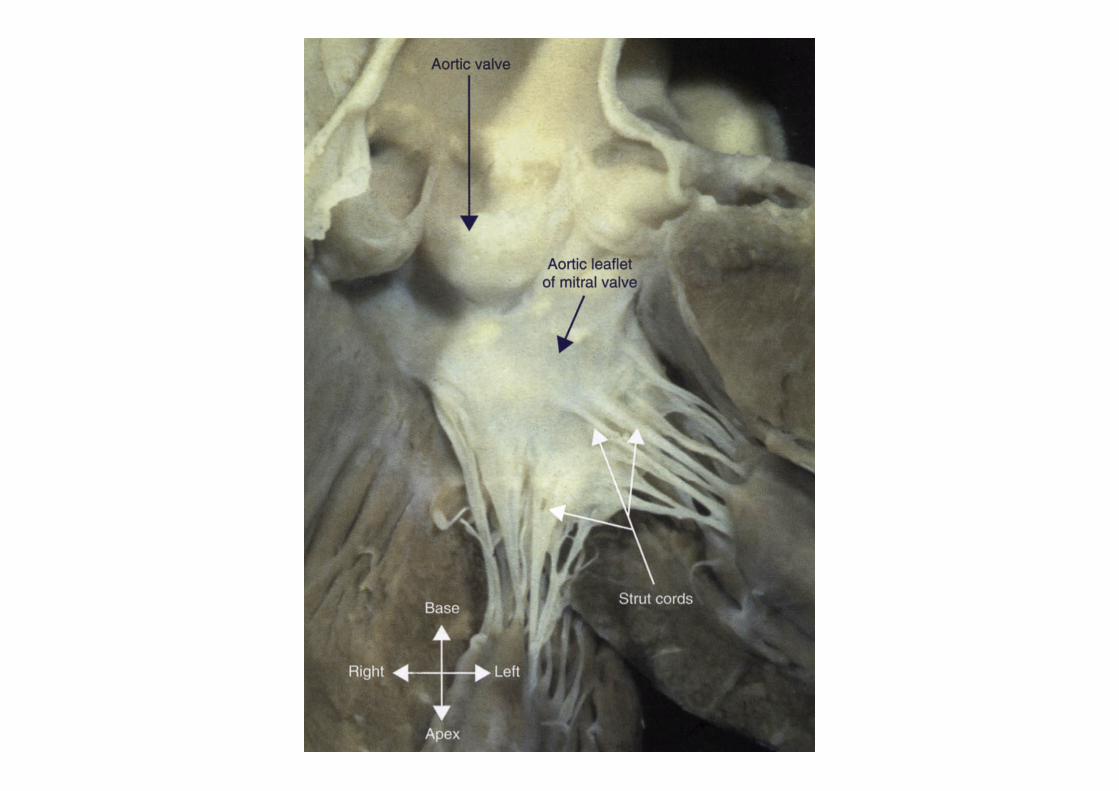
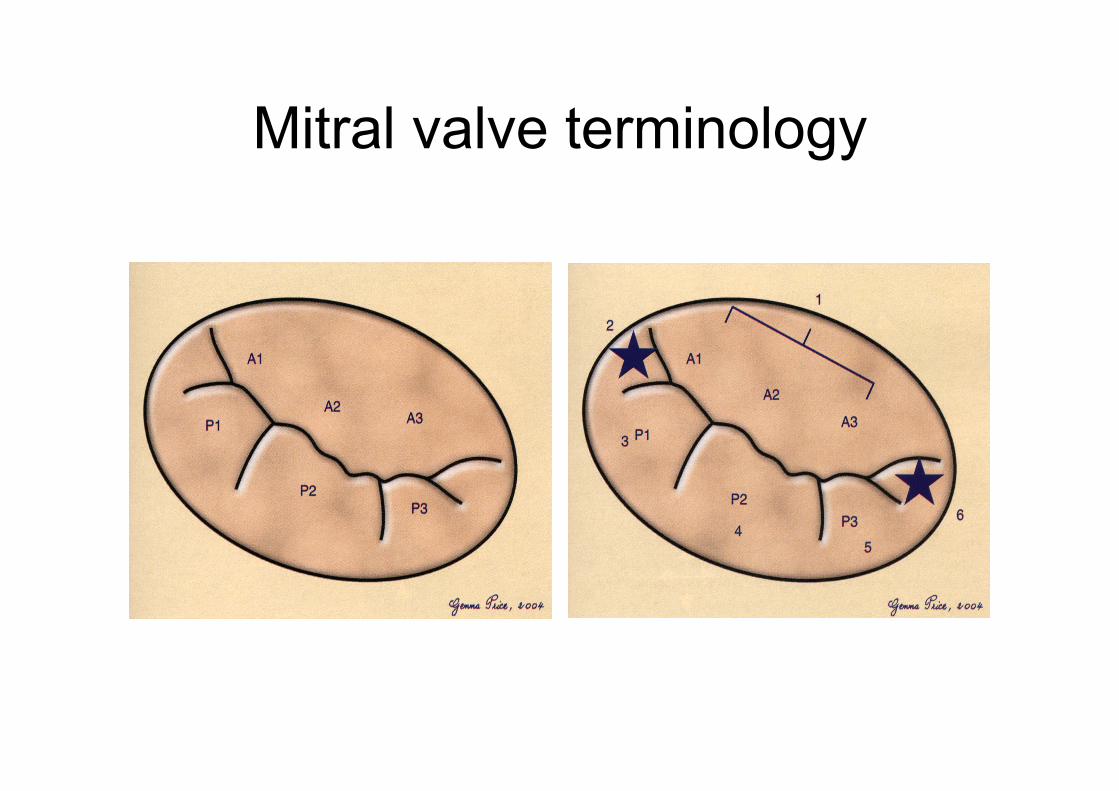
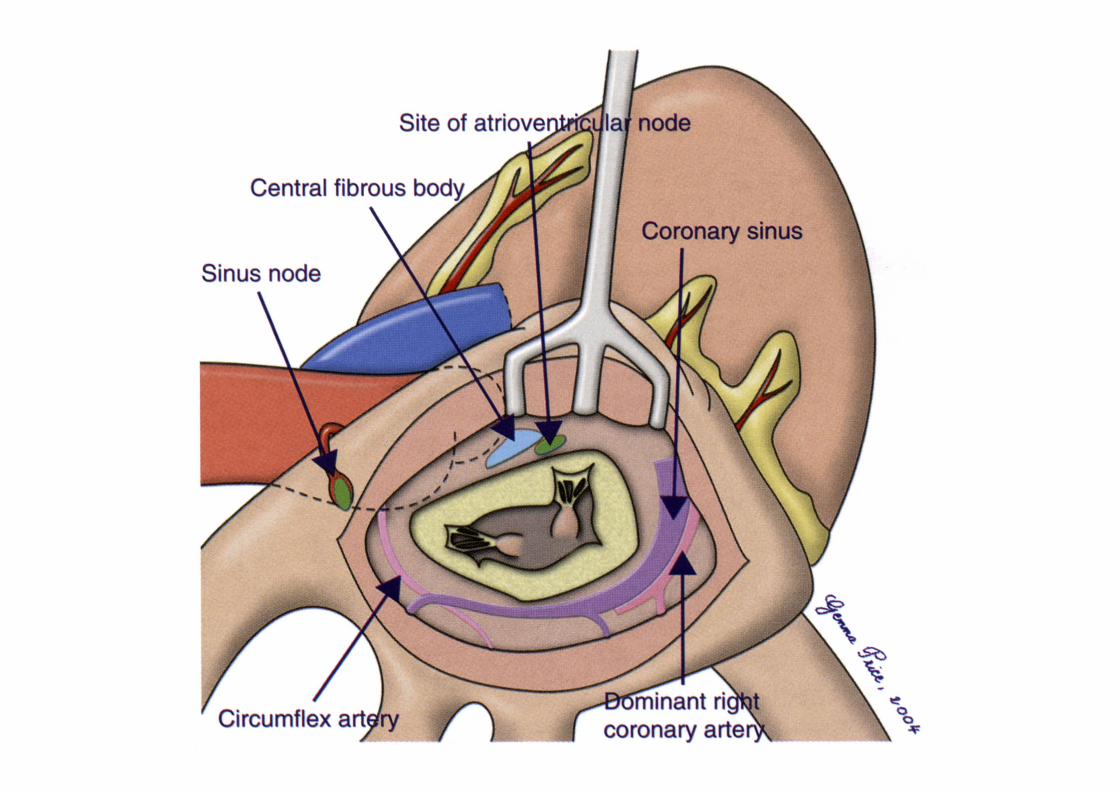
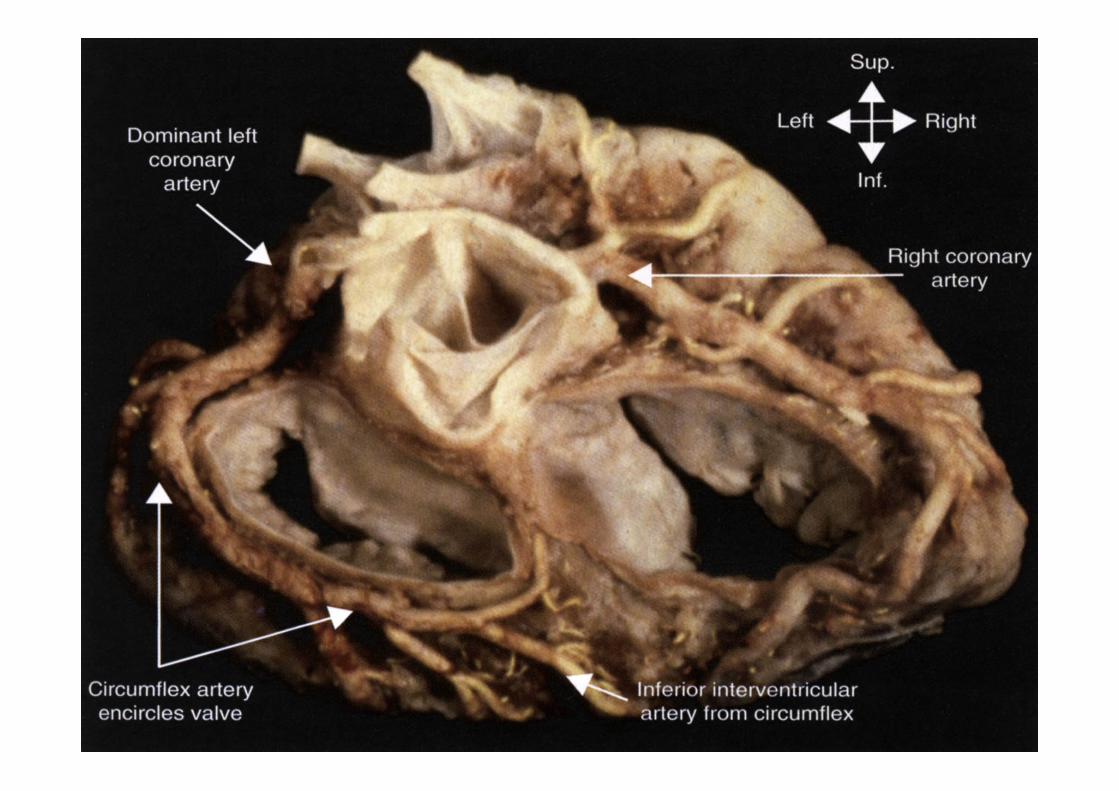
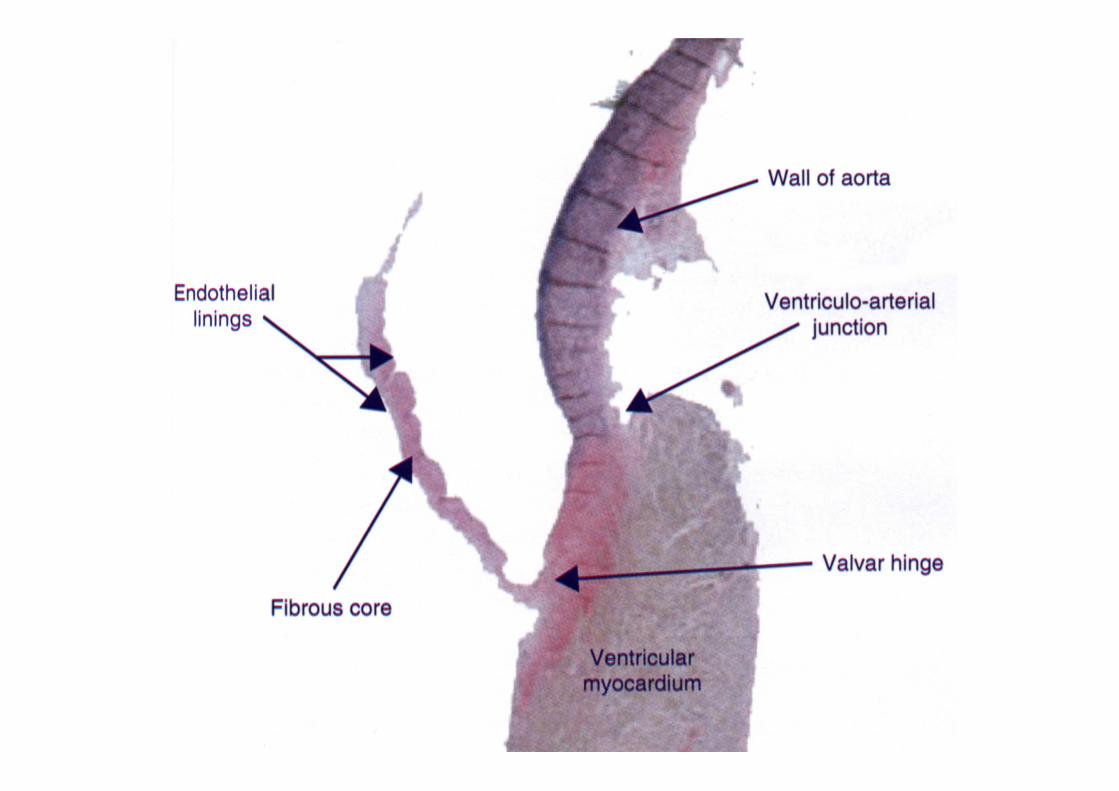
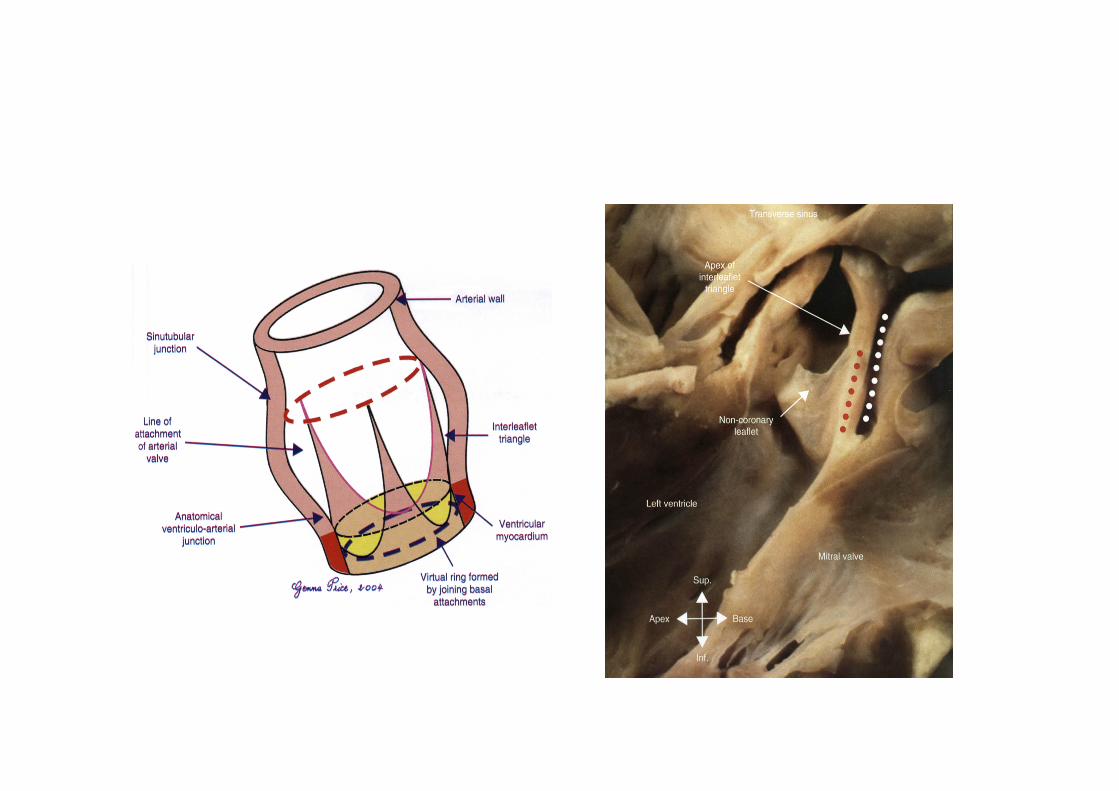
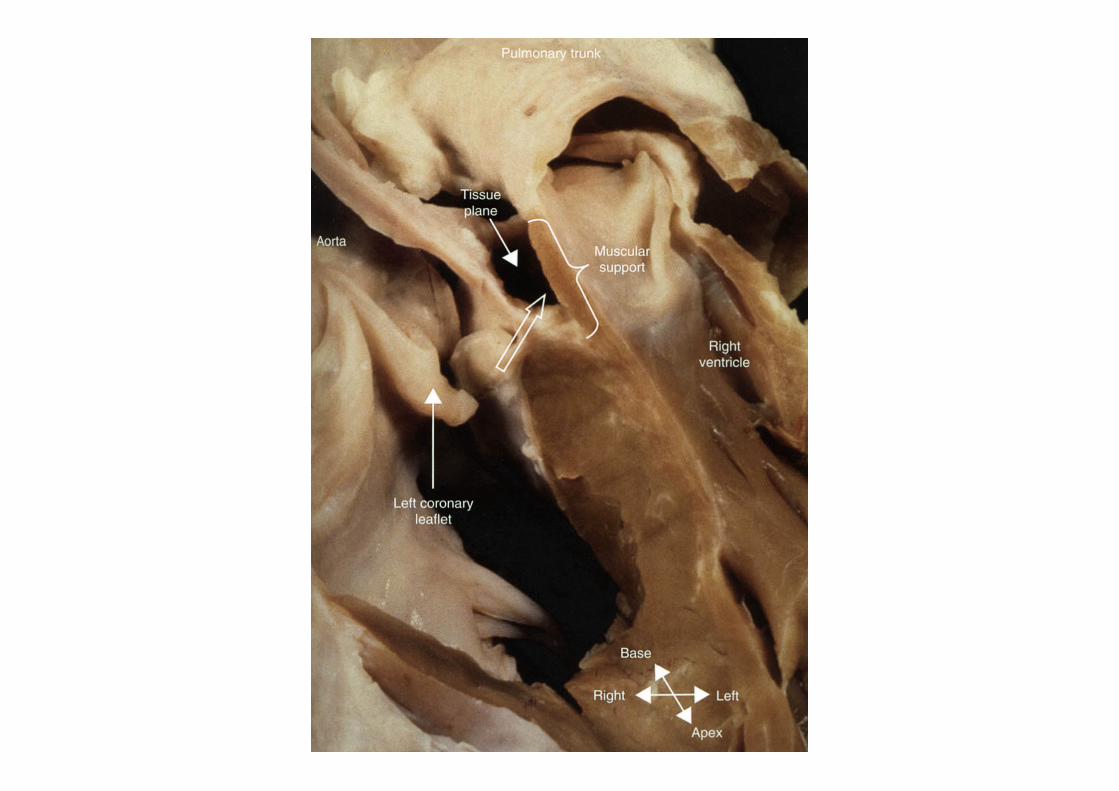
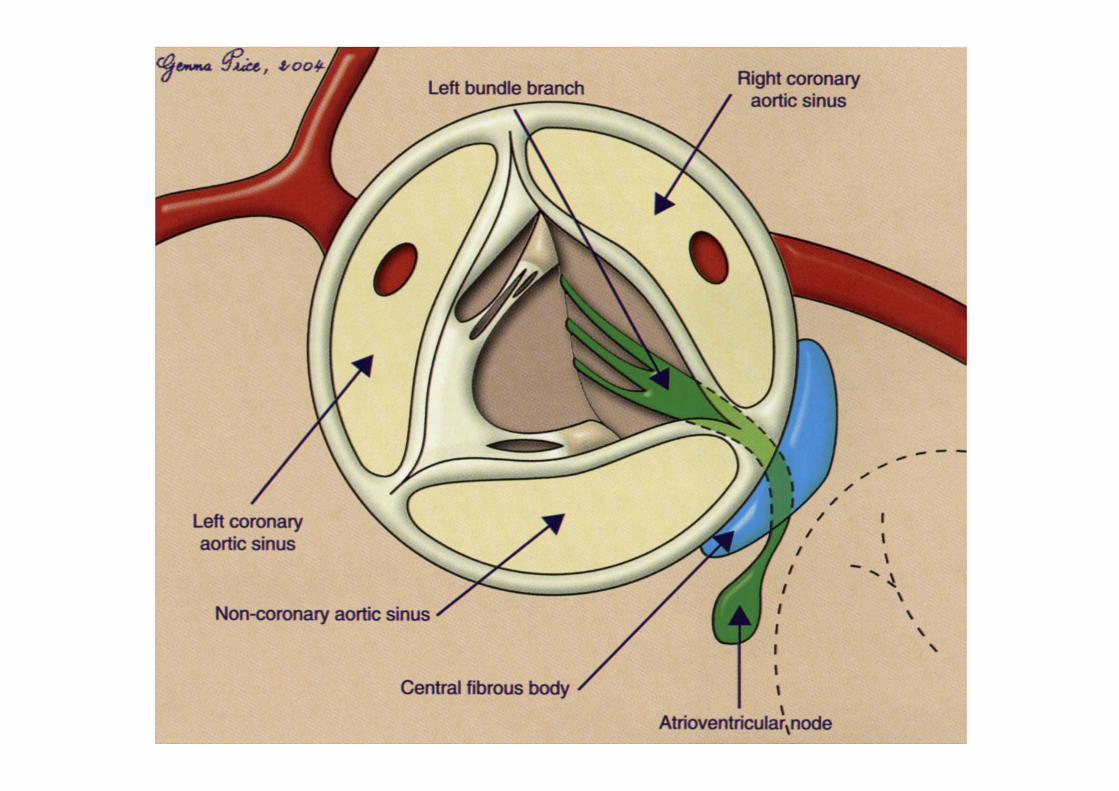
Mitral valve terminology
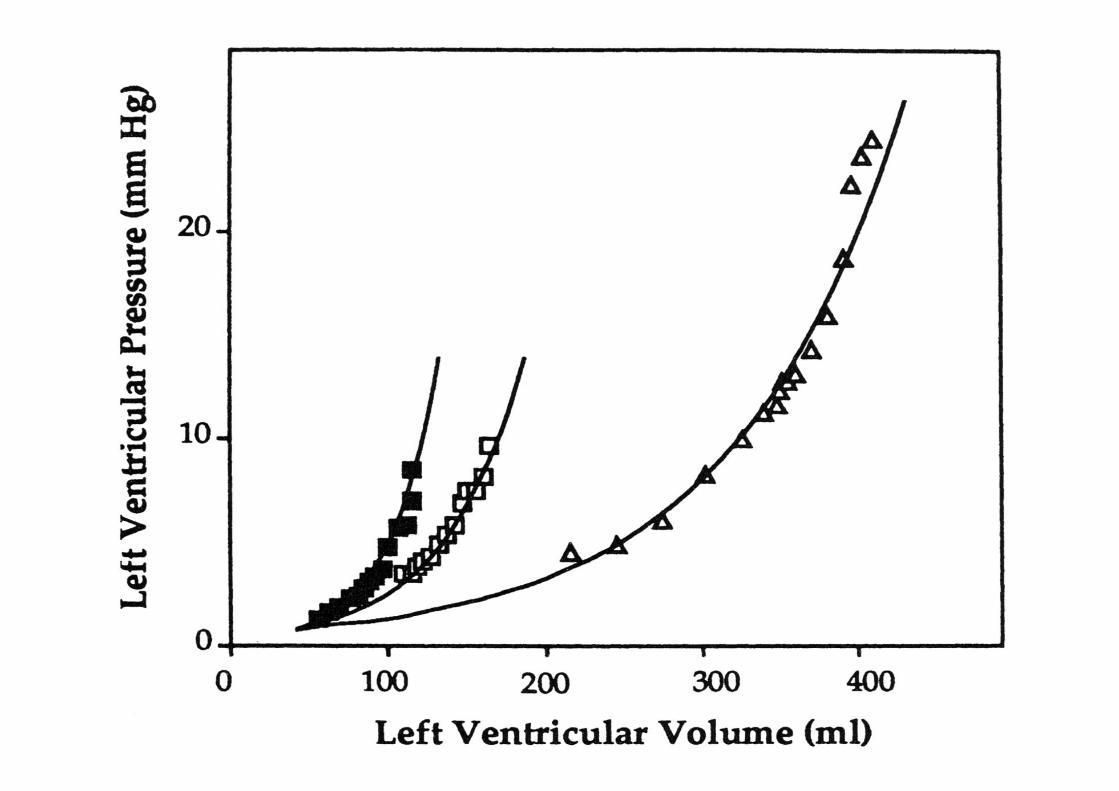
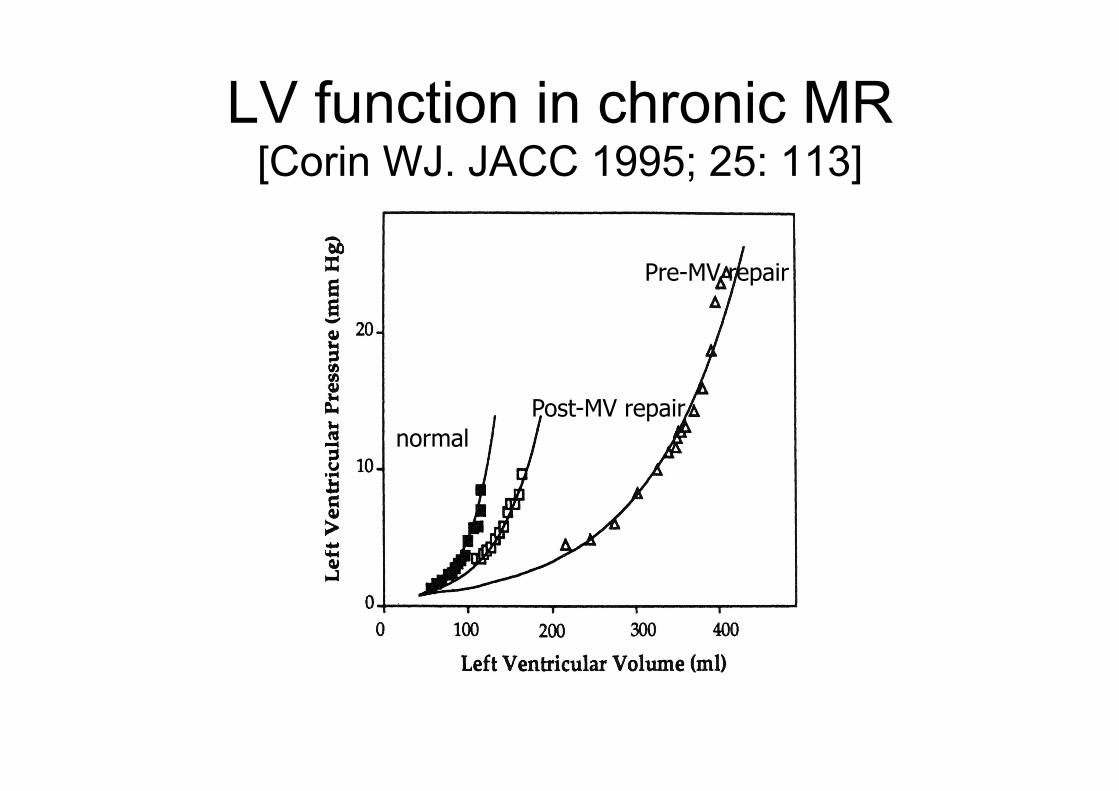
LV function in chronic MR [Corin WJ. JACC 1995; 25: 113]
Pre-MV repair
Post-MV repair normal
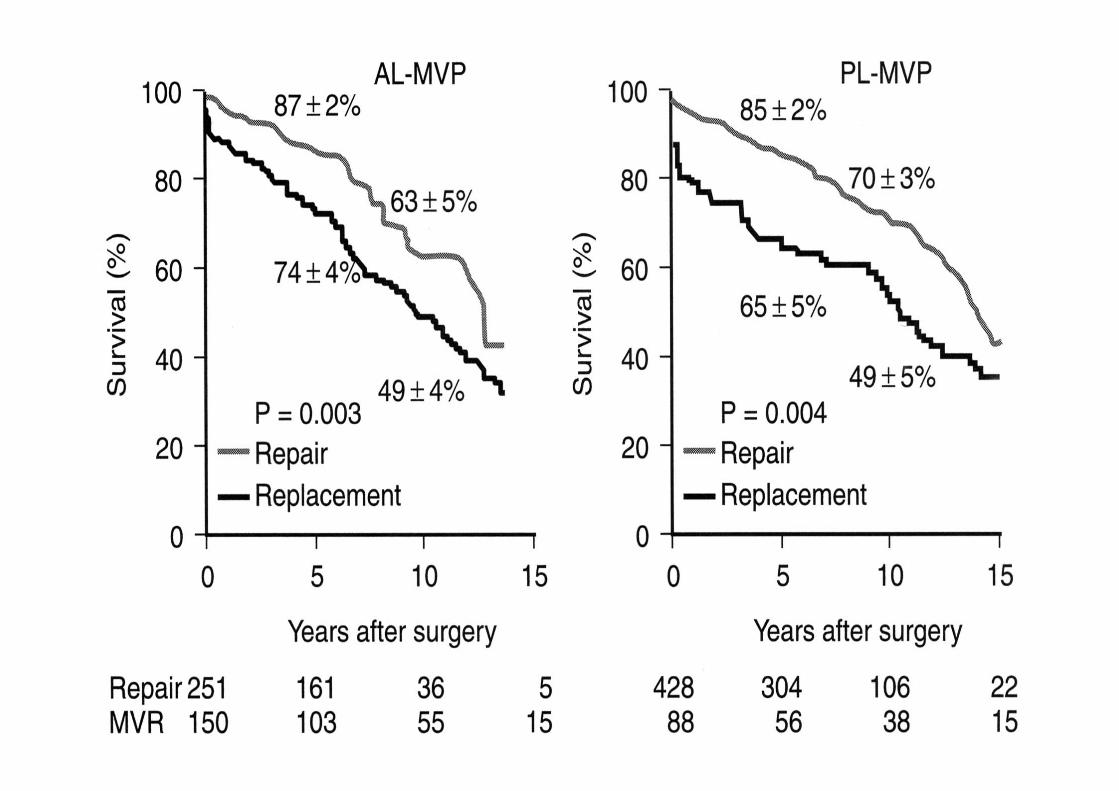
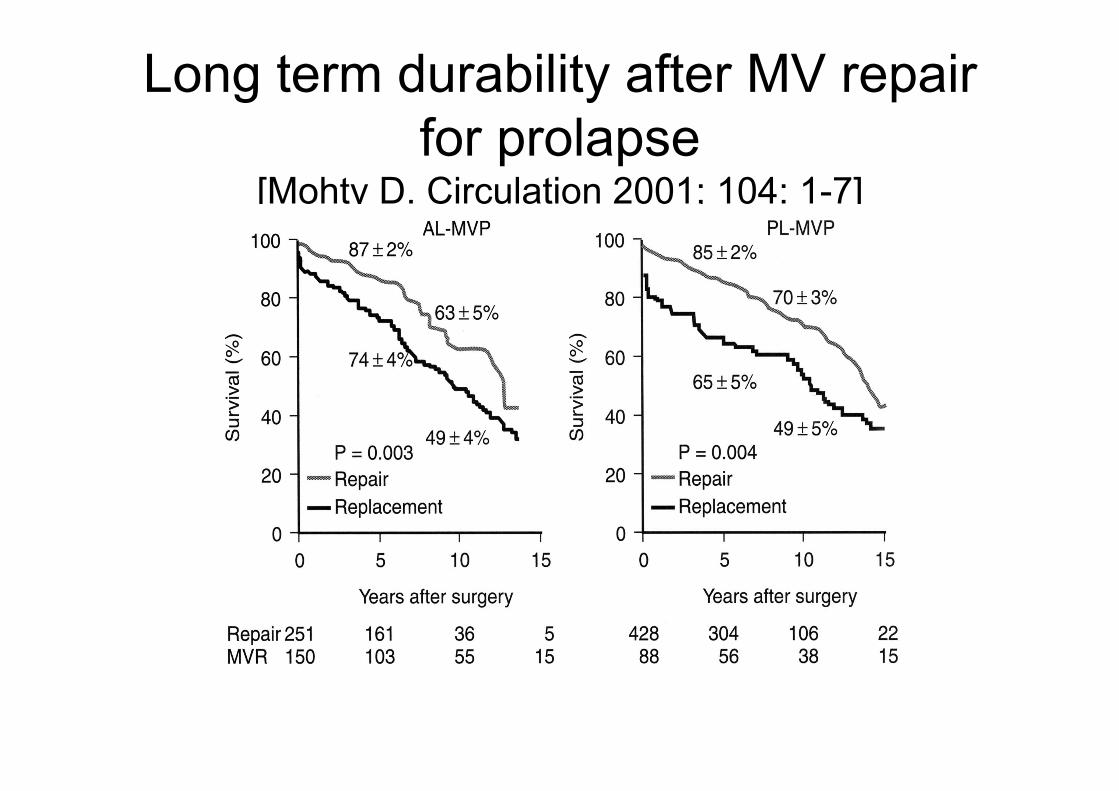
Long term durability after MV repair for prolapse
[Mohty D. Circulation 2001; 104: 1-7]
Departments of Cardiothoracic Surgery, Cardiology, Cardiovascular Magnetic
Resonance, and the Clinical Trials and Evaluation Unit
Royal Brompton & Harefield NHS Trust and
Imperial College, London
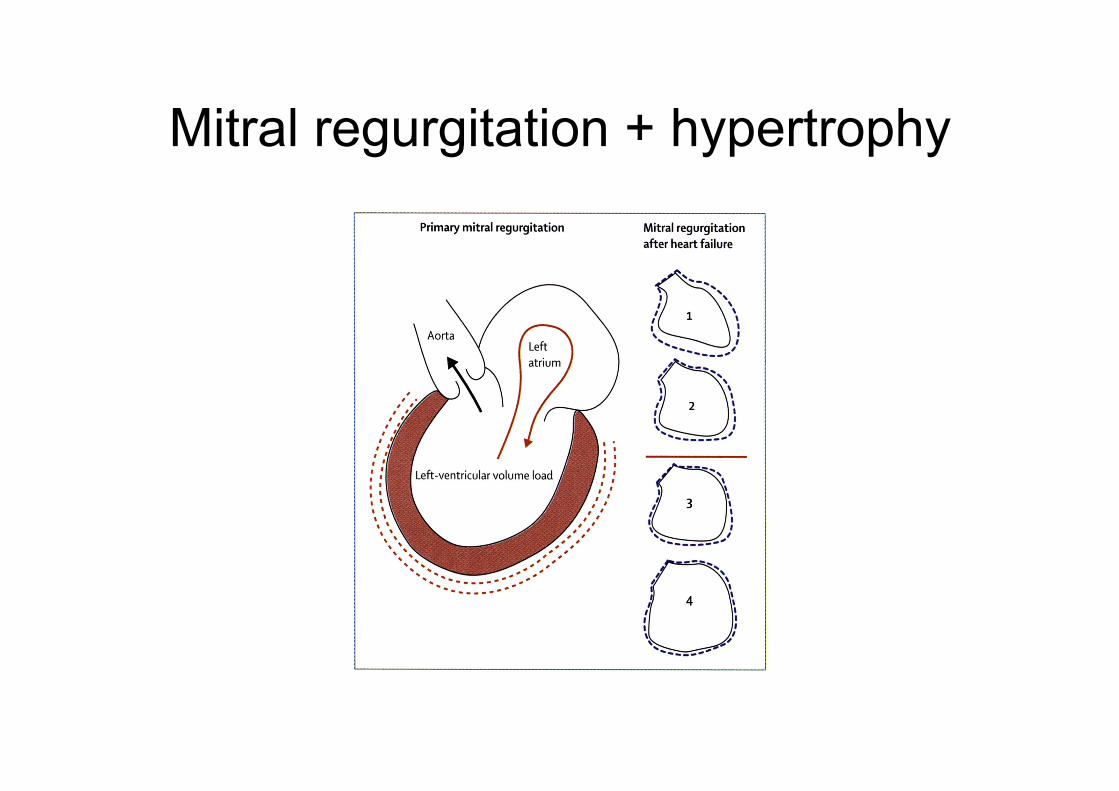
Mitral regurgitation + hypertrophy

Post infarct patterns
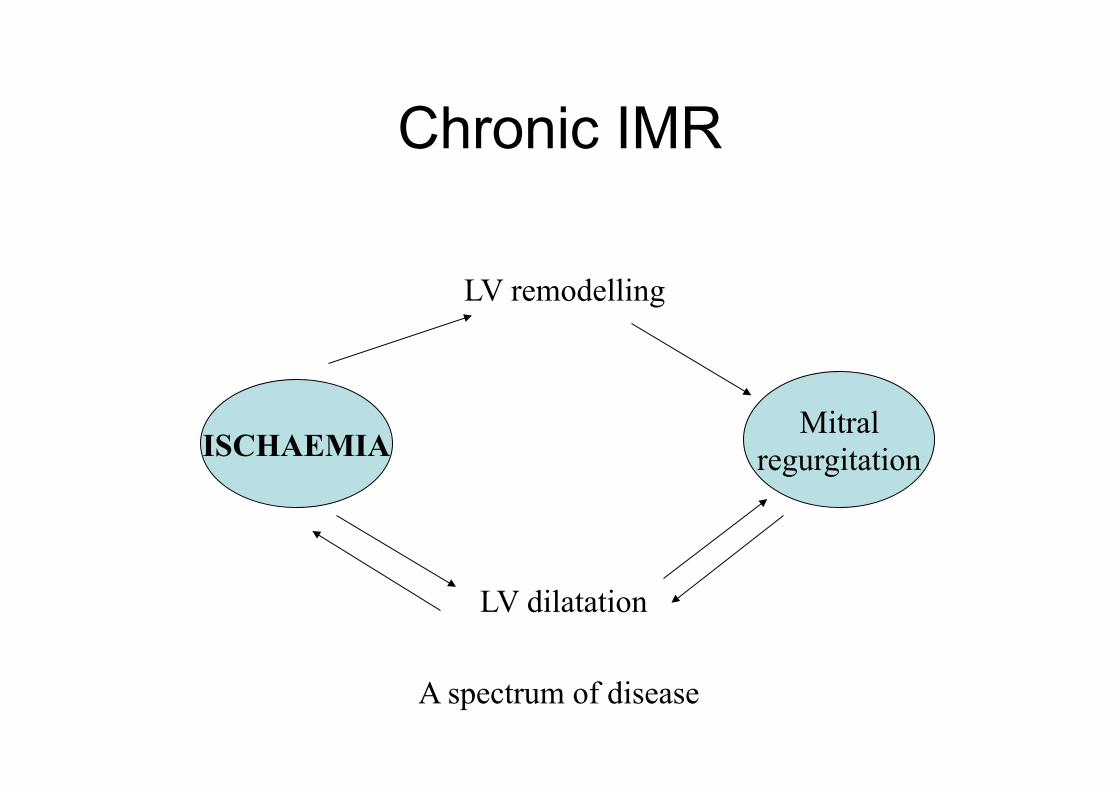
Chronic IMR
ISCHAEMIA Mitral
regurgitation
LV remodelling
LV dilatation
A spectrum of disease
IMR
• Acute myocardial infarction • Papillary muscle rupture • Papillary muscle ischaemia • Ischaemic cardiomyopathy with impaired
LV function
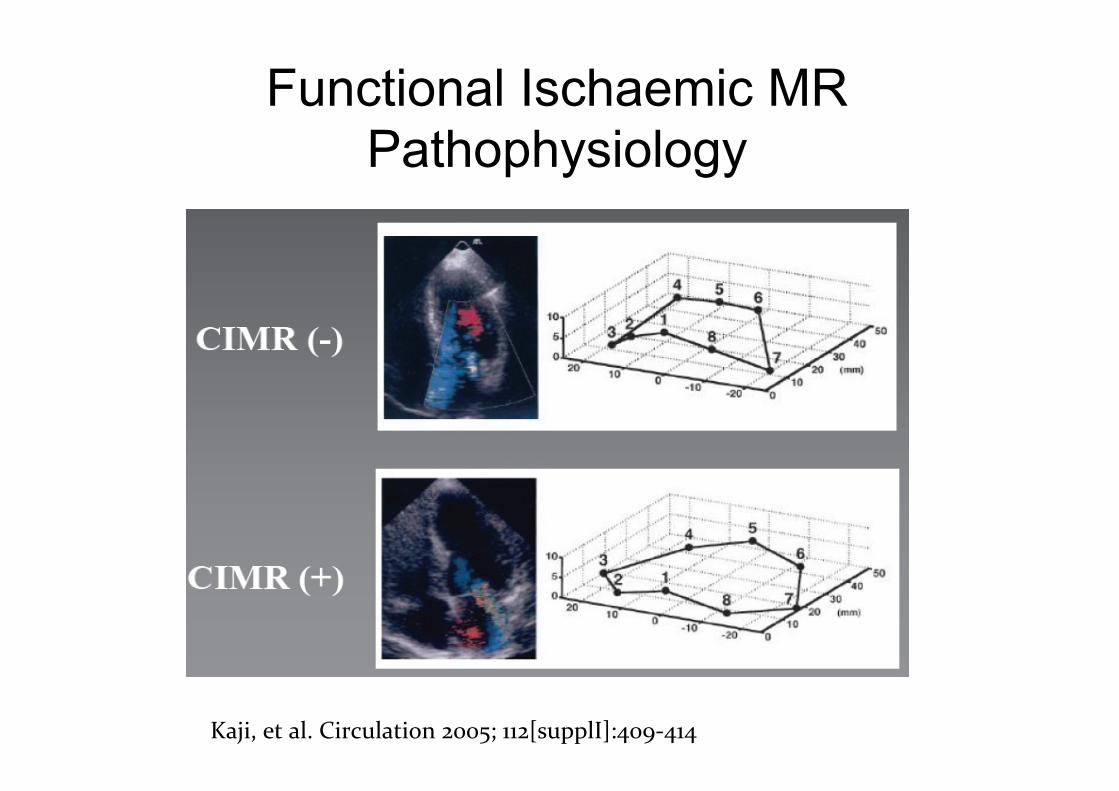
Functional Ischaemic MR Pathophysiology
Kaji, et al. Circulation 2005; 112[supplI]:409-‐414
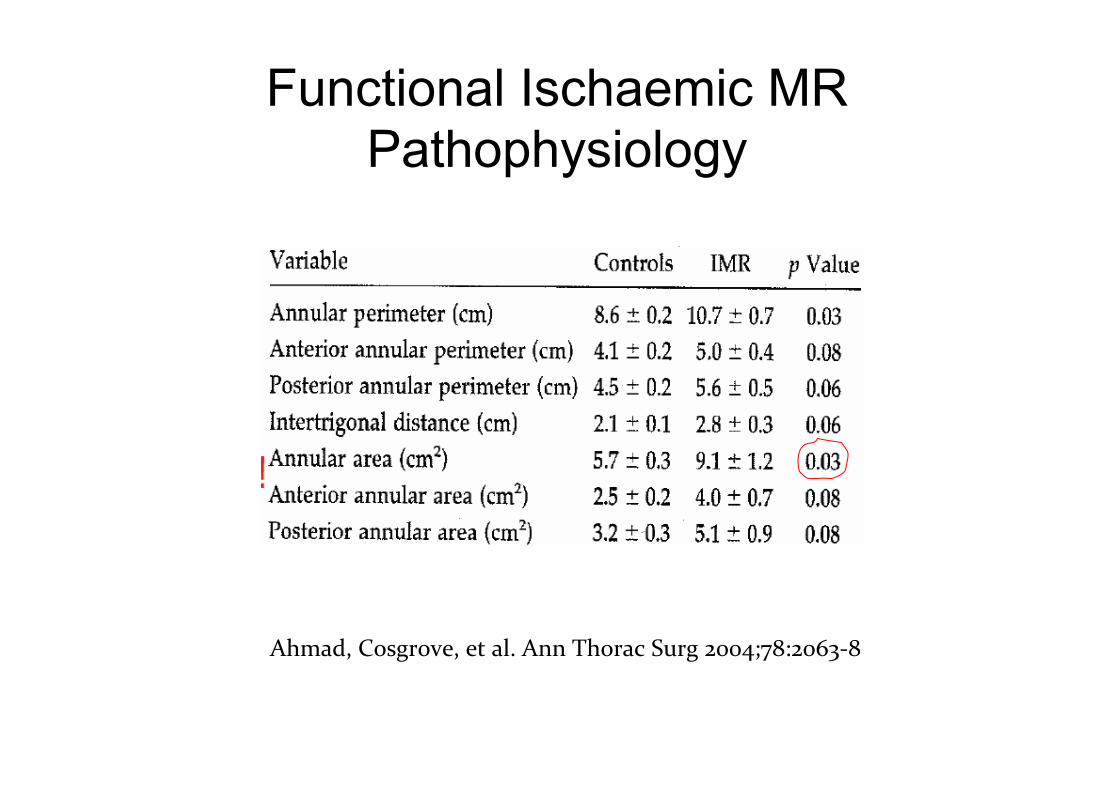
Functional Ischaemic MR Pathophysiology
Ahmad, Cosgrove, et al. Ann Thorac Surg 2004;78:2063-‐8
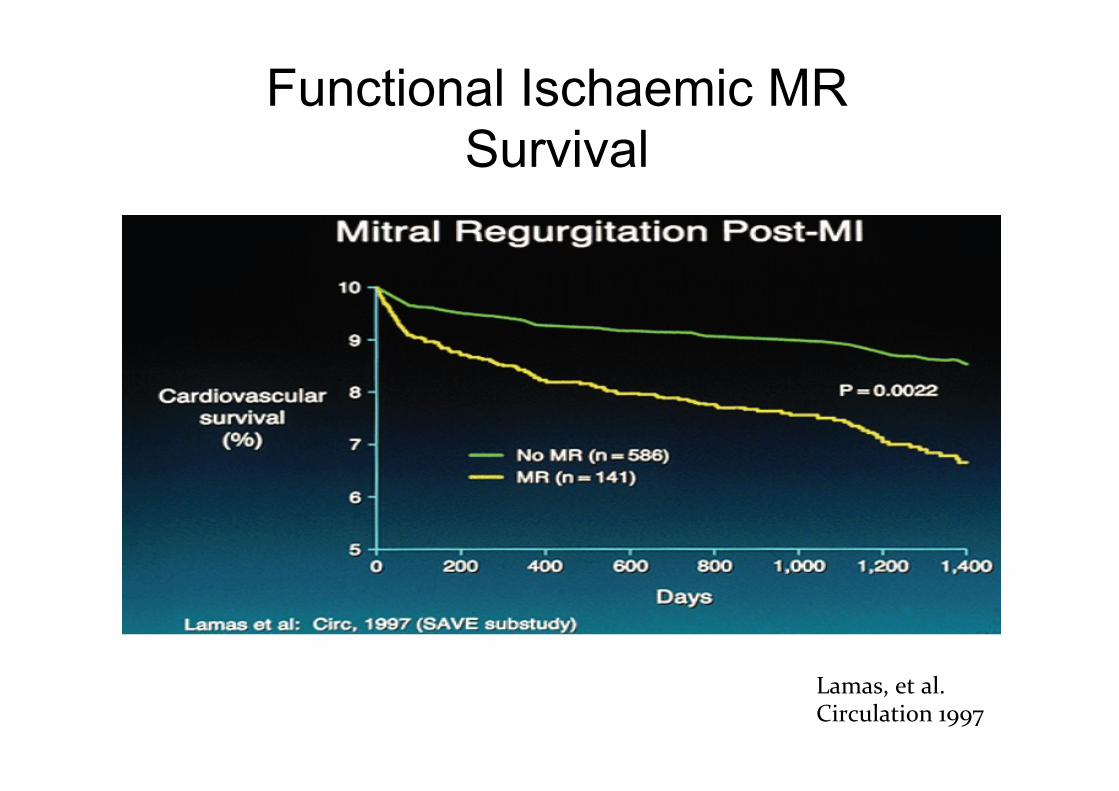
Functional Ischaemic MR Survival
Lamas, et al. Circulation 1997
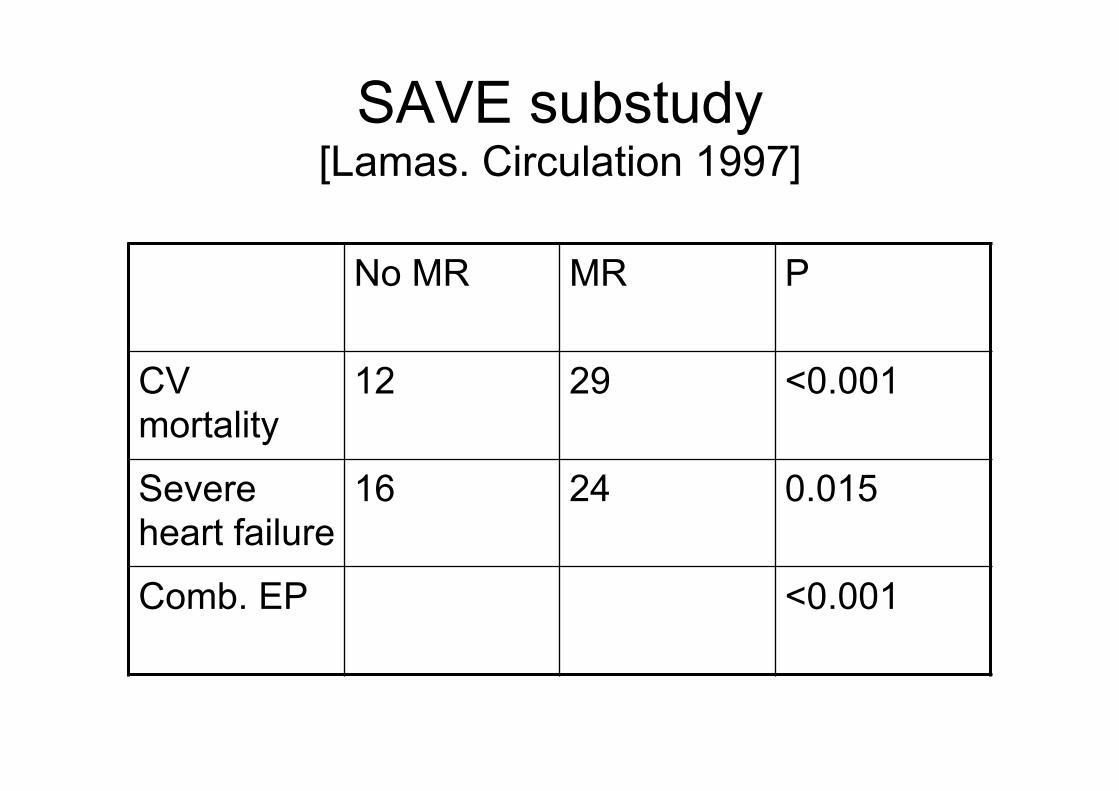
SAVE substudy [Lamas. Circulation 1997]
No MR MR P
CV mortality
12 29 <0.001
Severe heart failure
16 24 0.015
Comb. EP <0.001
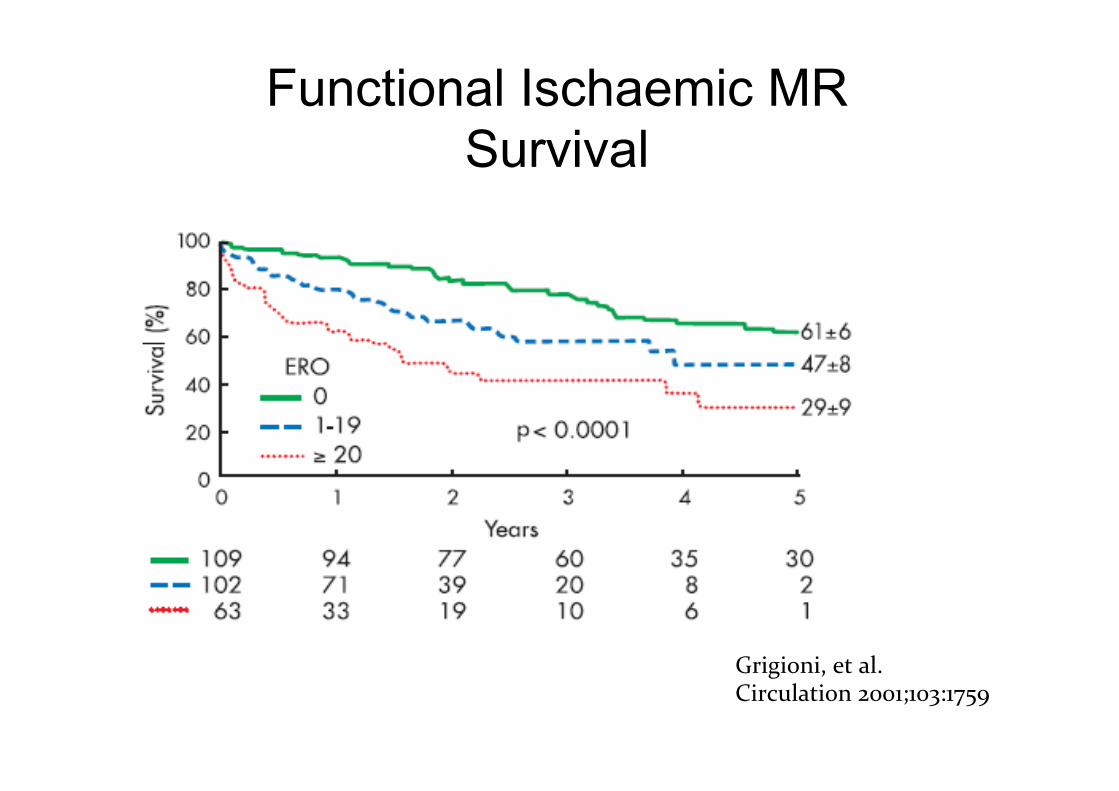
Functional Ischaemic MR Survival
Grigioni, et al. Circulation 2001;103:1759
Functional Ischaemic MR
• Does CABG improve moderate functional ischaemic MR?
• Does it improve outcome?
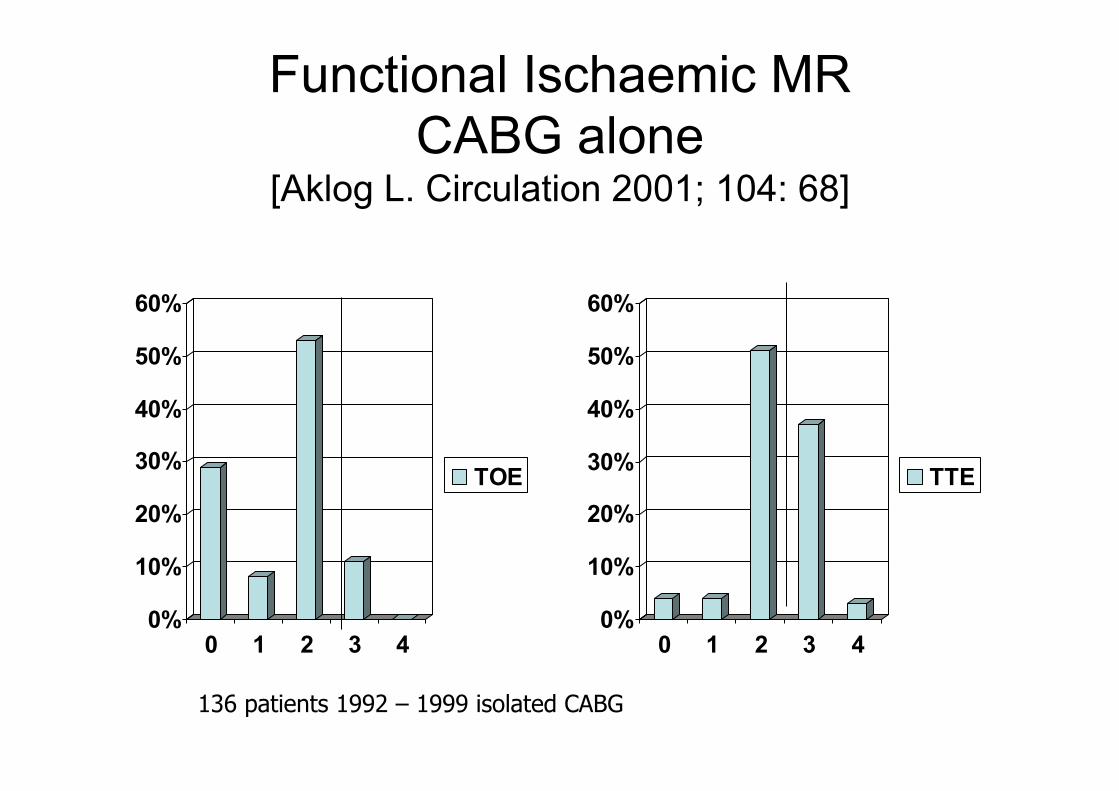
Functional Ischaemic MR CABG alone
[Aklog L. Circulation 2001; 104: 68]
0%
10%
20%
30%
40%
50%
60%
0 1 2 3 4
TTE
0%
10%
20%
30%
40%
50%
60%
0 1 2 3 4
TOE
136 patients 1992 – 1999 isolated CABG
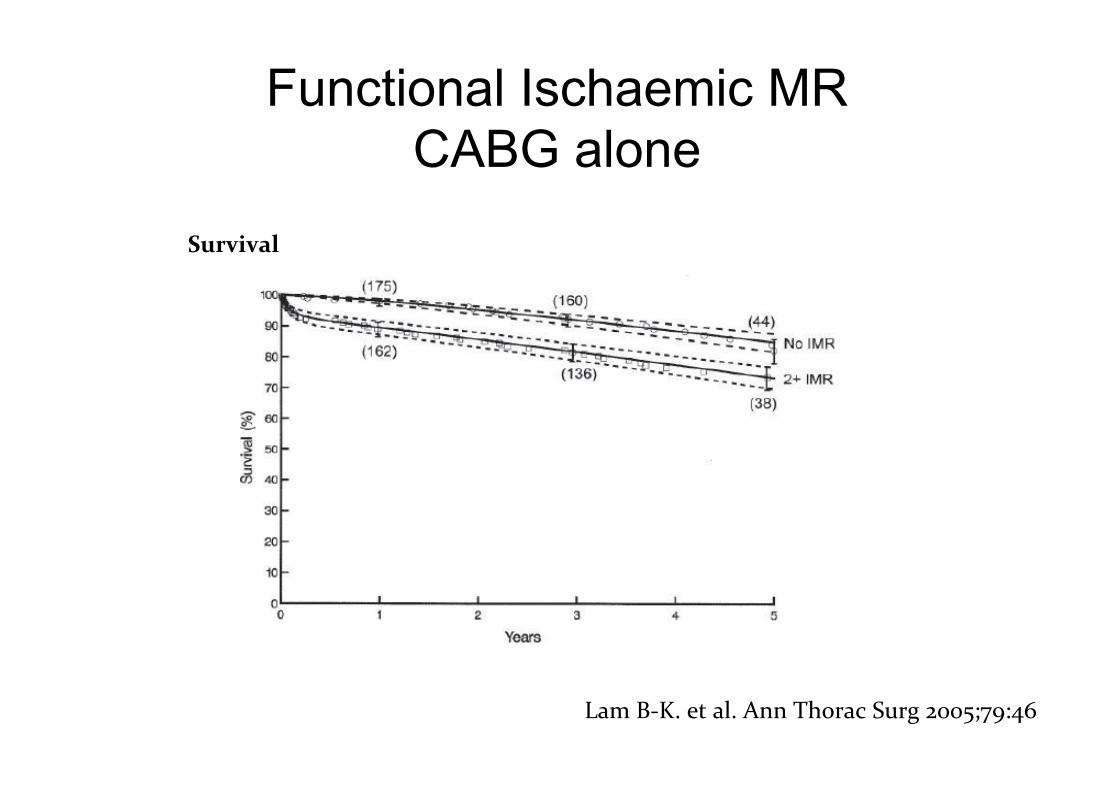
Functional Ischaemic MR CABG alone
Lam B-‐K. et al. Ann Thorac Surg 2005;79:462
Survival
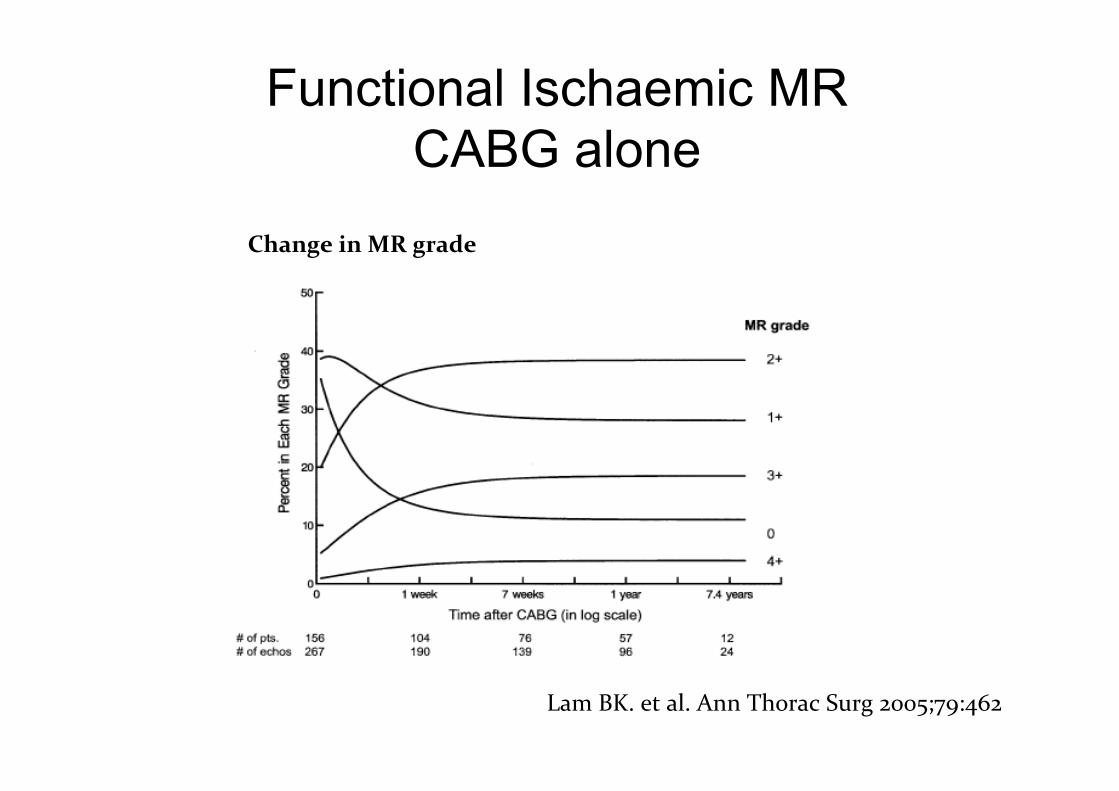
Functional Ischaemic MR CABG alone
Lam BK. et al. Ann Thorac Surg 2005;79:462
Change in MR grade
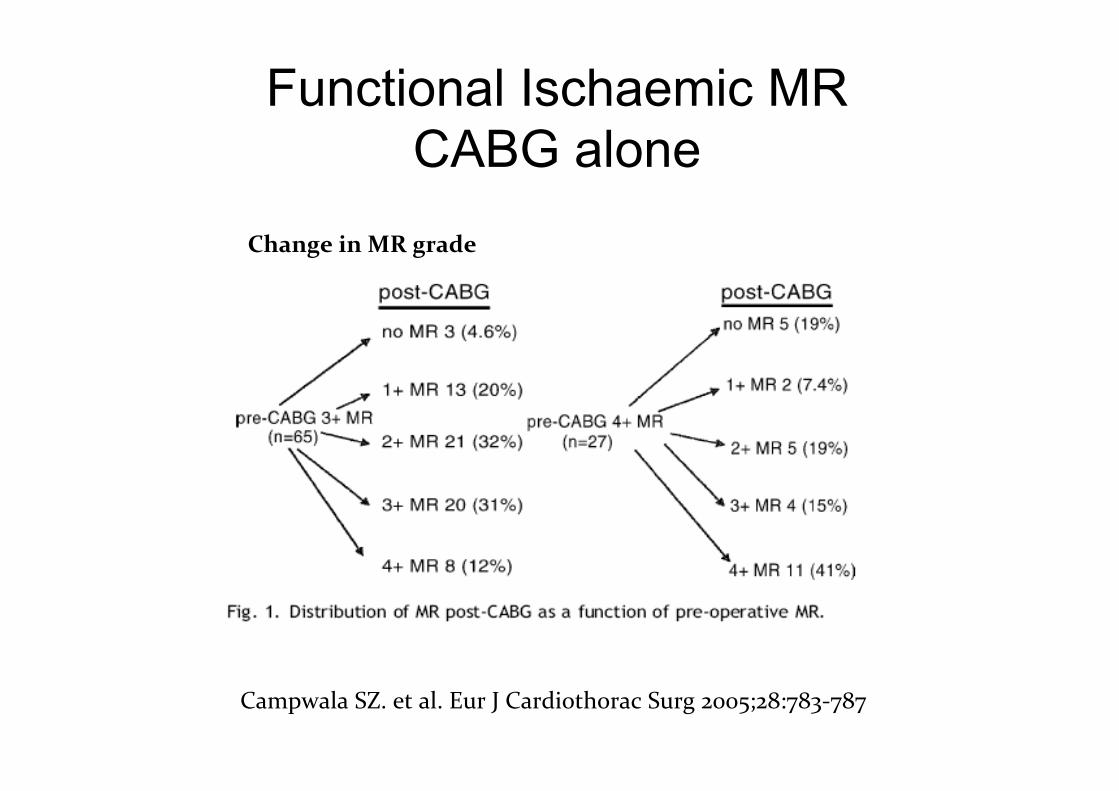
Functional Ischaemic MR CABG alone
Campwala SZ. et al. Eur J Cardiothorac Surg 2005;28:783-‐787
Change in MR grade
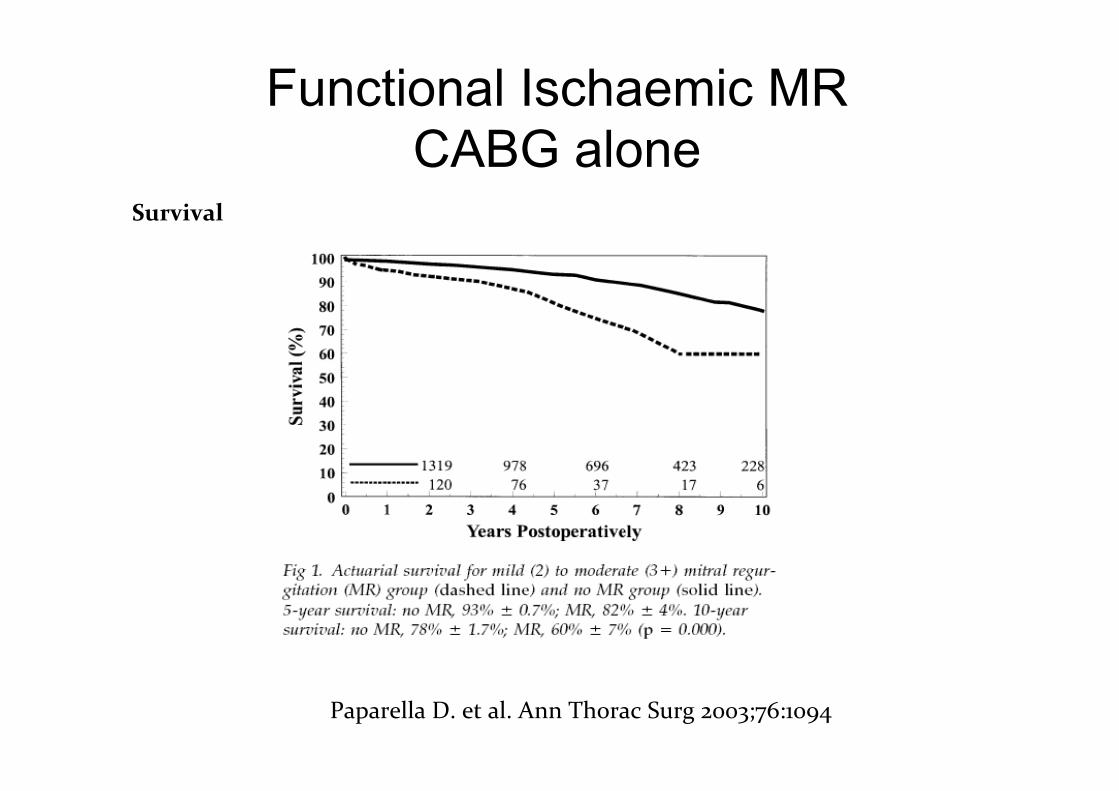
Functional Ischaemic MR CABG alone
Paparella D. et al. Ann Thorac Surg 2003;76:1094
Survival
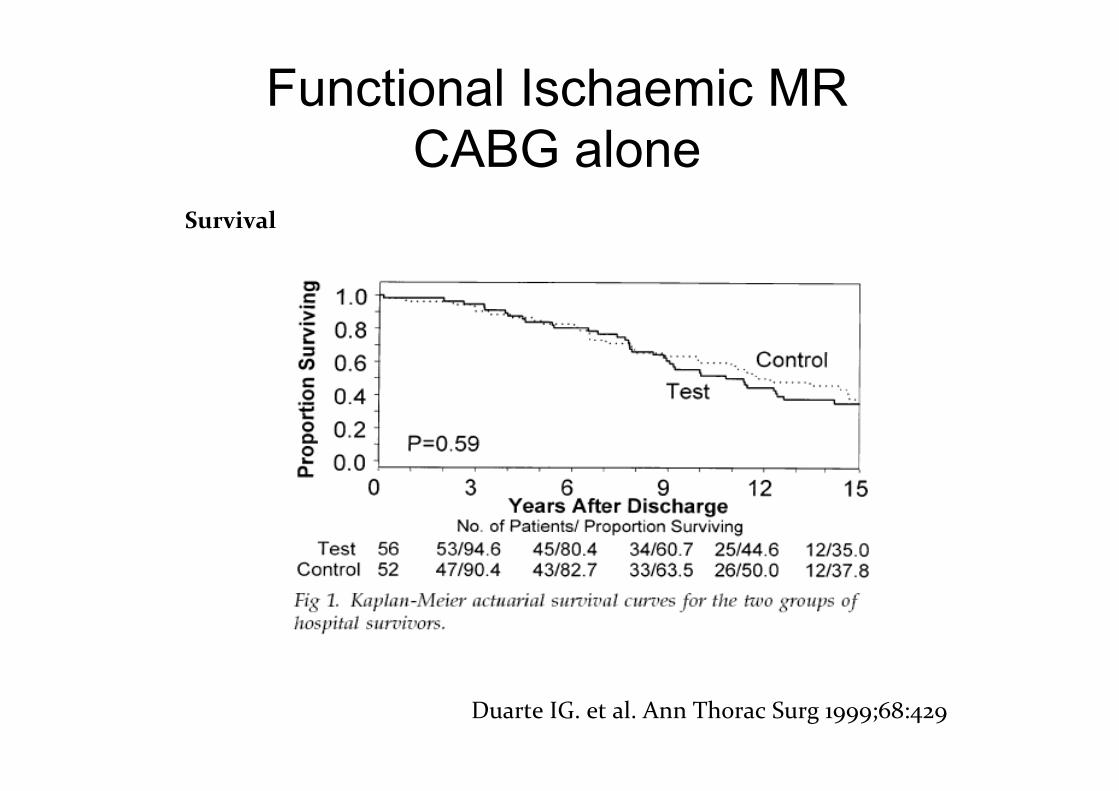
Functional Ischaemic MR CABG alone
Duarte IG. et al. Ann Thorac Surg 1999;68:429
Survival
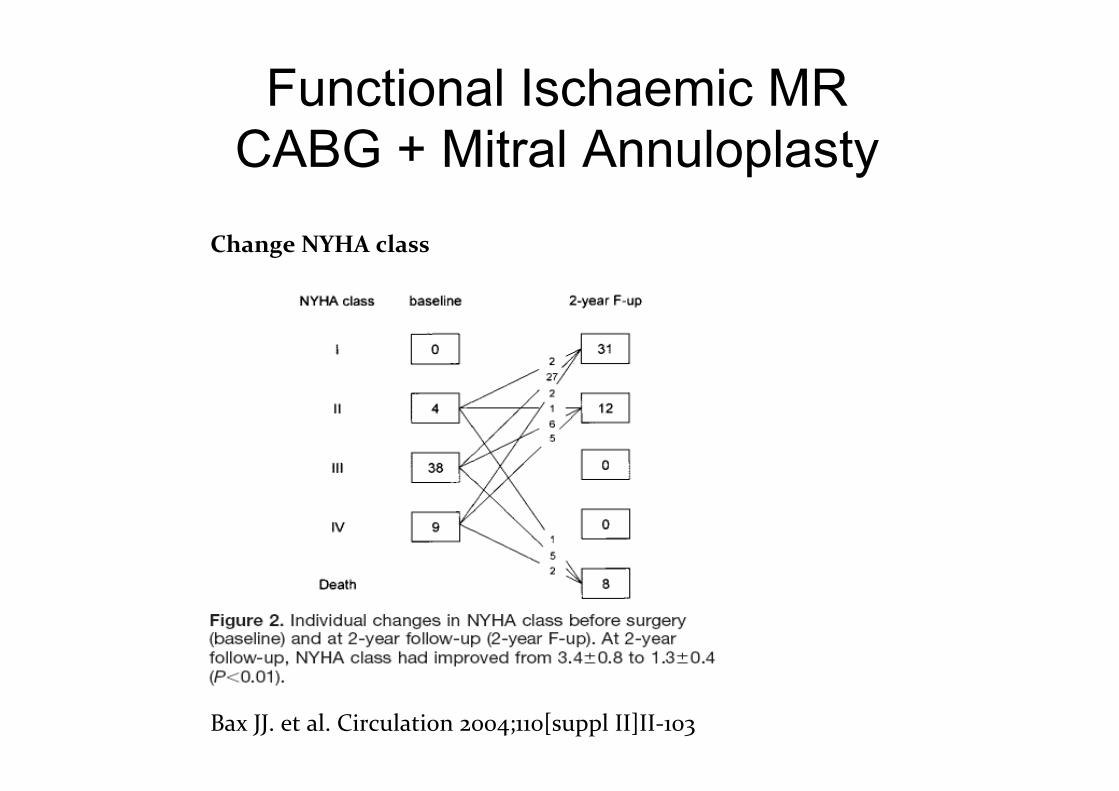
Functional Ischaemic MR CABG + Mitral Annuloplasty
Bax JJ. et al. Circulation 2004;110[suppl II]II-‐103
Change NYHA class
Functional Ischaemic MR CABG + Mitral Annuloplasty
• Does CABG + mitral annuloplasty improve outcome?
Functional Ischaemic MR CABG + Mitral Annuloplasty
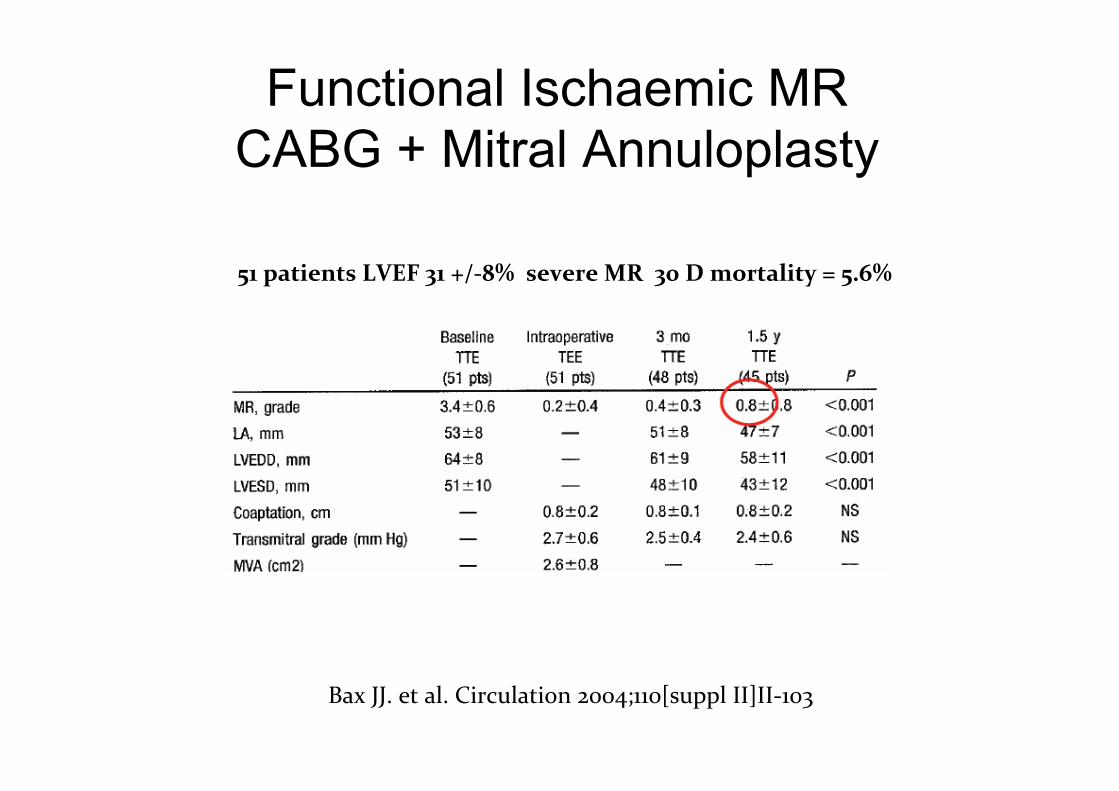
Bax JJ. et al. Circulation 2004;110[suppl II]II-‐103
51 patients LVEF 31 +/-‐8% severe MR 30 D mortality = 5.6%
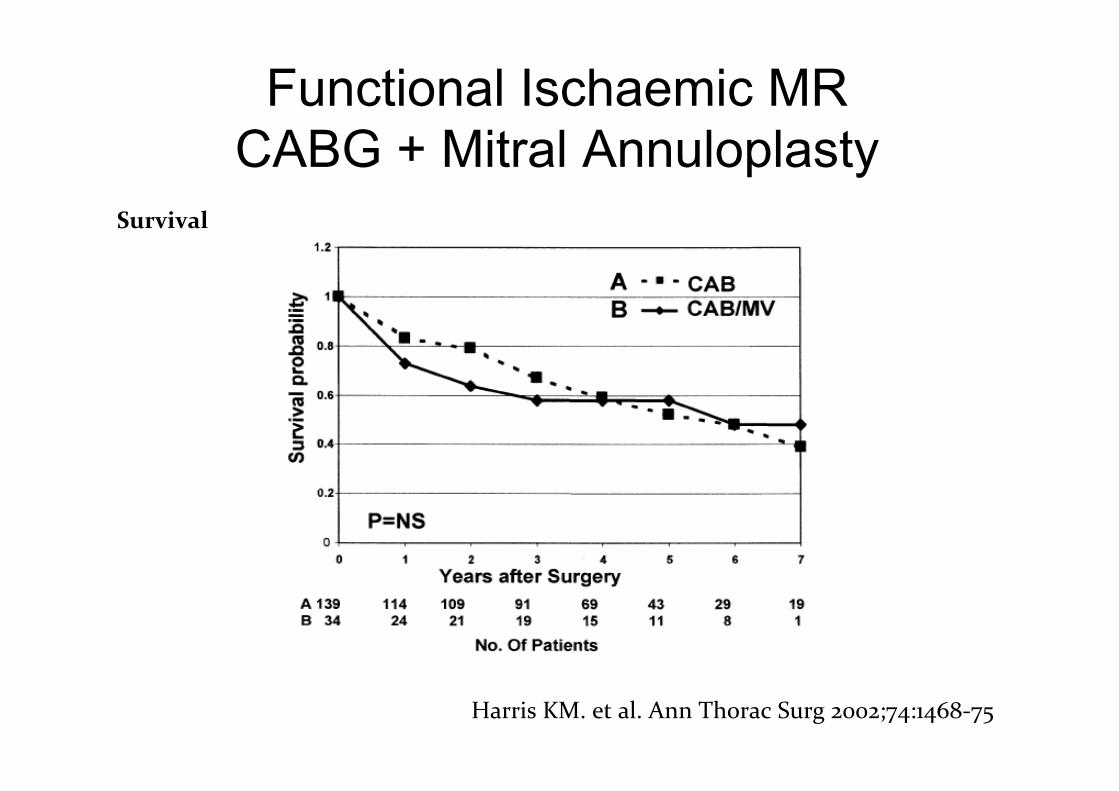
Functional Ischaemic MR CABG + Mitral Annuloplasty
Harris KM. et al. Ann Thorac Surg 2002;74:1468-‐75
Survival

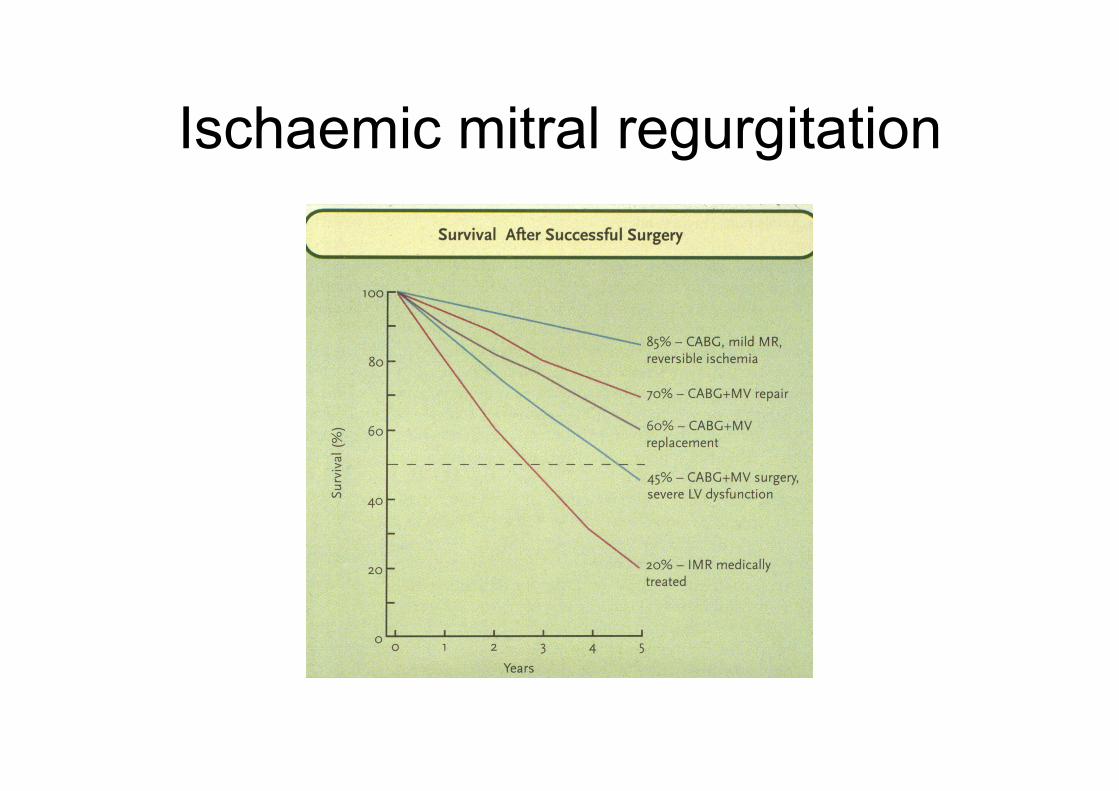
Ischaemic mitral regurgitation

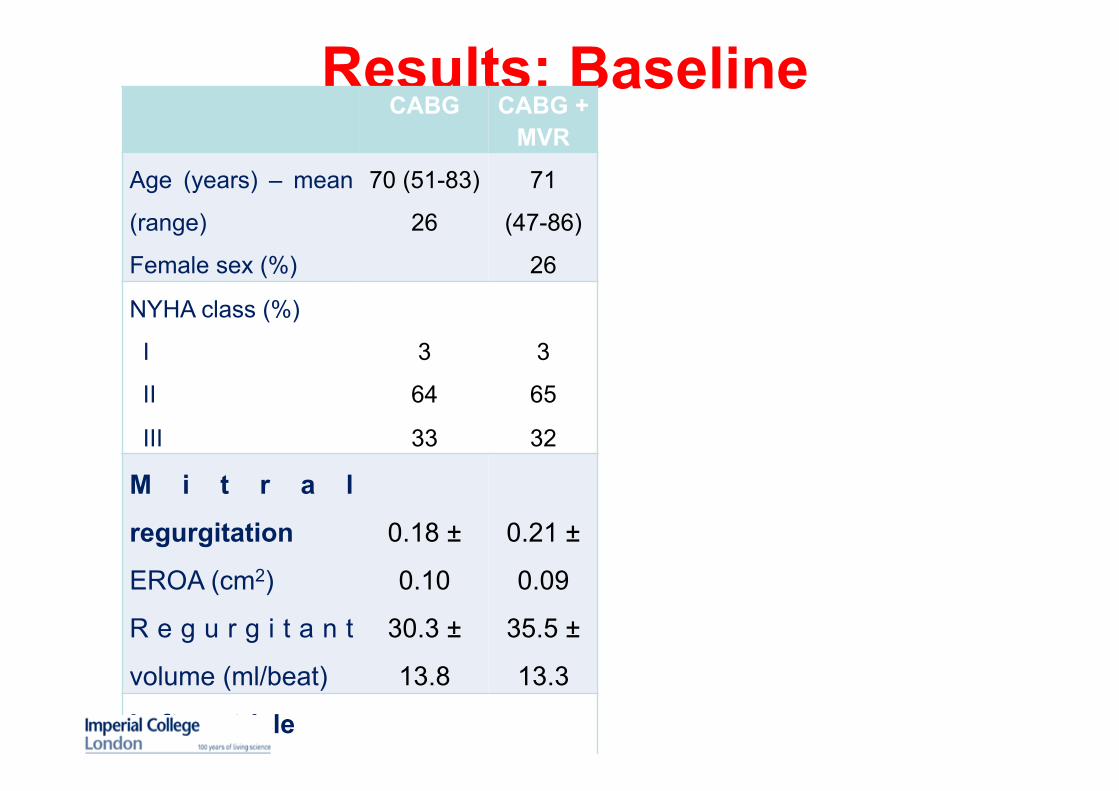
Results: Baseline CABG CABG +
MVR
Age (years) – mean
(range)
Female sex (%)
70 (51-83)
26
71
(47-86)
26
NYHA class (%)
I
II
III
3
64
33
3
65
32
M i t r a l
regurgitation
EROA (cm2)
R e g u r g i t a n t
volume (ml/beat)
0.18 ±
0.10
30.3 ±
13.8
0.21 ±
0.09
35.5 ±
13.3
Left ventricle
LVESD (mm)
LVEDD (mm)
L V E j e c t i o n
fraction (%)
43.3 ±
9.5
56.5 ±
12.0
40.3 ±
16.1
45.7 ±
7.4
56.5 ±
12.6
40.0 ±
17.3