Liver metastasis in prostate cancer: a predictor of poor ...

British Journalof Urology (1993), 12,933-936 6 1993 British Journal of Urology
Patterns of Bone Metastasis and their Prognostic Significance in Patients with Carcinoma of the Prostate
A. RANA, G. D. CHISHOLM, M. KHAN, S. S. SEKHARJIT, M. V. MERRICK and R . A. ELTON
University Department of SurgerylUrology and Department of Nuclear Medicine, Western General Hospital; Medical Statistics Unit, University of Edinburgh, Edinburgh
Summary-The different patterns of bone metastasis, metastatic load and their prognostic significance were examined in a consecutive series of 169 men with prostatic cancer and bone metastasis at presentation. Patients with an isolated metastasis in the pelvis or dorsal vertebrae had a better prognosis than those whose metastases were either diffuse or involved more distal sites such as the skull or the sternum, although all of these patients were classified as having M 1 disease. Bone metastasis involving an area equivalent to 1 vertebral body equalled a metastatic load of 2. Based on their total metastatic load, 3 prognostic groups were identified with significant differences in case-specific survival despite receiving the same hormonal treatment. When comparing the potential efficacy of various treatments one must stratify the metastatic load, which is a powerful prognostic indicator of the outcome in patients with metastatic carcinoma of the prostate.
Prostatic cancer with metastases to bone is catego- rised as M1 disease by the TNM system (Wallace et al., 1975) or D2 disease by the Whitmore-Jewett system (Benson and Olsson, 1989). This indicates a poor prognosis and 85% of patients who die from prostatic cancer have bone metastases (McCrea and Karafin, 1958).
Hormonal manipulation is the basis of palliation for advanced disease. Currently, much attention is focused on the choice between monotherapy and combination therapy (Labrie et al., 1983 ; Iversen, 1990; The Canadian Anandron Study Group, 1990; Tyrrell et al., 1991). However, the influence of intrinsic patterns of bone metastasis on the clinical outcome has rarely been taken into account.
Bone metastases may vary from one isolated hot spot on the pelvis to dissemination involving a distal site such as the skull or multiple regional bony sites with large bulky deposits within one bone. Such varied patterns could influence the prognosis despite identical treatment. In 1988, Soloway et a/. reported a semiquantitative grading
Accepted for publication 1 June 1993
system for the extent of disease based on initial bone scans from 166 patients with prostatic cancer. The present study examines the different patterns of bone metastases, the metastatic load and their prognostic significance in a consecutive series of 169 men with M1 disease at presentation.
Patients and Methods
Between January 1978 and December 1990, a consecutive series of 169 men had unequivocal bone metastases at presentation diagnosed by 99mTc-labelled MDP bone scans and skeletal X-ray of relevant hot spots. Following routine clinical, haematological and biochemical tests (including serum markers) all patients received primary hormone treatment with subcapsular orchiectomy. These variables were stored prospectively in a database and updated every 3 months when patients were reviewed in a dedicated prostate cancer clinic. The end-point for the present study was either 31 December 1991 or death.
The causes of death, either cancer-related or otherwise, were recorded. For the analysis of survival the outcome of interest was cancer death; hence the non-cancer deaths were censored. A total

934 BRITISH JOURNAL OF UROLOGY
of 116 patients (69%) had prostate cancer-specific deaths. The original bone scan and skeletal X-rays were reviewed and the sites of metastases at presentation were recorded. The metastatic load was determined as recommended by Soloway et al. (1988). A metastasis involving the equivalent area of 1 vertebral body amounted to a metastatic load of 2. Based upon their total metastatic load, patients were divided into 3 groups (metastatic load 1-5,6- 20 and >20 representing Groups I, I1 and I11 respectively). The survival rates for different metas- tatic loads were estimated by the Kaplan-Meier method and compared using log-rank tests for significance of difference.
Results
At presentation, 37 patients had low (Group I), 62 had intermediate (Group 11) and 70 had high (Group 111) metastatic loads. The metastatic load was a useful prognostic indicator, with Group I patients surviving longer than Groups11 or 111 (Fig. l), and this difference was highly significant
Of the different bony sites, the pelvis was the most frequent site for metastasis (76%), followed closely by the dorsal (73%) and the lumbar vertebrae (63%); there was, however, considerable overlap (Table 1). Skull (7%) and sternum (14%) were less commonly involved at presentation. The mean metastatic load was 36 when the pelvis was involved and it increased progressively as the distal sites were involved, with a maximum load (mean 83) when the metastasis involved the skull, with the
(P<O.O001).
Years
Fig. 1 patients with increasing metastatic load at presentation.
Kaplan-Meier estimates of survival for 3 groups of
Table 1 Metastatic Load and Case-specific Survival
Frequency of Metastases a t Various Bony Sites,
Mean Kaplan- Meier No. of metastatic estimates:
Site of metastases patients load median at presentation (%) (95% CL) survival (days)
Pelvis 129 (76) 36 (30-41) 700 Dorsalvertebrae 123 (73) 37 (3143) 650 Lumbarvertebrae 107 (63) 41 (3447) 610 Rib 96 (57) 40 (3048) 645 Sacrum 80 (47) 50 (42-57) 625 Femur 48 (28) 54 (42-65) 500
Humerus 31 (18) 61 (47-74) 325 Sternum 23 (14) 65 (47-84) 375 Skull 12 (7) 83 (57-108) 315
Cervicalvertebrae 42 (25) 54 (43-65) 490
consequent shorter median survival of 315 days compared with 700 days for the pelvic metastasis.
Multiple bony sites were involved more often than a single site. In 5% of patients the metastasis was limited to the pelvis, but in 72% the disease had spread to the pelvis plus another site (Table 2). Similarly, 3.6% had a metastasis limited to a dorsal vertebra and 69% had a metastasis in the dorsal vertebra plus another bony site. When either the sternum or the skull was involved, a metastasis was always present elsewhere. When the pelvis was the only metastatic site the metastatic load was low (mean 6) and these patients had a better prognosis (median survival 1578 days) than those with metastases in the pelvis plus another site. Similarly, when only a dorsal vertebra was involved, the mean metastatic load was 2 with longer survival compared with a mean load of 39 when dorsal vertebra plus another bony site were involved with consequent short survival.
Table 2 Single or Multiple Metastatic Sites, Metastatic Load and Prognostic Significance
Mean Kaplan- Meier No. of metastatic estimates:
Site of metastases patients load median at presentation (%I (95% CL) survival (days)
Pelvis only 8 (5) 6 (1-11) 1578 Dorsalvertebraeonly 6 (3.6) 2 (0.6-3) 1250 Pelvis+elsewhere 121 (72) 38 (3243) 675 Dorsal vertebrae +elsewhere 117 (69) 39 (3345) 625 Sternum+elsewhere 23 (13.6) 65 (47-84) 321 Skulli-elsewhere 12 (7) 83 (57-108) 281

PATTERNS OF BONE METASTASIS AND THEIR PROGNOSTIC SIGNIFICANCE IN PROSTATIC CANCER
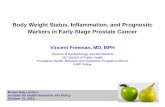
Fig. 2 J.H. (284751) had metastatic disease at D11 (arrow) at presentation on 29/01/1980 with metastatic load 2, serum alkaline phosphatase 55 and prostatic acid phosphatase 213 u/l. He was still alive on 31/12/1992.
Discussion
Prostate cancer, when spread to bone, frequently involves the axial sites. Scanning of the bones with ""technetium identifies the hot spots (McCarthy and Pollack, 1991). However, relevant radiographs are always complementary in order to exclude uptake due to benign causes such as osteoarthritis, Paget's disease or trauma.
The theory expounded by Batson (1940) of a valveless vertebral venous system was based on elaborate experimental models and he demon- strated that the pelvis was the first catchment site for the blood flowing from the prostate gland with associated risk of metastasis. Blood flowed cephalad
935
Fig.3 E.C. (441417)hadwidespread bonemetastasesinvolving (A ) skull, (B) ribs, (C) pelvis and vertebrae at presentation on 21/12/1988 with metastatic load >20, serum alkaline phospha- tase 1125 and prostatic acid phosphatase 10.7 u/l. He died from cancer on 05/03/1989 despite maximum androgen blockade.

936 BRITISH JOURNAL OF UROLOGY
along the spine and then to peripheral sites. However, this haemodynamic effect alone cannot explain why the dorsal vertebrae should be more frequently involved than the more proximal sacral or lumbar vertebrae. The hypothesis of “Seed in Fertile Soil” (Paget, 1889) highlights the fact that a successful metastasis is determined by tumour cell and host factors. Presumably, 12 dorsal vertebrae have a greater volume of “fertile soil” than 5 lumbar or 5 sacral vertebrae. Various growth factors in the bone marrow have also been linked to a high frequency of osseous metastasis from prostatic tumour (Chackal-Roy et al., 1989). Tumour cell invasion and migration are equally important determinants of site-specific metastasis from pros- tate cancer (Zeter, 1990). An isolated bone metas- tasis at presentation is infrequent but has a low metastatic load and better prognosis (Fig. 2) than disseminated or distal metastases with high metas- tatic load (Fig. 3).
Metastatic load is an excellent prognostic indi- cator in cancer of the prostate. The higher the metastatic load the shorter the survival. The difference was significant not only between Groups I and I1 (P = 0.01 1) but also between Groups I1 and I11 (P=0.007). Thus our results differ slightly from those reported by Soloway et al. (1988), who found no significant difference between Groups I1 and 111. However, the present series comprised only patients with M1 disease at presentation and not those who presented with MO disease and subse- quently developed bone metastasis. This is partic- ularly important because there were no superscans in the present series, whereas Soloway et al. (1 988) had a 12% incidence of “superscan or its equivalent” which formed a separate Group (IV) and thus limited the sample size within their Group I11 patients.
In conclusion, patients with an isolated metas- tasis in the pelvis or dorsal vertebra have a better prognosis than those with metastasis at distal sites such as the skull or the sternum; this is due to the difference in metastatic load, despite the fact that they are grouped together as having M1 disease. When comparing the efficacy of various treatments, prognostic factors that can be considered in M1 disease include performance status, bone pain, alkaline phosphatase and haemoglobin. In this study the pattern of bone metastasis, when quanti- fied in terms of metastatic load, was a powerful prognostic factor that influenced the outcome of patients with disseminated cancer of the prostate.
References Batson, 0. V. (1940). The function of the vertebral veins and
their role in the spread of metastases. Ann. Surg., 112, 138- 149.
Benson, M. C. and Olson, C. A. (1989). The staging and grading of prostatic cancer. In The Prostate, ed. Fitzpatrick, J . M. and Krane, R. J . Pp. 261-272. Edinburgh: Churchill Livingstone.
Chackal-Roy, M., Neimeyer, C., Moore, M. et d. (1989). Stimulation of human prostatic carcinoma cell growth by factors present in human bone marrow. J . Clzn. Invest., 84,
Iversen, P. (1990). Zoladex plus Flutamide vs. orchidectomy for advanced prostatic cancer. Eur. Urol. (Suppl. 3), 18,41-44.
Labrie, F., Dupont, A., Belanger, A. el al. (1983). New approach in the treatment of prostate cancer : complete instead of partial withdrawal of androgens. Prostate, 4 , 579-594.
McCarthy, P. and Pollak, H. M. (1991). Imaging of patients with stage D prostatic carcinoma. Urol. Clin. North Am., 18, 35-53.
McCrea, L. E. and Karafin, L. (1958). Carcinoma of the prostate: metastases, therapy, and survival. A statistical analysis of 500 cases. In!. Coll. Surg. J . , 29,123-128.
Paget, J. (1889). The distribution of secondary growth in cancer ofthe breast. Lancet, 1,571.
Soloway, M. S., Hardeman, S. W., Hickey, D. et al. (1988). Stratification of patients with metastatic prostate cancer based on extent of diseases on initial bone scan. Cancer, 61, 195- 202.
The Canadian Anandron Study Group (1990). Total androgen ablation in the treatment of metastatic prostatic cancer. Semin. Urol., VIII, 159--165.
Tyrrell,C. J.,Altwein, J. E. and Klippel, F. (1991). A multicenter randomised trial comparing the luteinizing hormone-releasing hormone analogue goserelin acetate alone and with flutamide in the treatment of advanced prostate cancer. J . Urol., 146,
Wallace, D. M., Chisholm, G. D. and Hendry, W. F. (1975). TNM classification for urological tumours. Br. J . Urol., 47, 1-12.
Zeter, B. R. (1990). The cellular basis of site-specific tumor metastasis. N . Engl. J . Med. , 322,605-612.
43-50.
132 1-1 326.
The Authors A. Rana, MS, FRCS(G), FRCS(I), DUrol(London), Registrar,
G . D. Chisholm, CBE, ChM, PPRCSEd, FRCS, Professor,
M. Khan, FRCSEd, Registrar, University Department of
S. S. Sekharjit, MS, MCh, Commonwealth Medical Fellou,
M. V. Merrick, FRCR, FRCP, Consultant, Department of
R. A. Elton, PhD, Senior Lecturer, Medical Statistics Unit. Requests for reprints to: A. Rana, University Department of Surgery/Urology, Western General Hospital, Edinburgh EH4 2XU.
University Department of Surgery/Urology.
University Department of Surgery/Urology.
Surgery/Urology.
University Department of Surgery/Urology.
Nuclear Medicine.