PD Inservice
42
The Patie n t with Parkinson’s Disease: Examination and Management Darcy Jame s, SPT
-
Upload
darcy-james -
Category
Documents
-
view
37 -
download
0
Transcript of PD Inservice

The
Patie
nt with
Park
inso
n’s
Diseas
e: E
xam
inat
ion a
nd
Manag
emen
t
Darcy
Jam
es, S
PT
overview
Introduction to Parkinson’s Disease Etiology Cardinal signs
Examination procedure
Physical therapy interventions and management

PD: an introduction
Second most prevalent neurodegenerative disorder Impacts approximately 1.5 million in the United States
Differential diagnosis Idiopathic PD or primary PD verse parkinsonism or parkinsonian
features
In general, all individuals have a dysfunction in the dopamine pathways of the basal ganglia
Underlying cause is unknown
(Kegelmeyer, 2014)

The role of the basal ganglia and dopamine
Located in the midbrain and includes substantia nigra, globus pallidus, and striatum
Responsible for a variety of functions including voluntary motor control, procedural learning, motivation, and executive function
Dopamine has many functions, one being voluntary movement and is present in the midbrain
Lack of dopamine in the basal ganglia impacts the motor pathways
leading to symptoms such as bradykinesia and postural instability
Inhibition of motor systems
(Kegelmeyer, 2014)

Cardinal motor symptoms of PD
Diagnosis of PD is based on the presence of at least two of the four cardinal motor signs:
Bradykinesia
Resting tremor
Rigidity
Postural instability
(Kegelmeyer, 2014)

bradykinesia
Defined as a slowness of movement
Other terms associated include hypokinesia and akinesia Hypokinesia refers to small movements, believed to be one of the
primary causes of reduced walking velocity due to reduction in step length
Akinesia refers to lack of movement, typically associated with the inability to initiate movement or “freezing”
Causes prolonged time to complete ADLs and may impair reflexive movements
Typical parkinsonian gait pattern is described as shuffling gait
(Kegelmeyer, 2014)

Resting tremor
Noted at rest but diminishes when the limb is moving
“Pill rolling” tremor Flexion and extension of the fingers in connection with adduction and
abduction of the thumb Usually appears unilaterally but may become bilateral
(Kegelmeyer, 2014)

Rigidity
Increased stiffness of the muscles, which is not speed dependent
Affects proximal musculature first and eventually spreads to the muscles of the face and extremity
Cogwheel verse lead pipe rigidity Cogwheel: jerky, ratchet-like resistance to passive movement as
muscles alternately tense and relax Lead pipe: constant uniform resistance to passive movement
Can lead to muscle shortening, loss of motion, slowness, and fatigue
(Kegelmeyer, 2014)

Postural instability
Impaired balance and balance reactions due to damage to basal ganglia pathways
Difficulty recovering balance
Respond to inability with abnormal muscle co-activation patterns
Exhibit difficulty with feed-forward postural control
(Kegelmeyer, 2014)

Autonomic problems
Damage to the autonomic nervous system leads to problems involving the major organ systems including cardiovascular, gastrointestinal, and urogenital systems
Orthostatic hypotension is the most noticeable change to the cardiovascular system
Drop in systolic blood pressure > 20 mm Hg or drop in diastolic blood pressure > 10 mm Hg that occurs within 3 minutes of either standing or head-up tilt to at least 60 degrees
Can result in dizziness and falls
(Kegelmeyer, 2014)

Additional associated symptoms
Dual task inability
Impaired dexterity and coordination
Fatigue
Muscle aches or cramps
Feelings of fear and anxiety
(Kegelmeyer, 2014)

Hoehn and Yahr classification

Examination
History
Body structure and function
Neurologic system
Musculoskeletal system
Gait assessment
Falls screening
Balance
Function
Participation measures
(Kegelmeyer, 2014)
Neurologic system
Every examination should include routine neurologic tests such as:
Proprioception, sensation, reflexes, and tone
MDS-UPDRS Scales for the clinician and patient self-report to include information on impairments specific to PD
Bradykinesia: finger/toe tapping test Balance: pull test for postural instability Tremor: described in terms of location, amplitude, and consistency Dyskinesia: present or not present Freezing: rapid-360 degree turn, observe gait in a confined space Movement scale: repetitive finger-to-finger movements
(Kegelmeyer, 2014)

Musculoskeletal systemMuscle rigidity and postural changes can make people with PD
susceptible to muscle shortening and decreased ROM leading to contractures
Specific muscle groups prone to shortening Pectoralis muscles Iliopsoas Hamstrings Gastrocnemius
Scoliosis should be assessed
Trunk rotation should be assessed as it is the key to many functional activities such as walking with long strides and reaching
(Kegelmeyer, 2014)

Gait assessment
Gait speed can be correlated with both function and health outcomes
Slowing of gait has been shown to correlate to increased disability in ADLs and increased fall risk
For valid measurements, speed should be measured over the longest distance feasible and include sufficient space for acceleration and deceleration
10 meter walk test
(Kegelmeyer, 2014)

Gait assessment
Many falls occur in situations requiring a backward step, procedures for testing backwards walking have been established
Backwards walking velocity < 0.60 m/s was indicative of high fall risk 10 meter walk test
Tinetti Mobility Test Made up of two scales, balance and gait Mobility portion can be used to examine gait and has been found to have
a good correlation with gait speed
6 Minute Walk Test Most commonly used measure of functional walking ability and endurance Studies have shown that the distance walked is less for those with PD than
for community dwelling elderly (PD = 392 m; elderly = 631 m)
(Kegelmeyer, 2014)

Fall screening
Critical for ensuring safety of patients
One of the best predictors for fall risk is fall history Individuals who have fallen are at risk for future falls
Balance Evaluation Systems Test (BESTest) Combines elements of tests such as the TUG and Berg Balance Scale Two shorter versions available as well which are both highly
recommended for fall screening (Mini BESTest)
(Kegelmeyer, 2014)
Fall screen comparison
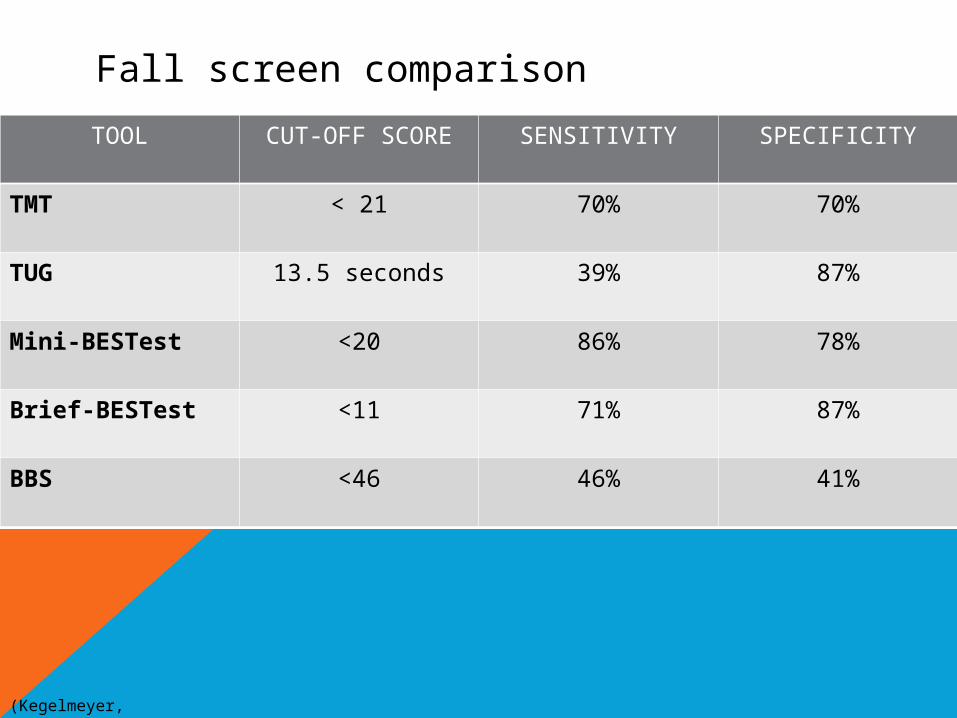
TOOL CUT-OFF SCORE SENSITIVITY SPECIFICITY
TMT < 21 70% 70%
TUG 13.5 seconds 39% 87%
Mini-BESTest <20 86% 78%
Brief-BESTest <11 71% 87%
BBS <46 46% 41%
(Kegelmeyer, 2014)
Balance assessments
Berg Balance Scale is one of the most commonly used tests for assessing balance
Has been shown to have ceiling effect with people with PD, may not be appropriate for some individuals with more subtle balance problems
Functional Gait Assessment
Mini-BESTest
Four-square step test Assesses coordination and balance while stepping forward, side-to-side, and
backward Does not allow for the assessment of ability to reverse directions, step over
an object, and step sideways and backwards Can also be used to measure bradykinesia since it is timed
(Kegelmeyer, 2014)

Balance assessment
Impairments that are usually assessed include limits of stability, postural response to perturbation, and both static and dynamic balance
Functional reach test Provides indication of anticipatory balance responses
Static balance Single leg stance Romberg test Sharpened Romberg
(Kegelmeyer, 2014)

Functional assessment
Measures should be chosen based on the goals of the individual
Modified Physical Performance Test Examines mobility, upper extremity function, and a few ADLs
Timed chair rise Several varieties of the test
OPTIMAL Measures difficulty and self confidence in performing movements
(Kegelmeyer, 2014)

Participation measures
Several quality of life measures used in research studies
Will be necessary for clinicians to use participation measures because with insurance changes insurers are now looking for therapists to demonstrate that therapy is impacting participation
Lead to better tracking of return to participation-level activities and improve reimbursement
Parkinson’s Disease Questionnaire (PDQ-39)
Short Form Health Survey (SF-36)
(Kegelmeyer, 2014)

Management of Parkinson’s Disease

neuorplasticityChanges that occur in the reorganization of the brain as a result of
experience In neurodegenerative diseases, the brain must constantly be reorganized due
to loss of neurons
Animal studies Demonstrated that exercise immediately after lesion is neuroprotective Treadmill training improves motor symptoms and neurochemical deficits
Fisher et al. (2008) Treadmill training in individuals improved walking function and corticomotor
excitability Indicated that the pattern of activity in the brain was different after treadmill
training
Physical therapy interventions are bringing both changes about function and neuroplastic changes in the central nervous system
(Kegelmeyer, 2014)
Key components for Therapy ProgramsRepetition Neuroplasticity relies on repetition Treadmill training verse over-ground walking
Cueing Found to influence the speed and amplitude of movement Studies have shown that self-given auditory cue is more effective than
external cues Visual cues and benefits on gait
Useful of meaningful, functional activities Practice the specific task that an individual wants to improve
Exercises designed to specifically address individual impairments Address underlying impairments and specific functional activities
(Kegelmeyer, 2014)

Orthostatic hypotension
Significant safety issue because these can leads to episodes of falls
Education and exercise treatment approach Slow position changes Ankle pumps, lower extremity isometrics prior to standing Pause after standing Have something to grab onto when standing, if possible
(Kegelmeyer, 2014)

Range of motion/stretching
Primary deficit is rotation in all joints
Stretching should be initiated early in the disease and become part of the daily routine
Shoulder internal rotation/adduction, hip flexion with knee extension, hip extension, and trunk extension
Muscles are prone to contractures, causing the need for a flexibility program to be initiated early in the disease course
(Kegelmeyer, 2014)

strength
Strength training needs to address muscle groups associated with functional activity
Gross strength impairments are not common until later in the disease process, but it is indicated early
Due to early postural changes, core strengthening may benefit as well
(Kegelmeyer, 2014)
balance
Most falls occur when an individual is turning or getting out of a chair, activities which include stepping laterally and backward
Backwards walking would be beneficial
Many functional activities require prolonged periods of time spent on a single leg
Single leg stance activities
Balance training incorporating the proprioceptive system Goal of decreasing visual reliance or teaching individuals to
compensate for proprioceptive deficits in the later stages
(Kegelmeyer, 2014)

mobility
Treadmill training has been shown to improve gait, walking confidence, and quality of life
Advantages of treadmill training Preset pace of walking Consistent pace, repetition of stepping pattern Increased stride length and decreased variability in stride length
Studies have shown that treadmill training has decreased bradykinesia and hypokinesia while promoting neuroplasticity
(Kegelmeyer, 2014)

Treadmill training recommendations
Conduct 3 sessions per week lasting 20-30 minutes
Based on pace retraining Start with comfortable walking speed and increased by 0.4 miles per
hours after a warm-up period Participant should be able to increase the pace with the goal of
attaining a speed of 1.2 m/s
Conducted while the participant is at peak dose dopaminergic medication
(Kegelmeyer, 2014)

Effect of physical exercise-movement strategies programme on mobility, falls, and quality of life in parkinson’s disease Geogry, Barnsley, chellappa (2011)
Participants: 15 patients with idiopathic PD
Intervention: Participants attended weekly (first year) and biweekly (second year) 90-minute standardized rehabilitation sessionsSessions focused on improving cardiovascular fitness, strength, flexibility, balance, posture, and gait patternCombination of two interventions: standardized mat/chair program and movement strategy training to improve gait and reduce freezing and risk of falls
Outcome Measures: Tinetti, New Freezing of Gait Questionnaire, PDQ-39
Conclusion: Combination of regular exercise and movement strategy training has the potential for reducing falls risk, and improving mobility, functional capacity, and quality of life in people with PD.

The effects of an exercise program on fall risk factors in people with parkinson’s disease: a randomized controlled trialAllen, et al. (2010)
Participants: 48 participants with idiopathic PD
Intervention: Participants were randomly allocated into a control or an exercise groupExercise group: Participated in a 40-60 minute program of progressive lower limb strengthening and balance exercises 3x/week for 6 months; attended a monthly exercise class; cueing strategies to reduce freezing during gait
Outcome Measures: PD falls risk score, swaymeter, alternate step-test component of BBS, Freeing of Gait Questionnaire, Falls Efficacy Scale-International questionnaire, PDQ-39
Conclusion: People with PD are able to exericse at home which results in improvement of freezing of gait, sit-to-stand time, overall falls risk, knee extensor muscle strength, fast walking speed, and fear of falling. Greater supervision may improve results by encouraging participants to exercise more often and at a higher intensity.

LVST BiG intervention
Based on the findings that hypokinesia movements are underlying impairments leading to decreases in movement speed
Started initially as a voice treatment focusing on movement amplitude, program developed based on same principles for movement
Focuses on need to practice large amplitude movements in order to obtain long-term changes in movement size
Involves intensive therapy lasting 60 minutes, 4 days/week for 4 weeks
(Kegelmeyer, 2014)
Comparing exercise in parkinson’s disease – the berlin big studyEbersbach et al. (2010)
Participants: 60 patients with PD
Intervention: Participants were assigned to Nordic walking, BIG intervention, or home programBIG intervention: 16 1-hour session, 50% of exercises consist of standardized whole-body movements with maximal amplitude, repetitive multidirectional movements, and stretching; second half of exercises includes goal-directed ADLs with high-amplitude movementsWalk group: 16 1-hour sessions consisting of a standardized protocol including warming up, practicing Nordic walking, and finally a cool down as sessions were performed in a local park with groups of 4-6 participantsHome: received 1-hour instruction of domestic training including stretching, and active workouts for muscular power and posture
Outcome Measures: UPDRS-III score, PDQ-39, TUG, time to walk 10 meters
Conclusion: Training BIG led to improved motor performance and was found to be more effective than Nordic walking and the home program.
Tango dancing
Used to capitalize on partnering to improve movement and the use of muscle to set the pace and cue movement
Studies have demonstrated improvement in the BBS and UPDRS demonstrating that tango dancing helps to improve functional balance
(Kegelmeyer, 2014)

Randomized controlled trial of community-based dancing to modify disease progression in parkinson disease
Duncan & Earhart (2012)
Participants: 62 participants clinically defined with PD
Intervention: Participants were randomly assigned to the Tango or control groupTango group: attended 2x weekly, 1-hour community based Argentine Tango classes for 12 months Control group: no prescribed exercise and were instructed to go about their lives as usual
Outcome Measures: MDS-UPDRS, MiniBESTest, Freezing of Gait Questionnaire, GAITrite, Nine-Hole Peg Test
Conclusion: Long-term participation in Tango dancing benefits people with PD, which may be attributed to the specific movements incorporated such as backwards walking, physical and cognitive challenges, low level aerobic activity, and movements challenging gait and balance while requiring high-level of multitasking.

Fall prevention
Multifactorial approach Environmental and intrinsic factors
Prescription of assistive device No research currently exists demonstrating that A.D.s actually
prevent falls, but they have looked at the impact on gait parameters Rollator walker has been shown to improve walking and safety,
producing least variability in all gait measurements
Falls diary Determine a pattern of falls Timing of medication? Time of day? Location of falls?
(Kegelmeyer, 2014)

recapParkinson’s Disease is the second most prevalent neurodegenerative
disease in the world
Important to encourage long-term planning for maintaining and improving ability to participate in activities
Initial goal of physical therapy should be aimed at prevention of associated problems
Create a long-term fitness program
As disease progresses, the shift must focus on including more task-based activities
Components of any program should include flexor stretching, balance exercises individualized to the patient, practice with larger movements, and use of repetition and functional practice

referencesAllen, N., Canning, C., Sherrington, C., Lord, S., Latt, M., Close, J.,
O’Rourke, S., Muray, S., & Fung, V. (2010). The effects of an exercise program on fall risk factors in people with Parkinson’s Disease: A randomized controlled trial. Movement Disorders, 25(9), 1217-1225. doi: 10.1002/mds.23082.
Duncan, R. & Earhart, G. (2011). Randomized controlled trial of community-based dancing to modify disease progression in Parkinson Disease. Neurorehabilitation and Neural Repair, 26, 132. doi: 10.1177/154596831142614.
Ebersbach, G., Ebersbach, A., Elder, D., Kaufhold, O., Kusch, M., Kupsch, A., & Wissel, J. (2010). Comparing exercise in Parkinson’s Disease – The Berlin BIG study. Movement Disorders, 00 (00), 000-000. doi: 10.1002/mds.23212.
Georgy, E., Barnsley, S., & Challeppa, R. (2011). Effect of physical exercise-movement strategies programme on mobility, falls, and quality of life in Parkinson’s disease. International Journal of Therapy and Rehabilitation, 19(2), 88-96.
Kegelmeyer, D. (2014). Examination and management of the client with Parkinson’s Disease. Western Schools.

questions