26
w w w .f u t u r e - d r u g s .c o m 39 10.1586/14737175. 8.3.397 © 2008 Future Drugs Ltd ISSN 1473- 7175 Revie w Pseudotumor cerebri presenting as headache Expert Rev. Neurotherapeeutics 8(3), 397–407 (2008) Deborah I Friedman University of Rochester School of Medicine and Dentistry, 601 Elmwood Avenue, Box 659, Rochester, NY 14642, USA Tel.: +1 585 275 5332 Fax: +1 585 276 0292 deborah_friedman@ urmc.rochester.edu Pseudotumor cerebri (PTC) is characterized by intracranial hypertension without ventriculomegaly, in the absence of a mass lesion or meningeal process. When there is no secondary cause, it is termed ‘idiopathic intracranial hypertension’. Headache is the most common symptom of PTC, present in over 90% of patients. The headache is often disabling and nonspecific in character; thus, ophthalmoscopy is imperative for all patients being evaluated for headache. Visual loss is the major morbidity of PTC, requiring prompt diagnosis and treatment to prevent permanent deficits. Medical and surgical treatments are employed, although evidence-based treatment guidelines do not exist. This review discusses the diagnosis, differential diagnosis and management strategies for patients with PTC. KEYWORDS: cerebrospinal fluid shunt • headache disorder • intracranial hypertension • obesity • papilledema • pseudotumor cerebri • secondary History: what’s in a name? This disorder has been known by many names since it was first described by Taylor in 1880. Pseudotumor cerebri (PTC) was recognized as a distinct entity when Quincke published a detailed report in 1897 of ‘serous meningitis’ affecting several patients [1]. The term ‘pseudo- tumor cerebri’ was coined by Nönne in 1904, defining the clinical syndrome simulating a brain tumor in the absence of a tumor. In 1937, Davidoff and Dyke proposed the name ‘hyper- tensive meningeal hydrops’ after finding a his- tory of otitis media in four of their 15 cases. Dandy published another 22 cases the same year of “intracranial pressure without brain tumor” and proposed that changes in intra- cranial volume of blood or cerebrospinal
-
Upload
santri-dwizamzami-nasution -
Category
Documents
-
view
12 -
download
0
description
ptc
Transcript of PDF

w w w .f u t u r e - d r u g s .c o m 39710.1586/14737175.8.3.397
© 2008 Future Drugs Ltd
ISSN 1473-7175
Review
Pseudotumor cerebripresenting as headacheExpert Rev. Neurotherapeeutics 8(3), 397–407 (2008)
Deborah I Friedman University of Rochester School of Medicine and Dentistry, 601 Elmwood Avenue, Box 659, Rochester, NY 14642, USATel.: +1 585 275 5332Fax: +1 585 276 0292 deborah_friedman@ urmc.rochester.edu
Pseudotumor cerebri (PTC) is characterized by intracranial hypertension without ventriculomegaly, in the absence of a mass lesion or meningeal process. When there is no secondary cause, it is termed ‘idiopathic intracranial hypertension’. Headache is the most common symptom of PTC, present in over 90% of patients. The headache is often disabling and nonspecific in character; thus, ophthalmoscopy is imperative for all patients being evaluated for headache. Visual loss is the major morbidity of PTC, requiring prompt diagnosis and treatment to prevent permanent deficits. Medical and surgical treatments are employed, although evidence-based treatment guidelines do not exist. This review discusses the diagnosis, differential diagnosis and management strategies for patients with PTC.
KEYWORDS: cerebrospinal fluid shunt • headache disorder • intracranial hypertension • obesity • papilledema• pseudotumor cerebri • secondary
History: what’s in a name?
This disorder has been known by many names since it was first described by Taylor in 1880. Pseudotumor cerebri (PTC) was recognized as a distinct entity when Quincke published a detailed report in 1897 of ‘serous meningitis’ affecting several patients [1]. The term ‘pseudo- tumor cerebri’ was coined by Nönne in 1904, defining the clinical syndrome simulating a brain tumor in the absence of a tumor. In 1937, Davidoff and Dyke proposed the name ‘hyper- tensive meningeal hydrops’ after finding a his- tory of otitis media in four of their 15 cases. Dandy published another 22 cases the same year of “intracranial pressure without brain tumor” and proposed that changes in intra- cranial volume of blood or cerebrospinal fluid (CSF) were responsible. Foley coined the term‘benign intracranial hypertension’ in 1955 and realized that most of his 95 cases were idio- pathic. Buchheit and colleagues debunked that term in 1969 noting that “the syndrome is nei- ther a benign process nor a false tumor” as sev- eral of their patients lost vision. Unfortunately, Foley’s term continues to be used despite almost40 years of experience supporting Buchheit.
‘Idiopathic intracranial hypertension’ (IIH)was introduced into the literature in the early1990s and remains the preferred term when no secondary cause is identified. The original Dandy criteria for diagnosis were revised by
Smith in 1985 to incorporate computed tomog- raphy, and further refined by Friedman and Jacobson to reflect modern imaging, asympto- matic patients and the occasional lack of papilledema [2].
Treatment in the mid-20th century consisted of subtemporal decompression or repeated lum- bar punctures. Weight reduction gained favor in the 1960s. Medical management with aceta- zolamide and furosemide, and surgical treat- ments of optic nerve sheath fenestration and shunting entered the scene in the 1970s. Many secondary causes have been described in the interim, but the mechanism of PTC remains uncertain. To date, there are no prospective treatment trials in PTC; thus evidence-based guidelines for therapy do not exist [3].
Epidemiology
The idiopathic form of PTC generally occurs in patients under age 50 years, and most commonly affects obese women of childbearing age. The incidence of PTC in the USA has risen over the past 15 years, possibly attributable to the increas- ing prevalence of obesity or heightened awareness of the disorder. Current estimates place the inci- dence of PTC between two and 5.2 per 100,000 in the general population, thus affecting approxi- mately 20–22 per 100,000 obese women between the ages of 20 and 44 years [4,5]. Risk

398 Expert Rev. Neurotherapeutics 8(3), (2008)
Review Friedman
factors for developing PTC include female sex, high body mass index (often over 30), moderate weight gain (5–15% of body weight) during the year prior to symptom onset, and the use of tetracycline antibiotics within 6 months of symptom onset [6].
Diagnosis
Criteria for diagnosis include the following [2]:
• Symptoms, if present, are caused by intracranial hypertension
(ICH) or papilledema;
• Signs, if present, are caused by ICH or papilledema;
• Lumbar puncture shows an elevated opening pressure and normal CSF contents;
• Neuroimaging demonstrates no ventriculomegaly, mass or abnormal enhancement;
• Normal mental status;
• No other cause is identified (IIH).
Symptoms
Headache is present in over 90% of patients and is usually the initial symptom. The headache is frequently described as “the worst of my life”. It may begin slowly or gradually, often evolv- ing into a chronic daily headache [7]. The location is variable, including frontal, posterior or hemicranial cephalgia. Neck, back and shoulder pain are more prominent than headache in some patients. The headache is most frequently described as retro-ocu- lar, frontal and pressure-like [8]. However, throbbing headaches similar to migraine may occur, with associated photophobia, phonophobia and nausea. Cluster-like headaches with nocturnal awakening, severe periorbial pain and autonomic features rarely occur [9]. The importance of performing ophthalmoscopy on all patients with new-onset headaches or a change in headache pat- tern is underscored by these cases, as the headache of PTC is often similar to that of a primary headache disorder.
A B
Transient visual obscurations occur in approximately 75% of patients. They may be uniocular or binocular, consisting of par- tial or complete visual loss that is often provoked by a change in posture. The visual obscurations usually last less than 60 secs and reflect papilledema. They do not correspond to the overall visual status, nor do they predict long-term visual outcome. PTC is one of the few conditions causing transient visual obscurations, although they sometimes occur with optic disc drusen. Disc drusen are calcifications that occur on or below the anterior sur- face of the optic nerves. They produce an irregular optic-nerve contour that may simulate disc edema, and sometimes co-exist with disc edema.
Pulsatile tinnitus is present in approximately 50% of PTC patients. This symptom is often not volunteered and must be specifically queried. Other visual symptoms include binocular diplopia, blurred vision and subjective visual field loss. Less com- mon symptoms include ataxia, vertigo, disturbed hearing, torti- collis and facial palsy. Neck, back or radicular pain is sometimes prominent. Fever, meningismus or focal neurological deficits suggest another diagnosis. CSF rhinorrhea is a rare presenting symptom of PTC [10].
Signs
The hallmark of PTC is papilledema, which is usually bilateral, but may be asymmetric or unilateral [11]. There is considerable controversy about the timing of papilledema in relation to the patient’s symptoms. Papilledema may be present early in the course; some experts maintain that it develops before the patient becomes symptomatic. It is uncertain whether it begins acutely or evolves over days to weeks. A study of patients
admitted to a neurosurgical intensive care unit with acute ICH of various etiologies, and examined daily, found that only a small percentage developed papilledema by 1 week.
The con- troversy is compounded by the technical difficulty of visualiz- ing the optic nerves well using a direct
ophthalmoscope. This may account for some cases of missed PTC in patients evalu- ated in the emergency department.
How-ever, the diagnosis is initially missed in many cases because of failure to examine the optic nerves.
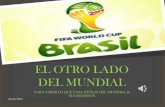
Features of papilledema that correlate with the severity of IIH include obscura- tion of the major vessels coursing over the disc margin, disc elevation, loss of the physiologic cup and a peripapillary halo. Hemorrhages, exudates, retinal infarcts, choroidal folds and macular edema may also be present (FIGURES 1 & 2). Low grade or early papilledema may be difficult to
Figure 1. Optic nerve appearance (March 2007) in a 17-year-old female with blurred vision, headache and diplopia for 2 weeks.She began taking doxycycline a few weeks previously. Her opening pressure was over550 mm cerebrospinal fluid. There is severe papilledema with disc hyperemia, nerve fiber layer hemorrhages, exudates and an early macular star. (A) Right eye and (B) left eye.
detect using a direct ophthalmoscope and an ophthalmological consultation is recommended. Stereoscopic viewing of the optic disc is also useful to distinguish true papilledema from pseudopapilledema

399ww w . f u t ur e - drug s . c o m
Pseudotumor cerebri presenting as headache Review
caused by anomalous discs, tiled optic nerves or optic disc drusen. Spontaneous venous pulsations usually suggest that the intracranial pressure (ICP) is below250 mm CSF but their presence does not completely exclude increased ICP. Approximately 25% of the population lacks spontaneous venous pulsations, so their absence is not helpful as an early sign of papilledema unless one is certain that they were previously present.
Central vision is usually impaired late in the course of papilledema but the visual field is involved early. Early visual field defects include enlargement of the physio- logic blind spot, inferonasal loss and gen- eralized constriction of the visual field (FIGURES 3 & 4) [12]. Visual field constriction from IIH must be differentiated from
A B
Figure 2. Same patient as Figure 1, 5 weeks after bilateral optic nerve sheath fenestration, several multiple lumbar punctures and acetazolamide treatment (May 2007).There is improvement in the papilledema although the optic nerves are still edematous and hyperemic with a peripapillary halo. The exudate in the papillomacular bundle is more distinct, reflecting the natural pattern of resolution. (A) Right eye and (B) left eye.
non-organic visual field constriction, which may be co-existent. Quantitative perimetry (automated threshold testing or Gold- mann) is required for the diagnosis and subsequent monitoring of the visual field. Decreased visual acuity early in the course is an ominous prognostic sign and requires prompt treatment.
A unilateral or bilateral abducens nerve palsy may be present, producing binocular diplopia that is worse at a distance (‘diver- gence insufficiency’). Other ocular motor deficits, such as oculomotor nerve palsy, trochlear nerve palsy and generalized ophthalmoparesis, are rare and suggest a secondary cause.
Neuroimaging
Neuroimaging is mandatory for patients with suspected PTC, both to exclude a secondary cause and to look for subtle changes suggestive of increased ICP. MRI is recommended unless there is a medical contraindication or the patient’s weight exceeds the gantry limit. Computed tomography may be performed urgently prior to the lumbar puncture but should be followed with MRI if possible. Ventricular size is normal. Indicators of increased ICP on MRI include an empty sella, distention of the optic nerve sheaths, flattening of the posterior sclerae and protrusion of the optic nerve papillae into the vitre- ous. A Chiari type 1 malformation is more common in patients with PTC than in the general population [13].
Magnetic resonance venography (MRV) frequently shows smooth-walled stenosis of the transverse sinuses [14]. In most cases, this appears to be the result of the ICH rather than the cause of it, as the stenosis resolves when the ICP is lowered [15,16]. Nonetheless, this finding has generated much enthusiasm for employing venous sinus stenting to treat PTC. Other venous sinus abnormalities may be present, including discontinuities and filling defects from enlarged arachnoid granulations. It is controversial whether MRV is necessary in every patient with PTC. Venous sinus thrombosis,
particularly superior sagittal sinus thrombosis, may produce a clinical syndrome identical to

399ww w . f u t ur e - drug s . c o m
PTC and is treated differently. MRV should be performed in any atypical patient (e.g., slim individuals,
children or men) or in patients who do not improve with treatment, noting that obese young women may
also develop venous sinus thrombosis. Bilateral transverse sinus stenosis is occasionally found in
patients with an otherwise typical migraine without aura. Increased ICP should be considered as a possible
etiologic fac- tor in obese patients with a relatively new onset of migraine
without aura [17].
Cerebrospinal fluid examination
A CSF examination measuring its opening pressure is required for diagnosis. It is tempting to make a diagnosis based on symp- toms, signs and neuroimaging studies, but foregoing the lumbar puncture is not advised. Important secondary causes of ICH may be missed without a spinal fluid examination. Additionally, if treatment is initiated without the CSF examination, the accu- racy of the diagnosis and need to continue therapy may be ques- tioned later without recourse. The diagnostic opening pressure should be 250 mm CSF or greater in adults. Values between200 and 250 mm CSF are indeterminate. Prolonged monitor- ing is sometimes required as CSF pressure fluctuates. Normal values for CSF pressure are not well established in young chil- dren, but ICH is suspected with pressures greater than 100 mm of CSF for children under 8 years of age, and over 200 mm of CSF for those between ages 8 to 12 years of age [18].
If the spinal needle is introduced with the patient in the sit- ting position, or performed under fluoroscopy, the patient must be moved to the lateral decubitus position for an accurate pres- sure reading. The patient must be relaxed with their legs par- tially extended; in one study, patients with normal resting opening pressures raised their pressure by 120–310 mm CSF simply by performing a Valsalva maneuver [19]. Pretreatment of patients with anxiolytics may help in this regard, as the lumbar punctures may be technically difficult in an obese patient.

400 Expert Rev. Neurotherapeutics 8(3), (2008)
Review Friedman
A B
30 30
central acuity and it may be difficult to determine the relative contributions of macular edema and optic neuropathy to central visual loss. Macular exudates usu- ally take several months to resolve and there may be a residual visual deficit after the fluid is reabsorbed.
Figure 3. Automated perimetry in the same patient as Figure 1 (March 2007). (A) Left eye: there is marked enlargement of the blind spot which extends almost to fixation. (B) Right eye: the blind spot is enlarged.
Etiology & pathogenesis
There are many secondary causes of PTC, some better substantiated than oth- ers. The literature is ripe with case reports of various conditions associated with ICH, making it hard to determine which
The CSF protein is normal or low and routine studies (including cytology) are recommended on the diagnostic lum- bar puncture to exclude hemorrhage, acute or chronic menin- gitis, inflammation or malignancy. The symptomatic response to CSF drainage is not diagnostic and postlumbar puncture headaches may occur.
Visual testing
Ophthalmic assessment includes best corrected visual acuity, pupil examination, visual field testing, intraocular pressure measurement, external examination and stereoscopic viewing of the fundi. Failure to measure the visual acuity in the acute/emergent setting may contribute to misdiagnosis or a delay in treatment. It is imperative to perform quantitative visual field testing by automated or kinetic (Goldmann) perimetry, as the visual acuity and visual fields are the major factors guiding therapy.
Patients who experience permanent visual loss generally have severe papilledema, although severe papilledema may be present with minimal visual sequelae. Fundus photogra- phy is helpful in following the optic nerve appearance. Reti- nal and macular exudates may occur with severe papilledema (FIGURES 1 & 2). Macular involvement produces a decline in
A B
factors are truly causal. The best substantiated associated con- ditions are listed in BOX 1. Prepubertal children are likely to have an underlying condition producing PTC, such as otitis media with secondary venous sinus thrombosis.
The pathogenesis of PTC is uncertain. The medications that produce ICH have no common mechanism or property that provides insight into the pathophysiology of the dis- order. Recent reports focus on the relationship between the cerebral venous system and ICP. There is no doubt that the cerebral venous system influences CSF pressure; CSF pressure must be higher than cerebral venous pressure at all times for normal homeostasis between the CSF and blood. Therefore, any rise in central venous pressure causes CSF pressure to increase. This relationship accounts for the development of ICH with venous sinus thrombosis, which may clinically mimic PTC [20].
The relationship between venous sinus stenosis and PTC is less clear. High resolution MRV shows smooth walled
stenoses of the transverse sinuses in many PTC patients, as well as fill- ing defects and irregularities in the contour of cerebral veins [14]. Manometry frequently demonstrates a
pressure gra- dient across the transverse sinuses in PTC that decreases acutely after CSF pressure is lowered [15,16].
This suggests that venous hypertension and venous sinusstenosis is a result of the ICH rather than the cause of it [15,21].
Is it possible that elevated central venous pressure and decreased venous return from obesity leads to raised cere-bral venous pressure and ICH? Some
30 30
Figure 4. Automated perimetry in the same patient as Figure 1 (May 2007).The blind spots are still enlarged, but improved since the initial examination.(A) Left eye and (B) right eye.
investigators postulate that an inward intra-abdominal pressure gradient in cen- tral obesity is the primary mechanism for PTC in obese patients [22]. If so, one would expect a high incidence of PTC during pregnancy, a state characterized by increased venous blood volume and infe- rior vena cava compression from the expanding uterus. The incidence of PTC

401ww w . f u t ur e - drug s . c o m
Pseudotumor cerebri presenting as headache Review
during pregnancy is the same as in control subjects. Moreover, the pressure gradient is not inwardly directed unless the
patient is in the supine position. Thus, this mechanism seems unlikely. Hypervitaminosis A is associated with PTC, and
some patients with IIH have high serum retinol levels and elevated CSF vitamin A levels [23]. This does not appear to be a
result of obesity, although vitamin A is lipid soluble. The postulated mechanism of vitamin A-related PTC is a
toxic reaction between retinol and cellular membranes of the arachnoid gran- ulations, impeding CSF absorption [24].
Various hormones, including estrogen, progestin, grehlin and leptin, are not differ- ent in PTC patients compared to
control subjects, but CSF vasopressin levels are consistently higher in PTC patients than controls. Impaired egress of CSF
through the lymphatic systemis another possible mechanism [25].
Although most patients with PTC have papilledema, it may be asymmetrical, unilateral or, uncommonly, absent. The lack of papilledema in some eyes has been attributed to variable con- tinuity of the CSF subarachnoid space between the optic nerves and the brain. It is presumed that CSF has a bidirectional flow between the optic nerve sheath and the brain but computerized tomographic cisternography in patients with papilledema indi- cates compartmentalization of the intraorbital CSF space [26]. This corresponds to a concentration gradient of lipocalin-like prostaglandin D-synthase between the spinal CSF space and the subarachnoid space surrounding the optic nerve [26].
Treatment
Treatment decisions are generally based on visual status.
Box 1. Conditions associated with intracranial hypertension.
Obstruction to venous drainage*
• Cerebral venous sinus thrombosis
• Aseptic (hypercoagulable state)
• Septic (middle ear or mastoid infection)
• Bilateral radical neck dissection with jugular vein ligation
• Superior vena cava syndrome
• Increased right heart pressure
• Cerebral arterial–venous sinus shunts
Endocrine disorders
• Obesity, recent weight gain*
• Orthostatic edema*
• Polycystic ovarian syndrome
• Addison’s disease
• Hypoparathyroidism
Exogenous agents
• Chlordecone (kepone)
• Corticosteroids (particularly withdrawal)*
• Growth hormone
• Leuprorelin acetate (leutinizing hormone-releasing hormone analogue)
• Levothyroxine (children)
• Lithium carbonate
• Nalidixic acid®
Treatments used to restore/preserve vision may or may not improve headaches and vice versa. A separate strategy is often
• Levonogastrel (Norplant
• Sulfa antibiotics
system)
required for headache management. There are no randomized trials of therapy in this disorder. All medications used to treat it are off-label, and treatment strategies are based on case series, retrospective data and experience.
General measures
If a secondary cause is identified, the underlying condition is treated or the provoking agent is discontinued. Treating a sec- ondary cause may not reverse the ICH rapidly enough to spare vision, so the ICP should be treated concurrently as needed.
Weight loss is recommended for obese patients as a long- term management strategy. The evidence supporting weight loss as an effective treatment is largely retrospective, and sug- gests that losing approximately 6% of body weight is associ- ated with an improvement in papilledema grade [27]. The effect of weight loss on headache and the other associated symptoms of IIH have not been studied, nor has any particular dietary protocol. Since many women with IIH have systemic fluid retention, a low-salt diet that avoids excessive fluid intake may be helpful [28]. Strict fluid restriction is not necessary. Weight loss may improve the general health of morbidly obese patients but does not
guarantee relief of IIH symptoms, particularly

401ww w . f u t ur e - drug s . c o m
• Tetracycline and related compounds*
– Minocycline– Doxycycline
• Vitamin A and related compounds*
• Accutane
– Vitamin supplements, liver– All-trans-retinoic acid (for acute promyelocytic leukemia)
Other medical conditions
• Antiphospholipid antibody syndrome
• Chronic obstructive pulmonary disease
• Renal failure
• Sleep apnea
• Systemic lupus erythematosis
• Turner syndrome
*Common, well-established associations.
headache. The role of bariatric surgery is controversial; it pro- duces more rapid and, generally, sustained weight loss. Propo- nents of bariatric surgery for PTC postulate that its effective- ness is related to decreasing intra-abdominal pressure, but this proposed mechanism has no physiologic basis.

402 Expert Rev. Neurotherapeutics 8(3), (2008)
Review Friedman
Medications
Diuretics are routinely employed in the treatment of IIH, although they have never been prospectively evaluated. Aceta- zolamide, a carbonic anhydrase inhibitor, is used as a first-line therapy to decrease CSF secretion from the choroid plexus. It may also cause mild anorexia and has a nonspecific therapeutic effect on headaches. Doses of 1–2 g daily are usually employed in adults. Higher doses, up to 4 g daily, may be used as tolerated. Common side effects of acetazolamide include paresthesias, drowsiness and altered taste sensation (especially for carbonated beverages). Mildly decreased serum bicarbonate levels are expected but do not generally require treatment. Severe adverse reactions include allergy, Stevens–Johnson syndrome, aplastic anemia and renal stones. Aplastic anemia is idiosyncratic and cannot be predicted by routinely monitoring the blood count. Methazolamide, another carbonic anhydrase inhibitor, is an alternative to acetazolamide. If carbonic anhydrase inhibitors are not successful, furosemide or other diuretics are used. Consider using triamterene or spironolactone in patients who are allergic to carbonic anhydrase inhibitors and furosemide.
Headaches from IIH respond variably to diuretics but are managed medically. Medications for headache prevention are useful, such as topiramate, tricyclic antidepressants, verapamil, gabapentin and valproate. As weight gain may exacerbate IIH, the patient’s weight should be monitored carefully during treatment. Topiramate is a preferred initial preventive medica- tion since it may facilitate weight loss [29,30]. Its weak carbonic anhydrase activity may be inadequate to decrease CSF produc- tion, so its therapeutic benefit is for headaches of PTC rather than the visual status. Care must be taken with co-administra- tion of topiramate and acetazolamide, monitoring the electro- lytes to avoid extreme acidosis or hypokalemia. Topiramate rarely produces acute angle-closure glaucoma, which must be distinguished from precipitous visual loss of PTC. Topiramate- induced angle-closure glaucoma is an idiosyncratic reaction to the sulfa moiety, is generally binocular and usually occurs dur- ing the early dose-titration phase of treatment [31]. It is reversi- ble but requires prompt treatment by an ophthalmologist and drug discontinuation.
Symptomatic treatment with migraine-specific medications may be useful, but the use of daily analgesics should be avoided to prevent medication-overuse headache. Patients with IIH commonly continue to experience headaches after their ICP is successfully treated, requiring long-term headache management [32].
In general, corticosteroid use should be avoided in IIH patients, as the ICP may rise as dose is tapered and because of weight gain [33]. Corticosteroids may be useful in the setting of acute visual loss to control the ICP prior to a surgical proce- dure. However, some experts feel that corticosteroids may be detrimental in this setting.
Depression and anxiety are commonly present in patients with PTC and should be addressed with psychotherapy, counseling or pharmacologic treatment [34].
Surgical treatment
Surgery is employed when patients have significant visual loss at presentation (based on visual acuity or visual field) or if their vision continues to deteriorate despite maximum medical treat- ment. Surgery is not generally recommended for the treatment of headache alone. Optic nerve sheath fenestration and shunt- ing are most commonly employed. Neither procedure has been studied prospectively nor are there studies directly comparing the two procedures. The decision to employ one or the other is often based on the available local expertise. Some patients may require both procedures if one surgical modality fails [35].
Optic nerve sheath fenestration is performed by an experi- enced orbital surgeon. Papilledema and visual loss must be present to consider this therapeutic option. Unilateral (on the eye with the worst vision) or bilateral, simultaneous procedures may be performed using either a medial or lateral orbital approach. The surgeon places several fenestrations or excises a window in the optic nerve sheath. The mechanism underlying the effectiveness of the procedure is uncertain. There is an immediate lowering of CSF pressure in the subarachnoid space surrounding the optic nerve as fluid is released through the fen- estration. Once the fenestration heals, the optic nerve may be protected from trabeculations of scar tissue between the optic nerve sheath and the optic nerve, compartmentalization of the optic nerve or from a filtering mechanism. Papilledema usually improves following optic nerve sheath fenestration. Approxi- mately 75% of eyes have improvement in the visual field, 65% of patients have improvement in their headaches and about half experience improved vision in the unoperated eye [36,37]. The procedure is similarly effective in children [38] and patients with severe visual loss may improve or stabilize [39]. The complica- tions are generally minor and transient, including diplopia, ocular discomfort and a tonic pupil. Visual loss resulting from the surgery occurs in less than 10% of patients, and is probably caused by ischemia [40]. Failure with recurrent visual loss may occur months to years later. The major advantages of the proce- dure are the lack of hardware, short duration of the procedure and amenability to outpatient surgery.
Various types of shunts are employed to treat IIH. Propo- nents of shunting over optic nerve sheath decompression sur- gery emphasize that it ‘treats the underlying problem’ of increased ICP. The preference for lumboperitoneal (LP) or ven- triculoperitoneal shunts has oscillated over the years. According to a national hospital admission database, the number of shunt procedures for IIH increased by 350% from 1998 to 2002, with new shunt placements increasing by 320% [41]. This rise may reflect heightened awareness of the disorder, increased incidence or a lower threshold for surgical treatment in patients with PTC. Shunting almost always works initially, but shunts frequently fail.
PTC is commonly treated using LP shunts. Their dis- advantages include overdrainage with an acquired Chiari mal- formation or low-pressure headaches, radiculopathy and a high

402 Expert Rev. Neurotherapeutics 8(3), (2008)
incidence of shunt failure. In a retrospective review of 27 IIH

403ww w . f u t ur e - drug s . c o m
Pseudotumor cerebri presenting as headache Review
patients treated with LP shunts with a mean follow-up of6 years, 56% required revision. The average revision rate was2.4 per patient with a median time to first revision of11 months. The most common reasons for shunt revision were shunt failure and low CSF pressure [42]. Another study review- ing CSF diversion procedures in 37 patients (73 LP and nine ventricular shunts) showed an average time to shunt failure of9 months (range from 1 day to more than 15 years) [43].
Review of a 30-year experience with shunting for PTC at Johns Hopkins School of Medicine studied 115 shunt proce- dures (79 LP and 36 ventriculoperitoneal or ventriculoatrial) in42 patients [44]. A total of 45% of patients had one procedure,24% underwent two, 19% underwent three to five and 12% had six or more procedures. Although 95% had a significant improvement in headaches 1 month after the procedure, head- aches recurred in 48% of patients by 36 months; visual func- tion was not assessed. LP shunts were more likely to require revision (86%) than ventricular shunts (44%). LP shunts were more prone to overdrainage and tonsillar herniation, and they were twice as likely to become obstructed compared to ven- tricular shunts. Ventricular shunts inserted with frameless stereotactic guidance were all successfully placed, but 75% failed by 24 months postinsertion.
In this series, lack of papilledema and symptoms lasting longer than 2 years were risk factors for treatment failure. Ven- triculoperitoneal shunts have the advantage of incorporating programmable valves, although their utility in PTC has not been confirmed.
Visual loss may be the first evidence of shunt failure [45]. Other manifestations of shunt malfunction are the return of headaches, marked worsening of headaches, or the develop- ment of other PTC symptoms (e.g., intracranial noises and transient obscurations of vision). Shunt failure may be difficult to verify, as radiographic continuity does not ensure patency. Sometimes the site of dysfunction is only found at the time of shunt revision.
Interventional radiological treatment
The discovery of venous sinus stenosis in PTC patients raises the possibility of using venous sinus stenting to treat it. This presumes that increased pressure in the dural venous sinuses is the cause of increased ICP, a concept that is controversial with much evidence to the contrary. The procedure may help in some cases and has inconsistent effectivness.
The initial report of stenting for PTC included 12 patients with intractable headaches and a visual disturbance lasting5 months to 12 years [46]. Two patients had severe visual loss and eight had chronic papilledema. All had previously received medical treatment, optic nerve sheath fenestration or a shunt procedure. No surgery had been performed within 10 months of stenting. Ten patients underwent unilateral sinus stenting only and two underwent contralateral stent placement later. At follow-up, five patients were asymptomatic, two had improved except for residual headache and five were
unchanged.

403ww w . f u t ur e - drug s . c o m
Papilledema resolved in four patients and improved in one. Venography after stenting showed a reduction in intrasinus pressure that did not correlate with clinical improvement.
An additional eight patients with IIH were subsequently stented [47]. The duration of disease and previous treatment were not described in the report. All had papilledema prior to stenting that resolved after the procedure. Seven patients had headaches over the stenting site that resolved in days to weeks. Six of seven had long-term improvement in vision that was dramatic in one case (light perception to almost normal vision within weeks), whilst another had resolution of bilateral abducens palsies.
Nine consecutive patients at another center were evaluated with direct retrograde cerebral venography and manometry, with simultaneous CSF pressure measurement in two patients [48]. All patients had been previously treated with vari- ous modalities including acetazolamide (three patients), optic nerve sheath fenestration (three patients), shunt (six patients, five of whom had numerous revisions) and subtemporal decom- pression (one patient). Five patients had partial transverse sinus obstruction and four were treated with stents. One patient with complex venous anatomy was not stented but had a shunt placed with a successful outcome. Four patients were feeling well and required no additional treatment. The authors concluded that IIH may be caused by dural venous sinus thrombosis in some patients and cause venous stenosis in others.
Complications of stenting include headache, transient hear- ing loss, transient unsteadiness and one life-threatening acute subdural hematoma [47]. The subdural hematoma developed during venography and stenting in one patient who also had an optic nerve sheath fenestration and external ventricular drain- age. The procedure is painful if general anesthesia is not employed, and re-stenosis of the venous sinuses may occur. Stenting, still in its exploratory phases, is not currently recommended for routine use.
Special circumstances
Pregnancy
Although PTC may develop or recur during pregnancy, preg- nancy is not contraindicated in women with PTC. Most preg- nant women are successfully managed using acetazolamide and intermittent lumbar punctures. If necessary, surgery may be performed. Since the expanding uterus may obstruct the shunt catheter, optic nerve sheath may be preferred to surgically treat visual decline. Corticosteroids may also be used. Medical treat- ment options for headache are limited and sodium valproate is contraindicated. Venous sinus thrombosis should be considered when PTC develops in the peripartum period.
Children
Diagnostic criteria for PTC in children do not currently exist and are proposed by Rangwalla and Liu (BOX 2). Prior to puberty, PTC affects boys and girls equally, and obesity is present less often than in adults [49]. Among adolescents, girls are affected

404 Expert Rev. Neurotherapeutics 8(3), (2008)
Review Friedman
Box 2. Proposed diagnostic criteria for idiopathic intracranial hypertension in pre-pubertal children.* [18].
• If symptoms or signs present, they may only reflect those of generalized intracranial hypertension or papilledema (normal mental status).
• Documented elevated intracranial pressure (age appropriate) measured in the lateral decubitus position.
– Age less than 8 years with papilledema: less than 100 mm H20
– Age 8 years or above or less than 8 years without papilledema: less than 250 mm H20
• Normal cerebrospinal fluid composition except in neonates who may have up to 32 white blood cells/mm3 and protein as high as150 mg/dl.
• No evidence of hydrocephalus, mass, structural or vascular lesion on MRI, with and without contrast, and MR venography. Narrowing of the tranverse sinuses is allowed.
• Cranial nerve palsies allowed if they are of no other identifiable etiology and improve with reduction in cerebrospinal fluid pressure or resolution of other signs and symptoms of intracranial hypertension.
• No other identified cause of intracranial hypertension.
*In boys, supported by no evidence of pubic hair. In girls, supported by lack of breast development, growth of pubic hair or menarche. Reproduced with permission from [18].
more frequently than boys. IIH in young children may present with somnolence, a stiff neck, apathy, ataxia, irritability or tor- ticollis [50]. If the skull sutures are still open, papilledema may be mimimal or absent. A secondary cause is frequently found, such as infection, medication or otitis media [51]. Management of IIH in children is similar to adults. Papilledema is occasion- ally discovered in asymptomatic children during a routine eye exam [52]. After excluding a secondary cause, these children may be followed conservatively if their visual function is normal.
Fulminant (‘malignant’) IIH
In some cases, the manifestations of IIH appear rapidly with early visual loss. Such patients generally have marked visual field loss or decreased central visual acuity at presentation. There may be marked papilledema, evidence of optic nerve ischemia and macular edema. These patients require aggressive management, employing medical and surgical measures. However, the visual outcome may be poor despite rapid intervention [53].
IIH variants
A case–control study described IIH without papilledema (n = 25) in overweight women seeking care for chronic daily headache at a headache center [54]. Compared with control sub- jects (n = 60), those with ICH were more commonly obese and had pulsatile tinnitus. There was a high rate of medication-over- use headache in both groups of subjects. Approximately half of patients improved with lumbar punctures or dihydro- ertgotamine. A third of patients responded to diuretics. Shunting was performed in five patients; headaches improved but most patients required more than one procedure. IIH with normal CSF pressure by lumbar puncture has also been described.
Prognosis
The disorder is usually monophasic and self-limited. However, some patients continue to have lifelong symptoms,
with head- ache being the most pervasive residual symptom. Episodic or

404 Expert Rev. Neurotherapeutics 8(3), (2008)
chronic tension-type headache, or migraine without aura is present in over two thirds of patients after other symptoms and signs of ICH resolve, and often requires long-term treatment [32]. It may be difficult to discern whether the persist- ence or return of headaches in patients with IIH represents recurrent disease or a benign headache disorder. This is particu- larly problematic in patients with residual optic atrophy, as their optic nerves may not swell in response to high ICP.
There are little prospective data assessing the long-term visual prognosis in PTC. The visual outcome is generally good, although residual visual field defects persist in up to 50% of patients when assessed by sensitive perimetric methods. The most common persistent visual field defects are generalized vis- ual constriction, superior or inferior nasal field loss, arcuate scotomas and enlarged blind spots. Factors associated with vis- ual loss are high grade papilledema, atrophic papilledema, sub- retinal hemorrhages at presentation, optociliary shunt vessels, intraocular hypertension, anemia, systemic hypertension and renal failure. Visual acuity loss at presentation and rapid decline of visual function early in the course are unfavorable prognostic indicators. Legal blindness or complete blindness occurs in less than 5% of patients.
Overall quality of life is impacted upon in IIH. Patients with IIH have significantly lower health-related quality of life and vision-specific health-related quality of life (assessed by SF-26 and NEI VFQ-25, respectively) scores compared to neuro- ophthalmologic control patients and a disease-free reference group. Depression and anxiety are common, and not attributable to obesity.
Expert commentary
The incidence of PTC is rising in parallel with the increase in obesity in the Western world. Recognition of the disorder seems to be improving but the diagnosis is often initially missed, particularly in the emergency room/urgent care setting. Failure to diagnose PTC in the acute stages often leads to a

405ww w . f u t ur e - drug s . c o m
Pseudotumor cerebri presenting as headache Review
delay in treatment and increases the risk of permanent visual loss. Thus, it is important to perform fundoscopy in all patients evaluated for headache to assess for papilledema.
Patients with chronic daily headaches and no papilledema may also have ICH, although treating the ICP is generally unsatisfactory. These patients may have undetected obstructive sleep apnea provoking their headaches and ICH. Obesity is a recognized risk factor for chronic daily headache; it is uncertain whether or not chronically elevated ICP is a contributing factor or a confounder [55].
The management of PTC requires a team approach, prefera- bly by physicians familiar with the treatment of this disorder. Neurologists, ophthalmologists, neurosurgeons, radiologists and primary physicians are involved in the care of these patients and close communication amongst all providers is paramount. In general, neurologists are in the best position to take charge of PTC management, but require input from the ophthalmologist regarding the patient’s visual status. A neuro-ophthalmologist should be involved whenever possible.
The lack of evidence-based treatment guidelines and prospec- tive PTC studies have produced ambiguity regarding thera- peutic strategies. A study comparing optic nerve sheath fenestra- tion to shunting was explored by the Neuro-Ophthalmology Research Disease Investigator Consortium (NORDIC) but deemed unfeasible owing to sample size constraints and the lack of convincing evidence in the existing literature that one proce- dure is more effective than the other. The disease is not rare, and the lack of funded research on PTC to date is disappointing.
Currently, patients with normal vision or mild visual loss are treated medically, and those with moderate or severe visual loss (based on visual acuity and visual field) are candidates for surgery.
Headaches are managed medically. Weight loss seems to be help- ful in the long term in obese patients. Secondary causes are treated concurrently with management of the ICP.
Five-year view
Advances in neuroimaging, such as auto-triggered, elliptic-cen- tric-ordered (ATECO) 3D-enhanced MRI will continue to enhance our ability to diagnose PTC and detect cerebral venous abnormalities. Non-invasive alternatives for measuring ICP are being studied. If successful, this option will be helpful for screening patients with suspected ICH and monitoring the sta- tus of ICP, although it will probably not replace the diagnostic lumbar puncture in most cases.
In the words of Lueck and McIlwaine from their Cochrane review, “There is insufficient information to generate an evi- dence-based management strategy for IIH. Of the various treat- ments available, there is inadequate information regarding which are truly beneficial and which are potentially harmful. Properly designed and executed trials are needed” [3]. NORDIC submitted two treatment trial proposals to the NIH in 2006, including one study of medical management for patients with mild visual loss and a second study incorporating early optic nerve sheath fenes- tration in patients with moderate visual loss. Should the study of mild visual loss commence in 2009, evidenced-based guidelines for treating this group of patients will be available in approxi- mately 5 years. Visual prognosis, headache disability and the effect on quality of life will be established using these prospective data. It is unlikely that additional new treatments will emerge within the next 5 years, but the ongoing studies of stenting will determine its role in the treatment armamentarium.
Key issues
• Pseudotumor cerebri (PTC) is characterized by intracranial hypertension without ventriculomegaly or a mass lesion. The idiopathic form, idiopathic intracranial hypertension (IIH), most frequently affects individuals under age 45 years, particularly obese women of childbearing age.
• The incidence of PTC is increasing, commensurate with the rise in obesity in the Western world.
• Prompt diagnosis and treatment are needed to prevent permanent visual loss. Thus, optic nerve examination by fundoscopy is important when evaluating headache patients.
• Headache is the most common symptom of PTC, present in over 95% of patients at diagnosis. There are no specific characteristics of the headache that differentiate the headaches of PTC from other conditions, although they are often described as the worst headache of one’s life. Transient visual obscurations and pulsatile tinnitus are common initial symptoms.
• Diagnosis requires neuroimaging, a lumbar puncture with opening pressure measurement and spinal fluid examination, and exclusion of secondary causes. Venous sinus thrombosis may simulate IIH and should be considered in all patients, especially men, pregnant or post-partum women, and individuals of normal weight.
• The goal of treatment is to preserve vision. Management is best guided by a neurologist or neuro-ophthalmologist. A team approach is required for optimal care, including critical input from an ophthalmologist regarding the patient’s visual status.
• Risk factors for permanent visual loss include severe papilledema, visual loss at onset and early deterioration of vision (with or without treatment), anemia, systemic hypertension and renal failure.
• Both medical and surgical treatment options exist, although there are currently no evidence-based guidelines for treating PTC. Medical management is preferred for headache treatment.
• The prognosis is generally good, although a small percentage of patients go blind. Recurrence is possible and headaches often persist after the intracranial pressure is controlled.

406 Expert Rev. Neurotherapeutics 8(3), (2008)
Review Friedman
Research studies of arachnoid granulation histology, lym- phatic drainage from the brain and neuroimaging are in progress, and may lend additional insight into the pathogene- sis of IIH within the next 5–10 years. The randomized, multi- center clinical trial proposed by NORDIC will assess the con- tribution of various obesity-related hormones and genetic factors to IIH. Thus, it is possible that investigations during the next 5–10 years will have a significant impact on our understanding of IIH and provide a more definite direction for its treatment.
Financial & competing interests disclosure
This work was supported by a Research to Prevent Blindness Challenge
Grant and the National Eye Institute K23EY015525. The author has
no other relevant affiliations or financial involvement with any
organization or entity with a financial interest in or financial conflict
with the subject matter or materials discussed in the manuscript apart
from those disclosed.
No writing assistance was utilized in the production of this manuscript.
References
1 Bandyopadhyay S. Pseudotumor cerebri.Arch. Neurol. 58, 1699–1701 (2001).
2 Friedman DI, Jacobson DM. Diagnostic criteria for idiopathic intracranial hypertension. Neurology 59, 1492–1495 (2002).
3 Lueck C, McIlwaine G. Interventions for idiopathic intracranial hypertension. Cochrane Database Syst. Rev. CD003434 (2005).
4 Garrett JH, Corbett JJ, Braswell R.The incidence of idiopathic intracranial hypertension in Mississippi. In: North American Neuro-Ophthalmology Society. Orlando, FL, USA 269 (2004).
5 Jacobs DA, Corbett JJ, Balcer LJ.Annual incidence of idiopathic intracranial hypertension (IIH) in the Philadelphia area. In: North American Neuro-Ophthalmolog y Society. Orlando, FL, USA 286 (2004).
6 Daniels AB, Liu GT, Volpe NJ et al.Profiles of obesity, weight gain, and quality of life in idiopathic intracranial hypertension (pseudotumor cerebri). Am. J. Ophthalmol. 143, 635–641 (2007).
7 Evans RW. Diagnostic testing for chronic daily headache. Curr. Pain Headache Rep.11(1), 47–52 (2007).
8 Wall M. The headache profile of idiopathic intracranial hypertension. Cephalalgia 10,331–335 (1990).
9 Volcy M, Tepper SJ. Cluster-like headache secondary to idiopathic intracranial hypertension. Cephalalgia 26(7), 883–886 (2006).
10 Suryadevara AC, Fattal M, Woods CI.Nontraumatic cerebrospinal fluid rhinorrhea as a result of pseudotumor cerebri. Am. J. Otolaryngol. 28, 242–246 (2007).
11 Huna-Baron R, Landau K, Rosenberg ML, Warren FA, Kupersmith MJ. Unilateral swollen disc due to increased intracranial pressure. Neurolog y 56, 1588–1590 (2001).
12 Friedman DI. Pseudotumor cerebri. Neurol.
Clin. 22, 99–131 (2004).
13 Banick R, Lin D, Miller NR. Prevalence of Chiari I malformation and cerebellar ectopia in patients with pseudotumor cerebri.J. Neurol. Sci. 247, 71–75 (2006).
14 Farb RI, Vanek I, Scott JN et al. Idiopathic intracranial hypertension. The prevalence and morphology of sinovenous stenosis. Neurology 60, 1418–1424 (2003).
15 King JO, Mitchell PJ, Thomson KR, Tress BM. Manometry combined with cervical puncture in idiopathic intracranial hypertension. Neurology 58, 26–30 (2002).
16 Rohr A, Dörner L, Stingele R et al.Reversibility of venous sinus obstruction in idiopathic intracranial hypertension. AJNR Am. J. Neuroradiol. 28, 656–659 (2007).
17 Bono F, Messina D, Gilberto C et al.Bilateral transverse sinus stenosis predicts IIH without papilledema in patients with migraine. Neurology 67, 419–423 (2006).
18 Rangwalla LM, Liu GT. Pediatric idiopathic intracranial hypertension. Surv. Ophthalmol.52(6), 597–617 (2007).
19 Neville L, Egan RA. Frequency and amplitude of elevation of cerebrospinal fluid resting pressure by the Valsalva maneuver. Can. J. Ophthalmol. 40, 775–777 (2005).
20 Biousse V, Ameri A, Bousser M-G. Isolated intracranial hypertension as the only sign of cerebral venous thrombosis. Neurology 53,1537–1542 (1999).
21 Corbett JJ, Digre KB. Idiopathic intracranial hypertension. An answer to, “the chicken or the egg?” Neurology 58, 5–6 (2002).
22 Friedman DI. Cerebral venous pressure, gastric bypass surgery and dural venous sinus stenting in idiopathic intracranial hypertension. J. Neuroophthalmol. 26,
61–64 (2006).
23 Warner JEA, Bernstein PS, Yemelyanov Aet al. Vitamin A in the cerebrospinal fluid of patients with and without idiopathic intracranial hypertension. Ann. Neurol. 52,647–650 (2002).

406 Expert Rev. Neurotherapeutics 8(3), (2008)
24 Jacobson DM, Berg R, Wall M et al.Serum vitamin A concentration is elevated in idiopathic intracranial hypertension. Neurolog y 53, 1114–1118 (1999).
25 Johnston M, Zakharov A, Papaiconomou C, Salmasi G, Armstrong D. Evidence of connections between cerebrospinal fluid and nasallymphatic vessels in humans, non-human primates and other mammalian species. Cerebrospinal Fluid Res. 1(2), 1–13 (2004).
26 Killer HE, Jaggi GP, Flammer J et al.Cerebrospinal fluid dynamics between the intracranial and subarachnoid space of the optic nerve. Is it always bidirectional? Brain130, 514–520 (2007).
27 Kupersmith MJ, Gamell L, Turbin R, Spiegel P, Wall M. Effects of weight loss on the course of idiopathic intracranial hypertension in women. Neurology 50,1094–1098 (1998).
28 Friedman DI, Streeten DHP. Idiopathic intracranial hypertension and orthostatic edema may share a common pathogenesis. Neurolog y 50, 1099–1104 (1998).
29 Finsterer J, Földy D, Fertl E. Topiramate resolves headache from pseudotumor cerebri. J. Pain Symptom Manage. 32(5),401–402 (2006).
30 Alore PL, Jay WM, Macken MP.Topiramate, pseudotumor cerebri, weight-loss and glaucoma: an ophthalmologic perspective. Semin. Ophthalmol. 21(1), 15–17 (2006).
31 Fraunfelder FW, Fraunfelder FT,Keates EU. Topiramate-associated acute, bilateral secondary angle-closure glaucoma. Ophthalmology 111, 109–111 (2004).
32 Friedman DI, Rausch EA. Headache diagnoses in patients with treated idiopathic intracranial hypertension. Neurolog y 58, 1551–1553 (2002).
33 Liu GT, Kay MD, Bienfang DC,Schatz NJ. Pseudotumor cerebri associated with corticosteroid withdrawal in inflammatory bowel disease. Am. J. Ophthalmol. 117, 352–357 (1994).

407ww w . f u t ur e - drug s . c o m
Pseudotumor cerebri presenting as headache Review
34 Kleinschmidt JJ, Digre KB, Hanover R.Idiopathic intracranial hypertension. Relationship to depression, anxiety, and quality of life. Neurology 54, 319–324 (2000).
35 Kelman SE, Sergott RC, Cioffi GA et al.Modified optic nerve decompression in patients with functioning lumboperitoneal shunts and progressive visual loss. Ophthalmolog y 98, 1449–1453 (1991).
36 Sergott RC, Savino PJ, Bosley TM. Optic nerve sheath decompression: a clinical review and proposed pathophysiologic mechanism. Aust. N. Z. Ophthalmol. 18,365–373 (1990).
37 Spoor TC, McHenry JG. Long-term effectiveness of optic nerve sheath decompression for pseudotumor cerebri. Arch. Ophthalmol. 111, 632–635 (1993).
38 Thuente DD, Buckley EG. Pediatric optic nerve sheath decompression.Ophthalmolog y 112(4), 724–727 (2005).
39 Chandrasekaran S, McCluskey P,Minassian D, Assaad N. Visual outcome for optic nerve sheath fenestration in pseudotumor cerebri and related conditions. Clin. Experiment. Ophthalmol.34(7), 661–665 (2006).
40 Brodsky MC, Rettele GA. Protracted postsurgical blindness with visual recovery following optic nerve sheath fenestration. Arch. Ophthalmol. 116, 107–108 (1998).
41 Curry WT Jr, Butler WE, Barker FG 2nd.
42 Eggenberger ER, Miller NR, Vitale S.Lumboperitoneal shunt for the treatment of pseudotumor cerebri. Neurology 46,1524–1530 (1996).
43 Rosenberg ML, Corbett JJ, Smith C et al.Cerebrospinal diversion procedures for pseudotumor cerebri. Neurology 43,1071–1072 (1993).
44 McGirt MJ, Woodworth G, Thomas Get al. Cerebrospinal fluid shunt placement for pseudotumor cerebri-associated intractable headache: predictors of treatment response and analysis of long term outcomes. J. Neurosurg. 101, 627–632 (2004).
45 Liu GT, Volpe NJ, Schatz NJ et al. Severe sudden visual loss caused by pseudotumor cerebri and lumboperitoneal shunt failure. Am. J. Ophthalmol. 122, 129–131 (1996).
46 Higgins JNP, Cousins C, Owler BK, Sarkies N, Pickard JD. Idiopathic intracranial hypertension: 12 cases treated by venous sinus stenting. J. Neurol. Neurosurg. Psychiatr. 74, 1662–1666 (2003).
47 Owler BK, Parker G, Halmagyi GM et al.Cranial venous outflow obstruction and pseudotumor cerebri syndrome. Adv. Tech. Stand. Neurosurg. 30, 108–174 (2005).
48 Owler BK, Parker G, Halmagyi GM et al.Pseudotumor cerebri syndrome: venous sinus obstruction and its treatment with stent placement. J. Neurosurg. 98,
50 Lessell S. Pediatric pseudotumor cerebri (idiopathic intracranial hypertension). Surv. Ophthalmol. 37, 155–166(1992).
51 Cinciripini GS, Donahue S, Borchert MS.Idiopathic intracranial hypertension in prepubertal pediatric patients: characteristics, treatment and outcome. Am. J. Ophthalmol. 127, 178–182 (1999).
52 Weig SG. Asymptomatic idiopathic intracranial hypertension in young children. J. Child Neurol. 17(3), 239–241 (2002).
53 Thambisetty M, Lavin PJ, Newman NJ, Biousse V. Fulminant idiopathicintracranial hypertension. Neurolog y68(3), 229–232 (2007).
54 Wang S-J, Silberstein SD, Patterson S, Young WB. Idiopathic intracranial hypertension without papilledema. A case–control study in a headache center. Neurolog y 51, 245–249 (1998).
55 Scher AI, Stewart WF, Ricci JA,Lipton RB. Factors associated with the onset and remission of chronic daily headache in a population-based study. Pain 106(1–2), 81–89 (2003).
Affiliation
• Deborah I Friedman, MDUniversity of Rochester School of Medicine
Rapidly rising incidence of cerebrospinal 1045–1055 (2003). and Dentistry, 601 Elmwood Avenue,fluid shunting procedures for idiopathic 49 Balcer LJ, Liu GT, Forman S et al. Box 659, Rochester, NY 14642, USAintracranial hypertension in the United Idiopathic intracranial hypertension: Tel.: +1 585 275 5332States, 1988–2002. Neurosurgery 57(1), Relation of age and obesity in children. Fax: +1 585 276 029297–108 (2005). Neurolog y 52, 870–872 (1999). d e b o r a h _ f r ie d m a n @ u r m c . r o c h e s t e r . e d u

Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.







![H20youryou[2] · 2020. 9. 1. · 65 pdf pdf xml xsd jpgis pdf ( ) pdf ( ) txt pdf jmp2.0 pdf xml xsd jpgis pdf ( ) pdf pdf ( ) pdf ( ) txt pdf pdf jmp2.0 jmp2.0 pdf xml xsd](https://static.fdocuments.net/doc/165x107/60af39aebf2201127e590ef7/h20youryou2-2020-9-1-65-pdf-pdf-xml-xsd-jpgis-pdf-pdf-txt-pdf-jmp20.jpg)