
Pediatric Renal Transplantation Abul Rish Experience and Story Professor Hani AbdelRaouf Morsi Cairo...
38
Pediatric Renal Transplantation Abul Rish Experience and Story Professor Hani AbdelRaouf Morsi Cairo university
-
Upload
clifton-stokes -
Category
Documents
-
view
226 -
download
1
Transcript of Pediatric Renal Transplantation Abul Rish Experience and Story Professor Hani AbdelRaouf Morsi Cairo...

Pediatric Renal Transplantation
Abul Rish Experience and Story
Professor Hani AbdelRaouf Morsi
Cairo university


Between 2 articles lies the story
2006
• Laparoscopic Live Donor Nephrectomy for Pediatric Recipients
2014
• Outcome of Renal Outcome of Renal Transplantation in Transplantation in Children Weighing 20 kg Children Weighing 20 kg or Lessor Less

Laparoscopic live donor nephrectomy for pediatric
recipients
Hazem Abouel Fettouh, Hani Abdel Raouf Morsi, Hossam Agabo, Ahmed Shnofy, I Abouel Fettouh
Journal of transplantation procedures 2006

Advantages
• The procedure is less morbid & more appealing to the donor.
• There is less pain, blood loss, pleural injury, disfigurement, earlier return to work.
• Avoids associated complication with the large flank incision.

Extraction incision

Renal arteryRenal vein

• All 39 cases were completed laparoscopically and no open conversion.
• The mean operative time was 145 ± 24 min.• The mean artery length was 3.1 ± 0.6 cm.• The mean vein length was 2.5 ± 0.3 cm.• The mean ureter length was 12.5 ± 1.3cm.
• The mean Nadir creatinine was 0.7 ± 0.3mg%

Conclusion
• Laparoscopic donor nephrectomy is a good option for pediatric recipient.
• No effect on the graft survival 97%
• This may expand the donor pool by a less morbid procedure used for live donation.
Outcome of Renal Outcome of Renal Transplantation in Children Transplantation in Children
Weighing 20 kg or LessWeighing 20 kg or Less
Mohammed Elsheemy, Ali Yousef, A Shoman, A Shokry, Hany Morsi, Fatina Fadel, Hesham Badawy
Journal of ped urology 2014

Patients & MethodsPatients & Methods

Recipients` data
Mean age ±SD (range) Mean weight ±SD (range)Medical history: Hypertension (HTN) CardiomyopathySurgical history: UVR, PUV, VIU
8±1.81 years (4-11)16.46±2.61 kg (11-20)
11/26 patients (42%)3/26 patients (11%) 7 patients (24%)
Mean pre-Tx dialysis ± SD 13.19±15.6months


Follow-up3 years

Complications

Survival
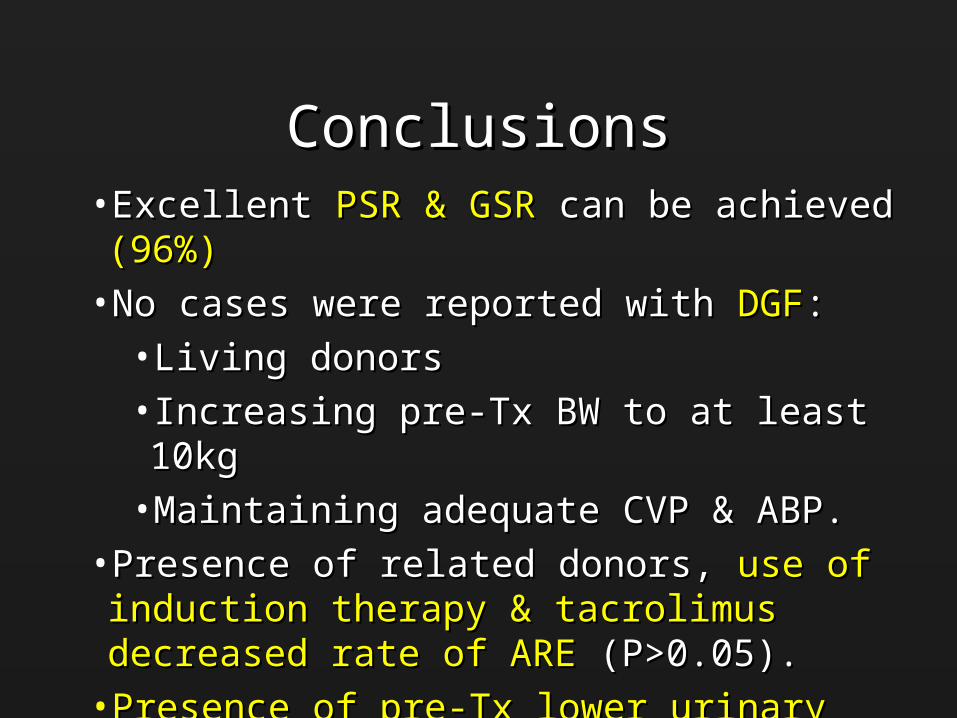
ConclusionsConclusions• Excellent Excellent PSR & GSR PSR & GSR can be achieved can be achieved (96%)(96%)
• No cases were reported with No cases were reported with DGFDGF::
• Living donorsLiving donors
• Increasing pre-Tx BW to at least 10kg Increasing pre-Tx BW to at least 10kg
• Maintaining adequate CVP & ABP. Maintaining adequate CVP & ABP.
• Presence of related donors, Presence of related donors, use of induction therapy & use of induction therapy & tacrolimus decreased rate of AREtacrolimus decreased rate of ARE (P>0.05). (P>0.05).
• Presence of pre-Tx lower urinary tract surgical Presence of pre-Tx lower urinary tract surgical interventions increased rate of UCinterventions increased rate of UC (P>0.05). (P>0.05).

Overview of 100 children

Interesting results• Age 10 years
• Weight 52% less than 20 Kg
• Sex 73% males
• Aetiology 45% urologic cause
• nephrectomy 30%
• Pretransplant Augmentation 5%
• Preemptive 4%!!

• Dondor mother 55% father 19%
Female 60% male 40%• 100% extraperitoneal• Aorta 73%• IVC 78%• Vascular anomalies 10%• Ischemia less than 1 hour in 93%• Immediate redo anastomosis in 3%!!• Direct Implantation of the ureter in 4%!!
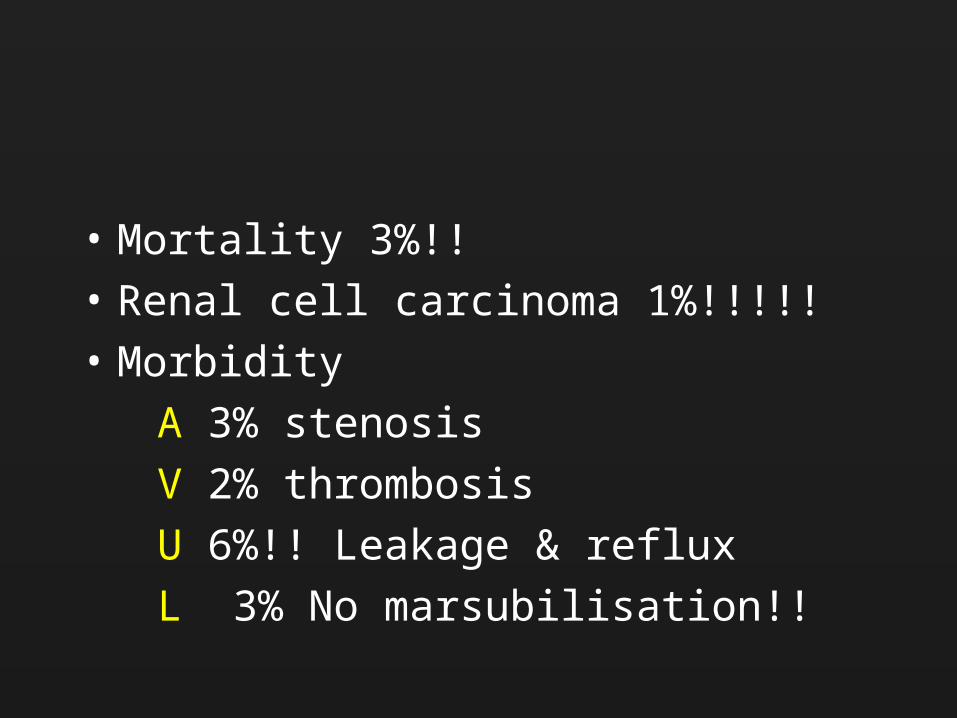
• Mortality 3%!!
• Renal cell carcinoma 1%!!!!!
• Morbidity
A 3% stenosis
V 2% thrombosis
U 6%!! Leakage & reflux
L 3% No marsubilisation!!

4 pediatric liver & kidney Tx
• 1 mortality due to liver and sepsis
• 3 doing very well (4 years follow up)

Points to remember
• Michon in Paris in christmas of 1952.
Mother to her 16 years old son, no
immunosupression, but for only 3 weeks!!
• In 1962 Starzl reached 3 years using total
body irradiation & azathioprine & steroids
Mother to her 12 years old son, again!!

Adult vs pediatric
The differences are not only related to age and size, but includes, The etiology of ESRD, physiology, technical aspects, donors, immunology, pharmacokinetics and post-transplant complications.
In addition, ESRD and transplantation have a unique effect on development and growth

Adult vs pediatric
Urological anomaly is a frequent cause of ESRD
Individualized management is the key for success of a pediatric renal transplant program. Correction of structural urogenital abnormalities and optimization of emptying and storage function of the bladder must be achieved before transplantation

Adult vs pediatric
• Vascular
• Ureteric
• Bladder
• Immunosupression
• Long life expectancy
Developing Counteries
• The true prevelance of ESRD• 10% have access to dialysis & 1% toTx• Specialisation, training, fund• Aetiology unknown, obstructive congenital anomalies, reflux,
stones,• Acute rejection 30 to 50%• Infections & malignancy PTLPD!• Growth & rehabilitation!!!

Recurrence
• FSGS
• HUS
• Congenital nephrotic syndrome
• Primary Oxalosis
• IgA nephropathy

Vaccination
• Hepatitis A & B
• DTP
• MMR
• Polio
• Pneumo
• Influenza

Infections
• Pulmonary
• Urinary
• Viral CMV
• Fungal

Malignancy
• 10 to 20 times more• PTLPD, Kaposi, Kidney & others• Follow up of donor kidney• Oncovirus• Inmunosuppressive status• Direct oncogenic effect of Immnusuppressive
drugs• Use of mTORi !!!

Corticosteroids
• CVD
• Bone and growth
• Diabetes
• Dyslipidemia & obesity

Mortality
• CVD the first cause of death in the long-term renal transplant recipients
• Pulmonary infections
• Sepsis
• Fluid & electrolytes imbalance
Molière The Imaginary Invalid
Nearly all men die of their remedies
and not of their illnesses
Almost all transplants were lost due to
CNI, not due to rejection.

Learned Lessons
• TEAM
• PROTCOL
• Tx is not the optimum solution
• Future,Dialysis, tissue engineering, bioartificial kidney,
stem cell therapy

Thank you

Thanks to Mothers


















