Pediatric Chapter4

of 14
-
Upload
nisa-khair -
Category
Documents
-
view
238 -
download
0
Transcript of Pediatric Chapter4
-
7/31/2019 Pediatric Chapter4
1/14
NATIONAL CENTER FOR HEARING ASSESSMENT & MANAGEMENT
eBook Chapter 4 Assessment of the Young Pediatric Patient 4-1
A RESOURCE GUIDE FOR EARLY HEARING DETECTION & INTERVENTION
Parents often donot understand that
the diagnostic andhabilitation process in
young children withhearing loss is a process,
and that process goeson for many years as
communication skills
emerge.
Chapter 4Assessment of the
Young PediatricPatientDiane L. Sabo, PhD
Assessment
T
he assessment and habilitationprocesses are of equal importanceand need to occur for infants and
young children within the first few monthsof life to maximize optimal outcome for achild. is chapter will focus on assessingyoung infants and children so that timelyintervention can be initiated.
e management process, includingappropriate amplification and habilitation, isdependent on having a reliable definition ofthe childs hearing loss. Tese two processesin children start off sequentially but occursimultaneously as more information isobtained about the hearing loss.
Complete audiological information isnecessary before the hearing aid fittingprocess can be completed, but reliableestimates at enough frequencies to fit ahearing aid can be used to initiate theamplification and habilitation process,with refinements and adjustments of thehearing aid fitting occurring as more and
more precise information is obtained.Delays in habilitation need not occurwhen only partial information is available,and valuable time should not be wastedwaiting for complete information. is
concept of audiologic management of theyoung child needs to be conveyed to theparents. ey oen do not understand thatthe diagnostic and habilitation processin young children with hearing loss is aprocess, and that process goes on for manyyears as communication skills emerge.
e methods used for assessment varyas a function of age as the child acquiresdifferent skills and, therefore, capabilitiesfor participation in the evaluation.Furthermore, in comparison to adultevaluation, where hearing loss can bedefined in one clinic visit, children oenrequire repeated visits before the exactconfiguration, degree, and nature of thehearing loss is defined. e audiologicassessment of children in general is atime-intensive and an ongoing process,particularly when assessing the very younginfant.
http://www.infanthearing.org/index.html -
7/31/2019 Pediatric Chapter4
2/14
A RESOURCE GUIDE FOR EARLY HEARING DETECTION & INTERVENTION
eBook Chapter 4 Assessment of the Young Pediatric Patient 4-2
The assessmentprotocols change withdevelopmental age . . .
It should be highlighted
here that behavioralaudiologic testing of theyoung child can yield
reliable results if properprocedures are followed
during the test session.
Both behavioral and physiologic tests areused in the audiologic assessment of the
very young pediatric patient. Behavioraltests are usually thought of as subjective,and physiologic tests are thought of asobjective because of their reliance or
non-reliance on patient participation,respectively. e electrophysiologic testfindings (e.g., auditory brainstem response[ABR]) oen predominate in decision-making about the management of the veryyoung child with a hearing loss, as theyare not capable of the full participationthat is necessary for behavioral testing. Forolder children, generally, the behavioralaudiologic findingswith or without ABRsupporting dataare used to determinemanagement of the hearing loss.Electrophysiologic and behavioral tests,
however, provide information on differentaspects of the childs auditory function andcannot serve as perfect substitutes for eachother. Hearing thresholds do not exactlymatch when obtained using these differentmethods.
What follows are brief descriptions ofthe behavioral and electrophysiologictests that are appropriate for theyoung pediatric patient. Typically,the assessment protocols change withdevelopmental agewith 6 months being
the typical age where children switchfrom needing physiologic testing as theprimary means of estimating thresholdsto behavioral means of assessingthresholds. It should be highlighted herethat behavioral audiologic testing of theyoung child can yield reliable results ifproper procedures are followed during thetest session.
Audiologic Assessment of
the 0 to 6 Month OldFor children referred from newbornhearing screening programs, the typicalprotocol is to obtain a diagnosticaudiologic evaluation aer two failedscreens. e exception to this are babiesin the neonatal intensive care nursery(NICU) who are referred for diagnostictesting aer one failed screen.
When the child is seen for the diagnosticaudiologic evaluation, ABR is typicallythe primary test conducted, but not inisolation of other tests. e ABR alonedoes not provide sufficient informationbut is essential for making proper
decisions about management (AmericanSpeech-Language-Hearing Association,2004). e other necessary components ofevaluation for the young child are the casehistory, acoustic immittance testing, andotoacoustic emissions.
e use of the ABR to construct theaudiogram has some limitations,although the benefits far outweigh thelimitations. e major limitation isthe choice of stimuli available that canbe used to elicit the evoked response.
Synchronous neural firing of multipleneurons is essential to record an ABR.e best stimulus to elicit a response is arapid or abrupt onset stimulus, such as aclick that stimulates a broad area of thebasilar membrane (the structure withinthe cochlea that houses the sensory cellsfor hearing and that, when stimulated,activates the auditory nerve) and thereforegenerates synchronous neural dischargein a large number of neurons. e ABRto click stimuli will provide an overallassessment of the integrity of the auditory
pathway and provide a basis on which tostart investigating thresholds at specificfrequencies.
Responses to click stimuli have been foundto correlate best with audiometric findingsin the higher frequency range fromabout 1000-4000 Hz (Coats & Martin,1977; Gorga, Reiland, & Beauchaine,1985; Gorga, Worthington, Reiland,Beauchaine, & Goldgar, 1985; Mller& Blegvad, 1976; Stapells, 1989). Sincethe click stimulus contains energy in abroad frequency range, the responsesobtained are not considered to be fromany one frequency (i.e., is not frequencyspecific). Responses obtained to clickstimuli cannot detect impairments atspecific frequencies. Use of this stimulusalone can either underestimate or miss ahearing loss at a particular frequency orfrequencies depending on the degree and
-
7/31/2019 Pediatric Chapter4
3/14
NATIONAL CENTER FOR HEARING ASSESSMENT & MANAGEMENT
eBook Chapter 4 Assessment of the Young Pediatric Patient 4-3
The stimulus commonlyused to obtain
frequency-specificinformation is a brief
duration tone burst
referred to as atone pip.
configuration of the hearing loss (Balfour,Pillion, & Gaskin, 1998; Stapells & Oates,1997). While the use of age-appropriate,latency-intensity functions together withthe threshold search will help to identifyimpairments, exact quantification of the
impairment at each frequency cannot bedone using the click stimulus. Frequency-specific or tonal stimuli must be used todetermine response levels at individualfrequencies.
e stimulus commonly used to obtainfrequency-specific information is abrief duration tone burst referred toas a tone pip. With the use of thisstimulus, fairly good synchronousneural firing can occur. e tradeoff inbecoming frequency-specific or tonal by
increasing the rise time of the stimulusis the reduction of synchronous neuraldischarge. e aim is to achieve a balanceof tonality with enough synchronousneural firing to elicit a response. It isnecessary to maintain a fast enough risetime to elicit a response yet reduce the
acoustic splatter to frequencies aboveand below the nominal frequency ofthe stimulus. Producing a frequency-specific stimulus without significantcontribution from other frequenciescan best be achieved by using gating
or stimulus shaping envelopes, such asBlackman functions (Gorga & ornton,1980). ere is some debate whether thedifference in stimulus spectrum whenusing these two gating functions equatesinto difference in the ability to predictthresholds at particular frequencies(Gorga, Kaminski, Beauchaines, &Jesteadt, 1988; Stapells & Oates, 1997).While producing a stimulus that does nothave contributions from other frequenciesis important, it will not ensure a place-specific region of excitation on the basilar
membrane. Physiologically, there isan upward spread of excitation on thebasilar membrane as the intensity level ofthe stimulus is increased beyond 70 dBSPL (Pickles, 1986). Spread of energy tofrequencies with better hearing will resultin an underestimation of threshold level.
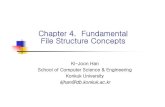
Stimulus Setting
Filter 30- 3000Hz bandpass lter
Rate Approximately 20/sec for click [remember to use an oddinteger number (e.g., 17.1, 21.3, etc.)] and approximately30/sec for tone bursts (e.g., 33.5, 31.7/sec)
Notch lter O
Amplication 100,000
Electrode array High forehead, earlobe, and low forehead
Number of sweeps 1000-2000 for clicks; 2000-4000 for tone bursts
(closer to threshold, more sweeps are needed)Time window 20 msec (15 at the minimum)
Transducer Insert earphones, unless malformations do not allow fortheir use
Starting intensity 40 dB, unless strong suspicion of severe hearing loss ispresent
Number of channels 2
Table 1Suggested Protocol
-
7/31/2019 Pediatric Chapter4
4/14
A RESOURCE GUIDE FOR EARLY HEARING DETECTION & INTERVENTION
eBook Chapter 4 Assessment of the Young Pediatric Patient 4-4
ere is not universal agreement that ABRtesting should start with a click stimulus.Many believe that starting with the clickwill give an overall estimate of quality ofresponse and, secondly, should there notbe clear identifiable waveforms, the click
can help to assess whether any cochlearresponse can be obtained (i.e., cochlearmicrophonic). e click can be thoughtof as similar to the speech recognitionthreshold (SRT). e SRT tells us verylittle of overall hearing; yet it sets a startingpoint for us to know what degree of loss(in some frequencies) might be present.While a click ABR does not tell us muchabout thresholds across the frequencyrange, it allows us to get a starting pointfor the tone bursts and assessment ofquality of response. e ABR to tonal
stimuli does not produce the high-qualityresponse that we see with the click, andknowing the type of response that anideal stimulus produces for the ABR helpswhen evaluating the ABR to tone bursts.Others, however, believe that the way toobtain frequency-specific estimation of theaudiogram is to start with a tone burst thatproduces the most click-like response (i.e.,2-4 kHz).
e rationale for this approach is that timeis saved by not getting responses to a clickstimuli. e click ABR would only be donein cases where there is no response anda need to further probe the nature of thehearing loss.
Responses to both air- and bone-conducted stimuli should be obtainedwith bone conduction to click stimuli atminimumto assess presence or absenceof air-bone gaps. While there are intensityoutput limitations in bone-conductiontesting, it oen helps to confirm thetype of auditory impairment. resholddifferences of greater than 15 dB, withbetter bone-conduction threshold thanair-conduction threshold, is indicativeof conductive involvement. To ensure
accuracy in bone-conduction thresholdtesting, particular caution needs to be paidto assure adequate headband pressure(Yang, Rupert, & Moushegian, 1987) andproper placement of the bone vibrator onthe mastoid.
A practical consideration in bone-conduction testing is electrode
placement. Electrodes cannotbe placed on the mastoidwhen bone-conductiontesting is being done because
of the small area of themastoid in children and theelectromagnetic interferencethat can occur when theelectrode is close to thebone vibrator. Moving theelectrode off the mastoidto the earlobe or in frontof the tragus in very younginfants is necessary. Use ofinsert earphones permitsplacement of the bonevibrator and maskingearphone on a small childshead. Bone-conductiontesting does require theuse of masking, althoughthere appears to be moreinteraural attenuationin young children thanadults (Stuart, Yang, &Stenstrum, 1990).
PhotocourtesyofNatusMedic
al
-
7/31/2019 Pediatric Chapter4
5/14
NATIONAL CENTER FOR HEARING ASSESSMENT & MANAGEMENT
eBook Chapter 4 Assessment of the Young Pediatric Patient 4-5
The goal of evokedpotential testing,
specifically the ABR,is to predict the
audiogram sufficiently,so that if a sensory
impairment is present,amplification can be
fit. The optimal time toconduct an ABR on achild is during sleep.
In summary, prediction of the audiogramusing the ABR is possible if proper testingconditions and parameters are used.e correspondence between behavioralthresholds and ABR thresholds is good,and the two types of thresholds are within
10-20 dB of each other (Balfour et al.,1998; Fjermedal & Laukli,1989; Gorga etal., 1988, 1985; Kileny & Magathan, 1987;Stapells, Gravel, & Martin, 1995; Stapells,Picton, & Durieux-Smith, 1994).
e goal of evoked potential testing,specifically the ABR, is to predict theaudiogram sufficiently, so that if a sensoryimpairment is present, amplification canbe fit. e optimal time to conduct anABR on a child is during sleep. ereis always an uncertainty as to how long
a child will sleep, even when sedationis used, unless conducted under verycontrolled environments, such as aprocedure room or operating room,where anesthesiologists are controllingthe state of the child. ere shouldbe a prioritization of the sequence offrequencies used during testing, as sleepstate may not sustain or it may become
very costly in the case of anesthesiology-controlled state. If the ABR is initiatedto click stimuli or 2000 Hz tone burst,the next step would be to follow this
stimulus with a low-frequency stimulus,such as a 250 or 500 Hz tone burststimulus. Following this, more frequency-specific (4000 and 1000 Hz tone burst)and bone-conduction testing shouldbe completed. While this is a guidelineon the sequence of testing, each childsfindings must be viewed and decisionsmade individually to maximize obtaininginformation about the type, degree, andcontour of impairment.For example, ifthe findings to click stimuli suggest thatan impairment is conductive, then testingby bone conduction might follow the clickwith low-frequency testing last. If theclick results imply a sloping configuration(based on the latency intensity functionsand thresholds obtained), then testingshould be done using a high-frequencystimulus followed by a low-frequencystimulus, with testing by boneconduction last.
e ABR measures the integrity of aportion of the auditory system throughapproximately the level of the midbrainand does not measure hearing in thetrue meaning of the word. As statedearlier, while agreement exists between
behavioral thresholds and ABR thresholds,there are instances where they will notagree. ere are cases of normal ABR,yet no ability to recognize or use soundto hear. Conversely, and more commonthan normal ABR and no response tosounds, is the absence of an identifiablewaveform on an ABR test that does notnecessarily equate to thresholds in thesevere-to-profound range, or no hearing.First, the ABR equipment is more limitedin output than most audiometers used totest behavioral thresholds. Consequently,
an absent ABR should not have aninterpretation of no residual hearing.Secondly, the ABR will be affected bythe neurologic status of the child. If theauditory system is damaged and neuronscannot fire synchronously, or if there aredisruptions of the auditory pathway due toan insult, then there will be no identifiableABR waveform or a partial waveformwith later waves absent, even thoughthe end organ of hearing (the cochlea)may be functioning normally. With theavailability of technology to monitor
otoacoustic emissions (OAEs) from thecochlea, discrepancies between behavioralaudiologic findings and ABR, wherebehavioral audiologic findings show betterresponses to sound than can be predictedby the ABR, are being substantiated by thepresence of OAEs.
Auditory Steady-StateResponse (ASSR)
ASSR is another evoked potential thatholds promise for predicting frequency-specific thresholds in individuals whocannot provide reliable or valid behavioralthresholds (e.g., young infants andchildren with developmental delays; Cone-Wesson, Dowell, Tomlin, Rance, & Ming,2002; Dimitrijevic, John, Van Roon, etal., 2002; Rance, Roper, Symonds, et al.,2005; Vander Werff, Brown, Gienapp,
-
7/31/2019 Pediatric Chapter4
6/14
A RESOURCE GUIDE FOR EARLY HEARING DETECTION & INTERVENTION
eBook Chapter 4 Assessment of the Young Pediatric Patient 4-6
The influence of age onthe ASSR suggests that
maturation has someinfluence on thresholddetermination in very
young infants.
Schmidt, & Kelly, 2002). e advantage ofthis measure is that it is truly an objectivemeasure, not only because there is noparticipation by the child, but also becausethe response presence or absence is basedon statistical analysis and not on visual
detection methods, as with the ABR.ASSR is oen used as a supplement to theABR and not as the only test to estimatethreshold levels, as there is still a relativepaucity of information compared to thewealth of information on the ABR.
e generation of the 80-Hz ASSR, likethe ABR, is believed to be primarily inthe brain stem (Herdman, Lins, VanRoon, Stapells, Scherg, & Picton, 2002).ASSR uses tonal stimuli (carriers) that areamplitude- and/or frequency-modulated
to evoke a response and can provideaccurate frequency-specific estimatesof air-conduction hearing levels. Forpediatric applications, the modulationoccurs at frequencies of about 80 to100 Hz, because the 80Hz ASSR can beobtained in infants and young childrenwho are asleep (Cohen, Rickards, & Clark,1991). Single or multiple stimuli presentedsimultaneously have been used to elicitthe ASSR (Picton, John, Dimitrijevic, &Purcell, 2003). is test also has the abilityto monitor both ears simultaneously,
making it attractive for possible reductionin test time compared to the ABR. Moreresearch is needed before conclusionscan be drawn as to whether there is trulya time savings monitoring both earssimultaneously.
reshold prediction using the ASSRconducted on adults and childrenwith hearing loss has been shown toprovide fairly accurate estimates of thebehavioral audiogram (Aoyagi, Suzuki,Yokota, Furuse, Wantanabe, & Ito, 1999;Dimitrijevic et al., 2002; Lins, Picton,Boucher, & Durieux-Smith,1996; Rance,Dowell, Richards, Beer, & Clark, 1998;Rance, Rickards, Cohen, et al.,1995; Stueve& ORourke, 2003; Swanepoel, Hugo, &Roode, 2004). Hearing thresholds havebeen estimated within about 10 to 15 dBin adults with normal hearing and hearingloss using the multi-frequency ASSR
(Dimitrijevic et al., 2002; Kaf, Durrant,Sabo, Boston, Taubman, & Kovacyk,2006). Less data, however, exists regardingthe use of the ASSR for measurement ofhearing in infants and children. Perez-Abalo, Savio, Torres, Martin, Rodriguez,
& Galan (2001)
found that although theywere able to determine hearing loss in thesevere and profound range, in general,only fair agreement was found betweenASSR thresholds and hearing levelsin children with mild hearing loss ornormal hearing. Recently, concerns havearisen regarding artifact under certainstimuli conditions (Gorga, Neely, Hoover,Dierking, Beauchaine, & Manning, 2004;Small & Stapells, 2003).
Little data exists regarding the use of ASSR
employing bone-conduction stimulation.Small and Stapells (2006)used multiplebone-conduction stimuli that were bothfrequency- and amplitude-modulated in agroup for preterm infants (32 to 43 weeks)and a group of post-term (0 to 8 months).e results indicated that the findings ininfants were different from those obtainedin adults, and the threshold estimates arebetter in the lower frequencies and poorerin the higher frequencies when comparedto adults.
e influence of age on the ASSRsuggests that maturation has someinfluence on threshold determination in
very young infants. Rance and Rickards(2002) found that in infants withhearing loss, the prediction of hearingthresholds was similar between young(1 to 8 months) infants and older subjectswith hearing loss. Results obtainedfrom infants with normal hearing havesuggested that maturational factors thatare sufficient to affect the differentiationbetween normal hearing and mild-to-moderate hearing loss may influence thefindings of ASSR assessments carried outin the first few weeks of life (Cone-Wessonet al., 2002; Levi, Folsom, & Dobi,1995;Rance et al., 2005; Rance & Rickards, 2002;Lins et al.,1996; Rickards, Tan, Cohen,Wilson, Drew, & Clark, 1994; Savio,Cardenas, Perez, Gonzalez, & Valdes,2001).
-
7/31/2019 Pediatric Chapter4
7/14
NATIONAL CENTER FOR HEARING ASSESSMENT & MANAGEMENT
eBook Chapter 4 Assessment of the Young Pediatric Patient 4-7
Otoacoustic emissionsare sounds that can
be recorded in the earcanal and originate from
physiologic activityinside the cochlea.
The literature is richwith evidence that this
ctivity is associated withnormal to near normal
hearing processes.
Recently, Rance and Tomlin (2006)
evaluated neonates and young infantswith normal hearing and found thatASSR threshold levels are different fromthose observed in older subjects. eyconcluded that when used clinically,
ASSR will need to take into accountdevelopmental changes occurring in thefirst weeks of life. eir findings indicatedthat ASSR thresholds in normal-hearingbabies at 6 weeks of age were not yetmature. Clearly, this is a tool that hasmuch promise as an assessment measurefor infants and young children, but furtherresearch and refinement is needed on allaspects of the ASSR to determine if it willproduce accurate audiogram predictionsin all infants.
Otoacoustic Emissions
Otoacoustic emissions are sounds thatcan be recorded in the ear canal andoriginate from physiologic activity insidethe cochlea. e literature is rich withevidence that this activity is associatedwith normal to near normal hearingprocesses. e sensory (outer) haircells within the organ of corti (sits onthe basilar membrane) are thought beresponsible for the generation of OAEs,
specifically the electromotility of the outerhair cells (Schrott, Puel, & Rebillard,1991). OAEs give us the ability to view thefunctioning of the cochlea, although notwithout contribution of the middle ear.Sounds created in the cochlea are passedthrough the middle ear via the ossicularchain and eardrum (i.e. , the middle earbones that are linked together and coupledto the eardrum) and are recorded byplacing a microphone in the ear canal.
Healthy middle ears that can transmit
sound to and from the cochlea effectivelyare essential to being able to record OAEs.Recording OAEs allows measurementof cochlear function objectively andnoninvasively. OAEs are generatedexclusively by outer hair cells. Sincemost hearing losses do not involve innerhair cell damage without outer hair celldamage (i.e., outer hair cells are generallymore vulnerable to disease and damage
than inner hair cells), the presence of anemission provides us with reasonableassurance that hearing thresholds are 30to 40 dB or better in the frequency rangewhere the emission is present. OAEs maybe absent due to middle ear dysfunction
(i.e. , the inability of the emission tobe transmitted effectively through themiddle ear or due to a sensory hearingloss affecting the outer hair cells). OAEs,however, cannot accurately predict hearinglevels, and their presence does not ensurenormal hearing. In young children, OAEsare oen of low amplitude relative tophysiologic and ambient low-frequencynoise (1000 Hz and below). Consequently,absent OAEs in low-frequency regionsalone are insufficient for determiningpresence or absence of hearing loss.
Te OAE should constitute one test in abattery of tests for accurate interpretation.OAEs are sensitive to hearing losses andcan be absent with as little as a 20 to 30 dBHL hearing loss. Te absence of an OAEresponse, however, must be viewed withinthe context of the condition of the middleear, since both the stimulus and responsepass through the middle ear. Absence ofan OAE is diagnostically significant forsensorineural hearing loss only whenmiddle ear function is relatively normal.
Consequently, middle ear status needs tobe evaluated and rounds out the clinicalprofile of hearing in children by combiningOAEs, ABR, behavioral audiometry, andacoustic immittance test results.
Acoustic Immittance
Acoustic immittance testing helps todifferentiate and/or substantiate othertest findings. Acoustic immittancetesting consists of tympanometry
and acoustic reflex testing and canbe completed on children of all ages.Standard tympanometry uses a low-frequency probe tone of 220 or 226 Hz formeasurement. However, the interpretationof the tympanogram and acoustic reflexfindings may be compromised when thisprobe tone is used with infants less than4 months of age. Findings in the ears ofinfants with middle ear fluid show normal-
-
7/31/2019 Pediatric Chapter4
8/14
A RESOURCE GUIDE FOR EARLY HEARING DETECTION & INTERVENTION
eBook Chapter 4 Assessment of the Young Pediatric Patient 4-8
appearing tympanograms when a low-frequency probe tone is used (Paradise,Smith, & Bluestone, 1976; Shurin, Pelton,& Finkelstein, 1977). e reasons forthis have not been definitively identified,although it is known that the mass and
stiffness contributions are differentbetween adults and children. Childrenhave a more mass-dominated, comparedto the adult stiffness-dominated, system.e use of a higher-probe frequency (e.g.,1000 Hz) yields tympanograms that area more valid indication of middle earfunction for infants aged 4 months or less(ASHA, 1988; Bennett & Weatherby, 1982;Himelfarb, Popelka, & Shannon, 1979;Marchant, McMillan, Shurin, et al., 1986;Margolis, 1978; Margolis, Bass-Ringdahl,Hanks, Holte, & Zapala, 2003; Margolis
& Hunter, 1991; Margolis & Popelka,1975; McKinley, Grose, & Roush, 1997;Weatherby & Bennett, 1980). e acousticreflex can be a very useful part of theaudiologic evaluation in infants. A presentreflex is added support for determiningnormal middle ear function. It is alsoimportant to use a high-frequency probeto measure the acoustic reflex in infantsunder 6 months of age (Weatherby &Bennett, 1980).
Behavioral AudiometricTesting
Behavioral Observation Audiometry (BOA)provides information about the type of
auditory response the child makes and theauditory development of the child. However,the presence of overt responses to auditorystimuli cannot be used to predict speechand language development. Knowingthe type of auditory response that a childmakes provides a basis for knowing whatresponses parents and audiologists shouldlook for once amplification is introduced.
For children over 5 to 6 months ofage, the preferred technique is VisualReinforcement Audiometry (VRA).
VRA is an operant conditioning techniquethat allows for a head turn response thatoen occurs spontaneously to sound tobe maintained through the use of visualreinforcement. VRA may be used in soundfield, but obtaining ear- and frequency-specific information is only accomplishedusing insert earphones. To maximize thequantity of information obtained duringa clinic visit (as not all children willcomplete testing for both ears in one visit),the order of stimuli presentation shouldbe prioritized to provide information
about the degree and configuration ofthe hearing loss. A good starting pointfor conditioning is to use speech stimuli,because children oen find this moreinteresting than tonal stimuli and respondnaturally with a head turn response,which then can be reinforced.
Much like the ABR, the order of testingvarious frequenciesalternating ahigh and low frequencywill yieldan audiogram that provides some,if not all, information necessary topredict the contour of a hearing loss.For example, 2000 Hz would be thestarting frequency, followed by 500Hz, 4000 Hz, and then 1000 Hz. Ifthe child stops responding before allof the frequencies have been tested,the partial results can give an idea ofthe contour of the hearing loss andimpact on the audibility of speech.
-
7/31/2019 Pediatric Chapter4
9/14
NATIONAL CENTER FOR HEARING ASSESSMENT & MANAGEMENT
eBook Chapter 4 Assessment of the Young Pediatric Patient 4-9
Play audiometry is theterm used to describe
a technique in which agame activity is used
to obtain thresholdinformation.
In the case of a severe-to-profoundhearing loss, if there is a lack ofresponsiveness at higher frequencies,the clinician should move quickly toa stimuli at 500 Hz or below. Whenconditioning to tonal stimuli cannot
be achieved, the use of a bone vibratorwith a low-frequency stimulus at high-intensity levels should be attempted. egoal is to achieve conditioning to a tactileresponse in order to verify that the childcan do the task. Possibly, the stimuluswas not audible (when presented viaphone), and, therefore, the reasonconditioning to auditory stimulus wasnot achieved.
By using reversals (i.e., change fromdecreasing-to-increasing or increasing-to-
decreasing stimulus levels), the numberof responses obtained before the childfatigues can be increased. It is reasonableto include 4 to 5 (2 to 3 responses)reversals in a testing session. eanticipated starting point can be inferredfrom the SAT or SRT, and bracketingcan then be done. Some childrenrequire reconditioning when going fromfrequency to frequency. erefore, it maybe necessary to present stimuli aboveanticipated threshold to remind theinfant what to do. Use of control trials is
the best way to reduce subjectivity andensure valid findings. Control trialsortrials with no stimulus to observe randomhead turning behaviorshould be usedto rate the reliability of the session bydetermining the number and percentageof false positive responses that occur ina session. A false positive rate greaterthan 30% would indicate that the datafrom that session was not reliable enoughto make a statement about the childshearing.
If the child is able to be conditioned, thechilds maturational or developmentallevel does not influence the thresholdlevel, and thresholds obtained usingVRA do not differ substantially fromthose obtained with adults (Nozza, 1995;Olsho, Koch, Carter, Halpin, & Carter,1987). In general, a decrease in thresholdlevel is not observed with an increase in
age, as long as conditioning is achieved(Wilson & Moore, 1978). VRA not onlyallows for assessment of threshold butalso provides information on the integrityof the auditory pathway and the childsability to detect or discriminate auditory
stimulation.
Play audiometry is the term used todescribe a technique in which a gameactivity is used to obtain thresholdinformation. Play audiometry can be usedstarting at approximately 24 months ofage, but is better at 2 1/2 to 3 years of age.Play audiometry involves conditioningthe child to respond to sound usingan activity, such as placing a peg in apegboard, placing blocks in a container,stacking rings on a stick, or placing
puzzle pieces into a puzzle. If successful,conditioning usually occurs aer four orfive guided responses or demonstrations.Oen, a social reinforcement, such asclapping hands or praising the child, isused to help to establish conditioning.Using this technique, frequency-specific and ear-specific informationcan be obtained to both air- and bone-conduction stimulation. For veryyoung children or children who havedifficulty staying on task, the sequence offrequencies should emphasize obtaining
information necessary to predict thecontour and degree of hearing loss.Complete testing of one ear need not bedone before the opposite ear is tested.Oen, if a child is responding consistentlyto a specific frequency in one ear, thatsame frequency can be rapidly tested inthe opposite ear before moving to anotherfrequency. It may be preferable to getpartial frequency information from bothears rather than complete informationfrom one ear.
Conventional audiometry can be usedby the time the child is 5 to 6 years ofage. e response is typically the same asthat used for adults, such as conditioningthe child to raise their hand in responseto the sound. As with all behavioral testtechniques, the chronological age is notthe determinant of technique; rather, it isthe developmental level of the child.
-
7/31/2019 Pediatric Chapter4
10/14
A RESOURCE GUIDE FOR EARLY HEARING DETECTION & INTERVENTION
eBook Chapter 4 Assessment of the Young Pediatric Patient 4-10
To summarize, behavioral audiologicfindings can yield reliable results, butcare must be taken to eliminate falsepositive responses. Using control trialsto observe the childs responses duringtimes of no stimulus can reduce false
positive results. Awareness of parentalcueing (oen unintentionally), patterningof presentation cues, or examiner bias canhelp to reduce subjectivity and error.
Audiologic information is necessaryto start the habilitative process. Teaudiologic evaluation in the pediatricpopulation, however, does not end with theaudiogram. Counseling, family support,and management of the hearing loss areintegral components of the evaluation.
When a child comes to the clinic, theyalways bring along a family. Audiologistsare faced not only with the challenges ofobtaining accurate audiologic informationbut helping the families with theiracceptance and readiness to advance intohabilitation if a hearing loss is identified.e audiologists skill in obtaining accurateaudiologic information is important, butso is their ability to counsel and effectivelycommunicate with the childs family.Management of hearing loss in childrenstarts with family counseling prior to
moving onto fitting of amplification andenrollment into an educational programgeared to helping those with hearing loss,such as early intervention. While thehearing aid fitting process is beginning,referral to and enrollment in an earlyintervention program is a must, so thatthe families have the educational help andsupport they need on an ongoing basis.
Counseling begins the moment youintroduce yourself to the family. It isat that time that you start to build thetrusting relationship that will be thecornerstone for effective counseling andfollow-up. Counseling should not be
thought of as something that occurs in aparticular time sequence or has a definitebeginning and end point. Counseling, likemost other aspects of pediatric audiology,is an ongoing process. Counseling shouldinvolve not only providing informationbut creating a supportive environmentfor families to work through the myriadof emotions they will experience.Information provided to families needsto be redundant, given in various forms,and repeated oen. Families need toreceive information that is balanced and
addresses the options available in theirlocal area.
e relationship between the audiologistand family changes over time as thefamily acquires the necessary knowledgeand skill to become their childs advocate.is shi will change the counselingsessions from the audiologist beingthe expert providing information onhearing and hearing loss to the familyassuming the expert role as theybecome aware of what information they
need and experts on their childs needs.ere is no set time for this change tooccur, since each child and family isdifferent with different needs, emotions,and abilities. Each family will set itsown pace of acceptance and becomingan advocate for their child. Our role aspediatric audiologists is to help familiesreach this point.
The relationshipbetween the audiologist
and family changesover time as the familyacquires the necessaryknowledge and skill to
become their childsadvocate.
-
7/31/2019 Pediatric Chapter4
11/14
NATIONAL CENTER FOR HEARING ASSESSMENT & MANAGEMENT
eBook Chapter 4 Assessment of the Young Pediatric Patient 4-11
References
American Speech-Language-Hearing Association. (1988). Tutorial on tympanometry:ASHA Working Group on Aural Acoustic-Immittance Measurements Committee onAudiologic Evaluation.Journal of Speech and Hearing Disorders, 53, 354-377.
American Speech-Language-Hearing Association. (2004). Guidelines for the audiologic
assessment of children from birth to 5 years of age. Retrieved September 22, 2009, fromhttp://www.asha.org/docs/html/GL2004-00002.htmlAoyagi, M., Suzuki, Y., Yokota, M., Furuse, H., Wantanabe, T., & Ito, T. (1999). Reliability
of 80-Hz amplitude-modulation-following response detected by phase coherence.Audiology & Neuron-otology,4, 2837.
Balfour, P., Pillion, J., & Gaskin, A. (1998). Distortion product otoacoustic emission andauditory brainstem response measures of pediatric sensorineural hearing loss withislands of normal sensitivity. Ear and Hearing, 19, 463-472.
Bennett, M., & Weatherby, L. (1982). Newborn acoustic reflexes to noise and pure tonesignals.Journal of Speech and Hearing Research, 25, 383-387.
Coats, A., & Martin, J. (1977). Human auditory nerve action potentials and brainstem-evoked responses: Effects of audiogram shape and lesion.Archives of Otolaryngology,103, 605-622.
Cohen, L. T., Rickards, F. W., & Clark, G. (1991). A comparison of steady-state-evokedpotentials to modulated tones in awake and sleeping humans.Journal of the
Acoustical Society of America,90, 24672479.Cone-Wesson, B., Dowell, R. C., Tomlin, D., Rance, G., & Ming, W. J. (2002). e auditory
steady-state response: Comparison with the auditory brainstem response.Journal ofthe American Academy of Audiology, 13, 173-187.
Dimitrijevic, A., John, M. S., Van Roon, P., Purcell, D. W., Adamonis, J., Ostroff., J.,Nedzelski, J. M., & Piston, T. W. (2002). Estimating the audiogram using multipleauditory steady-state responses.Journal of the American Academy of Audiology, 13,205-224,
Fjermedal, O., & Lazuli, E. (1989). Pediatric auditory brainstem response and pure-toneaudiometry: reshold comparison.Audiology, 18,105-111.
Gorga, M. P., Kaminski, J., Beauchaine, K., & Jesteadt, W. (1988). Auditory brainstem
responses to tone burst in normally hearing subjects.J Speech Hear Research, 31, 87-97.Gorga, M. P., Neely, S. T., Hoover, B. M., Dierking, D., Beauchaine, K., & Manning,
C. (2004). Determining the upper limits of stimulation for auditory steady-stateresponse measurements. Ear and Hearing, 25, 302-307.
Gorga, M. P., Reiland, J., & Beauchaine, K. (1985). Auditory brainstem responses in a caseof high-frequency hearing loss.Journal of Speech and Hearing Disorders, 50, 346-350.
Gorga, M. P., & ornton, A. (1980). e choice of stimuli for ABR measurements. Earand Hearing, 10, 217-230.
Gorga, M., Worthington, D., Reiland, J., Beauchaine, K., & Goldgar, D. (1985). Somecomparisons between auditory brainstem response thresholds, latencies, and pure-tone audiogram. Ear and Hearing, 6, 105-112.
Herdman, A., Lins, O., Van Roon, P., Stapells, D. R., Scherg. M., & Picton, T. W. (2002).Intracerebral sources of human auditory steady-state responses.Brain Topography,15, 6986.
Himelfarb, M., Popelka, G., & Shannon, E. (1979). Tympanometry in normal neonates.Journal of Speech and Hearing Research, 22, 179-191.
Kef, W. A., Durant, J. D., Sabo, D. L., Boston, J. R., Taubman, L. B., & Kovacyk, K. (2006).Validity and accuracy of electric response audiometry using the auditory steady-stateresponse: Evaluation in an empirical design. International Journal of Audiology, 45,211-23.
Kileny, P., & Magathan, M. (1987). Predictive value of ABR in infants and children withmoderate to profound hearing impairment. Ear and Hearing, 8, 217-221.
http://www.asha.org/docs/html/GL2004-00002.htmlhttp://www.asha.org/docs/html/GL2004-00002.html -
7/31/2019 Pediatric Chapter4
12/14
A RESOURCE GUIDE FOR EARLY HEARING DETECTION & INTERVENTION
eBook Chapter 4 Assessment of the Young Pediatric Patient 4-12
Levi, E. C., Folsom, R. C., & Dobie, R. A. (1995). Coherence analysis of envelope-following response (Errs) and frequency-following responses (Firs) in infants andadults. Hearing Research, 89, 21-27.
Lins, O. G., Picton, T. W., Boucher, B. L., & Duryea-Smith, A. (1996). Frequency-specificaudiometry using steady-state responses.Ear and Hearing, 2, 8196.
Margolis, R. H. (1978). Tympanometry in infants. State of the art. In E. R. Harford, F. H.
Bess, C. D. Bluestone, & J. O. Klein (Eds.), Impedance screening for middle ear diseasesin children (pp. 41-56). New York: Grunge & Stratton.Margolis, R. H, Bass-Ringdahl, S., Hanks, W. D., Holte, L., & Zapala, D. A. (2003).
Tympanometry in newborn infants1 kHz norms.Journal of the American Academyof Audiology, 14(7), 383-392.
Margolis, R. H., & Hunter, L. (1999). Tympanometry. Basic principles and clinicalapplications. In F. E. Musiek & W. I. Rintelmann (Eds.), Contemporary perspectives inhearing assessment(pp. 89-130.) Boston: Ally & Bacon.
Margolis, R. H., & Opelika, G. R. (1975). Static and dynamic acoustic impedancemeasurements in infants ears.Journal of Speech and Hearing Research, 18, 435-443.
McKinley, A. M., Grose, J. H., & Roush, J. (1997). Multi-frequency tympanometry andevoked otoacoustic emissions in neonates during the first 24 hours of life.Journal ofthe American Academy of Audiology, 8, 218223.
Merchant, C., McMillan, P., Shurin, P., Johnson, C., Turczyk, V., Feinstein, J., & Panek, D.(1986). Objective diagnosis of otitis media in early infancy by tympanometry andipsilateral acoustic reflex threshold.Journal of Pediatrics, 109, 590-595.
Moller, K., & Blegvad, B. (1976). Brainstem response in patients with sensorineuralhearing loss. Scandinavian Audiology, 5, 115-127.
Nozza, R. (1995). Estimating the contribution of nonsensory factors to infant-adultdifferences in behavioral thresholds. Hearing Research, 91, 72-78.
Olsho, L., Koch, E., Carter, E., Halpin, C., & Carter, E. (1987). An observer-basedpsychoacoustic procedure for use with young infants. Developmental Psychology, 23,627-641.
Paradise, J., Smith, C., & Bluestone, C. (1976). Tympanometric detection of middle eareffusion in infants and young children. Pediatrics, 58, 198-210.
Perez-Abalo, M. C., Savior, G., Torres, A., Martin, V., Rodriguez, E., & Galan, L. (2001).
Steady-state responses to multiple amplitude-modulated tones: An optimized methodto test frequency-specific thresholds in hearing-impaired children and normal-hearing subjects. Ear and Hearing, 22, 200211.
Pickles, J. O. (1986).An introduction to the physiology of hearing. San Diego: Academic Press.Picton, T. W., John, M. S., Dimitrijevic, A., & Purcell, D. (2003). Human auditory steady-
state responses. International Journal of Audiology, 42, 177-219.Rance, G., Dowell, R. C., Richards, F., Beer, D. E., & Clark, G. (1998). Steady-state evoked
potential and behavioral hearing thresholds in a group of children with absent click-evoked auditory brainstem response.Ear and Hearing,19, 4861.
Rance, G., & Rickards, F. W. (2002). Prediction of hearing threshold in infants usingauditory steady-state evoked potentials.Journal of the American Academy of
Audiology, 13, 236-45.Rance, G., Rickards, F. W., Cohen, L. T., De Vidi, S., & Clark, G. (1995). e automated
prediction of hearing thresholds in sleeping subjects using auditory steady-stateevoked potentials.Ear and Hearing,16, 499507.
Rance, G., Roper, R., Symonds, L., Moody, L., Poulis, C., Dourlay, M., & Kelly, T. (2005).Hearing threshold estimation in infants using auditory steady-state responses.Journalof the American Academy of Audiology, 16, 291-300.
Rance, G., & Tomlin, D. (2006). Maturation of auditory steady-state responses in normalbabies. Ear & Hearing, 27, 20-29.
Rickards, F. W., Tan, L. E., Cohen, L. T., Wilson, O., Drew, J., & Clark, G. (1994). Auditorysteady-state evoked potentials in newborns. British Journal of Audiology, 28, 327-337.
-
7/31/2019 Pediatric Chapter4
13/14
-
7/31/2019 Pediatric Chapter4
14/14
A RESOURCE GUIDE FOR EARLY HEARING DETECTION & INTERVENTION