
Pediatric Safety and Prevention. Improving child health “health maintenance” “preventive...
52
Pediatric Safety Pediatric Safety and Prevention and Prevention
-
Upload
ashley-quinn -
Category
Documents
-
view
216 -
download
0
Transcript of Pediatric Safety and Prevention. Improving child health “health maintenance” “preventive...

Pediatric Safety Pediatric Safety and Preventionand PreventionPediatric Safety Pediatric Safety and Preventionand Prevention

Improving child health
• “health maintenance”
• “preventive health”

Health PromotionHealth Promotion

Immunizations• Effective in decreasing childhood infectious diseases.
• Center for Disease Control (CDC) and American Academy of Pediatrics recommend that children be immunized against 14 communicable diseases before they reach 2 years of age.
• R Risks are outweighed by the life- • saving effects of immunizations.

Immunizations
• Specific recommendations by APA:– Minor infections without fever are not
contraindication– If reaction occurs, consult dr. before
next immunization– Pertussis not give for children over 6

Immunization Schedule
4mos-6 yrs of age:• DTaP (4 doses)• IPV (3 doses)• HepB (3 doses)• MMR (@ 12 months)• PCV (1 dose)
7-18 yrs of ageTd (every 10
years after initial immunizations)
IPV (not rec. if >18 yrs of age)


Nursing Responsibilities
• Review immunization schedule for updates• Know storing and handling requirements for all vaccines• Know the action of the vaccine• Know administration routes, dosages, sites and technique• Aspirate with each injection• May have multiple injections on same day, • just be sure to give in separate sites
•
Nursing Responsibilities• Prior to administration, assess if immunocompromised
people are in the household (discuss with M.D. alternatives to live virus)
• Obtain careful history. Children should have their immunization status assessed during all health care visits, hospitalizations, and in school. If immunizations are not current, arrange to update them
• Assess if any reactions to past vaccines or any • allergies to eggs.

Nursing Responsibilities• Have parents sign permit with educational instructions.
• Document - Record lot# and manufacturer of vaccine; patient reaction
• Advise parents of side effects. Teach use of antipyretics for fever. If fever persists for >than 24 hours, or has other concerns - call M.D.
• Teach use of cold compresses to injection sites for first 24 hours, then warm compresses

Do Not Forget!Do Not Forget!
• Assess for reaction 15-30 min after injection
• Epinephrine 1:1000 available• Check immunization records with
each visit• Parent teaching: fever, or other
symptoms

Prevention of InjuriesPrevention of Injuries

Definitions
• Mortality- the # of deaths/100,000
• Morbidity- used to express the ratio of sick to well in a community
• Infant mortality- # of children per 1000 live births who die before 1st birthday

Major causes of death during infancy and childhood (these represent death rates for the ages of 1-14 yrs per 100,000)
• Accidents• Congenital abnormalities• Cancer• Homicide• Heart disease• Pneumonia & influenza• Suicide• Human immunodeficiency disease

Injuries
• Injuries are a major cause of death in children.
• All children are at risk for injury because of their normal curiosity, impulsiveness, and desire to master new skills.


INFANT
• SIDS• Motor Vehicle• Infections• Dehydration• Respiratory Problems• Child abuse
TODDLER• Injuries: MVA• Toddler fracture• Poisoning• Foreign Body airway obstruction• Asthma, Croup, Respiratory problems• Vomiting, Dehydration• Child Abuse

PRESCHOOL
• Motor Vehicle -- Bicycle• Trauma• Poisoning• Asthma, Respiratory infections• Drowning• Child Abuse

SCHOOL AGE
• Motor vehicle: pedestrian - vehicle; bike - vehicle
• Sports injuries

ADOLESCENT
• Trauma• Motor Vehicle• Knife and gunshot wounds• Pregnancy complications• Suicide• Poisoning• Drowning

Common Safety Common Safety ProblemsProblems
Common Safety Common Safety ProblemsProblems
Injury Prevention MeasuresInjury Prevention Measures

Common Safety Problems
• Aspiration• MVA• Burns• Drowning• Bodily injury/fractures

Aspiration
• Asphyxiation by foreign material in respiratory tract is leading cause of fatal injury in children under 1 year of age.
• Puts everything in mouth
• Very interested in body and newly found openings

Aspiration – Preventive Measures
• Carefully inspect toys for potential danger / removable parts.
• Keep small objects out of reach, floors free of objects
• Do NOT feed hard candy, nuts, food with pits or seeds, circular pieces of hot dogs
• Hold infant for feeding, do NOT prop bottle
• Use pacifier with one-piece construction and loop handle.

Motor Vehicle Accident
• Vehicle – children improperly restrained• Pedestrian
– Walking, running, especially after objects thrown into street
– Poor perception of speed, lack of experience to foresee danger
– Able to open doors and gates and get outside– Children often unseen because of small size, can be run
over by car backing out of drive. – Ride toys, bikes in path of danger

Motor Vehicle AccidentsPreventive Measures
– Use federally approved car restraints– Supervise child while playing outside. Do not allow playing behind cars. Supervise riding of toys, bikes.– Lock fences, gates, doors– Teach to obey pedestrian safety rules

Burns
• Children are inquisitive and will pull pots off stove, plays with matches, inserts
objects into wall sockets• They can climb - reaches stove, oven, ironing board
and iron, cigarettes on table• Unaware of sources of heat or• fire

Burns - Preventive Measures
• Turn pot handles toward back of stove, place guardrails in front of radiators, fireplaces, stoves.• Store lighters and matches in locked container• Cover electrical outlets with protective covers.
Keep electrical cords hidden• Check bath water. Do not allow • child to play with faucet

Drowning
• Child does not recognize danger of H2O
• Unaware of inability to breath underwater
• No conception of water depth• Has curiosity about water
Hypoxia greatest concern

Drowning – Preventive Measures
• Fence around pools , have self-locking gate
• Supervise when near water sources• Keep bathroom doors closed and toilet seat down• Teaching swimming and water safety

Bodily Harm - Fractures
• Like to climb, run, jump• Still developing sense of balance• Easily distracted from tasks and hurt self• Able to open doors and windows• Poor depth perception

Bodily Harm – Prevention Measures
• Keep screens in the windows and locked• Place gates at top and bottom of stairs• Apply non-skid decals in bathtub or shower• Remove unsecured rugs, scatter rugs• Never leave unattended in shopping cart• Avoid giving sharp or pointed objects. • Do not allow lollipops in mouth when
running

PoisoningIngestion of toxic agents is common during early childhood.
Most common in 2 y/o• 75% of poisons are ingested, others are by dermal,
inhalation, and ocular• Reasons for poisoning:
Improper storage Learning new tastes /textures, loves to put things in
mouth Developing fine motor skills – able to open bottles, jars,
cabinets. Climbs onto shelves Cannot read labels

Sources of Poisoning
• Cosmetics, personal care products
• Household cleaners: Soaps, polishes
• Plants
• Drugs
•Insecticides• Hydrocarbons -- gasoline

Therapeutic Interventions
A poisoning may or may not require emergency intervention, but all should have medical attention
Parents are advised to call the Poison Control Center BEFORE BEFORE initiating any interventions

Therapeutic Interventions
1. Assess the child – treat the child first, not the poison– Take vital signs– assess ABC’s– Maintain respiratory function – provide ventilatory
and oxygen support– Start IV infusion– Draw blood for toxicology screen– Apply cardiac monitor– Initiate measure to reduce effects of shock if
applicable.

Therapeutic Intervention
2.Remove the child from exposure– Empty out mouth of any pills, plants,
or other material– Flush eyes with tap water– Flush skin and wash with soap– Bring child of inhalation poison into
fresh air

Therapeutic Intervention
3.Identify the Poison Question the child and witnesses. Try to
find out if only single product ingested. Look around environment for clues Do the products ingested breakdown to
other substances? Find out amount ingested? Amounts that
cause concern 1 ½ - 3 year old = 4.5 ml Adult = 15 ml

Therapeutic Intervention
4. Remove the Poison and Prevent absorption

Therapeutic Intervention
• Give activated charcoal– Give orally
• Available in ready to drink solution• Give in covered cup with a straw so child does
not see the black liquid
– Give through a gastric tube
– Give only after vomiting stops

Therapeutic Intervention
• Do NOT NOT induce vomiting if:– Patient is lethargic, comatose, seizuring, has
an absent gag reflex– Patient ingested an unidentified material, a
corrosive substance or petroleum product
• Insert gastric tube and perform gastric lavage with normal saline once airway is protected with a cuffed endotracheal tube
• Place child in side-lying position to decrease chance of aspiration.
Lead Poisoning• Also called
Plumbism
• An environmental disease caused
by the ingestion of lead-based materials.

Lead Poisoning
Causes• Lead based paint• Lead solder• Battery casings• Lead fishing sinkers, curtain weighs• Bullets• Some ceramic ware, pottery, pewter

Lead PoisoningPathophysiology
• Lead in the body moves in the blood to soft tissues and organs, teeth, and bones.
• Competes with calcium interfering with the regulation of calcium
• Interferes with neurotransmission in the brain causing encephalopathy and mental retardation
• Interferes with synthesis of heme causing anemia
• Damages tubules in the renal system

Assessment• Gastrointestinal symptoms:
– Unexplained, repeated vomiting– Vague chronic abdominal pain, colic– Anorexia, anemia
• Central Nervous System symptoms– Irritability, difficulty concentrating– Drowsiness– Ataxia, loss of skills, paresis or paralysis– Convulsive seizures from encephalopathy– Arthralgia

Blood tests that indicate presence of lead in the blood
*Levels of 10 u is harmful to the body
Diagnostic Tests

Therapeutic Intervention• Criteria for treatment:
– < 9 units = not lead poisoning– 10-14 units = trigger prevention activities,
rescreen– 15-19 units = nutritional and educational
interventions and rescreening– 20-44 units = environmental evaluation and medications.– 45-69 units = medical and environmental interventions. Chelation therapy– > 70 units = medical emergency
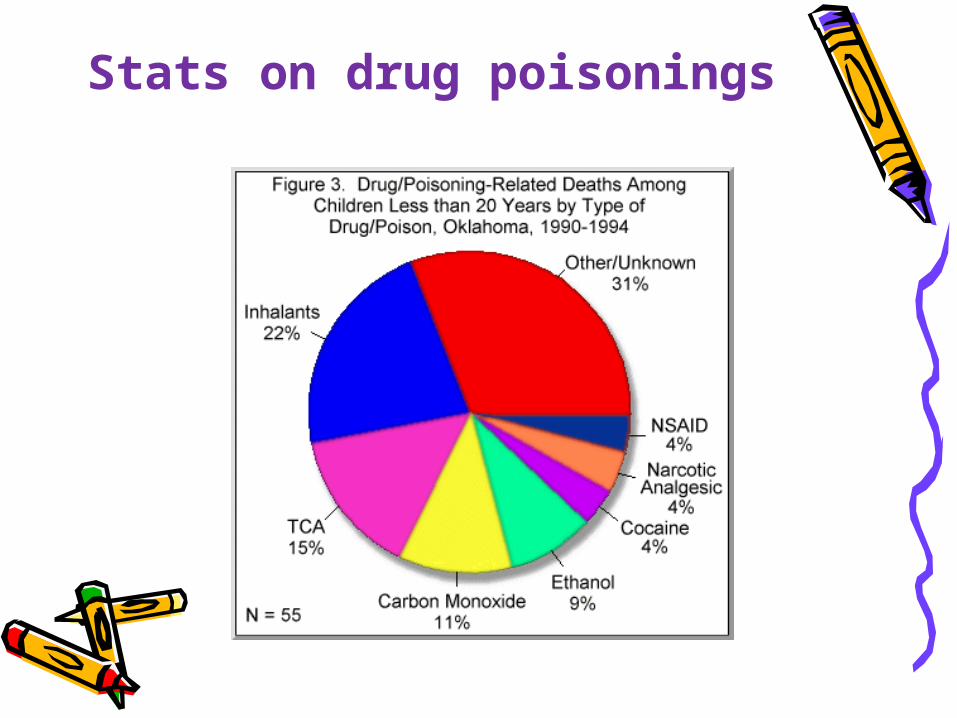
Stats on drug poisonings

Ask yourself:
• Why do you think the American Pediatric Association no long advises parents to keep syrup of Ipecac in the home?

Lead Poisoning Therapeutic Intervention
• Acute care– Gastric lavage followed my magnesium
sulfate. Enema. Just want to rid body of lead.
• Chronic Care / Chelation therapy– Administer meds that bind with the lead
• Calcium disodium edentate (EDTA) -- IV• Dimercaprol (BAL) or D-Penicillamine -- IM• Succimer -- orally
– Assess I & O – must have adequate urinary output. Force fluids.
– Monitor mineral levels

Preventive Measures
• Make environment lead-free• Inspect buildings >25 years of age• Areas painted with lead paint should be
covered with plywood or linoleum• Educate the parents• Follow up testing for lead levels• Screening all school age children
(required in some states)


















