PCI in a case of dual (type IV) LAD with anomalous origin ... · coronary sinus. This RCA was ... 4...
4
PCI in a case of dual (type IV) LAD with anomalous origin of the LCx from RCA Harinder K. Bali a,⇑ , Kapil Chattree a , Surinder K. Bali b , Hiteshi K.C. Chauhan a , C.P. Shukla a a Dept. of Cardiology, Fortis Hospital, Mohali; b Dept. of Medicine, Medical College, Jammu; a, b India Dual left anterior descending coronary artery (LAD) originating from the left main stem and the right coronary artery (type IV LAD) is a rare congenital anomaly. Its association with an anomalous origin of the left circumflex (LCx) from RCA is even rarer. We describe a patient presenting with acute inferior wall myocardial infarction, who was subsequently found to have this coronary anomaly. He underwent staged PCI of the dominant RCA and anomalous LCx successfully through the radial route. We conclude that anomalous coronaries can be safely and successfully treated through the radial route after careful evaluation of origin and course of the anomalous vessels. CT coronary angiography is extremely useful in delineating the vessel course and particularly their relation to great arteries. Ó 2013 Production and hosting by Elsevier B.V. on behalf of King Saud University. Keywords: Anomalous coronaries, Dual LAD, Radial PCI Introduction A dual left anterior descending (LAD) coronary artery originating from the left main stem and the right coronary artery (type IV LAD) in association with an anomalous left circumflex (LCx) from the right coronary artery (RCA) is an extremely rare coronary anomaly. Case A 60-year-old male was admitted with com- plaint of crescendo angina over a period of ten days. He had one episode of prolonged rest pain associated with diaphoresis lasting for 30 min. The electrocardiogram (EKG) revealed ST-seg- ment elevation in the inferior leads. Echocardiog- raphy revealed a left ventricular ejection fraction (LVEF) of 55% with mild hypokinesia of inferior wall. The patient was taken up for urgent coronary angiography (CAG) from the right radial artery with the intention of primary angioplasty. CAG revealed left main artery giving rise to a diminutive left anterior descending artery (LAD), which terminated in the proximal part of the P.O. Box 2925 Riyadh – 11461KSA Tel: +966 1 2520088 ext 40151 Fax: +966 1 2520718 Email: [email protected] URL: www.sha.org.sa Production and hosting by Elsevier CASE REPORT Disclosure: Authors have nothing to disclose with regard to commercial support. Received 1 April 2013; revised 11 June 2013; accepted 16 July 2013. Available online 26 July 2013 ⇑ Corresponding author. Address: Fortis Hospital, Sector 62, Phase VIII, Mohali, Punjab 160062, India. Tel.: +91 9872735980. E-mail address: [email protected] (H.K. Bali). 1016–7315 Ó 2013 Production and hosting by Elsevier B.V. on behalf of King Saud University. Peer review under responsibility of King Saud University. URL: www.ksu.edu.sa http://dx.doi.org/10.1016/j.jsha.2013.07.003
Transcript of PCI in a case of dual (type IV) LAD with anomalous origin ... · coronary sinus. This RCA was ... 4...
P.O. Box 2925 Riyadh – 11461KSATel: +966 1 2520088 ext 40151Fax: +966 1 2520718Email: [email protected]: www.sha.org.sa
CA
SE R
EPO
RTDisclosure: Authors have nothing to disclose with regard to commercialsupport.
Received 1 April 2013; revised 11 June 2013; accepted 16 July 2013.Available online 26 July 2013
⇑ Corresponding author. Address: Fortis Hospital, Sector 62, PhaseVIII, Mohali, Punjab 160062, India. Tel.: +91 9872735980.
E-mail address: [email protected] (H.K. Bali).PCI in a case of dual (type IV) LAD withanomalous origin of the LCx from RCA
Production and hosting by Elsevier
1016–7315 � 2013 Production and hosting by Elsevier B.V. on behalf of King Saud University.
Peer review under responsibility of King Saud University.
URL: www.ksu.edu.sa
http://dx.doi.org/10.1016/j.jsha.2013.07.003
Harinder K. Bali a,⇑, Kapil Chattree a, Surinder K. Bali b, Hiteshi K.C. Chauhan a,C.P. Shukla a
a Dept. of Cardiology, Fortis Hospital, Mohali; b Dept. of Medicine, Medical College, Jammu;a, b India
Dual left anterior descending coronary artery (LAD) originating from the left main stem and the right coronary artery(type IV LAD) is a rare congenital anomaly. Its association with an anomalous origin of the left circumflex (LCx) fromRCA is even rarer.
We describe a patient presenting with acute inferior wall myocardial infarction, who was subsequently found tohave this coronary anomaly. He underwent staged PCI of the dominant RCA and anomalous LCx successfullythrough the radial route.
We conclude that anomalous coronaries can be safely and successfully treated through the radial route aftercareful evaluation of origin and course of the anomalous vessels. CT coronary angiography is extremely useful indelineating the vessel course and particularly their relation to great arteries.
� 2013 Production and hosting by Elsevier B.V. on behalf of King Saud University.
Keywords: Anomalous coronaries, Dual LAD, Radial PCI
Introduction
Adual left anterior descending (LAD) coronaryartery originating from the left main stem
and the right coronary artery (type IV LAD) inassociation with an anomalous left circumflex(LCx) from the right coronary artery (RCA) is anextremely rare coronary anomaly.
Case
A 60-year-old male was admitted with com-plaint of crescendo angina over a period of ten
days. He had one episode of prolonged rest painassociated with diaphoresis lasting for 30 min.The electrocardiogram (EKG) revealed ST-seg-ment elevation in the inferior leads. Echocardiog-raphy revealed a left ventricular ejection fraction(LVEF) of 55% with mild hypokinesia of inferiorwall.
The patient was taken up for urgent coronaryangiography (CAG) from the right radialartery with the intention of primary angioplasty.CAG revealed left main artery giving rise to adiminutive left anterior descending artery (LAD),which terminated in the proximal part of the
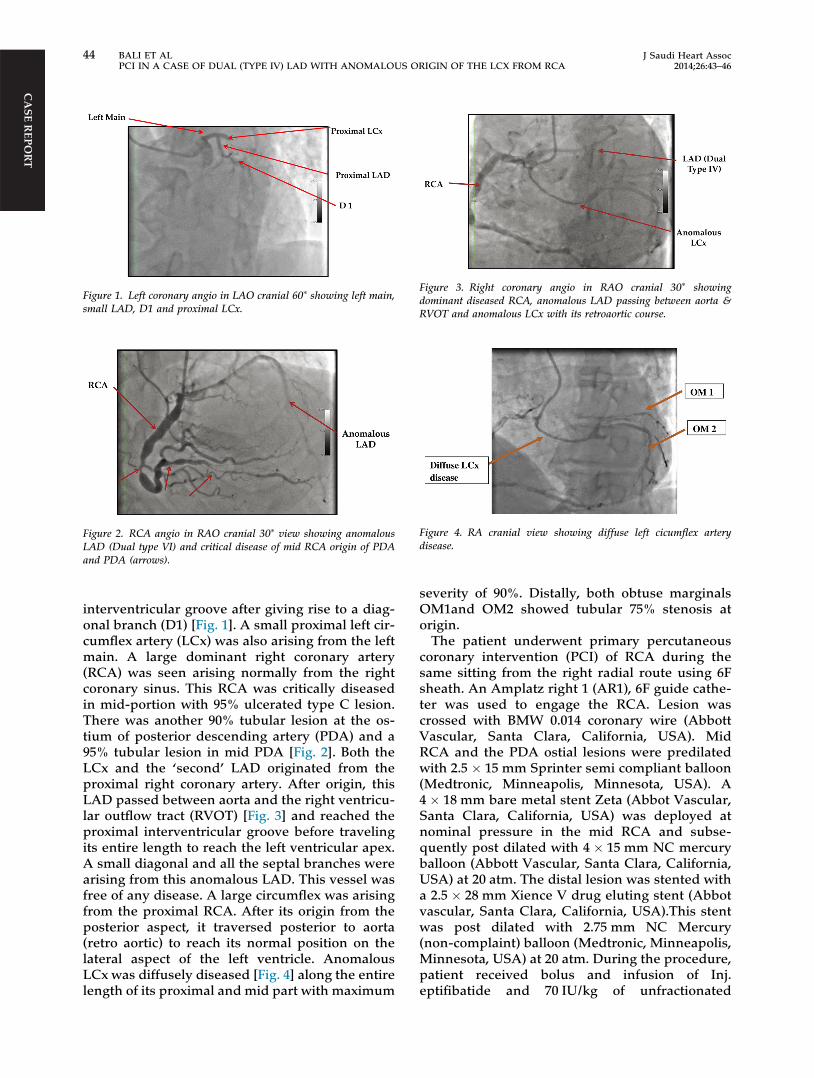
Figure 1. Left coronary angio in LAO cranial 60⁄ showing left main,small LAD, D1 and proximal LCx.
Figure 2. RCA angio in RAO cranial 30⁄ view showing anomalousLAD (Dual type VI) and critical disease of mid RCA origin of PDAand PDA (arrows).
Figure 3. Right coronary angio in RAO cranial 30⁄ showingdominant diseased RCA, anomalous LAD passing between aorta &RVOT and anomalous LCx with its retroaortic course.
Figure 4. RA cranial view showing diffuse left cicumflex arterydisease.
CA
SE REPO
RT
44 BALI ET ALPCI IN A CASE OF DUAL (TYPE IV) LAD WITH ANOMALOUS ORIGIN OF THE LCX FROM RCA
J Saudi Heart Assoc2014;26:43–46
interventricular groove after giving rise to a diag-onal branch (D1) [Fig. 1]. A small proximal left cir-cumflex artery (LCx) was also arising from the leftmain. A large dominant right coronary artery(RCA) was seen arising normally from the rightcoronary sinus. This RCA was critically diseasedin mid-portion with 95% ulcerated type C lesion.There was another 90% tubular lesion at the os-tium of posterior descending artery (PDA) and a95% tubular lesion in mid PDA [Fig. 2]. Both theLCx and the ‘second’ LAD originated from theproximal right coronary artery. After origin, thisLAD passed between aorta and the right ventricu-lar outflow tract (RVOT) [Fig. 3] and reached theproximal interventricular groove before travelingits entire length to reach the left ventricular apex.A small diagonal and all the septal branches werearising from this anomalous LAD. This vessel wasfree of any disease. A large circumflex was arisingfrom the proximal RCA. After its origin from theposterior aspect, it traversed posterior to aorta(retro aortic) to reach its normal position on thelateral aspect of the left ventricle. AnomalousLCx was diffusely diseased [Fig. 4] along the entirelength of its proximal and mid part with maximum
severity of 90%. Distally, both obtuse marginalsOM1and OM2 showed tubular 75% stenosis atorigin.
The patient underwent primary percutaneouscoronary intervention (PCI) of RCA during thesame sitting from the right radial route using 6Fsheath. An Amplatz right 1 (AR1), 6F guide cathe-ter was used to engage the RCA. Lesion wascrossed with BMW 0.014 coronary wire (AbbottVascular, Santa Clara, California, USA). MidRCA and the PDA ostial lesions were predilatedwith 2.5 � 15 mm Sprinter semi compliant balloon(Medtronic, Minneapolis, Minnesota, USA). A4 � 18 mm bare metal stent Zeta (Abbot Vascular,Santa Clara, California, USA) was deployed atnominal pressure in the mid RCA and subse-quently post dilated with 4 � 15 mm NC mercuryballoon (Abbott Vascular, Santa Clara, California,USA) at 20 atm. The distal lesion was stented witha 2.5 � 28 mm Xience V drug eluting stent (Abbotvascular, Santa Clara, California, USA).This stentwas post dilated with 2.75 mm NC Mercury(non-complaint) balloon (Medtronic, Minneapolis,Minnesota, USA) at 20 atm. During the procedure,patient received bolus and infusion of Inj.eptifibatide and 70 IU/kg of unfractionated
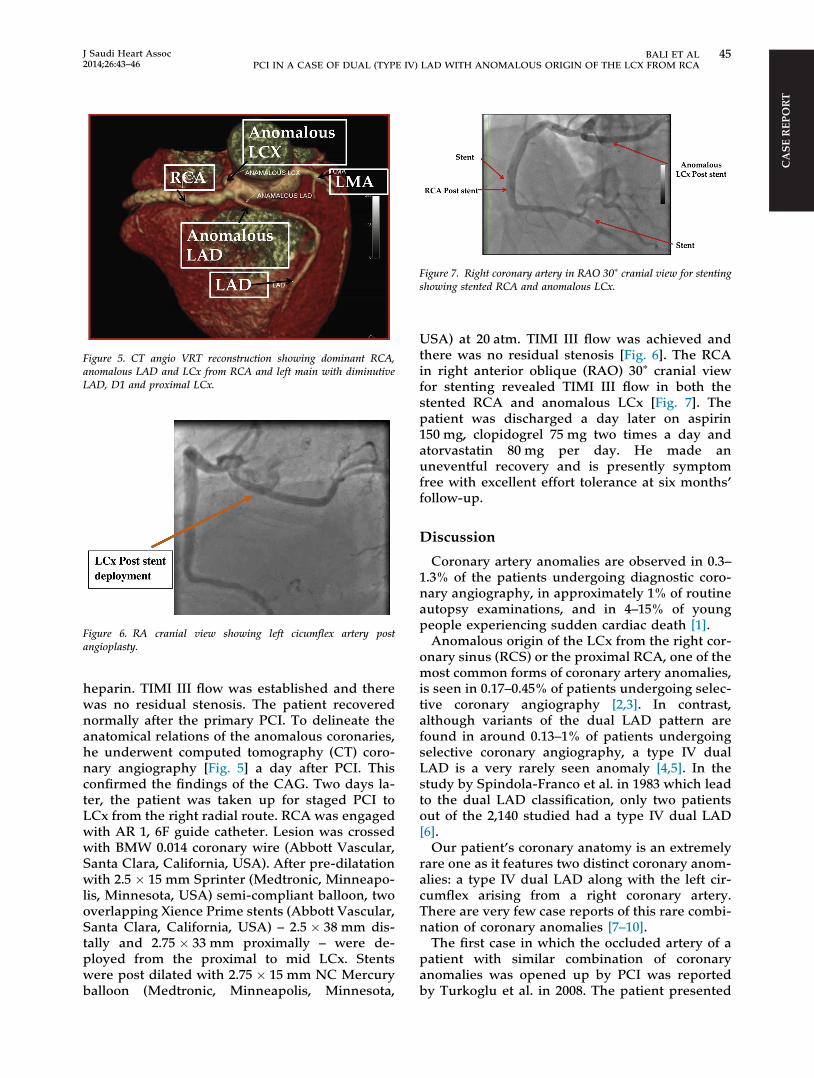
Figure 5. CT angio VRT reconstruction showing dominant RCA,anomalous LAD and LCx from RCA and left main with diminutiveLAD, D1 and proximal LCx.
Figure 6. RA cranial view showing left cicumflex artery postangioplasty.
Figure 7. Right coronary artery in RAO 30⁄ cranial view for stentingshowing stented RCA and anomalous LCx.
CA
SE R
EPO
RT
J Saudi Heart Assoc2014;26:43–46
BALI ET AL 45PCI IN A CASE OF DUAL (TYPE IV) LAD WITH ANOMALOUS ORIGIN OF THE LCX FROM RCA
heparin. TIMI III flow was established and therewas no residual stenosis. The patient recoverednormally after the primary PCI. To delineate theanatomical relations of the anomalous coronaries,he underwent computed tomography (CT) coro-nary angiography [Fig. 5] a day after PCI. Thisconfirmed the findings of the CAG. Two days la-ter, the patient was taken up for staged PCI toLCx from the right radial route. RCA was engagedwith AR 1, 6F guide catheter. Lesion was crossedwith BMW 0.014 coronary wire (Abbott Vascular,Santa Clara, California, USA). After pre-dilatationwith 2.5 � 15 mm Sprinter (Medtronic, Minneapo-lis, Minnesota, USA) semi-compliant balloon, twooverlapping Xience Prime stents (Abbott Vascular,Santa Clara, California, USA) – 2.5 � 38 mm dis-tally and 2.75 � 33 mm proximally – were de-ployed from the proximal to mid LCx. Stentswere post dilated with 2.75 � 15 mm NC Mercuryballoon (Medtronic, Minneapolis, Minnesota,
USA) at 20 atm. TIMI III flow was achieved andthere was no residual stenosis [Fig. 6]. The RCAin right anterior oblique (RAO) 30⁄ cranial viewfor stenting revealed TIMI III flow in both thestented RCA and anomalous LCx [Fig. 7]. Thepatient was discharged a day later on aspirin150 mg, clopidogrel 75 mg two times a day andatorvastatin 80 mg per day. He made anuneventful recovery and is presently symptomfree with excellent effort tolerance at six months’follow-up.
Discussion
Coronary artery anomalies are observed in 0.3–1.3% of the patients undergoing diagnostic coro-nary angiography, in approximately 1% of routineautopsy examinations, and in 4–15% of youngpeople experiencing sudden cardiac death [1].
Anomalous origin of the LCx from the right cor-onary sinus (RCS) or the proximal RCA, one of themost common forms of coronary artery anomalies,is seen in 0.17–0.45% of patients undergoing selec-tive coronary angiography [2,3]. In contrast,although variants of the dual LAD pattern arefound in around 0.13–1% of patients undergoingselective coronary angiography, a type IV dualLAD is a very rarely seen anomaly [4,5]. In thestudy by Spindola-Franco et al. in 1983 which leadto the dual LAD classification, only two patientsout of the 2,140 studied had a type IV dual LAD[6].
Our patient’s coronary anatomy is an extremelyrare one as it features two distinct coronary anom-alies: a type IV dual LAD along with the left cir-cumflex arising from a right coronary artery.There are very few case reports of this rare combi-nation of coronary anomalies [7–10].
The first case in which the occluded artery of apatient with similar combination of coronaryanomalies was opened up by PCI was reportedby Turkoglu et al. in 2008. The patient presented

CA
SE REPO
RT
46 BALI ET ALPCI IN A CASE OF DUAL (TYPE IV) LAD WITH ANOMALOUS ORIGIN OF THE LCX FROM RCA
J Saudi Heart Assoc2014;26:43–46
with acute lateral wall MI and the infarct-relatedartery LCx was successfully stented [11]. Recently,Masuda et al. have reported a similar case reportin which successful transradial intervention wasdone for two lesions with dual anomalous originsof coronary arteries [12].
Conclusion
We conclude that anomalous coronaries can besafely and successfully treated through the radialroute after careful evaluation of the origin andcourse of the anomalous vessels. CT coronaryangiography is extremely useful in delineatingthe vessel course and particularly its relation togreat arteries.
References
[1] Angelini P, Velasco JA, Flamm S. Coronary anomalies:incidence, pathophysiology, and clinical relevance.Circulation 2002;105(20):2449–54.
[2] Bunce NH, Lorenz CH, Keegan J, Lesser J, Reyes EM,Firmin DM, et al.. Coronary artery anomalies: assessmentwith free-breathing three-dimensional coronary MRangiography. Radiology 2003;227(1):201–8.
[3] Page Jr HL, Engel HJ, Campbell WB, Thomas Jr CS.Anomalous origin of the left circumflex coronary artery.Recognition, angiographic demonstration and clinicalsignificance. Circulation 1974;50(4):768–73.
[4] Baltaxe HA, Wixson D. The incidence of congenitalanomalies of the coronary arteries in the adultpopulation. Radiology 1977;122(1):47–52.
[5] Sajja LR, Farooqi A, Shaik MS, Yarlagadda RB, Baruah DK,Pothineni RB. Dual left anterior descending coronaryartery: surgical revascularization in 4 patients. Tex HeartInst J 2000;27(3):292–6.
[6] Spindola-Franco H, Grose R, Solomon N. Dual left anteriordescending coronary artery: angiographic description ofimportant variants and surgical implications. Am Heart J1983;105(3):445–55.
[7] Taghipour HR, Dadjou Y, Mafi AR, Moharamzad Y. A veryrare case of single coronary artery anomaly, with leftanterior descending and left circumflex arteriesoriginating separately from the proximal right coronaryartery. J Card Surg 2008;23(1):67–9.
[8] Bartorelli AL, Capacchione V, Ravagnani P, Pepi M.Anomalous origin of the left anterior descending andcircumflex coronary arteries by two separate ostia from theright sinus of Valsalva. Int J Cardiol 1994;44(3):294–8.
[9] Talanas G, Delpini A, Casu G, Bilotta F, Pes R, Terrosu P. Adouble left anterior descending coronary artery emergingfrom the right Valsalva sinus: a case report and briefliterature review. J Cardiovasc Med (Hagerstown)2009;10(1):64–7.
[10] Kimbiris D. Anomalous origin of the left main coronaryartery from the right sinus of Valsalva. Am J Cardiol1985;55(6):765–9.
[11] Turkoglu S, Balcioglu S, Ozdemir M. Type IV dual leftanterior descending artery associated with anomalousorigin of the left circumflex coronary artery from theright coronary artery: a case report. J Invasive Cardiol2008;20(12):669–70.
[12] Masuda N, Matsukage T, Ikari Y. Successful transradialintervention for two lesions with dual anomalous originsof coronary arteries. J Invasive Cardiol 2011;23(5). E117–20.