
Pelvic floor trauma following vaginal delivery Hans...
10
Pelvic floor trauma following vaginal delivery Hans Peter Dietz Purpose of review Recent years have seen a steady increase in the information available regarding pelvic floor trauma in childbirth. A review of this information is timely in view of the ongoing discussion concerning elective caesarean section. Recent findings In addition to older evidence regarding pudendal nerve injury, it has recently been shown that inferior aspects of the levator ani and fascial pelvic organ supports such as the rectovaginal septum can be disrupted in childbirth. Such trauma is associated with pelvic organ prolapse, bowel dysfunction, and urinary incontinence. Elective caesarean section seems to have a limited protective effect that appears to weaken with time. Older age at first delivery may be associated with a higher likelihood of trauma and subsequent symptoms. Summary Pelvic floor trauma is a reality, not a myth. It is currently not possible, however, to advise patients as to whether avoidance of potential intrapartum pelvic floor trauma is worth the risk, cost, and effort of elective caesarean section. In some women this may well be the case. The identification of women at high risk for delivery-related pelvic floor trauma should be a priority for future research in this field. Keywords childbirth, delivery, levator muscle, pelvic floor, prolapse, ultrasound Curr Opin Obstet Gynecol 18:528–537. ß 2006 Lippincott Williams & Wilkins. Nepean Campus, Western Clinical School, University of Sydney, Penrith, Australia Correspondence to H.P. Dietz, PhD, 193 Burns Rd, Springwood 2777 NSW, Australia Tel: +61 2 4751 8140; fax: +61 2 4734 1817; e-mail: [email protected] Current Opinion in Obstetrics and Gynecology 2006, 18:528–537 Abbreviations MRI magnetic resonance imaging POP-Q pelvic organ prolapse quantification system ß 2006 Lippincott Williams & Wilkins 1040-872X Introduction Obstetrics is currently undergoing its most major change since the introduction of antenatal ultrasound. At times one wonders whether in the long run vaginal childbirth is destined to become a practice limited to fringe groups and resource-poor settings. Not surprisingly, the issue often elicits emotional responses as any change in the status quo would have major implications for the relative role of healthcare providers and require significant redis- tribution of scarce resources. Inevitably, discussion of pelvic floor trauma in childbirth is seen as partisan, due to the fact that a growing awareness of potential negative effects of vaginal childbirth, such as urinary and faecal incontinence and pelvic organ prolapse, is very likely to contribute to rising caesarean section rates, even if other factors may currently predominate [1,2]. There is no doubt, however, that caesarean section, whether primary or secondary, can lead to significant and occasion- ally major morbidity and even mortality. For now we have no means of determining whether this risk outweighs the risk of attempted vaginal childbirth in a given patient, and this must be reflected in the advice that we provide to our patients. For some forms of pelvic floor morbidity, it is not clear whether pregnancy or childbirth is to blame [3,4], and long latencies between the presumptive cause (child- birth) and effect (incontinence and prolapse) further complicate research. Despite all this, we now have rela- tively firm epidemiologic evidence on the association between vaginal childbirth and urinary incontinence and prolapse [4,5 ,6], as summarized in Fig. 1 first published in a review article by DeLancey [5 ]. Regarding prolapse, pregnancy and childbirth are well documented as major risk factors [3,6]. Caesarean deliv- ery is associated with less need for surgical correction of incontinence or prolapse [3] and seems protective against symptomatic prolapse [7]. Regarding urinary inconti- nence, several large epidemiologic studies have shown that caesarean section provides partial protection from stress incontinence [4,8,9 ]. The one randomized con- trolled trial that may shed light on the degree of protec- tion to be expected from elective caesarean section is the Term Breech Trial. It showed a relative risk of 0.62 in the elective caesarean section group 3 months after childbirth [8], but of course these data are of limited use due to the special nature of breech delivery. Any protective effect appears to fade over time [9 ] as congenital factors and changes related to ageing will increasingly outweigh the 528
-
Upload
truongcong -
Category
Documents
-
view
223 -
download
2
Transcript of Pelvic floor trauma following vaginal delivery Hans...

Pelvic floor trauma following va
ginal deliveryHans Peter DietzPurpose of review
Recent years have seen a steady increase in the information
available regarding pelvic floor trauma in childbirth. A review
of this information is timely in view of the ongoing discussion
concerning elective caesarean section.
Recent findings
In addition to older evidence regarding pudendal nerve
injury, it has recently been shown that inferior aspects of the
levator ani and fascial pelvic organ supports such as the
rectovaginal septum can be disrupted in childbirth. Such
trauma is associated with pelvic organ prolapse, bowel
dysfunction, and urinary incontinence. Elective caesarean
section seems to have a limited protective effect that
appears to weaken with time. Older age at first delivery may
be associated with a higher likelihood of trauma and
subsequent symptoms.
Summary
Pelvic floor trauma is a reality, not a myth. It is currently not
possible, however, to advise patients as to whether
avoidance of potential intrapartum pelvic floor trauma is
worth the risk, cost, and effort of elective caesarean section.
In some women this may well be the case. The identification
of women at high risk for delivery-related pelvic floor trauma
should be a priority for future research in this field.
Keywords
childbirth, delivery, levator muscle, pelvic floor, prolapse,
ultrasound
Curr Opin Obstet Gynecol 18:528–537. � 2006 Lippincott Williams & Wilkins.
Nepean Campus, Western Clinical School, University of Sydney, Penrith, Australia
Correspondence to H.P. Dietz, PhD, 193 Burns Rd, Springwood 2777 NSW,AustraliaTel: +61 2 4751 8140; fax: +61 2 4734 1817; e-mail: [email protected]
Current Opinion in Obstetrics and Gynecology 2006, 18:528–537
Abbreviations
MRI m
528
agnetic resonance imaging
POP-Q p elvic organ prolapse quantification system� 2006 Lippincott Williams & Wilkins1040-872X
IntroductionObstetrics is currently undergoing its most major change
since the introduction of antenatal ultrasound. At times
one wonders whether in the long run vaginal childbirth is
destined to become a practice limited to fringe groups
and resource-poor settings. Not surprisingly, the issue
often elicits emotional responses as any change in the
status quo would have major implications for the relative
role of healthcare providers and require significant redis-
tribution of scarce resources. Inevitably, discussion of
pelvic floor trauma in childbirth is seen as partisan,
due to the fact that a growing awareness of potential
negative effects of vaginal childbirth, such as urinary and
faecal incontinence and pelvic organ prolapse, is very
likely to contribute to rising caesarean section rates, even
if other factors may currently predominate [1,2]. There is
no doubt, however, that caesarean section, whether
primary or secondary, can lead to significant and occasion-
ally major morbidity and even mortality. For now we have
no means of determining whether this risk outweighs the
risk of attempted vaginal childbirth in a given patient,
and this must be reflected in the advice that we provide to
our patients.
For some forms of pelvic floor morbidity, it is not clear
whether pregnancy or childbirth is to blame [3,4], and
long latencies between the presumptive cause (child-
birth) and effect (incontinence and prolapse) further
complicate research. Despite all this, we now have rela-
tively firm epidemiologic evidence on the association
between vaginal childbirth and urinary incontinence
and prolapse [4,5��,6], as summarized in Fig. 1 first
published in a review article by DeLancey [5��].
Regarding prolapse, pregnancy and childbirth are well
documented as major risk factors [3,6]. Caesarean deliv-
ery is associated with less need for surgical correction of
incontinence or prolapse [3] and seems protective against
symptomatic prolapse [7]. Regarding urinary inconti-
nence, several large epidemiologic studies have shown
that caesarean section provides partial protection from
stress incontinence [4,8,9��]. The one randomized con-
trolled trial that may shed light on the degree of protec-
tion to be expected from elective caesarean section is the
Term Breech Trial. It showed a relative risk of 0.62 in the
elective caesarean section group 3 months after childbirth
[8], but of course these data are of limited use due to the
special nature of breech delivery. Any protective effect
appears to fade over time [9��] as congenital factors and
changes related to ageing will increasingly outweigh the

Trauma following vaginal delivery Dietz 529
Figure 1 The effect of vaginal parity on the prevalence of urinary
incontinence and pelvic organ prolapse
10
8
6
4
2
00 1 2 3 >4
Parity
Prolapse
1
2
4
89
10.7
2.42.6 2.8
Urinary incontinence
Relative risk
Parity and associated relative risks. Originally adapted from [6] and [4];reproduced with permission from [5��].
effects of traumatic childbirth as women grow older. One
may contend, however, that any protective effect will
apply during the most active decades of a woman’s life
and therefore be desirable, even if this protection is lost
later in life.
Paradoxically, the situation seems less clear as regards
faecal incontinence, despite its being associated with
the one type of pelvic floor trauma that is often clearly
evident at the time of delivery, i.e. anal sphincter
trauma. Epidemiologic evidence generally does not
support a protective effect of caesarean section in
comparison with normal vaginal delivery [9��,10],
although much of the data is diluted by caesarean
section performed in labour. The risk of anal incon-
tinence seems significantly higher after forceps deliv-
ery [9��,10–12], however, and older age at first delivery
is another risk factor [9��].
Our knowledge base regarding the impact of vaginal
childbirth on the anatomy and function of the female
pelvic floor has increased markedly over the past two
decades. While it was established in the 1980s and
1990s that vaginal childbirth (or even just the attempt
at vaginal delivery) may significantly change pudendal
nerve conduction patterns [13,14], the limited useful-
ness of tests of nerve function in clinical practice [15]
has cast doubts on the relevance of denervation as a
major aetiologic factor in pelvic floor disorders. Con-
centric needle electromyography may provide more
accurate information but is technically difficult and
unlikely to attract many volunteers. It is not surprising
therefore that little recent electrophysiologic work
has been reported, although what there is tends to
confirm previous findings of electromyographic altera-
tions in parous women [16–18]. This review therefore
focuses on imaging evidence accumulated over the past
5 years.
Recent investigations using techniques such as magnetic
resonance imaging (MRI) and three-dimensional or four-
dimensional ultrasound have focused on pelvic organ
support, the integrity of fascial support structures, func-
tion and morphology of the levator ani muscle, and the
external and internal anal sphincter. While the relative
roles of muscle and fascia for pelvic organ support con-
tinue to be debated, both seem to be subject to delivery-
related trauma.
Pelvic organ supportClinical studies of pelvic organ support were until
recently limited by a lack of sufficiently sensitive tools
for prolapse assessment. This has changed with the
introduction of the pelvic organ prolapse quantification
system (POP-Q) [19]. Vaginal parity seems to be a risk
factor for pelvic organ prolapse as defined by the POP-Q
assessment [20] and is associated with higher degrees of
pelvic organ mobility as shown by POP-Q in young
women [21], but studies comparing antepartum with
postpartum findings are scarce due to the fact that even
such a simple assessment is invasive and less well toler-
ated in pregnancy and puerperium.
Several authors have demonstrated increased pelvic
organ mobility in parous women on using real-time
ultrasound imaging, whether in cohorts of symptomatic
older patients presenting to urogynaecology clinics [22] or
in the puerperium. There are few data on the effect of
pregnancy itself [23], but several authors have observed
the effect of labour and delivery, examining women both
before and after childbirth [24–27]. From this evidence,
it seems clear that prelabour caesarean section and
caesarean section in first stage result in little change
in bladder neck support. Vaginal delivery, conversely,
in particular operative vaginal delivery, is associated with
a highly significant increase in bladder neck mobility. An
example of markedly increased bladder and urethral
mobility after a vacuum extraction for failure to progress
in second stage is shown in Fig. 2 [27].
There seems to be sufficient proof for the hypothesis that
pelvic organ support can be impaired by vaginal child-
birth. It is unclear whether this effect is due to stretching
or avulsion of structures and whether the observed
changes are primary (i.e. directly due to childbirth) or
the medium-term or long-term consequence of levator
impairment. Several mechanisms may well coexist in one
individual. Risk factors are operative vaginal delivery,
prolonged second stage, and possibly high birth weight.
The extent of such trauma, however, clearly varies from
one person to the next.
Furthermore, it has recently been shown that any deliv-
ery-related changes occur against the background of
marked variations in pelvic organ support in young

530 Urogynecology
Figure 2 Bladder neck mobility on Valsalva manœuvre at 37 weeks (a) and 3 months postpartum (b)
Markedly increased bladder and urethral mobility after a vacuum extraction for failure to progress in second stage. Reproduced with permission from[27].
nulliparous women [28]. As the most significant changes
are observed in those with the least organ mobility
antenatally [29], the effect of childbirth may be a partial
equalization of those interindividual differences. We are
not currently able to distinguish between preexisting or
postpartum (postdelivery) prolapse, but recent develop-
ments hold out promise that this may soon change.
Direct evidence of fascial traumaSeveral attempts have been made to define fascial trauma
after vaginal delivery. In the anterior compartment it
has long been assumed that childbirth may result in dis-
ruption of the ‘endopelvic fascia’, in particular of para-
urethral and paravaginal structures. To date, such attempts
have generally been unsuccessful, although transrectal
three-dimensional or four-dimensional ultrasound using
Figure 3 Comparison of posterior compartment imaging (midsagit
vaginal delivery (b), on maximal Valsalva manœuvre
The anorectal junction appears normal on the left.On the right, there is a rectocoele of a depth ofabout 2 cm, filled with stool. Reproduced withpermission from [30�].
high-frequency transducers may be able to identify the
subvesical part of the endopelvic fascia. Contrary to what
has been surmised in the past, such defects may be
multiple and, analogous to striae gravidarum, too complex
to invite surgical reconstruction.
As opposed to the situation regarding the anterior compart-
ment, posterior compartment prolapse commonly provides
indirect evidence of fascial trauma, due to the distinct
appearances of a ‘true’ rectocoele, which is thought to
represent a defect of the rectovaginal septum or Denon-
villier’s fascia. Analogous to increased bladder descent
after childbirth, there is a highly significant increase in
caudal displacement of the rectal ampulla after childbirth
[27]. In addition, however, it has recently been shown that
vaginal childbirth also results in an increased prevalence of
tal plane) in the third trimester (a) and 3 months after normal

Trauma following vaginal delivery Dietz 531
true rectocoele, i.e. presumptive defects of the rectovagi-
nal septum, and that existing defects seem to grow larger
[30�]. Such defects are strongly associated with symptoms
of pelvic organ prolapse and obstructed defecation [31].
Figure 3 [30�] shows a case of de-novo true rectocoele 3
months after vaginal delivery.
Levator traumaWhat clinicians and physiotherapists call ‘the pelvic floor’
is, for practical purposes, the pubococcygeus–puborecta-
lis complex. This muscle complex forms a V-shaped or
U-shaped sling around the anorectal junction, inserting
on the pelvic sidewall from the pubic rami to the ischial
spine. The levator hiatus, i.e. the space bordered by this
sling, contains the urethra anteriorly, the vagina centrally,
and the anorectum posteriorly (see Fig. 4 [32��] for a
comparison of MRI and ultrasound imaging of the hiatus
in the axial plane).
The area of the levator hiatus in young nulliparous
women varies from 6 to 36 cm2 on Valsalva manœuvre
[33�]. The area of the average fetal head in the plane of
minimal diameters measures 70–90 cm2 (equivalent to a
head circumference of 300–350 mm), requiring marked
distension and deformation of the levator complex. Lien
et al. [34] in Ann Arbor, Michigan, have been able to show
with the help of MRI-based computer modelling that the
most inferior and medial parts of the levator complex may
have to increase in length by a factor of 3 or more during
crowning of the fetal head. Given this degree of acute
distension, it is remarkable that many women seem to go
through childbirth without sustaining major soft tissue
trauma.
Evidence on the effects of childbirth on levator structure
and function is available both from clinical research on
Figure 4 A comparison of magnetic resonance (a) and three-dime
muscle in a 23-year-old nulliparous volunteer
The pelvic floor consists of the pubococcygeus–puborectalis complex, which forms a V-shaped orU-shaped sling around the anorectal junction,inserting on the pelvic sidewall from the pubicrami to the ischial spine. The levator hiatus, i.e. thespace bordered by this sling, contains the urethraanteriorly, the vagina centrally, and the anorectumposteriorly. Reproduced with permission from[32��].
pelvic floor function, usually obtained by physiotherapists,
and from imaging. Several papers over the past decade
have described patterns of injury observed on MRI,
although no comparative study of antepartum and post-
partum levator anatomy has been published to date. From
studies in parous women [35,36], it has been speculated
that the change in the typical H-shaped appearance of the
vagina may be due to traumatic loss of paravaginal supports
unilaterally or bilaterally. Hoyte et al. [37] have shown a
significant decrease in levator muscle volume and
increase in levator hiatus width in women with stress
incontinence and prolapse. Other authors [38] have
attributed abnormalities in density and structure of the
levator ani to childbirth-related trauma.
With the advent of sonographic three-dimensional
imaging techniques, pelvic floor ultrasound is now also
capable of demonstrating both the normal pubococcy-
geus–puborectalis complex and abnormalities seen in
parous women [32��,39,40��]. Recent technologic devel-
opments such as speckle reduction algorithms and tomo-
graphic or multislice imaging have markedly increased
resolutions and now allow quantification of levator trauma
in all dimensions [41] (Figs. 5–8). As a result, four-
dimensional pelvic floor ultrasound now achieves spatial
resolutions similar to or better than MRI in all three
dimensions, while temporal resolutions are markedly
superior to MRI, allowing the real-time observation of
manœuvres.
Presence and extent of levator defects seem to be associ-
ated with symptoms and signs of pelvic organ prolapse,
especially of the anterior and central compartment
[32��,40��,41]. While levator avulsion was observed in
11% of women with normal uterine support, it was found
in 25% of all women with uterine descent and in about
nsional pelvic floor ultrasound (b) imaging of the pubovisceral

532 Urogynecology
Figure 5 A comparison of magnetic resonance (a) and ultrasound (b) imaging in patients with a typical right-sided avulsion injury
(arrows) to the pubovisceral muscle
Reproduced with permission from [40��].
half of those with second-degree or third-degree uterine
prolapse [40��]. There appears to be a link between
levator trauma and worsened or de-novo stress incon-
tinence 3 months postpartum [32��], although this asso-
ciation seems to disappear later in life [40��], an
observation that accords with the fact that epidemiologic
evidence demonstrates much stronger associations
between childbirth and prolapse than between parity
and stress incontinence (Fig. 1). Avulsion of the pubo-
rectalis may be the cause of stress incontinence, or it
may just be a marker for (currently undetectable) trauma
to fascial supports of the urethra and anterior vaginal
wall.
Figure 6 Small unilateral trauma to the left anterior aspect of the
translabial three-dimensional/four-dimensional ultrasound
(a) Image obtained at 37 weeks; (b) 4 monthspostpartum.
Major trauma to the levator ani, as described in Fig. 5
[40��] and Figs 6–8, is palpable and was first described in
1943 [42]. Palpation of the levator ani by physiotherapists
and gynaecologists or urogynaecologists does not cur-
rently include a morphologic assessment, however, and
the digital diagnosis of such defects may require signifi-
cant teaching. In a recent study comparing three-
dimensional ultrasound and levator palpation by a
conventionally trained physiotherapist, agreement bet-
ween the two methods was very poor [43], but another
paper comparing digital assessment by a specifically
trained physician and MRI showed better agreement
[44�].
pubovisceral muscle (asterisk), as seen in the axial plane on
Trauma following vaginal delivery Dietz 533
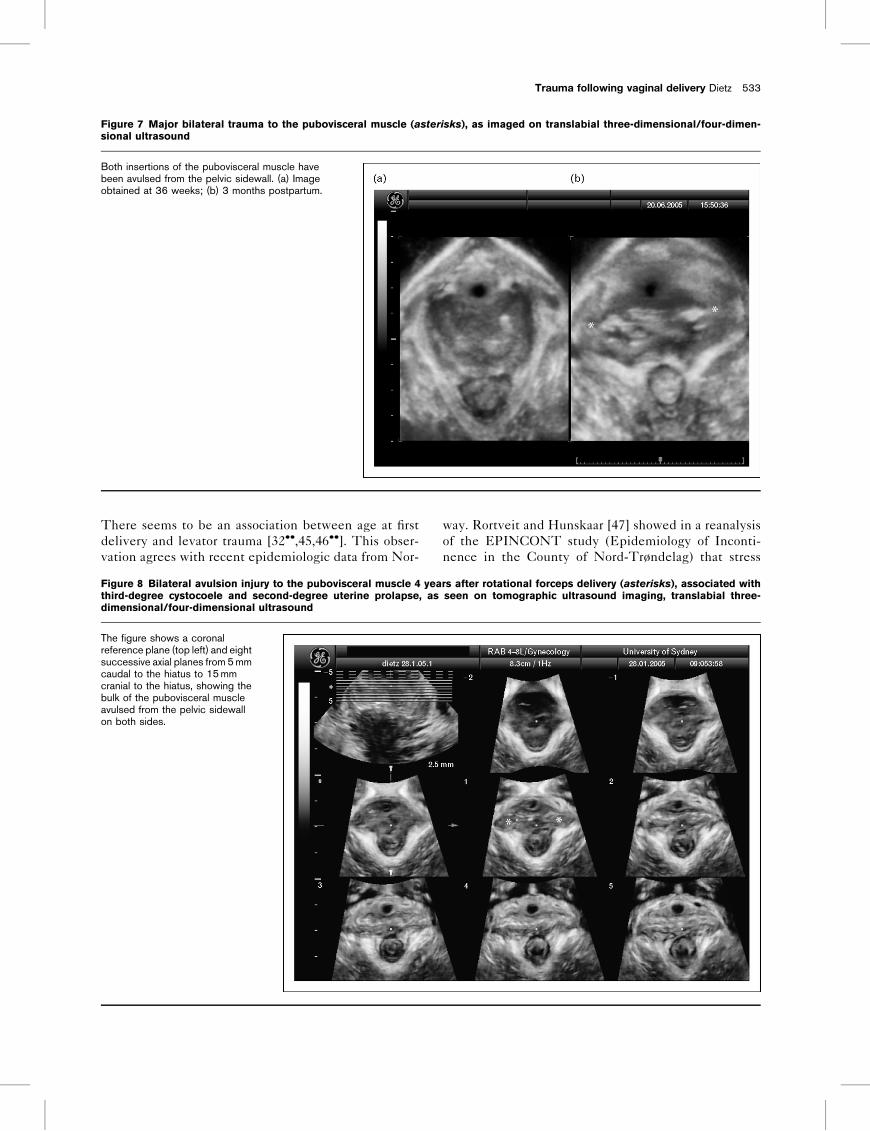
Figure 7 Major bilateral trauma to the pubovisceral muscle (asterisks), as imaged on translabial three-dimensional/four-dimen-
sional ultrasound
Both insertions of the pubovisceral muscle havebeen avulsed from the pelvic sidewall. (a) Imageobtained at 36 weeks; (b) 3 months postpartum.
There seems to be an association between age at first
delivery and levator trauma [32��,45,46��]. This obser-
vation agrees with recent epidemiologic data from Nor-
Figure 8 Bilateral avulsion injury to the pubovisceral muscle 4 yea
third-degree cystocoele and second-degree uterine prolapse, as
dimensional/four-dimensional ultrasound
The figure shows a coronalreference plane (top left) and eightsuccessive axial planes from 5 mmcaudal to the hiatus to 15 mmcranial to the hiatus, showing thebulk of the pubovisceral muscleavulsed from the pelvic sidewallon both sides.
way. Rortveit and Hunskaar [47] showed in a reanalysis
of the EPINCONT study (Epidemiology of Inconti-
nence in the County of Nord-Trøndelag) that stress
rs after rotational forceps delivery (asterisks), associated with
seen on tomographic ultrasound imaging, translabial three-

534 Urogynecology
Figure 9 Hiatal dimensions before (a) and 4 months after vaginal delivery (b) as seen on maximal Valsalva manœuvre in the axial
plane
These images were obtained by translabial four-dimensional ultrasound, with the plane of minimaldimensions identified in the midsagittal plane androtated through 908 to obtain a representation ofthe hiatus in the axial plane. It is evident that hiataldimensions – both diameters and area – areincreased in the postpartum image on the right.
incontinence was more likely in women who had had
their first baby at an older age, a finding that has since
been confirmed by others [48��]. These observations
may have significant public health implications, as in
Western societies the age of primiparae has risen by
about 10 years over the past two generations.
Childbirth does not just affect morphology or macro-
anatomic appearances, it seems to have an effect on
biomechanics as well. Childbirth clearly changes both
dimensions and distensibility of the hiatus [32��,49], as
Figure 10 Appearances on translabial ultrasound, coronal plane, in t
anal sphincter tears
Scars or defects are indicated byasterisks.
shown in Fig. 9, but it is currently unclear whether this is
due to functional or morphologic change.
Anal sphincter traumaAnal sphincter injury is a form of pelvic floor trauma
familiar to all practising obstetricians, and (since it is
generally obvious to the naked eye) there seems little
scope for debating a causal link with childbirth. While
primary repair is undertaken at delivery as a matter of
course, the quality of both detection and repair of
such trauma seems to vary significantly. Anal sphincter
hree women (a–c) 6–8 weeks after primary repair of third-degree

Trauma following vaginal delivery Dietz 535
Figure 11 Appearances on translabial ultrasound of a major fourth-degree tear
(a) Coronal plane and (b) midsagittal plane. EAS,external anal sphincter, IAS, internal anal sphincter.Image courtesy of Dr A. Steensma, Rotterdam.
injuries may well occur more frequently than previously
reported, in up to one-quarter of vaginal deliveries, with
lower estimates due to ineffective intrapartum detection
rather than covered ‘occult’ defects [50�]. The main risk
factor is considered to be instrumental vaginal delivery
[51]. Anal incontinence is common after third-degree
and fourth-degree tears, even if they are recognized and
repaired at the time of injury, and can have a major effect
on a woman’s quality of life. As in other pelvic floor
disorders, however, the condition may be influenced by
several other aetiologic factors such as chronic diarrhoea,
anorectal surgery, cognitive impairment, and neuro-
pathy (either as a result of traumatic childbirth or due
to other causes). Not surprisingly, the strength of the
association between obstetric factors and faecal incon-
tinence varies with the age of the population under
scrutiny [9��]. It seems that many if not most women
remain asymptomatic after anal sphincter injury [52].
Conversely, evidence of old sphincter trauma is found in
more than 70% of women with late-onset faecal incon-
tinence [53].
The anal sphincter is generally imaged by endoanal
ultrasound, using high-resolution probes with a field of
vision of 3608. This method is firmly established as one of
the cornerstones of a colorectal diagnostic workup for anal
incontinence and is covered extensively in the colorectal
and radiologic literature [54–56]. Due to the limited
availability of such probes, obstetricians and gynaecolo-
gists have taken to using high-frequency curved array
probes placed exoanally, i.e. transperineally [57,58,59�] in
the coronal rather than the midsagittal plane.
On exoanal or translabial ultrasound, the external
sphincter appears as an isoechoic to hyperechoic ring
structure, while the internal anal sphincter is hypo-
echoic. Anal sphincter defects appear as a discontinuity
of these ring structures (Figs 10 and 11). In the coronal
plane, defects are conveniently described using a clock
face notation. In the longitudinal plane, sphincter
defects can be described by measuring defect length
relative to total sphincter length.
After repair of third-degree and fourth-degree tears,
ultrasound commonly demonstrates residual defects,
and the extent of such incompletely or inadequately
repaired defects seems associated with decreased
sphincter pressures and an increased risk of anal incon-
tinence [60�]. Figure 10 shows the degree to which
appearances in the coronal plane may vary after primary
repair of third-degree anal sphincter trauma, and Fig. 11
illustrates the potential cranial extent of such trauma.
ConclusionThere is little doubt that some women suffer significant
trauma to pelvic floor structures as a consequence of
(successful or unsuccessful) attempts at vaginal child-
birth. Trauma may affect the pudendal nerve or its
branches, the anal sphincter, the puborectalis–pubococ-
cygeus complex, or pelvic fascial structures. The more
protracted a delivery is and the longer the duration of
second stage, the higher seems the likelihood of ana-
tomic or functional alteration, although some forms of
trauma may also occur as a result of precipitate labour.
Vaginal operative delivery seems to be a risk factor for all
forms of impairment mentioned above, whether inde-
pendently or due to its association with prolonged second
stage. Changes in demographics and obstetric practice
may influence the likelihood of pelvic floor trauma
and future incontinence or prolapse. Ever-increasing
caesarean section rates may ultimately prevent the need
for pelvic floor surgery in some women, but for the next
few decades we are likely to see an increase in the
prevalence of pelvic floor morbidity, especially pelvic
organ prolapse, due to delayed childbearing.
Delivery-related pelvic floor trauma is a reality, not a
myth. It is an entirely different question, however, as to
whether such trauma is common or severe enough to
require a change in clinical practice. Currently, we cannot

536 Urogynecology
be sure whether avoidance of potential intrapartum pel-
vic floor trauma is worth the risk, cost, and effort of
performing an elective caesarean section. In order to
make preventive intervention feasible, we may first have
to learn to identify women most at risk of delivery-related
pelvic floor trauma, and this should be a priority topic for
future research. Ultimately, however, only randomized
controlled trials of planned vaginal birth versus planned
caesarean section, whether in high-risk patients or in an
unselected population, will eventually provide meaning-
ful information to women and their healthcare providers.
References and recommended readingPapers of particular interest, published within the annual period of review, havebeen highlighted as:� of special interest�� of outstanding interest
Additional references related to this topic can also be found in the CurrentWorld Literature section in this issue (pp. 577–578).
1 Fisk NM. Caesarean section for all patients? In: Ben-Rafael Z, Lobo R,Shoham Z, editors. Controversies in obstetrics, gynaecology and infertility.Bologna: Monduzzi Editore; 2002. pp. 111–115.
2 Minkoff H, Chervenak FA. Elective primary cesarean delivery. N Engl J Med2003; 348:946–950.
3 MacLennan AH, Taylor AW, Wilson DH, Wilson PD. The prevalence of pelvicfloor disorders and their relationship to gender, age, parity and mode ofdelivery. Br J Obstet Gynaecol 2000; 107:1460–1470.
4 Rortveit G, Daltveit AK, Hannestad YS, et al. Urinary incontinence aftervaginal delivery or cesarean section. N Engl J Med 2003; 348:900–907.
5
��DeLancey J. The hidden epidemic of pelvic floor dysfunction: achievable goalsfor improved prevention and treatment. Am J Obstet Gynecol 2005; 192:1488–1495.
Excellent overview of the current situation as regards the epidemiology of pelvicfloor dysfunction and a bold outline of future research priorities.
6 Mant J, Painter R, Vessey M. Epidemiology of genital prolapse: observationsfrom the Oxford Family Planning Association Study. Br J Obstet Gynaecol1997; 104:579–585.
7 Tegerstedt G, Miedel A, Maehle-Schmidt M, et al. Obstetric risk factors forsymptomatic prolapse: a population-based approach. Am J Obstet Gynecol2006; 194:75–81.
8 Hannah ME, Hannah WJ, Hodnett ED, et al. Outcomes at 3 months afterplanned cesarean vs planned vaginal delivery for breech presentation at term:the international randomized Term Breech Trial. JAMA 2002; 287:1822–1831.
9
��MacArthur C, Glazener C, Lancashire R, et al. Faecal incontinence and modeof first and subsequent delivery: a five year longitudinal study. Br J ObstetGynaecol 2005; 112:1075–1082.
Outstanding longitudinal observational study with detailed obstetric data fromseveral centers in the UK and New Zealand.
10 Assassa P, Dallosso HM, Perry SI, et al. The association between obstetricfactors and incontinence: a community survey [abstract]. Br J ObstetGynaecol 2000; 107:822.
11 Eason E, Labrecque M, Marcoux S, Mondor M. Anal incontinence afterchildbirth. CMAJ 2002; 166:326–330.
12 Groutz A, Fait G, Lessing JB, et al. Incidence and obstetric risk factors ofpostpartum anal incontinence. Scand J Gastroenterol 1999; 34:315–318.
13 Snooks SJ, Swash M, Mathers SE, Henry MM. Effect of vaginal delivery on thepelvic floor: a 5-year follow-up. Br J Surg 1990; 77:1358–1360.
14 Allen RE, Hosker GL, Smith AR, Warrell DW. Pelvic floor damage andchildbirth: a neurophysiological study. Br J Obstet Gynaecol 1990; 97:770–779.
15 Vodusek DB, Fowler CJ. Electromyography. In: Cardozo L, Staskin D, editors.Textbook of female urology and urogynaecology, 1st ed London: Isis MedicalMedia; 2001. pp. 240–250.
16 Shafik A, El-Sibai O. Study of the levator ani muscle in the multipara: role oflevator dysfunction in defecation disorders. J Obstet Gynaecol 2002; 22:187–192.
17 Marshall K, Walsh DM, Baxter GD. The effect of a first vaginal delivery on theintegrity of the pelvic floor. Clin Rehabil 2002; 16:795–799.
18 Gregory WT, Lou JS, Stuyvesant A, Clark AL. Quantitative electromyographyof the anal sphincter after uncomplicated vaginal delivery. Obstet Gynecol2004; 104:327–335.
19 Bump RC, Mattiasson A, Bo K, et al. The standardization of terminology offemale pelvic organ prolapse and pelvic floor dysfunction. Am J ObstetGynecol 1996; 175:10–17.
20 Swift SE. The distribution of pelvic organ support in a population of femalesubjects seen for routine gynecologic health care. Am J Obstet Gynecol2000; 183:277–285.
21 Dannecker C, Lienemann A, Fischer T, Anthuber C. Influence of spontaneousand instrumental vaginal delivery on objective measures of pelvic organsupport: assessment with the pelvic organ prolapse quantification (POPQ)technique and functional cine magnetic resonance imaging. Eur J ObstetGynecol Reprod Biol 2004; 115:32–38.
22 Dietz HP, Clarke B, Vancaillie TG. Vaginal childbirth and bladder neckmobility. Aust N Z J Obstet Gynaecol 2002; 42:522–525.
23 Dietz H, Eldridge A, Grace M, Clarke B. Does pregnancy affect pelvic organmobility? Aust N Z J Obstet Gynaecol 2004; 44:517–520.
24 Meyer S, Schreyer A, De Grandi P, Hohlfeld P. The effects of birth on urinarycontinence mechanisms and other pelvic-floor characteristics. Obstet Gyne-col 1998; 92 (4 Pt 1):613–618.
25 Peschers U, Schaer G, Anthuber C, et al. Changes in vesical neck mobilityfollowing vaginal delivery. Obstet Gynecol 1996; 88:1001–1006.
26 Wijma J, Weis Potters AE, de Wolf BT, et al. Anatomical and functionalchanges in the lower urinary tract following spontaneous delivery. Br J ObstetGynaecol 2003; 110:658–663.
27 Dietz HP, Bennett MJ. The effect of childbirth on pelvic organ mobility. ObstetGynecol 2003; 102:223–228.
28 Dietz H, Eldridge A, Grace M, Clarke B. Pelvic organ descent in youngnulliparous women. Am J Obstet Gynecol 2004; 191:95–99.
29 Dietz HP, Steensma AB. Which women are most affected by delivery-relatedchanges in pelvic organ mobility? Eur J Obstet Gynecol Reprod Biol 2003;111:15–18.
30
�Dietz HP, Steensma AB. The role of childbirth in the aetiology of rectocele. Br JObstet Gynaecol 2006; 113:264–267.
First direct evidence on the role of childbirth in the aetiology of rectocoele.
31 Dietz HP, Korda A. Which bowel symptoms are most strongly associated witha true rectocele? Aust N Z J Obstet Gynaecol 2005; 45:505–508.
32
��Dietz H, Lanzarone V. Levator trauma after vaginal delivery. Obstet Gynecol2005; 106:707–712.
This small observational study in women 2–4 weeks before and 2–6 months afterchildbirth provides direct proof for the hypothesis that childbirth is responsible forcertain morphologic abnormalities observed in parous women and suggests thatolder age at first delivery is a risk factor for such trauma.
33
�Dietz H, Shek K, Clarke B. Biometry of the pubovisceral muscle and levatorhiatus by three-dimensional pelvic floor ultrasound. Ultrasound ObstetGynecol 2005; 25:580–585.
First description of translabial three-dimensional pelvic floor ultrasound as a tool toassess biometric indices of the levator ani muscle and hiatus.
34 Lien KC, Mooney B, DeLancey JO, Ashton-Miller JA. Levator ani musclestretch induced by simulated vaginal birth. Obstet Gynecol 2004; 103:31–40.
35 Klutke C, Golomb J, Barbaric Z, Raz S. The anatomy of stress incontinence:magnetic resonance imaging of the female bladder neck and urethra. J Urol1990; 143:563–566.
36 Huddleston H, Dunnihoo D, Huddleston P, Meyers P. Magnetic resonanceimaging of defects in DeLancey’s vaginal support levels I, II, and III. Am JObstet Gynecol 1995; 172:1778–1782.
37 Hoyte L, Schierlitz L, Zou K, et al. Two- and 3-dimensional MRI comparison oflevator ani structure, volume, and integrity in women with stress incontinenceand prolapse. Am J Obstet Gynecol 2001; 185:11–19.
38 Tunn R, DeLancey JO, Howard D, et al. MR imaging of levator animuscle recovery following vaginal delivery. Int Urogynecol J 1999; 10:300–307.
39 Dietz H. Ultrasound imaging of the pelvic floor: 3D aspects. UltrasoundObstet Gynecol 2004; 23:615–625.
40
��Dietz H, Steensma A. The prevalence of major abnormalities of the levatorani in urogynaecological patients. Br J Obstet Gynaecol 2006; 113:225–230.
First ultrasound study to estimate the prevalence of levator avulsion injury insymptomatic women and the first to show an association between such traumaand pelvic organ prolapse.
41 Dietz HP. The classification of major morphological abnormalities of thepubovisceral muscle. Neurourol Urodyn; 2006; 25 In press.

Trauma following vaginal delivery Dietz 537
42 Gainey HL. Postpartum observation of pelvic tissue damage. Am J ObstetGynecol 1943; 46:457–466.
43 Dietz H, Hay-Smith E, Hyland G. Vaginal palpation and 3D pelvic floorultrasound in the diagnosis of avulsion defects of the levator ani. NeurourolUrodyn. 2006; 25 In press.
44
�Kearney R, Miller JM, Delancey JO. Interrater reliability and physical examina-tion of the pubovisceral portion of the levator ani muscle: validity comparisonsusing MR imaging. Neurourol Urodyn 2006; 25:50–54.
This paper demonstrates that levator trauma identified on imaging can be palpatedvaginally, although palpation requires significant training and may underestimatethe extent of trauma.
45 Dietz HP. Does delayed childbearing increase the risk of levator injury inlabour? Neurourol Urodyn. 2006;25 In press.
46
��Kearney R, Miller J, Ashton-Miller J, Delancey J. Obstetric factors associatedwith levator ani muscle injury after vaginal birth. Obstet Gynecol 2006;107:144–149.
This paper investigates obstetric risk factors for levator trauma and confirms thatolder age at first delivery seems to be a risk factor.
47 Rortveit G, Hunskaar S. The association between the age at the first and lastdelivery and urinary incontinence. Neurourol Urodyn 2004; 23 (5/6):562–563.
48
��S Glazener CM, Herbison GP, MacArthur C, et al. New postnatal urinaryincontinence: obstetric and other risk factors in primiparae. BJOG 2006;113:208–217.
Another outstanding paper that has arisen from the study mentioned in MacArthuret al. (Br J Obstet Gynaecol 2005; 112:1075–1082).
49 Steensma AB, Dietz H. 3D pelvic floor ultrasound in the assessment of thelevator ani muscle complex [abstract]. Ultrasound Obstet Gynecol 2004;24:258.
50
�Andrews A, Sultan A, Thakar R, Jones P. Occult anal sphincter injuries: mythor reality? Br J Obstet Gynaecol 2006; 113:195–200.
A very interesting study suggesting that ‘occult’ anal sphincter injuries are gen-erally visible on diligent examination and that previous low prevalence estimates foranal sphincter injuries are due to our failure to detect sphincter trauma.
51 Sultan AH, Kamm MA, Hudson CN, et al. Anal sphincter disruption duringvaginal delivery. N Engl J Med 1993; 329:1905–1911.
52 Oberwalder M, Connor J, Wexner SD. Meta-analysis to determine theincidence of obstetric anal sphincter damage. Br J Surg 2003; 90:1333–1337.
53 Oberwalder M, Dinnewitzer A, Baig MK, et al. The association between late-onset fecal incontinence and obstetric anal sphincter defects. Arch Surg2004; 139:429–432.
54 Williams AB, Bartram CI, Halligan S, et al. Alteration of anal sphinctermorphology following vaginal delivery revealed by multiplanar anal endo-sonography. Br J Obstet Gynaecol 2002; 109:942–946.
55 Gold DM, Bartram CI, Halligan S, et al. Three-dimensional endoanal sono-graphy in assessing anal canal injury. Br J Surg 1999; 86:365–370.
56 Frudinger A, Bartram CI, Halligan S, Kamm M. Examination techniques forendosonography of the anal canal. Abdom Imaging 1998; 23:301–303.
57 Peschers UM, DeLancey JO, Schaer GN, Schuessler B. Exoanal ultrasound ofthe anal sphincter: normal anatomy and sphincter defects. Br J ObstetGynaecol 1997; 104:999–1003.
58 Timor-Tritsch IE, Monteagudo A, Porges RF, Santos R. Simple ultrasoundevaluation of the anal sphincter in female patients using a transvaginaltransducer. Ultrasound Obstet Gynecol 2005; 25:177–183.
59
�Yagel S, Valsky DV. Three-dimensional transperineal sonography for evalua-tion of the anal sphincter complex: another dimension in understandingperipartum sphincter trauma. Ultrasound Obstet Gynecol 2006; 27:119–123.
Interesting paper describing the use of three-dimensional pelvic floor ultrasoundfor the assessment of anal sphincter tears.
60
�Starck M, Bohe M, Valentin L. The extent of endosonographic anal sphincterdefects after primary repair of obstetric sphincter tears increases over timeand is related to anal incontinence. Ultrasound Obstet Gynecol 2006;27:188–197.
Important longitudinal study showing that most women show evidence of residualsphincter defects after repair and that the extent of such defects is associated withcontractile function and symptoms of anal incontinence.


















