Pediatric Atopic Dermatitis
101
P E D I A T R I C A T O P I C D E R M A T I T I S 1 カイルパン タラ non-commercial document; school paperwork PEDIATRIC ATOPIC DERMATITIS Author: Caroline C Spagnola, MD Consulting Staff, Department of Allergy and Immunology, Kaiser Permanente South Bay Last Updated: Apr 7, 2010 http://emedicine.medscape.com/article/911574 Introduction Background Atopic dermatitis (AD) is a chronically relapsing skin disorder with an immunologic basis. The clinical presentation varies from mild to severe. In the worst cases, atopic dermatitis may interfere with normal growth and development. Treatment consists of adequate skin hydration, avoidance of allergenic precipitants, topical anti- inflammatory medications, systemic antihistamines, and antibiotic coverage of secondary infections. Although often used interchangeably, the terms eczema and atopic dermatitis are not equivalent. Eczema is a reaction pattern with various causes and the most common pediatric cause is atopic dermatitis. Other causes of eczematous dermatitis include allergic contact dermatitis, irritant contact dermatitis, seborrheic dermatitis, nummular eczema, dyshidrotic eczema, asteatotic eczema, and lichen simplex chronicus. Eczematous reactions can be classified as acute, subacute, or chronic, depending on historical and physical characteristics. The images below depict patients with atopic dermatitis.
-
Upload
tara-sefanya-kairupan -
Category
Documents
-
view
124 -
download
2
description
Non commercial document, used only for school work
Transcript of Pediatric Atopic Dermatitis

P E D I A T R I C A T O P I C D E R M A T I T I S
1
カイルパン タラ
non-commercial document; school paperwork
PEDIATRIC ATOPIC DERMATITIS
Author: Caroline C Spagnola, MD Consulting Staff, Department of Allergy and Immunology, Kaiser Permanente South Bay
Last Updated: Apr 7, 2010 http://emedicine.medscape.com/article/911574
Introduction
Background
Atopic dermatitis (AD) is a chronically relapsing skin disorder with an immunologic basis. The clinical presentation varies from mild to severe. In the worst cases, atopic dermatitis may interfere with normal growth and development. Treatment consists of adequate skin hydration, avoidance of allergenic precipitants, topical anti-inflammatory medications, systemic antihistamines, and antibiotic coverage of secondary infections.
Although often used interchangeably, the terms eczema and atopic dermatitis are not equivalent. Eczema is a reaction pattern with various causes and the most common pediatric cause is atopic dermatitis. Other causes of eczematous dermatitis include allergic contact dermatitis, irritant contact dermatitis, seborrheic dermatitis, nummular eczema, dyshidrotic eczema, asteatotic eczema, and lichen simplex chronicus. Eczematous reactions can be classified as acute, subacute, or chronic, depending on historical and physical characteristics.
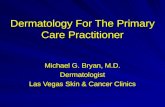
The images below depict patients with atopic dermatitis.

P E D I A T R I C A T O P I C D E R M A T I T I S
2
カイルパン タラ
non-commercial document; school paperwork
Typical atopic dermatitis on the face of an infant.
Flexural involvement in childhood atopic dermatitis.
Pathophysiology
Clinically unaffected skin in patients with atopic dermatitis has increased numbers of T-helper type 2 (Th2) cells compared with skin in patients without atopic dermatitis. Increased levels of interleukin (IL)-4 and IL-13 (Th2 cytokines) are seen in acute atopic dermatitis skin lesions, whereas chronic atopic dermatitis lesions show increased expression of IL-5 (Th2 cytokine) and IL-12 and interferon (IFN)-γ (Th1 cytokines). Chronic atopic dermatitis lesions also exhibit greater eosinophil infiltration compared with skin in patients without atopic dermatitis.
IL-4 enhances differentiation of T-helper cells along the Th2 pathway, and IL-13 acts as a chemoattractant for Th2 cells to infiltrate atopic dermatitis lesions. IL-13 may also directly induce IL-5 expression and eosinophil infiltration, thereby facilitating the transition from acute lesions into chronic lesions.[1]
In addition, patients with atopic dermatitis appear to have significantly decreased levels of skin barrier molecules compared with normal controls. Ceramide lipids in the stratum corneum, which are responsible for water retention and permeability functions, and skin barrier proteins such as filaggrin are expressed at significantly lower levels in the skin of patients with atopic dermatitis compared with the skin of patients without atopic dermatitis.[1,2]

P E D I A T R I C A T O P I C D E R M A T I T I S
3
カイルパン タラ
non-commercial document; school paperwork
Frequency
United States
Atopic dermatitis occurs in approximately 10-20% of children and 2% of adults.[1] Children with concurrent asthma or hayfever have a 30-50% incidence of developing atopic dermatitis.
International
Prevalence rates for atopic dermatitis in children over a 1-year period ranged from around 2% in Iran and China to about 20% in Australasia, England, and Scandinavia.[3] Interestingly, populations that migrate from areas of low prevalence to areas of higher prevalence have shown an increased incidence of atopic dermatitis, bolstering the idea of strong environmental influences in the development of atopic dermatitis.
Race
No clear racial predilections have been identified.
Sex
Males and females are affected with equal incidence and severity.
Age
Atopic dermatitis may occur in people of any age but often starts in infants aged 2-6 months. Ninety percent of patients with atopic dermatitis experience the onset of disease prior to age 5 years.[4]
Seventy-five percent of individuals experience marked improvement in the severity of their atopic dermatitis by age 14 years; however, the remaining 25% continue to have significant relapses during their adult life. A recent study concluded that the prevalence of atopic dermatitis in children younger than 2 years was 18.6%.[5]
Clinical
History
Diagnostic criteria for atopic dermatitis (AD) have been proposed by Hanifin and Rajka (1980) and largely adopted by the American Academy of Allergy, Asthma, and Immunology.[6] Appropriate cases

P E D I A T R I C A T O P I C D E R M A T I T I S
4
カイルパン タラ
non-commercial document; school paperwork
must have at least 3 major characteristics and at least 3 minor characteristics.
Major characteristics include the following: o Pruritus o Typical morphology and distribution (ie, flexural
lichenification and linearity in adults, facial and extensor involvement in infants and young children)
o Chronic or chronically relapsing dermatitis o Personal or family history of atopy (eg, asthma, allergic
rhinoconjunctivitis, atopic dermatitis)
Minor characteristics are as follows: o Xerosis (dry skin) o Ichthyosis, palmar hyperlinearity, keratosis pilaris o Hand dermatitis, foot dermatitis o Cheilitis o Nipple eczema o Susceptibility to cutaneous infection (eg, with
Staphylococcus aureus, herpes simplex virus [HSV], other viruses, warts, molluscum, dermatophytes)
o Erythroderma o Perifollicular accentuation o Pityriasis alba o Early age of onset o Impaired cell-mediated immunity o Recurrent conjunctivitis o Orbital darkening o Infraorbital fold (eg, Dennie pleat, Morgan fold) o Anterior neck folds o Keratoconus o Anterior subcapsular cataracts o Sensitivity to emotional factors o Food intolerance o Pruritus with sweating o Intolerance of wool o White dermographism o Immediate type I skin test response

P E D I A T R I C A T O P I C D E R M A T I T I S
5
カイルパン タラ
non-commercial document; school paperwork
o Elevated total serum immunoglobulin E (IgE) o Peripheral blood eosinophilia
Most children with atopic dermatitis relate a history notable for intense pruritus and dry skin. The quality of the pruritus is referred to as a spreading itch. Affected children often have a lowered itch threshold, resulting in increased levels of cutaneous reactivity in response to stimuli. Patients may succumb to a vicious itch-scratch-itch cycle, in which pruritus stimulates a bout of scratching. This, in turn, increases skin inflammation and triggers a greater sensation of itching, thus exacerbating flares.
Altered cell-mediated immunity has been noted in patients with atopic dermatitis. This is clinically observed as a history of repeated unusual cutaneous infections (eg, eczema herpeticum, warts, molluscum, dermatophytes).
Physical
Three classes of skin lesions are recognized. o Acute - Intensely pruritic erythematous papules and vesicles
overlying erythematous skin; frequently associated with extensive excoriations and erosions accompanied by serous exudates
o Subacute - Erythema, excoriation, and scaling o Chronic - Thickened plaques of skin, accentuated skin
markings (lichenification), fibrotic papules (prurigo nodularis); possible coexistence of all 3 types of lesions in chronic atopic dermatitis
Typical locations of lesions by age o Nonmobile infant - Face and scalp o Crawling infant - Extensor surfaces of extremities, trunk, face,
and neck o Older child and adolescent - Wrists, ankles, antecubital
fossae, popliteal fossae, and neck o Adult - May be limited to hand and foot eczema
Associated findings in atopic dermatitis include keratosis pilaris; accentuated palmar creases; lichenification; atopic pleats; allergic shiners; transverse nasal crease; pallor around

P E D I A T R I C A T O P I C D E R M A T I T I S
6
カイルパン タラ
non-commercial document; school paperwork
the nose, mouth, and ears; white dermographism; cataracts; and keratoconus.
o Keratosis pilaris, or plucked-chicken skin, consists of large cornified plugs in the upper part of hair follicles and produces a stippled appearance of the skin on the outer aspects of the arms and legs and on the buttocks and trunk.
o Hyperlinear palms are usually present at birth and persist throughout life. These consist of an increased number of fine lines and accentuated markings on the palms.
o Lichenification of the wrists, ankles, popliteal fossae, or antecubital fossae is characteristic of chronic atopic dermatitis. It is observed as thickened, leathery, hyperpigmented patches of skin with a deepening of normal skin creases.
o Atopic pleats (also referred to as Morgan-Dennie folds, Morgan folds, Dennie pleats, or mongolian lines) are skin folds observed just below the lower lid of both eyes and are retained throughout life.
o Allergic shiners are violet-gray infraorbital discolorations caused by underlying vascular stasis. Increased pressure on nasal and paranasal venous plexuses causes edema in these areas, leading to development of atopic pleats and allergic shiners.
o A prominent transverse nasal crease is a common sign of concurrent allergic rhinitis and, along with allergic shiners and atopic pleats, may be a clue to the diagnosis of an atopic diathesis.
o Dermographism is a normal reaction in 5% of the population. After a firm pointed instrument is stroked against the skin, the path of the instrument is observed as a red line followed by an erythematous flare that ultimately develops into a wheal. This response occurs within 3 minutes of the insult. White dermographism is a paradoxical reaction wherein the initial red line is replaced within 10 seconds by a white line and an absence of a wheal. This reaction can be observed in atopic dermatitis and allergic contact dermatitis.
o Atopic cataracts affect 4-12% of patients with AD and occur much earlier in life than senile cataracts. They typically are bilateral, central, and shield-shaped, and they mature rapidly. Because patients generally are asymptomatic, diagnosis is

P E D I A T R I C A T O P I C D E R M A T I T I S
7
カイルパン タラ
non-commercial document; school paperwork
usually made by slit lamp examination. Incidence of cataracts in atopic patients appears to be unrelated to the use of topical steroids.
o Keratoconus is an elongation of the corneal surface that is thought to be caused by long-term eye rubbing and may be a degenerative change in the cornea. Keratoconus affects approximately 1% of children with atopic dermatitis and can generally be alleviated with the use of contact lenses.
Causes
The etiology of atopic dermatitis appears to be linked both to genetic causes and to environmental agents.
The prevalence of atopic dermatitis in children with one affected parent is 60% and rises to nearly 80% for children of two affected parents. Additionally, nearly 40% of patients with newly diagnosed cases report a positive family history for atopic dermatitis in at least one first-degree relative. Children of parents with atopic dermatitis have an increased risk of developing atopic dermatitis by age 3 years.[7]Much higher concordance rates for atopic dermatitis are observed in monozygotic twins (77%) than in dizygotic twins (15%).[1]
Recent evidence has demonstrated a strong genetic predisposition towards the development of atopic dermatitis in patients with loss-of-function mutations in the gene that encodes the epidermal structural protein filaggrin (FLG). Filaggrin deficiency causes a significant defect in the normal epidermal barrier that allows for enhanced allergen absorption through the skin, resulting in a higher incidence of dermatitis. FLG gene mutations have been associated with a more severe atopic dermatitis phenotype, earlier onset of atopic dermatitis, increased levels of systemic allergen sensitivity, and a higher proportion of patients with atopic dermatitis who eventually develop asthma.[8]
In addition, the specific loss-of-function null mutation R501x in the filaggrin gene appears to confer a higher risk of developing eczema herpeticum, which is a rare but serious complication that requires treatment with antiviral medications.[9]

P E D I A T R I C A T O P I C D E R M A T I T I S
8
カイルパン タラ
non-commercial document; school paperwork
Prenatal risk factors for atopic dermatitis are under investigation. Term infants of mothers who had gestational diabetes during pregnancy had an almost 8-fold increase in the prevalence of atopic dermatitis by age 6 years. Interestingly, this relationship did not occur in preterm infants of mothers with gestational diabetes. The reasons for this discrepancy are yet to be determined.[10]
Environmental allergens repeatedly have been shown to trigger exacerbations of atopic dermatitis in susceptible individuals. Contact irritants, climate, sweating, aeroallergens, microbial organisms, and stress/psyche commonly trigger exacerbations.
o Contact irritants (eg, soaps, solvents, wool clothing, mechanical irritants, detergents, preservatives, perfumes) compromise the integument, creating inflammation, irritation, and a portal of entry for further environmental insult. These surface irritants, along with the macerative effects of sweating and the drying effects of low humidity, lower the pruritic threshold. A vicious cycle of itching and scratching ensues, in which added cutaneous damage caused by scratching further lowers the pruritic threshold and subsequently causes increased itching.
o Aeroallergens (eg, house dust mite, molds, pollen, dander) induce peripheral eosinophilia and elevate serum IgE levels. These early effects lead to increased histamine release from IgE-activated mast cells and elevated activity of the T-helper cell–mediated immune system. The increased release of vascular mediators (eg, bradykinin, histamine, slow-reacting substance of anaphylaxis [SRS-A]) induces vasodilation, edema, and urticaria, which in turn stimulate pruritus and inflammatory cutaneous changes.
o Microbial agents (eg, S aureus, Pityrosporum yeasts, Candida organisms, Trichophyton dermatophytes) act in 2 different ways to promote the flares of atopic dermatitis. The microorganisms directly invade the skin, creating local injury and inflammation, and they induce a systemic allergic response to specific antigens, causing a rise in serum IgE and enhanced activity of the immune system.

P E D I A T R I C A T O P I C D E R M A T I T I S
9
カイルパン タラ
non-commercial document; school paperwork
Nearly all patients with atopic dermatitis are colonized by S aureus on lesional skin. More than half of patients with atopic dermatitis are colonized by S aureus strains capable of producing superantigens. These patients can develop superantigen-specific IgE antibodies that activate inflammatory cells in the skin. Staphylococcal enterotoxin B is a superantigen known to upregulate interleukin (IL)-31 expression in skin. IL-31 has been shown to induce pruritus and skin lesions resembling atopic dermatitis in mice.[1]
Specific IgE levels to Malassezia furfur have been correlated with atopic dermatitis severity in a subgroup of patients. These Malassezia -specific IgE antibodies have been shown to crossreact with autoantigens in atopic dermatitis skin.[1]
o Food allergy is implicated as a cause in one third to one half of children with atopic dermatitis. Food allergens may be the initial trigger for IgE autoreactivity to epithelial autoantigens in young children with atopic dermatitis.[1]The most common food allergens in children are egg, soy, milk, wheat, fish, shellfish, and peanut, which together account for 90% of food-induced cases of atopic dermatitis in double-blind, placebo-controlled food challenges. Fortunately, many clinically significant food allergies self-resolve within the first 5 years of life, eliminating the need for long-term restrictive diets.
o Stress may trigger atopic dermatitis at the sites of activated cutaneous nerve endings, possibly by the actions of substance P, vasoactive intestinal peptide (VIP), or via the adenyl cyclase–cyclic adenosine monophosphate (cAMP) system.
Differential Diagnoses
Acrodermatitis Enteropathica Phenylketonuria
Contact Dermatitis Scabies
Herpes Simplex Virus Infection
Hyperimmunoglobulinemia E
Staphylococcus Aureus Infection
(Job) Syndrome Wiskott-Aldrich Syndrome

P E D I A T R I C A T O P I C D E R M A T I T I S
10
カイルパン タラ
non-commercial document; school paperwork
Other Problems to Be Considered
Seborrheic dermatitis
Psoriasis
Workup
Laboratory Studies No definitive laboratory tests are used to diagnose atopic
dermatitis (AD). Elevated serum immunoglobulin E (IgE) levels and peripheral
blood eosinophilia occur in most individuals with atopic dermatitis, and these findings may be useful in confirming the atopic status of suspected cases.
The presence of serum IgE directed against the cell wall of S aureus is observed in hyper-IgE syndrome and atopic dermatitis.
Common infections that mimic or complicate atopic dermatitis can be tested for as follows: conduct a Tzanck smear for herpes simplex virus (HSV), a potassium hydroxide (KOH) preparation for dermatophytes, and a Gram stain for bacterial infections.
Other Tests Prick skin testing to common allergens can help identify
specific triggers of atopic dermatitis. For accuracy, antihistamines must be discontinued for 1 week and topical steroids for 2 weeks prior to testing. Although skin tests are used most often in young children with moderate-to-severe disease, false-negative and false-positive test results are not uncommon in children younger than 8 years. If positive, these tests do not necessarily indicate clinically significant triggers. Prick skin tests only indicate that the patient has been sensitized to particular antigens. For example, most children shown to have multiple food allergies by skin tests only demonstrate clinically detectable allergic reactions to 3 or fewer foods when tested by double-blind randomized provocative testing.
Radioallergosorbent test (RAST) and enzyme-linked immunosorbent assay (ELISA) in vitro tests identify serum IgE

P E D I A T R I C A T O P I C D E R M A T I T I S
11
カイルパン タラ
non-commercial document; school paperwork
directed toward specific allergens (allergen-specific IgE). As with prick skin tests, these diagnostic methods show a poor predictive value for clinically significant food allergies and may produce false-positive results when the patient's serum contains elevated nonspecific (or total) IgE levels.
Histologic Findings Acute eczematous lesions show histologic markings of
hyperkeratosis, parakeratosis, and acanthosis with a decreased or absent granular cell layer.
Important features in histologic diagnosis include spongiosis (accumulation of fluid in the intercellular and intracellular areas) and exocytosis (infiltration of leukocytes through the epidermis).
Chronic eczematous lesions display hyperkeratosis with areas of parakeratosis and papillomatosis (upward proliferation of dermal papillae).
Treatment
Medical Care The most fundamental and important step in combating atopic
dermatitis (AD) is rehydration of the stratum corneum. Adequate rehydration preserves the stratum corneum barrier, minimizing the direct effects of irritants and allergens on the skin and maximizing the effect of topically applied therapies, thus decreasing the need for topical steroids.
o Lukewarm soaking baths lasting 10-20 minutes are ideal.[4]Extremely hot water should be avoided to prevent both vasodilation, which can trigger pruritus, and the damage to the skin barrier caused by scalding.
o Small amounts of bath oils or emulsification agents may be used for added hydration benefits in older children and adolescents. Bath oils or emulsification agents result in slippery conditions; warn patients and parents of the resultant risks of trauma and drowning after a fall. Readily available over-the-counter bath agents include Aveeno

P E D I A T R I C A T O P I C D E R M A T I T I S
12
カイルパン タラ
non-commercial document; school paperwork
Colloid Oatmeal, RoBathol, Maypo, cottonseed oil with Brij 93, or mineral oil.
o Recommended soaps are mild and unscented with a neutral pH. Examples include Dove, Oil of Olay, Caress, Camay, Aveeno, and Purpose. Even these mild soaps are often too drying for atopic skin. If the children are prepubertal, bathing in water alone may be preferable. Postpubertal patients need to use soap in the axillae and groin but do not need it elsewhere.
o If soaps are too irritating to the skin, hydrophobic lotions and creams, such as Cetaphil, Diprobase, and Unguentum Merck, may be used. These agents have excellent cleansing properties and low potential for irritation. They should be applied without water and rubbed gently over the skin surface until a light foaming occurs. A soft cotton cloth or tissue can then be applied to wipe away the agent, leaving behind a protective film of stearyl alcohol and propylene glycol.
o Baby shampoo may be used to manage scalp dermatitis.
Baths should be followed by the immediate application of an occlusive emollient over the entire skin surface to retain moisture in the epidermis. If an emollient is not applied within 3 minutes of leaving the bath, evaporation causes excess drying of the skin. Skin should not be completely dried with a towel prior to application of the emollient; rather, lightly patting the skin with a towel to remove excess moisture is sufficient.
o Frequently recommended emollients are hydrophobic and ointment-based; these include Vaseline petrolatum jelly, Crisco, vegetable oil, Aquaphor, and Elta. Occasionally, parents may find these agents too greasy for everyday use, and cream-based alternatives may be offered. Common creams include DML Forte, Moisturel, Aveeno, Curel, Purpose, Dermasil, Neutrogena, and Eucerin. This latter group of moisturizers is less effective because of the weaker occlusive effects of creams as compared to ointments; thus, they should be used only if the ointment-based emollients are not well tolerated.

P E D I A T R I C A T O P I C D E R M A T I T I S
13
カイルパン タラ
non-commercial document; school paperwork
o The newest type of moisturizing product is a ceramide-dominant, lipid-based emollient (TriCeram) aimed at repairing the stratum corneum barrier function lost in atopic dermatitis. One study showed a significant decrease in clinical severity scores and a decrease in transepidermal water loss in children whose traditional moisturizers were replaced by TriCeram for 3 weeks.[11]
o Urea-containing products have been shown to soften and moisturize dry skin. Commonly available preparations include Aquacare cream or lotion and Ureacin Crème. Alpha-hydroxy and lactic acid preparations also are helpful as moisturizers. Name brands include Aqua Lacten Lotion, AmLactin Lotion, LactiCare Lotion, Lac-Hydrin Lotion, and Nutraderm 30. In addition, 12% ammonium lactate lotion has been shown to improve skin barrier function and even to mitigate dermal or epidermal atrophy induced by corticosteroids.[11]Because of the stinging sensation experienced by children with acute or fissured dermatoses, the 10% urea concentration is preferred over the higher concentrations, and care should also be used in the application of the alpha-hydroxy and lactic acid preparations. LactiCare-HC Lotion also contains hydrocortisone to further benefit acute flares of atopic dermatitis.
o For children with repeated cutaneous infections, adding 2 teaspoons of household bleach (eg, Clorox) per gallon of bath water can help reduce the incidence of such infections. A typical bathtub holds approximately 25-40 gallons of water. During acute atopic dermatitis exacerbations, pouring 1 cup of table salt into the bath may ameliorate the stinging effect these children frequently experience while bathing.
o Wet dressings are very useful for diverse types of atopic dermatitic flares. They can be used on dry lichenified lesions to improve hydration and increase the penetration of topical corticosteroids; they also work well to dry weeping or oozing lesions via evaporation. The cooling sensation on the skin that results from slow evaporation with wet dressings has an anti-inflammatory effect and suppresses itching. The mechanical barrier of the wet dressing also prevents scratching, allows more rapid healing of lesions, and offers protection from contact with allergens and bacteria. Care

P E D I A T R I C A T O P I C D E R M A T I T I S
14
カイルパン タラ
non-commercial document; school paperwork
should be taken to use only adequately diluted corticosteroid preparations (if used) under occlusive dressings to prevent hypothalamic-pituitary-adrenal axis suppression and local adverse effects on the skin. Wet wrap implementation should be delayed at least 2-3 days after beginning antibiotic treatment for superinfected lesions to allow for observation of clinical improvement of infected sores.[2]
o Burow solution 1:40 is a commonly used wet dressing because it is germicidal and directly suppresses weeping lesions by precipitation of protein. The solution is prepared easily by dissolving one Domeboro packet or effervescent tablet in a pint of tepid or lukewarm tap water. Using lukewarm water is essential because hot water induces vasodilatation with increased weeping and pruritus, whereas cold water causes vasoconstriction and secondary vasodilation. Submerge a soft cloth (eg, handkerchief, thin diaper, strips of bed sheets) into the solution until moderately wet but not dripping. Place the dressing over the affected skin site, periodically rewetting the compress. In severe cases, a topical corticosteroid may be applied after the compress for enhanced penetration and action of the medication.
o Seek psychologic counseling, biofeedback, relaxation techniques, massage therapy, and behavioral modifications if emotional stressors are a contributing factor to atopic dermatitis.
Ultraviolet light may benefit some patients. o Ultraviolet light in the UVB range may provide control and
eliminate or markedly reduce the need for steroids. The new narrow band units are especially effective. Ultraviolet light in the UVA range has been used alone, in combination with oral psoralen administration (PUVA), or with high-dose UVA 1 (ie, 340-400 nm spectrum units).
o A significant decline in the usage of UVA light therapy and psoralen has been recently observed because this regimen clearly accelerates photoaging and increases the risk of skin cancer. UVA 1 spectrum light works by reducing cellular immunoglobulin E (IgE) binding sites and inducing apoptosis in inflammatory cells and has demonstrated significant efficacy in treating atopic dermatitis. A small number of

P E D I A T R I C A T O P I C D E R M A T I T I S
15
カイルパン タラ
non-commercial document; school paperwork
patients develop erythema or disease flares with light treatment.
Allergen immunotherapy is currently indicated only for patients with allergic rhinitis or allergic asthma. However, several small randomized controlled trials have shown a significant clinical benefit of subcutaneous immunotherapy or sublingual immunotherapy with house dust mite extract in patients sensitized to the house dust mite. Larger randomized, double-blind, placebo-controlled trials are needed to confirm these findings.[12]
Consultations Consider consultation with an allergist/immunologist or dermatologist for the following conditions:
Atopic dermatitis that is severe (eg, 20% skin involvement, 10% skin involvement with eyelids/hands/intertriginous areas affected) or is refractory to first-line treatments
Erythroderma or extensive exfoliation Infectious complications Ocular complications Psychosocial complications Coexisting asthma or allergic rhinitis Impaired quality of life Identification of triggers and allergens Atopic dermatitis requiring hospitalization or more than one
course of systemic steroids Uncertain diagnosis
Diet
Whether breastfeeding can help prevent development of atopic dermatitis in children remains unclear. A clinical report from the American Academy of Pediatrics recommended exclusive breastfeeding as opposed to cow's milk formula feeding over the first 4 months of life to prevent development of atopic dermatitis in infants at high risk of developing atopy.[13] However, several studies have found no protective

P E D I A T R I C A T O P I C D E R M A T I T I S
16
カイルパン タラ
non-commercial document; school paperwork
benefit of exclusive breastfeeding in the first 3-6 months of life.[14,15]
Supplementation with extensively hydrolyzed formulas in infants at high risk of developing atopic dermatitis appeared to be more effective at preventing atopic dermatitis than supplementation with partially hydrolyzed formulas or cow's milk formulas.[13]
For children older than 5 years, nutritionally adequate elimination diets are the goal if double-blind placebo-controlled trials indicate a clinically significant food allergy. However, most skin tests, radioallergosorbent tests (RASTs), and enzyme-linked immunosorbent assays (ELISA) that reveal positive results against food allergens are not borne out to cause disease flares in clinical trials; thus, elimination diets are only rarely indicated.
Activity
Prohibit smoking in the home and in other areas that are frequented by children with allergies.
Implement dust mite control measures for children with documented sensitivity to dust mites. Counsel parents to use dust mite–proof plastic cases around pillows, mattresses, and box springs. Wash bedding in hot water weekly to remove dust mites. Remove carpets and drapes from the bedroom or vacuum carpets and drapes weekly to remove dust mites.
In the subgroup of children with atopic dermatitis who also experience respiratory allergies to animal allergens, parents should consider removing animals from the home or confining them to areas of the house where susceptible children do not come into contact with their dander or saliva.
Avoid irritants that trigger the itch-scratch-itch cycle (eg, soaps, detergents, chemicals, abrasive clothing, extremes of temperature and humidity).
o Use pH-neutral minimally defatting soaps (eg, Dove). Avoid excessive drying of the skin with alcohol-containing astringents. Launder new clothes before wearing to remove manufacturing chemicals. Use liquid detergent rather than

P E D I A T R I C A T O P I C D E R M A T I T I S
17
カイルパン タラ
non-commercial document; school paperwork
powder detergent and add a second rinse cycle to remove all residual detergent.
o Wear loose fitting open-weave cotton or cotton-blend clothing; avoid wool.
o Use a humidifier in the winter to prevent excessive skin dryness and an air conditioner in the summer to prevent sweating and associated macerative effects on the skin. Decreased humidity indoors helps prevent the growth of mold.
Medication
Topical corticosteroids are the mainstay of treatment of atopic dermatitis (AD). These medications reduce inflammation and pruritus primarily by inhibiting the transcriptional activity of various proinflammatory genes. Topical steroids should be applied only to areas of acute exacerbations, whereas emollients should be used over the remainder of the skin. The absorption of topical steroids is much better through hydrated skin; thus, the ideal time for application is in the first 3 minutes after a bath or shower. The various topical steroid formulations, in ascending order of occlusiveness, include lotions, creams, gels, and ointments.
Lotions contain water and may be drying because of the evaporative effect; thus, they are used mostly in scalp and beard areas where drying effects are not as problematic. Lotions containing alcohol may cause a burning sensation upon application, especially on skin with fissured or ulcerated areas. Lotions may contain preservatives, solubilizers, and fragrances that can irritate the skin.
Creams are generally well tolerated but are less moisturizing than ointments. Creams are popular for their nongreasy appearance on treated skin and are more convenient during hot weather because they cause less occlusion of eccrine sweat glands than ointments and gels. As with lotions, creams may contain preservatives, solubilizers, and fragrances that can irritate the skin.
Gels are highly occlusive, but the propylene glycol base is irritating to the skin and promotes dryness. Therefore, gels, similar to lotions, are used mostly in scalp and beard areas where the drying effects are not

P E D I A T R I C A T O P I C D E R M A T I T I S
18
カイルパン タラ
non-commercial document; school paperwork
as problematic. They are very effective in the management of acute weeping or vesicular lesions of atopic dermatitis.
Ointments are the most moisturizing of the topical steroid vehicles, but their occlusiveness may not be well tolerated because of their interference with sweat gland function and resultant development of sweat retention dermatitis, especially in warm humid climates. Ointments are the preferred vehicle for thickened, lichenified plaques of atopic dermatitis.
Systemic corticosteroids have been used in severe chronic atopic dermatitis, but use has been limited in the pediatric population because of the risk of severe adverse effects associated with chronic usage, including growth retardation and immune suppression.
Oral antihistamines are effective as systemic antipruritics, sedatives, and mild anxiolytics. These are beneficial especially at nighttime because pruritus is usually worse at night. Commonly used oral antihistamines include diphenhydramine, hydroxyzine, and doxepin. Pramoxine is a topical antipruritic agent and can be found as Prax, Pramosone, or PrameGel.
Coal tar topical preparations have antipruritic and anti-inflammatory effects. They work as disinfectants and astringents and help to correct abnormal keratinization by decreasing both epidermal proliferation and dermal infiltration. They are effective as second-line agents for subacute, chronic, and lichenified atopic dermatitis. Cosmetically acceptable preparations recently have been made available and include AquaTar, Estar, Fototar, PsoriGel, and Neutrogena T/Derm Tar Emollient. Tar shampoos, such as Neutrogena T-Gel, are effective for scalp involvement. Adverse effects may include folliculitis and photosensitivity.
Topical calcineurin inhibitors (eg, tacrolimus, pimecrolimus) are the newest class of topical medications for atopic dermatitis. These nonsteroidal immunomodulators act by down-regulating the mediator release or cytokine expression of various cells, including Th1 helper cells, Th2 helper cells, mast cells, eosinophils, keratinocytes, and Langerhans cells. Calcineurin inhibitors may be

P E D I A T R I C A T O P I C D E R M A T I T I S
19
カイルパン タラ
non-commercial document; school paperwork
especially useful for treating face, groin, or axillary areas, where steroid-sparing treatments are preferred.
Systemic cyclosporine can dramatically reverse severe flares of atopic dermatitis. Because of the risk of severe adverse effects, this treatment should be limited in duration. Once control is obtained, alternative maintenance therapy should be instituted.
Experimental treatments for atopic dermatitis have included trials of gamma-interferon and IL-2; both are inhibitors of Th2 cell functions and have been promising. Oral mycophenolate mofetil, an inhibitor of purine synthesis, has also been shown to be an effective alternative form of treatment for severe disease. A small study of 6 patients with severe atopic dermatitis showed promising results for treatment with anti-CD20 monoclonal antibody (Rituximab).[16]
Some evidence suggests that the use of traditional Chinese medicine herb combinations may result in short-term improvements in SCORing of Atopic Dermatitis (SCORAD) index scores, quality of life scores, and topical steroid use.[17]However, larger trials to evaluate safety and long-term efficacy are needed.
Conflicting results have been reported regarding the use of probiotics (eg, Lactobacillus, Bifidobacterium) in preventing atopic dermatitis or in controlling symptoms in children.[17]A recent meta-analysis indicated that prenatal and postnatal probiotic supplementation may be helpful in preventing the development of atopic dermatitis in young children but does not appear to be effective in treating existing atopic dermatitis.[18]Further studies on the subject are needed prior to developing firm conclusions on the usefulness of this complementary medicinal treatment.
Topical Corticosteroids
In older children and adolescents, treat mild cases of atopic dermatitis with a low-potency (class VI or VII) topical steroid twice a day to decrease inflammation. Examples include hydrocortisone cream or ointment, 1% and 2.5%. For moderate cases of atopic dermatitis, intermediate-potency steroids (class III, IV, V) may be used for brief periods (<2 wk) to control an eczematous flare.

P E D I A T R I C A T O P I C D E R M A T I T I S
20
カイルパン タラ
non-commercial document; school paperwork
Subsequently, low-potency steroids can be used to maintain remission. For severe cases of atopic dermatitis, pulse therapy with high-potency topical steroids (class II) or oral steroids may be beneficial in adolescents. Use only low-potency steroids on the face, axillae, groin, and intertriginous areas because of increased absorption and increased local steroid side effects.
For mild atopic dermatitis in infants, class VI or VII topical steroids should be effective. If the infant has more severe atopic dermatitis, a moderate-potency steroid can be prescribed for as long as 1 week and then tapered down to a lower-potency medication for maintenance therapy. In general, do not treat infants with topical steroids in the high-potency classes (class II or above) without a referral to a dermatologist.
Cordran tape is a corticosteroid-impregnated polyethylene film that enhances topical steroid penetration up to 100-fold. Occlusion of a topical steroid under plastic wrap seems to work equally well. These methods are especially useful for chronic lichenified plaques of atopic dermatitis.
In order to achieve a quick, complete remission of atopic dermatitis symptoms, adequate amounts of topical steroid must be used. Many patients initially use suboptimal amounts of topical steroid products, leading to poor control of their atopic dermatitis symptoms and ultimate discontinuation of their therapy. Approximately 30 grams of medication is needed to cover the entire surface area of an adult body. For children, the fingertip unit (FTU) has been shown to accurately measure an appropriate amount of medication. The FTU is defined as the amount of topical medication that will cover the child's index finger from the tip to the metacarpophalangeal joint. For topical steroids, 1 FTU covers the hand or groin, 2 FTUs cover the face or foot, 3 FTUs cover an arm, 6 FTUs cover a leg, and 14 FTUs cover the trunk.
Atopic dermatitis increases the risk of developing lymphoma (both Hodgkin disease and non-Hodgkin lymphoma). This risk correlates with increasing severity of disease. One study found an even higher risk of lymphoma in patients with atopic dermatitis treated with

P E D I A T R I C A T O P I C D E R M A T I T I S
21
カイルパン タラ
non-commercial document; school paperwork
topical corticosteroids. The risk rose with increasing potency of the topical corticosteroid and with longer duration of use.[19]
Hydrocortisone topical (Cortizone, Dermolate, Westcort)
Adrenocorticosteroid derivative suitable for application to skin or external mucous membranes. It has mineralocorticoid and glucocorticoid effects resulting in anti-inflammatory activity.
Dosing
Adult
1% or 2.5%: Apply sparingly bid to areas of mild eczema, preferably after baths
2.5% or 5%: Apply sparingly bid to areas of moderate eczema
2.5%: Apply sparingly bid to face and intertriginous areas affected by severe eczema
Pediatric
Infants: Apply 0.5% sparingly to affected skin bid in mild-to-moderate eczema; 1% bid in moderate-to-severe eczema
Older children: Apply 1% sparingly to affected skin bid for mild-to-moderate eczema; 2.5% bid in severe eczema
Adolescents: Apply 2.5% or 5% sparingly to affected skin bid for moderate eczema
Interactions: None reported
Contraindications: Documented hypersensitivity; viral, fungal, and bacterial skin infections
Precautions
Pregnancy: C - Fetal risk revealed in studies in animals but not established or not studied in humans; may use if benefits outweigh risk to fetus
Precautions: Prolonged use, applying over large surface areas, application of potent steroids, and occlusive dressings may increase systemic absorption of corticosteroids and cause Cushing syndrome, reversible HPA axis suppression, hyperglycemia, and glycosuria

P E D I A T R I C A T O P I C D E R M A T I T I S
22
カイルパン タラ
non-commercial document; school paperwork
Triamcinolone Topical (Kenalog)
It treats inflammatory dermatosis that is responsive to steroids. It decreases inflammation by suppressing the migration of polymorphonuclear leukocytes and reversing capillary permeability.
Dosing
Adult
0.025%: Apply sparingly to trunk and extremities bid/tid for mild to moderate AD
0.1%: Apply sparingly to trunk and extremities bid/tid for moderate AD
0.5%: Apply sparingly to trunk and extremities bid/tid for severe AD
Pediatric
Infants and young children: Apply 0.025%-0.1% sparingly to trunk and extremities bid/tid for severe AD
Adolescents: Apply 0.025%-0.1% sparingly to trunk and extremities bid/tid for moderate AD.
Apply 0.5% sparingly to trunk and extremities bid/tid for severe AD
Interactions: None reported
Contraindications: Documented hypersensitivity; fungal, viral, and bacterial skin infections
Precautions
Pregnancy: C - Fetal risk revealed in studies in animals but not established or not studied in humans; may use if benefits outweigh risk to fetus
Precautions: Do not use in decreased skin circulation; prolonged use, applications over large areas, and use of potent steroids and occlusive dressings may result in systemic absorption; systemic absorption may cause Cushing syndrome, reversible HPA axis suppression, hyperglycemia, and glycosuria
Flurandrenolide (Cordran Tape)
Intermediate-potency topical corticosteroid. Each square cm provides 4 mcg.

P E D I A T R I C A T O P I C D E R M A T I T I S
23
カイルパン タラ
non-commercial document; school paperwork
Dosing
Adult : Apply to trunk or extremities for 8-12 h qd on successive days for chronic, lichenified patches of AD
Pediatric : Administer as in adults
Interactions: None reported
Contraindications: Documented hypersensitivity; application with plastic wrap in acutely infected areas or in areas with enhanced absorption of topical steroids (eg, face, axillae, groin, intertriginous areas) because of the increased risk of adverse effect
Precautions
Pregnancy: C - Fetal risk revealed in studies in animals but not established or not studied in humans; may use if benefits outweigh risk to fetus
Precautions: Use extreme caution to prevent overuse and consequent development of skin changes, including atrophy, striae, or local infection (eg, miliaria, folliculitis)
Systemic Corticosteroids
Symptoms typically dramatically improve in the first few days of treatment with systemic steroids, only to be followed by an equally dramatic rebound flare after cessation of treatment. Tapering oral steroids over 10-14 days may mitigate this effect. In addition, an intensified focus on hydration with bathing and appropriate use of topical steroids should be emphasized to prevent rebound phenomena after discontinuation of systemic steroids.
Prednisone (Deltasone, Orasone)
Decreases inflammation by reversing increased capillary permeability and suppressing PMN activity.
Dosing
Adult: 1-2 mg/kg/d PO for 7- to 14-d pulse therapy; followed by slow taper
Pediatric: Adolescents with severe refractory eczema: Administer as in adults

P E D I A T R I C A T O P I C D E R M A T I T I S
24
カイルパン タラ
non-commercial document; school paperwork
Interactions: Coadministration with estrogens may decrease prednisone clearance; concurrent use with digoxin may cause digitalis toxicity secondary to hypokalemia; phenobarbital, phenytoin, and rifampin may increase metabolism of glucocorticoids (consider increasing maintenance dose); monitor for hypokalemia with coadministration of diuretics
Contraindications: Documented hypersensitivity; viral infection; peptic ulcer disease; hepatic dysfunction; connective tissue infections; fungal or tubercular skin infections
Precautions
Pregnancy: B - Fetal risk not confirmed in studies in humans but has been shown in some studies in animals
Precautions: Development of striae, atrophy of skin, perioral dermatitis, rosacea, and telangiectasias; abrupt discontinuation of glucocorticoids may cause adrenal crisis; hyperglycemia, edema, osteonecrosis, myopathy, peptic ulcer disease, hypokalemia, osteoporosis, euphoria, psychosis, myasthenia gravis, growth suppression, and infections may occur with glucocorticoid use
Antimicrobials
Antistaphylococcal antibiotics (eg, topical mupirocin or bacitracin, first-generation cephalosporins, macrolides, penicillinase-resistant extended-spectrum penicillins such as oxacillin or dicloxacillin if resistant strains of S aureus are encountered, amoxicillin-clavulanate) are helpful in secondary bacterial infections. Herpes simplex superinfections (eczema herpeticum) should be suspected if vesicles are present or if no improvement is observed with oral antibiotics. Tzanck smear of the base of vesicles is positive in 70% of cases. Treat with oral or intravenous acyclovir for 10 days. Varicella infections may become severe in the setting of atopic dermatitis, and early treatment with acyclovir is recommended. Counsel all children with atopic dermatitis as to the benefits of vaccination against varicella. Treat dermatophyte infections with topical or oral antifungals, such as topical ketoconazole cream or shampoo.
Mupirocin topical cream or ointment (Bactroban)
Inhibits bacterial growth by inhibiting RNA and protein synthesis.

P E D I A T R I C A T O P I C D E R M A T I T I S
25
カイルパン タラ
non-commercial document; school paperwork
Dosing
Adult :Apply a thin film topically to the affected area 2-5 times per d for 5-14 Pediatric : Administer as in adults
Interactions: None reported
Contraindications: Documented hypersensitivity
Precautions
Pregnancy: B - Fetal risk not confirmed in studies in humans but has been shown in some studies in animals
Precautions: Prolonged use may result in the growth of nonsusceptible organisms
Cephalexin (Keflex, Keftab)
First-generation cephalosporin arrests bacterial growth by inhibiting bacterial cell wall synthesis. Bactericidal activity against rapidly growing organisms. Primary activity against skin flora.
Dosing
Adult : 250-500 mg PO qid
Pediatric : 25-100 mg/kg/d PO divided qid
Interactions: Coadministration with aminoglycosides increases nephrotoxic potential
Contraindications: Documented hypersensitivity
Precautions
Pregnancy: B - Fetal risk not confirmed in studies in humans but has been shown in some studies in animals
Precautions: Adjust dose in renal impairment
Erythromycin (E.E.S., Erythrocin) or azithromycin (Zithromax)
Macrolide antibiotics that inhibit bacterial growth, possibly by blocking dissociation of peptidyl tRNA from ribosomes causing RNA-dependent protein synthesis to arrest. For treatment of staphylococcal and streptococcal infections.

P E D I A T R I C A T O P I C D E R M A T I T I S
26
カイルパン タラ
non-commercial document; school paperwork
Dosing
Adult
Erythromycin: 250-500 mg PO qid
Azithromycin: 500 mg PO on day 1, followed by 250 mg PO qd for next 4 d
Pediatric
Erythromycin: 30-50 mg/kg/d PO divided tid/qid
Azithromycin: 10 mg/kg PO on day 1, followed by 5 mg/kg PO qd for next 4 d
Interactions: Coadministration may increase toxicity of theophylline, digoxin, carbamazepine, and cyclosporine; may potentiate anticoagulant effects of warfarin; coadministration with lovastatin and simvastatin increases risk of rhabdomyolysis
Contraindications
Documented hypersensitivity
Precautions
Pregnancy: B - Fetal risk not confirmed in studies in humans but has been shown in some studies in animals
Precautions: Caution in liver disease
Oxacillin or dicloxacillin
Bactericidal antibiotic that inhibits cell wall synthesis. Used in the treatment of infections caused by penicillinase-producing staphylococci. May be used to initiate therapy when a staphylococcal infection is suspected.
Dosing
Adult
Oxacillin: 500-1000 mg PO q4-6h
Dicloxacillin: 125-500 mg PO qid
Pediatric
Oxacillin: 50-100 mg/kg/d PO divided q6h

P E D I A T R I C A T O P I C D E R M A T I T I S
27
カイルパン タラ
non-commercial document; school paperwork
Dicloxacillin: 25-100 mg/kg/d PO divided q6h
Interactions: Decreases efficacy of PO contraceptives; increases effects of anticoagulants; probenecid and disulfiram may increase levels
Contraindications: Documented hypersensitivity
Precautions
Pregnancy: B - Fetal risk not confirmed in studies in humans but has been shown in some studies in animals
Precautions: Caution in impaired renal function
Amoxicillin and clavulanate (Augmentin)
Drug combination treats bacteria resistant to beta-lactam antibiotics. Base dosage regimen on amoxicillin content. Because of different amoxicillin-clavulanic acid ratios in 250-mg tab (250/125) versus 250-mg chewable tab (250/62.5), do not use 250-mg tab until child weighs >40 kg.
Dosing
Adult : 250-500 mg PO tid or 500-875 mg PO bid
Pediatric :20-40 mg/kg/d PO divided tid or 25-45 mg/kg/d PO divided bid
Interactions: Increased risk of amoxicillin rash with concurrent allopurinol; probenecid and disulfiram may increase penicillin levels
Contraindications: Documented hypersensitivity
Precautions
Pregnancy: B - Fetal risk not confirmed in studies in humans but has been shown in some studies in animals
Precautions: Caution in impaired renal function
Acyclovir (Zovirax)
Patients experience less pain and faster resolution of cutaneous lesions when used within 48 h of rash onset. May prevent recurrent outbreaks.

P E D I A T R I C A T O P I C D E R M A T I T I S
28
カイルパン タラ
non-commercial document; school paperwork
Dosing
Adult
Herpes zoster: 800 mg PO 5 times per d for 7-10 d
Varicella-zoster: 800 mg PO qid for 5 d
Pediatric
Mucocutaneous HSV: 25-30 mg/kg/d PO divided q8h for 7-10 d for initial infection or for 5 d for recurrence
Varicella zoster: 80 mg/kg/d PO divided qid for 5 d; not to exceed 3200 mg/d
Interactions: Concomitant use of probenecid or zidovudine prolongs half-life and increases CNS toxicity of acyclovir
Contraindications: Documented hypersensitivity
Precautions
Pregnancy: B - Fetal risk not confirmed in studies in humans but has been shown in some studies in animals
Precautions: Caution in renal failure or when using nephrotoxic drugs
Ketoconazole (Nizoral)
Imidazole broad-spectrum antifungal agent. Inhibits synthesis of ergosterol, causing cellular components to leak, resulting in fungal cell death.
Dosing
Adult
Tinea: Apply 2% cream to affected skin bid
Scalp involvement: Use 2% shampoo twice a week
Pediatric: Administer as in adults
Interactions: None reported
Contraindications: Documented hypersensitivity

P E D I A T R I C A T O P I C D E R M A T I T I S
29
カイルパン タラ
non-commercial document; school paperwork
Precautions
Pregnancy: C - Fetal risk revealed in studies in animals but not established or not studied in humans; may use if benefits outweigh risk to fetus
Precautions: If sensitivity or irritation develops, discontinue use; for external use only; avoid contact with eyes
Antipruritics
Topical local anesthetics or antihistamines (topical or systemic) may be used to decrease pruritus.
Pramoxine (Prax, PrameGel) or doxepin topical cream (Zonalon)
Pramoxine elicits anesthetic effect by blocking nerve conduction and impulses by inhibiting depolarization of neurons. Doxepin topical cream is a potent antihistamine and is indicated for pruritus.
Dosing
Adult
Pramoxine: Apply to affected skin tid/qid prn for pruritus
Doxepin: Apply 5% cream to affected skin qid
Pediatric
Pramoxine: Apply to affected skin tid/qid prn for pruritus
Doxepin: Not recommended
Interactions: None reported
Contraindications: Documented hypersensitivity
Precautions
Pregnancy: C - Fetal risk revealed in studies in animals but not established or not studied in humans; may use if benefits outweigh risk to fetus
Precautions: Pramoxine: Caution in patients with trauma in area to be treated; Doxepin: >20% of patients experience drowsiness if applied to >10% of body surface area

P E D I A T R I C A T O P I C D E R M A T I T I S
30
カイルパン タラ
non-commercial document; school paperwork
Diphenhydramine (Benadryl), hydroxyzine (Vistaril), or doxepin (Sinequan)
For symptomatic relief of symptoms caused by release of histamine in allergic reactions.
Dosing
Adult
Diphenhydramine: 25-50 mg PO qhs or q6h
Hydroxyzine: 25-50 mg PO qhs or q4-6h
Doxepin: 25-75 mg PO qhs
Pediatric
Diphenhydramine: 5 mg/kg/d PO divided q6h
Hydroxyzine: 2 mg/kg/d PO divided q6-8h
Doxepin: Not recommended
Interactions: CNS depression may increase with alcohol or other CNS depressants
Contraindications: Documented hypersensitivity
Precautions
Pregnancy: C - Fetal risk revealed in studies in animals but not established or not studied in humans; may use if benefits outweigh risk to fetus
Precautions: Caution in cardiovascular disease, conduction disturbances, seizure disorders, urinary retention, hyperthyroidism, and thyroid replacement therapy
Immunomodulators
Topical tacrolimus ointment and pimecrolimus cream have both been shown to diminish pruritus and inflammation markedly within 3 days of initiating therapy and to have persistent effects for as long as 12 months. Several studies have documented the rapid and prolonged improvement in clinical severity scores in children and adults with a range of severity of atopic dermatitis. Research has shown the beneficial effect of topical calcineurin inhibitors in patients refractory

P E D I A T R I C A T O P I C D E R M A T I T I S
31
カイルパン タラ
non-commercial document; school paperwork
to topical corticosteroid therapy.[20,21]The most common adverse effect is a local burning sensation upon application, but this symptom tends to diminish after the first few days of use.
In January 2006, the Food and Drug Administration (FDA) approved a black box warning for tacrolimus and pimecrolimus topical medications. The warning emphasized the lack of long-term safety data and a possible link to malignancies. No causal link between these agents and the development of malignancies has been established. Long-term studies on the safety of these agents in humans are not yet available, and the black box warning was based on case reports in humans and on animal studies. An analysis of tacrolimus ointment use in patients with atopic dermatitis over 4 years did not show any increased risk of infections or cancer.[22]However, longer term studies (10 y of follow-up or longer) are needed before firm conclusions about these concerns can be reached. Establishing the long-term safety profile of topical calcineurin inhibitors is of paramount importance because they appear to provide an effective alternative to topical corticosteroid treatment in certain patients. Furthermore, pimecrolimus has been shown to improve the epidermal skin barrier without the concurrent risk of local skin atrophy commonly seen with topical corticosteroid treatment.[23]Thus, pimecrolimus appears to be an attractive candidate for long-term use in either a therapeutic or preventative capacity.
At the present time, physicians are advised to use the following guidelines when prescribing topical immunomodulators such as tacrolimus and pimecrolimus:[24,25] Use in patients older than 2 years. Use intermittently as needed, not on a daily basis for prolonged
periods (ie, >6 weeks). Avoid use in immunocompromised patients or in those with
neoplasms. Atypical atopic dermatitis, including new onset disease in an adult,
should warrant a skin biopsy prior to topical immunomodulator

P E D I A T R I C A T O P I C D E R M A T I T I S
32
カイルパン タラ
non-commercial document; school paperwork
use, to rule out other diagnoses (eg, cutaneous T-cell lymphoma, Netherton syndrome).
Encourage sun protection to reduce the risk of photocarcinogenesis.
Oral cyclosporine has proven beneficial in patients with severe atopic dermatitis refractory to treatment with topical steroids. Discontinuation of cyclosporine frequently results in rapid relapse of skin disease. Significant adverse effects (eg, nausea, abdominal discomfort, hypertrichosis, paresthesias, hypertension, hyperbilirubinemia, renal impairment) have diminished enthusiasm for this drug, especially with the advent of the topical immunomodulators mentioned above.
A small, nonrandomized, nonblinded study of 6 patients with severe atopic dermatitis showed significant improvement in skin symptoms within the first 4-8 weeks of treatment with Rituximab.[16]Larger, randomized controlled studies are needed to verify this finding.
Tacrolimus, topical (Protopic)
The mechanism of action of tacrolimus in atopic dermatitis is not known. This agent reduces itching and inflammation by suppressing the release of cytokines from T cells. It also inhibits transcription for genes that encode IL-3, IL-4, IL-5, GM-CSF, and TNF-α, all of which are involved in the early stages of T-cell activation. Additionally, this agent may inhibit the release of preformed mediators from skin mast cells and basophils, and it may downregulate the expression of FCeRI on Langerhans cells. Used for the short-term or intermittent long-term treatment of moderate-to-severe atopic dermatitis that is unresponsive to first-line therapies (eg, topical corticosteroids) or in cases where first-line therapies are not applicable. The manufacturer and FDA recommend that the smallest amount and lowest potency that is efficacious be used to achieve control of symptoms. It is available as an ointment in concentrations of 0.03% and 0.1%.
Dosing
Adult
Apply 0.03% or 0.1% to affected skin bid
For short-term and intermittent use only

P E D I A T R I C A T O P I C D E R M A T I T I S
33
カイルパン タラ
non-commercial document; school paperwork
Pediatric
<2 years: Not established
2-15 years: Apply 0.03% to affected skin bid
>15 years: Administer as in adults
For short-term and intermittent use only
Interactions: None reported
Contraindications: Documented hypersensitivity
Precautions
Pregnancy: C - Fetal risk revealed in studies in animals but not established or not studied in humans; may use if benefits outweigh risk to fetus
Precautions
Patients may experience a burning sensation during first few days of application; skin can become photosensitive, caution patients about exposure to direct or artificial sunlight and encourage use of sunscreen; safety and efficacy in infected AD is not known; application under occlusion, which may promote systemic exposure, has not been evaluated (do not use tacrolimus ointment with occlusive dressings); absorption of tacrolimus following topical applications of tacrolimus ointment is minimal (relative to systemic administration), but tacrolimus is excreted in human milk and, thus, a decision should be made whether to discontinue breastfeeding or to discontinue drug, taking into account importance of drug to mother (potential for serious adverse reactions in breastfeeding infants from tacrolimus should also be a concern). The FDA issued a public health advisory in 2004 based on reports of a possible link between use of the topical calcineurin inhibitors and malignancies; this concern is based on information from animal studies, case reports in a small number of patients, and knowledge of how drugs in this class work; human studies of 10 years or longer may be needed to determine if Protopic is linked to cancer; in the meantime, this risk is uncertain, and the FDA advises that Protopic should be used only as labeled and only after other prescription treatments have failed to work or cannot be tolerated

P E D I A T R I C A T O P I C D E R M A T I T I S
34
カイルパン タラ
non-commercial document; school paperwork
Pimecrolimus (Elidel cream)
First nonsteroid cream approved in the US for mild-to-moderate atopic dermatitis. Derived from ascomycin, a natural substance produced by fungus Streptomyces hygroscopicus var. ascomyceticus. This agent selectively inhibits production and release of inflammatory cytokines from activated T cells by binding to cytosolic immunophilin receptor macrophilin-12. The resulting complex inhibits phosphatase calcineurin, thus blocking T-cell activation and cytokine release. Cutaneous atrophy was not observed in clinical trials, a potential advantage over topical corticosteroids. This agent is indicated only after other treatment options have failed. Available as a 1% cream.
Dosing
Adult
Apply topically to affected areas bid
Short-term and intermittent use only
Pediatric
<2 years: Not established
≥ 2 years: Administer as in adults
Short-term and intermittent use only
Interactions: None reported
Contraindications: Documented hypersensitivity
Precautions
Pregnancy: C - Fetal risk revealed in studies in animals but not established or not studied in humans; may use if benefits outweigh risk to fetus
Precautions
Potential exacerbation of existing infection at site of application; may cause burning and irritation; caution with conditions that suppress the immune system (eg, AIDS, cancer); possible risk of lymph node or skin cancer based on animal studies and a small number of patients; may increase risk of viral infections; other adverse effects include headache, sore throat, flulike symptoms, fever, and cough. The FDA issued a public health advisory in 2004 based on reports of a possible link between use of the topical calcineurin inhibitors and malignancies, this

P E D I A T R I C A T O P I C D E R M A T I T I S
35
カイルパン タラ
non-commercial document; school paperwork
concern is based on information from animal studies, case reports in a small number of patients, and knowledge of how drugs in this class work; human studies of 10 years or longer may be necessary to determine if use of Elidel is linked to cancer; in the meantime, this risk is uncertain, and the FDA advises Elidel should be used only as labeled after other prescription treatments have failed to work or cannot be tolerated
Cyclosporine (Sandimmune, Neoral)
Cyclic polypeptide that suppresses some humoral immunity and, to a greater extent, cell-mediated immune reactions.
Dosing
Adult : 5 mg/kg/d PO qd
Pediatric : Not established
Interactions: Carbamazepine, phenytoin, isoniazid, rifampin, and phenobarbital may decrease cyclosporine concentrations; azithromycin, itraconazole, nicardipine, ketoconazole, fluconazole, erythromycin, verapamil, grapefruit juice, diltiazem, aminoglycosides, acyclovir, amphotericin B, and clarithromycin may increase cyclosporine toxicity; acute renal failure, rhabdomyolysis, myositis, and myalgias increase when taken concurrently with lovastatin
Contraindications: Documented hypersensitivity; uncontrolled hypertension or malignancies; concomitant administration with PUVA or UVB radiation in psoriasis (may increase risk of cancer)
Precautions
Pregnancy: C - Fetal risk revealed in studies in animals but not established or not studied in humans; may use if benefits outweigh risk to fetus
Precautions: Evaluate renal and liver functions often by measuring BUN, serum creatinine, serum bilirubin, and liver enzymes; may increase risk of infection and lymphoma; reserve IV use only for those who cannot take PO

P E D I A T R I C A T O P I C D E R M A T I T I S
36
カイルパン タラ
non-commercial document; school paperwork
Follow-up
Further Outpatient Care
Frequent follow-up is needed early in the course of atopic dermatitis (AD) to ensure compliance and assess patient responsiveness to therapy. Analyze treatment failures for the presence of resistant organisms, contact dermatitis to a medication (eg, preservatives in steroid preparations, bacitracin), or parental noncompliance.
Deterrence/Prevention
Prevention of acute flares and the subsequent development of chronic lesions of atopic dermatitis are indicators of successful treatment for this disease. Maintenance of adequate hydration of the stratum corneum, avoidance of known or probable allergens and irritants, rapid self-treatment with the proper class of topical steroids, and judicious use of complementary therapies (eg, antipruritics, stress relievers, antibiotics) are the cornerstones of ensuring a high quality of life unimpeded by the more severe aspects of this disease.
Nonspecific triggers of inflammation in patients with atopic dermatitis may include physical or chemical irritants. The following simple measures should be followed in daily life to reduce the frequency and severity of irritant-induced atopic dermatitis flares:[26]
o Skin care products that contain alcohol and astringents should be avoided.
o New clothes should be laundered before use to remove formaldehyde and other chemicals.
o Liquid detergents are preferred over powder detergents for laundering clothes, as liquids are easier to rinse out. A second rinse cycle may also improve removal of residual detergent.
o Patients should shower immediately after swimming in chlorinated pools and should subsequently apply moisturizer.
o Fragrance-free skin products that are hypoallergenic or made for "sensitive skin" may be less irritating than other kinds of skin products.

P E D I A T R I C A T O P I C D E R M A T I T I S
37
カイルパン タラ
non-commercial document; school paperwork
Prenatal and postnatal probiotic supplementation may be helpful in preventing the development of atopic dermatitis in young children. In a recent meta-analysis, the most commonly studied probiotic was Lactobacillus rhamnosus GG.[18]Larger, randomized controlled studies are needed to confirm these initial findings.
A dog living in the home at the time of birth has also been associated with a 50% decrease in the incidence of atopic dermatitis at age 3 years.[7]
Complications
The most common complication of atopic dermatitis is secondary infection.
Staphylococcus species and group A beta-hemolytic streptococci are the most frequent organisms cultured from skin lesions. Superinfected eczematoid lesions appear as erythema associated with serous or purulent exudates and crusting. Greasy moist scales on the surface of the lesions and small pustules at the advancing edges may be present. Always consider infection in acute flares of chronic atopic dermatitis or in cases that are unresponsive to appropriate therapy.
Topical antibiotic therapy is useful for localized infections; however, systemic treatment is preferred for recurrent or widespread infections. The agent of choice is penicillin G if group A streptococci is the known infectious organism. Use erythromycin or a semisynthetic penicillin (eg, nafcillin, oxacillin, dicloxacillin) if S aureus is a possible cause. Hospitalization and use of intravenous antibiotics are indicated in cases of invasive infection (eg, osteomyelitis). Perform urinalysis and closely observe patients for symptoms for at least 7 weeks after treatment in endemic areas because systemic antibiotic treatment does not prevent postinfectious glomerulonephritis after a cutaneous infection with nephritogenic M strains of streptococci.
Less commonly, patients with atopic dermatitis may develop an explosive vesicular eruption known as Kaposi varicelliform eruption or eczema herpeticum. Vesicles and pustules are

P E D I A T R I C A T O P I C D E R M A T I T I S
38
カイルパン タラ
non-commercial document; school paperwork
typically umbilicated and are initially confined to eczematous skin but may later spread to normal skin. Later in the course of the disease, erosions may be commonplace and confluent, resulting in denuded areas. Tzanck smear of vesicles or a viral culture confirms the diagnosis. Treatment is with acyclovir (if mild, administer 25-30 mg/kg/d, up to 200 mg 5 times per day orally; if severe, administer 5 mg/kg/dose every 8 h or 1.5 g/m2/d intravenously).
Atopic dermatitis nearly doubles an individual's risk of developing lymphoma. This risk increases with usage of potent topical steroids, especially for prolonged time periods.[19]
Prognosis Atopic dermatitis persists into adulthood in 20-40% of children
with the condition. Many children outgrow severe atopic dermatitis and only experience itchy or inflamed skin if exposed to exogenous irritants as adults.
REFERENCES 1. Ong PY, Leung DY. Immune dysregulation in atopic dermatitis. Curr Allergy Asthma
Rep. Sep 2006;6(5):384-9. [Medline]. 2. Oranje AP, Devillers AC, Kunz B, et al. Treatment of patients with atopic dermatitis using wet-
wrap dressings with diluted steroids and/or emollients. An expert panel's opinion and review of the literature. J Eur Acad Dermatol Venereol. Nov 2006;20(10):1277-86. [Medline].
3. Williams H, Stewart A, von Mutius E, Cookson W, Anderson HR,. Is eczema really on the increase worldwide?. J Allergy Clin Immunol. Apr 2008;121(4):947-54.e15. [Medline].
4. Ong PY, Boguniewicz M. Atopic dermatitis. Prim Care. Mar 2008;35(1):105-17, vii. [Medline]. 5. [Best Evidence] Kvenshagen B, Jacobsen M, Halvorsen R. Atopic dermatitis in premature and
term children. Arch Dis Child. Mar 2009;94(3):202-5. [Medline]. 6. Hanifin JM, Rajka G. Diagnostic features of atopic dermatitis. Acta Derm Venreol. 1980;92:44-
7. 7. Bisgaard H, Halkjaer LB, Hinge R, et al. Risk analysis of early childhood eczema. J Allergy Clin
Immunol. Jun 2009;123(6):1355-60.e5. [Medline]. 8. Leung DY. Our evolving understanding of the functional role of filaggrin in atopic dermatitis. J
Allergy Clin Immunol. Sep 2009;124(3):494-5. [Medline]. 9. Gao PS, Rafaels NM, Hand T, et al. Filaggrin mutations that confer risk of atopic dermatitis
confer greater risk for eczema herpeticum. J Allergy Clin Immunol. Sep 2009;124(3):507-13, 513.e1-7. [Medline].
10. Kumar R, Ouyang F, Story RE, et al. Gestational diabetes, atopic dermatitis, and allergen sensitization in early childhood. J Allergy Clin Immunol. Nov 2009;124(5):1031-8.e1-4. [Medline].
11. Chamlin SL, Kao J, Frieden IJ, et al. Ceramide-dominant barrier repair lipids alleviate childhood atopic dermatitis: changes in barrier function provide a sensitive indicator of disease activity. J Am Acad Dermatol. Aug 2002;47(2):198-208. [Medline].
12. Novak N. Allergen specific immunotherapy for atopic dermatitis. Curr Opin Allergy Clin Immunol. Dec 2007;7(6):542-46. [Medline].

P E D I A T R I C A T O P I C D E R M A T I T I S
39
カイルパン タラ
non-commercial document; school paperwork
13. [Guideline] Greer FR, Sicherer SH, Burks AW. Effects of early nutritional interventions on the development of atopic disease in infants and children: the role of maternal dietary restriction, breastfeeding, timing of introduction of complementary foods, and hydrolyzed formulas. Pediatrics. Jan 2008;121(1):183-91. [Medline].
14. Yang YW, Tsai CL, Lu CY. Exclusive breastfeeding and incident atopic dermatitis in childhood: a systematic review and meta-analysis of prospective cohort studies. Br J Dermatol. Aug 2009;161(2):373-83. [Medline].
15. Miyake Y, Tanaka K, Sasaki S, et al. Breastfeeding and atopic eczema in Japanese infants: The Osaka Maternal and Child Health Study. Pediatric Allergy & Immunology. May 2009;20:234-241. [Medline].
16. Simon D, Hosli S, Kostylina G, Yawalkar N, Simon HU. Anti-CD20 (rituximab) treatment improves atopic eczema. J Allergy Clin Immunol. Jan 2008;121(1):122-8. [Medline].
17. Bukutu C, Deol J, Shamseer L, Vohra S. Complementary, holistic, and integrative medicine: atopic dermatitis. Pediatr Rev. Dec 2007;28(12):e87-94. [Medline].
18. Lee J, Seto D, Bielory L. Meta-analysis of clinical trials of probiotics for prevention and treatment of pediatric atopic dermatitis. J Allergy Clin Immunol. Jan 2008;121(1):116-121.e11. [Medline].
19. Arellano FM, Arana A, Wentworth CE, et al. Lymphoma among patients with atopic dermatitis and/or treated with topical immunosuppressants in the United Kingdom. J Allergy Clin Immunol. May 2009;123(5):1111-6, 116.e1-13. [Medline].
20. Leung DY, Hanifin JM, Pariser DM, et al. Effects of pimecrolimus cream 1% in the treatment of patients with atopic dermatitis who demonstrate a clinical insensitivity to topical corticosteroids: a randomized, multicentre vehicle-controlled trial. Br J Dermatol. Aug 2009;161(2):435-43. [Medline].
21. Doss N, Reitamo S, Dubertret L, et al. Superiority of tacrolimus 0.1% ointment compared with fluticasone 0.005% in adults with moderate to severe atopic dermatitis of the face: results from a randomized, double-blind trial. Br J Dermatol. Aug 2009;161(2):427-34. [Medline].
22. Remitz A, Reitamo S. Long-term safety of tacrolimus ointment in atopic dermatitis. Expert Opin Drug Saf. Jul 2009;8(4):501-6. [Medline].
23. Jensen JM, Pfeiffer S, Witt M, et al. Different effects of pimecrolimus and betamethasone on the skin barrier in patients with atopic dermatitis. J Allergy Clin Immunol. May 2009;123(5):1124-33. [Medline].
24. [Guideline] Patel TS, Greer SC, Skinner RB Jr. Cancer concerns with topical immunomodulators in atopic dermatitis: overview of data and recommendations to clinicians. Am J Clin Dermatol. 2007;8(4):189-94. [Medline].
25. Ring J, Mohrenschlager M, Henkel V. The US FDA 'black box' warning for topical calcineurin inhibitors: an ongoing controversy. Drug Saf. 2008;31(3):185-98. [Medline].
26. Boguniewicz M. Topical treatment of atopic dermatitis. Immunol Allergy Clin North Am. Nov 2004;24(4):631-44, vi-vii. [Medline].
27. Beltrani VS. Atopic dermatitis: An update. J Allergy Clin Immunol. Sep 1999;104(3 Pt 2):S85-6. [Medline].
28. Boguniewicz M. Advances in the understanding and treatment of atopic dermatitis. Curr Opin Pediatr. Dec 1997;9(6):577-81. [Medline].
29. Boguniewicz M. Topical treatment of atopic dermatitis. Immunol Allergy Clin North Am. Nov 2004;4:631-44. [Medline].
30. Drake L, Prendergast M, Maher R, et al. The impact of tacrolimus ointment on health-related quality of life of adult and pediatric patients with atopic dermatitis. J Am Acad Dermatol. Jan 2001;44(1 Suppl):S65-72. [Medline].
31. [Guideline] Drake LA, Ceilley RI, Cornelison RL, et al. Guidelines of care for nevi I (nevocellular nevi and seborrheic keratoses). Committee on Guidelines of Care. Task Force on Nevocellular Nevi. J Am Acad Dermatol. Apr 1992;26(4):629-31. [Medline].
32. Eichenfield LF, Lucky AW, Boguniewicz M. Safety and efficacy of pimecrolimus (ASM 981) cream 1% in the treatment of mild and moderate atopic dermatitis in children and adolescents. J Am Acad Dermatol. Apr 2002;46(4):495-504. [Medline].

P E D I A T R I C A T O P I C D E R M A T I T I S
40
カイルパン タラ
non-commercial document; school paperwork
33. Gdalevich M, Mimouni D, David M, Mimouni M. Breast-feeding and the onset of atopic dermatitis in childhood: a systematic review and meta-analysis of prospective studies. J Am Acad Dermatol. Oct 2001;45(4):520-527. [Medline].
34. Grundmann-Kollmann M, Kaufmann R, Zollner TM. Treatment of atopic dermatitis with mycophenolate mofetil. Br J Dermatol. Aug 2001;145(2):351-2. [Medline].
35. Gutman ab, Kligman am, Sciacca j, James WD. Soak and smear: A standard technique revisited. Arch Dermatol. 2005;141:1556-9. [Medline].
36. Halbert AR, Weston WL, Morelli JG. Atopic dermatitis: is it an allergic disease?. J Am Acad Dermatol. Dec 1995;33(6):1008-18. [Medline].
37. Hamzavi I, Lui H. Using light in dermatology: an update on lasers, ultraviolet phototherapy, and photodynamic therapy. Dermatol Clin. Apr 2005;23(2):199-207. [Medline].
38. Hanifin JM, Tofte SJ. Update on therapy of atopic dermatitis. J Allergy Clin Immunol. Sep 1999;104(3 Pt 2):S123-5. [Medline].
39. Ho VC, Gupta A, Kaufmann R, et al. Safety and efficacy of nonsteroid pimecrolimus cream 1% in the treatment of atopic dermatitis in infants. J Pediatr. Feb 2003;142(2):155-62. [Medline].
40. Hurwitz S. Eczematous eruptions in childhood. In: Clinical Pediatric Dermatology: A Textbook of Skin Disorders of Childhood and Adolescence. 2nd ed. Philadelphia, PA: WB Saunders Co; 1993:45-60.
41. Kang S, Lucky AW, Pariser D, et al. Long-term safety and efficacy of tacrolimus ointment for the treatment of atopic dermatitis in children. J Am Acad Dermatol. Jan 2001;44(1 Suppl):S58-64. [Medline].
42. Knoell KA, Greer KE. Atopic dermatitis. Pediatr Rev. Feb 1999;20(2):46-51; quiz 52. [Medline]. 43. Krutmann J, Diepgen TL, Luger TA, et al. High-dose UVA1 therapy for atopic dermatitis:
results of a multicenter trial. J Am Acad Dermatol. Apr 1998;38(4):589-93. [Medline]. 44. Leung DY, Nicklas RA, Li JT, et al. Disease management of atopic dermatitis: an updated
practice parameter. Joint Task Force on Practice Parameters. Ann Allergy Asthma Immunol. Sep 2004;93(3 Suppl 2):S1-21. [Medline].
45. Rasmussen JE. Advances in nondietary management of children with atopic dermatitis. Pediatr Dermatol. Sep 1989;6(3):210-5. [Medline].
46. Reynolds NJ, Franklin V, Gray JC, et al. Narrow-band ultraviolet B and broad-band ultraviolet A phototherapy in adult atopic eczema: a randomised controlled trial. Lancet. Jun 23 2001;357(9273):2012-6. [Medline].
47. Rosenfeldt V, Benfeldt E, Nielsen SD, et al. Effect of probiotic Lactobacillus strains in children with atopic dermatitis. J Allergy Clin Immunol. Feb 2003;111(2):389-95. [Medline].
48. Rudikoff D, Lebwohl M. Atopic dermatitis. Lancet. Jun 6 1998;351(9117):1715-21. [Medline]. 49. Ruzicka T, Bieber T, Schopf E, et al. A short-term trial of tacrolimus ointment for atopic
dermatitis. European Tacrolimus Multicenter Atopic Dermatitis Study Group. N Engl J Med. Sep 18 1997;337(12):816-21. [Medline].
50. Sherertz EF. Atopic Dermatitis: Pathogenesis and Treatment. Medscape from WebMD. Available at http://www.medscape.com/viewarticle/427351. Accessed November 14, 2008.
51. Uehara M, Sugiura H, Sakurai K. A trial of oolong tea in the management of recalcitrant atopic dermatitis. Arch Dermatol. Jan 2001;137(1):42-3. [Medline].
52. Wahn U, Bos JD, Goodfield M, et al. Efficacy and safety of pimecrolimus cream in the long-term management of atopic dermatitis in children. Pediatrics. Jul 2002;110(1 Pt 1):e2. [Medline].

P E D I A T R I C A T O P I C D E R M A T I T I S
41
カイルパン タラ
non-commercial document; school paperwork
DERMATITIS ATOPIK PADA ANAK Provided by: CHILDREN ALLERGY CENTER. Yudhasmara Foundation
Clinical and Editor in Chief : Dr Widodo Judarwanto SpA, Pediatrician Last Updated: May 17, 2009
http://childrenallergyclinic.wordpress.com/2009/05/17/dermatitis-atopik/
Dermatitis atopik (DA) adalah penyakit kulit reaksi inflamasi yang didasari oleh faktor herediter dan faktor lingkungan, bersifat kronik residif dengan gejala eritema, papula, vesikel, kusta, skuama dan pruritus yang hebat. Bila residif biasanya disertai infeksi, atau alergi, faktor psikologik, dan sebagainya.
Dermatitis atopik atau eksema adalah peradangan kronik kulit yang kering dan gatal yang umumnya dimulai pada awal masa kanak-kanak. Eksema dapat menyebabkan gatal yang tidak tertahankan, peradangan, dan gangguan tidur. Penyakit ini dialami sekitar 10-20% anak. Umumnya episode pertama terjadi sebelum usia 12 bulan dan episode-episode selanjutnya akan hilang timbul hingga anak melewati masa tertentu. Sebagian besar anak akan sembuh dari eksema sebelum usia 5 tahun. Sebagian kecil anak akan terus mengalami eksema hingga dewasa.
Penyakit ini dinamakan dermatitis atopik oleh karena kebanyakan penderitanya memberikan reaksi kulit yang didasari oleh IgE dan mempunyai kecenderungan untuk menderita asma, rinitis atau keduanya di kemudian hari yang dikenal sebagai allergic march.

P E D I A T R I C A T O P I C D E R M A T I T I S
42
カイルパン タラ
non-commercial document; school paperwork
Walaupun demikian, istilah dermatitis atopik tidak selalu memberikan arti bahwa penyakit ini didasari oleh interaksi antigen dengan antibodi. Nama lain untuk dermatitis atopik adalah eksema atopik, eksema dermatitis, prurigo Besnier, dan neurodermatitis.
Diperkirakan angka kejadian di masyarakat adalah sekitar 1-3% dan pada anak < 5 tahun sebesar 3,1% dan prevalensi DA pada anak meningkat 5-10% pada 20-30 tahun terakhir.
Sangat mungkin peningkatan prevalensi ini berasal dari faktor lingkungan, seperti bahan kimia industri, makanan olahan, atau benda asing lainnya. Ada dugaan bahwa peningkatan ini juga disebabkan perbaikan prosedur diagnosis dan pengumpulan data.
PATOGENESIS
Sampai saat ini etiologi maupun mekanisme yang pasti DA belum semuanya diketahui, demikian pula pruritus pada DA. Tanpa pruritus diagnosis DA tidak dapat ditegakkan. Rasa gatal dan rasa nyeri sama-sama memiliki reseptor di taut dermoepidermal, yang disalurkan lewat saraf C tidak bermielin ke saraf spinal sensorik yang selanjutnya diteruskan ke talamus kontralateral dan korteks untuk diartikan. Rangsangan yang ringan, superfisial dengan intensitas rendah menyebabkan rasa gatal, sedangkan yang dalam dan berintensitas tinggi menyebabkan rasa nyeri. Sebagian patogenesis DA dapat dijelaskan secara imunologik dan nonimunologik.
Multifaktor DA mempunyai penyebab multi faktorial antara lain faktor genetik, emosi, trauma, keringat, imunologik
Respon Imun Sistemik Terdapat IFN-g yang menurun. Interleukin spesifik alergen yang diproduksi sel T pada darah

P E D I A T R I C A T O P I C D E R M A T I T I S
43
カイルパン タラ
non-commercial document; school paperwork
perifer (interleukin IL-4, IL-5 dan IL-13) meningkat. Juga terjadi Eosinophilia dan peningkatan IgE.
Imunopatologi Kulit Pada DA, sel T yang infiltrasi ke kulit adalah CD45RO+. Sel T ini menggunakan CLA maupun reseptor lainnya untuk mengenali dan menyeberangi endotelium pembuluh darah. Di pembuluh darah perifer pasien DA, sel T subset CD4+ maupun subset CD8+ dari sel T dengan petanda CLA+CD45RO+ dalam status teraktivasi (CD25+, CD40L+, HLADR+). Sel yang teraktivasi ini mengekspresikan Fas dan Fas ligand yang menjadi penyebab apoptosis. Sel-sel itu sendiri tidak menunjukkan apoptosis karena mereka diproteksi oleh sitokin dan protein extracellular matrix (ECM). Sel-sel T tersebut mensekresi IFN g yang melakukan upregulation Fas pada keratinocytes dan menjadikannya peka terhadap proses apoptosis di kulit. Apoptosis keratinocyte diinduksi oleh Fas ligand yang diekspresi di permukaan sel-sel T atau yang berada di microenvironment
Respon imun kulit Sel-sel T baik subset CD4+ maupun subset CD8+ yang diisolasi dari kulit (CLA+ CD45RO+ T cells) maupun dari darah perifer, terbukti mensekresi sejumlah besar IL-5 dan IL-13, sehingga dengan kondisi ini lifespan dari eosinofil memanjang dan terjadi induksi pada produksi IgE. Lesi akut didominasi oleh ekspresi IL-4 dan IL-13, sedangkan lesi kronik didominasi oleh ekspresi IL-5, GM-CSF, IL-12, dan IFN-g serta infiltrasi makrofag dan eosinofil.
Genetik Pengaruh gen maternal sangat kuat. Ada peran kromosom 5q31-33, kromosom 3q21, serta kromosom 1q21 and 17q25. Juga melibatkan gen yang independen dari mekanisme alergi. Ada peningkatan prevalensi HLA-A3 dan HLA-A9. Pada umumnya berjalan bersama penyakit atopi lainnya, seperti asma dan rhinitis. Resiko seorang kembar monosigotik yang saudara kembarnya menderita DA adalah 86%.

P E D I A T R I C A T O P I C D E R M A T I T I S
44
カイルパン タラ
non-commercial document; school paperwork
Reaksi Imunologis DA
Sekitar 70% anak dengan DA mempunyai riwayat atopi dalam keluarganya seperti asma bronkial, rinitis alergi, atau dermatitis atopik. Sebagian besar anak dengan DA (sekitar 80%), terdapat peningkatan kadar IgE total dan eosinofil di dalam darah. Anak dengan DA terutama yang moderat dan berat akan berlanjut dengan asma dan/atau rinitis alergika di kemudian hari (allergic march), dan semuanya ini memberikan dugaan bahwa dasar DA adalah suatu penyakit atopi.
Ekspresi sitokin
Keseimbangan sitokin yang berasal dari Th1 dan Th2 sangat berperan pada reaksi inflamasi penderita Dermatitis Atopik (DA). Pada lesi yang akut ditandai dengan kadar Il-4, Il-5, dan Il-13 yang tinggi sedangkan pada DA yang kronis disertai kadar Il-4 dan Il-13 yang lebih rendah, tetapi kadar Il-5, GM-CSF (granulocyte-macrophage colony-stimulating factor), Il-12 dan INFg lebih tinggi dibandingkan pada DA akut.
Anak dengan bawaan atopi lebih mudah bereaksi terhadap antigen lingkungan (makanan dan inhalan), dan menimbulkan sensitisasi terhadap reaksi hipersentivitas tipe I. Imunitas seluler dan respons terhadap reaksi hipersensitivitas tipe lambat akan menurun pada 80% penderita dengan DA, akibat menurunnya jumlah limfosit T

P E D I A T R I C A T O P I C D E R M A T I T I S
45
カイルパン タラ
non-commercial document; school paperwork
sitolitik (CD8+), sehingga rasio limfosit T sitolitik (CD 8+) terhadap limfosit T helper (CD4+) menurun dengan akibat kepekaan terhadap infeksi virus, bakteri, dan jamur meningkat.
Di antara mediator yang dilepaskan oleh sel mast, yang berperan pada pruritus adalah vasoaktif amin, seperti histamin, kinin, bradikinin, leukotrien, prostaglandin dan sebagainya, sehingga dapat dipahami bahwa dalam penatalaksanaan DA, walaupun antihistamin sering digunakan, namun hasilnya tidak terlalu menggembirakan dan sampai saat ini masih banyak silang pendapat para ahli mengenai manfaat antihistamin pada DA.
Trauma mekanik (garukan) akan melepaskan TNF-a dan sitokin pro inflammatory lainnya di epidermis, yang selanjutnya akan meningkatkan kronisitas DA dan bertambah beratnya eksema.
Antigen Presenting Cells
Kulit penderita DA mengandung sel Langerhans (LC) yang mempunyai afinitas tinggi untuk mengikat antigen asing (Ag) dan IgE lewat reseptor FceRI pada permukaannya, dan beperan untuk mempresentasikan alergen ke limfosit Th2, mengaktifkan sel memori Th2 di kulit dan yang juga berperan mengaktifkan Th0 menjadi Th2 di dalam sirkulasi.
Faktor Non-Imunologis
Faktor non imunologis yang menyebabkan rasa gatal pada DA antara lain adanya faktor genetik, yaitu kulit DA yang kering (xerosis). Kekeringan kulit diperberat oleh udara yang lembab dan panas, banyak berkeringat, dan bahan detergen yang berasal dari sabun. Kulit yang kering akan menyebabkan nilai ambang rasa gatal menurun, sehingga dengan rangsangan yang ringan seperti iritasi wol, rangsangan mekanik, dan termal akan mengakibatkan rasa gatal.

P E D I A T R I C A T O P I C D E R M A T I T I S
46
カイルパン タラ
non-commercial document; school paperwork
FAKTOR-FAKTOR PENCETUS
Makanan
Berdasarkan hasil Double Blind Placebo Controlled Food Challenge (DBPCFC), hampir 40% bayi dan anak dengan DA sedang dan berat mempunyai riwayat alergi terhadap makanan. Bayi dan anak dengan alergi makanan umumnya disertai uji kulit (skin prick test) dan kadar IgE spesifik positif terhadap pelbagai macam makanan. Walaupun demikian uji kulit positif terhadap suatu makanan tertentu, tidak berarti bahwa penderita tersebut alergi terhadap makanan tersebut, oleh karena itu masih diperlukan suatu uji eliminasi dan provokasi terhadap makanan tersebut untuk menentukan kepastiannya.
Alergen hirup
Alergen hirup sebagai penyebab DA dapat lewat kontak, yang dapat dibuktikan dengan uji tempel, positif pada 30-50% penderita DA, atau lewat inhalasi. Reaksi positif dapat terlihat pada alergi tungau debu rumah (TDR), dimana pada pemeriksaan in vitro (RAST), 95% penderita DA mengandung IgE spesifik positif terhadap TDR dibandingkan hanya 42% pada penderita asma di Amerika Serikat. Perlu juga diperhatikan bahwa DA juga bisa diakibatkan oleh alergen hirup lainnya seperti bulu binatang rumah tangga, jamur atau ragweed di negara-negara dengan 4 musim.

P E D I A T R I C A T O P I C D E R M A T I T I S
47
カイルパン タラ
non-commercial document; school paperwork
Infeksi kulit
Penderita dengan DA mempunyai tendensi untuk disertai infeksi kulit oleh kuman umumnya Staphylococcus aureus, virus dan jamur. Stafilokokus dapat ditemukan pada 90% lesi penderita DA dan jumlah koloni bisa mencapai 107 koloni/cm2 pada bagian lesi tersebut. Akibat infeksi kuman Stafilokokus akan dilepaskan sejumlah toksin yang bekerja sebagai superantigen, mengaktifkan makrofag dan limfosit T, yang selanjutnya melepaskan histamin. Oleh karena itu penderita DA dan disertai infeksi harus diberikan kombinasi antibiotika terhadap kuman stafilokokus dan steroid topikal.
MANIFESTASI KLINIS
Umumnya gejala DA timbul sebelum bayi berumur 6 bulan, dan jarang terjadi di bawah usia 8 minggu. Dermatitis atopik dapat menyembuh dengan bertambahnya usia, tetapi dapat pula menetap bahkan meluas dan memberat sampai usia dewasa. Terdapat kesan bahwa makin lama dan makin berat dermatitis yang diderita semasa bayi makin besar kemungkinan dermatitis tersebut menetap sampai dewasa, sehingga perjalanan penyakit dermatitis atopik sukar diramalkan.
Terdapat tiga bentuk klinis dermatitis atopik, yaitu bentuk infantil, bentuk anak, dan bentuk dewasa.
Bentuk infantil Secara klinis berbentuk dermatitis akut eksudatif dengan predileksi daerah muka terutama pipi dan daerah ekstensor ekstremitas. Bentuk ini berlangsung sampai usia 2 tahun. Predileksi pada muka lebih sering pada bayi yang masih muda, sedangkan kelainan pada ekstensor timbul pada bayi sel sudah merangkak. Lesi yang paling menonjol pada tipe ini adalah vesikel dan papula, serta garukan yang menyebabkan krusta dan terkadang infeksi sekunder. Gatal merupakan gejala yang mencolok sel bayi gelisah dan rewel dengan tidur yang terganggu. Pada sebagian penderita dapat disertai infeksi bakteri maupun jamur.
Bentuk anak Seringkali bentuk anak merupakan lanjutan dari bentuk infantil, walaupun diantaranya terdapat suatu periode remisi. Gejala klinis ditandai oleh kulit kering (xerosis) yang lebih

P E D I A T R I C A T O P I C D E R M A T I T I S
48
カイルパン タラ
non-commercial document; school paperwork
bersifat kronik dengan predileksi daerah fleksura antekubiti, poplitea, tangan, kaki dan periorbita.
Bentuk dewasa DA bentuk dewasa terjadi pada usia sekitar 20 tahun. Umumnya berlokasi di daerah lipatan, muka, leher, badan bagian atas dan ekstremitas. Lesi berbentuk dermatitis kronik dengan gejala utama likenifikasi dan skuamasi.
Stigmata pada dermatitis atopik Terdapat beberapa gambaran klinis dan stigmata yang terjadi pada DA, yaitu:
‘White dermatographism’ Goresan pada kulit penderita DA akan menyebabkan kemerahan dalam waktu 10-15 detik diikuti dengan vasokonstriksi yang menyebabkan garis berwarna putih dalam waktu 10-15 menit berikutnya.
Reaksi vaskular paradoksal Merupakan adaptasi terhadap perubahan suhu pada penderita DA. Apabila ekstremitas penderita DA mendapat pajanan hawa dingin, akan terjadi percepatan pendinginan dan perlambatan pemanasan dibandingkan dengan orang normal.
Lipatan telapak tangan Terdapat pertambahan mencolok lipatan pada telapak tangan meskipun hal tersebut bukan merupakan tanda khas untuk DA.
Garis Morgan atau Dennie Terdapat lipatan ekstra di kulit bawah mata.
Sindrom ‘buffed-nail’ Kuku terlihat mengkilat karena selalu menggaruk akibat rasa sangal gatal.
‘Allergic shiner’ Sering dijumpai pada penderita penyakit alergi karena gosokan dan garukan berulang jaringan di bawah mata dengan akibat perangsangan melanosit dan peningkatan timbunan melanin.
Hiperpigmentasi Terdapat daerah hiperpigmentasi akibat garukan terus menerus.
Kulit kering Kulit penderita DA umumnya kering, bersisik, pecah-pecah, dan berpapul folikular hiperkeratotik yang disebut keratosis pilaris. Jumlah kelenjar sebasea berkurang sehingga terjadi pengurangan pembentukan sebum, sel pengeluaran air dan xerosis, terutama pada musim panas.
‘Delayed blanch’ Penyuntikan asetilkolin pada kulit normal menghasilkan keluarnya keringat dan eritema. Pada penderita

P E D I A T R I C A T O P I C D E R M A T I T I S
49
カイルパン タラ
non-commercial document; school paperwork
atopi akan terjadi eritema ringan dengan delayed blanch. Hal ini disebabkan oleh vasokonstriksi atau peningkatan permeabilitas kapiler.
Keringat berlebihan Penderita DA cenderung berkeringat banyak sehingga pruritus bertambah.
Gatal dan garukan berlebihan Penyuntikan bahan pemacu rasa gatal (tripsin) pada orang normal menimbulkan gatal selama 5-10 menit, sedangkan pada penderita DA gatal dapat bertahan selama 45 menit.
Variasi musim
Mekanisme terjadinya eksaserbasi sesuai dengan perubahan musim belum difahami secara menyeluruh. Beberapa penelitian menunjukkan bahwa kelembaban nisbi tinggi musim baik pada kekeringan kulit penderita DA. Pada daerah dengan kelembaban nisbi tinggi musim panas berpengaruh buruk, sedangkan lingkungan sejuk dan kering akan berpengaruh baik pada kulit penderita DA.
DIAGNOSIS
Hanifin dan Lobitz (1977) menyusun petunjuk yang sekarang diterima sebagai dasar untuk menegakkan diagnosis DA Mereka mengajukan berbagai macam kriteria yang dibagi dalam kriteria mayor dan kriteria minor.
Kriteria minimal untuk menegakkan diagnosa DA meliputi pruritus dan kecenderungan dermatitis untuk menjadi kronik atau kronik residif dengan gambaran morfologi dan distribusi yang khas.
Dermatitis atopik dikenal sebagai gatal yang menimbulkan kelainan kulit, bukan kelainan kulit yang menimbulkan gatal. Tetapi belum ada kesepakatan pendapat mengenai hal ini, karena pada pengamatan, lesi di muka dan punggung bukan diakibatkan oleh garukan, selain itu dermatitis juga terjadi pada bayi yang belum mempunyai mekanisme gatal-garuk.

P E D I A T R I C A T O P I C D E R M A T I T I S
50
カイルパン タラ
non-commercial document; school paperwork
Kriteria diagnosis dermatitis atopik dari Hanifin dan Lobitz, 1977
Kriteria mayor ( > 3)
Pruritus
Morfologi dan distribusi khas: o dewasa : likenifikasi fleksura o bayi dan anak : lokasi kelainan di daerah muka dan ekstensor
Dermatitis bersifat kronik residif
Riwayat atopi pada penderita atau keluarganya
Kriteria minor ( > 3)
Xerosis
Iktiosis/pertambahan garis di palmar/keatosis pilaris
Reaktivasi pada uji kulit tipe cepat
Peningkatan kadar IgE
Kecenderungan mendapat infeksi kulit/kelainan imunitas selular
Dermatitis pada areola mammae
Keilitis
Konjungtivitis berulang
Lipatan Dennie-Morgan daerah infraorbita
Keratokonus
Katarak subskapular anterior
Hiperpigmentasi daerah orbita
Kepucatan/eritema daerah muka
Pitiriasis alba
Lipatan leher anterior
Gatal bila berkeringat
Intoleransi terhadap bahan wol dan lipid solven
Gambaran perifolikular lebih nyata
Intoleransi makanan
Perjalanan penyakit dipengaruhi lingkungan dan emosi
White dermographism/delayed blanch

P E D I A T R I C A T O P I C D E R M A T I T I S
51
カイルパン タラ
non-commercial document; school paperwork
PEMERIKSAAN LABORATORIUM
Telah dilaporkan pelbagai hasil laboratorium penderita DA, walaupun demikian sulit untuk menghubungkan hasil laboratorium ini dengan defek yang ada. Imunoglobulin IgG, IgM, IgA dan IgD biasanya normal atau
sedikit meningkat pada penderita DA. Tujuh persen penderita DA mempunyai kadar IgA serum yang rendah, dan defisiensi IgA transien banyak dilaporkan pada usia 3-6 bulan. Kadar IgE meningkat pada 80-90% penderita DA dan lebih tinggi lagi bila sel asma dan rinitis alergika. Tinggi rendahnya kadar IgE ini erat hubungannya dengan berat ringannya penyakit, dan tinggi rendahnya kadar IgE tidak mengalami fluktuasi baik pada saat eksaserbasi, remisi, atau yang sedang mendapat pengobatan prednison atau azatioprin. Kadar IgE ini akan menjadi normal 6-12 bulan setelah terjadi remisi.
Leukosit Limfosit Jumlah limfosit absolut penderita alergi dalam batas
normal, baik pada asma, rinitis alergilk, maupun pada DA

P E D I A T R I C A T O P I C D E R M A T I T I S
52
カイルパン タラ
non-commercial document; school paperwork
Walaupun demikian pada beberapa penderita DA berat. dapat disertai menurunnya jumlah sel T dan meningkatnya sel B.
Eosinofil Kadar eosinofil pada penderita DA sering meningkat. Peningkatan ini seiring dengan meningkatnya IgE, tetapi tidak seiring dengan beratnya penyakit.
Leukosit polimorfonuklear (PMN) Dari hasil uji nitro blue tetrazolium (NBT) ternyata jumlah PMN biasanya dalam batas normal.
Komplemen Pada penderita DA kadar komplemen biasanya normal atau sedikit meningkat.
Bakteriologi Kulit penderita DA aktif biasanya mengandung bakteri patogen, seperti Staphylococcus aureus. walaupun tanpa gejala klinis infeksi.
Uji kulit dan provokasi Diagnosis DA ditegakkan hanya berdasarkan gejala klinis. Untuk mencari penyebab timbulnya DA harus disertai anamnesis yang teliti dan bila perlu dengan uji kulit serta uji eliminasi dan provokasi. Korelasi uji kulit hanya baik hasilnya bila penyebabnya alergen hirup. Untuk makanan dianjurkan dengan uji eliminasi dan provokasi. Reaksi pustula terhadap 5% nikel sulfat yang diberikan dengan uji tempel dianggap karakteristik untuk DA oleh beberapa pengamat. Patogenesis reaksi pustula nikel fosfat ini belum diketahui walaupun data menunjukkan reaksi iritan primer.
DIAGNOSIS BANDING Dermatitis Kontak Alergi Dermatophytosisataur dermatophytids Sindrom defesiensi imun Sindrom Wiskott-Aldrich Sindrom Hyper-IgE Penyakit Neoplastik Langerhans’ cell histiocytosis Penyakit Hodgkin Dermatitis Numularis Skabies Dermatitis Seborrheic

P E D I A T R I C A T O P I C D E R M A T I T I S
53
カイルパン タラ
non-commercial document; school paperwork
Skabies: Pada bayi gejala klinis DA terutama mulai dari pipi dan tidak mengenai telapak tangan serta kaki. Tanda skabies pada bayi ditandai dengan papula yang relatif besar (biasanya pada punggung atas), vesikel pada telapak tangan dan kaki, dan terdapat dennatilis pruritus pada anggota keluarga. Tungau dan telur dapat dengan mudah ditemukan dari scraping vesicle. Skabies memberi respons yang baik terhadap pengobatan dengan γ-benzen heksaklorida.
Dermatitis seboroik infantile: Penyakit ini dibedakan dari DA dengan: (1) pruritus ringan, (2) onset invariabel pada daerah pantat halus, tidak bersisik, batas jelas, merah terang, dan (3) sisik kuning gelap pada pipi, badan dan lengan. Dermatitis seboroik infantil sering berhubungan dengan dermatitis atopik. Pada suatu penelitian, 37% bayi dengan dermatitis seboroik akan menjadi DA 5-13 tahun kemudian.
Dermatitis kontak Anak yang lebih tua dengan DA dapat menjadi eksema kronik pada kaki. Bentuk ini harus dibedakan dengan dermatitis kontak karena sepatu.
KOMPLIKASI Pada anak penderita DA, 75% akan disertai penyakit alergi lain di
kemudian hari. Penderita DA mempunyai kecenderungan untuk mudah mendapat infeksi virus maupun bakteri (impetigo, folikulitis, abses, vaksinia. Molluscum contagiosum dan herpes).
Infeksi virus umumnya disebabkan oleh Herpes simplex atau vaksinia dan disebut eksema herpetikum atau eksema vaksinatum. Eksema vaksinatum ini sudah jarang dijumpai, biasanya terjadi pada pemberian vaksin varisela, baik pada keluarga maupun penderita. lnfeksi Herpes simplex terjadi akibat tertular oleh salah seorang anggota keluarga. Terjadi vesikel pada daerah dermatitis, mudah pecah dan membentuk krusta, kemudian terjadi penyebaran ke daerah kulit normal.
Penderita DA, mempunyai kecenderungan meningkatnya jumlah koloni Staphylococcus aureus.

P E D I A T R I C A T O P I C D E R M A T I T I S
54
カイルパン タラ
non-commercial document; school paperwork
PENGOBATAN Dermatitis atopik umumnya tidak dapat disembuhkan, tetapi
dapat dikontrol. Sebagian penderita mengalami perbaikan sesuai dengan bertambahnya usia. Langkah yang penting adalah menjalin hubungan baik dengan orang tua penderita, menjelaskan mengenai penyakit tersebut secara rinci, termasuk perjalanan penyakit, dampak psikologis, prognosis, dan prinip penatalaksanaan. Langkah pertama dalam penatalaksanaan penderita DA adalah menghindari atau sedikitnya mengurangi faktor penyebab, misalnya eliminasi makanan, faktor inhalan, atau faktor pencetus sel Walaupun masih kontroversial ternyata Ibayi yang memperoleh air susu ibu lebih jarang menderita DA dibandingkan bayi yang memperoleh pengganti air susu ibu.
Penghindaran faktor alergen pada bayi berumur kurang dari l tahun akan mengurangi beratnya gejala. DA. Maka dianjurkan agar bayi dengan riwayat keluarga alergi memperoleh hanya ASI sediIkitnya 3 bulan, bila mungkin 6 bulan pertama dan ibu yang menyusui dianjurkan untuk tidak makan telur, kacang tanah, terigu, dan susu sapi. Susu sapi diduga merupakan alergen kuat pada bayi dan anak, maka bagi mereka yang jelas alergi terhadap susu dapat dipergunakanbangkan untuk menggantinya dengan susu kedelai, walaupun kemungkinan alergi terhadap susu kedelai masih ada. \60% penderita DA di bawah usia 2 tahun memberikan reaksi positif pada uji kulit terhadap telur, susu, ayam, dan gandum. Reaksi positif ini akan menghilang dengan bertambahnya usia. Walaupun pada uji kulit positif terhadap antigen makanan tersebut di atas, belum tentu mencerminkan gejala klinisnya. Demikian pula hasil uji provokasi, sehingga membatasi makanan anak tidak selalu berhasil untuk mengatasi penyakitnya.
Membutuhkan terapi yang integral dan sistemik, meliputi hidrasi kulit, terapi topikal, identifikasi dan eliminasi faktor penyebab dan pencetus dan bila perlu terapi sistemik.
Penatalaksanaan dasar diberikan untuk semua kasus baik yang ringan, sedang maupun berat, berupa berupa perawatan kulit, hidrasi, kortikosteroid topikal, antihistamin, tars, antibiotik bila perlu, identifikasi dan eliminasi faktor-faktor pencetus kekambuhan.

P E D I A T R I C A T O P I C D E R M A T I T I S
55
カイルパン タラ
non-commercial document; school paperwork
Perawatan Kulit Hidrasi adalah terapi DA yang esensial. Dasar hidrasi yang adekuat adalah peningkatan kandungan air pada kulit dengan cara mandi dan menerapkan sawar hidrofobik. untuk mencegah evaporasi. Mandi selama 15-20 menit 2 kali sehari tidak menggunakan air panas dan tidak menambahkan oil (minyak) karena mempengaruhi penetrasi air. Sabun dengan moisturizers disarankan Setelah mandi memberihkan sisa air dengan handuk yang lembut. Bila perlu pengobatan topikal paling baik setelah mandi karena penetrasi obat jauh lebih baik. Pada pasien kronik diberikan 3-4 kali sehari dengan water-in-oil moisturizers sediaan lactic acid.
Pengobatan topikal adalah untuk mengatasi kekeringan kulit dan peradangan. Mengatasi kekeringan kulit atau memelihara hidrasi kulit dapat dilakukan dengan mandi memakai sabun lunak tanpa pewangi. Meskipun mandi dikatakan dapat memperburuk kekeringan kulit, namun berguna untuk mencegah terjadi infeksi sekunder. Jangan menggunakan sabun yang bersifat alkalis dan sebaliknya pakailah sabun atau pembersih yang mempunyai pH 7,0. Pemberian pelembab kulit penting untuk menjaga hidrasi antara lain dengan dasar lanolin, krim air dalam minyak, atau urea 10% dalam krim. Untuk mengatasi peradangan dapat diberikan krim kortikosteroid. Penggunaan kortikosteroid topikal golongan kuat sebaiknya berhati-hati dan tidak digunakan di daerah muka. Apabila dermatitis telah teratasi maka secepatnya pengobatan dialihkan pada penggunaan kortikosteroid golongan lemah atau krim pelembab. Untuk daerah muka sebaiknya digunakan krim hidrokortison 1%.
Dengan pengobatan topikal yang baik dapat dicegah penggunaan pengobatan sistemik. Karena perjalanan penyakit DA adalah kronik dan residif, maka untuk pemakaian kortikosteroid topikal maupun sistemik untuk jangka panjang sebaiknya diamati efek samping yang mungkin terjadi. Bila dengan kortikosteroid topikal tidak adekuat untuk menghilangkan rasa gatal dapat ditambahkan krim yang mengandung mental, fenol, lidokain, atau asam salisilat. Bila dengan pengobatan topikal ini tetap tidak adekuat, maka dapat dipertimbangkan pemberian pengobatan sistemik

P E D I A T R I C A T O P I C D E R M A T I T I S
56
カイルパン タラ
non-commercial document; school paperwork
Kortikosteroids topikal Kortikosteroid topikal mempunyai efek antiinflamasi, antipruritus, dan efek vasokonstriktor. Yang perlu diperhatikan pada penggunaan kortikosteroid topikal adalah: segera setelah mandi dan diikuti berselimut untuk meningkatkan penetrasi; tidak lebih dari 2 kali sehari; bentuk salep untuk kulit lembab bisa menyebabkan folikulitis; bentuk krim toleransinya cukup baik; bentuk lotion dan spray untuk daerah yang berambut; pilihannya adalah obat yang efektif tetapi potensinya terendah; efek samping yang harus diperhatikan adalah: atropi, depigmentasi, steroid acne dan kadang-kadang terjadi absorbsi sistemik dengan supresi dari hypothalamic-pituitary-adrenal axis; bila kasus membaik, frekuensi pemakaian diturunkan dan diganti dengan yang potensinya lebih rendah; bila kasus sudah terkontrol, dihentikan dan terapi difokuskan pada hidrasi.
Antihistamin Untuk mengurangi rasa gatal dapat diberikan antihistamin (H1) seperti difenhidramin atau terfenadin, atau antihistamin nonklasik lain. Kombinasi antihistamin H1 dengan H2 dapat menolong pada kasus tertentu. Pada bayi usia muda, pemberian sedasi dengan kloralhidrat dapat pula menolong. Penggunaan obat lain seperti sodium kromoglikat untuk menstabilkan dinding sel mast dapat memberikan hasil yang memuaskan pada 50% penderita.
Penggunaan kortikosteroid oral sangat terbatas, hanya pada kasus sangat berat dan diberikan dalam waktu singkat, misalnya prednison 0,5-1,0 mg/kgBB/hari dalam waktu 4 hari.
Merupakan terapi standar, tetapi belum tentu efektif untuk menghilangkan rasa gatal karena rasa gatal pada DA bisa tak terkait dengan histamin.
Tars Mempunyai efek anti-inflamasi dan sangat berguna untuk mengganti kortikosteroid topikal pada manajemen penyakit kronik. Efek samping dari tar adalah folikulitis, fotosensitisasi dan dermatitis kontak.
Antibiotik sistemik Antibiotik sistemik dapat dipertimbangkan untuk mengatasi DA yang luas dengan infeksi sekunder. Antibiotik yang dianjurkan adalah eritromisin, sefalosporin, kloksasilin, dan terkadang ampisilin Infeksi di curigai bila ada krusta yang luas, folikulits, pioderma dan furunkulosis. S. aureus yang resisten

P E D I A T R I C A T O P I C D E R M A T I T I S
57
カイルパン タラ
non-commercial document; school paperwork
penisilin merupakan penyebab tersering dari flare akut. Bila diduga ada resistensi penisilin, dicloxacillin atau sefalexin dapat digunakan sebagai terapi oral lini pertama. Bila alergi penisilin, eritromisin adalah terapi pilihan utama, dengan perhatian pada pasien asma karena bersama eritromisin, teofilin akan menurunkan metabolismenya. Pilihan lain bila eritomisin resisten adalah klindamisin.. Dari hasil pembiakan dan uji kepekaan terhadap Staphylococcus aureus 60% resisten terhadap penisilin, 20% terhadap eritromisin, 14% terhadap tetrasiklin, dan tidak ada yang resisten terhadap sefalosporin Imunoterapi dengan ekstrak inhalan umumnya tidak menolong untuk mengatasi DA pada anak.
Identifikasi dan eliminasi faktor-faktor eksaserbasi Sabun dan baju yang bersifat iritatif dihindari. Baju iritatif dari wol dihindari. Demikian juga keringat dapat juga mengiritasi kulit. Stres sosial dan emosional juga harus dihindari. Eliminasi alergen makanan, binatang dan debu rumah.
Selain manajemen dasar dilaksanakan pada DA berat terapi imunomodulasi sudah harus dilaksanakan.
Kortikosteroid sistemik. Efek perbaikannya cepat, tetapi flare yang parah sering terjadi pada steroid withdrawal. Bila tetap harus diberikan, tapering dan perawatan intensif kulit harus dijalankan.
Thymopentin. Untuk dapat mengurangi gatal-gatal dan eritem digunakan timopentin subkutan 10 mg/ dosis 1 kali/hari selama 6 minggu, atau 3 kali/minggu selama 12 minggu.
Interferon-gamma. Dosis yang digunakan g /m2/ hari subkutan diberikan selama 12 minggu.ug-100uantara 50
Siklosporin A. Pemberian per oral 5 mg/kg/hari selama 6 minggu. Dapat pula diberikan secara topikal dalam bentuk salep atau gel 5%.
Tacrolimus. Digunakan takrolimus 0,1 % dan 0,03 % topikal dua kali sehari. Obat ini umumnya menunjukan perbaikan pada luasnya lesi dan rasa gatal pada minggu pertama pengobatan. Tacrolimus tidak mempengaruhi fibroblasts sehingga tidak menyebabkan atropi kulit.
Pimecrolimus Pemakaian pimecrolimus 1,0 % mereduksi gejala sebesar 35 %.

P E D I A T R I C A T O P I C D E R M A T I T I S
58
カイルパン タラ
non-commercial document; school paperwork
Gammaglobulin Bekerja sebagai antitoksin, antiinflamasi dan anti alergi. Pada DA Gammaglobulin intravena (IVIG) adalah terapi yang sangat mahal, namun harus dipertimbangkan pada kasus kasus khusus.
Probiotik Lactobacillus rhamnosus GG 1 kapsul (109) kuman/dosis dalam 2 kali/hari memperbaiki kondisi kulit setelah 2 bulan.
Perlakuan khusus diperlukan untuk penderita DA Berat. Penentuan gradasi berat-ringannya DA dapat mempergunakan kriteria Rajka dan Langeland sebagaimana tabel berikut :
1. Luasnya lesi kulit fase anak/dewasa
< 9% luas tubuh + 1
9-36% luas tubuh + 2
36 % luas tubuh + 3 fase infantil
< 18% luas tubuh + 1
18-54% luas tubuh + 2
54% luas tubuh + 3 2. Perjalanan penyakit
remisi > 3 bulan/tahun + 1
remisi < 3 bulan/tahun + 2
kambuhan + 3 3. Intensitas penyakit
gatal ringan, gangguan tidur + 1
gatal sedang, gangguan tidur + 2
gatal berat, gangguan tidur + 3 Penilaian skor
3-4 : ringan 5-7 : sedang 8-9 : berat
REFERENSI Jacoeb TNA. Manifestasi Klinis Dermatitis Atopik pada Bayi dan Anak. Dalam: Boediardja
SA, Sugito TL, Rihatmadja R. Dermatitis pada Bayi dan Anak. Jakarta: Fakultas Kedokteran Universitas Indonesia, 2004.
Sugito TL. Penatalaksanaan Terbaru Dermatitis Atopik. Dalam: Boediardja SA, Sugito TL, Rihatmadja R. Dermatitis pada Bayi dan Anak. Jakarta: Fakultas Kedokteran Universitas Indonesia, 2004.
Sularsito SA, Djuanda S. Dermatitis. Dalam: Djuanda A, Hamzah M, Aisah S (Editor). Ilmu Penyakit Kulit dan Kelamin. Edisi Kelima. Jakarta: Fakultas Kedokteran Universitas Indonesia, 2007.

P E D I A T R I C A T O P I C D E R M A T I T I S
59
カイルパン タラ
non-commercial document; school paperwork
UNDERSTANDING ATOPIC DERMATITIS AND ITS MANAGEMENT IN CHILDREN
Author: Prof. Jayakar Thomas MD, DD, MNAMS, PhD. Senior Consultant Dermatologist, Kanchi Kamakoti CHILDS Trust Hospital, Chennai, INDIA
From: e-Journal of the Indian Society of Teledermatology, 2007; Vol I, No.1 http://www.insted.in/ejournal/review11.pdf
Introduction Atopic dermatitis (AD) is a common condition that affects more than one in ten children, and the incidence is increasing. There are probably several reasons for this, including higher exposure to air pollution, smaller families with less exposure to infections, more pets, higher maternal age, a wider range of foods, and the practice of evidencebased medicine. There is clearly also an important hereditary component to atopic eczema. This is complex because not all affected children are atopic, though the genes implicated in atopy are likely to be involved, together with others as yet unknown. AD usually presents during the first year of life, and when it is severe it is extremely disabling. It may also cause major psychological problems.1 Most affected children are also allergic to house dust mite, and this is probably a major cause of exacerbation of the condition. Probably less than 10% overall have IgE mediated food allergy, but some have late phase reactions with positive results on patch tests to foods.
Pathogenesis Several observations suggest that AD is the cutaneous manifestation of a systemic disorder that also gives rise to asthma, food allergy, and allergic rhinitis. These conditions are all characterized by elevated serum IgE levels and peripheral eosinophilia. AD is often the initial step in the so-called "atopic march," which leads to asthma and allergic rhinitis in the majority of afflicted patients.2,3,4 In experimental models of AD, the induction of allergic skin

P E D I A T R I C A T O P I C D E R M A T I T I S
60
カイルパン タラ
non-commercial document; school paperwork
inflammation by epicutaneous application of allergens has been found to augment the systemic allergic response and airway hyperreactivity characteristic of asthma. At least two forms of AD have been delineated: an "extrinsic" form associated with IgE-mediated sensitization involving 70–80% of the patients, and an "intrinsic" form without IgE-mediated sensitization involving 20–30% of the patients. Both forms of AD have associated eosinophilia. In extrinsic AD, memory T cells expressing the skin homing receptor, cutaneous lymphocyte-associated antigen (CLA), produce increased levels of Th2 cytokines. These include IL-4 and IL-13, which are known to induce isotype switching to IgE synthesis, as well as IL-5, which plays an important role in eosinophil development and survival. These CLA+ T cells also produce abnormally low levels of IFN- , a Th1 cytokine known to inhibit Th2 cell function. Intrinsic AD is associated with less IL-4 and IL-13 production than extrinsic AD.5
Clinical aspects AD is usually the first manifestation of atopy and may coincide with food allergy; asthma often follows, then allergic rhinitis. There is a wide spectrum of presentations of atopic eczema, from minimal flexural eczema to erythroderma. The skin of a child with eczema is generally dry. Dryness of skin or xerosis is the hallmark of atopic dermatitis in children. The eczema can occur anywhere, but there are particular patterns that are more common at certain ages. The face is usually the first to be affected. In crawling infants the forearms, extensor aspects of the knees, and the ankle flexures are often the most affected. In older children the flexor aspects of the elbows and the knees are mostly affected. The eczema may be moist and weeping or may be thickened (lichenified) and dry. In Indian children with darker skin the rash may have a papular nature. Scratch marks are always seen. The course of the condition fluctuates: causes of exacerbations may be evident but usually are not (particularly with reference to severe cutaneous reaction to mosquito bites). Infective complications are common. Staphylococcal infection may manifest as typical bullous impetigo or simply as a worsening of the eczema with increased redness and oozing. Staphylococcal folliculitis may occur as a result of occlusion from greasy emollients or wet

P E D I A T R I C A T O P I C D E R M A T I T I S
61
カイルパン タラ
non-commercial document; school paperwork
dressings. Streptococcal infection may manifest as increased redness and erosion of the skin or as pustular lesions. Atopic children are particularly prone to severe widespread herpes simplex infections; the spread of the condition is mainly systemic but the areas most affected are the areas of active eczema. The child's life is limited by the constraints of care of the skin, which can separate the child from his or her peers. This can include sport, swimming, and dietary restrictions. The child feels unattractive and different and may have problems with self image and self confidence. Most children with eczema are atopic and are therefore allergic to inhalants such as house dust mite, grass pollens, and animal dander. Some children develop eczema on the face during the pollen season, and many parents report that their child's eczema is worse after close contact with pets. The highest proportion of IgE is produced against house dust mite and mosquitoes, and this must be the most important allergen in the exacerbation of eczema.6 House dust mite is present in large numbers in children's beds and as well as causing asthma causes exacerbations of eczema. Several studies have shown that actions to reduce dust mite numbers are associated with amelioration of eczema. This is not surprising as in children highly allergic to the mites, skin contact is bound to have a deleterious effect on the eczema. The role of delayed hypersensitivity to house dust mite is also likely to be important. People with AD have positive results to patch tests and positive lymphoproliferative responses to the mite. Unfortunately, in everyday life minimization of house dust mite in bedding is difficult to achieve. In general, food allergy is caused by immunological mechanisms, food intolerance is not. Food intolerance is relatively common: certain chemicals in foods may cause worsening of the eczema for example, tartrazine or other colourings in food by mechanisms that are unclear. Food allergy is age dependent. It may be severe in the infant and become less so with age. Allergy to some foods (such as egg and cows' milk) is relatively transient, whereas allergy to peanuts or shellfish may continue throughout life. The association between atopic eczema and food allergy is complex, though it is usually children with severe atopic eczema who have food allergy. Probably

P E D I A T R I C A T O P I C D E R M A T I T I S
62
カイルパン タラ
non-commercial document; school paperwork
less than 10% of all children with atopic eczema have IgE mediated food allergy with angioedema and urticaria, when the diagnosis is obvious from the immediacy of the symptoms and can be confirmed by a wheal more than 5 mm in diameter after a skin prick test. Some of these children have multiple food allergies. There is no doubt that IgE mediated food allergy can act as a trigger for exacerbations of eczema, but most parents recognize the allergy and the food is avoided. What is not clear is the role of late phase food reactions, which cause exacerbations of the eczema without urticaria or angioedema. These can be confirmed by atopy patch tests and food provocation tests.7,8,9 This is receiving increasing attention. Woolen material in direct contact with the skin is a major irritant. Shiny nylon materials and some acrylics may irritate, but cottonpolyester mixtures are usually well tolerated. Soap in excess and bubble baths excessively dry the skin, and many perfumed and "medicated" products applied to the skin will cause irritation. Some of the plant extracts preparations favoured by alternative practitioners act as irritants or allergens and a query about the use of these should always be part of the history taking.
Management Explanation and counseling are a vital part of the successful management of childhood eczema. Parents will have received a barrage of advice from a range of medical, paramedical, and nonmedical "experts" and require a clear understanding of the nature of the condition, a long term management plan, and a realistic expectation of the results of treatment. Terminology is often confusing; the terms atopic eczema and atopic dermatitis are often used synonymously. It is essential to talk in terms of control rather than cure, otherwise parents will search for an end point after which care will no longer be required, and this is an unrealistic expectation. The condition should be explained as a multifactorial disorder, and it must be appreciated that just as there is no "cure" there is no single "cause." Often no explanation can be found for a particular flare up of the condition, and many factors are probably working in combination at all times.

P E D I A T R I C A T O P I C D E R M A T I T I S
63
カイルパン タラ
non-commercial document; school paperwork
Dealing with xerosis Bath oils and products containing oatmeal are useful and prevent the drying of the skin that bathing can induce. Bath oils that contain antiseptic may have added benefit in certain cases but have a tendency to over-dry and sometimes actually irritate the skin. The child should have either a bath with additive or a short shower. It is essential to find a suitable moisturizer that can be applied all over twice a day whether or not there is active eczema. Creams containing moisturizing agents, emulsifying ointment, and creams or ointments with lanolin can be used. If a product stings the skin it must be abandoned. The most likely irritant in emollient creams is the stabilizer propylene glycol. Products that contain urea almost always sting broken skin and are unsuitable in these children. Use of wet dressings Wet dressings are useful in children with severe widespread eczema. This is essentially an inpatient procedure but can be used for short periods at home.10 A water based emollient is applied all over; a corticosteroid cream (rather than ointment in this case because cream is more water miscible) is applied to the areas of active eczema. The creams are covered with a double layer of wrapping, the innermost of which is wetted with tepid water. The material may be cotton sheeting covered with a crepe bandage, though an easier alternative is the use of a double layer of tubular elasticized bandage. The procedure is repeated three times a day. This treatment is usually effective in clearing the eczema in three or four days. Avoidance of allergens House dust mite is the most important allergen. Avoidance measures have to be carried out assiduously and must include encasing the mattress and pillows as well as dealing with the top covers, either by encasement or by hot (>60°C) washing. If food allergy is suspected, the child should be referred to a paediatric dietician. In general, it is children with severe atopic eczema who have food allergy or food

P E D I A T R I C A T O P I C D E R M A T I T I S
64
カイルパン タラ
non-commercial document; school paperwork
intolerance. Children with flexural eczema are unlikely to have food allergy, unless the history suggests otherwise. Topical corticosteroids It is often necessary to spend some time counseling the parents that topical steroid preparations used appropriately are safe. The strength chosen depends on the severity of the eczema and the site affected. The frequency of application depends on the individual product. The caution, however, is to be aware of steroid dependency which can be currently avoided/prevented by the use of topical calcineurin inhibitors (TCI). Topical antibacterials Staphylococcus aureus is commonly cultured from eczematous skin, and there may be obvious signs of infection. For localized infections, mupirocin, sisomycin, and fusidic acid ointment may be effective. To prevent infections it is useful to bathe the child in preparations containing triclosan or benzalkonium chloride.11 Topical immunosuppressants/ Topical calcineurin inhibitors Tacrolimus is a potent immunosuppressive drug used in organ transplantation. A topical formulation has been shown to be effective in trials in patients with moderate to severe atopic dermatitis. Studies specifically related to childhood eczema have confirmed its efficacy. The main side effect is a sensation of burning. A concern has been raised as to whether application to skin exposed to sun could increase the long term risk of skin cancer. Pimecrolimus (an ascomycin derivative) is a newer immunosuppressive agent, similar to tacrolimus. Studies in children are very encouraging. The approval of topical calcineurin inhibitors for the treatment of AD represents a significant advance in our management options for this disease.12,13,14 The distinction between pimecrolimus and tacrolimus is that the former is a cream while the latter is an ointment. Tacrolimus is currently marketed as an ointment that is more potent but also more irritating. Importantly, there are situations in which these topical calcineurin inhibitors (TCI) may be advantageous over topical corticosteroids and

P E D I A T R I C A T O P I C D E R M A T I T I S
65
カイルパン タラ
non-commercial document; school paperwork
may be useful as first-line therapy. These would include treatment of patients who are poorly responsive to topical steroids or have steroid phobia, and treatment of face and neck dermatitis where ineffective, low-potency topical corticosteroids are usually used due to fears of steroid-induced skin atrophy. The potential use of topical calcineurin inhibitors as maintenance therapy is also intriguing for prevention of AD flares and progression of the atopic march. However, although systemic absorption of these compounds is low, there is a need for careful surveillance to rule out the possibility that skin cancers and increased viral skin infections will appear when such agents are used long-term. One has to remember that TCIs are not a substitute for topical steroids. But when used in combination and the as solo therapy TCIs are by far the best to give the early care and prevent flare. Oral medications Immunosuppressive drugs Severe atopic eczema is a serious condition, with huge loss of quality of life for the child on a par with juvenile rheumatoid arthritis. It is therefore essential that such children are treated adequately. The use of oral steroids should be avoided because of severe rebound of the eczema on withdrawal, the eczema becoming unstable after several courses, and the long term side effects. There are generally two alternatives for severe eczema, cyclosporin and azathioprine. Ciclosporin Recent studies have confirmed the efficacy of ciclosporin (2 to 4 mg/Kg) in childhood atopic eczema. Regrettably the improvement is often not maintained after withdrawal of the drug. Continuous treatment is rarely justified in view of the long term risks (such as hypertension and renal dysfunction).15,16 However, it has a place as an effective, safe, and well tolerated short term option for the management of severe refractory disease in children. Azathioprine (1mg/Kg) is a safer drug for long term use, though it does have several side effects, including nausea, fatigue, myalgia, and liver dysfunction. It is essential to assay for thiopurine methyltransferase before treatment starts as children deficient in this enzyme will experience marked bone marrow suppression. In

P E D I A T R I C A T O P I C D E R M A T I T I S
66
カイルパン タラ
non-commercial document; school paperwork
most children it is effective at low dosage. The main long term side effect that could theoretically occur (as with ciclosporin) is the development of lymphoma.17 The advantage of this drug is that it can be used continuously. Other possibilities include the leukotriene inhibitors zafirlukast and montelukast, given orally.18,19 Chinese herbal medicines have also been used successfully but are not without danger.20 Antihistamines Sedating antihistamines such as promethazine given at bedtime are useful. The sedation is an important feature of their antipruritic action. It is still debatable whether non-sedating antihistamines such as cetirizine and loratadine are useful because generally the role of histamine in eczema is somewhat limited. However, a large study of the use of cetirizine in adults with atopic eczema showed a significant reduction of clinical manifestations in those treated.21
Summary • Atopic dermatitis in children is a complex condition • Four in five children with atopic eczema have IgE mediated
allergy to inhalants or foods • House dust mite and mosquitoes exacerbates atopic dermatitis • Food allergy exacerbates eczema in less than one in ten
children • To reduce the need for admission to hospital children with
severe eczema can be treated with topical or oral immunosuppression
REFERENCES 1. Howlett S. Emotional dysfunction, child-family relationships and childhood atopic dermatitis.
Br J Dermatol 1999; 140: 381-384 2. Spergel, J.M., and Paller, A.S. 2003. Atopic dermatitis and the atopic march. J. Allergy Clin.
Immunol. 112:S128-S139 3. Novak, N., Bieber, T., and Leung, D.Y.M. 2003. Immune mechanisms leading to atopic
dermatitis. J. Allergy Clin. Immunol. 112:S128-S139 4. Holgate ST, Church MK, eds. Allergy. London: Gower Medical Publishing, 1993 5. Barnetson RS, Wright AL, Benton EC. IgE-mediated allergy in adults with severe atopic
eczema. Clin Exp Allergy 1989; 19: 321-325 6. Tan BB, Weald D, Strickland I, Friedmann PS. Double-blind controlled trial of effect of
housedustmite allergen avoidance on atopic dermatitis. Lancet 1996; 347: 15-18

P E D I A T R I C A T O P I C D E R M A T I T I S
67
カイルパン タラ
non-commercial document; school paperwork
7. Mitchell EB, Crow J, Chapman MD, Jouhal SS, Pope FM, Platts-Mills T. Basophils in allergen-induced patch test sites in atopic dermatitis. Lancet 1982; i:127-130
8. Eigenmann PA, Sicherer SH, Borkowski TA, Cohen BA, Sampson HA. Prevalence of IgE-mediated food allergy among children with atopic dermatitis. Pediatrics 1998; 101: 108
9. Roehr CC, Reibel S, Ziegert M, Sommerfield C, Wahn U, Niggemann B. Atopy patch tests, together with determination of specific IgE levels, reduce the need for oral food challenges in children with atopic dermatitis. J Allergy Clin Immunol 2001; 107: 548-553
10. Goodyear HM, Spowart K, Harper JI. `Wet-wrap' dressings for the treatment of atopic eczema in children. Br J Dermatol 1991; 125: 604
11. Sporik R, Kemp AS. Topical triclosan treatment of atopic dermatitis. J Allergy Clin Immunol 1997; 99:861.
12. Boguniewicz M, Fiedler VC, Raimer S, Lawrence ID, Leung DY, Hanifin JM. A randomized, vehiclecontrolled trial of tacrolimus ointment for the treatment of atopic dermatitis in children. J Allergy Clin Immunol 1998; 102: 637-644
13. Kang S, Lucky AW, Pariser D, Lawrence I, Hanifin JM. Long-term safety and efficacy of tacrolimus ointment for the treatment of atopic dermatitis in children. J Am Acad Dermatol 2001; 44(suppl 1): S58-S64
14. Harper J, Green A, Scott G, Gruendl E, Dorobek B, Cardno M, Burtin P. First experience of topical SDZ ASM 981 in children with atopic dermatitis. Br J Dermatol 2001; 144: 781-787
15. Berth-Jones J, Finlay AY, Zaki I, Tan B, Goodyear H, Lewis-Jones S, et al. Cyclosporine in severe atopic dermatitis: a multicenter study. J Am Acad Dermatol 1996; 34: 1016-1021
16. Harper JI, Berth-Jones J, Camp RDR, Dillon MJ, Finlay AY, Holden CA, et al. Cyclosporin for atopic dermatitis in children. Dermatology 2001; 203: 3-6
17. Murphy LA, Atherton DJ. Azathioprine in severe childhood eczema: value of TPMT as a predictor of outcome and safety in treatment. Br J Dermatol 2001; 144: 927.
18. Carucci JA, Washenik K, Weinstein A, Shupack J, Cohen DE. The leucotriene antagonist zafirlukast as a therapeutic agent for atopic dermatitis. Arch Dermatol 1998; 134: 785-786
19. Pei AY, Chan HH, Leung TF. Montelukast in the treatment of children with moderate-to-severe atopic dermatitis: a pilot study. Pediatr Allergy Immunol 2001; 12: 154-158
20. Graham-Brown R. Toxicity of Chinese herbal remedies. Lancet 1992; 340: 673-674 21. Hannuksela M, Kalimo K, Lammintausta K, Mattila T, Turjanmaa K, Varjonen E, et al. Dose
ranging study: cetirizine in the treatment of atopic dermatitis inadults. Ann Allergy 1993; 70: 127-133

P E D I A T R I C A T O P I C D E R M A T I T I S
68
カイルパン タラ
non-commercial document; school paperwork
TOPICAL CALCINEURIN INHIBITORS: EFFICACY AND SAFETY IN ATOPIC DERMATITIS
Author: L. Guenther, MD, FRCPC Division of Dermatology, University of Western Ontario, London, ON, Canada
Last modified: September 16, 2010 http://www.skintherapyletter.com/fp/2007/3.2/3.html
Atopic Dermatitis
Atopic Dermatitis (AD) is a chronic or chronic-relapsing inflammatory skin disease associated with hyperreactivity to environmental triggers; it can affect up to 20% of children [Williams H, et al. J Allergy Clin Immunol 103(1 Pt 1):125-38 (1999 Jan).]. Symptoms include flexural (facial and extensor in children) erythema, excoriations, lichenification, and xerosis.
Part of the atopic triad (AD, hay fever, asthma).
Itch is often so intense that patients cannot sleep or concentrate.
Patients commonly scratch to the point of bleeding and may have secondary infection.
Significantly impacts the sufferer as well as his or her family. It is a ‘life-altering’ disease.
Treatments include:
Avoidance of triggers
Emollients
Topical corticosteroids
Topical calcineurin inhibitors (TCIs)
Antimicrobials for infection
Oral antihistamines for pruritus
Systemic corticosteroids, systemic immunosuppressants and phototherapy for severe disease
Mechanism of Action of TCIs
Blocks T-cell activation and suppress release of pro-inflammatory cytokines.

P E D I A T R I C A T O P I C D E R M A T I T I S
69
カイルパン タラ
non-commercial document; school paperwork
Binds to FK-506 binding protein-12, forming a complex that inhibits calcineurin, thereby preventing activation of the nuclear factor of activated T cells (NFAT), which in turn blocks gene transcription for interleukin-2.
Tacrolimus reduces Langerhans cell activation of T cells, and cytokine production in eosinophils, mast cells, and basophils.
Approved Indication of TCIs
The US FDA approved tacrolimus ointment for moderate-to-severe AD (0.03% for 2+ years, 0.1% for 16+ years) in December 2000, and pimecrolimus 1% cream for mild-to-moderate AD for 2+ years in December 2001.
Both medications are indicated for short-term and intermittent long-term treatment in patients for whom conventional therapies are contraindicated, not tolerated, or not sufficiently effective.
Black Box Warning for TCIs
A Black Box warning, issued in January 2006, resulted from the FDA’s concern that the TCIs were aggressively and inappropriately marketed as first-line agents for AD and that physicians were using them off-label in children <2 years. In 2004, 13% of all pimecrolimus and 7% of all tacrolimus were administered to children
Rare cases of malignancy, including skin cancer and lymphoma, have been reported, although a causal relationship has not been established.
Long-term safety is not established.
Avoid long-term continuous use in any age group.
Limit application to areas affected with AD.
Only the 0.03% tacrolimus concentration is indicated for 2- to15-year-old children. [FDA Public Health Advisory issued January 19, 2006. [http://www.fda.gov/bbs/topics/news/2006/NEW01299.html]

P E D I A T R I C A T O P I C D E R M A T I T I S
70
カイルパン タラ
non-commercial document; school paperwork
Following the FDA's action, Health Canada issued a “dear doctor” letter to outline these concerns to Canadian healthcare professionals.
Efficacy
Three studies (n=589) showed that 41% of subjects were clear/almost clear after 6 weeks of pimecrolimus (vs. 20% on vehicle).[Eichenfield LF, et al. J Am Acad Dermatol 46(4):495-504 (2002 Apr); Ho VC, et al. J Pediatr 142(2):155-62 (2003 Feb).]
Three weeks of betamethasone valerate 0.1% cream was superior to pimecrolimus (50% vs. 11%, respectively, clear/almost clear).[Luger T, et al. Br J Dermatol 144(4):788-94 (2001 Apr).]
Three studies (n=655) showed 90+% improvement after 12 weeks of tacrolimus 0.1% in 37% and tacrolimus 0.03% in 28% of adults, and 41% and 36% of children (0.1% and 0.03%, respectively) vs. 7% on vehicle.[Hanifin JM, et al. J Am Acad Dermatol 44(1 Suppl):S28-
38 (2001 Jan); Paller A, et al. J Am Acad Dermatol 44(1 Suppl): S47-57 (2001 Jan).]
Tacrolimus 0.1% has similar efficacy to hydrocortisone butyrate (midpotent steroid).[Reitamo S, et al. J Allergy Clin Immunol
109(3):547-55 (2002 Mar).]
Tacrolimus 0.03% and 0.1% are more effective than 1% hydrocortisone ointment.[Reitamo S, et al. J Allergy Clin Immunol 109(3):539-46 (2002 Mar).]
Tacrolimus 0.1% is more efficacious than pimecrolimus 1% in adults (54.1% vs. 34.9% respective reduction in EASI score, p<0.0001) and children (67.2% vs. 56.4% respective reduction, p=0.04) with moderate-tovery severe AD.[Paller AS, et al. J Am Acad
Dermatol 52(5):810-22 (2005 May).]
Tacrolimus 0.03% ointment and pimecrolimus 1% have similar efficacy in children with mild AD (52.1% vs. 42.7% respective reduction in EASI score, p=0.07).[Paller A, et al. J Am Acad Dermatol 44(1 Suppl):S47-57 (2001 Jan).]

P E D I A T R I C A T O P I C D E R M A T I T I S
71
カイルパン タラ
non-commercial document; school paperwork
Treatment with 0.1% tacrolimus ointment over 6 months was shown to be significantly more efficacious than a corticosteroid ointment regimen in adults with moderate-to-severe AD.[Reitamo S, et al. Br J Dermatol 152(6):1282-9 (2005 Jun).
Safety of Calcineurin Inhibitors
Skin burning and pruritus may occur at the start of treatment; typically resolve within the first 2 weeks.
Low blood levels seen in a small minority of patients (not invthe range typically associated with immunosuppression).
High blood levels rarely seen in patients with compromised epidermal barriers, e.g., Netherton syndrome. [Allen A, et al. Arch Dermatol 137(6):747-50 (2001 Jun).Arch Jun).]
Do not cause atrophy, striae, or pigmentation changes (in contrast to topical steroids).
No increase in systemic infections, and no increased risk of malignancy in clinical studies.[FDA Pediatric Advisory Committee. February 15, 2005, Briefing Information. http://www.fda.gov/ohrms/dockets/ac/05/briefing/2005-4089b2. htm.]
The American Academy of Dermatology (AAD) task force found that “there is no causal proof that TCIs cause lymphoma or nonmelanoma skin cancer.”[Berger TG, et al. J Am Acad Dermatol
54(5):818-23 (2006 May).]
Animal studies showed an increase in lymphoma at doses far exceeding those achieved with topical use. The applicability of animal studies to humans is poor due to differences in biology, concomitant exposures, and innate protective mechanisms.[Berger
TG, et al. J Am Acad Dermatol 54(5):818-23 (2006 May).]
The blood concentrations detected in a few patients with AD, including young children with extensive disease, have been insufficient to cause sustained immunosuppression leading to the development of lymphomas.[Bieber T, et al. Dermatology 211(2):77-
8 (2005).]

P E D I A T R I C A T O P I C D E R M A T I T I S
72
カイルパン タラ
non-commercial document; school paperwork
There have been rare spontaneous reports of lymphomas in the >7.5 million patients treated with TCIs, but their histology and clinical presentation are not in keeping with lymphomas occurring in the setting of immunosuppressive therapy.[Ormerod AD. Br J Dermatol 153(4):701-5 (2005 Oct).]
An odds ratio analysis (with a 95% Confidence Interval [CI]) of 293,253 patients with A.D. showed no increased risk of lymphoma in patients treated with TCIs. [Arellano FM, et al. J Invest Dermatol
127(4):808-16 (2007 Apr).]
DNA repair in keratinocytes is inhibited in vitro by TCIs, suggesting a theoretical risk that they might affect local skin carcinogenesis. Clinical evidence is however lacking.[Berger TG, et al. J Am Acad Dermatol 54(5):818-23 (2006 May).]
The AAD task force recommends use in patients at high risk for developing skin cancer (e.g., patients on immunosuppressants, or with xeroderma pigmentosum or nevoid basal cell carcinoma syndrome) only after failure of reasonable alternatives. Broad-spectrum sunscreen should be applied to exposed skin.
The TCI task force of the American College of Allergy, Asthma, and Immunology and the American Academy of Allergy, Asthma, and Immunology concluded that the risk/benefit ratio of TCIs was similar to those of most conventional therapies for chronic relapsing AD. Use in children <2 years of age who require more than emollients might be necessary since most topical steroids and other immunomodulators have not been studied or approved in this age group.[Fonacier L, et al. J Allergy Clin Immunol 115(6):1249-53 (2005 Jun).]
Conclusions
TCIs have an important place in the therapeutic armamentarium for AD. They are approved as second line agents for individuals >2 years of age, and have a good safety profile when used short-term or intermittently long-term. Studies so far have not shown an increase in malignancy in humans, but long-term vigilance is required to ensure that this remains the case.

P E D I A T R I C A T O P I C D E R M A T I T I S
73
カイルパン タラ
non-commercial document; school paperwork
DETERMINING THE SEVERITY OF ATOPIC DERMATITIS
IN CHILDREN PRESENTING IN GENERAL PRACTICE: AN EASY AND FAST METHOD
Authors: Marjolein G. Willemsen,1 Rosalinda W. C. van Valburg,
1 Pauline C. Dirven-Meijer,
2
Arnold P. Oranje,3 Johannes C. van der Wouden,
1 and Heleen Moed
1
1Department of General Practice, Erasmus MC—University Medical Center, Rotterdam,
2General Practice, Renswoude;
3Department of Dermatology and Venereology (Pediatric Dermatology), Erasmus MC
University Medical Center Rotterdam/Sophia Children's Hospital, Rotterdam, The Netherlands Received 9 June 2009; Accepted 10 September 2009
http://www.hindawi.com/journals/drp/2009/357046/
Abstract
Assessment of the severity of atopic dermatitis (AD) is necessary to evaluate the disease process. This study evaluates and validates the TIS in children with AD presenting in general practice. Independent investigators determined the severity of AD using the TIS and the objective SCORAD. The interobserver agreement for the TIS and SCORAD was calculated, as was the correlation TIS and SCORAD. The mean time to assess the TIS was less than one minute. A moderate-to-good agreement between the observers was found for the TIS (κ=0.604 or 0.464), or SCORAD (κ=0.695 or 0.700). There was an excellent correlation between TIS and SCORAD (rs=0.755–0.839). In conclusion, the TIS is an easy and fast method to score AD. Because of the moderate to good interobserver agreement and the high correlation with the SCORAD, we recommend the TIS to determine the severity of AD in general practice.
1. Introduction
It is important to determine the severity of atopic dermatitis (AD) when assessing the course of the disease, for example, before and after treatment [1]. Because there are no serologic markers that accurately reflect AD, measurements and severity are primarily based on signs and symptoms [2]. Valid and reliable clinical outcome measures are prerequisites for evidence-based practice [3].

P E D I A T R I C A T O P I C D E R M A T I T I S
74
カイルパン タラ
non-commercial document; school paperwork
Investigators can currently select from 20 different measurements of AD disease severity. Of these, only the EASI (Eczema Area Severity Index) [4], POEM (patient-oriented eczema measure) [5], and SCORAD (SCORing Atopic Dermatitis) index [6, 7] have been sufficiently validated to recommend their use in clinical trials and everyday practice [8].
The most widely used clinical scoring system is the SCORAD index [7]. The SCORAD index (including six objective items and two subjective issues) or the objective SCORAD (SCORAD from now on, without subjective measures) is an excellent system for clinical trials but is too complicated and time consuming (scoring takes about 7–10 minutes per patient) for a routine clinical setting. For this reason, the Three Item Severity score (TIS), a simplified version of the SCORAD, was developed [1, 9].
The TIS has been tested in a dermatology outpatient department; a high correlation and a moderate-to-fair interobserver agreement were found between the TIS and the SCORAD [9]. The Dutch College of General Practitioners’ guideline on AD recommends treating patients according to the severity of AD [11]. The guideline acknowledges that the value of the TIS has not yet been established in general practice and recommends more research in this area [11].
Therefore, the present study explored whether the TIS is useful in children treated in general practice. For this, we evaluated and validated the TIS, and calculated the interobserver agreement for and the correlation between the TIS and the SCORAD.
2. Materials and Methods
2.1. Patient Selection
This prospective study was conducted in general practices in greater Rotterdam and a regional Child Health Center (Renswoude area) between November 2007 and March 2008. Included were all patients with AD under 7 years of age. The children were selected from the computerized files of general practitioners (GPs). Children were selected either by diagnosis, coded according to the International Classification of Primary Care (ICPC) [12], or by prescribed medication,

P E D I A T R I C A T O P I C D E R M A T I T I S
75
カイルパン タラ
non-commercial document; school paperwork
coded according to the Anatomical Therapeutic Chemical (ATC) classification scheme [13].
Patients were selected using the ICPC code S87 (Atopic Dermatitis), and/or ATC codes for topical treatment of AD (zinc products, soft paraffin, and fat products, other emollients and protectives, tars, topical corticosteroids, all different potencies), and according to the inclusion and exclusion criteria (Table 1).
Table 1: Inclusion and exclusion criteria.
Inclusion criteria Exclusion criteria
Patient selection (computer search)
– Aged 0–6 years – Diagnosis of AD by GP – Had consultation for AD
complaints within last 3 months or repeated their prescriptions for AD treatment in last 3 months
– Chronic disease other than AD, asthma, food intolerance, or allergic rhinitis
– Psychological problems which could influence follow-up
– GP checked the selected patients and could exclude patients
Telephone questionnaire
– AD complaints at time of telephone questionnaire (excoriations and skin lesions)
– Short-term illness at time of telephone questionnaire
– Parent or caretaker unable to read or write Dutch or English
First visit – Informed consent – Diagnosis of AD using
Williams’ criteria [10]
– Other skin conditions precluding proper assessment of AD severity
– Short-term illness
AD: atopic dermatitis, GP: general practitioner.
The study was approved by the ethics committee of Erasmus MC. All parents provided written informed consents to participate in the study.
2.2. Materials
The SCORAD index consists of the interpretation of the extent of the disorder, that is, the intensity, composed of six items (erythema, oedema/papules, effect of scratching, oozing/crust formation, lichenification, and dryness), and two subjective symptoms (itch and sleeplessness) [1]; the maximum score is 103 points (Table 2).

P E D I A T R I C A T O P I C D E R M A T I T I S
76
カイルパン タラ
non-commercial document; school paperwork
Table 2: Classification of the severity of atopic dermatitis for the SCORAD-index, the (objective) SCORAD, and Three Item Severity score (TIS)±.
Instrument Classification of severity of AD
Mild Moderate Severe
SCORAD-index 0–24 25–50 51–103 (Objective) SCORAD
0–14 15–40 41–83/93
TIS 0–2 3–5 6–9
Adapted± from Oranje et al. [1].
In the SCORAD the subjective symptoms (itch and sleeplessness) are not assessed; the total score is 83 points (Table 2) [6]. “Bonus points” for disfiguring lesions or functional limiting lesions will receive 10 extra points (Table 2).
The TIS is the sum of the three items: erythema, oedema, and excoriations (scored on a scale from 0 to 3); each item should be scored on the most representative lesion, that is, a lesion which represents the mean intensity for that item (Table 2) [9]. The TIS items are identical to their SCORAD counterparts.
Two investigators (MW and RVV) were trained by a pediatric dermatologist (APO) to complete the TIS and SCORAD. To assess interobserver variability, both investigators determined the severity of AD in all children simultaneously using the TIS and SCORAD. As a third observer, a GP (PDM) simultaneously scored a subset of patients.
During the examination, the observers scored the severity of AD using first the TIS and then using the SCORAD.
To assess usability of the TIS the observers recorded the time required to assess the total TIS per patient.
All patients were observed at 3- to 4-week intervals, and digital images of the most representative lesions were made in all patients.
Because the symptoms of AD can fluctuate greatly, all the observers examined the patients during the same visit; during each examination, the other observers were in a separate room. The results of each examination were immediately stored in a sealed envelope, ensuring that the other observers were unaware of these

P E D I A T R I C A T O P I C D E R M A T I T I S
77
カイルパン タラ
non-commercial document; school paperwork
results. The envelopes remained sealed until the last observer had examined the patients for the second time.
2.3. Statistical Analysis
The total scores of the TIS and SCORAD were calculated per patient for each observer. The total scores of the TIS (0–9) and the SCORAD (0–83/93) were then categorized into three groups: mild, moderate, and severe. We chose to categorize the scores into these groups since treatment of AD is based on this classification. The scores were categorized as shown in Table 2.
Statistical analysis was performed with SPSS version 15 (SPSS Inc, Chicago) and STATA version 10 (StataCorp, College Station). Interobserver agreement for both the SCORAD and TIS (categorized scores) was calculated using Cohen’s kappa. Agreement for each item separately (lichenification, oozing/crusts, dryness, erythema, oedema/populations, and excoriations) was also calculated using Cohen’s kappa. We consider an agreement between the observers above 0.75 as an excellent agreement and below 0.40 as a poor agreement; results between 0.4 and 0.75 were regarded as fair to good [14]. Agreement regarding the extent of the disease was calculated with the intraclass correlation coefficient (ICC).
The correlation between the TIS and SCORAD (uncategorized scores) was calculated using Spearman’s rank correlation. The correlation between the categorized SCORAD (i.e., classification into mild, moderate, and severe) and categorized TIS was calculated using the ICC. The correlations between SCORAD (the uncategorized scores) and the different items (lichenification, oozing/crusts, dryness, erythema, oedema/papulations, excoriations, and the extent) and between the TIS (the uncategorized scores) and the three items (erythema, oedema/populations, and excoriations) were calculated using Spearman’s rank correlation.

P E D I A T R I C A T O P I C D E R M A T I T I S
78
カイルパン タラ
non-commercial document; school paperwork
3. Results
3.1. Study Population
A total of 45 GPs agreed to participate in the study. A total of 278 patients with an age below 7 years and with a history of AD (ICPC S87) or use of medical treatment for AD were selected in the database of the GP. These selected patients were invited by mail to participate. Of these, 89 had self-reported complaints of AD at the moment and were willing to participate. Finally 66 patients were included in the study. Twenty three children were excluded for the following reasons: 12 had no AD complaints at the time of inclusion, 3 parents were unable to fill in the consent forms and another 8 were excluded because their answer forms were received after the inclusion period had closed. Thus, the final study population consisted of 66 patients (57.6% girls, mean age of 31 months—range 0.5–83 months). Of these, 50 were examined by two observers and 16 by three observers. All 66 patients were available for the first visit, and 65 patients were observed during the second visit.
3.2. Severity of AD
The mean TIS scores were 2.1 (SD=1.1, determined at the first visit) and 1.8 (SD=1.0, at the second visit). The mean SCORAD scores were 13.5 (SD=8.7) at the first visit and 11.9 (SD=7.8) at the second visit. The severity of AD was predominantly mild, accounting for 73% of the cases according to the TIS (score 0–2) and for 70% of the cases according to the SCORAD (0–14). Moderate AD accounted for 24.6% according to the TIS (score 3–5) and for 27.6% according to the SCORAD (score 15–40). Severe AD accounted for 2.4% in both scoring systems.
3.3. Evaluation of the TIS and SCORAD
The mean time to assess the TIS per patient was 43 seconds (range 7–170). Moderate-to-good interobserver agreement (weighted κ=0.604 for visit 1 and 0.464 for visit 2) was found between the two observers for the categorized TIS (i.e., severity classified into mild,

P E D I A T R I C A T O P I C D E R M A T I T I S
79
カイルパン タラ
non-commercial document; school paperwork
moderate, and severe). Similar results were found in a smaller group where patients were observed by three observers (Table 3).
Table 3: Interobserver agreement for the TIS (categorized into mild, moderate, or severe).
First visit (n=66) Second visit (n=65)
Observer 1 versus 2 κ=0.562 κ=0.464
Weighted κ=0.604 Weighted κ=0.464
First visit (n=16) Second visit (n=15)
3 observers κ=0.758 κ=0.481
For the SCORAD (categorized into mild, moderate, and severe) the interobserver agreement also showed a good agreement (κ=0.665 for first visit and κ=0.776 for second visit).
3.4. Correlation between the TIS and SCORAD
We calculated the correlation between the TIS and SCORAD. For all three observers for both visits, a good correlation was found between the two scoring methods (Table 4, Figures 1(a) and 1(b)). The correlation between the categorized TIS (i.e., severity classified into mild, moderate, and severe, Table 2) and categorized SCORAD (same classification) was also good or excellent for all observers at both visits (rs=0.637 to 0.985; P=.01; ICCs 0.622 to 0.933).
Table 4: Correlation between TIS and SCORAD.
First visit (n=66) Second visit (n=65)
Observer 1; TIS versus SCORAD rs=0.807 (P=.01) rs=0.755 (P=.01)
Observer 2; TIS versus SCORAD rs=0.791 (P=.01) rs=0.839 (P=.01)
First visit (n=16) Second visit (n=15)
Observer 3; TIS versus SCORAD rs=0.809 (P=.01) rs=0.791 (P=.01)
rs, Spearman’s rank.

P E D I A T R I C A T O P I C D E R M A T I T I S
80
カイルパン タラ
non-commercial document; school paperwork
Figure 1: Correlation between TIS and SCORAD. Observations from the two independent observers (obs 1 and 2) are displayed in one figure ((a)
first visit, (b) second visit).

P E D I A T R I C A T O P I C D E R M A T I T I S
81
カイルパン タラ
non-commercial document; school paperwork
3.5. Correlation between Separate Intensity Items and TIS or SCORAD
The correlation between the TIS and the separate intensity items (erythema, oedema, and excoriations) was calculated. For all observers, all intensity items correlated well with the TIS (rs 0.611–0.980 for erythema; 0.604–0.838 for oedema; 0.639–0.860 for excoriations). The items erythema, oedema, and excoriations also correlated well with the SCORAD for all observers (rs from 0.495 to 0.826). Regarding the other items of the SCORAD, the items dryness and extent showed a moderate-to-good correlation with the SCORAD for all observers (rs 0.324 to 0.855 for dryness and 0.697 to 0.963 for extent). Only the items oozing/crusts and lichenification showed a weak correlation with the SCORAD (rs from 0.197 to 0.638).
3.6. Interobserver Agreement on Separate Intensity Items
The interobserver agreement for the separate intensity items showed highly variable kappa values. Only the item “erythema” showed a fair-to-good agreement between the observers (κ=0.603 or 0.621). Also a good agreement for the item “extent” (item A of the SCORAD) was found between the observers (ICC 0.761 and 0.857, for visit 1 and 2, resp.).
4. Discussion
In the present study a moderate-to-good interobserver agreement was found between the observers for the TIS. The overall agreement between observers was sufficiently good to recommend use of the TIS to assess the severity of AD in general practice. The TIS is a simple method to determine the severity of AD, and assessment of the total TIS took about 43 seconds per patient. Therefore, the TIS is suitable for use in daily practice. Because a good correlation was found between the TIS and the different intensity items, we conclude that these items (erythema, oedema, and excoriations) are suitable determinants to evaluate the severity of AD with the TIS.

P E D I A T R I C A T O P I C D E R M A T I T I S
82
カイルパン タラ
non-commercial document; school paperwork
In accordance with other studies [1, 9], we found a good correlation between the TIS and SCORAD. The classification of the severity of AD into mild, moderate, and severe also showed good correlations, but were lower than the uncategorized scores. A possible explanation is that these categorized scores were rearranged on an arbitrary line. Thereby, some patients had a difference of only one point between the two observers on the TIS, but were placed in a different category (mild, moderate, or severe). When the patient scores were uncategorized, these minor differences between the observers had no influence on the calculated correlation; therefore, these correlation scores are higher. The high correlation between TIS and SCORAD is not surprising, because the TIS is a simplified version of the SCORAD.
For the SCORAD, a good interobserver agreement was found between all observers. Similar to clinical trials in which good interobserver agreement for the SCORAD has been established [1, 9], the SCORAD also showed good agreement in our general practice patients. We conclude that, although SCORAD is an effective scoring system and is suitable to determine the severity of AD in clinical trials, it is too extensive and time consuming for use in daily care in general practice.
Because the items erythema, oedema, and excoriations correlated well with the SCORAD, we conclude that implementing these items in the TIS is a feasible choice.
The interobserver agreement between the different intensity items showed a wide range of differences, therefore these items alone cannot be used to determine the severity of AD.
In contrast to previous studies [6, 15], the item “extent” (of the SCORAD) showed good agreement between all our observers. Furthermore, we found a good correlation between the SCORAD and the item “extent.” An explanation for this good correlation could be the fact that children who visit a GP for their eczema in general have a mild form of eczema. The extent of this mild form is easier to score, since it is all in the same (low) range. The extent of AD is not assessed in the TIS; its addition could provide additional information about the severity of AD in children who visit the GP for eczema.

P E D I A T R I C A T O P I C D E R M A T I T I S
83
カイルパン タラ
non-commercial document; school paperwork
4.1. Limitations of the Present Study
A weakness of this study is that, because we included patients who had already received treatment for AD, the severity of their AD was probably diminished at the time of the first visit (several days/weeks after the visit to the GP). Nevertheless, when comparing AD complaints assessed during the first and second visit, a decrease in these complaints was observed at the second visit. This indicates that AD complaints during the first visit were determined during a period with fair complaints of AD.
Because of the mild distribution of the severity of AD in our study population, it is difficult to predict whether our results (e.g., interobserver agreements and correlations) are comparable with results in other populations. The interobserver agreement between the three observers was only available for a relatively small sample; therefore, these results should be considered with caution. The interobserver agreement between the two observers could be calculated for a much larger sample size.
4.2. Conclusion
In conclusion, the TIS is an easy and fast scoring system. Because of the moderate-to-good interobserver agreement and the high correlation with the SCORAD, we recommend that the TIS be used to determine the severity of AD in general practice.
REFERENCES 1. A. P. Oranje, E. J. Glazenburg, A. Wolkerstorfer, and F. B. de Waard-van der Spek, “Practical
issues on interpretation of scoring atopic dermatitis: the SCORAD index, objective SCORAD and the three-item severity score,” British Journal of Dermatology, vol. 157, no. 4, pp. 645–648, 2007.
2. A. Y. Finlay, “Measurement of disease activity and outcome in atopic dermatitis,” British Journal of Dermatology, vol. 135, no. 4, pp. 509–515, 1996.
3. M.-M. Chren, “Giving “scale” new meaning in dermatology: measurement matters,” Archives of Dermatology, vol. 136, no. 6, pp. 788–790, 2000.
4. J. M. Hanifin, M. Thurston, M. Omoto, et al., “The eczema area and severity index (EASI): assessment of reliability in atopic dermatitis,” Experimental Dermatology, vol. 10, no. 1, pp. 11–18, 2001.
5. C. R. Charman, A. J. Venn, and H. C. Williams, “The patient-oriented eczema measure: development and initial validation of a new tool for measuring atopic eczema severity from the patients' perspective,” Archives of Dermatology, vol. 140, no. 12, pp. 1513–1519, 2004.

P E D I A T R I C A T O P I C D E R M A T I T I S
84
カイルパン タラ
non-commercial document; school paperwork
6. B. Kunz, A. P. Oranje, L. Labrèze, J.-F. Stalder, J. Ring, and A. Taïeb, “Clinical validation and guidelines for the SCORAD index: consensus report of the European Task Force on Atopic Dermatitis,” Dermatology, vol. 195, no. 1, pp. 10–19, 1997.
7. C. Charman, C. Chambers, and H. Williams, “Measuring atopic dermatitis severity in randomized controlled clinical trials: what exactly are we measuring?” Journal of Investigative Dermatology, vol. 120, no. 6, pp. 932–941, 2003.
8. J. Schmitt, S. Langan, and H. C. Williams, “What are the best outcome measurements for atopic eczema? A systematic review,” Journal of Allergy and Clinical Immunology, vol. 120, no. 6, pp. 1389–1398, 2007.
9. A. Wolkerstorfer, F. B. de Waard-van der Spek, E. J. Glazenburg, P. G. H. Mulder, and A. P. Oranje, “Scoring the severity of atopic dermatitis: three item severity score as a rough system for daily practice and as a pre-screening tool for studies,” Acta Dermato-Venereologica, vol. 79, no. 5, pp. 356–359, 1999.
10. H. C. Williams, P. G. J. Burney, A. C. Pembroke, and R. J. Hay, “The U.K. working party's diagnostic criteria for atopic dermatitis. III. Independent hospital validation,” British Journal of Dermatology, vol. 131, no. 3, pp. 406–416, 1994.
11. J. P. Cleveringa, P. C. Dirven-Meijer, G. Harteveld-Faber, M. M. G. Nonneman, P. Weisscher, and F. S. Boukes, “NHG-standaard constitutioneel eczeem: eerste herziening,” Huisarts en Wetenschap, vol. 49, no. 9, pp. 458–465, 2006.
12. H. Lamberts and M. Wood, International Classification of Primary Care, Oxford University Press, New York, NY, USA, 1987.
13. WHO, “WHO collaborating centre for drug statistics methodology,” ATC/DDD Index 2007, http://www.whocc.no/atcddd.
14. J. L. Fleiss, Statistical Methods for Rates and Proportions, John Wiley & Sons, New York, NY, USA, 2nd edition, 1981.
15. C. R. Charman, A. J. Venn, and H. C. Williams, “Measurement of body surface area involvement in atopic eczema: an impossible task?” British Journal of Dermatology, vol. 140, no. 1, pp. 109–111, 1999.

P E D I A T R I C A T O P I C D E R M A T I T I S
85
カイルパン タラ
non-commercial document; school paperwork
ATOPIC DERMATITIS SEVERITY AND SKIN BARRIER FUNCTION LINKED TO LOW
γ-LINOLENIC ACID EDITOR: Joyce A. Nettleton, D.Sc., Nutrition Scientist and Communications Professional
specializing in seafood nutrition and omega-3 fatty acids; Consultant practictioner Last Updated: June 2008
http://www.fatsoflife.com/article.php?nid=1&edition=&id=578&issueid=65
The complexity of atopic dermatitis, an allergic skin disease, has made it especially difficult to find effective treatments and prevention strategies. Atopic dermatitis involves interactions among environmental, genetic, immunologic, biochemical and dietary factors. It has been known
for many years that polyunsaturated fatty acid (PUFA) metabolism is perturbed in patients with atopic dermatitis, although findings are inconsistent and appear to be associated with immunoglobulin E (IgE) levels. A frequent observation is increased concentrations of linoleic acid and reduced levels of γ-linolenic acid, the first desaturation product of linoleic acid. Studies providing γ-linolenic acid to patients with the condition have reported improved outcomes. Reduction in long-chain omega-3 PUFAs (n-3 LC-PUFAs) has been reported in atopic dermatitis, but trials in which exposure to n-3 LC-PUFAs was increased have reported only modest results, if any.
Phospholipids of the epidermis are significantly increased in the condition, with a notable decrease in omega-6 (n-6) PUFAs, especially arachidonic acid. Free arachidonic acid concentrations in epidermis, however, are significantly elevated, suggesting an abnormality in transformation of phospholipids to other lipid classes. Arachidonic acid serves as a substrate for cyclooxygenase and lipoxygenase

P E D I A T R I C A T O P I C D E R M A T I T I S
86
カイルパン タラ
non-commercial document; school paperwork
enzymes whose products, prostaglandin E2 and leukotriene B4 are elevated. In contrast to these inflammatory derivatives, lipoxins derived from arachidonic acid and n-3 LC-PUFAs have potent anti-inflammatory and anti-proliferative effects.
Another consequence of abnormal n-6 PUFA metabolism is impaired water barrier function of the skin. This abnormality is also characteristic of essential fatty acid deficiency, as described in the 1950s by Hugh Sinclair. Defective skin permeability contributes to the pathogenesis of atopic dermatitis and correlates with disease severity and sensitization to aeroallergens. Arachidonic acid and its oxygenated derivatives are also needed for water barrier formation and healthy skin. The biosynthesis of free ceramides and the concentrations of fatty acids of more than 25 carbons are also significantly decreased in atopic dermatitis and these aberrations contribute to impaired epidermal barrier function. A report in elderly volunteers found that the consumption of borage oil providing 360 or 720 mg/day of γ-linolenic acid was associated with improved epidermal barrier function, reduced itch and an 11% decrease in transepidermal water loss.
In the observational studies described here, investigators examined the skin barrier function in children with atopic dermatitis and compared the findings with children having other atopic diseases and with nonatopic controls. Chiung-Hui Yen and colleagues at the National Taiwan University compared different groups of children and adolescents who had atopic diseases—dermatitis, asthma or rhinitis—with non-atopic controls for their serum fatty acids, severity of dermatitis and transdermal water loss. All patients had serum IgE levels greater than 150 U/mL. Recently published reference values (95th percentile) for non-smoking adults are 148 and 169 U/mL for women and men, respectively. Severity of dermatitis was scored by a single dermatologist, according to the Scoring Atopic Dermatitis (SCORAD) criteria developed in 1993 by the European Task Force on Atopic Dermatitis. Participants included 101 young people aged 2 to 17 years, 35 with atopic dermatitis, 35 with either atopic asthma or rhinitis, and 31 nonatopic controls. Fourteen dermatitis patients had SCORAD levels of at least 50, where the maximum score is 103. The

P E D I A T R I C A T O P I C D E R M A T I T I S
87
カイルパン タラ
non-commercial document; school paperwork
SCORAD index is based on the extent, intensity and subjective symptoms of the patient’s lesions.
Serum fatty acid analyses
documented no significant
differences among the groups in linoleic or arachidonic acid concentrations. Both groups of atopic patients had significantly lower concentrations of γ-linolenic acid and
dihomo-γ-linolenic acid compared with
controls, but there was no significant difference in these fatty acids between atopic dermatitis patients and those with either asthma or rhinitis (Figure). Differences in these fatty acid levels between the asthma or rhinitis patients and controls, while lower, did not reach significance.
Transepidermal water loss was assessed on the right volar (palm side) forearm in patients with atopic dermatitis using a Tewameter TM 300 instrument and expressed as loss of water in g/m2/hr. Significant inverse associations were observed between transepidermal water loss and serum γ-linolenic acid
and its derivative, dihomo-γ-linolenic acid and between SCORAD assessments and both fatty acids. Thus, water loss and clinical severity were lowest in dermatitis patients with the highest levels of these two n-6 PUFAs. Arachidonic acid concentration was unrelated to these parameters. Regrettably, the investigators did not report the serum concentrations of n-3 PUFAs.

P E D I A T R I C A T O P I C D E R M A T I T I S
88
カイルパン タラ
non-commercial document; school paperwork
Jayanta Gupta and colleagues at the University of Cincinnati College of Medicine, USA, investigated the disease severity and skin barrier function in African-American and Caucasian children with atopic dermatitis. They report that children with atopic dermatitis have inherently compromised skin barrier function as assessed by the Tewameter TM 300 device and that epidermal water loss was related to the severity of the disease assessed using SCORAD. Children with asthma or rhinitis did not have impaired skin barrier function.
These studies support the view that impaired skin permeability is a primary characteristic of atopic dermatitis. It is directly linked to studies more than 50 years ago on the importance of essential fatty acids in maintaining the epidermal permeability barrier. Reductions in skin barrier function exacerbate atopic dermatitis, undermine protection from ultraviolet light and interfere with the skin’s antimicrobial function. How to harness the importance of PUFAs in alleviating atopic dermatitis, however, remains elusive.
REFERENCES
Yen CH, Dai YS, Yang YH, Wang LC, Lee JH, Chiang BL. Linoleic acid metabolite levels and transepidermal water loss in children with atopic dermatitis. Ann Allergy Asthma Immunol 2008;100:66-73. [PubMed]
Gupta J, Grube E, Ericksen MB, Steveneson MD, Lucky AW, Sheth AP, Assa’ad AH, Jhurana Hersehy GK. Intrinsically defective skin barrier function in children with atopic dermatitis correlates with disease severity. J Allergy Clin Immunol 2008;121:725-730.e2. [PubMed]

P E D I A T R I C A T O P I C D E R M A T I T I S
89
カイルパン タラ
non-commercial document; school paperwork
ATOPIC DERMATITIS PATHOPHYSIOLOGY: GENETIC FACTORS Author: Astellas Pharma Europe LTD.
Last Updated: February, 2010 http://www.epgonline.org/page.cfm/pageId/2620/type/print/
Atopic dermatitis has strong familial associations, and the risk of developing the disease is nearly doubled in children with affected parents. Twin studies have shown that if one monozygotic twin has atopic dermatitis, the chance of the other twin having the condition is approximately 86%, compared with 21% between dizygotic twins.1
These findings demonstrate that the inheritance of specific susceptibility genes can predispose individuals towards developing atopic dermatitis. Genetic predisposition to a disease occurs when a specific genetic variation leads to altered biological responses resulting in either susceptibility to the condition or changes in how the body responds to the condition. In the case of atopic dermatitis, candidate genes have been located on a number of chromosomes.1,2,3
A list of these genes, and their associated clinical phenotype, is presented in the table. As research into the underlying genetic susceptibility continues, this list is likely to increase.
In addition to the direct effects of susceptibility genes, interactions between the genetic traits and the surrounding environment can increase the chances of developing atopic dermatitis and exacerbate the severity of the symptoms. For example, children with loss-of-function mutations in the FLG gene were statistically more likely to develop atopic dermatitis when exposed to cats from birth. Loss-of-function FLG mutations alone are sufficient to predispose infants to atopic

P E D I A T R I C A T O P I C D E R M A T I T I S
90
カイルパン タラ
non-commercial document; school paperwork
dermatitis4; however, the risk of developing the disease increases significantly when combined with exposure to cat allergens.5
TABLE: Susceptibility genes involved in atopic dermatitis.1,2,3
Gene Gene product Associated phenotype
FLG profilaggrin Extrinsic atopic dermatitis, early onset of atopic dermatitis
SPINK5 LETKI atopic dermatitis
TLR 2 Toll-like receptor-2 Severe atopic dermatitis with elevated IgE
TLR 9 Toll-like receptor-9 Intrinsic atopic dermatitis
IRF 2 IFN regulatory factor 2 atopic dermatitis (found in Japanese children)
GM-CSF GM-CSF Prevention of severe symptoms in atopic dermatitis patients
MS4A 2 FCεR1β atopic dermatitis
TGFβ1 Transforming Growth Factor β
atopic dermatitis in children
IL3 IL-3
IL4 IL-4 atopic dermatitis
IL12 IL12 Susceptibility to atopic dermatitis
IL13 IL13 atopic dermatitis with elevated total serum IgE
IL 18 IL18 atopic dermatitis
ILRA IL-4 receptor α chain Adult atopic dermatitis
STAT6 Signal transducer and activator of transcription 6
Elevated serum IgE
PFH11 Plant homology domain finger protein 11
Childhood atopic dermatitis with elevated total serum IgE
REFERENCES 1. Bowcock AM, Cookson WO. The genetics of psoriasis, psoriatic arthritis and atopic dermatitis.
Hum Mol Genet 2004; 13 Spec No 1: R43-55. 2. Maintz L, Novak N. Getting more and more complex: the pathophysiology of atopic eczema.
Eur J Dermatol 2007; 17: 267-83. 3. Ekelund E, Saaf A, Tengvall-Linder M, et al. Elevated expression and genetic association links
the SOCS3 gene to atopic dermatitis. Am J Hum Genet 2006; 78: 1060-5. 4. Sandilands A, O'Regan GM, Liao H, et al. Prevalent and rare mutations in the gene encoding
filaggrin cause ichthyosis vulgaris and predispose individuals to atopic dermatitis. J Invest Dermatol 2006; 126: 1770-5.
5. Bisgaard H, Simpson A, Palmer CN, et al. Gene-environment interaction in the onset of eczema in infancy: filaggrin loss-of-function mutations enhanced by neonatal cat exposure. PLoS Med 2008; 5: e131.

P E D I A T R I C A T O P I C D E R M A T I T I S
91
カイルパン タラ
non-commercial document; school paperwork
LOWER OCCURRENCE OF ATOPIC DERMATITIS
IN CHILDREN WHOSE MOTHERS WERE EXPOSED TO FARM ANIMALS AND CATS DURING PREGNANCY
editorial adaptations by ScienceDaily staff; materials provided by University of Zurich http://www.sciencedaily.com/releases/2010/12/101202124215.htm
Last Updated: December 5, 2010
ScienceDaily (Dec. 5, 2010) — Atopic dermatitis (also known as atopic eczema) is a chronic and extremely painful inflammation of the skin that frequently occurs in early childhood, generally starting in infancy. Up to 20 percent of all children in industrialized countries are affected, making it one of the most common childhood skin diseases.
The need to better understand this disease is all the greater considering the suffering it causes in small children. Atopic dermatitis is, however, an allergic condition and all allergic reactions result from complex interactions of genetic and environmental factors on the immune system. Earlier research has already indicated that allergies are less common in children who grow up on farms and whose mothers live on farms during their pregnancy. Exposure to farm animals and bacteria frequently found in farms as well as drinking milk from the dairy offer the immune system protection. However, proof of this protective effect in connection with atopic dermatitis has remained elusive.
Now, the Journal of Allergy & Clinical Immunology (JACI) has published a study by Caroline Roduit from the research team of Roger Lauener, University of Zurich. The study analyzes how prenatal environmental factors and genetic mechanisms influence the development of atopic dermatitis during the first two years of life. The authors of the study examined children in rural areas of five European countries: Austria, Finland, France, Germany and Switzerland. Of the 1,063 children taking part in the study, 508 were from families that lived on farms, 555 were not farm children.

P E D I A T R I C A T O P I C D E R M A T I T I S
92
カイルパン タラ
non-commercial document; school paperwork
The researchers were able to demonstrate that women who spend their pregnancy in the proximity of farm animals and cats have children with a reduced risk of developing atopic dermatitis in their first two years of life. The research team also identified two genes in these children that are of vital importance for innate immunity and was able to link the expression of these genes to a lower likelihood of a doctor diagnosis of an allergic condition. The findings of the study are not only significant in the face of the frequency of the disease and the suffering it causes: They also support the theory that gene-environment interaction with the developing immune system influences the development of atopic dermatitis in young children.
REFERENCE 1. Caroline Roduit, Johanna Wohlgensinger, Remo Frei, Sondhja Bitter, Christian Bieli, Susanne
Loeliger, Gisela Büchele, Josef Riedler, Jean-Charles Dalphin, Sami Remes. Prenatal animal contact and gene expression of innate immunity receptors at birth are associated with atopic dermatitis. Journal of Allergy and Clinical Immunology, 2010; DOI: 10.1016/j.jaci.2010.10.010

P E D I A T R I C A T O P I C D E R M A T I T I S
93
カイルパン タラ
non-commercial document; school paperwork
NOT EVERY CHILD WITH ATOPIC DERMATITIS NEEDS ALLERGY TESTING
Author: American Academy of Dermatology Last Updated: October, 2010
http://www.skincarephysicians.com/eczemanet/allergy_testing.html
The role that allergy testing plays in managing atopic dermatitis is often confusing. Allergies can trigger atopic dermatitis, so parents frequently ask if their child should have allergy tests. Concerned parents often believe that if only the allergies could be identified, the child could avoid the allergens. This, in turn, would bring much-needed relief.
The truth is no one thing — not even allergen avoidance — can control atopic dermatitis. Successfully managing this complex condition requires a multi-faceted approach. Proper skin care, using medication as directed, and avoiding common skin irritants such as wool clothing all play a role. For most patients, sticking to this plan keeps atopic dermatitis under control.
Who May Benefit from Allergy Testing
For patients with severe atopic dermatitis and those whose condition seems resistant to treatment, allergy testing can be beneficial. An estimated one-third of patients with atopic dermatitis have food allergies. For a few of these patients, eating foods to which they are allergic causes eczema to flare. Why this happens is not entirely clear, but research shows that it most commonly occurs in infants and patients with severe disease.
Types of Allergy Tests
To identify allergens, a doctor takes a complete medical history and orders appropriate allergy tests. When the doctor suspects an

P E D I A T R I C A T O P I C D E R M A T I T I S
94
カイルパン タラ
non-commercial document; school paperwork
allergy caused by food or something in the environment, one of the following tests may be ordered. An allergist generally performs these tests:
Blood test – When an allergic reaction occurs, specific antibodies appear in the blood. This test, called a RAST test, measures antibodies associated with allergic reactions.
Skin prick test – Also called the scratch test, this is the most common allergy test. It involves placing a small amount of suspected allergens on the patient’s skin, often on the forearm or back. The skin is then scratched or pricked so that the each substance can get beneath the skin. Allergic reactions develop within 15 to 20 minutes. If a reaction occurs, the skin tends to itch and the area may swell or turn red.
Another type of allergy test is used to detect cutaneous allergens (substances that cause an allergic reaction on the skin). Called a patch test, it is usually performed by a dermatologist. As the name implies, this test requires the patient to wear a type of patch on the skin. Each patch, also called a panel, contains a number of common allergens. The patient usually wears the panel(s) for 48 hours, returning once before the 48-hour period for an initial reading. The second reading is usually taken at 48 hours. During each visit, the dermatologist evaluates the reactions on the skin.
Test Results Can Be Misleading
Results that indicate food allergies can be especially misleading. While a negative result provides strong evidence that the child is not allergic to a food, false positive results are common. Dermatologists also find that while the test can indicate a food allergy, eating the suspect food usually does not cause the child’s eczema to flare.
The only reliable way to find out if a food actually causes the eczema to flare is to perform a food challenge test. This requires

P E D I A T R I C A T O P I C D E R M A T I T I S
95
カイルパン タラ
non-commercial document; school paperwork
the child to eat the suspect food while being observed by a medical professional. If the child develops signs of eczema — redness, papules, and wheals — or has increased and widespread itch within 2 hours of eating the food, the test concludes that the food causes eczema to flare.
Study after study finds that this reaction is exceeding rare. Even children hospitalized for severe and recalcitrant atopic dermatitis seldom test positive when given a food challenge test. A study conducted in Oregon found only 1 positive food challenge in 17 children hospitalized due to severe atopic dermatitis that had not responded to treatment.
In all, 58 food challenges were performed. The foods tested were those most commonly associated with food allergies — eggs, milk, wheat, and soy. Nuts were not tested because life-threatening allergic reactions can occur. The study concluded that while food allergies are common in patients with atopic dermatitis, eating foods to which they are allergic rarely causes atopic dermatitis to flare. This finding has been observed in similar studies.
Another study suggests that even in children who have food allergies, relief comes from caring for the child’s skin. This study found that when children with moderate to severe atopic dermatitis received long-term — at least 3 months — treatment with tacrolimus ointment, the severity of the eczema decreased significantly. With the eczema under control, the number of parents who reported that the eczema worsened after the child ate certain foods also decreased. Parents concerns about food allergy also declined dramatically. The researchers attributed these changes to better control of the atopic dermatitis.
Skin Care Plays Central Role
Most dermatologists advise parents to focus on caring for the child’s skin. Follow your dermatologist’s skin care guidelines, use medication as directed, and help the child avoid common triggers such as becoming overheated. If these fail to control the child’s atopic dermatitis, then it is time to ask about allergy testing.

P E D I A T R I C A T O P I C D E R M A T I T I S
96
カイルパン タラ
non-commercial document; school paperwork
REFERENCES:
1. Halbert AR, Weston WL, Morelli JG. Atopic dermatitis: is it an allergic disease? Journal of the American Academy of Dermatology 1995; 33: 1008-18.
2. Kerschenlohr K, Darsow U, Burgdorf WH et al. Lessons from atopy patch testing in atopic dermatitis.Current Allergy and Asthma Reports 2004; 4: 285-9.
3. Rowlands D, Tofte SJ, Hanifin JM. Does food allergy cause atopic dermatitis? Food challenge testing to dissociate eczematous from immediate reactions. Dermatologic Therapy 2006; 19: 97-103.
4. Thompson MM, Hanifin JM. Effective therapy of childhood atopic dermatitis allays food allergy concerns.Journal of the American Academy of Dermatology 2005; 53: S214-9.
5. Tofte SJ, Hanifin JM. Current management and therapy of atopic dermatitis. Journal of the American Academy of Dermatology 2001; 44: S13-6.

P E D I A T R I C A T O P I C D E R M A T I T I S
97
カイルパン タラ
non-commercial document; school paperwork
COMPLICATIONS OF ATOPIC DERMATITIS
Author: Dr Amy Stanway, Department of Dermatology, Health Waikato Last Updated: December 24, 2007
http://www.dermnetnz.org/dermatitis/pdf/atopicdermatitiscomplications- dermnetnz.pdf
Psychosocial aspects
Any chronic illness can have a major impact on the sufferer's life, and this is particularly so for childhood eczema, as well as on the lives of their families. Most people with eczema continue to lead normal lives but for a few, the eczema can be a source of major psychosocial distress.
Young children often suffer sleep disturbances which are difficult for parents and may cause behavioural problems in the child. Older children may become shy and withdrawn due to the embarrassment of a visible skin condition. Activities such as sport, school camps and swimming may have to be restricted, which further alienates the child. Long absences from school may result from both the eczema itself, and from the social avoidance that develops in some children.
Adults may also suffer shyness and withdrawal due to the appearance of the eczema. Work may be difficult and some people with bad eczema will have to change jobs to cope with their eczema.
Retarded growth
Severe eczema may slow the growth rate in children. This is most often due to the eczema rather than itstreatment. Corticosteroids, particularly oral corticosteroids, can also cause short term growth retardation, so use of these drugs is closely monitored.

P E D I A T R I C A T O P I C D E R M A T I T I S
98
カイルパン タラ
non-commercial document; school paperwork
Bacterial infections
Bacterial infection is extremely common in atopic dermatitis. This is usually with staphylococcal or streptococcal bacteria (see staphylococcal skin infections and streptococcal skin infections). People who have atopic dermatitis are particularly prone to skin infections. This is in part due to the breaks in the skin from very dry, split skin and from scratching the itchy areas. People with atopic dermatitis also seem to have a reduced ability to fight against these common bacteria on the skin. As a result people with atopic dermatitis frequently suffer from boils, folliculitis and infections of their eczema. This begins a viscious cycle as infection causes the eczema to worsen and become more resistant to the usual treatment with emollients and topical steroids. Antibiotics are often required to eliminate the infection before the eczema can once more be brought under control.
Rarely, bacterial infection can be especially severe, involving much of the skin surface. This can cause blood poisoning (septicaemia) and require hospital admission. Infants are particularly at risk of severe skin infections.
Staphylococcal Infection in Atopic Dermatitis
Viral infections
Viral infections, in particular herpes simplex virus (the virus that causes cold sores and genital herpes), is more common in patients with atopic dermatitis. A herpes simplex infection can spread rapidly in the presence of eczema and cause a severe infection known as eczema herpeticum. This may present as a generalised illness with fever, malaise and a widespread crusted, blistering rash. It can also be more localised, often confined to areas with active eczema. A

P E D I A T R I C A T O P I C D E R M A T I T I S
99
カイルパン タラ
non-commercial document; school paperwork
history of a recent coldsore in the affected individual or a close contact is useful in making the diagnosis before swab results become available. Because of the severity of the condition, treatment with oral antiviral agents such as aciclovir is often started before any swab results are available.
Eczema Herpeticum
Molluscum contagiosum is another common viral skin infection, seen particularly in children. It may be more common in people with atopic dermatitis. Molluscum infection often causes an increase in eczema symptoms, usually worst around the areas affected with molluscum. Molluscum lesions often resolve more slowly in people with atopic dermatitis and the eczema may continue to be more active until the molluscum finally disappears.
Resolution can be hastened by mild traumatising of one or two molluscum lesions at a time to generate an inflammatory response. This can be done by quick pinching with clean tweezers of one or two lesions each night for a few nights. This is usually better tolerated if done while the child is asleep.
Molluscum Contagiosum

P E D I A T R I C A T O P I C D E R M A T I T I S
100
カイルパン タラ
non-commercial document; school paperwork
Erythroderma
Erythroderma is a generalised redness of the skin. It is a very severe skin condition that can be fatal. It is caused by a number of conditions including eczema, psoriasis, other inflammatory skin conditions, drugs and malignancies.
Erythrodermic eczema usually occurs in patients with worsening or unstable eczema. Treatment of erythroderma is similar despite the many underlying causes. Inpatient hospital treatment is usually required to cool the skin and support the hydration and temperature control of the affected individual. Skin infection is also common in the setting of erythrodermic eczema and intravenous antibiotics are commonly given for a period of time. Treatment for erythrodermic eczema may include:
Hospitalisation for supportive care including intravenous fluids and temperature regulation
Bland emollients and cooling wet dressings
Bed rest
Topical steroids
Antibiotics
Treatment of complications (or example diuretics (water tablets), nutritional support)
Treatment with wet wraps, emollients and topical steroids, and bed rest results in rapid improvement in the majority of affected individuals. Early treatment leads to a better outcome.
Complications of erythroderma include:
Dehydration
Heart failure
Infection
Hypothermia
Protein loss and malnutrition
Oedema (swelling)
Death
Eye abnormalities

P E D I A T R I C A T O P I C D E R M A T I T I S
101
カイルパン タラ
non-commercial document; school paperwork
Many eye changes may be seen in association with atopic dermatitis. A Dennie-Morgan fold is a fold of skin under the lower eyelid. It is often seen in atopic dermatitis but may also be seen independent of atopic dermatitis and is of no significance to the overall health of the person.
Conjunctival irritation is also common. It may be due to an allergic reaction, as in hayfever, or an irritant response.
Keratoconus (conical-shaped eyeball) is a rare condition which is occasionally associated with atopic dermatitis. It is due to degeneration and weakening of the cornea (the front of the eye) which results in pushing of the front of the eye outwards due to the normal pressure within the eyeball. It can result in marked visual disturbances and can be partially corrected by contact lenses. Onset of keratoconus is after childhood and progression is usually self-limited.
Cataracts can also occur in association with severe atopic dermatitis, usually around 15-25 years of age. They are almost always bilateral and may have a characteristic appearance on eye examination which helps distinguish them from other causes of cataract.
Retinal detachment is when part of the inner eye lining breaks away from the underlying structures. This is a very rare complication seen in association with atopic dermatitis.
REFERENCES
On DermNet NZ: Atopic dermatitis; Causes of atopic dermatitis; Treatment of atopic dermatitis; Dermatitis
Other websites: Atopic dermatitis – emedicine dermatology, the online textbook