
PCMH Learning Community - Learning Session 2 Slide …c.ymcdn.com/sites/ · Learning Community...
51
6/5/2012 1 Learning Session 2 June 6, 2012 Welcome
Transcript of PCMH Learning Community - Learning Session 2 Slide …c.ymcdn.com/sites/ · Learning Community...
6/5/2012
1
Learning Session 2
June 6, 2012
Welcome
6/5/2012
2
Learning Community Structure
Assessments
Gap Analysis
Workplans
Learning Community Structure
• Webinars• Monthly, 1 hour long• Detailed explanation of each of the standards• Tutorial for use of NCQA submission tools• Practice transformation for certain standards
• Group Technical Assistance• Bi‐Weekly, 90 mins• PCMH content experts available to answer specific questions
• Regular check‐ins on progress of the work
6/5/2012
3
Learning Community Structure
Learning Sessions• Collaborative learning on PCMH, practice
transformation• Over half of the day is action• Impart training around content areas• Share best practices from various centers• Encourage unity amongst centers around healthcare
initiatives• A chance to meet other committed community
health staff
AgendaAM (1 break)
• PCMH Ice Breaker
• Sustainability
• PCMH Standard 6 ‐ Quality
LUNCH (60 minutes)
PM (1 break)
• PCMH: Before and After
• PCMH 2D – Population Management
• The Patient Experience
6/5/2012
4
Patient Centered Soul Scramble
• Let’s stand up and meet colleagues with the same letter at the respective easel
• At your easel is an envelope with letters
• The letters make up a word(s) related to PCMH
6/5/2012
5
• Unscramble the letters to identify the medical home concept
• List what comes to mind when you hear that word/concept
• Think of a dance that would best represent that word/concept
7 mins
Patient Centered Soul Scramble
You CAN Use

6/5/2012
6
6 Principles of Sustainability
1. Management Prioritizes Goal
All principles adapted from: 5 Million Lives Campaign. Getting Started Kit: Rapid Response Teams. Cambridge, MA: Institute for Healthcare Improvement; 2008. (Available at www.ihi.org)
6 Principles of Sustainability
2. Foolproof Change
All principles adapted from: 5 Million Lives Campaign. Getting Started Kit: Rapid Response Teams. Cambridge, MA: Institute for Healthcare Improvement; 2008. (Available at www.ihi.org)
6/5/2012
7
6 Principles of Sustainability
3. Transparent Feedback Systems
All principles adapted from: 5 Million Lives Campaign. Getting Started Kit: Rapid Response Teams. Cambridge, MA: Institute for Healthcare Improvement; 2008. (Available at www.ihi.org)
6 Principles of Sustainability
4. Clinic‐Wide Understanding of Improvement Process
All principles adapted from: 5 Million Lives Campaign. Getting Started Kit: Rapid Response Teams. Cambridge, MA: Institute for Healthcare Improvement; 2008. (Available at www.ihi.org)
6/5/2012
8
6 Principles of Sustainability
5. Staff Engaged in a Culture of Improvement
All principles adapted from: 5 Million Lives Campaign. Getting Started Kit: Rapid Response Teams. Cambridge, MA: Institute for Healthcare Improvement; 2008. (Available at www.ihi.org)
6 Principles of Sustainability
6. Capacity Building Programs
All principles adapted from: 5 Million Lives Campaign. Getting Started Kit: Rapid Response Teams. Cambridge, MA: Institute for Healthcare Improvement; 2008. (Available at www.ihi.org)

6/5/2012
9
You CAN Use
MEASURE PERFORMANCE
Standard 6 A
6/5/2012
10
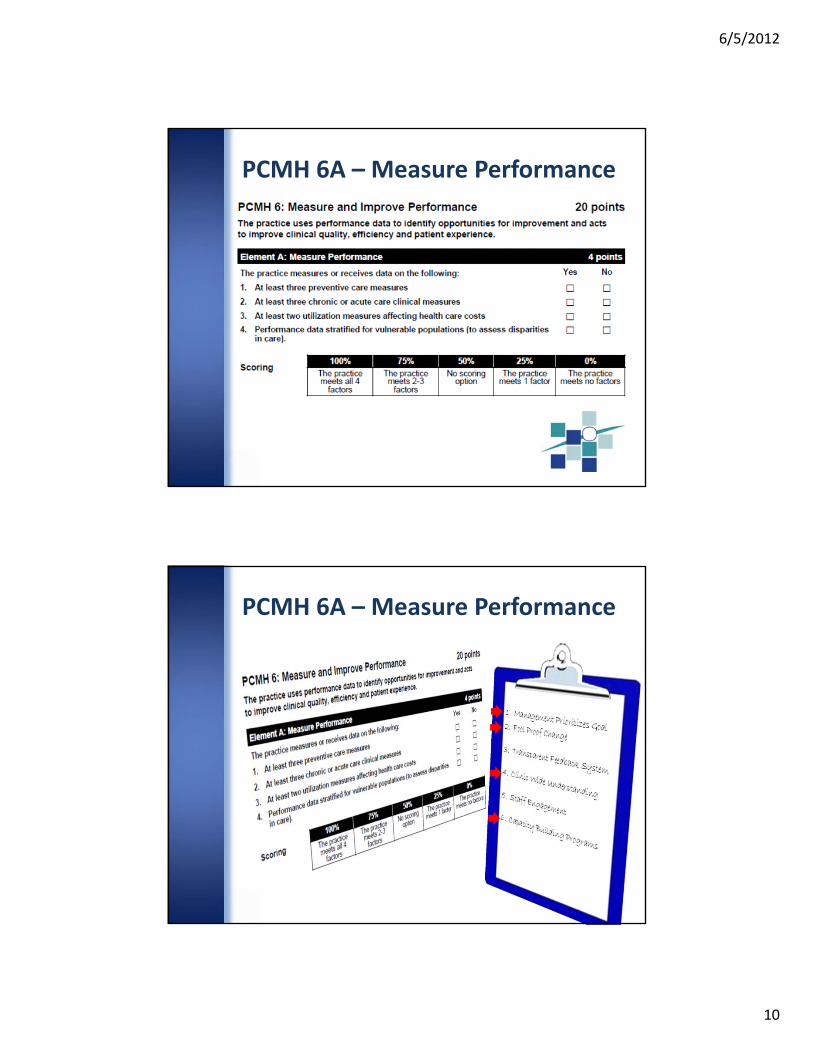
PCMH 6A – Measure Performance
PCMH 6A – Measure Performance
6/5/2012
11
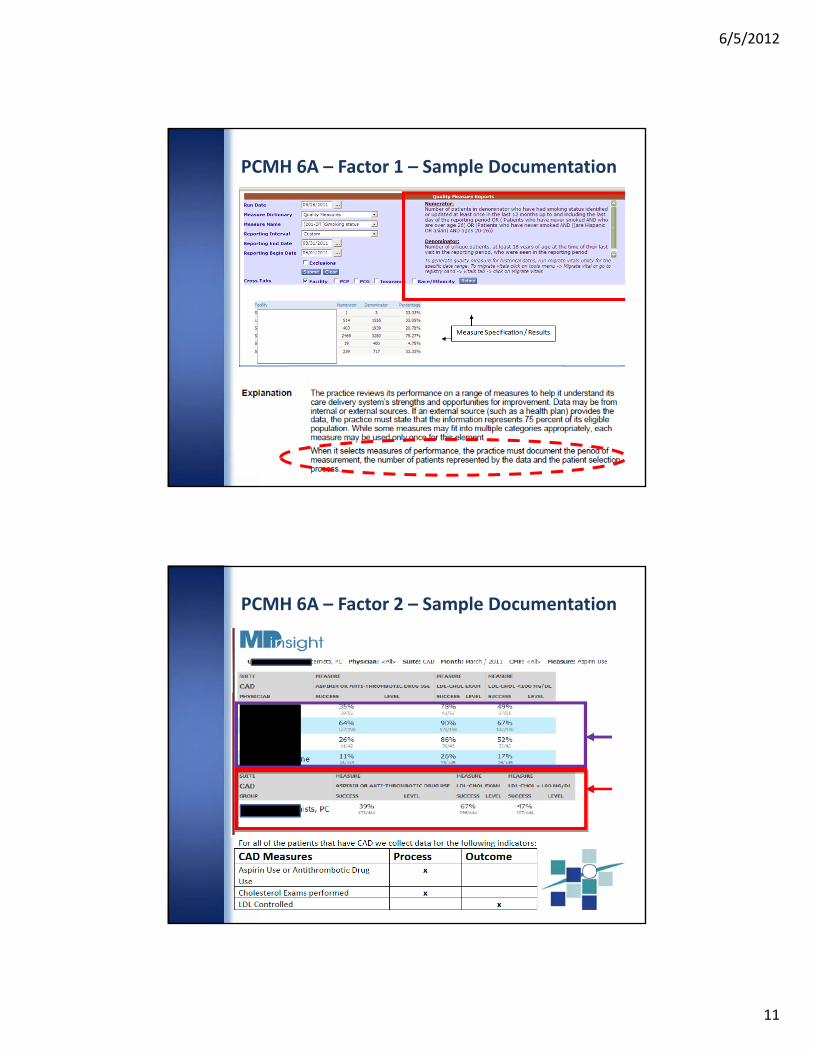
PCMH 6A – Factor 1 – Sample Documentation
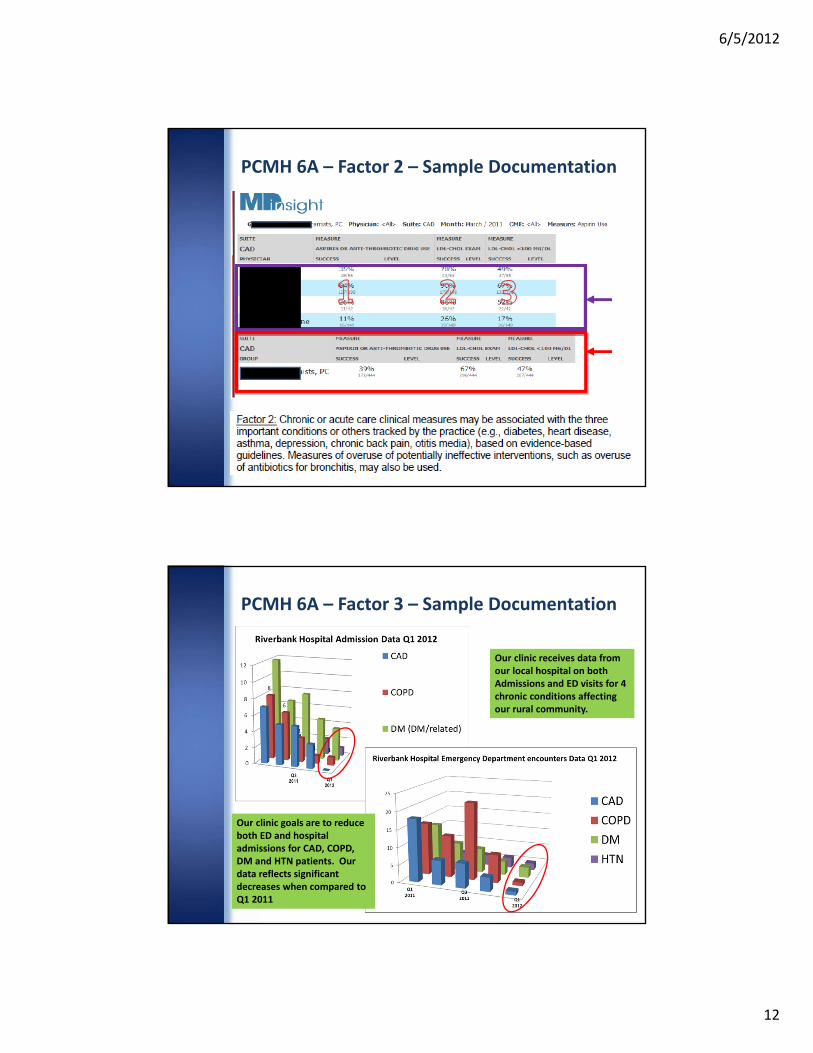
PCMH 6A – Factor 2 – Sample Documentation
6/5/2012
12
PCMH 6A – Factor 2 – Sample Documentation
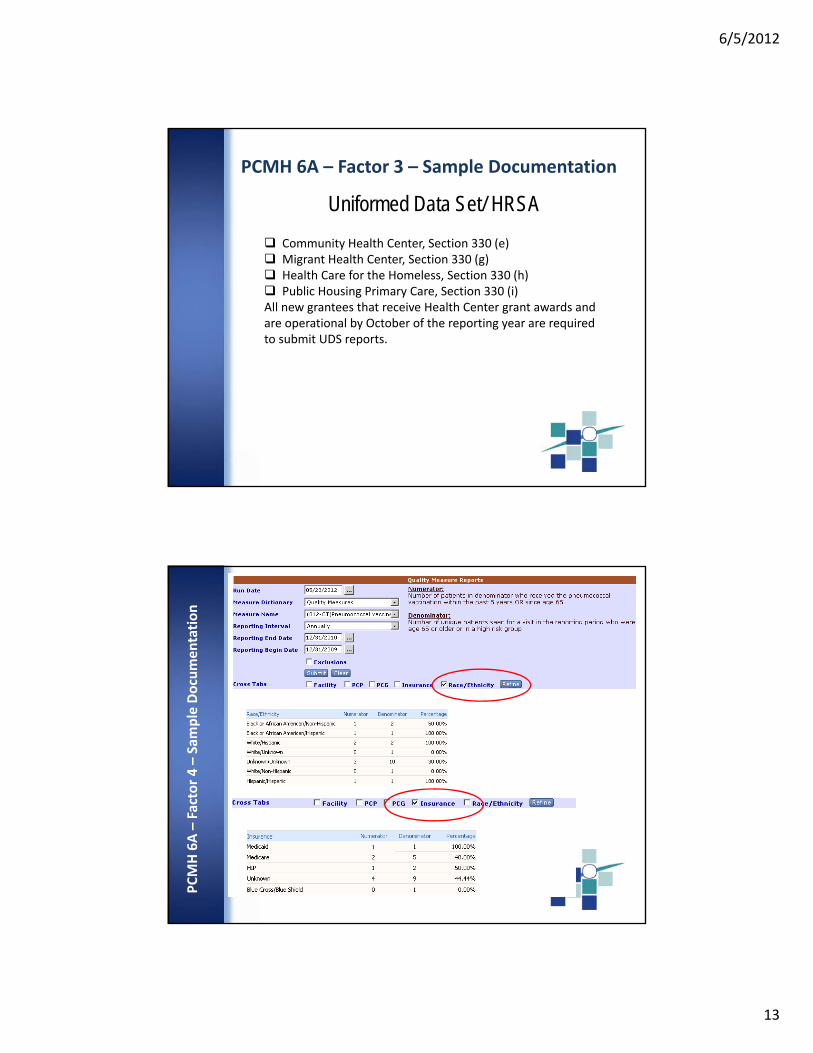
Our clinic receives data from our local hospital on both Admissions and ED visits for 4 chronic conditions affecting our rural community.
Our clinic goals are to reduce both ED and hospital admissions for CAD, COPD, DM and HTN patients. Our data reflects significant decreases when compared to Q1 2011
PCMH 6A – Factor 3 – Sample Documentation
6/5/2012
13
Community Health Center, Section 330 (e) Migrant Health Center, Section 330 (g) Health Care for the Homeless, Section 330 (h) Public Housing Primary Care, Section 330 (i)All new grantees that receive Health Center grant awards and are operational by October of the reporting year are required to submit UDS reports.
Uniformed Data Set/ HRSA
PCMH 6A – Factor 3 – Sample DocumentationPCMH 6A –Factor 4 –Sample Documentation
6/5/2012
14
Element 6A – Activity – Measures Race
• “Measures Race” Sheet• List 3 preventative care measures reviewed by QI committee or clinical committee
• List 3 acute or chronic care measures reviewed by QI committee or clinical committee
• List either 2 utilization measures or one measure that you stratify vulnerable patient populations for
7 mins
When sheet is completed, send a representative to the front for review
Element 6A – Activity – Measures Race

6/5/2012
15
Element 6A – Activity – Measures Race
What measures are we tracking?
Element 6A – Activity – Vulnerable Patients
• Understanding interventions closely relates to understanding populations
• Think about quality measures that may be heavier on a “vulnerable population”
• Looking at our current QI measures for a specific population
• Having UDS Measures makes this easier

6/5/2012
16
Element 6A – Activity – Vulnerable Patients
1 Choose a clinical measure 2 Subset Vulnerable Population
3 Re‐write out new measure & brainstorm intervention
Element 6A – Activity – Vulnerable Patients
4 Ideas of how to engage staff

6/5/2012
17
BREAK
PCMH Element 6C: Implement Continous
QI
6/5/2012
18
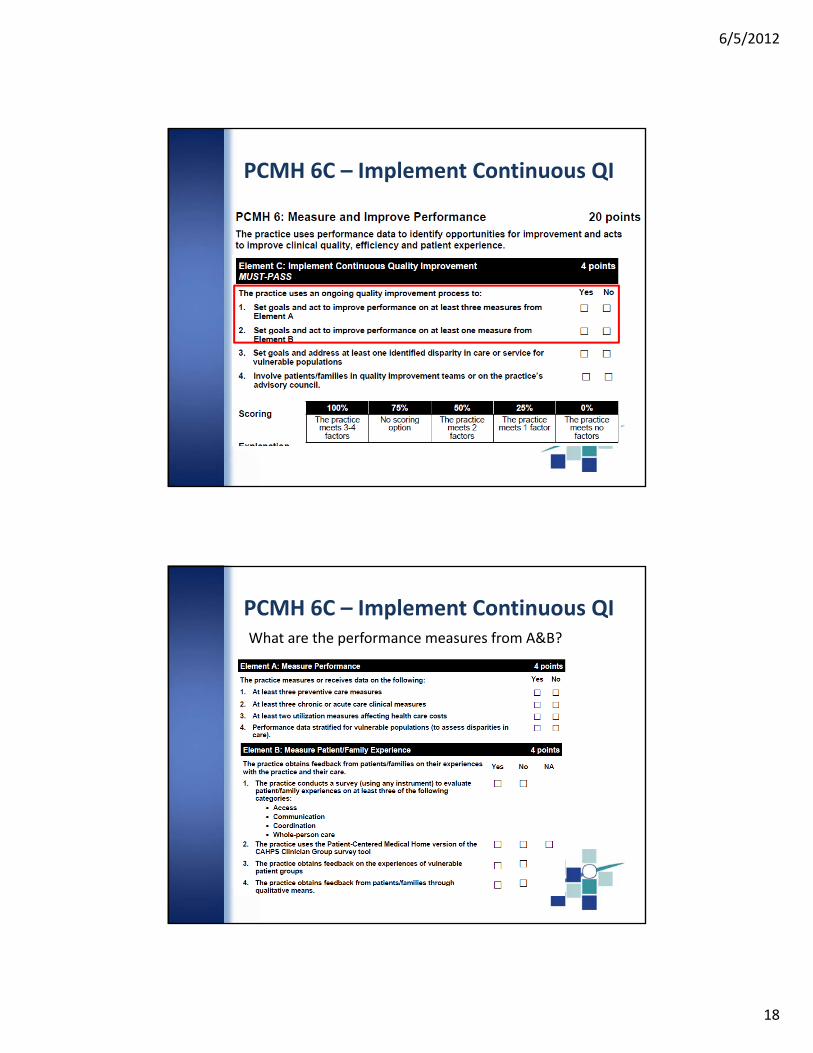
PCMH 6C – Implement Continuous QI
What are the performance measures from A&B?
PCMH 6C – Implement Continuous QI
6/5/2012
19
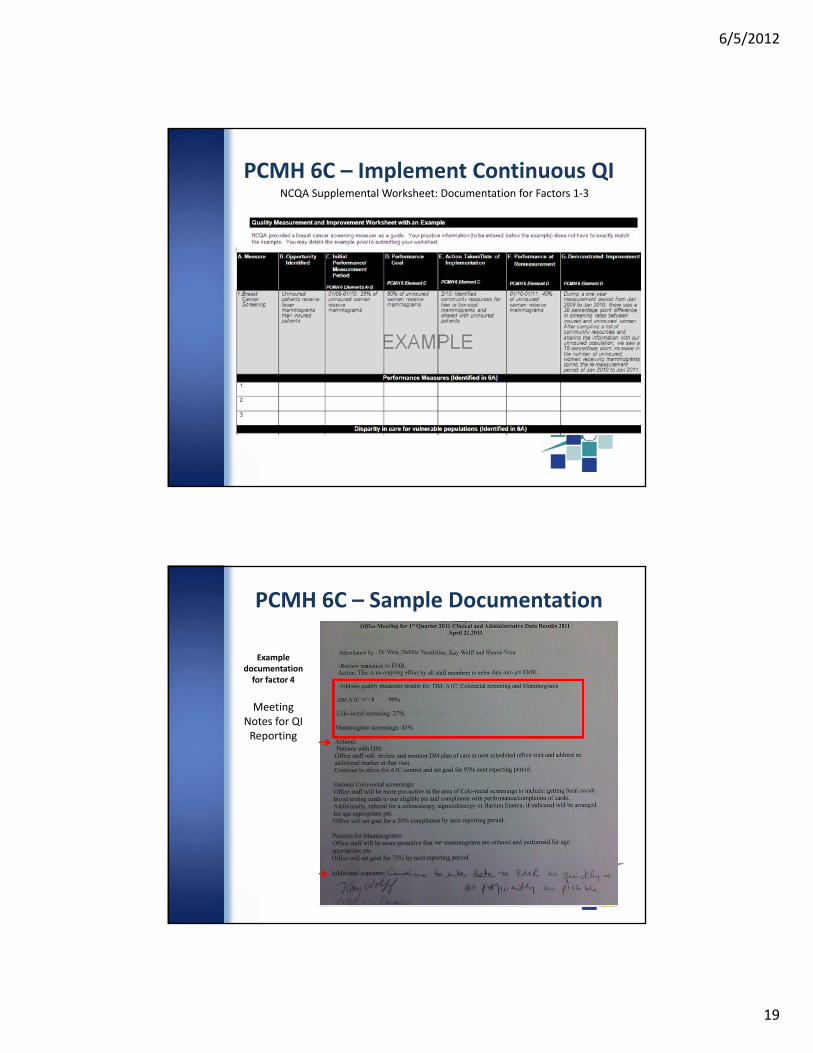
NCQA Supplemental Worksheet: Documentation for Factors 1‐3
PCMH 6C – Implement Continuous QI
Example documentation for factor 4
Meeting Notes for QI Reporting
PCMH 6C – Sample Documentation

6/5/2012
20
Activity Time
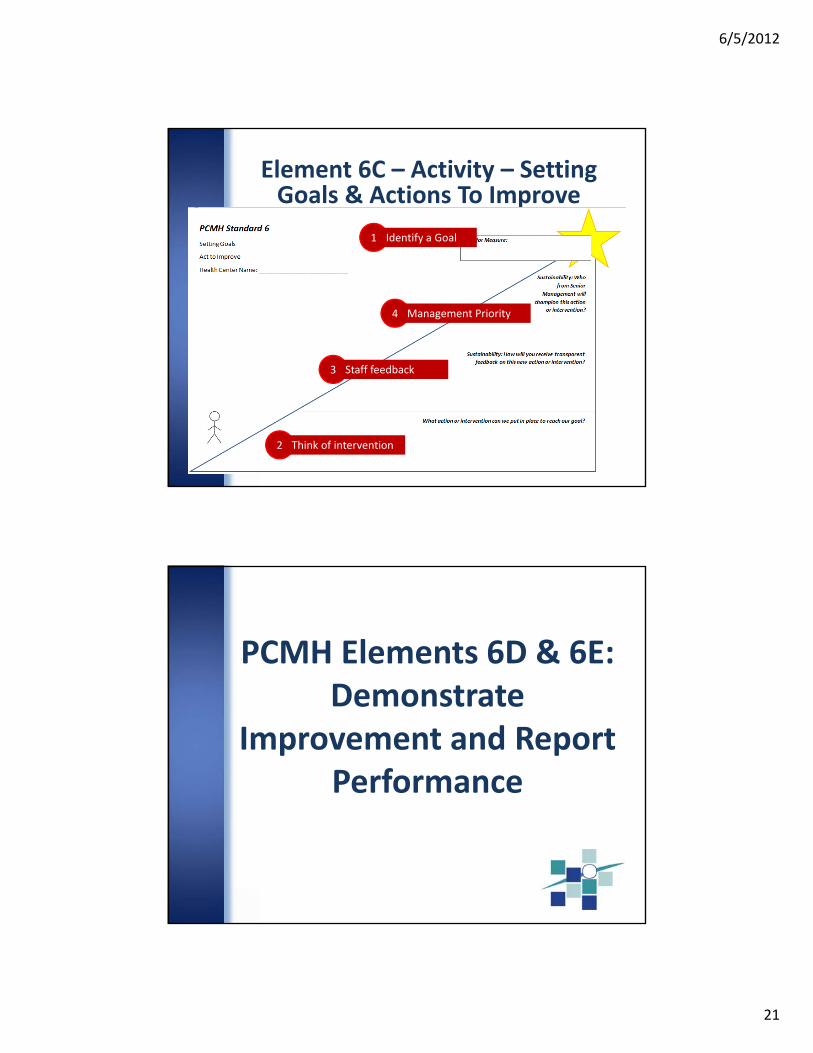
Element 6C – Activity – Setting Goals & Actions To Improve
• NCQA wants to see you set goals and act to improve
• Think about a reasonable goal for QI measure you selected from the previous activity
• Plan at least one intervention to address this goal and measure
• Sustainability: Transparent feedback and management priority
6/5/2012
21
Element 6C – Activity – Setting Goals & Actions To Improve
1 Identify a Goal
2 Think of intervention
3 Staff feedback
4 Management Priority
PCMH Elements 6D & 6E: Demonstrate
Improvement and Report Performance
6/5/2012
22
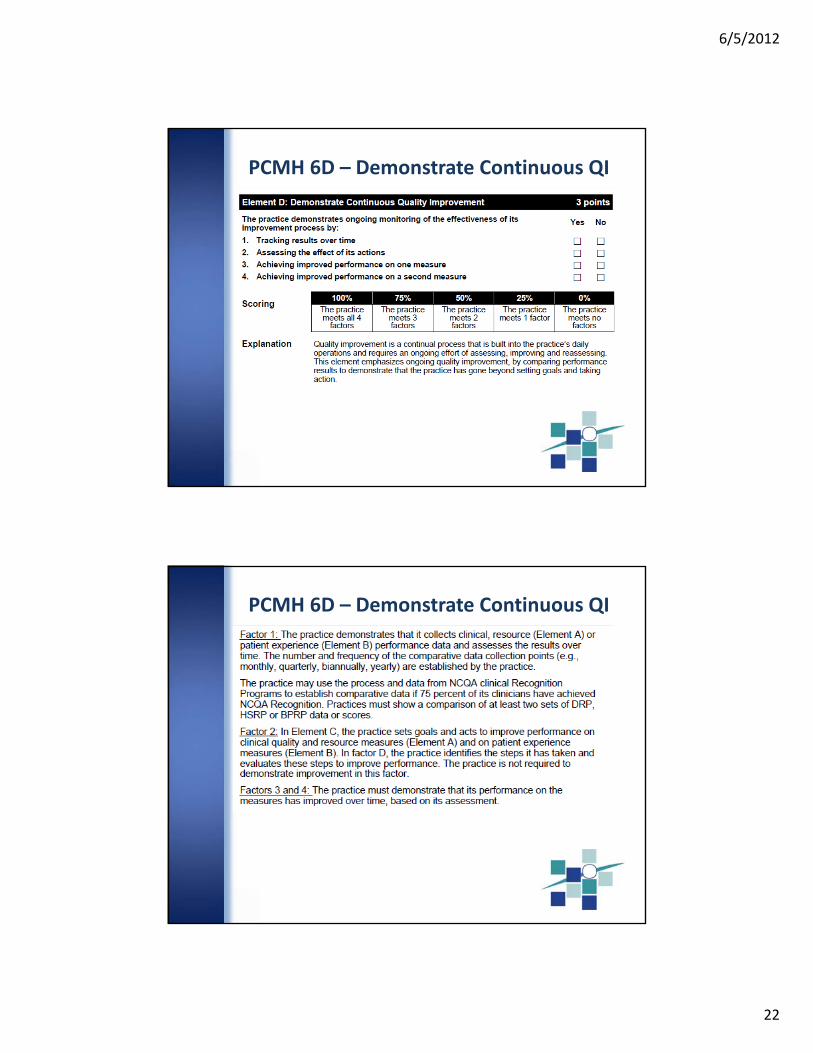
PCMH 6D – Demonstrate Continuous QI
PCMH 6D – Demonstrate Continuous QI
6/5/2012
23
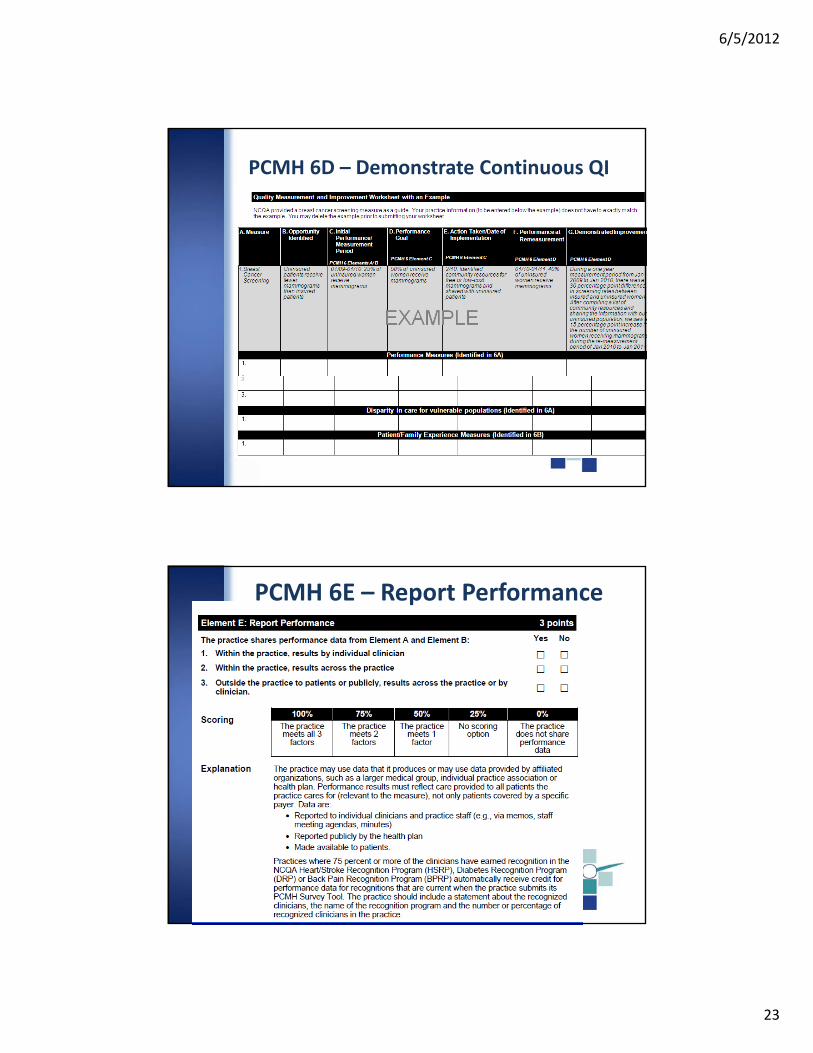
PCMH 6D – Demonstrate Continuous QI
PCMH 6E – Report Performance
6/5/2012
24
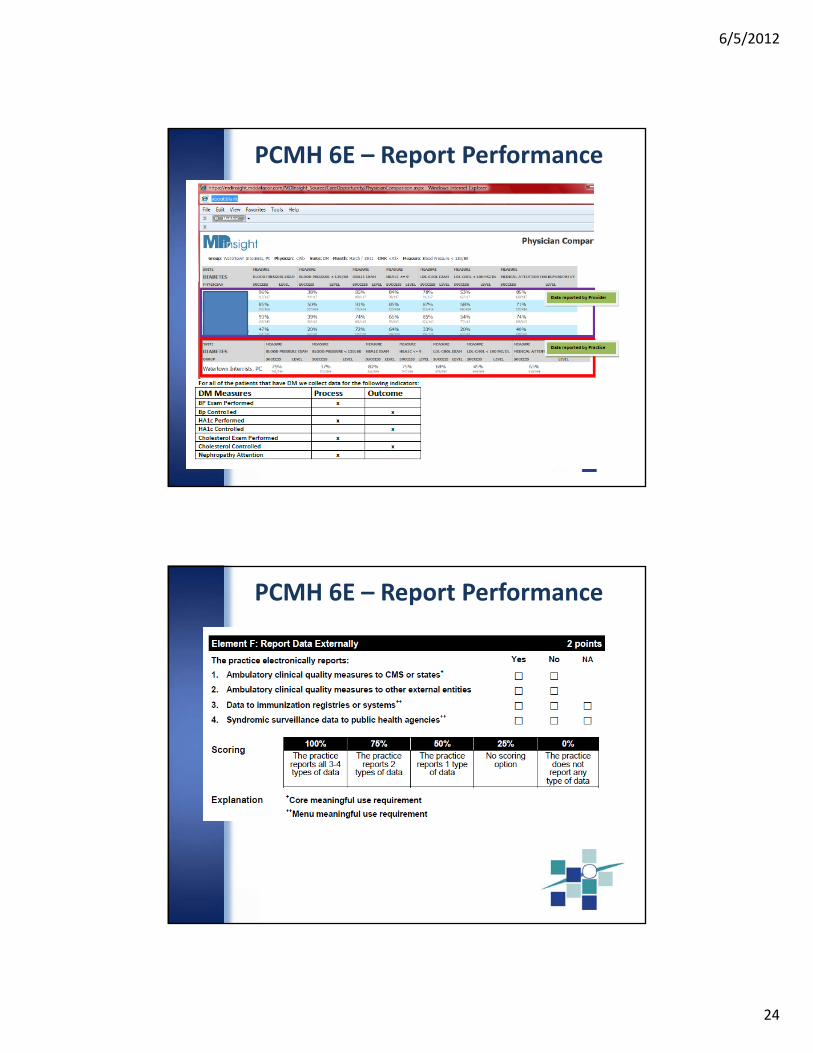
PCMH 6E – Report Performance
PCMH 6E – Report Performance

6/5/2012
25
Core Measures for all EP's Medicaid and Medicare
Measure Recommended Measure Title Recommended Measure Description
0013 AMA Hypertension: Blood Pressure Measurement
Percentage of patient visits for patients aged 18 years and older with a diagnosis of hypertension who have been seen for at least 2 office visits, with blood pressure (BP) recorded.
0028a AMAPreventive Care and Screening Measure Pair: a.Tobacco Use
Assessment
Percentage of patients aged 18 years or older who have been seen for at least 2 office visits, who were queried about tobacco use one or more times within 24 months.
0028b AMAPreventive Care and Screening Measure Pair: b.Tobacco
Cessation Intervention
Percentage of patients aged 18 years and older identified as tobacco users within the past 24 months who received cessation intervention.
0421 QIP Adult Weight Screening and Follow‐Up
Percentage of patients aged 18 years and older with a calculated BMI in the past six months or during the current visit documented in the medical record AND if the most recent BMI is outside parameters, a follow‐up plan is documented.
Alternate Core for all EP's Medicaid and Medicare
0024 NCQAWeight Assessment and Counseling for Children and
Adolescents
The percentage of patients 2‐17 years of age who had an outpatient visit with a PCP or OB/GYN and who had evidence of BMI percentile documentation, counseling for nutrition and counseling for physical activity during the measurement year.
0038 NCQA Childhood immunization Status
The percentage of children 2 years of age who had four diphtheria, tetanus and acellular pertussis (DTaP); three polio (IPV); one measles, mumps and rubella (MMR); two H influenza type B (HiB); three hepatitis B (Hep B), one chicken pox (VZV); four pneumococcal conjugate (PCV); two hepatitis A (Hep A); two or three rotavirus (RV); and two influenza (flu) vaccines by their second birthday. The measure calculates a rate for each vaccine and two separate combination rates.
0041 AMAPreventive Care and Screening: Influenza Immunization for
Patients ≥ 50 Years Old
Percentage of patients aged 50 years and older who received an influenza immunization during the flu season (September through February).
PCMH 6E – Report Performance – CMS
PCMH 6E – Report Performance – CMS
6/5/2012
26
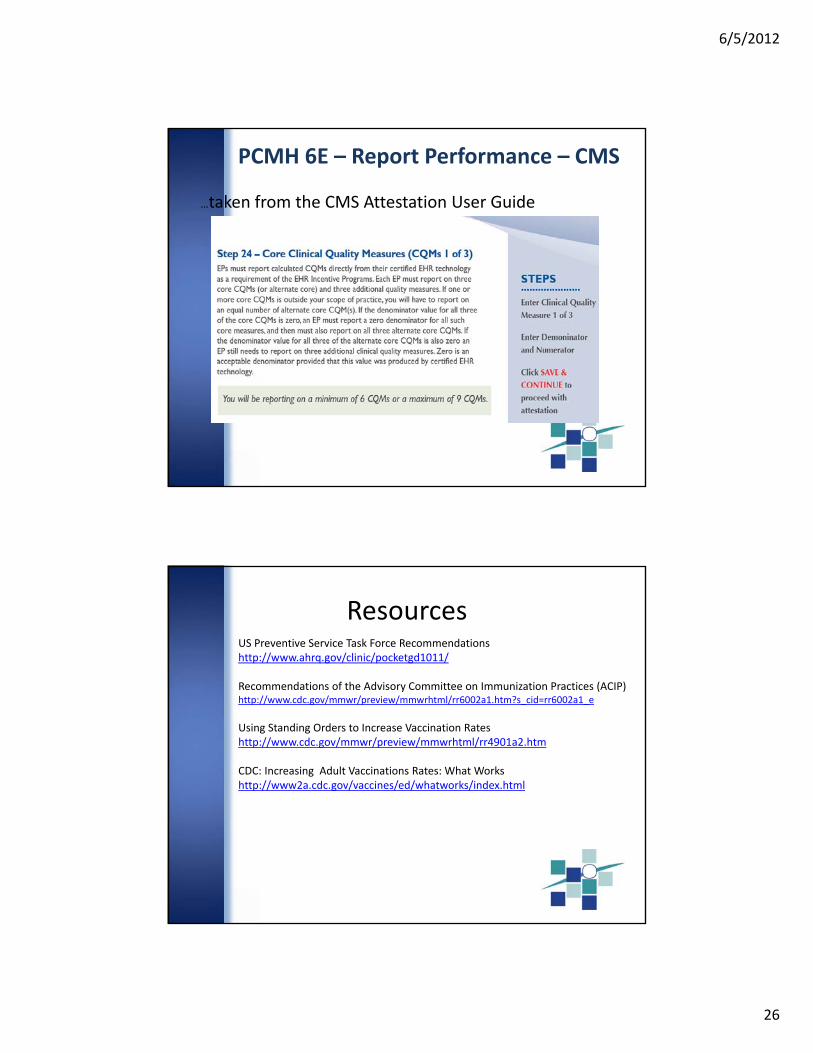
…taken from the CMS Attestation User Guide
PCMH 6E – Report Performance – CMS
US Preventive Service Task Force Recommendationshttp://www.ahrq.gov/clinic/pocketgd1011/
Recommendations of the Advisory Committee on Immunization Practices (ACIP)http://www.cdc.gov/mmwr/preview/mmwrhtml/rr6002a1.htm?s_cid=rr6002a1_e
Using Standing Orders to Increase Vaccination Rateshttp://www.cdc.gov/mmwr/preview/mmwrhtml/rr4901a2.htm
CDC: Increasing Adult Vaccinations Rates: What Workshttp://www2a.cdc.gov/vaccines/ed/whatworks/index.html
Resources

6/5/2012
27
Questions
Spread The Word
6/5/2012
28
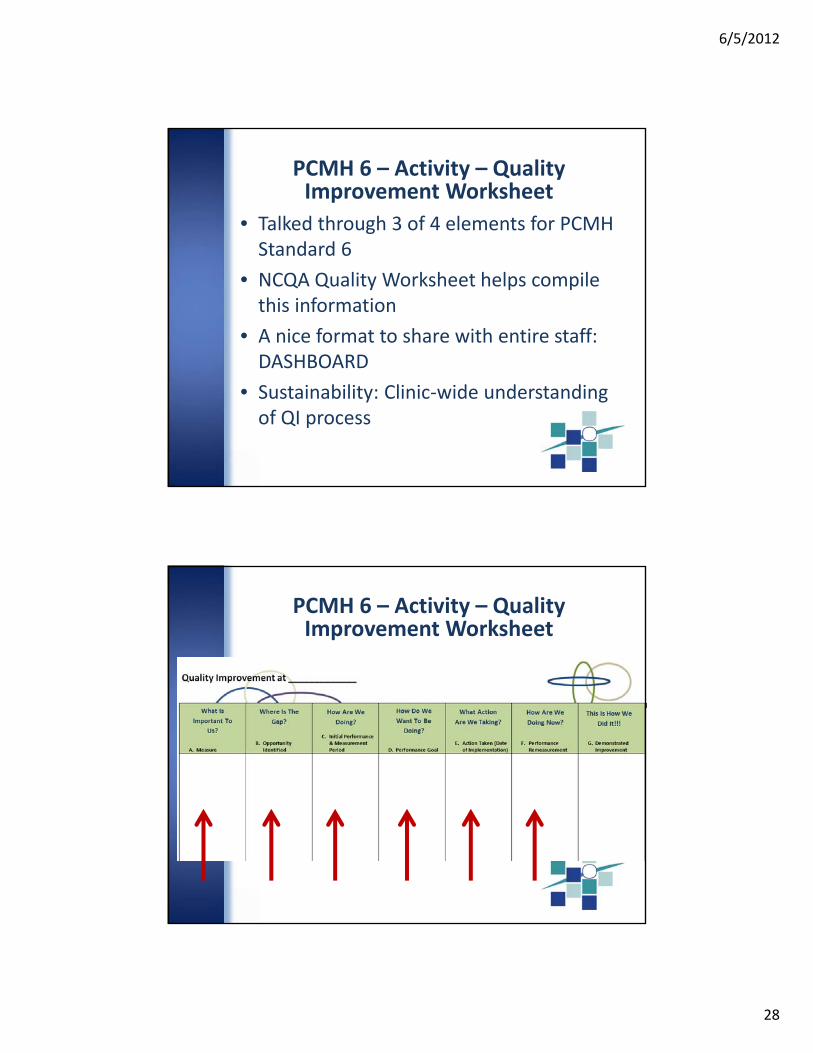
PCMH 6 – Activity – Quality Improvement Worksheet
• Talked through 3 of 4 elements for PCMH Standard 6
• NCQA Quality Worksheet helps compile this information
• A nice format to share with entire staff: DASHBOARD
• Sustainability: Clinic‐wide understanding of QI process
PCMH 6 – Activity – Quality Improvement Worksheet
6/5/2012
29
Spread The Word
Quiz
6/5/2012
30
Quiz – Question 1
Name a sustainability principle and give an example of what it looks like in a health center.
1) management prioritizes goals; 2) foolproof change; 3) transparent feedback systems; 4) clinic‐wide understanding of improvement process; 5) staff engaged in a culture of
improvement; 6) capacity building programs
Quiz – Question 2
True or False: the chronic or acute care clinical measures can be associated with the three important conditions tracked by the practice?
True
6/5/2012
31
Quiz – Question 3
What is a component of a clear and on‐going quality improvement strategy as defined by NCQA?
a. Guaranteed Success
b. Evaluation of performance against goals
c. Only the QI committee knows what QI initiatives are going on
d. Performance data is only reviewed once a year
LUNCH

6/5/2012
32
PCMH Before & After
Managing Patient
Populations
6/5/2012
33
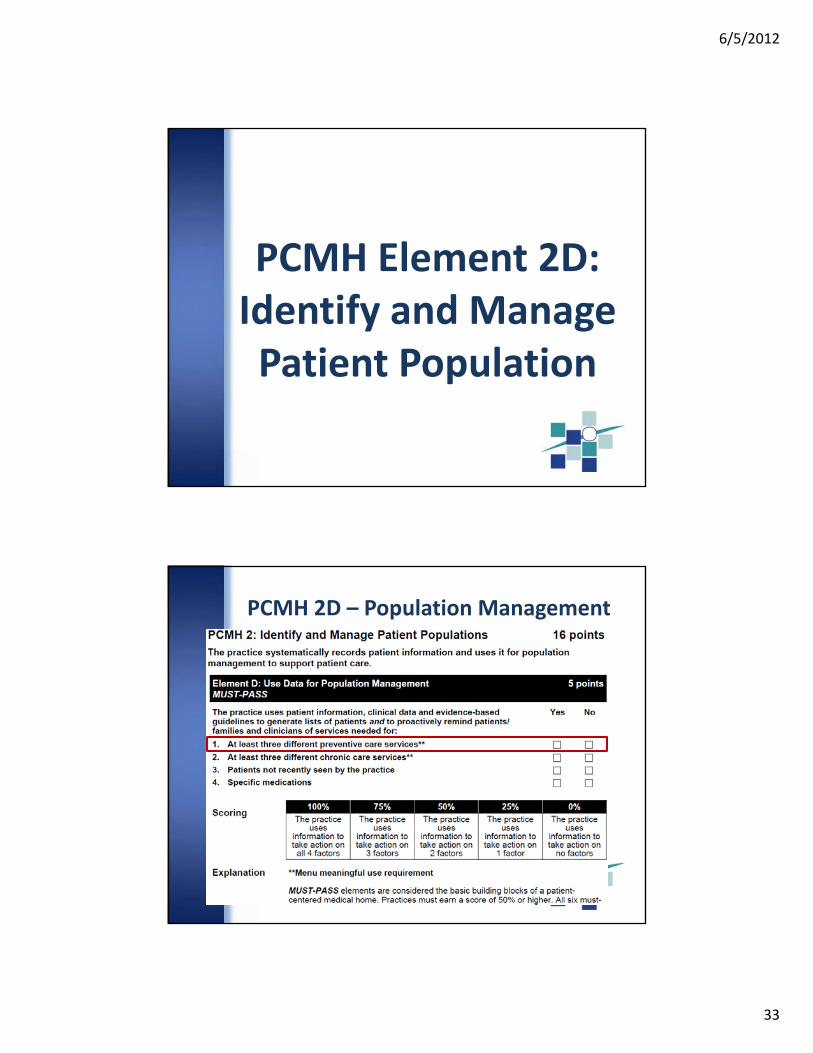
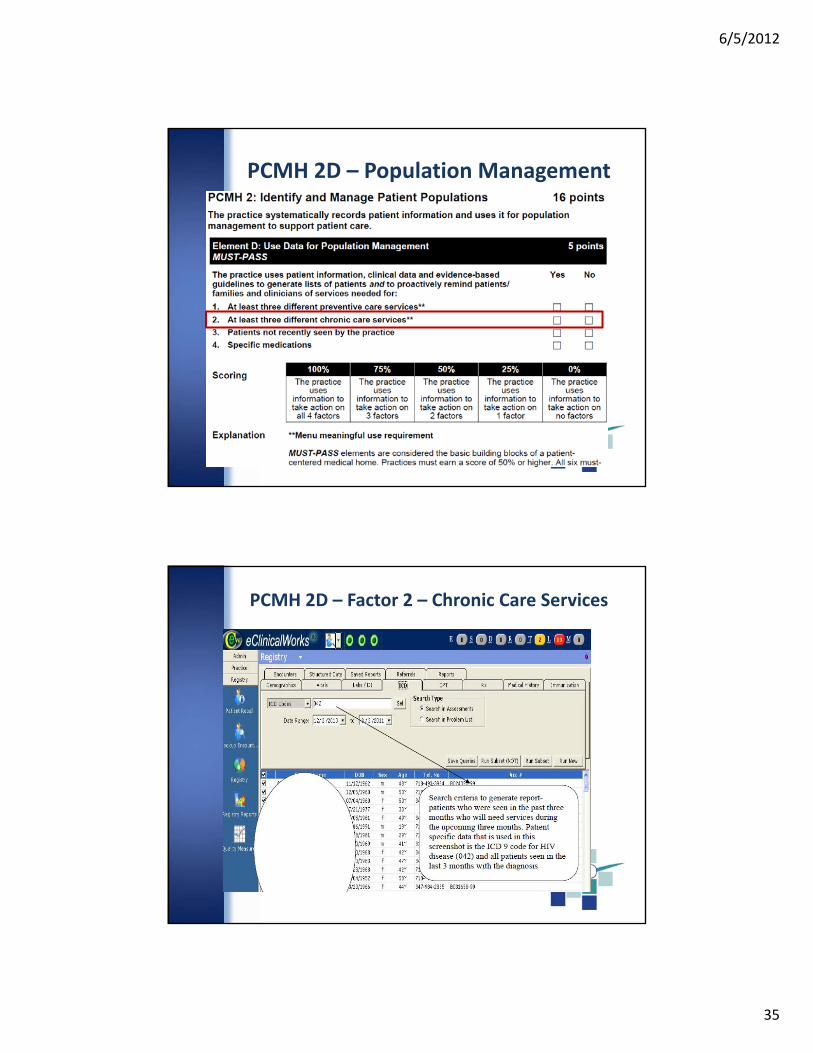
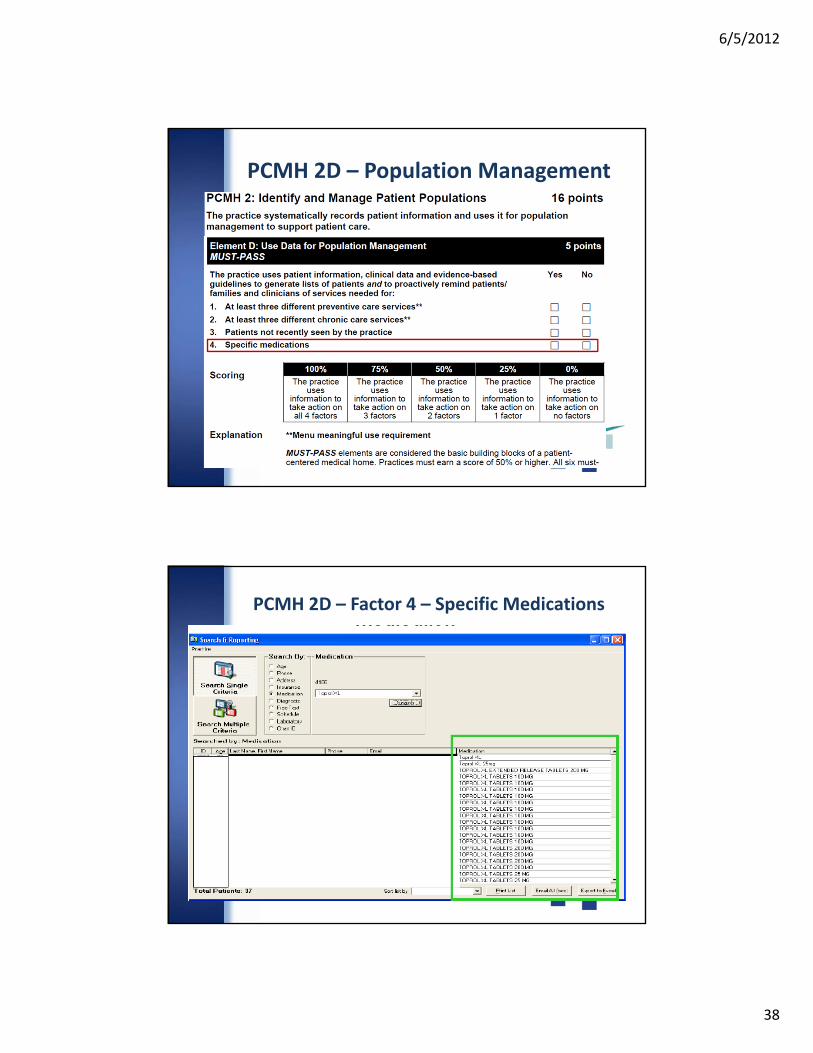
PCMH Element 2D: Identify and Manage Patient Population
PCMH 2D – Population Management
6/5/2012
34
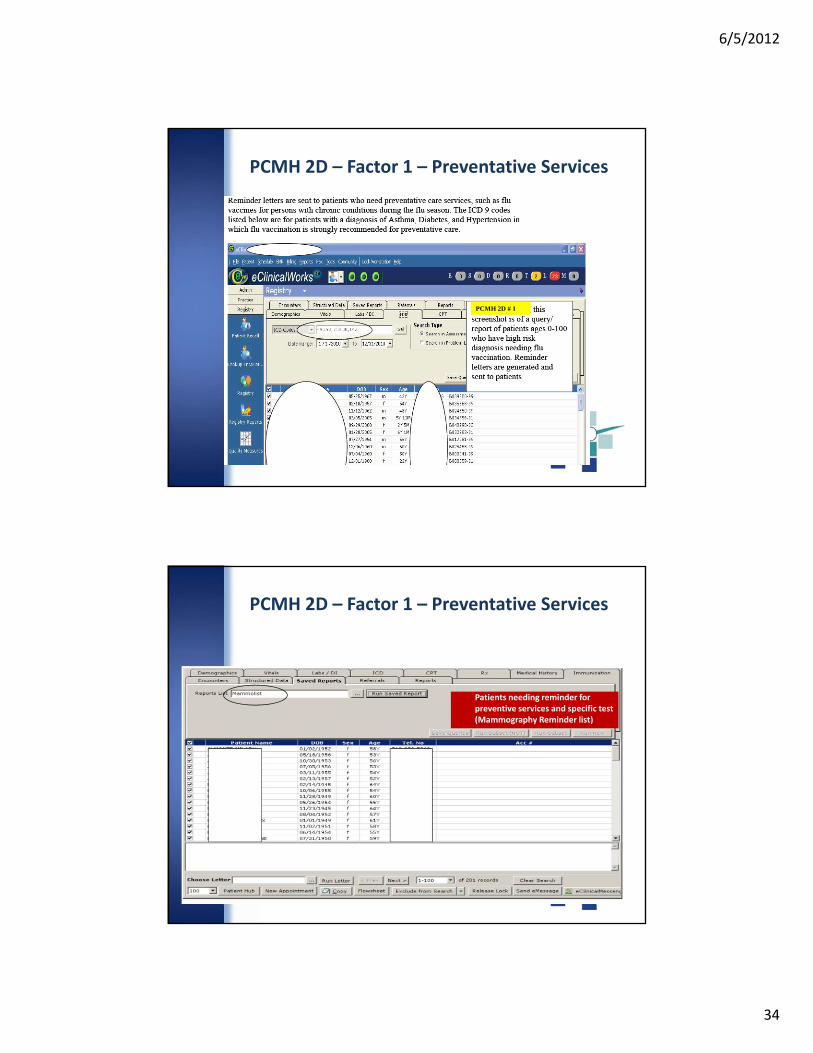
PCMH 2D # 1
PCMH 2D – Factor 1 – Preventative Services
PCMH 2D – Factor 1 – Preventative Services
Patients needing reminder for preventive services and specific test (Mammography Reminder list)
6/5/2012
35
PCMH 2D – Population Management
PCMH 2D – Factor 2 – Chronic Care Services
6/5/2012
36
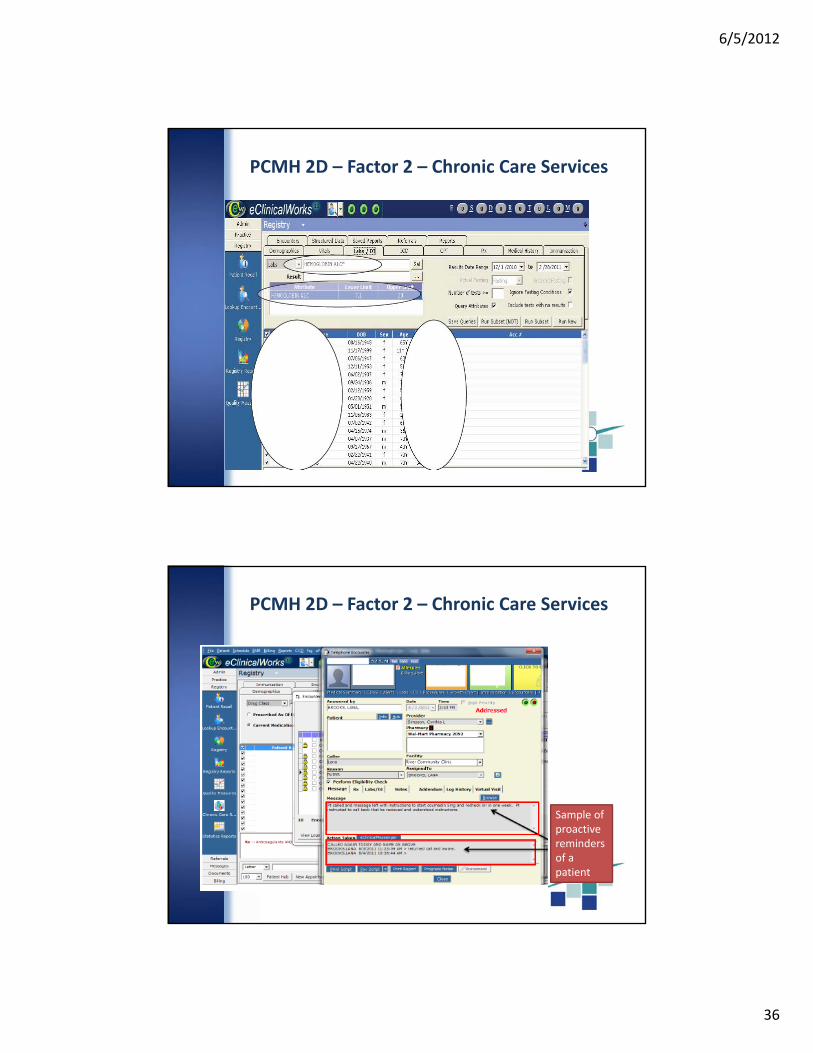
PCMH 2D – Factor 2 – Chronic Care Services
Sample of proactive reminders of a patient
PCMH 2D – Factor 2 – Chronic Care Services
6/5/2012
37
PCMH 2D – Population Management
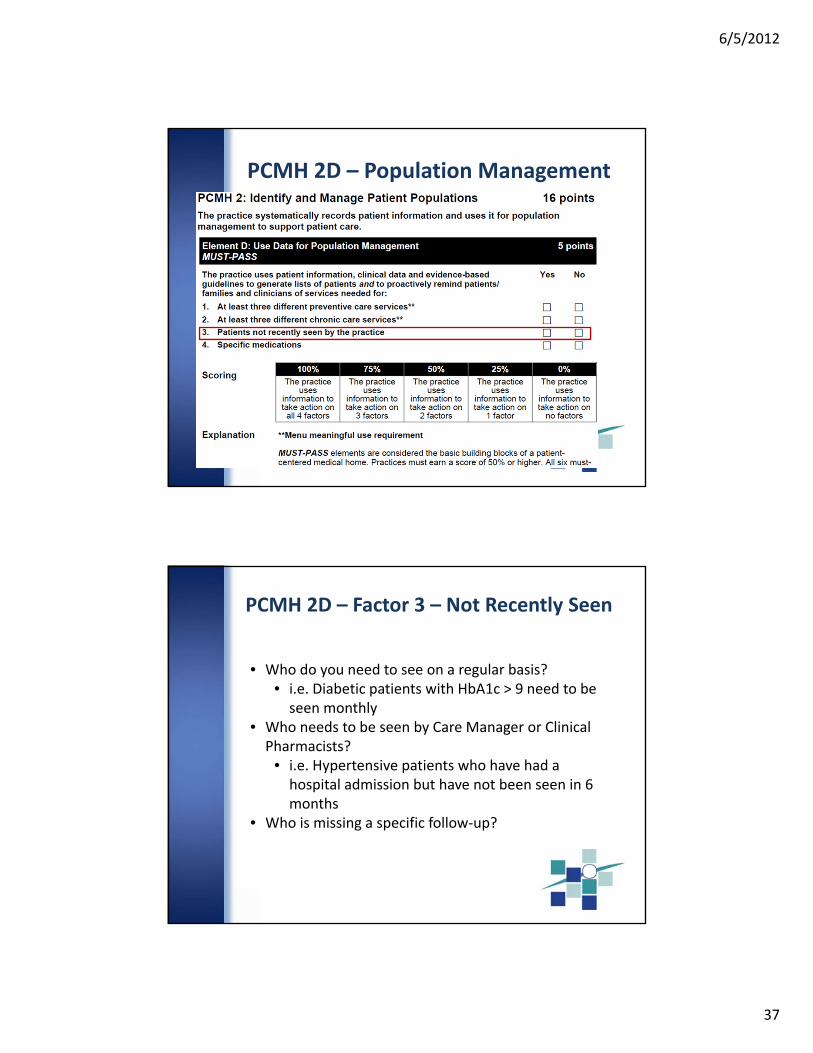
PCMH 2D – Factor 3 – Not Recently Seen
• Who do you need to see on a regular basis?• i.e. Diabetic patients with HbA1c > 9 need to be seen monthly
• Who needs to be seen by Care Manager or Clinical Pharmacists?
• i.e. Hypertensive patients who have had a hospital admission but have not been seen in 6 months
• Who is missing a specific follow‐up?
6/5/2012
38
PCMH 2D – Population Management
PCMH 2D – Factor 4 – Specific Medications
6/5/2012
39
Questions
PCMH Element 2D: Activity
6/5/2012
40
PCMH 2D Activity
Step 1: Using Part 1 worksheet, work as a team to select ONE preventive care service and ONE chronic care service
PCMH 2D Activity
Step 2: Using Part 2 worksheet work as a team to identify what registry you could create and what action you could take to address these gaps in services
Step 3: Who will be responsible? When will you start?
Step 4: What other resources will you need? How will you get them?
6/5/2012
41
PCMH Element 6B: Measure
Patient/Family Experience
Close Your Eyes
6/5/2012
42
PCMH 6B: Activity 1Goal: Experiencing what the patient experiences
1. Close your eyes and imagine you are a patient in the exam room waiting to see your doctor
2. When you feel like you’ve waited an appropriate amount of time for your doctor, open your eyes and stand up
Is this how long patients wait to see a provider at your health center?
Objectives
• Understand how patient experience relates to the medical home being “patient centered”
• Review of PCMH Standard 6, Element B

6/5/2012
43
New Focus on the Patient
PCMH 6B, Factor 1
6/5/2012
44
Patient Experience: Access
Sample questions:
– When you called to schedule this appointment, did you get an appointment as soon as you thought you needed one?
– In general, how often do you feel that you are able to get an appointment as soon as you think you need one?
Patient Experience: Communication
Sample questions:
– Did you have all of your concerns addressed and questions answered today?
– Did the nurse/provider communicate information about your health, medications and next steps in a way that was easy for you to understand?

6/5/2012
45
Patient Experience: Coordination of Care
Sample questions:– How often does your primary care physician seem informed and up‐to‐date about the care you got from a specialist?
– In the past year, did you and anyone in this provider’s office talk at each visit about all the prescription medicines you were taking?
Patient Experience: Self‐Management Support
Sample Questions:– In the past year, did you and anyone in this provider’s office talk about things in your life that worry you or cause stress?
– In the past year, did anyone in this provider’s office ask you if there are things that make it hard for you to take care of your health?

6/5/2012
46
PCMH 6B, Factor 2
Consumer Assessment of Healthcare Providers and Systems (CAHPS)
• Developed by the Agency for Healthcare Research and Quality (AHRQ)
• Practices can receive special acknowledgement from NCQA for administering the PCMH version of the CAHPS Clinical Group Survey Tool:
• Use specific method or vendor for collecting the data
• Report results to NCQA• Practices can compare benchmarks
6/5/2012
47
More Info on CAHPS
Please visit:
http://www.cahps.ahrq.gov/Surveys‐Guidance/CG/PCMH.aspx
Building Your Own Survey
• Written at a basic reading level
• Refer to specific activities
• Ensure responses can be tracked, analyzed, and compared
• Can include questions from CAHPS
6/5/2012
48
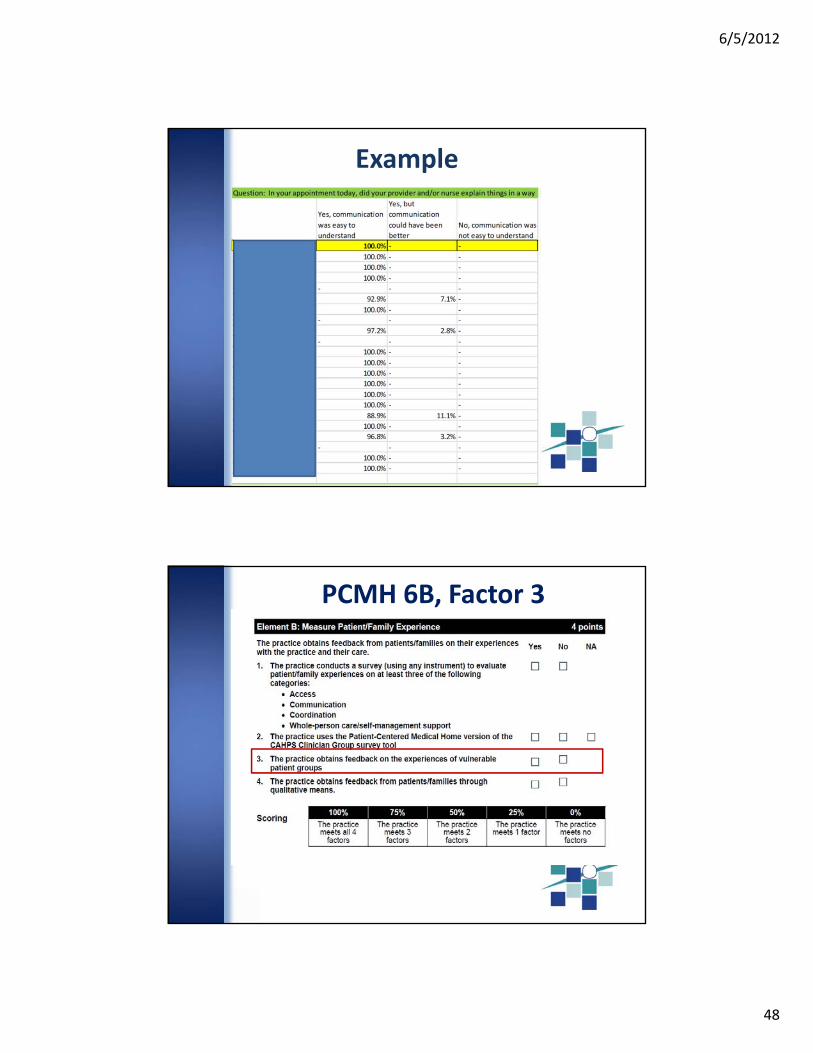
Example
PCMH 6B, Factor 3
6/5/2012
49
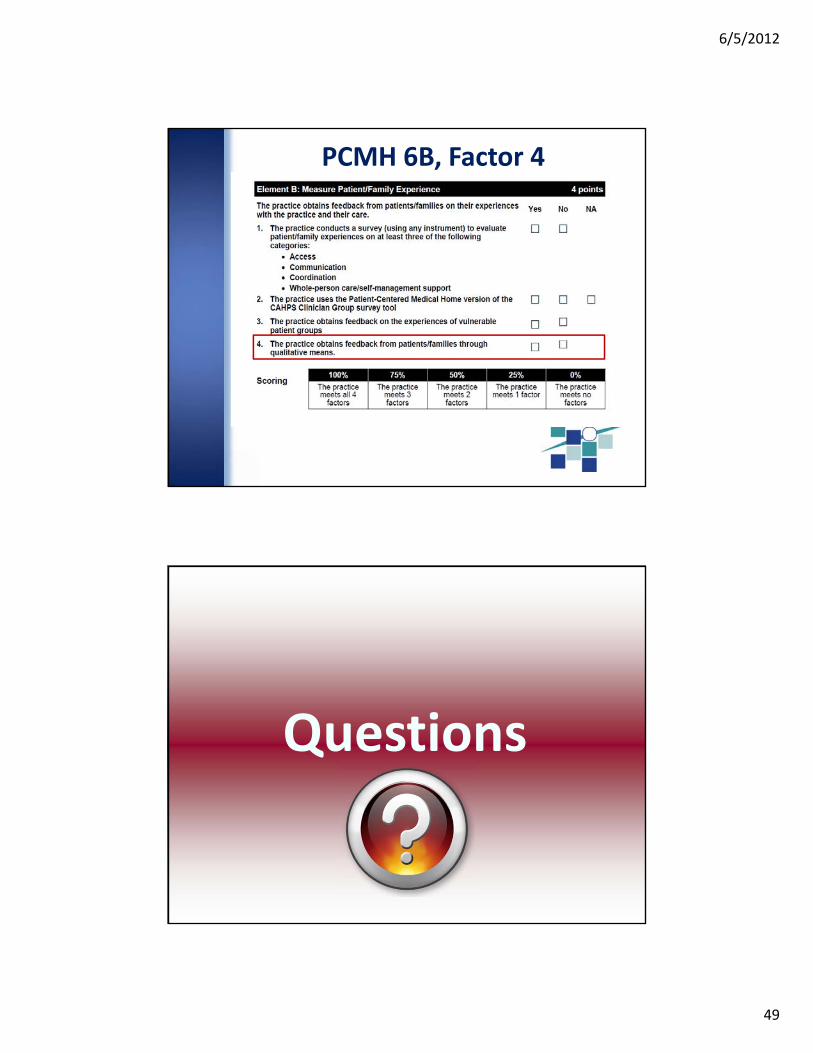
PCMH 6B, Factor 4
Questions
6/5/2012
50
BREAK
PCMH 6B: Activity 2
Let’s Move Around
Co‐Consulting Around Patient Experience
6/5/2012
51
PCMH 6B: Activity 2Goal: Think about patient experience from the patient’s perspective
1. Remember a time when you, as a patient, experienced something positive or negative related to one or more of the four patient experience categories (access, communication, coordination, self‐management).
2. Write down what questions you could ask on a patient experience survey that will let the health center staff know that they are doing well or poorly in that area.


















