Pediatric Ribs
18
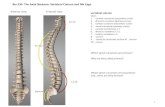
EDUCATION EXHIBIT 87 Pediatric Ribs: A Spectrum of Abnormalities 1 LEARNING OBJECTIVES FOR TEST 4 After reading this article and taking the test, the reader will be able to: Describe the vari- ous types of diagnos- tic features that occur in the ribs of children with bone dysplasias. Identify the rib changes that occur in child abuse. Recognize the ap- pearances of benign and malignant pri- mary bone tumors of the ribs. Ronald B. J. Glass, MD ● Karen I. Norton, MD ● Sandra A. Mitre, MD Eugene Kang, MD The manifestations of many congenital and acquired conditions can be seen in the ribs of children. Normal variants are usually clinically insig- nificant; they are occasionally palpated at clinical examination or de- tected incidentally at chest radiography. Signs of abnormality can ap- pear in the ribs as variations in number, size, mineralization, and shape. These changes can be focal or generalized. Abnormalities de- tected in the ribs may be the initial indication of previously unsus- pected systemic disease. The ribs can yield important diagnostic clues in the work-up of patients with congenital bone dysplasias, acquired metabolic diseases, iatrogenic conditions, trauma (especially child abuse), infection, and neoplasms. Routine evaluation of the ribs on every chest radiograph is important so that valuable diagnostic data will not be overlooked. The diagnostic information obtained from evalua- tion of the ribs can help tailor the radiologic and laboratory studies that may be necessary to complete a patient’s diagnostic work-up. © RSNA, 2002 Introduction Chest radiography is frequently the initial imaging study performed in children for a variety of diseases. Important information may be missed if attention is not directed to the ribs on every chest radiograph. Abnormalities detected in the ribs can some- times be the initial indication of systemic disease. Rib changes can indicate general- ized bone dysplasias, metabolic diseases, and trauma, especially abuse. Benign and malignant neoplasms occur in the ribs. Index terms: Ribs, 471.21, 471.50, 471.60, 471.80 ● Ribs, abnormalities, 471.14, 471.15, 471.16, 471.18 ● Ribs, fractures, 471.41 ● Ribs, neoplasms, 471.30 RadioGraphics 2002; 22:87–104 1 From the Department of Radiology, Mount Sinai School of Medicine, One Gustave L. Levy Pl, New York, NY 10029. Presented as an education exhibit at the 2000 RSNA scientific assembly. Received April 4, 2001; revision requested May 22 and received June 11; accepted June 14. Address correspondence to R.B.J.G. (e-mail: [email protected]). © RSNA, 2002 CME FEATURE See accompanying test at http:// www.rsna.org /education /rg_cme.html
-
Upload
angellisimal -
Category
Documents
-
view
18 -
download
1
description
Pediatric Ribs
Transcript of Pediatric Ribs

EDUCATION EXHIBIT 87
Pediatric Ribs:A Spectrumof Abnormalities1
LEARNINGOBJECTIVESFOR TEST 4After reading thisarticle and takingthe test, the reader
will be able to:
� Describe the vari-ous types of diagnos-tic features that occurin the ribs of childrenwith bone dysplasias.
� Identify the ribchanges that occur inchild abuse.
� Recognize the ap-pearances of benignand malignant pri-mary bone tumors ofthe ribs.
Ronald B. J. Glass, MD ● Karen I. Norton, MD ● Sandra A. Mitre, MDEugene Kang, MD
The manifestations of many congenital and acquired conditions can beseen in the ribs of children. Normal variants are usually clinically insig-nificant; they are occasionally palpated at clinical examination or de-tected incidentally at chest radiography. Signs of abnormality can ap-pear in the ribs as variations in number, size, mineralization, andshape. These changes can be focal or generalized. Abnormalities de-tected in the ribs may be the initial indication of previously unsus-pected systemic disease. The ribs can yield important diagnostic cluesin the work-up of patients with congenital bone dysplasias, acquiredmetabolic diseases, iatrogenic conditions, trauma (especially childabuse), infection, and neoplasms. Routine evaluation of the ribs onevery chest radiograph is important so that valuable diagnostic data willnot be overlooked. The diagnostic information obtained from evalua-tion of the ribs can help tailor the radiologic and laboratory studies thatmay be necessary to complete a patient’s diagnostic work-up.©RSNA, 2002
IntroductionChest radiography is frequently the initial imaging study performed in children for avariety of diseases. Important information may be missed if attention is not directedto the ribs on every chest radiograph. Abnormalities detected in the ribs can some-times be the initial indication of systemic disease. Rib changes can indicate general-ized bone dysplasias, metabolic diseases, and trauma, especially abuse. Benign andmalignant neoplasms occur in the ribs.
Index terms: Ribs, 471.21, 471.50, 471.60, 471.80 ● Ribs, abnormalities, 471.14, 471.15, 471.16, 471.18 ● Ribs, fractures, 471.41 ● Ribs, neoplasms,471.30
RadioGraphics 2002; 22:87–104
1From the Department of Radiology, Mount Sinai School of Medicine, One Gustave L. Levy Pl, New York, NY 10029. Presented as an educationexhibit at the 2000 RSNA scientific assembly. Received April 4, 2001; revision requested May 22 and received June 11; accepted June 14. Addresscorrespondence to R.B.J.G. (e-mail: [email protected]).
©RSNA, 2002
CME FEATURESee accompanying
test at http://www.rsna.org
/education/rg_cme.html

In this article, we review rib development andnormal anatomy and techniques for evaluatingthe ribs and present inherited abnormalities andacquired conditions of the pediatric ribs.
Rib Developmentand Normal Anatomy
Twelve paired ribs develop from cartilaginouscostal processes of the developing thoracic verte-brae. Rib development begins at 9 weeks; second-ary ossification centers appear at 15 years (1,2).The first seven “true” ribs connect to the sternumvia the costal cartilages by day 45. The lower five“false” ribs do not articulate with the sternum.Developmental rib abnormalities may be isolatedor occur in association with other congenitalanomalies.
Techniques forEvaluating the Ribs
The ribs are evaluated in most patients on thefrontal chest radiograph. However, routine radio-graphs of the chest are inadequate for rib de-tail, and better detail is achieved on dedicatedrib views. Such views are obtained by using theoverpenetrated grid technique, with additional
oblique views centered over the area of maximuminterest (3). The best method for evaluation ofinflammatory or neoplastic masses is computedtomography (CT) or magnetic resonance imaging.
Inherited Abnormalities
Cervical RibsCervical ribs arise from the seventh cervical verte-bra. They resemble hypoplastic first thoracic ribs,from which they are reliably differentiated bymeans of the adjacent transverse process, which isangulated inferiorly in the cervical spine and has amore cranial course in the thoracic spine (Fig 1).The reported prevalence of cervical ribs variesfrom 0.2% to 8% (4). Cervical ribs occur unilat-erally or bilaterally. They are most commonly anincidental finding or are associated with the Klip-pel-Feil anomaly (Fig 1). Cervical ribs are rarelysymptomatic in early childhood; in older childrenand adults, compression of the brachial plexus orsubclavian artery can give rise to the thoracic out-let syndrome (5,6). Cervical rib compression ofthe subclavian artery can result in aneurysm for-mation (7).
Figure 1. Cervical ribs with Klippel-Feil anomalyand esophageal atresia in a 10-year-old boy. Frontalradiograph shows cervical ribs that articulate with theinferiorly directed transverse processes (straight ar-rows), whereas the thoracic transverse processes extendin a superior direction (curved arrows). The left-sidedsoft-tissue mass (m) is caused by bowel interposition.
Figure 2. Supernumerary ribs in a neonate withacyanotic congenital heart disease, cardiomegaly, andshunt vascularity. Frontal chest radiograph shows 14pairs of ribs.
88 January-February 2002 RG f Volume 22 ● Number 1

Abnormal Number of RibsSupernumerary ribs may rarely be seen inciden-tally as a normal variant. Increased numbers ofribs are seen in trisomy 21 syndrome and with theVATER association (Fig 2)(8,9). It is more com-mon to see 11 pairs in the absence of associatedanomalies; this situation occurs in 5%–8% ofnormal individuals. Eleven pairs of ribs occur inone-third of patients with trisomy 21 syndrome(9), as well as in association with cleidocranialdysplasia and campomelic dysplasia.
Abnormal Sizeor Shortening of RibsShort ribs do not extend as far anteriorly as thesternum. The resultant diminished volume of thechest restricts respiratory motion and causes re-spiratory insufficiency. Short ribs constitute anintegral part of several syndromes. Definitive di-agnosis of the type of any skeletal dysplasia re-quires a complete skeletal survey. This surveyshould optimally be performed early in the neona-tal period to exclude a lethal dysplasia so that re-
suscitation policy can be planned. The differentialdiagnosis must include the short rib–polydactylysyndromes (Saldino-Noonan, Majewski, andVerma-Naumoff); chest diameter is criticallysmall in these syndromes.
Thanatophoric Dysplasia.—Thanatophoricdysplasia is a lethal dysplasia transmitted by adominant gene mutation. It is the most commonlethal neonatal skeletal dysplasia after osteogen-esis imperfecta type II (10, pp 939–943). Patientspresent very early with severe respiratory distress.The appearance on the chest radiograph is patho-gnomonic. The ribs are very short and do not ex-tend beyond the anterior axillary line. The verte-bral bodies assume an H or U shape, and the hu-meri are curved and short (Fig 3). Associatedfindings are cloverleaf skull deformity, polydac-tyly, and hypoplastic iliac bones. The differentialdiagnosis includes thanatophoric variants, as-phyxiating thoracic dysplasia, homozygousachondroplasia, and achondrogenesis.
Figure 3. Thanatophoric dysplasia in a male neonate. Frontal (a) and lateral (b) chest radiographs show flattenedvertebrae and curved humeri, which are pathognomonic.
RG f Volume 22 ● Number 1 Glass et al 89

Figure 4. Jeune asphyxiating dysplasia in a female neonate. (a) Frontal chest radiograph shows short ribs and avery narrow chest diameter. The humeral heads are prematurely ossified (arrowhead). (b) Lateral chest radiographobtained at 8 months of age shows short ribs that do not reach the sternum.
Figure 6. Achondroplasia in a female neonate.(a) Frontal chest radiograph shows short, anteriorlyflared ribs and wide humeral metaphyses. (b) Lateralchest radiograph obtained at 3 months of age showsshort ribs that are cupped and widened anteriorly. Notethe anterior “beaking” of L4 (arrow).
90 January-February 2002 RG f Volume 22 ● Number 1

Jeune Asphyxiating Thoracic Dysplasia.—Jeuneasphyxiating thoracic dysplasia is an autosomalrecessive dysplasia. Patients may present withrespiratory distress that may be sufficiently severeto cause neonatal death. The ribs are short, with ahorizontal course, and the chest diameter is sig-nificantly decreased compared with that of theabdomen (Fig 4). The long bones are shortened.The proximal humeral and femoral epiphyses arefrequently ossified at birth, and polydactyly is oc-casionally encountered. The iliac wings are small,and the acetabula typically have spurs. Althoughthe findings on the chest radiograph are highlysuggestive of Jeune dysplasia, the appearance alsoresembles that of Ellis–van Creveld dysplasia.Less severely affected children who survive intoadulthood have a high prevalence of medullarycystic renal disease (11).
Ellis–van Creveld Chondroectodermal Dys-plasia.—Ellis–van Creveld chondroectodermaldysplasia is an autosomal recessive dysplasia witha high prevalence among the Amish. The ribs areshort, and the chest is narrow (Fig 5). The nar-
row thorax exaggerates the heart size; cardiomeg-aly is often present because of associated anoma-lies, especially atrial septal defects. The appear-ance of the chest and pelvis closely resembles thatof Jeune dysplasia. Respiratory insufficiency canbe severe, resulting in death in up to 50% of af-fected neonates (10, pp 786–788). The proximalhumeral and femoral epiphyses may be prema-turely ossified at birth. Acromelic limb shorten-ing, polydactyly, and cone epiphyses are charac-teristic. The differential diagnosis includes Jeunedysplasia and the short rib–polydactyly syn-dromes.
Achondroplasia.—In achondroplasia, the ribsare short and wide with concavity at the rib end(Fig 6). The inheritance is autosomal dominant,with spontaneous mutation in 80% of cases (10,pp 749–751). The chest radiographic findings arehighly suggestive of achondroplasia. Rhizomelicshortening of the humeri may be apparent on thechest radiograph. Associated diagnostic features
Figure 5. Ellis–van Creveld dysplasia in a female neonate. Frontal (a) and lateral (b) chest radiographs show shortribs, which are most obvious on the lateral projection. The cardiomegaly and increased pulmonary vascularity are dueto a large atrial septal defect.
RG f Volume 22 ● Number 1 Glass et al 91

include macrocephaly, depression of the nasion,craniocaudal narrowing of the interpediculatespaces, square iliac bones, and a champagneglass–shaped pelvic inlet. A differential diagnosticconsideration is hypochondroplasia.
Diminished Bone DensityFour distinct subgroups of osteogenesis imper-fecta are recognized, according to the severity ofinvolvement (12). Affected patients have demin-eralization and bone fragility. Transmission isautosomal recessive in type III and dominant intypes I and IV. New dominant mutations accountfor most cases of type II osteogenesis imperfecta.Type II osteogenesis imperfecta is a lethal condi-tion, characterized by marked osteopenia and de-formity of long bones and ribs caused by in uterofractures (Fig 7). Affected neonates present withnonimmune hydrops and respiratory distress. Askeletal survey reveals generalized osteopenia andthin bone cortices. The skull is classically demin-eralized, and wormian bones are present in mostcases. Differential diagnostic considerations in-clude achondrogenesis, hypophosphatasia, andcampomelic dysplasia. In older children, the dif-ferential diagnosis of osteopenia also includestype I, III, and IV osteogenesis imperfecta; childabuse; and leukemia.
Increased Bone Density
Tuberous Sclerosis.—Tuberous sclerosis is aneurocutaneous syndrome with autosomal domi-nant transmission. It is characterized by hamarto-mas and central nervous system tumors. Bonechanges are characteristically patchy areas of scle-rosis (13). Any bone can be affected. Involvementof the ribs is most commonly seen as expansionand sclerosis (Fig 8). Affected patients have cuta-neous manifestations, seizures, and developmen-tal delay. The differential diagnosis includes fi-brous dysplasia, chronic infection, trauma, andprevious surgical subperiosteal rib resection.
Osteopetrosis.—Osteopetrosis is subdividedinto various subgroups, all of which are character-ized by a generalized increase in bone density (Fig
9). The congenital type is transmitted as an auto-somal recessive trait and is more severe than theautosomal dominant varieties that manifest later(10, pp 886–891). Neonates and infants experi-ence pancytopenia, hepatosplenomegaly, and pre-mature death. Older children develop cranial
Figure 7. Type II osteogenesis imperfecta and gener-alized osteopenia in a female neonate. Frontal chestradiograph shows that all of the ribs are deformed andthickened posteriorly. Periosteal new bone in multiplehealing fractures gives the ribs a beaded appearance.Healing fractures are present in the clavicles and hu-meri.
Figure 8. Tuberous sclerosis in an 8-year-old boywith seizures, developmental delay, and renal hamarto-mas. Frontal chest radiograph shows sclerosis and wid-ening isolated to the left fifth rib.
92 January-February 2002 RG f Volume 22 ● Number 1

nerve palsies, deafness, and blindness. The entireskeleton is dense, and the metaphyses and rib cos-tochondral junctions are splayed. Although thebones are dense, they are brittle and fractures
arise from minor trauma. The bone is susceptibleto osteomyelitis, and hematopoietic function isdecreased. The differential diagnosis includeschronic renal failure, oxalosis, and pyknodysosto-sis. Caveat: Physiologic sclerosis in neonatesshould not be mistaken for osteopetrosis.
Abnormal Rib Shape
Cerebrocostomandibular Syndrome.—Cere-brocostomandibular syndrome is very rare. Thegenetic transmission is uncertain (8). Eleven pairsof ribs are usually present. The ribs are character-ized by abnormal costovertebral articulations andposterior ossification gaps that resemble fractures(Fig 10); these gaps will ossify in later life. Respi-ratory distress is common in neonates due to flailchest and airway abnormalities. Other featuresare microcephaly, micrognathia, and congenitalheart disease. Multiple fractures must be consid-ered in the differential diagnosis.
Rib Notching.—Concave notches are found onthe inferior rib surface and are most commonly anormal variant. Pathologic notching is vascular
Figure 9. Osteopetrosis. (a) Frontal chest radiograph of a 1-month-old girl shows sclerotic bones and periostealnew bone formation along the lateral aspects of all of the ribs. (b) Frontal chest radiograph of a 5-year-old girl with afamily history of osteopetrosis shows that all of the bones are extremely dense but normal in shape. The left upperabdominal fullness suggests splenomegaly.
Figure 10. Cerebrocostomandibular syndrome in afemale neonate. Frontal chest radiograph shows lucentossification gaps in all of the posterior ribs. Only 10 ribpairs are present. The costovertebral junctions are ab-normal. Several ribs are caudally angulated.
RG f Volume 22 ● Number 1 Glass et al 93

or neural in origin. Notching associated with aor-tic coarctation usually affects ribs 4–8 and is rarebefore the age of 8 years (Fig 11) (13). Rib notch-ing is also encountered in neurofibromatosis andthalassemia. Notching is unilateral (right sided)with coarctation proximal to the origin of the leftsubclavian artery and a postoperative Blalock-Taussig shunt.
Pectus Excavatum.—Pectus excavatum is ananomaly that arises from posterior depression ofthe sternum, which compresses the heart againstthe spine and deviates it to the left (Fig 12), thusmimicking cardiomegaly. The displaced pulmo-nary vascularity and obscured right cardiac bor-der resemble a right middle lobe process. Theposterior ribs are horizontal, whereas the anteriorribs have a more vertical course. Pectus excava-tum is most commonly an isolated anomaly. Thischest deformity is also associated with prematu-rity, homocystinuria, Marfan syndrome, Noonansyndrome, and fetal alcohol syndrome. Surgicalcorrection is undertaken to relieve restrictive air-way disease and for cosmetic repair.
Bifid RibsGorlin basal cell nevus syndrome is a rare, auto-somal dominant syndrome characterized by mul-tiple nevoid basal cell carcinomas that arise in
childhood, jaw cysts, and bifid ribs (Fig 13). Thefourth rib has been reported to be the most com-monly bifid. Other rib anomalies include agen-esis, supernumerary ribs, distorted shape, andfusion of adjacent ribs (14). The lateral claviclemay be deficient. Associated features are mandib-ular hypoplasia, macrocephaly, and mental retar-dation. A single bifid rib is most commonly a nor-mal incidental finding and may be detected as apalpable chest wall mass.
Figure 11. Rib notching in a 16-year-old boy withaortic coarctation. Frontal chest radiograph shows anotched rib (arrow).
Figure 12. Pectus excavatum in a 12-year-old boy.(a) Frontal chest radiograph shows steep angulation ofthe anterior ribs. A poorly defined area of increasedopacity along the right cardiac border mimics a pulmo-nary infiltrate of the right middle lobe. (b) CT scanobtained through the midsternum shows a depressedsternum deviating the heart posteriorly and to the left.(Courtesy of Andrew K. Poznanski, MD, Children’sMemorial Hospital, Chicago, Ill.)
94 January-February 2002 RG f Volume 22 ● Number 1

Slender Ribs
Trisomy 18 Syndrome.—Marked phenotypicvariability is characteristic of trisomy 18 syn-drome. Eleven rib pairs are present, and they areclassically hypoplastic and thin (Fig 14). Theshort sternum causes the typical shield deformityof the chest. The acute iliac angle is diagnostic.
These children are spastic and neurologically de-layed. The fingers are characteristically main-tained in ulnar deviation with flexion deformities.Associated findings are dolichocephaly, micro-gnathia, and numerous multisystem anomalies.Differential diagnostic considerations include os-teogenesis imperfecta, trisomy 13 syndrome,Cockayne syndrome, and Werdnig-Hoffmanndisease.
Neurofibromatosis.—Peripheral neural tumorsare the hallmark of neurofibromatosis, an autoso-mal dominant neurocutaneous syndrome. Theribs are slender (Fig 15); they may be twisted,deformed, and separated by neurofibromas that
Figure 13. Gorlin basal cell nevus syndrome in a de-velopmentally delayed 1-year-old girl. Frontal chestradiograph shows bilateral bifid ribs (arrows).
Figure 14. Trisomy 18 syndrome and severe respira-tory distress in a male neonate. Frontal chest radio-graph shows very slender ribs. The iliac bones have analmost vertical orientation. Both hips are dislocated.
Figure 15. Neurofibromatosis in a 15-year-old girl.Frontal chest radiograph shows that several right ribsare thin and ribbonlike. Right ribs 5, 6, and 7 arenotched inferiorly (solid arrows). The posterior middleaspect of right rib 9 is expanded, with poorly definedborders and a thinned cortex (open arrow). Note alsothe bilateral apical neurofibromas.
RG f Volume 22 ● Number 1 Glass et al 95

arise from the intercostal nerves (15). The under-lying mesenchymal abnormality in neurofibroma-tosis results in modeling deformity and even bi-zarre appearance of the ribs. Intercostal neuromascan cause notching of the inferior surface. Sphe-noid dysplasia, modeling deformity of the longbones, and posterior vertebral body scalloping areassociated findings. The differential diagnosisincludes cleidocranial dysplasia, myotonic dystro-phy, Melnick-Needles osteodysplasty, and Werd-nig-Hoffmann disease.
Widened Ribs
Mucopolysaccharidosis.—The storage diseasesare a miscellaneous group of autosomal recessiveconditions in which specific enzyme deficienciescause accumulation of abnormal metabolite sub-strates that are deposited in the bone marrow andmultiple viscera (10, pp 672–681). In mucopo-lysaccharidosis, the ribs are thin proximally at thelevel of the neck and wider distally (Fig 16).Coarse trabeculation and heterogeneous bonedensity are due to deposition of accumulated pre-cursor metabolites in the bone marrow. The ap-pearance is variable, and definitive diagnosis ismade by means of a complete skeletal survey andbiochemical analysis. Helpful associated featuresinclude external flaring of the iliac bones, whichare inferiorly tapered; vertebral body flatteningand anterior beaking; atlantoaxial instability; andbrachydactyly. Differential diagnostic possibilitiesinclude Gaucher disease and Niemann-Pick dis-ease.
Thalassemia Major.—Thalassemia major is thesevere homozygous form of this hemoglobinopa-thy. Symptoms become evident in the first 2 yearsof life. Hyperplasia of the marrow destroys thetrabeculae and expands and thins the cortex (16).The ribs are undertubulated and broad, and ossi-fication is heterogeneous (Fig 17). This appear-ance is rarely encountered today because patientsare aggressively treated with blood transfusionsand chelation from an early age. Marrow expan-
sion also causes widened diploe, hypoplasia ofparanasal sinuses, paraspinal extramedullary foci,and hepatosplenomegaly. Other diagnostic possi-bilities include chronic anemias, storage diseases,and fibrous dysplasia.
Expansile Rib Deformity
Lymphangiomatosis.—Lymphangiomatosis isa rare and idiopathic disease of children and ado-lescents that is thought to represent a malforma-tion of lymphatic vessels (17). The abnormal lym-phatic vessels can be found diffusely in parenchy-mal viscera and bones. Rib lymphangiomas ap-pear as well-defined areas of lucency (Fig 18).These lucent lesions can coalesce and replacelarge parts of the affected bone. Lymphangioma-tosis of the ribs has been associated with chylo-thorax (17). Gorham disease is the term used whenone or more bones become replaced by abnormallymphatic vessels. Differential diagnostic possi-
Figure 16. Hurler syndrome in a 7-year-old boy withdevelopmental delay. Frontal chest radiograph showsthat the ribs are thin and tapered proximally; theywiden and become very broad distally.
96 January-February 2002 RG f Volume 22 ● Number 1

bilities include Langerhans cell histiocytosis, fi-brous dysplasia, and hyperparathyroidism (browntumors).
Fibrous Dysplasia.—Fibrous dysplasia is a be-nign condition in which there is proliferation offibrous tissues in the bones. Involvement may bemonostotic or polyostotic. Fibrous dysplasia isthe most common cause of a benign expansilelesion of the ribs, and the ribs are one of the mostcommon sites of monostotic involvement (18).The abnormal bone foci are classically lucent witha “ground-glass” matrix; bone expansion, corticalthinning, and modeling deformity are common(Fig 19). The differential diagnosis includessimple bone cyst, enchondroma, and hyperpara-thyroidism (brown tumors).
Figure 17. Thalassemia major in an 11-year-old girl. Frontal chest radiograph shows os-teopenic and widened ribs. The trabecular pat-tern is coarse.
Figure 18. Lymphangiomatosis in an 8-year-old boy. Frontal chest radiograph shows multiplecorticated areas of lucency in all of the ribs. Focalareas of expansion affect isolated ribs (arrows).The cortices remain intact.
Figure 19. Fibrous dysplasia in an 8-year-oldboy. Frontal chest radiograph shows widening ofanterior ribs 2 and 3. The ribs have heteroge-neous ground-glass opacity. A well-defined areaof lucency is present in anterior rib 4 (arrow).Areas of lucency are also present in the scapula(arrowheads).
RG f Volume 22 ● Number 1 Glass et al 97

Acquired Conditions
Metabolic DisordersAll the bone manifestations of chronic renal insuf-ficiency (ie, osteopenia, sclerosis, rickets, and hy-perparathyroidism) can be seen in the ribs.
Rickets.—Rickets results from abnormal calciummetabolism due to vitamin D deficiency or distur-bance of hydroxylation in the kidney or liver. Di-etary vitamin D deficiency is rare today. Rickets ismore common with extreme low-birth-weightprematurity and secondary to renal or hepaticdysfunction and anticonvulsant administration.Delayed ossification of the osteoid matrix in im-mature bones is most marked in the metaphysesaround the knees and wrists and the rib ends,which become concave and flared (Fig 20). Thehyperplastic rib osteoid may be palpable on thechest wall as the “rachitic rosary.” The metaphy-seal appearance is indistinguishable from that inphosphate-losing vitamin D–resistant rickets andrickets due to other causes. Other differential di-agnostic considerations for rib cupping and flar-ing include achondroplasia, hypophosphatasia,and metaphyseal chondrodysplasia.
Hyperparathyroidism.—Hyperparathyroidismoccurs most commonly secondarily to chronicrenal failure. Hyperparathyroidism results insubperiosteal and endosteal bone resorption.
Brown tumors are a rare manifestation of hyper-parathyroidism, in which well-defined lucent ar-eas of lysis occur without adjacent reactive boneformation. Progressive loss of bone matrix anddemineralization can lead to fractures and pro-gressive bone deformity (Fig 21). Renal osteodys-trophy can regress with correction of azotemia(19). The other differential diagnostic consider-ations are Langerhans cell histiocytosis, fibrousdysplasia, and enchondromas.
Iatrogenic ConditionsGeneralized new bone formation occurs withprostaglandin administration to children withcyanotic heart disease (Fig 22). The onset hasbeen reported to be as early as 6 days but is moreusual after 30–40 days of prostaglandin therapy.The changes are usually more symmetrical thanthose of infantile cortical hyperostosis (Caffeydisease or syndrome). After treatment, periostealnew bone becomes incorporated and remodeled(20). Differential diagnostic possibilities includechild abuse, extracorporeal membrane oxygen-ation, and infantile cortical hyperostosis. Caveat:Motion artifact can mimic the appearance of peri-osteal new bone.
Trauma
Child Abuse.—Fractures of the ribs with childabuse are well described and are consideredhighly specific for child abuse (21). Rib fracturesare rare with accidental injury and are unlikely to
Figure 20. Nutritional rickets in a 3-month-old boy. Frontal chest radiographshows that the ribs are flared anteriorly(arrows), as well as widened. The humeralgrowth plates are irregular (arrowheads).
98 January-February 2002 RG f Volume 22 ● Number 1

arise from cardiopulmonary resuscitation (22).Although abuse fractures can occur along anypart of the ribs, they are more common in theposterior arc because of the significant posteriorlevering force inflicted in the abuse situation.Healing fractures are more easily detectable than
in the acute phase. Not all fractures are detectablewith conventional radiography; some requirehigh-detail radiography, scintigraphy, or CT. Thepresence of acute and healing rib fractures is diag-nostic of abuse (Fig 23). Other diagnostic signsare metaphyseal “corner” fractures, retinal hem-orrhage, intracranial hemorrhage, and subdu-ral hygroma. The most important differential
Figure 21. Rapid progression of renal osteodystrophy over 4 years. (a) Frontal chest radiograph obtained duringthe early stages of azotemia shows no discernible bone abnormality. Cardiomegaly is present, and vagotomy clips arein place. (b) Frontal chest radiograph obtained at the age of 20 years shows that the thorax is deformed. Areas of lu-cency in the ribs, clavicles, and humerus represent brown tumors (arrows).
Figure 22. Results of prostaglandintherapy in an infant with cyanotic heartdisease. Frontal chest radiograph showsperiosteal new bone formation in theribs (arrowheads).
Figure 23. Child abuse in an 8-month-old girl with gastric perfora-tion and intraperitoneal air. Frontal chest radiograph shows bilateralhealing rib fractures (arrows), which are diagnostic of abuse.
RG f Volume 22 ● Number 1 Glass et al 99

diagnoses to consider are osteogenesis imperfecta,long-term ventilator therapy in prematurity, birthtrauma, and Menkes syndrome.
Surgical Changes.—Rib resection and defor-mity that result from thoracotomy are asymptom-atic. However, rib fusion will cause scoliosis andrestriction of chest wall expansion (Fig 24), whichmay require surgical intervention. Fused ribs arealso encountered in Gorlin syndrome.
InfectionRib osteomyelitis is most commonly acquiredfrom an adjacent focus of empyema or pneumo-nia (Fig 25). Hematogenous spread is extremelyrare. When present, hematogenous spread occursanteriorly near the costochondral junction or pos-teriorly near the rib angle (23). The changes re-semble those of typical chronic long bone infec-tion, in which there is formation of a sequestrumand involucrum in the presence of periosteal newbone formation. Radiographic differentiationfrom a neoplasm or Langerhans cell histiocytosismay be difficult.
Figure 24. Rib fusion after surgi-cal repair of a diaphragmatic herniain a 6-week-old boy. Frontal chestradiograph shows fusion of right ribs5–7. Note the separation betweenribs 4 and 5 and the crowding of theinterspace between ribs 5 and 6.
Figure 26. Enchondromatosis in a16-year-old girl. Frontal chest radio-graph shows enchondromas in theright and left ribs (arrows). Isolatedribs are widened anteriorly. A densemass (m) arises from right rib 6.Note also the areas of lucency andmodeling deformity of the left hu-merus and scapula.
100 January-February 2002 RG f Volume 22 ● Number 1

NeoplasmsThe prevalence of primary neoplasms originatingin the thoracic wall is 5%–10% of all bone tu-mors; malignant tumors are more common thanbenign (24). Large tumors extend intra- and ex-trathoracically; only that portion of the soft-tissuemass that extends externally will be clinically ob-vious. As a result, primary rib tumors are signifi-cantly larger than bone tumors in other locations(25).
Enchondromatosis.—The enchondromatosesare a group of disorders characterized by the pres-ence of medullary cartilaginous bone tumors,which are further subdivided by the presence ofhemangiomas (Maffucci syndrome) or their ab-sence (Ollier disease). Rib lesions are common inenchondromatosis (10, pp 814–815). Inheritanceis sporadic (10, pp 814–815). At radiography,enchondromas appear as areas of lucency in thebones (Fig 26), occasionally with areas of calcifi-cation in the cartilaginous matrix. Modeling de-
formity is not uncommon. The appearance issimilar to that of fibrous dysplasia. Enchondro-mas occur in association with a variety of systemicmalignancies and are themselves associated witha 25% prevalence of malignant degeneration(26,27). Differential diagnostic considerations areLangerhans cell histiocytosis and osteomyelitis, ifisolated.
Osteochondroma.—Exostoses are benign bonyexcrescences with a cartilage cap. They can besolitary or associated with multiple hereditaryexostoses. It has been estimated that rib osteo-chondromas arise in almost 50% of patients withmultiple hereditary exostoses (4). Those rib exos-toses that project externally are palpable on thechest wall. Internal exostoses can be asymptom-atic; hemothorax has been reported, likely causedby trauma to the adjacent lung (28). Osteochon-dromas can mimic pulmonary nodules; calcifiedosteochondromas resemble granulomas. CT ismost helpful in determining the nature of thesebone growths (Fig 27).
Figure 25. Osteomyelitis of the ribs and an extrapleural mass in a9-year-old boy with chronic granulomatous disease. (a) Frontal chestradiograph shows poorly defined periosteal elevation in anterior ribs 6and 7 (arrow), which is partially obscured by an inflammatory soft-tis-sue mass. (b) CT scan shows the periosteal elevation more clearly. Themass has heterogeneous attenuation. Sporotrichosis was proved at cul-ture.
RG f Volume 22 ● Number 1 Glass et al 101

Langerhans Cell Histiocytosis.—Langerhanscell histiocytosis is thought to be associated withimmune dysfunction. Although most bone lesionsare asymptomatic, some may manifest with apainful soft-tissue mass (29). The appearance isvariable: A well-defined area of lucency in thebone is a classic finding (Fig 28); expansile andpoorly defined lesions can appear aggressive. Theribs are commonly involved, and multiple boneinvolvement is frequent. Differential diagnostic
considerations include metastases, hyperparathy-roidism (brown tumors), Ewing sarcoma, Askintumor, and lymphoma.
Figure 27. Osteochondroma in a 7-year-old boy whowas followed up years after resection of a Wilms tumor.(a) Frontal chest radiograph shows a solitary osteo-chondroma (arrows), which mimics a pulmonary nod-ule. (b) CT scan shows that the mass is partially calci-fied and arises from a rib. (Courtesy of Andrew K.Poznanski, MD, Children’s Memorial Hospital, Chi-cago, Ill.)
Figure 28. Langerhans cell histiocytosis in a5-year-old boy. Frontal chest radiograph showsexpansile areas of lucency in multiple ribs (ar-rows).
Figure 29. Xanthogranuloma in a 2-year-oldboy. Frontal chest radiograph shows a xan-thogranuloma of rib 10 (arrows). The rib is fo-cally widened and lucent with indistinct borders.The cortex is intact.
102 January-February 2002 RG f Volume 22 ● Number 1

Xanthogranuloma.—Xanthogranulomas arerare benign tumors that occur in the ribs andother flat bones. They are invariably solitary le-sions and are almost twice as common in malepatients (30). The lesions are well defined withreactive bone or a sclerotic margin. They can beexpansile and lytic (Fig 29). The tumor is histio-cytelike and consists of benign giant cells, choles-terol clefts, and foam cells. Xanthogranulomasmay be the residua of previous fibrous dysplasiaor Langerhans cell histiocytosis. The tumor hasan excellent prognosis, and complete or partialremoval is curative (30). The differential diagno-sis includes aneurysmal bone cyst, hyperparathy-roidism (brown tumor), and Langerhans cell his-tiocytosis.
Ewing Sarcoma.—Ewing sarcoma is a very ag-gressive malignant tumor that occurs in adoles-cents and young adults. This is the most common
malignant tumor that affects the ribs of childrenand adolescents (25). Tumors infiltrate the bonein a permeative, “moth-eaten” pattern. Althoughmost tumors are lytic (Fig 30), sclerotic tumorsdo occur. Approximately one-third of costal Ew-ing sarcomas are expansile (31). Most Ewing sar-comas have an associated soft-tissue mass that issignificantly larger than the intraosseous tumor(31). Extensive periosteal reaction is not a majorfeature of primary Ewing sarcoma of the rib (31).The differential diagnosis includes osteomyelitis,Langerhans cell histiocytosis, osteosarcoma,primitive neuroectodermal tumor, metastaticneuroblastoma, and lymphoma.
Primitive Neuroectodermal Tumor.—Primi-tive neuroectodermal tumor (Askin tumor) is arare malignant tumor that arises from the chestwall, occasionally originating in a rib (Fig 31).This tumor very closely resembles Ewing sar-coma, and differentiation depends on detection ofneurosecretory granules at electron microscopy(32). Rib destruction occurs in 25%–63% of pa-tients. Pleural extension is common and results inmalignant effusion (33). Differential diagnosticconsiderations include osteomyelitis, Langerhanscell histocytosis, osteosarcoma, Ewing sarcoma,metastasis, and lymphoma.
Figure 30. Ewing sarcoma in a 10-year-oldgirl. (a) Frontal chest radiograph shows a Ewingsarcoma of rib 5. The rib is expanded posteriorly,and the cortex is obliterated superiorly (arrows).A soft-tissue mass arises from the rib. (b) CTscan shows that the rib is infiltrated by the tumor,which extends into the thorax.
Figure 31. Askin tumor originating from a ribin a 7-year-old boy. Frontal chest radiographshows poorly defined areas of lucency in an ante-rior rib (arrows). The superior cortex is dis-rupted. A large, homogeneous soft-tissue massopacifies the left hemithorax.
RG f Volume 22 ● Number 1 Glass et al 103

ConclusionsThere is a wealth of information readily availablefrom the ribs because they may indicate manylocal and systemic processes. Rib abnormalitiesdetected on chest radiographs are an importantindicator of known or unsuspected bone dyspla-sia, cardiac disease, metabolic disease, trauma,and neoplasms. The diagnostic information ob-tained from evaluation of the ribs can help tailorthe pertinent radiologic and laboratory studiesthat may be necessary to complete a patient’s di-agnostic work-up.
References1. Larsen WJ. Essentials of human embryology. New
York, NY: Churchill Livingstone, 1998; 47–51.2. Arey LB. Developmental anatomy: a textbook and
laboratory manual of embryology. 7th ed. Phila-delphia, Pa: Saunders, 1974; 409–410.
3. Meschan I. An atlas of anatomy basic to radiology.Philadelphia, Pa: Saunders, 1975; 628–631.
4. Guttentag AR, Salwen JK. Keep your eyes on theribs: the spectrum of normal variants and diseasesthat involve the ribs. RadioGraphics 1999; 19:1125–1142.
5. Panegyres PK, Moore N, Gibson R, RushworthG, Donaghy M. Thoracic outlet syndromes andmagnetic resonance imaging. Brain 1993; 116(pt4):823–841.
6. Durham JR, Yao JS, Pearce WH, Nuber GM, Mc-Carthy WJ 3rd. Arterial injuries in the thoracicoutlet syndrome. J Vasc Surg 1995; 21:57–69.
7. Engel A, Adler OB, Carmeli R. Subclavian arteryaneurysm caused by cervical rib: case report andreview. Cardiovasc Intervent Radiol 1989; 12:92–94.
8. Willich E, Richter E. The thorax. In: Ebel KD,Blickman H, Willich E, Richter E, eds. Differentialdiagnosis in pediatric radiology. New York, NY:Thieme, 1999; 124–134.
9. Edwards DK 3rd, Berry CC, Hilton SW. Trisomy21 in newborn infants: chest radiographic diagno-sis. Radiology 1988; 167:317–318.
10. Taybi H, Lachman RS. Radiology of syndromes,metabolic disorders, and skeletal dysplasias. 4thed. St Louis, Mo: Mosby, 1996.
11. Wynne-Davies R, Hall CM, Apley AG. Atlas ofskeletal dysplasias. London, England: ChurchillLivingstone, 1985; 304–308.
12. Sillence DO. Osteogenesis imperfecta: an expand-ing panorama of variants. Clin Orthop 1981; 155:11–25.
13. Gayler BW, Donner MW. Radiographic changesof the ribs. Am J Med Sci 1967; 235:588–619.
14. Gorlin RJ, Goltz RW. Multiple nevoid basal-cellepithelioma, jaw cysts and bifid rib: a syndrome.N Engl J Med 1960; 262:908–912.
15. Hunt JC, Pugh DG. Skeletal lesions in neurofibro-matosis. Radiology 1961; 76:1–19.
16. Middlemiss JH, Raper AB. Skeletal changes in thehemoglobinopathies. J Bone Joint Surg Br 1966;48:693–702.
17. Konez O, Vyas PK, Goyal M. Disseminated lym-phangiomatosis presenting with massive chylotho-rax. Pediatr Radiol 2000; 30:35–37.
18. Grabias SL, Campbell CJ. Fibrous dysplasia. Or-thop Clin North Am 1977; 8:771–783.
19. Resnick D. Endocrine diseases. In: Resnick D, ed.Diagnosis of bone and joint disorders. 3rd ed.Philadelphia, Pa: Saunders, 1995; 2036–2042.
20. Poznanski AK, Fernbach SK, Berry TE. Bonechanges from prostaglandin therapy. Skeletal Ra-diol 1985; 14:20–25.
21. Kleinman PK, Marks SC, Spevak MR, RichmondJM. Fractures of the rib head in abused infants.Radiology 1992; 185:119–123.
22. Spevak MR, Kleinman PK, Belanger PL, PrimackC, Richmond JM. Cardiopulmonary resuscitationand rib fractures in infants: a postmortem radio-logic-pathologic study. JAMA 1994; 272:617–618.
23. Guest JL, Anderson JN. Osteomyelitis involvingadjacent ribs. JAMA 1978; 239:133.
24. Teitelbaum SL. Twenty years’ experience withintrinsic tumors of the bony thorax at a large insti-tution. J Thorac Cardiovasc Surg 1972; 63:776–782.
25. Shamberger RC, Laquaglia MP, Krailo MD, et al.Ewing sarcoma of the rib: results of an intergroupstudy with analysis of outcome by timing of resec-tion. J Thorac Cardiovasc Surg 2000; 119:1154–1161.
26. Schwartz HS, Zimmerman NB, Simon MA,Wroble RR, Millar EA, Bonfiglio M. The malig-nant potential of enchondromatosis. J Bone JointSurg Am 1987; 69:269–274.
27. Bovee JV, Van Roggen JF, Cleton-Jansen AM,Taminau AH, Van Der Woude HJ, HogedoornPC. Malignant progression in multiple enchon-dromatosis (Ollier’s disease): an autopsy-basedmolecular genetic study. Hum Pathol 2000; 31:1299–1303.
28. Uchida K, Kurihara Y, Sekiguchi S, et al. Sponta-neous haemothorax caused by costal exostosis.Eur Respir J 1997; 10:735–736.
29. Resnick D. Lipoidoses, histiocytoses, and hy-poproteinemias. In: Resnick D, ed. Diagnosis ofbone and joint disorders. 3rd ed. Philadelphia, Pa:Saunders, 1995; 2215–2217.
30. Bertoni F, Unni KK, McLeod RA, Sim FH. Xan-thoma of bone. Am J Clin Pathol 1988; 90:377–384.
31. Moser RP Jr, Davis MJ, Gilkey FW, et al. PrimaryEwing sarcoma of rib. RadioGraphics 1990; 10:899–914.
32. Schulman H, Newman-Heinman N, Kurtzbart E,Maor E, Zirkin H, Laufer L. Thoracoabdominalperipheral primitive neuroectodermal tumors inchildhood: radiological features. Eur Radiol 2000;10:1649–1652.
33. Winer-Muram HT, Kauffman WM, GronemeyerSA, Jennings SG. Primitive neuroectodermal tu-mors of the chest wall (Askin tumors): CT andMR findings. AJR Am J Roentgenol 1993; 161:265–268.
104 January-February 2002 RG f Volume 22 ● Number 1
This article meets the criteria for 1.0 credit hour in category 1 of the AMA Physician’s Recognition Award. To obtaincredit, see accompanying test at http://www.rsna.org/education/rg_cme.html.