Pediatric Skull Xray Heather Patterson August 2, 2007.
42
Pediatric Skull Xray Heather Patterson August 2, 2007
-
Upload
rianna-winger -
Category
Documents
-
view
216 -
download
0
Transcript of Pediatric Skull Xray Heather Patterson August 2, 2007.

Pediatric Skull Xray
Heather Patterson
August 2, 2007

Objectives
• Brief review of anatomy• Approach to pediatric skull xray• Examples

Skull fractures
• Common in non-accidental trauma– 80% in first year– Rare after 2y of age

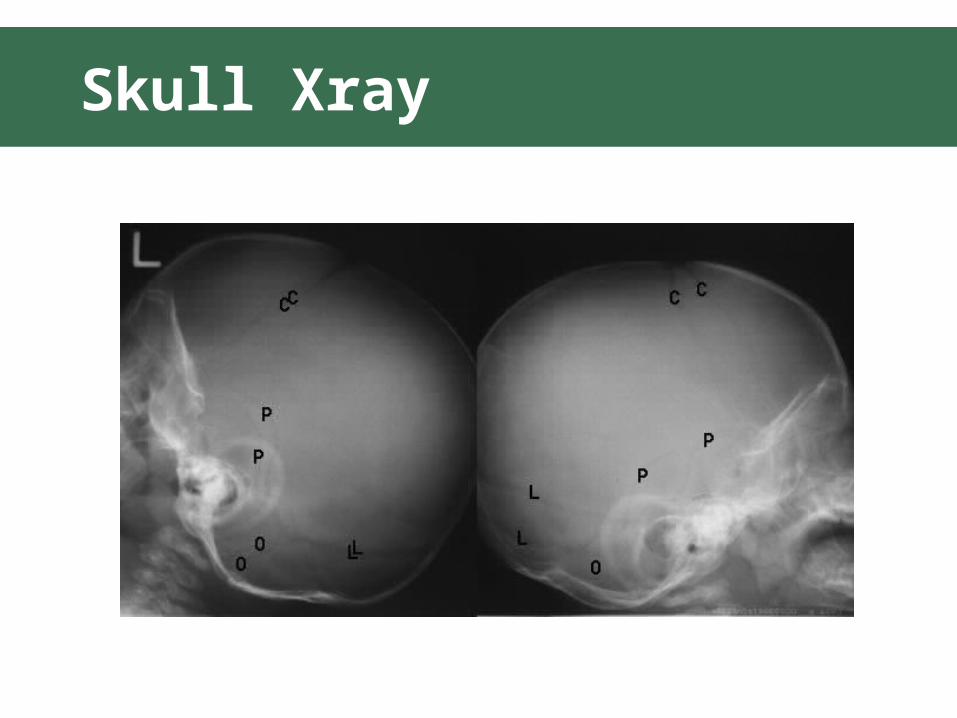
Anatomy

Anatomy

Skull Xray
• Full series 3-4 views– AP– Towne’s view (AP with neck flexed)– Lateral x 2

Skull Xray

Skull Xray

Skull Xray
Skull Xray

Approach
• Follow cortex • Identify suture lines• Identify abnormal lines

What is the big deal?
• Risk of “growing fracture”– Leptomeningeal cysts– Long term sequelae

Growing fracture/Leptomeningeal
Cyst• Rare
– <1% of skull fractures
• Pathophys– Dural deal with herniation of pia and
arachnoid through tear– CSF pulsations lead to erosion of bone– Diastasis of fracture over time

Growing fracture/Leptomeningeal
Cyst• Imaging
– Angular, linear lytic lesion– Scalloped margins
• Management– f/u with neurosurgery– Early intervention as needed

Case 1

Case 1

Case 1
• Linear fracture R posterior parietal and occipital bones
• Extends through lambdoid suture

Case 2

Case 2
• R parietal skull fracture

Case 3

Case 3

Case 3
• Linear fracture R occiput

Case 4

Case 4

Case 4
• Depressed skull fracture posterior right parietal bone
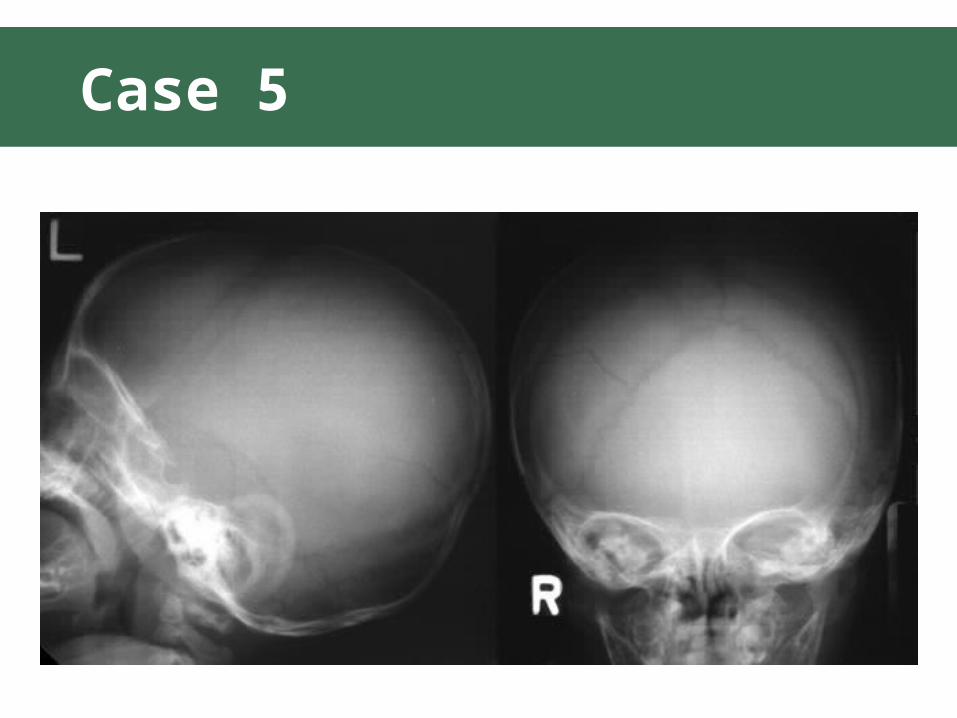
Case 5

Case 5
• R parietal fracture • Communicates
with lamboidal suture

Case 6

Case 6

Case 6
• R parietal fracture

Case 7

Case 7

Case 7
• L parietal fracture

Case 8

Case 8
• Persistent skull defect
• Encephalomalacic cystic defect– Consistent with
leptomeningeal cyst

Uganda

Uganda

Uganda

Uganda

Uganda

Uganda

Uganda