Jaypee Greens Kassia Sports City Greater Noida | +919560214267
Upload
maurice-cummingsCategory
view
222download
1
Peer Support – all of the Neuroanatomy...
Kassia and Dave
• A male aged 25 was admitted to hospital after a lorry vs pedestrian RTC. He was conscious and on initial examination you note a flaccid paralysis associated with the right hand and the right lower limb. Head CT was clear.
• What anatomical structure do you suspect has been damaged? What type of symptoms are these (LMN vs UMN)?
Spinal cord injury from trauma
LMN – flaccid paralysis, hyporeflexia, hypotonia, atrophy (due to spinal shock)
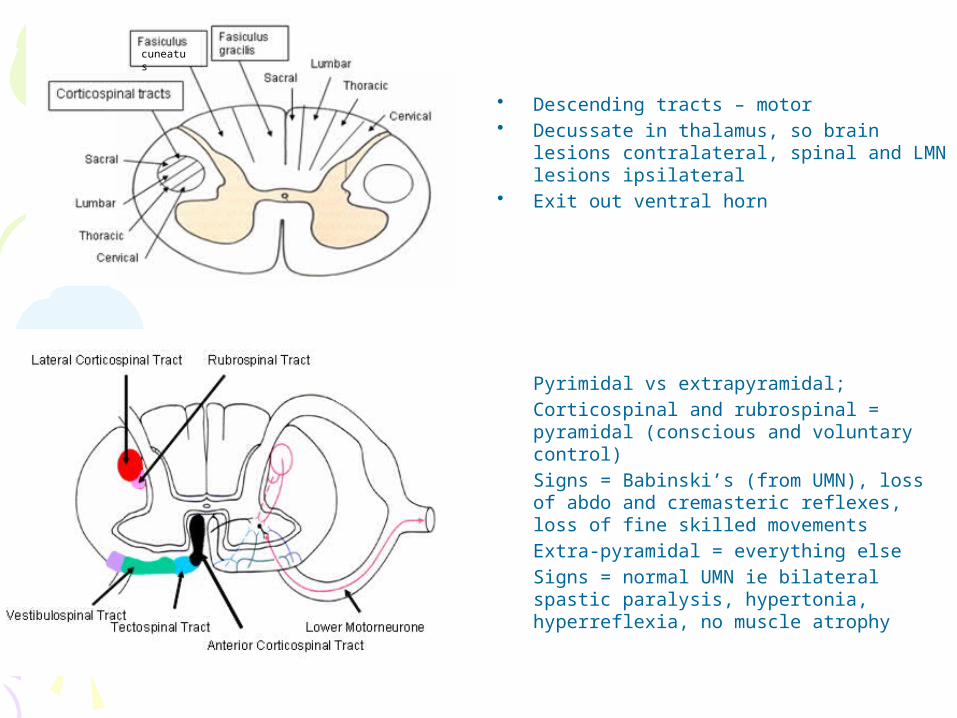
• Descending tracts – motor• Decussate in thalamus, so brain lesions
contralateral, spinal and LMN lesions ipsilateral
• Exit out ventral horn
• Pyrimidal vs extrapyramidal;• Corticospinal and rubrospinal = pyramidal
(conscious and voluntary control)• Signs = Babinski’s (from UMN), loss of abdo
and cremasteric reflexes, loss of fine skilled movements
• Extra-pyramidal = everything else• Signs = normal UMN ie bilateral spastic
paralysis, hypertonia, hyperreflexia, no muscle atrophy
cuneatus
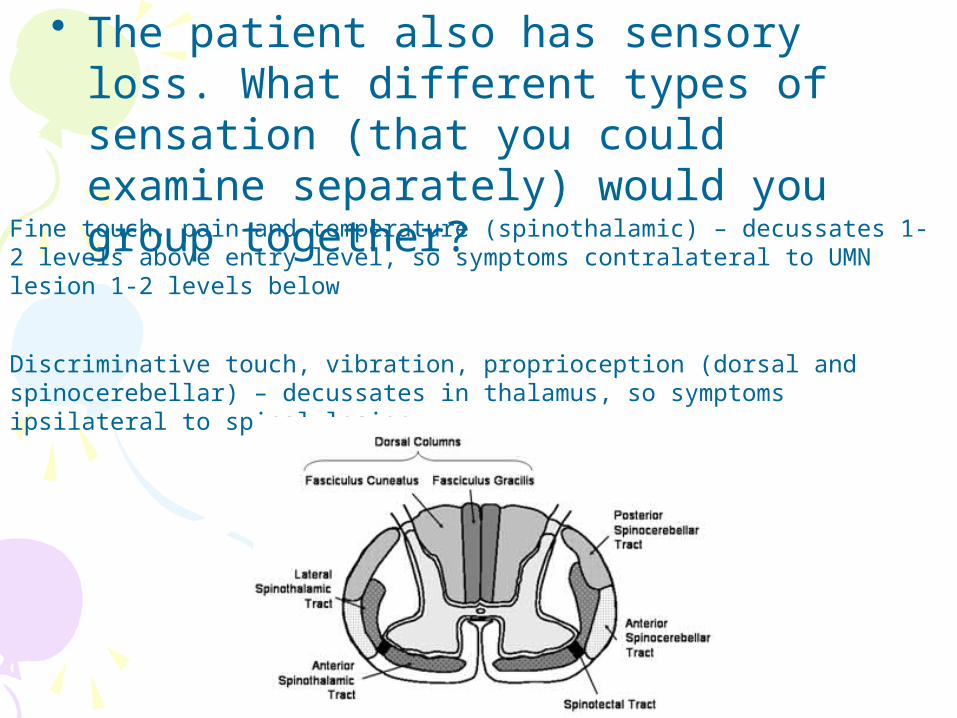
• The patient also has sensory loss. What different types of sensation (that you could examine separately) would you group together?
Fine touch, pain and temperature (spinothalamic) – decussates 1-2 levels above entry level, so symptoms contralateral to UMN lesion 1-2 levels below
Discriminative touch, vibration, proprioception (dorsal and spinocerebellar) – decussates in thalamus, so symptoms ipsilateral to spinal lesion
• Several months later you check on the progress of the patient and note further changes in motor function including paralysis and severe atrophy of muscles in medial aspects of the right hand and arm.
Furthermore, there is right lower limb paralysis along with hypertonia and hypereflexia. You also note clonus and an extensor plantar response (babinski sign) on stroking the sole of the right foot. However there appeared little muscle atrophy associated with the right leg compared to that observed in the hand. What type of symptoms are these? Do they suggest a specific descending tract has been affected?
UMN – no, both pyramidal and extrapyramidal signs
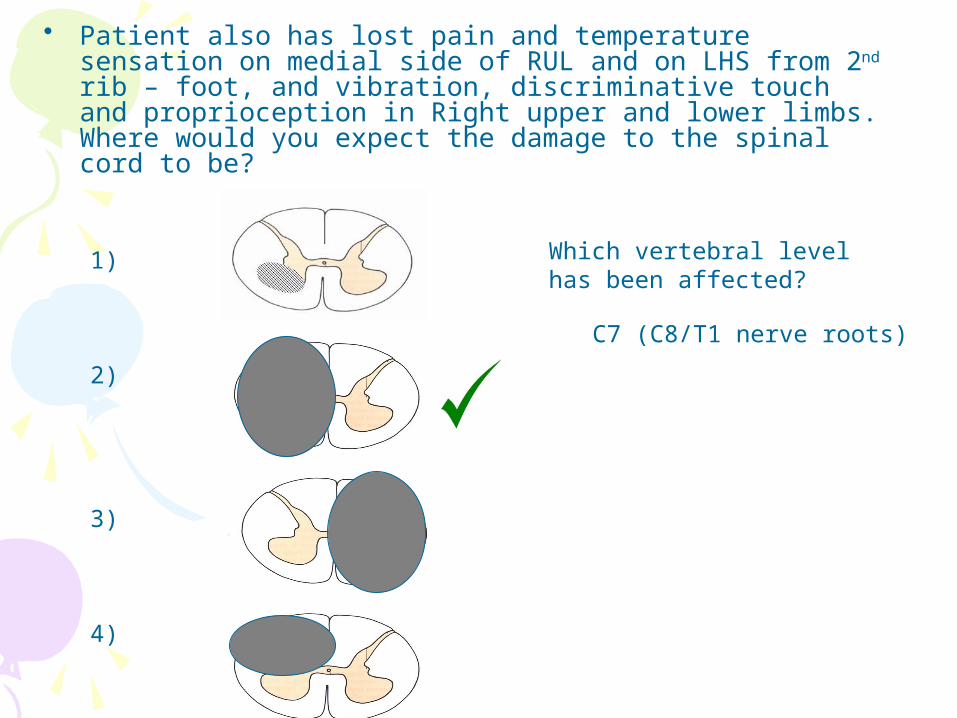
• Patient also has lost pain and temperature sensation on medial side of RUL and on LHS from 2nd rib – foot, and vibration, discriminative touch and proprioception in Right upper and lower limbs. Where would you expect the damage to the spinal cord to be?
1)
2)
3)
4)
Which vertebral level has been affected?
C7 (C8/T1 nerve roots)
Keith, a 68 year old man, was found collapsed at home by his wife. Examination revealed paralysis of his right upper limb and face but not his lower limb. Keith now has trouble comprehending spoken and written language and producing coherent speech.
What is the likely diagnosis?
Stroke
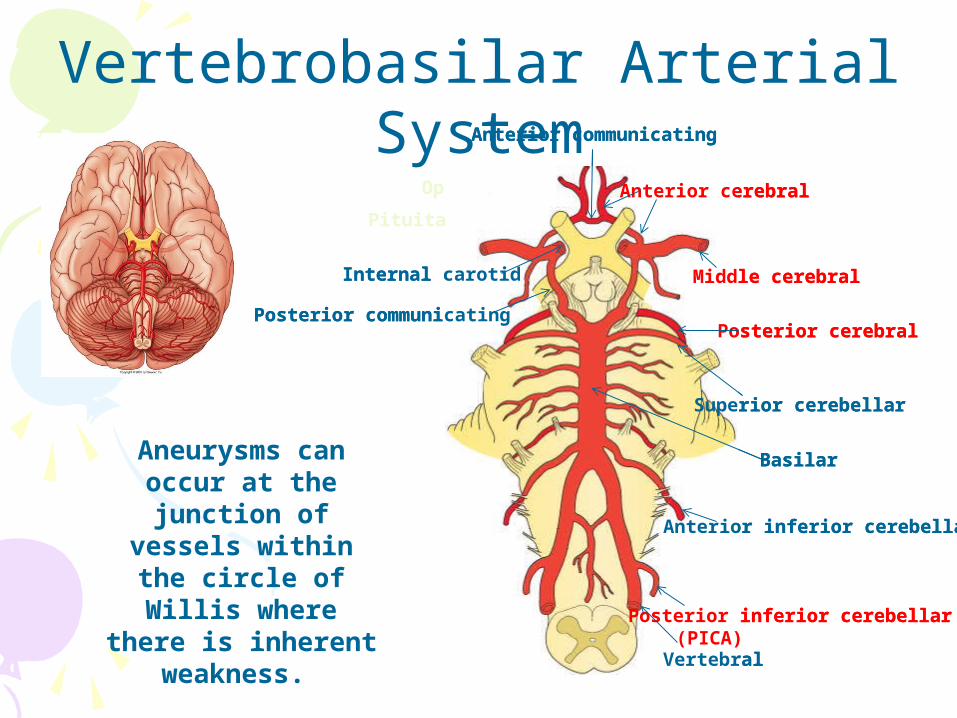
Aneurysms can occur at the
junction of vessels within the circle of Willis where there
is inherent weakness.
Anterior inferior cerebellar
Posterior inferior cerebellar(PICA)
Superior cerebellar
Middle cerebral
Anterior cerebral
Posterior cerebral
Basilar
Vertebral
Internal carotid
Anterior communicating
Posterior communicating
Vertebrobasilar Arterial System
Optic chiasm
Pituitary stalk
Anterior inferior cerebellar
Posterior inferior cerebellar(PICA)
Superior cerebellar
Middle cerebral
Anterior cerebral
Posterior cerebral
Basilar
Vertebral
Internal carotid
Anterior communicating
Posterior communicating
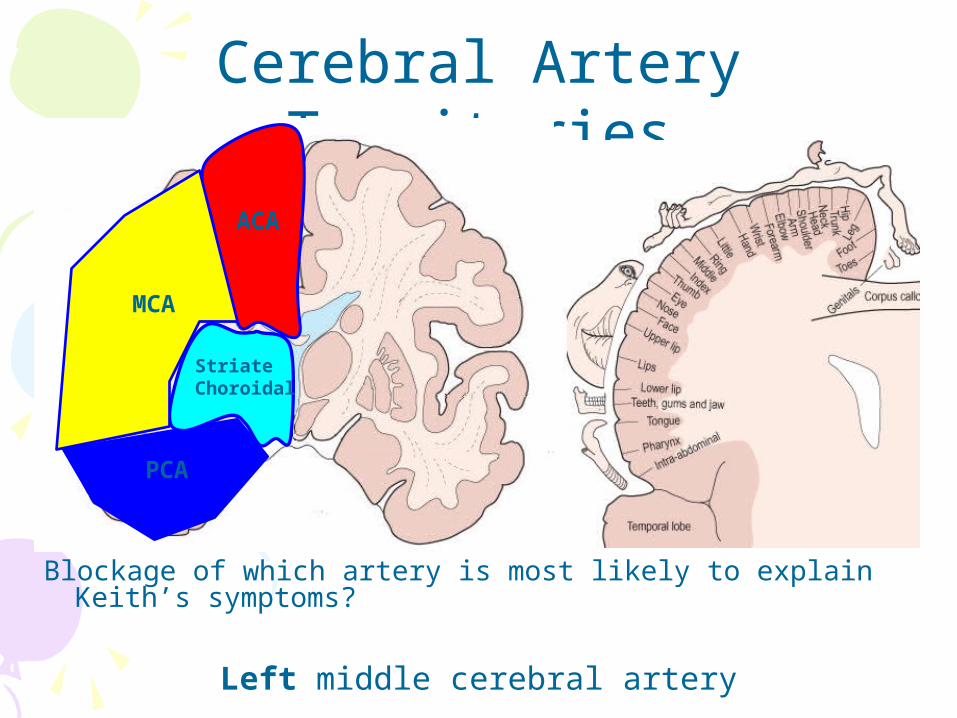
Blockage of which artery is most likely to explain Keith’s symptoms?
Cerebral Artery Territories
PCA
ACA
StriateChoroidal
MCA
Left middle cerebral artery
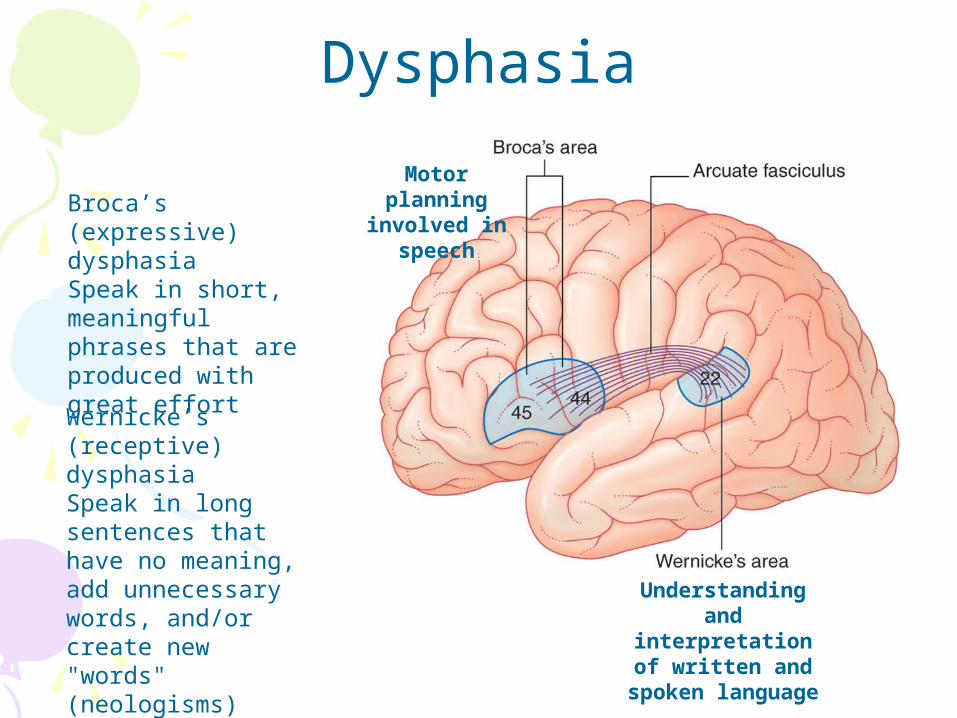
Understanding and interpretation of
written and spoken language
Motor planning involved in speech
Wernicke’s (receptive) dysphasiaSpeak in long sentences that have no meaning, add unnecessary words, and/or create new "words" (neologisms)
Broca’s (expressive) dysphasiaSpeak in short, meaningful phrases that are produced with great effort
Dysphasia
A 35 year old man complains of the worst headache of his life before losing consciousness. CT scan findings are consistent with a subarachnoid haemorrhage. Which of the following is the most likely aetiology?
a)Carotid artery occlusionb)Middle meningeal artery lacerationc)Ruptured aneurysm in the circle of Willisd)Middle meningeal artery occulsion
A 64 year old man is diagnosed with a stroke. His main deficit is a partial loss of his visual field resulting from a lesion in the occipital lobe. Which of the following arteries is likely to be involved?
a)Internal carotidb)External carotidc)Middle cerebrald)Posterior cerebral
Other stuff to revise• Basal Ganglia anatomy and pathways• Layers of the brain/meningitis• Groupings of cranial nerves eg
cavernous sinus, nuclei, bulbar vs pseudobulbar palsy
• Disc prolapse, cauda equina syndrome, sciatica, brown sequard, spinal shock

Brain + behaviour -> resources -> guides
• 62 yr old male patient comes into A+E with a arm laceration from a bike which he didn’t see. He complains of gradual progressive visual loss over the last 6 months, and when you do confrontation you discover he cannot see to his left. What is this called?
Left homonymous hemianopia
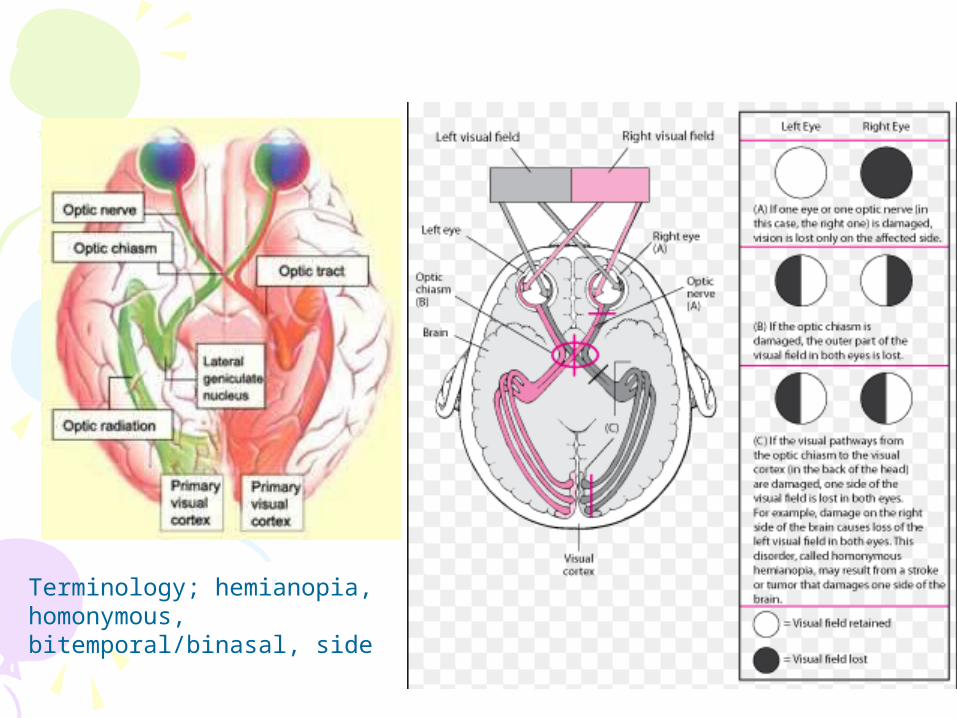
Terminology; hemianopia, homonymous, bitemporal/binasal, side
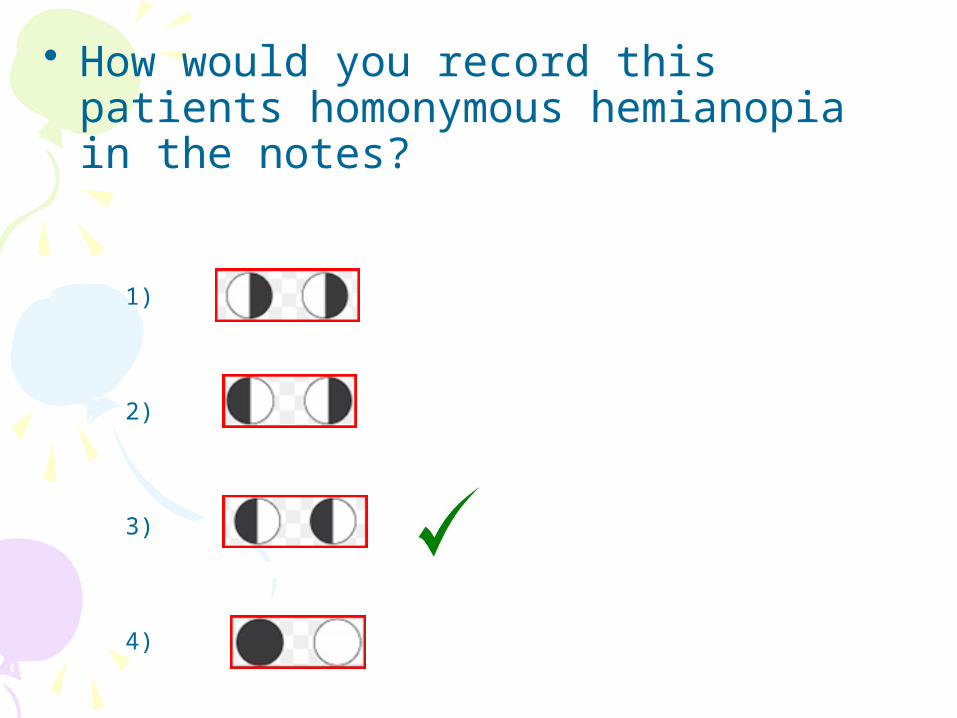
• How would you record this patients homonymous hemianopia in the notes?
1)
2)
3)
4)
• Where would the lesion have to be to cause these symptoms?
1) On the left optic nerve
2) On the left optic radiation
3) On the right occipital lobe
4) On the optic chiasm
Tom, a 22 year old student, presents to his GP complaining of double vision. He has no known previous medical conditions or visual problems. Examination revealed ptosis, an unreactive dilated pupil and displacement “down and out” in his left eye. Direct and consensual pupillary reflexes of the right eye were intact.
Which nerve palsy is demonstrated in this case?
Occulomotor (CNIII)
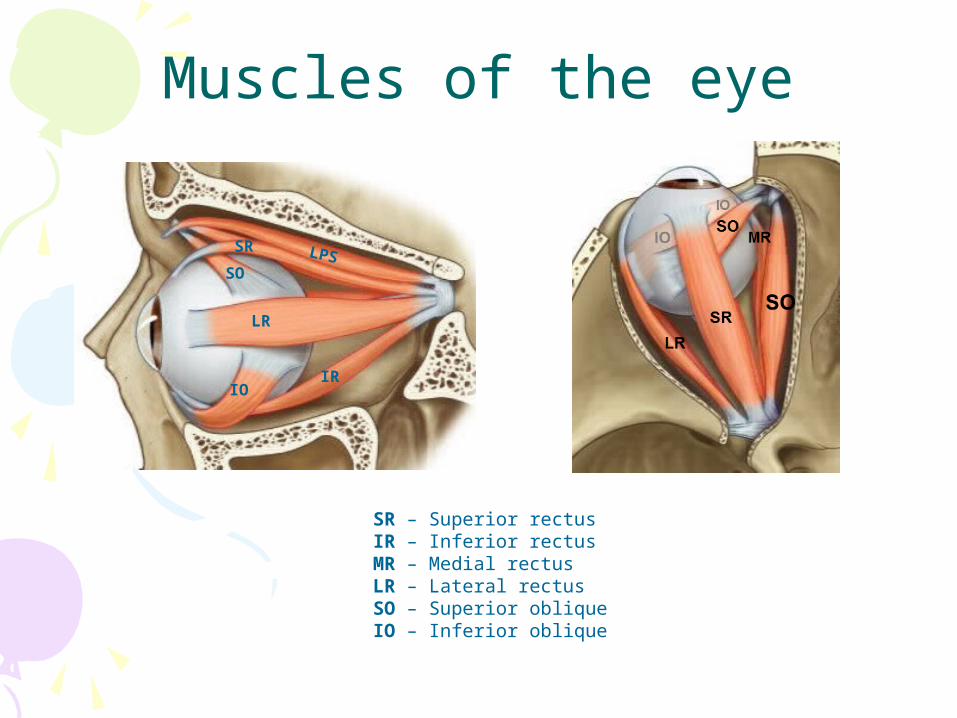
Muscles of the eye
SR – Superior rectusIR – Inferior rectusMR – Medial rectusLR – Lateral rectusSO – Superior obliqueIO – Inferior oblique
IR
LR
IO
SO
SR LPS
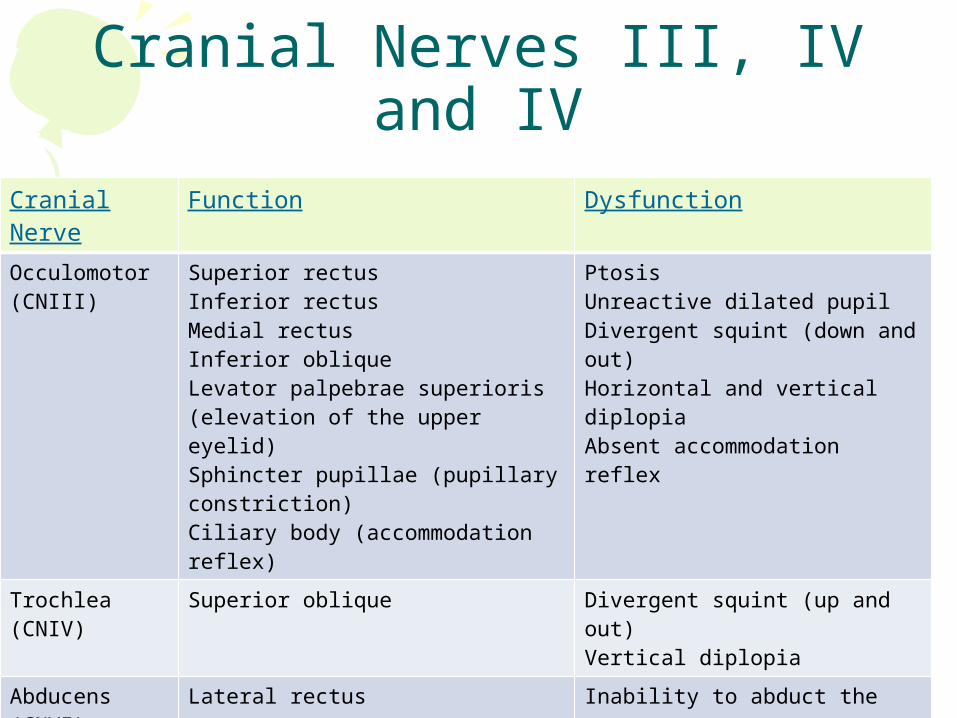
Cranial Nerves III, IV and IV
Cranial Nerve
Function Dysfunction
Occulomotor (CNIII)
Superior rectusInferior rectusMedial rectusInferior obliqueLevator palpebrae superioris (elevation of the upper eyelid)Sphincter pupillae (pupillary constriction)Ciliary body (accommodation reflex)
PtosisUnreactive dilated pupilDivergent squint (down and out)Horizontal and vertical diplopiaAbsent accommodation reflex
Trochlea (CNIV)
Superior oblique Divergent squint (up and out)Vertical diplopia
Abducens (CNVI)
Lateral rectus Inability to abduct the eyeConvergent squint (resting adduction)Horizontal diplopia
During a physical examination, you ask the patient to look laterally with her right eye and then upward. You have just tested the function of which muscle?
a)Left Superior rectusb)Right Superior rectusc)Right Inferior Obliqued)Right Superior oblique