
Paul Gross
14
HISummitPAPER220713.docx 1 Health Group Strategies Pty. Limited (INC. IN NSW) ABN: 16 003 974 507 AND INSTITUTE OF HEALTH ECONOMICS AND TECHNOLOGY ASSESSMENT LE GRAND BOIS, ST CHRISTOPHE EN BRIONNAIS, SAONE ET LOIRE, 71800 FRANCE PO BOX 4232 BALGOWLAH HEIGHTS NSW 2093 AUSTRALIA PHONE 61 2 9953 7003 FAX 61 2 9953 7006 Email: [email protected] Version: 22 July 2013 Long-term and short-term priorities for health and related social care in the first term of the next government: whither private health insurance? BY Paul F. Gross PhD Director, Health Group Strategies Pty Ltd (Australia and Greater China) Director, Institute of Health Economics and Technology Assessment, Australia and Greater China Parts of this paper were delivered at the Health Insurance Summit in Sydney on 22 July 2013.
-
date post
21-Oct-2014 -
Category
Health & Medicine
-
view
486 -
download
4
description
Transcript of Paul Gross
HISummitPAPER220713.docx 1
Health Group Strategies Pty. Limited (INC. IN NSW) ABN: 16 003 974 507
AND
INSTITUTE OF HEALTH ECONOMICS AND TECHNOLOGY ASSESSMENT
LE GRAND BOIS, ST CHRISTOPHE EN BRIONNAIS, SAONE ET LOIRE, 71800 FRANCE
PO BOX 4232 BALGOWLAH HEIGHTS NSW 2093 AUSTRALIA PHONE 61 2 9953 7003 FAX 61 2 9953 7006 Email: [email protected]
Version: 22 July 2013
Long-term and short-term priorities for health and related social care in the first term of the next government: whither private health
insurance?
BY
Paul F. Gross PhD
Director, Health Group Strategies Pty Ltd (Australia and Greater China) Director, Institute of Health Economics and Technology Assessment,
Australia and Greater China
Parts of this paper were delivered at the Health Insurance Summit in Sydney on 22 July 2013.

HISummitPAPER220713.docx 2
1. SOME DISCONNECTIONS BETWEEN HEALTHCARE AND SOCIAL CARE NEED POLITICAL LEADERSHIP
The current boundaries that demarcate the financing of health care, long-term care in
retirement and retirement living are unsustainable. Those barriers should be broken
down in the first term of a new government.
First, the warnings of the Henry report (totally ignored by the last two governments
and opposition) should have driven Australian politicians to think about why we
cannot afford to maintain these boundaries.
Second, the GFC signalled to all nations that we cannot afford to satisfy demand in
health and social care using dollars from Medicare, PHI and superannuation. Instead,
Australia spent like a drunken sailor, fiddled with health reform, did nothing about
aged care but then launched a new National Disability Insurance Scheme that has
many overlaps with medical services and aged care.
As a result, with a new government imminent, we now have the worst of all worlds:
• no sustainable policies for health care reform;
• overdue budget outlays on mental health and disability but minimal attention to
either the workforce gaps or the care coordination needed to spend the new
money wisely;
• a health care system under no pressure to provide safer or more efficient care;
• a social service system and a disability services sector totally unconnected
budget-wise or service-wise from the health care system; and
• too many politicians still pushing populist carts that ignore urgent reforms that can
create more accessible and affordable health and social services in the future.
HISummitPAPER220713.docx 3
Four other factors, both facilitated by the current pattern of government subsidy and
private payment, have been looming for years as policymakers took their hands off
the tiller.
• Medical technology has improved in each decade – and its average cost is rising
with each decade. Health insurance, via Medicare or PHI, is a major driver of the
supply of, and consumer demand for, medical technology. In a world where
subsidised social insurance (Medicare) and private health insurance cushion the
financial blow to consumers and encourages the supply side (doctors) to do all
that is possible, we are now seeing a belated recognition by governments (not
Australia, sadly) that this splurge on every technology does not guarantee value
for money purchasing.
• The MBS, private health insurers and other big payers of health care (such as
DVA and Workers Compensation schemes) reimburse the providers of care via a
fee-for-service (mainly doctors), a casemix payment (hospitals) and very rarely a
bundled payment for a defined claim of patient. That payment flows to the
provider regardless of the quality of the care provided – and in all nations of which
I have experience, the total payment for botched or unsafe care is higher than the
total payment for care that is of high quality. In 2013, the providers of medical and
hospital still have no incentive to be transparent about which episodes of care
regularly cause patient harm and/or higher costs to all payers. By any standard,
this is inconspicuous waste. Payment reforms worldwide – but not in Australia
where 10% of overnight stays indicate the presence of adverse events to patients.
– are attempting to reduce that waste by changing the incentives for quality care.1
• There are no incentives in the current payment system for innovations that might
change the dominant and most costly site of care, viz., the acute hospital bed. An
under-funded aged care system, threatened by the paucity of existing aged care
subsidies, has no hesitation in sending nursing home patients, mostly old, to
1 In Australia, some academics are arguing that pay-for-performance in unproven until they are given tax-payer subsidised grants to demonstrate what other nations have long known: incentives do work. 2 The Australian Medical Association is not the only medical union labeling the patient-doctor relationship as
HISummitPAPER220713.docx 4
respite care in an acute hospital, or to an emergency ward of a hospital, or to a
hospital that will be the last provider of care before the patient dies.
• Social care linked to medical care is almost invisible in Australia. In other nations,
this linkage is being strengthened (the UK health and social care legislation is an
example, albeit beset by GFC-induced budget cuts)) because the linkage has
been shown to accord with patient preferences, allow more appropriate care of
the aged and chronically ill, and allow households to make collective decisions on
the choice of care, and create competition in the market for innovations in care.
2. THE CURRENT PAYMENT CURRENCIES FOR DOCTORS AND HOSPITALS ARE OUTDATED, IMPEDE INTEGRATED CARE, INCREASE OUT-OF-POCKET COSTS, AND WEAKEN THE VALUE OF PHI
Health insurance via general tax revenue, a Medicare levy or a private health
insurance premium (and subsidised by the PHI rebate) currently exists alongside the
growing share of health expenditures funded by out-of-pocket payments by
consumers.
Often forgotten is the fact that it is the household that pays for care by all four routes.
The current mix of funding is incoherent if rising copayments are impeding access to
needed care, particularly when this rising share leaves patients vulnerable to the
charging whims of individual doctors and decisions by the federal government that
limit the rate of increases of subsidies for medical care via the Medicare Benefits
Scheme (MBS).

HISummitPAPER220713.docx 5
We now have the ludicrous situation where the formerly simple and “sacred”2
contract between the doctor and the patient is complicated by the actions of five
decision-makers:
• a government decision to hold MBS fees at levels that do not recognise the rising
costs incurred by doctors in their practices;
• a decision by the Australian Medical Association to set a higher range of fees that
doctors can charge (often 50% higher than the MBS fee);
• the decision by the Howard government, sustained by two Labor governments, to
create a new subsidy that allows patients to claim tax benefits after the Safety Net
thresholds for doctor charges and PBS outlays have been passed in any year,
thereby inspiring some medical specialists to generate more services knowing the
patient will not be paying after the threshold is exceeded in any year;
• a subsequent decision by the doctor to charge higher fees than the AMA
recommended fee and, in some cases depending on the market strength of the
individual specialist and how the Safety Net affects them, a very much higher
charge;
• decisions by health insurers on their rebates for specialist care in private
hospitals,3 with funds offering their members predictable out-of-pocket outlays
when the specialist agrees to charge PHI members “no extras”; and
• at the end of this daisy-chain of decisions, a decision by the patient to meet all or
any uninsured out-of-pocket payments, or to not seek a doctor's office-based
service, or to not attend a dental service, or to not fill a script written by any
doctor.
2 The Australian Medical Association is not the only medical union labeling the patient-doctor relationship as sacrosanct, or warning the population that any interference by governments of health insurers in fee determination is equivalent to US “managed care”. 3 The private insurer is required to pay the 25% gap between the fee and the 75% of that fee set in health insurance legislation as the insurer's responsibility for privately insured hospital payments.

HISummitPAPER220713.docx 6
The Australian healthcare system is now vulnerable to organisation mayhem and an
unwillingness to accept that the private health system is enlarging because the public
sees a public health system weakened by political bunfights.
For as long we leave COAG and its seven advisory bodies in charge of public
hospital reform, and while we avoid restructuring of private health insurance,
• there will be no innovation outside the hospital walls;
• rising out-of-pocket costs will continue to weaken the value of health insurance
and patients will defer care and not take essential medicines;
• nearly 12% of older Australians are estimated to spend over 10% of their
income on health costs and 5% (250,000) are estimated to spend over 20%,
seriously reducing their disposable income in retirement; and
• with no innovation, higher costs, and reduced access to essential care, future
household wealth and national productivity will decline.
The last health reform commission laboured long but its 123 recommendations were
a compromise, the absence of expertise in budget financing meant that its estimates
of costs were at best aspirational, it provided no incentives for a rapid transition to
higher quality and safer care, and it barely recognised the co-existence of a growing
private sector.
Starting in September 2013, the next government must focus on fiscally responsible
priorities, and 123 recommendations are 120 too many.
The three critical recommendations relate to the fed-state divide in health and social
care, the transparency of health system performance, and the gaps in current health
insurance that require cooperative de-regulation.
I have two modest suggestions for the next government.
ACTION 1: Think about whether it is time to seek a mandate to re-organise, by 2017, all health and social care payment currencies and assess the potential impact of pooled federal funding to the states

HISummitPAPER220713.docx 7
Budget pressures in the health and education portfolios, when we add unfunded
commitments to a national disability insurance scheme and the Gonski reforms,
mean that we cannot continue to promise universal benefits to everyone.
A corollary follows: if we cannot afford to fund every political promise, we need to cut
the obvious waste of two levels of government now oversighting health and welfare,
reduce administrative costs, and ensure best use of the public and private health and
educational systems.
We need to return some control of the health care system to consumers – and that
means jettisoning left-wing dogma that consumers cannot exert sufficient power to
change the dominance of doctors and hospitals. Contrary to the Abbott view while
Health Minister many moons ago, a targeted investment in specific types of
information systems can change the balance of power by rendering the health
system transparent. As noted in a recent US defence review by the Brookings
Institution, "speed and ubiquity of information creates pressures to act."4
The symmetry between the Health and Education policy arenas is now stark. We
have the spectre of three State governments, one arguing it already has the best
education funding policies that produce the best school results, delaying the Gonski
education reforms that require all States to come up to standards that are
measurable. The paltry logic: if you need $6 billion for the NDIS, cut it from the
Gonski funding.
In the health arena, the spectacle involves a similar façade. Here the States are
delaying reforms in hospital efficiency and patient safety by arguing that the feds
have stripped promised funding from them in mid-year. The states are demanding
the money originally promised – but they have done nothing to improve patient
access, patient safety or hospital quality.
In The Age on June 17 2013, the following indictment of hospital funding and quality
emerged:
4 Hamilton Project. "Real Specifics: 15 ways to reduce the federal budget. Part 1 budgeting for a modern military". Washington DC, Brookings Institution, 22 February 2013, 105 pages (at p 42 of transcript).

HISummitPAPER220713.docx 8
“Last week, Fairfax Media reported the Royal Children's Hospital was offering
patients access to a private room with more privacy and a lower risk of infection if
they used their private health insurance.”
I merely ask: Is the patient safety situation in a teaching hospital now so bad that we need to offer access to safe rooms? A health insurance executive might ask: Is this
the latest tool we have for marketing the value of PHI? Any politician looking back at
the last four years of talk might ask: did the COAG health reforms change anything in
state-run healthcare or criteria for public hospital admission and PHI payment?
The sad reality is that in health and education, the States are closer to the day-to-day
action of the schools and hospitals – and are in a better position that the feds to
apply tax dollars wisely and render hospitals safer. Under the COAG funding, they
still show no signs of so doing.
ACTION 2: Seek a mandate to render transparent with performance-based payment by 2016 the quality and safety of healthcare
At some point, we return to the real elephant in the room: the transparency of
measurement of the performance of public and private hospitals.
To date, this elephant has been put to pasture by health unions, Labor governments
and many clinicians. As in the schools, there is no appetite for transparency in a
funding system where one level of government allocates tax dollars and the other
spends the dollars in ways that defy transparent measurement.
In this conundrum, public schools and public hospitals are in the same under-funded
mess. No more money will be allocated until some improved outcomes of the funding
are visible to the feds.
The feds – with Abbott or anyone else as PM – have every right to demand
transparency in the quality of schools and hospitals – and we should not elect them
unless they are willing to man the spotlights.

HISummitPAPER220713.docx 9
3. THREE SHORT-TERM PRIORITIES FOR THE NEXT GOVERNMENT
These first two modest thoughts are a big stretch, so in the search for a relevant set
of short-term health reforms, my next three thoughts focus on the role of health
insurance in an ageing society that expects governments to provide all benefits with
no new taxes.
The next government should use its first term to
• define a vision for affordable care, creating an alternative to the Council on
Australian Governments to guide Australian priorities in healthcare funding
and reform,
• deregulate private health insurance, and push the insurance and financial
services industry towards new forms of insurance and savings that embed
incentives for appropriate use of health and social care.
ACTION 3: Give the nation a cooperative vision of affordable health and social care and a new national council to oversee reform across the health sector
With few new ideas coming from the health insurers or state governments, politicians
of all persuasions have been silent on the hard issues such as why we must
• cut back on overuse and other waste in the health system,
• harness the resources of the public and private systems,
• retain nurses and make better use of all health professionals,
• create more affordable health insurance covering all life stages, and
• help individuals and families to reduce risk factors that are driving 70% of the
health bill.
An incoming government should take no more than 12 months to
• assess specific proposals to make healthcare more affordable,

HISummitPAPER220713.docx 10
• identify the roles of governments, the private health sector and the voluntary
sector in the implementation of the proposals, and
• tell the public why patient-centred care will drive all future reforms, and why
little steps can bring about affordable care quicker than big-bang reforms.
Ignoring all exhortations for big-bang reform in its first term, the next government
should not (yet again) attempt restructuring of the roles of different levels of
government in healthcare.
An independent council should replace COAG and bring the public and private
sectors together. On the day the new Health Minister is appointed, the government
should announce an intent to replace COAG as the prime decision-maker by National
Health Priorities Council drawn from both levels of government, the private health
sector, the voluntary sector and patient support groups.
The new council should report to Parliament, as does the German equivalent that
has stood the test of time. Its reach across all parts of the health sector enables
messy reforms to be debated, honed and promulgated with at least a semblance of
cooperation between the lander (states) and the federal government.
ACTION 4. Deregulate health insurance in stages, starting with regulations whose benefits do not justify their hidden costs
Private health insurance is under threat because of costly and misplaced regulatory
zeal, its dependence on tax rebates, and the absence of incentives to insurers to
create less costly insurance or new types of insurance to cover rising copayments.
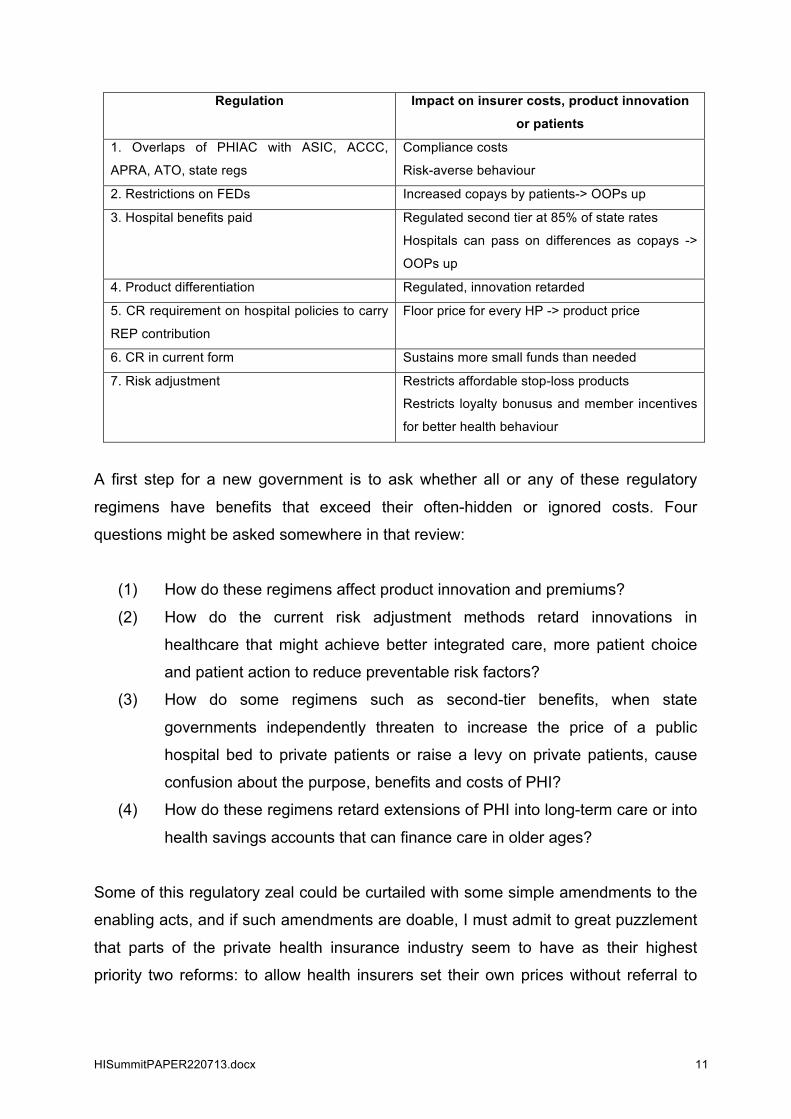
The regulatory armamentarium is illustrated, not exhausted, in the following table
whose acronyms and terminology should be familiar to this conference.
HISummitPAPER220713.docx 11
Regulation Impact on insurer costs, product innovation
or patients
1. Overlaps of PHIAC with ASIC, ACCC,
APRA, ATO, state regs
Compliance costs
Risk-averse behaviour
2. Restrictions on FEDs Increased copays by patients-> OOPs up
3. Hospital benefits paid Regulated second tier at 85% of state rates
Hospitals can pass on differences as copays ->
OOPs up
4. Product differentiation Regulated, innovation retarded
5. CR requirement on hospital policies to carry
REP contribution
Floor price for every HP -> product price
6. CR in current form Sustains more small funds than needed
7. Risk adjustment Restricts affordable stop-loss products
Restricts loyalty bonusus and member incentives
for better health behaviour
A first step for a new government is to ask whether all or any of these regulatory
regimens have benefits that exceed their often-hidden or ignored costs. Four
questions might be asked somewhere in that review:
(1) How do these regimens affect product innovation and premiums?
(2) How do the current risk adjustment methods retard innovations in
healthcare that might achieve better integrated care, more patient choice
and patient action to reduce preventable risk factors?
(3) How do some regimens such as second-tier benefits, when state
governments independently threaten to increase the price of a public
hospital bed to private patients or raise a levy on private patients, cause
confusion about the purpose, benefits and costs of PHI?
(4) How do these regimens retard extensions of PHI into long-term care or into
health savings accounts that can finance care in older ages?
Some of this regulatory zeal could be curtailed with some simple amendments to the
enabling acts, and if such amendments are doable, I must admit to great puzzlement
that parts of the private health insurance industry seem to have as their highest
priority two reforms: to allow health insurers set their own prices without referral to
HISummitPAPER220713.docx 12
the Health Minister or some umpire, or endorsement of a Medicare Select or a Dutch
health insurance model based on private health insurance competition.
In my view, the first argument is risible for a long as the prime task of the survival of
both PHI and the PHI rebate is to define a new role for PHI that makes care more
affordable and leads to better health outcomes.
The second argument is a political landmine. The cost of the Dutch health system
has doubled since 2000 as five health insurers controlled over 80% of the market,
hospitals ramped up the volume of hospital care under “free pricing”, and a rapid
surge in the cost of long-term care forced the government to think about moving
some of the insurer costs to local governments. The Dutch now spend over 13% of
GDP on health, and our 10% share would breech similar levels if we adopted the
current Dutch model.
There is also the small issue of the premiums charged in the Netherlands. My guess
is that insured Australians might ask why an community-rated, income-related
premium of 7% is something to be desired when they pay less than half that rate for
Medicare and PHI.
Because of other strengths (including its integration of care for certain chronic
conditions and its coverage of ‘exceptional expenses), we should be having an
informed debate about the Dutch model.
Burt we should also be assessing the new German models (given Germany’s
decisive action in January to provide subsidies for long-term care insurance or LTCI),
and Belgium’s risk-adjustment formula to encourage insurers not risk-select against
LTCI enrolees. Though I fully comprehend why insurers are not racing into LTCI
promulgation when the market demand is almost zilch and the pricing of future care
benefits almost impossible to predict, aged care funding without some form of tax-
incentivised insurance for care outside the institutional walls and self-care will be very
expensive.

HISummitPAPER220713.docx 13
ACTION 5: Provide the incentives for relevant health insurance and engender a new mentality of saving for healthcare in retirement
The debate about desirable changes in PHI ought to take place once we have had a
prior debate about broad principles that should underpin any health insurance reform:
• what outcomes are we seeking to achieve with any new approach,
• what options are feasible for achieving those goals,
• what ought to be covered,
• how shall it be paid for, tax-protected or tax incentivised
• how it fits with Medicare, disability insurance and aged care funding,
• what quality assurance methods should underpin payments to providers of
care,
• what existing subsidies should be modified,
• what safeguards are needed to ensure that it achieves its outcomes.
So here is my modest suggestion that is consistent with reforms that seek affordable
care and deregulated PHI. Assuming that the government wants to contain future
budget expenditures on the aged and chronically ill, by the end of the first week of
the new government the Productivity Commission should be given a mandate to
complete, within 12 months, a costed feasibility study of tax-subsidised health
savings accounts within private superannuation accounts, with those HSAs used to
pay for
• insurance against the risks of catastrophic costs in retirement, as in
Singapore, or
• supplementary insurance that triggers cash benefits once a doctor indicates
loss of independency as in Germany, or
• gap insurance that allows access to additional preference-sensitive benefits
above a basic level of benefits available to all citizens.
HISummitPAPER220713.docx 14
4. CONCLUSION
There is good reason to avoid big-bang healthcare reforms. The UK, US and
Australian reforms were all big-bang, all had some GFC-induced slow-downs and all
created new bureaucracies that were resented by clinicians and not fully applauded
by the citizenry. The private health sector was not visible in two of these
restructurings.
There are a swag of reasons to seek more affordable health and related social care
in bite-size chunks that engage all actors in reforms that are painful and difficult, such
as cutting adverse events, rather than the usual plea to wait for culture change in
hospitals or leave the problem for slow resolution by the ACSQHC.
The article in The Age on 17 June 2013, quoted above, tells us that we still have a
mess that has not been touched by the last health reform process.
The next reform process requires coalition-building and priorities, and a vision that
more of the same is a criminal waste of the nation’s resources and a threat to healthy
ageing.
My five modest suggestions are not intended to leave politicians tranquil about the
requirements of leadership, team-building and consensus-gathering across the
health and welfare sectors. I also have cautious hopes that leaders will emerge in the
PHI and related industries to inform the public that there are affordable alternatives.


















