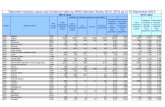
Pediatric vaccination 17/pop.pdfTetanus Cases Reported in ThailandTetanus Cases Reported in Thailand...
69
Pediatric vaccination Pediatric vaccination Pediatric vaccination รศ รศ . . นพ นพ . . ภพ ภพ โกศลารักษ โกศลารักษ ภาควิชากุมารเวชศาสตร ภาควิชากุมารเวชศาสตร คณะแพทยศาสตร คณะแพทยศาสตร มหาวิทยาลัยขอนแกน มหาวิทยาลัยขอนแกน
Transcript of Pediatric vaccination 17/pop.pdfTetanus Cases Reported in ThailandTetanus Cases Reported in Thailand...

Pediatric vaccinationPediatric vaccinationPediatric vaccination
รศรศ..นพนพ..ภพภพ โกศลารักษโกศลารักษ
ภาควิชากุมารเวชศาสตรภาควิชากุมารเวชศาสตร
คณะแพทยศาสตรคณะแพทยศาสตร
มหาวิทยาลัยขอนแกนมหาวิทยาลัยขอนแกน

Pediatric vaccination
• Basic knowledge
• Pitfalls in EPI vaccines
• Optional vaccines
• Questions and Answers

Host Defense Mechanism
• Physicoanatomical barrier
• Phagocytosis– Circulating phagocytosis e.g. PMN
– Fixed phagocytosis e.g. macrophage
• Reticuloendothelial system
• Humoral factors– Complement and properdin system
– Humoral immunity e.g. immunoglobulin
• Cell-mediated immunity

Immunization• Passive• Active
: vaccination

Active immunizationLive Vaccine : BCG, OPV, MMR, Var, Oty
Killed vaccine : pertussis, JE, Rabies, HAV
Toxoid : diphtheria, tetanus
Subunit (recombinant) : HBV, Influenza, Acel-P
Polysaccharide : Pnc, Meningococcal, Ty
Conjugated polysaccharide : Hib, Pnc

Active immunizationOral: OPV, Oral typhoid
Intramuscular: HBV, HAV, DTP, Rabies, Hib,
Influenza, Typhoid
Subcutaneous: MMR, Varicella, JE, Ty, Hib,
Influenza
Intradermal: BCG, Rabies

Injection Site for Vaccination• Vaccines should not be injected on the hip area
• Infants and young children: antero-lateral of mid-thigh
• Older children: deltoid

Vaccination - Aims
• Short term
: Prevention – individual, risk group
• Long term
: Eradication
: Smallpox, Polio, Measles, HBV

Vaccination• Mimic natural infection• Low adverse events• Protection
: antibody, antitoxin, CMIR: short term – killed vaccine: long term – attenuated vaccine

Pitfalls in EPI vaccines
• Vaccine schedule• Adverse reaction• Vaccine information system

Optional Immunization Schedule for Thai Children
Optional Immunization Schedule for Thai Children
Birth 1M 2M 4M 6M 9M 18M 4-6Y
BCG
HBV1 HBV2 HBV3
DTP1 DTP2 DTP3
OPV1 OPV2 OPV3
DTP4 DTP5
OPV4 OPV5
MMR1
JE1,2, 3, (4)
MMR2
ThendT q 10 yrs

Optional Immunization Schedule for Thai Children
Optional Immunization Schedule for Thai Children
2M 4M 6M 12M 18M 4-6Y 6Y 10-12Y
VarHib1 Hib2 (Hib3)
HAV1,2
DTaP1 DTaP2 DTaP4DTaP3 DTaP5, dTap
IPV1 IPV2 IPV3 IPV4
Var may give at >12 M
HAV may give at >12 M
dTap q10y

Rate of ReactogenicityRate of Rate of ReactogenicityReactogenicity
0102030405060708090
100
BCG Hib HBV M/MMR OPV T/DT DTP
Local Fever other systemic
Perc
ent

Summary of Rare, Serious vaccine Reactions, Onset and Rates
Summary of Rare, Serious vaccine Reactions, Summary of Rare, Serious vaccine Reactions, Onset and RatesOnset and Rates
Vaccine Reaction Onset Rate per 1 million doses
BCG SuppurativelymphadenitisBCG osteitisDisseminated BCG-it is
2-6 m1-12 m1-12 m
100-1,0001-700
2
HBV AnaphylaxisGBS (plasma-derived)
0-1 hr1-6 wks
1-25
Measles/MMR
Febrile seizureThrombocytopeniaAnaphylaxis
5-12 d15-35 d0-1 hr
33333
1-50
OPV VAPP 4-30 d 1.4-3.4*
WHO/V&B/00 36* VAPP: high risk in 1st dose

Summary of Rare, Serious vaccine Reactions, Onset and Rates
Summary of Rare, Serious vaccine Reactions, Summary of Rare, Serious vaccine Reactions, Onset and RatesOnset and Rates
Vaccine Reaction Onset Rate per 1 million doses
DTP Persistent screaming (>3 hr)SeizureHHEAnaphylaxis/shockEncephalopathy
0-24 hr0-3 d
0-24 hr0-1 hr0-3 d
1,000-60,0000570570200-1
JE Serious allergic reactionNeurological event
2 wk 10-1,0001-2.3
TT Brachial neuritisAnaphylaxisSterile abscess
2-28 d0-1 hr1-6 wk
5-101-6
6-10
WHO/V&B/00 36

Arthus’ ReactionArthus’ Reaction

BCG LymphadenitisBCG Lymphadenitis

BCG Complications
BCG should not be given at buttock or hip:
- irritation from diaper- contamination with urine/stool- difficult to examine scar

Multiple BCG Does Not Confer Better Immunity

More Local Reaction from Repeated BCG
MOPH no longer give second BCG unless there is no document of BCG at birth and no scar

Urticaria Following JE Vaccine
Next dose can be given in those experienced non immediate reaction
But need careful observation post vaccination!

อัตราความครอบคลุมโดยเฉลี่ยของวัคซีนในงานสรางเสริม
ภูมิคุมกันโรคในประเทศไทย
วัคซีน รอยละ
บีซีจี 99
คอตีบ-บาดทะยัก-ไอกรน (ดีทีพี) ครั้งที่ 3 98
โปลิโอ ครั้งที่ 3 98
ตับอักเสบบี ครั้งที่ 3 96
หัด 96
บาดทะยักในหญิงมีครรภ (2 ครั้งหรือกระตุน) 93
ไขสมองอักเสบครั้งที่ 2 87
จากการสํารวจดวยวิธี cluster survey โดยกรมควบคุมโรค พ.ศ.2546

Impact of VaccinationImpact of
Vaccination

Tetanus Cases Reported in ThailandTetanus Cases Reported in Thailand
0
5
10
15
20
25
1977
1980
1983
1986
1989
1992
1995
1998
2001
Case/100,000
Death%

Pertussis Cases Reported in ThailandPertussis Cases Reported in Thailand
0
2
4
6
8
10
12
1977
1980
1983
1986
1989
1992
1995
1998
2001
Case/100,000
Death%

Measles Cases Reported in ThailandMeasles Cases Reported in Thailand
0
20
40
60
80
100
1977
1980
1983
1986
1989
1992
1995
1998
2001
Case/100,000
Death%

EncephalitisEncephalitis
0
5
10
15
20
25
30
1977
1980
1983
1986
1989
1992
1995
1998
2001
Case/100,000
Death%

Optional vaccines
• Increase immunogenicity in infant: conjugated vaccine: H. influenza B, PCV, Meningococcus
• Less adverse event: IPV, acellular pertussis, rotavirus
• New vaccines: HPV, rotavirus: Varicella, HAV

Pichichero M. Consultant for Pediatricians 2005;June:263-7.
PolysaccharideConjugate Property
NoYesLack of hyporesponsiveness
NoYesBooster effect
NoYesPersistence of protection
NoYesHerd immunity
NoYesReduction of nasopharyngeal carriage of bacteria
NoYesImmune memory
NoYesT-cell-dependent immune response(response by children < 2 yo)
Comparison of Polysaccharide and Conjugate Vaccines

Rosenberg N.M. NEJM 2001;345(14):1042-53.
Principle of Polysaccharide-Protein Conjugate VaccinePrinciple of Polysaccharide-Protein Conjugate Vaccine

PCV-7 (Pneumococcal conjugated vaccine)
4 18C6B 19F9V 23F14
ConjugateNon-toxicdiphtheriavariant(CRM197)protein
Cover 71-86% of isolates from invasive disease in EU, US < 2yo.

1997
1998
1999
2000
2001
2002
2003
2004
2005
0
50
100
150
200
250<112-4
Year
IPD
rat
e / 1
00 0
00
http://http://www.cdc.gov/ncidod/dbmd/abcs/survreports.htmwww.cdc.gov/ncidod/dbmd/abcs/survreports.htm
PCV7PCV7
Impact on Invasive Pneumococcal Diseases

Centers for Disease Control and Prevention. MMWR 2005;54:893-7.
Routine use of PCV in 2000

Pneumococcal Disease Burden in ThailandA prospective study of meningitis in Lampang and Phisanulok:
Population < 5 yo = 105,269
N Rate/105<5yo
Potential meningitis (LP) 598 568Probable meningitis 28 26Laboratory confirmed 7 6.7
Hib 4 3.8 (1.0-9.7)
N.meningitidis 2 <3S.pneumoniae 1 (+1 pos H/C) <3
ATB detected in CSF 20/455 (4.4%)
Rerks-Ngarm S. Vaccine 2004;22:975-83.

Coverage of Invasive Pneumococcal Isolates by PCV in Thai Children 2000-2005
Collaborative study: Siriraj, NIH, Chula, Bhumipol, QSNICH
0
20
40
60
80
100
7-valent 9-valent 11-valent 13-valent
<1yo
<2yo
<5yo
Cover by:
%
N=11571 69
74 7476 76 7476 7785 86 88
Wanatpreeya Phongsamart, et al. Vaccine 2007; 25:1275-80

Bacterial Meningitis in Thai Children Etiology and Mortality (N=618)
Bacterial Meningitis in Thai Children Etiology and Mortality (N=618)
Chotpitayasunondh C. Southeast Asian J Trop Med Public Health 1994;25:107-115.
%
Hib S.pneumo N.mening Salmonella Others0
5
10
15
20
25
30
35
40Proportion Mortality

PCV
• Vaccine schedule: 2, 4, 6, 12-15 months

Rotavirus

Pathogenesis Rotaviruses adhere to the GI tract epithelia
(jejunal mucosa)
Atrophy of the villi of the gut
* *
Loss of absorptive area
Flux of water and electrolytes
NSP4 viral enterotoxin
Enteric nervous system activation
VOMITING AND
diarrhoea
*Rotavirus infection in an animal model of infection. Photographs are from an experimentally infected calf. Reproduced with permission from Zuckerman et al, eds. Principles and Practice of Clinical Virology. 2nd ed. London: John Wiley & Sons; 1990:182.
Micrographs courtesy of Dr. Graham Hall, Berkshire, UK.

Epidemiology- Global Perspective
Bacteria
Unknown Rotavirus
Calicivirus
Rotavirus
Escherichia coli
Parasites
Otherbacteria
Developed Countries
Adenovirus
CalicivirusAstrovirusAdenovirus
Astrovirus
Unknown
Less Developed Countries
From Kapikian AZ, Chanock RM. Rotaviruses. In: Fields Virology 3rd ed 1996; 1659. Philadelphia, PA: Lippincott-Raven.
Distribution of pathogens reported to cause endemic/epidemic gastroenteritis & infantile vomiting & diarrhea

Estimated global burden of rotavirus disease
24 million outpatient visits
114 million domiciliary episodes
1 : 205
1 : 50
EventRisk of Particular Event
611,000 deaths
2.4 million inpatient visits
1 : 5
1 : 1
Rotavirus- Burden of Disease
Glass R, et al. Lancet 2006; 368: 323–332.

Rotavirus Disease Burden in ThailandRotavirus Disease Burden in Thailand
56,000 rotavirus diarrhea inpatient visit
131,000 rotavirus diarrhea health care visit
586,000 Rotavirus diarrhea episode
4.8 million diarrhea episodes(in children < 5 yo)
1 : 85
1 : 36
1 : 8
1 : 1
Risk Events
Jiraphongsa C et al. JID 2005: 192 (suppl 1)May be underestimated!
2001-3, of the 1095 stools from hospitalized
diarrhea, rotavirus positive in 838 (43%)



0
5
10
15
20
0 10 20 30 40 50 60 70
RotaShield™ RIX4414/placebo
Occurrence of Definite IS Cases Compared with RotaShield™-associated Cases
V = VaccineP = Placebo
VP P
P PV V
VVP
VP P
Dose one
Dose two
V PVP P
P P P
IS cases
IS cases
75 83
107 145
VP
P P
1. Murphy TV, et al. N Engl J Med 2001;344(8):564−72. 2. Vesikari T, et al. 23rd Annual Meeting of the European Society for PaediatricInfectious Diseases−ESPID, Valencia, Spain, 18−20 May 2005.
0
5
10
15
20
0 10 20 30 40 50 60 70

Recommendation for Use of Rotavirus Vaccines
Pentavelent (HBRV) Monovalent (HRV)
Route Oral OralAge of 1st dose 6-12 week > 6 weekGeneral schedule 2, 4, 6 mo 2, 4 moInterval of dose 4-10 week >4 weeksAge of last dose 32 week 24 weeksConcurrent OPV not mention 14 d apart for 1st doseOther concurrent vac OK OKBreast feeding OK OKContraindication Immunocommpromised, age out-of-range
allergic to vaccine/component, Ac illness

Rotavirus vaccine
• high protection against severe RVGE
– 85%–100% efficacy against all rotavirus GE-
related hospitalizations
Efficacy

HPVHPV
• About 100 types• 16,18 accounted for 70% of cervical cancer• 6,11 accounted for 90% of genital warts• Mostly infected in late teens and early 20• By 50 year of age, 50% infected.• Acquire mainly from sexual contacts (insertive &
non-insertive)

Numbers of cases for each continent represent the annual incidence of cervical cancer. Pie charts show the proportion of cases caused by HPV-16 or HPV-18. Data are from the
Globocan 2002 database (www-dep.iarc.fr/globocan/database.htm).
Agosti JM. NEJM 2007;356:1908-10.

Schiffman M et al. Arch Path Lab Med. 2003;127:930–4
Peto, J., et al. (2004) Cervical HPV infection and neoplasia in a large population-based prospective study. British Journal of Cancer, 91: 942-953.
30% of dysplasia progress to cervical cancer over 10 –15 years
Type 16, 18 are > 70% of
oncogenictypes

HPV L1 VLP Vaccines CandidateHPV L1 VLP Vaccines Candidate
MSD• Quadrivalent• 16,18 and 6,11 (cause 90% of
genital warts)• Made in Yeast• Adjuvant:
– Aluminium• Schedule: 0, 2, 6 M
GSK• Bivalent• 16,18 • Made in Baculovirus• Adjuvant:
– AS04• Schedule: 0, 1, 6 M
L1 gene on HPV
DNA
Recombinant L1 protein produced in yeast or Baculovirus, then assemble into virus-like particles

IncidentPersistent
cytologyCIN lesions
Efficacy Data (HPV-001) HPV 16 and/or 18 Cervical Protection (GSK)
Efficacy Data (HPV-001) HPV 16 and/or 18 Cervical Protection (GSK)
Prevention of HPV-16/18 related infection & lesions
D. Harper et al, Lancet, 2004, 364 : 1757
50556065707580859095
100
ATP
V
91%100% 93% 100%
acci
ne E
ff ica
cy %
ITT

Phase 2 Trial of a Quadrivalent HPV Vaccine (MSD): Modified Intention of Treat (MITT) Efficacy
Phase 2 Trial of a Quadrivalent HPV Vaccine (MSD): Modified Intention of Treat (MITT) Efficacy
Villa LL et al. Lancet Oncol 2005; 6:271-8.
0102030405060708090
100
PersistentInfection
HPV-RelatedDisease
CIN Overall
% V
acci
ne E
ffica
cy
88%100%
89%100% Overall Efficacy:

Summary for HPVSummary for HPV• The vaccine cover for only 70% of cancer types (and 90%
wart types), still need Pap’s smear and risk reduction• Both vaccines are very effective against type specific
persistent infection/ sequelae, but do not treat infection that have occurred
• The best time to vaccinate is before getting infection• To give vaccine (9-26 yo.)
– No need to pre-screen– Can give to anyone regardless of prior HPV infection – Can give to immunocompromised– Can give to nursing mother– Should defer in pregnancy

Children’s Vaccine Initiative’s
“Ideal Vaccine”Children’s Vaccine Initiative’s
“Ideal Vaccine”• Oral• 1 - 2 doses• Early in life• Well tolerated
• Efficacious 100%• Safe• Can be administered:
- According to local schedule- With other vaccines
• Heat Stable• Affordable
The current vaccines:2-3 dosesExpensiveEfficacy 70-90%Heat sensitiveInterfered by OPV
World Health Forum 1992; 13 (1):93

Questions and Answer

Thank you

จํานวนผูปวยโปลโิอและความครอบคลมุ OPV3 ป 2504-2546
http://dpc7.ddc.moph.go.th/myoffice/sovo/physician_train/Polio%20Eradication%20Thailand%20170604.pdf
Last caseIn 2540

Advantages and Disadvantages of Different Poliovirus Vaccination Schedules
Vaccination ScheduleAttribute OPV only IPV only IPV/OPV
VAPP Yes No FewSystemic immunity High High HighMucosal immunity High Lower HighSecondary transmission Yes No SomeExtra injections or visits No Yes YesCompliance High Pos reduced Pos reducedFuture combination vaccine Unlikely Likely LikelyCost Low Higher Intermediate

Inactivated or Oral Poliomyelitis Vaccine
Wild polio virus OPV
No wild virus, Clinical Polio OPV
No lab or clinical polio IPV, OPVWild polio in neighboringcountries
Polio-free in whole region IPV
Polio eradication No vaccine

Carrier Rate in Infants Born toHBsAg+, HBeAg+ Mothers
Percent carriers
No prophylaxis 90HBIG one dose after birth 51HBIG 3 doses 23HB vaccine 3 doses start at one month 40HB vaccine 3 doses start at one week 25HB vaccine 3 doses start at one day 10HBIG at birth + HB vaccine 3 doses 5

Bacterial Meningitis in Children’s Hospital
Organism No. Percent
H. influenzae b 321 36.2%S. pneumoniae 172 19.4%Salmonella spp. 110 12.4%N. meningitides 28 3.2%E. coli 34 3.8%Pseudomonas spp. 37 4.2%Gr. B Streptococcus 22 2.5%Others 55 6.2%No growth 108 12.2%
Total 887 100%
1980-1997

ANTI-PRP AND H. INFLUENZAE MENINGITIS BY AGE
(S.Lolekha.)
0
20
40
60
80
100
120
<1 1-2 3-4 5-6 7-8 9-10 11-23
2 3 4 5 6-10
Months Years
Perc
ent p
ositi
ve
0
5
10
15
20
Meningitis anti-PRP Cases

HIB INCIDENCE* (<5 years)* Cases / 100,000 population per year
Hib meningitis Other HibUSA- Arizona : - Indians- Arizona : - natives
- non-native
25428269
-
601129
USASenegalSwedenAustralia - Aborigine
- AdelaideFinlandHongKong
19-636027
45030271.7
-
-
-
-
-
-
0.9

Incidence of Hib Meningitis in Thailand
• P. Sunakorn (1990-1995)– 157 cases of Hib meningitis
– 5.8/100,000/year
• S. Wattanasri (1990-1993)– 550 cases of meningitis, 43% Hib
– 5.2/100,000/year

Incidence of Hib Meningitis inChiangrai and Pitsanulok Jan-Dec 2000
• 511 cases have CNS symptoms
• Lumbar puncture 429 cases, 427 tested– culture 425, Latex 420, PCR 182
• Hib 3, S. pneumoniae 4, Meningo 1
• Others 10 (5 cases contaminated)
• Not LP 82 cases, meningitis 1 case
• Not enrolled 49 cases, likely meningitis 2
• 120,000 children under 5 years
• Incidence of Hib meningitis 2.5/100,000/yr

SOCIO-ECONOMIC RISK FACTORS FOR INVASIVE HAEMOPHILUS INFLUENZAE TYPE B DISEASES
• Day care attendance: 1.9-11• Crowding: 1.0-18• Presence of siblings
younger than school age: 0.9-5.8 • Previous hospitalizations: 1.0-3.4• Previous otitis media: 1.2-3.9• Bottle feeding
(Takala AK J Infect Dis 1992;165(Suppl 1):11-15)

GMT of Anti-PRP Before and After PRT-TCombined VS Separate Site of Injection
0.5 0.5
46
23.9
33.6
0
5
10
15
20
25
30
35
2 Mo 6 Mo 7 Mo
CombinedSeparate
GMT (microgram/ml)
AgeLolekha S. et al J Trop Pediatr. 2001;47:24-9

Kyaw MH. NEJM 2006;354:1455-63.
<< Those Caused by Penicillin-Nonsusceptiblestrains in > 2 yo
<<Among Children < 2 yo.
Annual Incidence of Invasive Pneumococcal
Disease in US
Annual Incidence of Invasive Pneumococcal
Disease in US