
PEGS, palliation and planning: Issues in caring for people with advanced MS
77
PEGS, palliation and planning: issues in caring for people with advanced MS Jonathan Martin Consultant in Palliative Medicine and Clinical Lead Camden, Islington Elipse, UCLH & HCA Palliative Care Team November 2015
-
Upload
ms-trust -
Category
Healthcare
-
view
419 -
download
0
Transcript of PEGS, palliation and planning: Issues in caring for people with advanced MS
PEGS, palliation and planning:
issues in caring for people with
advanced MS
Jonathan Martin Consultant in Palliative Medicine and Clinical Lead
Camden, Islington Elipse, UCLH & HCA Palliative Care Team
November 2015
Outline
Introduction:
• The palliative care approach
• The legal and ethical basis for palliation and planning
• Palliative issues in MS
Advance care planning:
• Advance decisions to refuse treatment
• Common issues with writing an ADRT
• On the receiving end: what to do when faced with an advance care plan

Objectives
By the end of this session you will:
• Understand some of the general issues that make advance care planning so challenging
• Be able to outline some of the specific issues with regard to advance care planning in MS

THE PALLIATIVE CARE
APPROACH: CONTEXTS AND
MEANINGS

Palliative Care
“Is patient and family-centred care that optimizes quality of life by anticipating, preventing and treating suffering.
Palliative care throughout the continuum of illness involves addressing physical, intellectual, emotional, social and spiritual needs and facilitates patient autonomy, access to information and choice.”
Dahlin C (ed) 3rd edition - www.nationalconcensusproject.org

Palliative Care
• Addressing suffering and healing George R Palliat Med 2009
• Integrating “biological realities with profound human needs for meaning, comfort and direction”
Kaldjian L et al. Am J Hospice & Palliat Care 2009
Through physical, psychological, social and spiritual care.
Not just end of life care
• Palliative care may be involved in the care of someone with life-limiting illness, regardless of how close to death they are.
• However, “palliative care” is often a hard-sell with patients early in their disease process, since it is often misunderstood to be only about end of life care
The wider cultural context of dying and death
“For the anonymous anyone, death is a fact of life and entirely unobjectionable. For the loved one, it is an offense, and for oneself it is unthinkable.”
“We have eminently good reasons for avoiding the matter altogether. It is the most disagreeable of subjects at the same time that it is inescapable…”
Fairfield P Death: a philosophical inquiry 2015

LEGAL BASIS FOR
PALLIATION AND PLANNING
Mental Capacity Act (2005)
• This is legislation developed over a period of several years after the Anthony Bland case heard by the Law Lords in 1993.
• Advance care planning has its basis in the MCA.

Life-prolonging treatments
• Following established ethical and legal (including human rights) principles, decisions concerning potentially life-prolonging treatment must not be motivated by a desire to bring about the patient’s death, and must start from a presumption in favour of prolonging life.
• However, there is no absolute obligation to prolong life irrespective of the consequences for the patient, and irrespective of the patient’s views, if they are known or can be found out.
GMC. Treatment and care towards the end of life: good practice in decision making, 2010
The ethics of withdrawing or withholding treatment
• Primary aim of starting a treatment is to provide a health benefit to the patient.
• The same justification applies to continuing a treatment already started.
• Psychologically may be easier to withhold a treatment than to withdraw it:
– Significant message may be contained within withdrawal (“giving up”)
– Withdrawal is a public act
– But no legal or moral distinction between the two in this case
– Withdrawing may be easier if treatment explicitly initiated to assess for benefit (a treatment trial)

Problems with treatment withdrawal ending in death
• Some members of the healthcare team… may find it more difficult to contemplate withdrawing a life-prolonging treatment than to decide not to start the treatment in the first place. This may be because of the emotional distress that can accompany a decision to withdraw life-prolonging treatment, or because they would feel responsible for the patient’s death.
• However, you should not allow these anxieties to override your clinical judgement…
GMC. Treatment and care towards the end of life:
good practice in decision making, 2010

“[T]he principle of self-determination requires that respect must be given to the wishes of the patient, so that if an adult of sound mind refuses, however unreasonably, to consent to treatment or care by which his life would or might be prolonged, the doctors responsible for his care must give effect to his wishes, even though they do not consider it to be in his best interests to do so… To this extent, the principle of the sanctity of human life must yield to the principle of self-determination…and…the doctors’ duty to act in the best interests of his patient must likewise be qualified… Moreover the same principle applies where the patient’s refusal to give his consent has been expressed at an earlier date, before he became unconscious or otherwise incapable of communicating it…”
Goff L. Airedale NHS Trust v Bland {1993} 2 WLR 316
When treatment refusal ends in death
Example: Ms B
• Vascular abnormality of the high cervical cord resulted in tetraplegia and ventilator dependence.
• The patient requested that mechanical ventilation be discontinued.
• On Application the Court confirmed the patient's mental competence and the validity of the refusal of treatment.
• Damages were awarded to the patient for civil assault, in failing to discontinue treatment when requested.
Ms B v An NHS Hospital Trust [2002]

Is this suicide?
Suicide Act 1961
• A person who aids, abets, counsels or procures the suicide of another, or an attempt by another to commit suicide, shall be liable on conviction on indictment to imprisonment for a term not exceeding 14 years
Refusal of treatment is not suicide
“I wish to add that, in cases of this kind, there is no question of the patient having committed suicide, nor therefore of the doctor having aided or abetted him in doing so….
It is simply that the patient has, as he is entitled to do, declined to consent to treatment which might or would have the effect of prolonging his life…”
Lord Goff in Airedale NHS Trust v Bland [1993] AC 789;
quoted in Ms B v An NHS Trust
When the patient asks for treatment withdrawal
Criminal battery
• “The law requires that an adult patient who is mentally and physically capable of exercising choice must consent if medical treatment of him is to be lawful...
Treating him without his consent or despite a refusal of consent will constitute the civil wrong of trespass to the person and may constitute a crime.”
Per Ld Donaldson MR in re T [1993] 3 Med LR p307
PALLIATIVE ISSUES IN MS
Palliation issues in the supportive phase
• Prognostic uncertainty – Initially issues are frequently more psychological than physical
– Focus on maintaining function and preserving well-being
• The importance of teamwork
• Information
• Consider our relationship with complementary practitioners
• Site of care
Maddocks I et al. Palliative Neurology, Cambridge; CUP: 2006
Common symptoms
• Bladder dysfunction
• Fatigue
• Impairment of movement
• Pain and sensory disturbances
• Bowel dysfunction
• Sexual impairment
• Affective disorders
Maddocks I et al. Palliative Neurology, Cambridge; CUP: 2006

Palliation issues in the terminal phase
The aim of treatment shifts from maximising function to minimising suffering and aiming for the patient’s comfort & dignity. Common problems:
• Motor impairments: weakness, wasting, contractures
• Cognitive impairments: memory loss, poor concentration
• Psychological changes: mood lability, depression
• Skin care: pressure areas due to inadequate nutrition and immobility
• Bowel management
• Swallow impairment: inadequate nutrition
• Medication administration Maddocks I et al. Palliative Neurology, Cambridge; CUP: 2006
These problems become more common as the MS advances, but even so some very disabled patients may live for years.
Campbell C et al. Clin Med 2010
End of life care
Death in MS is commonly related to:
• Respiratory problems: infection, aspiration pneumonia, PE
• Renal problems: failure, UTI
• Falls: hip fracture
• Pressure areas: sepsis
• Suicide Maddocks I et al. Palliative Neurology, Cambridge; CUP: 2006
Most MS patients die in hospital Campbell C et al. Clin Med 2010
INTRODUCTION TO ADVANCE CARE PLANNING
What is ACP?
Advance Care Planning (ACP) has been defined as a process of formal decision making that aims to help patients establish
decisions about future care which take effect when they lose capacity
Hayhoe B et al. Br J Gen Pract 2011

Ad
van
ce
Care
Pla
nn
ing
ACP is about the patient expressing their choices and
protecting those choices if incapacity later occurs. There
are a number of ways of doing this:
Advance Decisions to Refuse Treatment
Advance Statement of Wishes (priorities,
values, preferences)
Lasting Power of Attorney
Nominate someone to be consulted (or
someone who must not be consulted)
Preferred priorities of care / Preferred
place of death
ADVANCE STATEMENT OF
WISHES
Advance Statements of Wishes
• These are wide-ranging “requesting” statements about preferences for future care or treatment and may be very useful to carers.
• Advance Statements might include: – The individual’s concerns.
– Their important values or personal goals for care.
– Their understanding about their illness and prognosis.
– Their preferences for types of care or treatment that may be beneficial in the future.
• How much detail? How can this be captured?
ADVANCE DECISION TO
REFUSE TREATMENT
What is an Advance Decision to Refuse Treatment?
• Advance
• Decision
to
• Refuse
• Treatment

What is an Advance Decision to Refuse Treatment?
• Advance
– Written ahead of time, when the person still had capacity to make the decision in question.
What is an Advance Decision to Refuse Treatment?
• Advance
• Decision
– A choice that is to apply when the person can no longer make their wishes known in other ways i.e. when the person no longer has capacity to make that decision.
– An ADRT is decision-specific i.e. it has to specify both the decision and the circumstances in which it is to apply.
What is an Advance Decision to Refuse Treatment?
• Advance
• Decision
to
• Refuse
– ADRTs are only about refusals, not about demands or requests.
– Some things cannot be refused by ADRT
What is an Advance Decision to Refuse Treatment?
• Advance
• Decision
to
• Refuse
• Treatment
– It is principally about medical and some nursing treatments.
– It is not about place of care.

What things are outside the scope of an advance decision?
• Nothing currently illegal is permissible with an ADRT eg euthanasia
• ADRT cannot be used to refuse basic comfort and care (pain relief, shelter, warmth, nursing care such as washing and mouth care)
• Nor to refuse the offer of food and drink by mouth
• Cannot be used to demand specific forms of treatment
• Mental Health Act overrides (except ECT from November 2008)
PROS AND CONS OF ACP

Benefit of ACP for patients
Mixed evidence in the general literature, almost no MS-specific literature
Several early studies showed no benefit: • RCT found no difference between advance planning and control groups
for psychological & health outcomes and medical treatments (Schneiderman LJ et al. Ann Intern Med 1992;117:599-606)
• Controlled trial of the impact of combining improved communication about resuscitation preferences with information on prognosis found no
improvement in the quality of end of life care (The SUPPORT Principal
Investigators. JAMA 1995)
Benefit of ACP for patients
More recent studies have found limited benefits: • Opportunity to prepare for future is valued (Detering KM et al. BMJ, 2010)
• Care consistent with wishes (Mack JW et al. J Clin Oncol 2010)
• Many patients can hope for things other than cure, and find ACP empowering (Curtis JR et al. J Palliat Med 2008)
• Increased sense of control/hope (NEoLC Programme; Poppe et al. PLoS, 2013)
• Avoid interventions patient wouldn’t want (Molloy et al. JAMA, 2000)
• Avoid waste of resources (reduced hospital admissions) (Abel J et al. BMJ Support Palliat Care, 2013; Robinson L et al. Age Ageing 2012)
The burden on families where no ACP has been undertaken
• Evidence from dementia studies show that families may feel guilty about, and be burdened by, proxy decision making: – Carers find making decisions on behalf of the patient difficult,
especially around areas such as care homes, legal matters and end of life care (Livingston G et al. BMJ, 2010)
– Feelings such as a sense of guilt and failure when a person with dementia was placed in long term care, together with a lack of information about disease/prognosis, left family carers unprepared to make effective decisions about EOLC (Forbes et al. J Nurs Scholarship, 2000)
Benefit of ACP for families
• May help to resolve family conflict (Poppe et al. PLoS, 2013)
• May help families to prepare for the death of a loved one (Poppe et al. PLoS, 2013)
• Increased satisfaction of bereaved carers (Rhee JJ et al. Fam Pract, 2013.
Detering KM et al. BMJ, 2010)
• May help with bereavement and lead to lower levels of psychological morbidity (NEoLC Programme. Rhee JJ et al. Fam Pract, 2013.
Detering KM et al. BMJ, 2010)
Potential harms for patients
• ACP discussions involve thinking about deterioration and death (Barnes, 2007) – This may be too distressing for some patients – Cultural sensitivities – Give rise to conflict within families (Rhee, 2013)
• Common decision-making problems that may lead to “decision regret” include: – Self-doubt – Conflicting interests – Family recriminations – Bureaucratic insensitivity
(Regret Theory is a model of choice under uncertainty)
ACP may promise more than it can deliver
• We may in danger of implying that ACP extends the person’s autonomy exactly as if they retained capacity, but this is only true in a limited sense: a clinician still has to decide whether the circumstances envisaged in an ADRT have materialised
• May give an “illusion of certainty” about what the future holds (Brett AS. JAMA, 1991)
• Cannot fulfil every wish: some requests are too nuanced to be practically ‘captured’
• ‘False promise’ – limited resources or practicalities of caring for a person may mean that it is not possible to support their advance wishes e.g. to remain at home

ACP may promise more than it can deliver
• Lack of robust, long term outcomes data mean that it is still unclear whether ACP is a flawed concept or whether execution of ACP has been flawed (Perkins HS. Ann Intern Med, 2007)
• Inaccessibility of ACP decisions to clinicians or carers – The added value of completing an advance directive (AD) is
marginal if it cannot be accessed when needed • Needs to be shared (Randall F. Br J Hosp Med, 2011; Lorenz KA et al. Ann Intern
Med, 2008)
• Use of electronic medical records may change this (CmC)
Potential barriers for healthcare professionals
• Most patients expect their HCPs to raise issues of ACP (Barnes K et al. Palliat Med 2007; Kahana B et al. J Am Geriatr Soc, 2004)
– But HCPs may be unprepared, unmotivated (Lo B et al. Arch Intern Med, 2004) or daunted by the task, which may “bring death into full view” (Barnes, 2007)
– They may worry that honesty about prognosis will cause undue distress or destroy hope (Barnes, 2007)
• Time intensive: – Patients may need a lot of time to think and reflect, so ACP process
may extend over a number of conversations (RCP et al. Advance care planning. Concise Guidance to Good Practice series, No 12, 2009; Barnes, 2007).
•One study: 60 minutes over 1-3 conversations (Detering, 2010)
Disagreement about who should undertake this work
• Not enough professionals see it as their role to facilitate ACP • In favour of primary care (RCP, 2009; Seamark D et al. Prim Care Respir J, 2012)
• Know patient • Holistic perspective • Coordination of care • Excellent communication • And hospital not always a suitable environment
• Against primary care • Need to know what is likely to occur so should be undertaken by
those with specialist skills and experiences (Robinson L et al. Palliat Med, 2013)

BARRIERS TO ACP THAT ARISE FROM COGNITIVE BIASES
Thinking about your own death is unpleasant and stressful at best, so the benefits of an AD must be viewed as substantial in order to be sufficiently motivating

Cognitive bias
• A cognitive bias is a pattern of deviation in judgment, whereby inferences about other people and situations may be drawn in an illogical (“irrational”) fashion. Individuals create their own “subjective social reality” from their perception of the input, which may have implications for clinical judgements.

Cognitive biases, and other barriers, that may prevent patients from undertaking ACP
• Difficulty projecting yourself into the future (affective forecasting errors or projection bias) – “The hardest thing… is to really, deeply believe that we or our loved
ones will die” (Henig RM. New York Times, 2005)
– People with dementia had “difficulty considering their future selves” (Dening HK et al. Palliat Med, 2012)
• People have a tendency to stick with the default option (Halpern, 2012)
– Often this will be for more aggressive care
• Or they see ACP as irrelevant to them (Schickedanz AD et al. J Am Geriatr Soc, 2009)
Cognitive biases and other barriers
• Tendency is to discount future benefits (optimism bias) so as to avoid present pains (Halpern, 2012)
– Although this may not always be the case: some have a tendency to catastrophise at diagnosis and before they have ‘lived with’ the relevant disease for long

Cognitive biases and other barriers
• The frequently emphasised benefit of ACP to a person’s future ‘autonomy’ may be misaligned with the patients’ priorities (Halpern, 2012)
– Exaggeration of this single feature, compared to other benefits of ACP, by clinicians may produce a focusing illusion
– But the issues that patients consider most pressing (present-biased preferences) tend to be: • Those arising from direct experience (Levi BH et al. Am J Hosp Palliat Care 2010; Piers RD et al.
Patient Educ Couns 2013)
• Those arising out of concern for carers: the wish to protect loved ones from the burdens of future decision making without adequate guidance (Pautex S et al.. Palliat Med 2008)

Cognitive biases and other barriers
• Patients may believe that they can obtain control without use of an AD. In one study approx 90% of people believe that a loved one “knows what I want” (Seckler AB. Ann Intern Med, 1991)
– In reality significant numbers of family/carers do not know (Shalowitz DI et al. Arch Intern Med, 2006; Dening, 2012)
• Dening study (2012) details the wishes of carers over-riding patient preferences
– This may be partly based in an optimism for future life events eg smokers who believe they will not suffer the effects of smoking • Providing data does not help! • But ADs might

Cognitive biases and other barriers
• Patient’s perceptions that :
– They have insufficient information – The HCPs’ time constraints
(Schickedanz AD et al. J Am Geriatr Soc, 2009)
Advance care planning in couples
• One interview study of couples in which one partner had MS found that those most likely to make advance care plans:
– Had a desire to make decisions ahead of time
– Worked in a healthcare field
– Life-threatening health event for the care giving partner.
• Couples that had not discussed plans:
– Had diminished quality of communication between partners
– Were hoping for a cure.
• Findings suggest that providers may need to assess quality of communication between partners, as strained communication may negatively affect the process of informed health care decision making.
Chen H et al. J Neurosci Nurs 2013
AN APPROACH TO ADVANCE CARE PLANNING
“This world is above all a practical and moral one in which patients have life projects, everyday concerns, things ‘at stake’”
Mattingly C Healing dramas and clinical plots: The narrative structure of experience 1998
“Highly individual nature of preferences and needs of patients and relatives regarding information, involvement and communication about EOL care”.
Andreassen P et al. BMJ Support Palliat Care 2015

ACP issues in MS
• ACP would seem to be very relevant to someone facing a prolonged, variable but often progressively downhill course, in which cognitive impairment may prevent full participation in important decisions.
• But it may be difficult to anticipate and therefore plan for future outcomes, and individuals often die of unanticipated acute events
• On the other hand ACP guidance can make difficult decisions easier for families

Initiating an ACP conversation
• Knowing when to initiate a conversation – Needs to be while the patient retains mental capacity for
relevant decisions, but likely not at diagnosis
– Acceptance of diagnosis
– Acceptance of the need to make plans
– Wishes change over time (Response shift, Prospect theory)
– Problem of cognitive impairment later in the disease
• What are the particular issues facing MS patients?

Initiating the conversation (Mullick A et al. BMJ, 2013)
• Examples: – How have you been coping with your illness recently?
– Do you like to think about or plan for the future?
– When you think of the future, what do you hope for? (Pantilat S, Steimle A.
JAMA, 2004)
– When you think about the future, what worries you the most? (Pantilat
S, Steimle A. JAMA, 2004)
– Have you given any thought to what kinds of treatment you would want (and not want) if you became unable to speak for yourself? (Quill
T. JAMA, 2000)
– What do you consider your quality of life to be like now? (Quill T. JAMA,
2000)

Knowing when not to undertake an ACP conversation
• Having the courage of our convictions that even initiating such a discussion would be unwelcome intrusion at that particular time
• Or recognising that our relationship with the patient is not at a stage when ACP can be discussed
Process v. outcome
• My view is that the ACP process is more important than outcome. – Need for careful, sensitive conversations that avoid a ‘tick box’
approach
• But the outcome is also important

WRITING AN ADRT

Writing an ADRT
Task:
• The patient is a 62 year old woman with MS who tells you that she doesn’t want “anything”.
– What else might come under the heading of “anything”?

Writing an ADRT
Task:
• Working in pairs, start to write an ADRT, either:
– Your patient does not want to have a PEG inserted.
– Your patient does not want antibiotics for a chest infection.
– For this task please assume that you have already had the relevant discussions with the patient.

The ADRT special case
• The Mental Capacity Act (2005) states that an advance decision to refuse life-sustaining treatment is a special case
• Additional legal requirements: – The ADRT must be written
– Must state that it is to apply even if the patient’s “life is at risk as a result”
– Must be signed
– Signature must be witnessed • Witness is not testifying to capacity
What is life-sustaining treatment?
• The MCA states that this is a treatment which a healthcare professional, who is providing care to the person ,regards as necessary to sustain life – Not just the type of treatment, but the circumstances also
My approach
a. Recognise that it is not always possible to capture every nuance of a patient’s wishes
b. Keep the language simple and concise
c. Make the intention of the treatment the ‘decision point’ focus, not the outcome (we cannot know the outcome, we can only know what a treatment is intended to achieve) and not the route of administration
d. Balance refusals with additional information elsewhere in the document

ON THE RECEIVING END
(1) Advance decisions to refuse treatment
• A 71 year old lady with MS is admitted with a chest infection. Her ADRT, written four years previously, states that she does not wish to be treated with antibiotics, but her daughter is insisting that the infection is treated.

Issues and responses
• What is her capacity now?
• Validity and applicability of ADRT
– Does the ADRT actually exist?
– Aside: There are issues of personhood (is this the same “person” who wrote the document?)
• Otherwise best interests decision
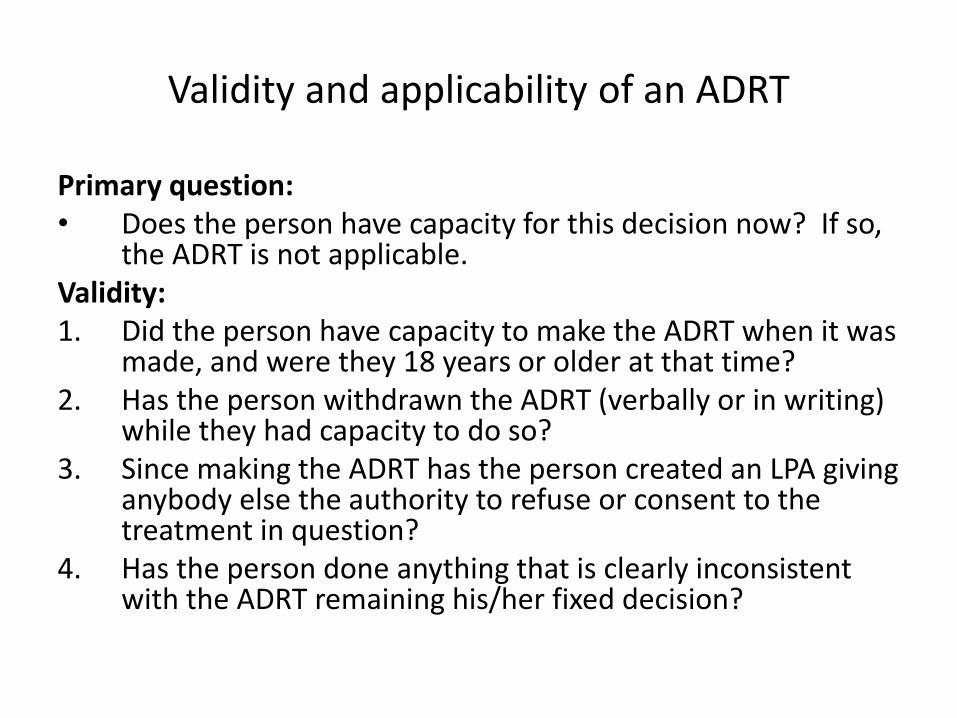
Validity and applicability of an ADRT
Primary question: • Does the person have capacity for this decision now? If so,
the ADRT is not applicable. Validity: 1. Did the person have capacity to make the ADRT when it was
made, and were they 18 years or older at that time? 2. Has the person withdrawn the ADRT (verbally or in writing)
while they had capacity to do so? 3. Since making the ADRT has the person created an LPA giving
anybody else the authority to refuse or consent to the treatment in question?
4. Has the person done anything that is clearly inconsistent with the ADRT remaining his/her fixed decision?
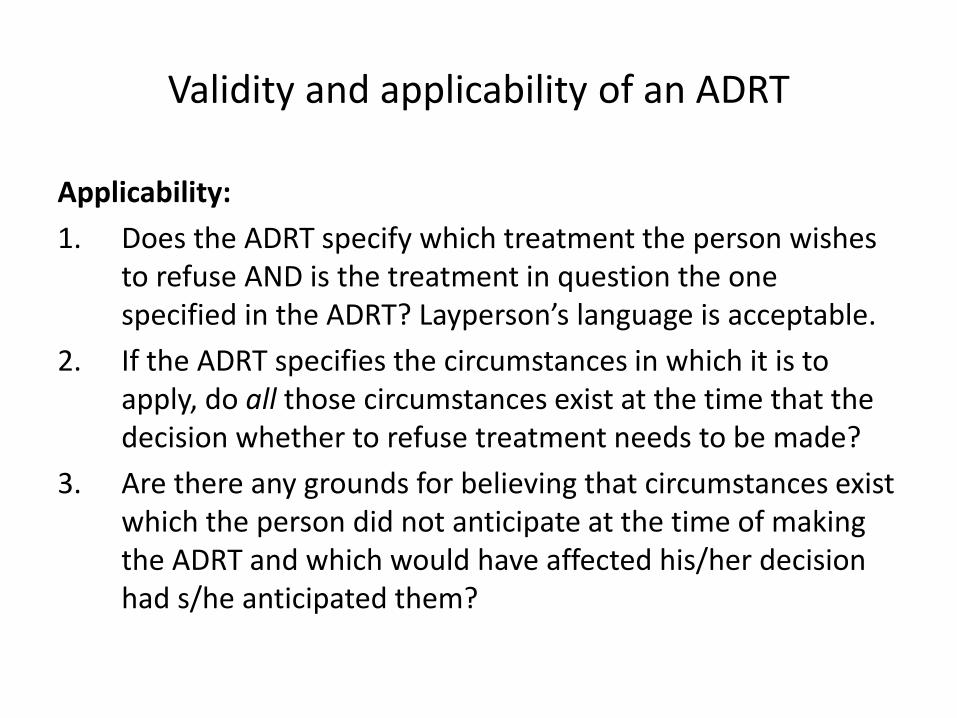
Validity and applicability of an ADRT
Applicability:
1. Does the ADRT specify which treatment the person wishes to refuse AND is the treatment in question the one specified in the ADRT? Layperson’s language is acceptable.
2. If the ADRT specifies the circumstances in which it is to apply, do all those circumstances exist at the time that the decision whether to refuse treatment needs to be made?
3. Are there any grounds for believing that circumstances exist which the person did not anticipate at the time of making the ADRT and which would have affected his/her decision had s/he anticipated them?
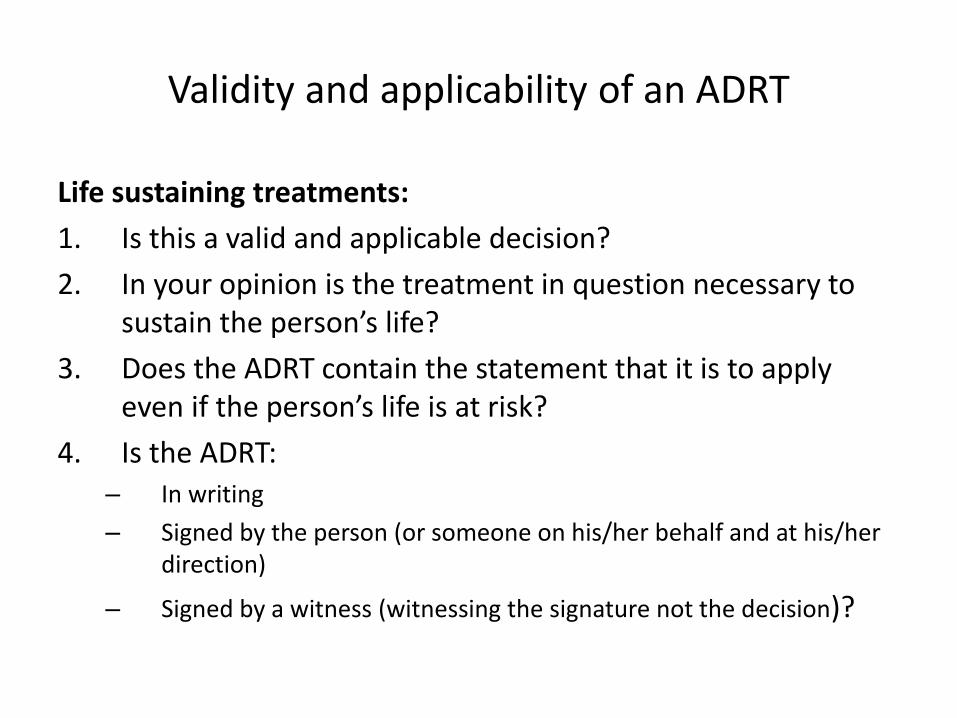
Validity and applicability of an ADRT
Life sustaining treatments:
1. Is this a valid and applicable decision?
2. In your opinion is the treatment in question necessary to sustain the person’s life?
3. Does the ADRT contain the statement that it is to apply even if the person’s life is at risk?
4. Is the ADRT: – In writing
– Signed by the person (or someone on his/her behalf and at his/her direction)
– Signed by a witness (witnessing the signature not the decision)?
(2) Lasting Power of Attorney
• A 75 year old gentleman with cognitive impairment secondary to MS is on the ward with a stroke, being actively treated. He does not have relevant capacity. His daughter shows you a Lasting Power of Attorney for issues pertaining to health and welfare, and tells you that he should not be for cardiopulmonary resuscitation.

Issues and responses
• Document: – Registered with the Office of the Public Guardian?
– Not withdrawn?
– What does the power of attorney encompass?
• Attorney (“Donee”): – Who (how many) attorneys are identified in the document?
• How are decisions to be taken eg jointly, jointly & severely, particular decisions made by particular attorneys
– Who is the person claiming to be the attorney (can she prove her identity)?
• Best interest: – Is there an ADRT and if so, was this written before or after the LPA?
– Is the DNACPR decision made in the person’s best interests (discussion with attorney about the grounds for this)? If not it should be challenged.
Objectives
By the end of this session you will:
• Understand some of the general issues that make advance care planning so challenging
• Be able to outline some of the specific issues with regard to advance care planning in MS















![Self-expandable metallic stents for the palliation of ...cancer-research-frontiers.org/wp-content/uploads/... · palliation of dysphagia in patients with esophageal cancer [9]. The](https://static.fdocuments.net/doc/165x107/5f0252b17e708231d403b3a8/self-expandable-metallic-stents-for-the-palliation-of-cancer-research-palliation.jpg)
