Dr. Patrick Treacy Botox 'Myths & Facts' lecture to AAAD in Mexico City
Upload
patrick-treacyCategory
view
238download
3
A Retrospective Study Of Nine Cases Concerning Surgical Correction Of Product Migration Caused By Semi-Permanent Lip Fillers.
43 June 2014
A Retrospective Study Of Nine Cases Concerning Surgical Correction Of Product Migration Caused By Semi-Permanent Lip Fillers.
INTRODUCTIONSynthetic biodegradable hyaluronic acid fillers are widely used as relatively safe injectable methods of lip augmentation but their duration is limited to only four months. Because of this many physicians use alternative non-biodegradable materials like polyacrylamide gels and polyvinyl acid, to create a longer lasting ‘semi-permanent’ product. However, these fillers, once more widely use,have an increased risk of product migration, granuloma formation and long-term adverse events. Treatment options include for these types of problems intra-lesional steroids, 5-fluorouracil (5-FU), anti-inflammatory and immunomodulatory drugs like minocycline, rifampicin or surgical correction. This report documents surgical correction of nine cases of problems related to the side-effects related to the semi-permanent fillers, Bio in Blue and Bio-Alcamid (both manufactured by Polymekon, Brindisi, Italy) over a three year period.
CASE REPORTNine female patients in good health were referred to the author with nodular swellings in their labial area over a period of nearly four years. They all reported a history of their lips having being injected with the cosmetic filler Bio in Blue or Bio-Alcamid at the site of the swelling to correct and project the labial profile. In every case a 23G needle was used and entrance was made 0.5cm medial to the oral commissure with infiltration done along the vermilion border.
Each hemilip was injected with a maximum of 0.5ml of Bio-Alcamid. Five of the patients were injected with Bio In Blue and four with Bio-Alcamid.
Four of the patients had previously been injected with another type of hyaluronic acid filler prior to the use of these semi-permanent type fillers. The labial swellings were all worsening in appearance as time passed and the patients were emotionally distressed. Numerous doctors had treated the patients with injections of Dexamethasone (40 mgs/ml) or Triamcinolone (40 mg/ml) at intervals, with no resolution of the swelling. There was no relevant medical history and the patient did not have any clinical evidence of autoimmune or allergic diseases. On palpation, each patient presented with firm longitudinal swellings measuring 3 cm × 2 cm along the lines of filler implantation in each patient (Fig 1-4).
Bio in Blue Extraction
Dr. Patrick Treacy,LRCSI, BCh, BCAM, MRCGP, DRCOG, DCH, BSc (Hons), H. Dip Dermatology.Dublin, Ireland.
Dr. Patrick Treacy.indd 43 7/15/2014 12:36:02 PM

A Retrospective Study Of Nine Cases Concerning Surgical Correction Of Product Migration Caused By Semi-Permanent Lip Fillers.
9June 2014
The nodules were prominent anteriorly and projected from inside the oral cavity. The patients were all were willing to accept surgical correction and histopathological evaluation of their underlying problem. Surgical excisions were carried out by direct use of a size 11 scalpel blade, usually without the use of local anaesthesia, by allowing the nodules to point under digital manipulation.
The wound was thoroughly cleaned and the vermillion tissues were approximated in some cases with 5-0 Vicryl Rapide sutures (Ethicon, Inc) to achieve haemostatis. (Fig 5-6) The operation sites healed well and most had healed within a few days. The first excision biopsies showed no evidence of foreign body giant cells or irregular crystalline structures and were considered not appropriate for the other patients.
DISCUSSIONInjectable fillers have become an important component of minimally invasive facial rejuvenation modalities. Their ease of use, effectiveness, low morbidity, and fast results with minimal
down-time are factors that have made them popular among patients (1)
The search for the ideal filling material has been ongoing for centuries. Various materials, including collagens, autologous fat, hyaluronic acids, poly-L-lactic acid, polyacrylamide, liquid injectable silicone and calcium hydroxylapatite, are among the products currently used for this indication(2). Bioin Blue (Polymekon, Brindisi, Italy) is high purity polyvinyl alcohol (8%) and water (92%). Polyvinyl alcohol is a non-toxic substance used in medicine as a drug-carrier and a substitute for human plasma expander.
Bio In Blue is a biodegradable substance with an immediate cosmetic effect can be maintained by treatment repeated at longer intervals than those necessary for other fillers. Bio-Alcamid (Polymekon, Brindisi, Italy) is considered novel in the field of aesthetic and reconstructive surgery, because of its chemical and physical characteristics. It is considered intermediate between injectable filler and a common prosthesis and often referred to as an injectable endoprosthesis(3). Bio-Alcamid is a non re-absorbable polymeric material composed of 96% of apyrogenic water and 4% of an alkylimide-amide group. These chemical aspects of Bio-Alcamid are responsible for a greater chemical stability of the polymer, a better resistance to basic and acid hydrolytic phenomena, and high resistance to water. Unlike other materials, Bio-Alcamid sometimes be removed even after long time after implantation. Its structure is quite similar to the adipose tissue (4). It is a stable substance, radio transparent, highly elastic and soluble in water. It can be extracted if necessary since it does not spread within the adjacent structures, given the fact that it gives rise to a very thin physiological capsule which isolates it from the surrounding tissues. The gel is colour less and trans-parent. It is supplied in packs containing two sterile 1-ml syringes for the lips (Bio-Alcamid LIPS) and one 3-ml syringe for the face (Bio-Alcamid FACE)(5).Some studies consider Bio-Alcamid to be almost an ideal injectable substance for the treatment of facial aesthetic defects. (6) It also used medically to treat soft tissue deficits such as pectus excavatum, gluteal atrophy, acne scars as well as HIV facial lipoatrophy and Poland syndrome, (7) (8) (9).
Since its initial use, numerous reports of adverse reactions have been reported including significant infections and migration resulting in significant facial deformity. (10) (11) (12)
Because of this, Bio-Alcamid has been taken off the market in many countries and the original manufacture has since stopped production. In Canada, some individuals have attempted to file class action lawsuits against the company (13)
Treatment options for filler complications include intra-lesional steroids, 5-fluorouracil (5-FU), anti-inflammatory and immunomodulatory drugs like minocycline, rifampicin or hydroxychloroquine.(14) Anecdotal reports also suggest some relief with the use of non-steroidal anti-inflammatory drugs (NSAIDs), antihistamines and tacrolimus(14) (15). In case of
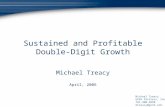
Bio In Blue Extraction Bio Alcamid Extraction
Bio Alcamid Extraction
Bio Alcamid Extraction
Bio Alcamid Extraction
Bio in Blue Lip Extract
Bio In Blue Lip Extract
Dr. Patrick Treacy.indd 9 7/15/2014 12:36:09 PM

A Retrospective Study Of Nine Cases Concerning Surgical Correction Of Product Migration Caused By Semi-Permanent Lip Fillers.
25June 2014
widespread lesions or repeated failure of conservative therapies, surgical excision is the treatment of choice. (16)
Surgical extirpation can also allow a dermatologist to prevent the cutaneous side effects of intradermal steroid or 5-FU injection and a histopathological confirmation can be done to rule out the possibility of a granuloma. (17).
CONCLUSIONThe purpose of this retrospective case report is to demonstrate surgical removal of semi-permanent dermal filler product when complications occur secondary to product migration, and to highlight the awareness in using semi-permanent lip fillers. The ideal agent for lip augmentation should be safe and effective; easy to obtain and administer; have a minimal risk for infection, extrusion, or migration; produce a minimal inflammatory reaction; and last for an acceptable degree of time. It should also be cost-effective, show consistency, and ultimately yield highly acceptable, positive aesthetic results. Despite high hope for the use of Bio-Alcamid to fulfil this role, because of its novel characteristics of apparent low incidence of risk of foreign body granulomas, the product had to be withdrawn because of other issues, relating to high incidence of infection and product migration. The long-term complications of dermal fillers can be particularly devastating, and thus, it is important to reinstate the importance of selecting the correct substance to minimise long-term complications of patients. Official documentation of all adverse effects with dermal filler(s) implantation, including infection and product migration must be made mandatory in order for cosmetic physicians and surgeons to make an informed choice when using injectable fillers.
REFERENCES1. Glavas I.P.: Filling agents. Ophthalmol Clin. North Am. 8: 249-257, 2005.2. Narins R.S. and Beer K.: Liquid injectable silicone: A review of its history, immunology, technical considerations, complications, and potential. Plast. Reconstr. Surg., 118 (3S): 77S-84S, 2006.3. Pacini S., Ruggiero M., Morucci G., Cammarota N Protopapa C. and Gulisano M.: Bio-Alcamid: A novelty for reconstructive and cosmetic surgery. It. J. Anat. Em-bryol., 107: 3, 2002.4. Spira M.: Failure to remove soft-tissue injected with liquid silicone without the use of suction and honesty in scientific medical reports. Plast. Reconstr. Surg., 105 (5): 1909-2000.5. Hönig, J. (2008). "Cheek
Augmentation with Bio-Alcamid in Facial Lipoatrophy in HIV Seropositive Patients". Journal of Craniofacial Surgery 19 (4): 1085–1088.6. Evaluation of the Safety and Efficacy of Bio-Alcamid for Facial Soft Tissue Augmentation.Mohammed Abd El Mageed.Egypt, J. Plast. Reconstr. Surg., Vol. 31, No. 2, July: 129-137, 20077. Treacy P.; Goldberg D., Use of a Bio Polymer Filler for Facial Lipodystrophy in HIV-Positive patients undergoing treatment with Anti Retro Viral Drugs. Journal of Dermatological Surgery Volume 32, Number 6, June 2006, pp. 804-808(5)June 6, 20068. Treacy P. The efficacy of dermal fillers in the treatment of atrophic acne scars. Prime International Vol 3 No 2 Page 40-49 March 1, 20139. Karim RB, Hage JJ, van Rozelaar L, et al. Complications of polyalkylimide 4% injections (Bio-Alcamid): a report of 18 cases. J PlastReconstrAesthetSurg 2006;59(12):1409-14. [PubMed]10. Goldan O, Georgiou I, Grabov-Nardini G, et al. Early and late complications after a nonabsorbable hydrogel polymer injection: a series of 14 patients and novel management.DermatolSurg 2007;33(Suppl 2):S199-206. 11. Ross AH, Malhotra R. Long-term orbitofacial complications of polyalkylimide 4% (Bio-Alcamid).O p h t h a l P l a s t R e c o n s t r S u r g 2009;25(5):394-7. 12. http://smithlawfirm.com/blog/2011/4/5/canadian-man-sues-maker-of-bio-alcamid-gel-claiming-disfigur.html13. De Boulle K. Management of complications after implantation of fillers. J Cosmet Dermatol.2004;3:2–15.14. Rossner M, Rossner F, Bachmann F, Wiest L, Rzany B. Risk of severe adverse reactions to an injectable filler based on a fixed combination of Hydroxyethylmethacrylate and ethylmethacrylate with Hyaluronic acid. Dermatol Surg. 2009;35:367–74.15. Lemperle G, Rullan PP, Gauthier-Hazan N. Avoiding and treating dermal filler complications. J Plast Reconstr Surg. 2006;118:92S–107S. 16. Wolfram D, Tzankov A, Piza-Katzer H. Surgery for foreign body reactions due to injectable fillers. Dermatology. 2006;213:300–4
Dr. Patrick Treacy.indd 25 7/15/2014 12:36:10 PM