Pediatrics 2012 Le Grange Peds.2011 1676
86
7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676 http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 1/86 Calculation of Expected Body Weight in Adolescents With Eating Disorders Daniel Le Grange, Peter M. Doyle, Sonja A. Swanson, Kali Ludwig, Catherine Glunz and Richard E. Kreipe Pediatrics; originally published online January 4, 2012; DOI: 10.1542/peds.2011-1676 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://pediatrics.aappublications.org/content/early/2012/01/02/peds.2011-1676 PEDIATRICS is the official journal of the American Academy of Pediatrics. A mont hly publication, it has been published continuously since 1948. PEDIATRICS is owned, published, and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2012 by the American Ac ademy of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-427 5. Downloaded from pediatrics.aappublications.org at Indonesia:AAP Sponsored on Jan uary 27, 2012
-
Upload
putranto-bhakti-prakosa -
Category
Documents
-
view
216 -
download
0
Transcript of Pediatrics 2012 Le Grange Peds.2011 1676

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 1/86
Calculation of Expected Body Weight in Adolescents With Eating Disorders
Daniel Le Grange, Peter M. Doyle, Sonja A. Swanson, Kali Ludwig, Catherine Glunz and Richard E. KreipePediatrics; originally published online January 4, 2012;DOI: 10.1542/peds.2011-1676
The online version of this article, along with updated information and services, islocated on the World Wide Web at:
http://pediatrics.aappublications.org/content/early/2012/01/02/peds.2011-1676
PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthlypublication, it has been published continuously since 1948. PEDIATRICS is owned, published, and trademarked by the American Academy of Pediatrics, 141 NorthwestPointBoulevard, Elk Grove Village, Illinois, 60007. Copyright © 2012 by the American Academy
of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.
Downloaded from pediatrics.aappublications.org at Indonesia:AAP Sponsored on January 27, 2012

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 2/86
ARTICLEARTICLECalculationofExpectedBodyWeightinAdolescentsWithEatingDisorders
AUTHORS:DanielLeGrange,PhD,aPeterM.Doyle,PhD,aSonja
A.Swanson,ScM,bKaliLudwig,BA,aCatherineGlunz,MD,candRichardE.Kreipe,
MDd
aDepartmentofPsychiatryandBehavioralNeuroscience,andcDepartmentofPediatrics
andInternalMedicine,TheUniversityofChicago,Chicago,Illinois;bDepartment

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 3/86
ofEpidemiology,HarvardSchoolofPublicHealth,Boston,Massachusetts;anddDivisionofAdolescentMedicine,DepartmentofPediatrics,UniversityofRochesterMedicalCenter,Rochester,New
York
KEYWORDS
adolescence,bodyweight,eatingdisorders
ABBREVIATIONS
ANanorexianervosaCDCCentersforDiseaseControlandPreventionCIconfidence
intervalDSM-IVTRDiagnosticandStatisticalManualofMentalDisorders,FourthEdition,

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 4/86
TextRevision
EBWexpectedbodyweight%EBWpercentexpectedbodyweight
Allauthorsmadesubstantialcontributionstoconceptionanddesign,acquisitionof
data,oranalysisandinterpretationofdata;draftingofthearticleorrevising
itcriticallyforimportantintellectualcontent;andfinalapprovaloftheversionto
bepublished.
www.pediatrics.org/cgi/doi/10.1542/peds.2011-1676
doi:10.1542/peds.2011-1676

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 5/86
AcceptedforpublicationSep26,2011
AddresscorrespondencetoDanielLeGrange,PhD,DepartmentofPsychiatryandBehavioralNeuroscience,TheUniversityof
Chicago,5841S.MarylandAve.,MC3077,Chicago,IL60637.E-mail:[email protected]
PEDIATRICS(ISSNNumbers:Print,0031-4005;Online,1098-4275).
Copyright©2012by
theAmericanAcademyofPediatrics
FINANCIALDISCLOSURE:Dr

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 6/86
LeGrangereceivesroyaltiesfromGuilfordPressandhonorariafromtheTrainingInstituteforChildandAdolescentEatingDisorders,LLC.Theotherauthorshave
indicatedtheyhavenofinancialrelationshipsrelevanttothisarticletodisclose.
FundedbytheNationalInstitutesofHealth(NIH).
WHATS
KNOWNONTHISSUBJECT:Eatingdisordersare
characterized

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 7/86
bypreoccupationwithweightandshape,whichis
manifestedbyarefusaltomaintainanormalweight.Anexact
determination
ofexpectedbodyweight(EBW)iscriticalfor
diagnosisandclinical
managementofthesedisorders.
WHATTHISSTUDYADDS:TheMcLarenand
MooremethodspresentwithseverallimitationswhencalculatingEBWfor

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 8/86
adolescentswitheatingdisorders.AcommonlyagreeduponmethodforEBWcalculationsuchastheBMIpercentilemethodisrecommendedforclinicalandresearch
purposes.
abstract
OBJECTIVE:Toexaminetheagreement
betweenthreemethodstocalculateexpectedbodyweight(EBW)foradolescentswitheating
disorders:(1)BMIpercentile,(2)McLaren,and(2)Mooremethods.

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 9/86
METHODS:Theauthorsconductedacross-sectionalanalysisofbaselineinformationfromadolescentsseekingtreatmentofdisorderedeatingatTheUniversityofChicago.
Adolescents(N=373)aged12to18years(mean=15.84,SD=1.72),
withanorexianervosa(n=130),bulimianervosa(n=59),oreating
disordernototherwisespecified(n=184).ConcurrencebetweentheBMI

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 10/86
percentile,McLaren,andMooremethodswasassessedforagreementaboveorbelowarbitrarycutpointsusedinrelationtohospitalization(75%),diagnosis(85%),and
healthyweight(100%).Patternsofabsolutediscrepancieswereexaminedbyheight,age,gender,
andmenstrualstatus.Limitationstosomeofthesemethodsallowedcomparisonbetweenall
3methodsinonly204participants.
RESULTS:Moderate

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 11/86
agreementwasseenbetweenthe3methods(kvalues,0.480.74),withpairwisetotalclassificationaccuracyateachcutpointrangingfrom84%to98%.
Themostdiscrepantcalculationswereobservedamongthetallest(.75thpercentile)andshortest
(,20thpercentile)casesandolderages(.16years).Manyofthemostdiscrepant
casesfellaboveandbelow85%EBWwhencomparingthe

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 12/86
BMIpercentileandMooremethods,indicatingdisagreementonpossiblediagnosisofanorexianervosa.
CONCLUSIONS:ThesemethodslargelyagreeonpercentEBWin
termsofclinicallysignificantcutpoints.However,theMcLarenandMooremethodspresent
withlimitations,andacommonlyagreed-uponmethodforEBWcalculationsuchasthe
BMIpercentilemethodisrecommendedforclinicalandresearchpurposes.

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 13/86
Pediatrics2012;129:19
PEDIATRICSVolume129,Number2,February2012
Downloaded from pediatrics.aappublications.org at Indonesia:AAP Sponsored on January 27, 2012

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 14/86
Eatingdisordersarecharacterizedbydisturbancesiningestivebehaviorandareusuallyaccompaniedbypreoccupationwithweightandshape.1Thispreoccupationisoften
manifestedbyaninabilitytomaintainanormalweightforageandheight
andistheprimarydiagnosticcriterionforanorexianervosa(AN).Determiningthedeviation
fromexpectedbodyweight(EBW)(oftenreferredtoasideal

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 15/86
bodyweight)isthereforeimportantinthediagnosisofAN(,85%EBW)andthedifferentialdiagnosisofbulimianervosa(.85%EBW)andeatingdisorder
nototherwisespecified(deviationfromEBWlessclearlydemarcated).
Inaddition
todiagnosis,EBWisusedasanindicatorofmedicalstability,asjustification
forhospitalization,tosetappropriatetargetweights,2,3andtotrack

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 16/86
progressintreatmentandassessrecovery.4,5Yet,thereisnoconsensusonhowbesttocalculateEBWforthepediatricandadolescenteatingdisorders
population.AlthoughabsoluteBMI(weightinkilograms/heightinmeters;seeref2)has
gainedattentioninbothclinicalandresearchsettings,itismostcommonlyused
toscreenforobesityandismostapplicabletothe

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 17/86
adultpopulation.6,7Moreover,BMIisbasedonheightandweightonlyanddoesnotaccountforuniquephenomenonsuchasshortstatureorstunted
lineargrowthduetomalnutrition.8Therefore,itisnotanoptimalmethodto
reflectnutritionalstatus,especiallyforadolescents.Forpediatricandadolescentpopulations,age-andgender-
adjustedBMIpercentilesaremoreappropriateasweightandheight

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 18/86
normallyincreaseuntil20yearsofage(CentersforDiseaseControlandPrevention[CDC]BMI-for-agegrowthcharts;www.cdc.gov/growthcharts).9
Examinationofanadolescents
weightinrelationtothe50thBMIpercentile,alsoknownastheBMI
percentilemethod,orBMImethod,isperhapsthe
mostfrequentlyused
methodtodeterminetheweightcriterionforaneatingdisorder

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 19/86
diagnosis.10,11InadditiontotheBMImethod,9othermethodsareusedtocalculateEBW;forexample,theMcLaren12andMoore13methods.TheBMI,McLaren,
andMooremethodsareallpediatricspecificandusethechildoradolescents
gender,age,andheighttocalculateEBWbutdonottakeothermeasures
ofanthropometry(eg,bodycompositionandbodyframe)intoaccount.

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 20/86
ResearchershavedemonstratedconsiderableagreementforEBWcalculationsacrossthese3methodsforhealthyadolescents.14However,suchcalculationsarewidelydiscrepantforolderhealthy
adolescentsatthelowestandhighestpercentiles.14
Instudiesofpatients
witheatingdisorders,authorsrarelydescribetheirmethodforcalculatingEBW.Therefore,the
primarygoalofthecurrentstudywastoexaminethe

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 21/86
agreementand/ordiscrepancybetweentheBMI,McLaren,andMooremethodswhencalculatingEBWforadolescentswitheatingdisorders.Asecondarygoalwastodetermine
whetherourfindingswouldallowforclearerguidelinesregardingthemostappropriatemethod(s)
tocalculateEBWforthepediatricandadolescenteatingdisorderspopulation.
METHODSSubjects
Subjectswere373treatment-seekingadolescents,including

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 22/86
researchparticipants,evaluatedatanoutpatienteatingdisordersclinicfromOctober1998throughDecember2009.Thesamplewascomposedof342(91.7%)femalesand
31(8.3%)males,aged12to18years(mean=15.84,SD=
1.72),whometDiagnosticandStatisticalManualofMentalDisorders,FourthEdition,Text
Revision(DSM-IVTR)1criteriaforAN(n=130),bulimianervosa

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 23/86
(n=59),oreatingdisordernototherwisespecified(n=184).Themajoritywerewhite
(74.1%),and13.2%wereHispanic,7.6%
black,1.9%Asian/PacificIslander,and3.2%identifiedasOther. Inadditiontoweight
andheightmeasures,participantsprovideddemographicinformationandcompletedstructureddiagnosticinterviews(ie,
theEatingDisorderExamination15andasetofpaper-and-pencilquestionnaires).

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 24/86
Forthepurposesofthisreport,weonlyusedweight,height,age,gender,menstrualstatus,ethnicity,anddiagnosis.Writteninformedconsentforpatientsaged
18yearsorparental/guardianconsentandadolescentassentforpatients,18years
ofagewereobtained.TheUniversityofChicagoInstitutionalReviewBoardapprovedthe
researchprotocol.
EBWCalculations
EBWwas

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 25/86
calculatedforeachsubjectlimitedtothreeindependentmethodsdescribedinthefollowingtext:BMI,9McLaren,12andMoore13methods.
IntheBMI
method,tocalculatepercentexpectedbodyweight(%EBW)foragivenparticipantbased
onhisorherheight,age,andgender,the50thpercentileBMIfor
exactageandheightatpresentationontheCDCBMI-for-age

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 26/86
percentileschart4wasused(%EBW=BMI/50thpercentileBMIforageandheight3100).ABMIatthe50thpercentilewouldbetheexpectedmedianina
groupofnormallydevelopingadolescents,orEBW.
TheMcLarenmethod12uses
agrowthchartbasedonheight-andweight-forageandforgender(eg,CDC).First,
theparticipantsheightisplottedonthechart.Aline

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 27/86
isextendedhorizontallytothe50thpercentileheight-for-ageofthatparticipant.Asecondlineisthenextendedverticallyfromthe50thpercentileheight-for-ageto
thecorresponding50thpercentileweight.This50thpercentileweightisdeemedtheparticipantsEBW.
TheMooremethod13alsousesagrowthchartbasedonheight-and
weight-forageandgender(eg,CDC),albeitinaslightlydifferent

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 28/86
way.Theparticipants
LEGRANGEetal
Downloaded from pediatrics.aappublications.org at Indonesia:AAP Sponsored on January 27, 2012

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 29/86
ARTICLEARTICLEheight-for-agepercentileisdetermined,andtheEBWistheweightthatcorrespondstothatweightpercentile(eg,aparticipantinthe30th
percentileheight-for-ageandgenderwouldhaveanEBWthatcorrespondstothe
30thpercentileweight-for-ageandgender).
Ofnote,becauseoftheasymptotic
natureoftheheightcurvesasadolescentscompletegrowth,the

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 30/86
McLarenmethodcannotcalculateEBWforgirls.163cmorforboys.176cm.Inaddition,theMooremethodcannotbeusedeasilyfor
children.97thor,3rdpercentileforheightorweightontheCDCgrowth
charts,asthesearethelimitsofwhatarepicturedonthecharts,
andmostpractitionersdonotreadilyaccesstherawCDC

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 31/86
dataforextremesofheightandweightpercentiles.Assuch,directcomparisonbetweenall3methodscouldonlybemadefor204(55%)participants
inourstudy.
ConcurrencebetweentheBMI,McLaren,andMooremethods
wasassessedprimarilyforagreementaboveorbelowEBWthresholdsof75%(hospitalization),
85%(ANdiagnosis),and100%(healthygoalweight).Patternsof

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 32/86
absolutediscrepancieswereexaminedbyheight,age,gender,andmenstrualstatus.Table1demonstratesthechallengesaroundthese3methodsbycalculating%EBWfor
a14-year-oldgirlstanding165.1cm(65in.)tall.
StatisticalAnalysis
StatisticalanalyseswerecompletedinRversion2.10.Usingcategoriesas
describedearlier(above/belowcutpoints
TABLE1Example

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 33/86
CalculationFor14-Year-
OldGirlMeasuring165.1cm(65
in.)and45.4kg(100lb)
MethodEstimatedEBWSubjects
%EBWBMI52.68kg(116.15lb)86.1Moore57.13kg(125.95lb)79.4
McLarenIncalculableaIncalculablea
a
Subjectsexpectedbodyweightand
percentexpectedbodyweightcouldnotbecalculatedusingthe

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 34/86
McLarenmethodbecausesheistallerthan163cm.
PEDIATRICSVolume129,Number2,February2012
forhospitalization,diagnosisof
AN,orahealthygoalweight),totalclassificationaccuracyandunweightedandquadratically
weightedkvalueswerecalculatedforpairwisecomparisonsofthe3methodsfor
EBWcalculation.Althoughbothtypesofkstatisticsreflectoverall

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 35/86
measuresofconcordance,quadraticallyweightedkvaluesgivemorepenaltytothelargerdiscrepancies(eg,asubjectinthe,75%EBWcategoryusingone
methodand.100%EBWcategoryusinganother)comparedwiththeunweightedkvalues.
Totalclassificationaccuracywasfurthercalculatedforthe3waycomparison.Inaddition,the
actualvaluesof%EBW(asopposedtothecategoriesmentioned

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 36/86
earlier)wereplottedaspairwisecomparisonsofthe3methods.Linearmodelswerefitforeachofthesecomparisons,andintraclasscorrelationswerecalculated.
Finally,thesepairwisedifferenceswereevaluatedacrosslevelsofthefollowingcovariates:age,
gender,heightpercentile,andmenstrualstatus.
RESULTSAgreement
Table
2presentsthepairwiseand3-wayagreementofeachof

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 37/86
thesemethodsbythe3predeterminedcutpoints.Lookingfirstatpairwiseagreement,all3possiblepairsperformmoderatelywellateachthreshold,with
totalclassificationagreementrangingfrom84.2%to97.5%.TheBMIandMooremethods
tendedtohavethelowestclassificationagreement(84.2%87.7%),followedbytheBMIand
McLarenmethods(87.7% 96.1%)andthentheMooreandMcLaren

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 38/86
methods(90.2%97.5%).Agreementtendedtoperformbestonthelowerextremecutpoints;thatis,betteragreementwasseenwhenpredictingwhetheradolescentswere
aboveorbelow75%EBW(87.7%97.5%)comparedwiththatforthe85%EBW
cutpoint(84.2%95.1%)andthe100%EBWcutpoint(85.8%90.2%).kvaluesindicate
moderate-to-goodagreement
overall,withtheunweightedkvalues

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 39/86
rangingfrom0.49to0.74andquadraticallyweightedkvaluesrangingfrom0.72to0.89.Thesuperiorityofthequadraticallyweightedkvaluesto
theunweightedkvaluesindicatesthatwhendisagreementoccurs,itmostoftenoccurs
onecellover(eg,onemeasureindicates,75%EBWwhereasanotherindicates75%
to85%EBW).
Three-wayagreementpatternsindicatethat

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 40/86
abouthalfofthetime,all3measuresagreeonclassificationaboveorbelow75%EBW(51.5%),85%EBW(46.9%),and100%EBW(46.6%).
Inaboutone-thirdofcases(35.1%35.9%),theMooreandBMImethodsagreeon
theclassification,whereastheMcLarencannotbecalculated(ie,aformofdisagreement).
Theremainingcasesrepresentmeasureddisagreement.
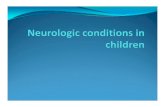
Figure1

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 41/86
plotsthepairwisecomparisonsofthe3methodscontinuously.Althoughtheindividualcomparisonsclusternearthelineofoptimalagreement,significantnoiseanddiscrepancies
canbeseen,especiallywhencomparingtheBMIandMooremethods.Intraclasscorrelation
fortheBMIandMooremethodswas0.88(95%confidenceinterval[95%CI],
0.85 0.90),fortheBMIandMcLarenmethodswas0.90

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 42/86
(95%CI,0.870.92),andfortheMooreandMcLarenmethodswas0.96(95%CI,0.950.97).
MostDiscrepantCases
Althoughagreement
atthecategoricallevelwasrelativelyhigh,someadolescentshadextremelydifferentcalculations
of%EBWforthevariousmethods,withthebiggestdiscrepancybeingnearly60%
EBW.Table3presentsthefivemostdiscrepantcasesfor

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 43/86
eachpairwisecomparison.Mostofthesediscrepancieswillbeclinicallyrelevantforeatingdisorderassessment.Forinstance,oneadolescentwasmeasuredas143.2%with
theBMImethodand196.0%intheMcLarenmethod.As
Downloaded from pediatrics.aappublications.org at Indonesia:AAP Sponsored on Jan
uary 27, 2012

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 44/86
both are above 85% EBW, they wouldnot distinguish AN from other eatingdisorders. Others crossed boundariesbetween characterizing the adolescentas severely underweight versus abovetheir ideal weight. For instance, oneadolescent was measured as 107.1%EBW with the BMI method and 55.4%EBW with the Moore method. Generally,these severely discrepant calculationsoccurred in females and older ages(primarily 1618 years). The 5 mostdiscrepant cases between the BMI andMoore methods tended to be tall,whereas the discrepant cases in theother comparisons ranged in height.Discrepancy by CovariatesPairwise discrepancies (eg, BMI methodestimate minus Moore method estimate)werecomparedacrosstherangeofheightTABLE 2 Total Classification Agreement and Overall k-Value Estimates for Pairwise and 3-Way ComparisonsAgreement 75% EBW Agreement 85% EBW Agreement 100% EBW Agreement, k
Comparison Na % Na % Na % Unweighted Quadratic WeightsBMIMoore comparison 0.487 0.721Agreement 327 87.7 314 84.2 320 85.8Disagreement 46 12.3 59 15.8 53 14.2BMIMcLaren comparison 0.592 0.824Agreement 196 96.1 180 88.2 179 87.7Disagreement 8 3.9 24 11.8 25 12.3MooreMcLaren comparison 0.737 0.888Agreement 199 97.5 194 95.1 184 90.2Disagreement 5 2.5 10 4.9 20 9.83-Way comparison NC NC3-Way agreement 192 51.5 175 46.9 174 46.6Disagreement (all methods measurable) 12 3.2 29 7.8 30 8.0
Disagreement (McLaren unmeasured) 35 9.4 35 9.4 38 10.2Moore/BMI agreement, McLaren unmeasured 134 35.9 134 35.9 131 35.1a When comparing BMI with Moore, N = 373. When comparing BMI with McLaren or Moore with McLaren, the McLaren method is unable to be calculated for several cases and thus the N = 204.NC, not calculable.FIGURE 1Pairwise comparisons of the 3 methods to calculate %EBWat the continuous level.Intraclass correlations associated with these 3 graphs were 0.879, 0.902, and0.960, respectively.4 LE GRANGE et alDownloaded from pediatrics.aappublications.org at Indonesia:AAP Sponsored on January 27, 2012

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 45/86
ARTICLE ARTICLETABLE3Characteristicsofthe5MostDiscrepantPairwiseDisagreements
ComparisonDiscrepancyofInterestaBMIWeight(kg)Height(cm)Age
(mo)Gender%EBWBMI%EBWMoore%EBWMcLarenBMIMoore51.72271.6180.3
195F107.155.4NC35.925.780.1176.5216F120.985
NC35.225.478175.3188F125.390.1NC

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 46/86
32.224.775.7175.3197F119.587.3NC30.523.271.2175.3196F112.682.1NCBMIMcLaren52.8b29.941.3117.5204
F143.2138.419649.9c38.9d34.331.359.953.1132.1130.2220
188FF160.6154.5171.2171.8210.5193.428.423.333.2119.4
156F124.5150.9152.927.1e37.993.9157.5213

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 47/86
F178.8189.9205.9MooreMcLaren57.6b29.941.3117.5204F143.2138.419639.3c21.6d34.331.359.953.1132.1130.2220188
FF160.6154.5171.2171.8210.5193.416e37.993.9157.5213
F178.8189.9205.912.329.372.6157.5217F137.5146.1158.4
aDiscrepancymeasuredastheabsolutedifferencebetween

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 48/86
the2referencemethodsofcalculating%EBW.beIndicatesthesamecaseappearingundermultiplepairwisediscrepancies.NC,notcalculable.
percentiles(Fig2),
age(Fig3),gender(Fig
4),andmenstrualstatus(Fig5).
Regardingheightpercentiles,anear-cubicrelationshipbetweenheightpercentileandtheBMIMoorediscrepancy
wasseen,withtheMooremethodyielding
much

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 49/86
largerestimatesfor%EBWatlowerheightpercentiles(eg,,20thpercentile)andtheBMImethodgivinglargerestimatesatthehigherheightpercentiles(eg,
.75thpercentile).IncomparingboththeBMIandMooremethodsagainstthe
McLarenmethod,thediscrepanciesweremostpronouncedforlowerheightpercentiles.
Intermsofage,theBMIandMooremethods

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 50/86
haveconsistentdisagreementacrossthisagerange(1218yearsold).
FIGURE2
Pairwisediscrepancyaccordingtoheightpercentile.
PEDIATRICSVolume129,Number2,February2012
Downloaded from pediatrics.aappublications.org at Indonesia:AAP Sponsored on January 27, 2012

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 51/86
FIGURE3
Pairwisediscrepancyaccordingtoage.
FIGURE4
Pairwisediscrepancyaccordingtogender.
LEGRANGEetal
Downloaded from pediatrics.aappublications.org at Indonesia:AAP Sponsored on January 27, 2012

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 52/86
ARTICLEARTICLEFIGURE5
Pairwisediscrepancyaccordingtomenstruationstatus.PA,primaryamenorrhea;SA,secondaryamenorrhea;oligo,oligomenorrhea;BC,birthcontrol.
WhencomparingtheBMIandMooremethodsagainsttheMcLarenmethod,the
discrepanciesincreasewithage.TheMooremethodtendstoestimatehighervaluesof
%EBWamongolderagescomparedwithbothothermethods,particularly

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 53/86
aboveage16years.
Withrespecttogender,theMcLarenmethodprovideslargerestimatesof%EBWthaneithertheMooreor
BMImethodsforgirls,butthisbiaswaslessforboys.Thereseems
tobemorevariabilityforgirlsthanforboys,whichcouldbea
functionofthefactthatoursamplewasmostlygirls.

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 54/86
Intermsofmenstrualstatus,forthoseonbirthcontroland/orwithregularmenses,theMcLarenmethodprovideslargerestimatesof%EBWthaneither
theMooreorBMImethods,butthisfindingcouldbeconfoundedbyage.
DISCUSSION
Theprimaryobjectivewastotest3methods
usedtocalculateEBWforadolescentswitheatingdisorders:BMI,

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 55/86
McLaren,andMoore.Specifically,wewereinterestedintheextenttowhichthesemethodsbroughtaboutagreementordisagreementoncutpoints
forhospitalization(75%EBW),diagnosis(85%EBW),andhealthyweight(100%EBW).Our
secondarygoalwastodeterminewhetherourfindingswouldallowforclearerguidelines
regardingthedeterminationofEBWforthispatientpopulation.

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 56/86
Overall,therewasmoderateagreementbetweenthe3methods,withpairwisetotalclassificationaccuracyateachcutpointrangingfrom84%to98%.
The3methodslargelyagreeon%EBWintermsofclinicallysignificantcut
pointswiththeexceptionofthediscrepantcalculationsforarelativelysmallnumber
ofcases(2.5%-15.8%).CorrelationswerelowestforBMIand

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 57/86
Moore(0.88)andhighestforMooreandMcLaren(0.96).Themostdiscrepantcalculationswereobservedamongthetallerpatients(.75thpercentile),shorterpatients(,20th
percentile),andthose.16
yearsofage.Manyofthesemost
discrepantcases,whencomparingtheBMIandMooremethods,fellaboveandbelow
85%EBW.Forinstance,thisdiscrepancynotonlyindicateddisagreement

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 58/86
ontheweightcriterionforpossiblediagnosisofAN,butalsothesameindividual(seeTable3,firstcase)wouldwarranthospitalizationgiventhe
Mooremethod(ie,55%EBW)whilesimultaneouslybeingconsideredclosetonormalweight
giventheBMImethod(ie,107%EBW).Theevidenceforagreementwasnot
asstrikingforgenderandmenstrualstatusasitwas

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 59/86
forheightandage.TheMcLarenmethodpresentedwiththemostsignificantlimitationinthatitcannotbeusedforboys.176cmor
girls.163cm(medianheightforgirlsaged$14years),whichlimitedour
originalsampleby.40%.Inaddition,theMooremethodischallengingatextremes
ofheightandweight.Therefore,ourstudydemonstrates,evenprior

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 60/86
totheanalyses,theimportanceoftheBMImethod
PEDIATRICSVolume129,Number2,February2012
Downloaded from pediatrics.aappublications.org at Indonesia:AAP Sponsored on January 27, 2012

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 61/86
asamethodologythatcanapplytochildrenandadolescentsatallages,heights,andweights.
Thesediscrepantcalculationsunderscorethe
implicationswhenusingonemethodratherthananotherfortheassessmentofadolescents
witheatingdisorderswhoareoutsidethenormforheightor.16years
ofage.Thisconsiderationisespeciallyimportantforresearchendeavors

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 62/86
whenstudyinclusioniscontingentuponadiagnosisthatisarrivedatviaEBWcalculations.Forexample,itisfairtosaythatfor
verytalladolescents,theBMImethodwillcalculatehigher%EBWthantheMoore
method.IfcliniciansareuncertainaboutthediagnosisofAN,theyshouldconsider
thetrade-offsofmakingafalse-positiveversusafalse-negative

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 63/86
diagnosiswhenchoosingonemethodoveranother.However,intheinterestofadvancingasharedlanguageamongcliniciansandresearchers,wesuggestthatthe
BMImethodbeusedasitmayposethefewestobstacles(easeof
calculation)orexceptions(heightandage).Weacknowledgethatinsomeinstancesclinical
decision-makingwillbecomplexandrequireamoreflexibleapproach.

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 64/86
However,auniformadherenceto1methodtocalculateEBWwillstrengthenclinicalandresearchpractice.
Somelimitationsandstrengthstoour
studyshouldbeconsidered.Wedidnotknowapriorithattheshortcomings
fortheMcLarenandMooremethodswouldresultinthesemethodsnotbeing
feasibleforEBWcalculationsinasubsetofoursample.

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 65/86
However,onlyuponattemptingcomparisonsofthesemethodsdidwelearnthat.40%ofoursamplecouldnotbecomparedinthisway.To
date,ithasnotbeenwellestablishedthateatingdisorderpatientswouldpresent
thismanyoutliers,norhassuchafindingbeenpresentedin
anempiricalmanner.Thus,ourstudyshowsthatthereis

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 66/86
littleutilityfortheMcLarenmethodinanadolescenteatingdisordersample.Alimitationofall3methodsinvolvestheinabilitytoaccountfor
stuntedgrowthinpediatricsubjectswitheatingdisorders(ie,heightstuntingwillaffect
calculationofEBWandwillunderestimateitinalllikelihood).Itisfor
practitionerstotakethislimitationintoconsiderationwhengrowthstunting

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 67/86
issuspectedclinically,basedongeneticpotentialasevidencedbyparentalheight,oronpriorgrowthrecordsshowingaclearslowingoflineargrowth.
Asaresult,cliniciansshouldanticipateperhapshavingtoaimforhighertreatment
goalweightsoradjustingEBWoncelineargrowthreturnstonormal.Second,it
iscrucialtoacknowledgethatthecutpointsstudiedhere,

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 68/86
althoughcommonlyusedinclinicalpractice,arearbitraryandshouldnotbeseenasabsoluteindicatorsofillnessorhealth.Forexample,hospitalizationis
notindicatedonlywhenweightisbelow75%EBW,andtheDSM-IVTRcut
pointof85%EBWwasinitiallyintendedasanexamplebutisoften
mistakenlyreifiedintoaconcretecutpoint.TheDSM-5Eating

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 69/86
DisorderWorkgroupspecificallynotedthatforclinicalpurposes,itwouldbeundesirabletosettleonaspecificnumericalstandard forweightforAN.16Finally,
weconsidered3methodsforEBWcalculation,whereasothersstillinuse(see,
eg,refs17and18)werenotincludedinthiscomparison.
CONCLUSIONS
Thisstudyrepresentsafirststepto

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 70/86
examinethelevelofagreementand/ordisagreementbetweentheBMI,McLaren,andMooremethods,andfutureresearchshouldinvestigatetheirperformance;thatis,
canthesemethodsbedelineatedonwhetheroneis
morepredictive
ofknownbiologicalmeasuresoflowweight,suchasbloodpressureorbody
temperature.Ourfindingswarrantsomeclosingconsiderations.First,cliniciansshould

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 71/86
refrainfromtalkingaboutideal weightorexpressingthistargetwithunrealisticaccuracy(eg,2decimalpoints).Itismoreinformativetousethe
termsaverage ormedian, ashasbeensuggestedbyothers,19orexpected as
weindicatehere,whenreferringtoreferenceweight.Second,itisimperativethat
theresearchandclinicalcommunitiesattemptacommonlanguageby

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 72/86
statingtheirmethodforEBWcalculationandstandardizingunitsofmeasurement(eg,kilogramsratherthanpounds).Basedonthisstudy,wewouldrecommendthe
BMImethodwhenassessingthepediatricandadolescenteatingdisorderspopulation.Third,the
useofanelectronicmedicalrecordthatincludesBMIchartsaspartof
pediatricsoftwarepackagesshouldbeencouraged.20Removingthebarrierof

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 73/86
calculatingBMIbyhandistimeandcostefficientinpediatricpractice.Finally,andinreferencetoarecentreportfromtheAmericanAcademy
ofPediatrics,21pediatriciansareattheforefrontintermsofdiagnosingeatingdisorders
andshouldthereforeroutinelycalculateandplotpatients weight,height,andBMIon
appropriateageandgendercharts.Pediatriciansshouldpaycloseattention

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 74/86
todeviationsfromanindividualchildsgrowthcurve(ie,fallingoffpersonaltrajectory)assuchpersonalizedgrowthcurvesprovideconsiderablesupportinthedetermination
ofhealthytargetandpotentiallyimproveearlyidentificationofeatingdisorders.
ACKNOWLEDGMENT
ThisstudywassupportedbygrantNRSAT32MH082761
fromtheNationalInstitutesofHealth.
LEGRANGE

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 75/86
etal
Downloaded from pediatrics.aappublications.org at Indonesia:AAP Sponsored on January 27, 2012

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 76/86
ARTICLEARTICLEREFERENCES
1.AmericanPsychiatricAssociation.DiagnosticandStatisticalManualofMentalDisorders,Revised4thed.Washington,DC:AmericanPsychiatricAssociation;
20002.GoldenNH,KatzmanDK,KreipeRE,etal;SocietyforAdolescent
Medicine.Eatingdisordersinadolescents:positionpaperoftheSocietyforAdolescentMedicine.
JAdolescHealth.2003;33(6):4965033.GoldenNH,JacobsonMS,Sterling

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 77/86
WM,HertzS.Treatmentgoalweightinadolescentswithanorexianervosa:useofBMIpercentiles.IntJEatDisord.2008;41(4):3013064.RomeES,
AmmermanS,RosenDS,etal.Childrenandadolescentswitheatingdisorders:the
stateoftheart.Pediatrics.2003;111(1):e98e1085.CouturierJ,LockJ.Whatis
remissioninadolescentanorexianervosa?Areviewofvariousconceptualizations

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 78/86
andquantitativeanalysis.IntJEatDisord.2006;39(3):1751836.HebebrandJ,WehmeierPM,RemschmidtH.Weightcriteriafordiagnosisofanorexianervosa.AmJPsychiatry.2000;157(6):10247.
YagerJ,PowersPS.ClinicalManualofEatingDisorders,1sted.Washington,DC:
AmericanPsychiatricPublishing;2007:4628.LantzouniE,FrankGR,GoldenNH,ShenkerRI.
Reversibilityofgrowthstuntinginearlyonsetanorexianervosa:a

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 79/86
prospectivestudy.JAdolescHealth.2002;31(2):1621659.KuczmarskiRJ,OgdenCL,Grummer-StrawnLM,etal.CDCgrowthcharts:UnitedStates.AdvData.2000;(314):127
10.HebebrandJ,HimmelmannGW,HesekerH,SchaferH,RemschmidtH.Useof
percentilesforthebodymassindexinanorexianervosa:diagnostic,epidemiological,andtherapeutic
considerations.IntJEatDisord.1996;19(4):35936911.HebebrandJ,Casper

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 80/86
R,TreasureJL,SchweigerU.Theneedtorevisethediagnosticcriteriaforanorexianervosa.JNeuralTransm.2004;111(7):82784012.McLarenDS,ReadWWC.
Classificationofnutritionalstatusinearlychildhood.Lancet.1972;2(7769):14614813.MooreDJ,Durie
PR,ForstnerGG,PencharzPB.Theassessmentofnutritionalstatusinchildren.Nutr
Res.1985;5:79779914.PhillipsS,EdlbeckA,KirbyM,Goday

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 81/86
P.Idealbodyweightinchildren.NutrClinPract.2007;22(2):24024515.FairburnCG,CooperZ.Theeatingdisordersexamination.In:FairburnCG,WilsonGT,
eds.BingeEating:Nature,Assessment,andTreatment,12thed.NewYork,NY:Guilford
Press;1993:317360
16.AmericanPsychiatricAssociation.DSM-5development.Availableat:www.dsm5.org/
ProposedRevisions/Pages/proposedrevision.aspx?rid=24.AccessedOctober20,201117.HamillPV,Drizd

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 82/86
TA,JohnsonCL,ReedRB,RocheAF,MooreWM.Physicalgrowth:NationalCenterforHealthStatisticspercentiles.AmJClinNutr.1979;32(3):60762918.Hamwi
GJ.Therapy:changingdietaryconcepts.In:DanowskiTS,ed.DiabetesMellitus:Diagnosisand
Treatment.Vol.1.NewYork,NY:AmericanDiabetesAssociation;1964:73 7819.PeeblesR,Hardy
KK,WilsonJL,LockJD.Arediagnosticcriteriaforeating

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 83/86
disordersmarkersofmedicalseverity?Pediatrics.2010;125(5):e1193e120120.BordowitzR,MorlandK,ReichD.Theuseofanelectronicmedicalrecordtoimprovedocumentation
andtreatmentofobesity.FamMed.2007;39(4):27427921.RosenDS;AmericanAcademyof
PediatricsCommitteeonAdolescence.Identificationandmanagementofeatingdisordersinchildrenand
adolescents.Pediatrics.2010;126(6):12401253PEDIATRICSVolume129,Number2,February

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 84/86
2012
Downloaded from pediatrics.aappublications.org at Indonesia:AAP Sponsored on January 27, 2012

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 85/86
Calculation of Expected Body Weight in Adolescents With Eating Disorders
Daniel Le Grange, Peter M. Doyle, Sonja A. Swanson, Kali Ludwig, Catherine Glunz and Richard E. KreipePediatrics; originally published online January 4, 2012;DOI: 10.1542/peds.2011-1676
ServicesUpdated Information &/peds.2011-1676http://pediatrics.aappublications.org/content/early/2012/01/02including high resolution figures, can be found at:Subspecialty Collections
_medicinehttp://pediatrics.aappublications.org/cgi/collection/adolescentAdolescent Medicinethe following collection(s):This article, along with others on similar topics, appears inPermissions & Licensingtmlhttp://pediatrics.aappublications.org/site/misc/Permissions.xh
tables) or in its entirety can be found online at:Information about reproducing this article in parts (figures,Reprintshttp://pediatrics.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthlypublication, it has been published continuously since 1948. PEDIATRICS is owned, published,and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, ElkGrove Village, Illinois, 60007. Copyright © 2012 by the American Academy of Pediat
rics. Allrights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.
Downloaded from pediatrics.aappublications.org at Indonesia:AAP Sponsored on January 27, 2012

7/26/2019 Pediatrics 2012 Le Grange Peds.2011 1676
http://slidepdf.com/reader/full/pediatrics-2012-le-grange-peds2011-1676 86/86