Patricia Maani Fogelman, DNP - Pediatric Nursing · 2013. 6. 19. · Loss, Grief, Mourning,...
37
ABC’s of Palliative Medicine: Interventions for the Child with Advanced or Terminal Illness Patricia Maani Fogelman, DNP Ruby Weller, CRNP Geisinger Health System Danville, PA DISCLOSURES |3 Objectives • Define Palliative Medicine and identify two patient care benefits it offers to healthcare today. • Identify appropriate timing for referral to palliative medicine consultation • Describe two palliative medicine interventions for the pediatric patient with advanced illness • Verbalize key phrases to discussing end-of-life care compassionately with patients/families • Recognize the key elements of a constructive, patient- centered family meeting • List three pharmacologic interventions to relieve distress at the end of life Pediatric Palliative Medicine America is a death-denying society Affects child, family, healthcare providers, and community Grief is an individual process Davies & Orloff, 2010 Palliative Medicine: Care Patients Want U.S. News and World Reports • Vigorous treatment of their pain and symptoms • Relief from worry, anxiety, and depression • Communication about their care over time. • Coordinated care throughout the multiple-year course of an illness • Support for family caregivers • Practical support • A sense of safety in the health care system
Transcript of Patricia Maani Fogelman, DNP - Pediatric Nursing · 2013. 6. 19. · Loss, Grief, Mourning,...

ABC’s of Palliative Medicine:Interventions for the Child with Advanced or Terminal Illness
Patricia Maani Fogelman, DNP
Ruby Weller, CRNP
Geisinger Health System
Danville, PA
DISCLOSURES
|3
Objectives
• Define Palliative Medicine and identify two patient care benefits it offers to healthcare today.
• Identify appropriate timing for referral to palliative medicine consultation
• Describe two palliative medicine interventions for the pediatric patient with advanced illness
• Verbalize key phrases to discussing end-of-life care compassionately with patients/families
• Recognize the key elements of a constructive, patient-centered family meeting
• List three pharmacologic interventions to relieve distress at the end of life
Pediatric Palliative Medicine
America is a death-denying society
Affects child, family, healthcare providers, and community
Grief is an individual process
Davies & Orloff, 2010
Palliative Medicine: Care Patients Want
U.S. News and World Reports
• Vigorous treatment of their pain and symptoms
• Relief from worry, anxiety, and depression
• Communication about their care over time.
• Coordinated care throughout the multiple-year course of an illness
• Support for family caregivers
• Practical support
• A sense of safety in the health care system

Background
• In 2010, 45,000 children died in the US• About ½ of these deaths are infants and
neonates• 25,000 are living with a serious illness
• Nearly 17 million adults are caring for a seriously ill child.
� Little experience with death
- Exaggerated sense of dying process
� No “typical” death
Kuhlthau K, Kahn R, Hill KS, Gnanasekaran S, Ettner SL. Matern Child health J 2010; 14(2): 155-63
Opportunity
FY 2011
NICU Total cases Deaths Cases LOS Deaths LOS
597 14 17.34 11.57
PEDS Total cases Deaths Cases LOS Deaths LOS
3901 20 3.36 14.26
| 8
Pediatric Palliative Medicine
• Children are living longer with complex chronic medical conditions.
• Multiple acute and chronic health crises create significant challenges for the child and family.
• Symptom management for these children presents a unique challenge to health care providers
• Interdisciplinary family-centered care is an integral part of the symptom management for a chronically or terminally ill child
Child/Family Expectations of Health Care Provider
• Be honest
• Non-abandonment
• Elicit values and goals
• Help explore realistic options
• Team communication/consistency
• Take time to listenHinds & Kelly, 2010
WHO Definition of Palliative Care for Children
• Active total care of the child’s body, mind and spirit, and also involves giving support to the family• Begins when the illness is diagnosed, and continues regardless
of whether or not a child receives treatment directed at the disease
• Health providers must evaluate and alleviate a child’s physical, psychological , and social distress
• Requires a broad multidisciplinary approach that includes the family and makes use of community resources
• Can be provided in tertiary care facilities, in community health centers and even in children’s homes
(WHO; 1998a)
Family Centered Care
Family shapes types of interventions
– Illness experience
– QOL and sources of suffering
– Goals of care
• Curative/restorative
• Life prolongation
• Comfort
– Relatively young children with an advanced illness can (depending on the circumstances) express their values/goals/preferences and participate in decisions
– Work toward keeping bereaved families intact and functional during illness and after child’s death

The Artful Conversation
Recognize how uncertain this time is for families, and how frightening it can be.
Reaffirm your commitment to them.
Respond to phone calls and questions.
– Patients and families believe that a demonstrated willingness to stay with them through crisis and challenging events is a sign of caring and commitment from their medical providers.
Health Care Professionals:Communication Barriers
• Feeling “like a failure”
• Fear of expressing emotions
• Spiritual concerns
• Fear of own mortality
• Lack of education
• Ethical issues/concerns Boyd et al., 2011; Dahlin, 2010
Communication
• Warning shot first - “I’m afraid I have some
bad news.”
• Is this a good time for this discussion?
• What does patient know?
• What does patient want to know?
• Recognize that patients often do not hear or retain
much of what is said
• Encourage patient to share verbalization of message
• Summarize, document and follow-up
Communication
• Summarize ‘big picture’ in a few sentences
• Avoid jargon and organ by organ review
• Avoid euphemisms and use ‘dying’ if appropriate
• Answer questions
• Respond to emotional reactions
• Prepare for common reactions• Acceptance
• Conflict/denial
• Grief/despair
• Respond empathically
| 16
Clinical Scenario
Delivering very bad news
Sample Response
I wish I had better news to give you.
Responding to unrealistic hopes
from a patient or family
I wish that were possible. It sounds like
all of us would be a lot happier if that
were so.
Responding to demands for
aggressive treatment when
prognosis is very poor
It must be very hard to come to the
intensive care unit every day and see so
little change. I wish medicine had the
power to turn things around.
Responding to expressions of loss,
grief, and hopelessness
It sounds like a terrible loss for you. I
wish it hadn’t turned out this way.
Quill et al Quill et al Ann Int Med 2001Ann Int Med 2001
Family Factors Influencing Communication
Siblings
– Anxiety
– Loss
– Guilt/shame/blame
– Plan of care for siblings
Malone & Price, 2012

Cultural Factors Influencing Communication
Community– Religion
– Spirituality
– Food preferences/prohibitions
– Economic situation
– Health beliefs regarding death, grief, pain
– Importance of rituals
Child/adolescent/family
Self-identification�Birthplace�Ethnic identity�Availability of support systems�Decision-making�Language and communication
Mazanec & Panke, 2010
Cultural Sensitivity
Knowledge and attitudes
Non-judgmental approach
Cross-cultural communication/ cultural assessment
Interdisciplinary approach
Spirituality and healingKagawa-Singer, 2011; Mazanec & Panke, 2010
Components of Cultural Assessment
Nurse and Interdisciplinary Team
– Self assessment
– Cultural beliefs of co-workers
– Training in cultural competency
Use of interpreters
Conversational style
Quality of Life Considerations
• Education• Grief and family
counseling• Peer support• Music therapy• Spiritual support• Respite care• Maintain role of child’s
previous medical caregivers
• Integration entire support system for patient and family
Language
UNCLEAR/DISTRESSFUL HELPFULIt’s time to pull back. Let’s think about/discuss
discontinuing treatments which are not providing benefit.
There is nothing more we can do. We may consider changing the goals of care. Let’s review the goals of care to see if any of them have changed.
A miracle may turn things around. In my experience, I have not seen a child in this situation survive.
LANGUAGE
HELPFUL PHRASES AVOID
May I just sit here with you? It was a blessing…
Is there anyone I can call for you? You have other children to think about.
What might be helpful to you at this time?
I know how you feel.
Would you like me to talk with your other family members, or be there with you when you talk with them?
This will make you a better/stronger person.

Listen With Parents’ Ears
WHAT HCP SAYS WHAT PARENT HEARS
His creatinine is better. He will get well.
She is stable today. She is getting better.
We have an experimental treatment.
This new therapy will cure my child.
Do you want us to do CPR? You think CPR will help.
Do you want us to “do everything” for your child?
Doing everything means you think my child will survive and get well.
Helpful Tips for Talking with Children
• Child Life Specialist
• Appropriate language for developmental age
• Begin with non-threatening topic
• Listen actively/observe non-verbals
• Ask child what he/she knows
• Give valid choices
• Respect opinions
• Allow time to plan
Loss, Grief, Mourning, Bereavement
Loss is absence of a possession or person
Grief is emotional response to loss
Mourning is the outward, social expression of loss
Bereavement includes grief and mourning
Strongly influenced by culture
Corless, 2010; Davies et al., 2010
Myths of Communication
Communication is deliberate
Words mean the same to BOTH the speaker and listener
Verbal communication is primary
Communication is one way
Can’t give too much information
Silence should always be filled
Symptom Management
| 29
Symptom Management : PainScope of the Problem
• Children’s pain experience
• 25-46% experience some level of pain <3 months
duration
• Up to 30% experience chronic or recurrent pain
severe enough to interfere with daily functioning
• Effect of pain on quality of life

Myths Related to Pain and Pain Management in Children
• Risk of respiratory depression
• Addiction
• Child that is sleeping/or playing does not have pain
• Presence of pain indicates worsening of disease or approaching death
Facts About Childhood Pain
• Opioid addictions are rare
• Repeated exposure to painful procedures leads to increased anxiety and perception of pain
• Studies have shown that children as young as 3 years old can use pain scales
Carter et al., 2011; Collins et al., 2011; Goldman et al., 2012; Hockenberry & Wilson, 2010
Myths Related to Neonatal/Infant Pain
• Incapable of feeling pain
• Immature nervous system
• Incomplete myelinization
• No memory• Objective assessment
impossible• Neonates cannot
communicate pain• Analgesics unsafe
Facts About Neonatal/Infant Pain
• Pain perception occurs early in life
• Neonates exhibit physiologic and behavioral cues
• No risk of addiction�Tolerance & physical dependence can occur
Impact of Pain
Research asked ‘What is it like to have a child with pain?’
– Unendurable
– Sense of helplessness
– Sense of total commitment
– Unprepared/unknowledgeable
– Horrible/frightening
– No pain in heaven
Dussel et al., 2010
Pain in Dying Children
90% of children dying of cancer experience pain or other symptoms
Nearly 50% had pain relief
Inadequate pain relief hastens death
Wolfe et al., 2008

End of Life Pain Management
• Assess by patient self-report when possible.• Opioid rotation /titration is common.• Opioid use rarely causes toxicity that would
occur after several weeks of use. beakthpain• Around-the-clock + prophylactic dosing is
recommended.
Pain Management Strategies
• Non-pharmacologic modalities
• Non-opioid analgesics
• Opioids
• Adjuvant analgesics
• Regional anesthetic techniques
WHO Analgesic Ladder
Oral administration when possible
Dosing at regular intervals
Prescribing based on intensity (step-wise approach)
Tailored to the individual
Not applicable to pure neuropathic pain
Codeine and other “weak opioids” no longer recommended
End of Life Pain Management
• Aggressive management of opioid-related toxicities is mandatory.
• Adequate breakthrough medications
• The family/caregivers must understand the goals of adequate pain management.
Assure patient and family of the goal for a pain free death.
Use of Opioids at End-of-Life
• Useful to relieve both pain and dyspnea
• Very high doses may be needed to control severe symptoms
• Sedation and respiratory depression are expected and acceptable side effects under the principle of double effect.
End of Life Pain Management
• No predictable correlation between plasma opioid level and analgesic efficacy or toxicity.ose”– Titrate for unrelieved pain regardless of dose.
• Palliative sedation may be necessary to assure comfort.
• Opioids will not relieve all pain or suffering
**Not all suffering is from pain**

Pain
• Pain must be assessed and managed consistently
• Interdisciplinary management
• Golden rules
– "If it would hurt you, it hurts them"
– Approach the child with the same respect you would an adult
– Requires trust and cooperation
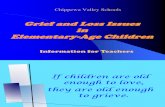
5653 51
42
22
14 12
0
10
20
30
40
50
60
70
80
Frequency of Symptoms–Last 48 Hours
Lichter and Hunt, 1990
De at h r at t le
Ur i na ry
d ys fu nc ti on
P ai n
Ag it at i on
Dy sp ne a
Na us ea /
Vo m
i t in g
My oc lo nu s
Opioids
Short-acting
– Morphine
– Oxycodone
– Hydromorphone
– Fentanyl
Long-acting
– Oxycontin
– Extended-release morphine
– Methadone
Opioids
Morphine
– Opioid standard – oral morphine equivalents (OME)
– PO, SL, IV, IM, SC, intrathecal (IT), epidural, nebulized
– Hydrophilic, does not cross blood-brain barrier well
– Oral bioavailability 20-30% (IV:PO = 1:3)
– Metabolized in the liver and renally excreted
• Use caution in patients with renal insufficiency
• Extreme caution in neonates (especially preterm)
– Long-acting tablet available, dosed q12 hours
Opioids
Oxycodone (1-1.5 OME)
– Tablet, 5 or 10 mg, oral bioavailability 60%
– 0.05-0.1 mg/kg PO q4 hours PRN
– Long-acting formulation (tablet) dosed q12 hours
Hydromorphone (4-6 OME)
– Available PO (tabs or liquid), IV, SC, IT, epidural
– No active metabolites, fewer side effects
– Half-life 3-6 hours
Opioids
Fentanyl (100-150 OME)
– Short-acting and highly lipophilic
– Available IV, IM, SC, transdermal, transmucosal, epidural
– Inactive metabolites excreted renally
– 0.5-2 mcg/kg/dose IV or IM useful for short painful procedures
– Rapid development of tolerance to continuous infusion (especially in neonates)

Methadone
• Long-acting, very effective for chronic pain relief
• Less tolerance (NMDA receptor blocker)
• Fewer side effects
• Addresses neuropathic as well as nociceptive pain
• No active metabolites – safe in hepatic or renal insufficiency• High oral bioavailability (85-90%)
• Long half-life (12-36 hours)
• Onset of analgesia 30-60 minutes
• Duration of analgesia 4-6 hours � 8-12 hours
Methadone
• Difficult to dose correctly, cannot titrate quickly
• Requires more careful monitoring
• More complicated equianalgesic dosing
• Causes prolonged QT interval in at-risk individuals (ECG recommended)
Methadone
• Starting dose (opioid naïve): 0.05-0.1 mg/kg/dose (2.5-5 mg PO q6-12 hours)
• Conversion ratio depends on previous total opioid needs and should be done by providers well experienced with use of methadone for pain management i.e., Palliative Medicine clinicians.
Rotating Opioids
• Often necessary in palliative care setting– Escalating doses with diminishing returns
– Opioid toxicity or intolerable side effects
• Based on theory of incomplete cross-tolerance
• Our practice is to go from shorter-acting to longer-acting
fentanyl � morphine � hydromorphone �methadone
Common Side Effects
• Sedation/respiratory depression
• Nausea/vomiting
• Urinary retention
• Pruritis
• Constipation
• Central nervous system effects
– Dysphoria
– Myoclonus
– Seizures
– Hyperalgesia
Status Epilepticus Due toOpioid Neurotoxicity
� Continuous seizures lasting ≥30 minutes or
� Intermittent seizures without full recovery
� Reduce or stop opioid
� First-line – lorazepam or diazepam
� Second-line – phenytoin or fosphenytoin
� Others – barbiturates, midazolam, propofol
Smith MT; Clin Exp Pharm & Physio 2000; 524-528EPERC Fast Fact #57 and #58

Complications
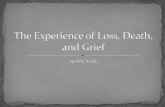
Terminal Delirium aka ‘The difficult road to death’
Medical management– May need Palliative Sedation with
• Lorazepam
• Haloperidol
• Midazolam
• Ketamine
• Propofol
Seizures
Family needs support, education
RestlessRestless
ConfusedConfused TremulousTremulous
HallucinationsHallucinations
Mumbling DeliriumMumbling Delirium
Myoclonic JerksMyoclonic JerksSleepySleepy
LethargicLethargic
ObtundeObtundedd
SemicomatoseSemicomatose
ComatoseComatose
SeizuresSeizures
THE USUAL ROAD
THE USUAL ROAD
THE DIFFICULT
ROAD
THE DIFFICULT
ROAD
NormalNormal
DeathDeath
2 Roads to Death
Treatment of Dyspnea at End of Life
• Treating symptoms or underlying cause
• Pharmacologic treatments
• Non-pharmacologic– Oxygen
– Pursed lip breathing
– Energy conservation
– Fans, elevation
– Counseling
– Other
Depression
• Manifestations in children may differ from adults
• Ranges from sadness to suicidal
• Chronic and terminally ill children are at risk
• Children tend to react to distress and emotions of adults closest to them.
Treatment of Depression
• Antidepressants
• Stimulants
• Promote autonomy
• Grief/psychiatric counseling
• Draw on strengths
• Therapy: Child Life teams, cognitive therapy, group support
Adjuvant Analgesics
Steroids decrease inflammation and are helpful for bone pain related to metastases
– Radiation therapy
– Bisphosphonates
Antispasmodics relieve pain from muscle spasms or intestinal colic
– Baclofen
– Benzodiazepines
Topical analgesics (lidocaine patch)

Adjuvant Analgesics
Anticonvulsants (gabapentin, pregabalin, carbamazepine, valproate, topiramate) reduce neuronal excitability and address neuropathic pain
– Gabapentin 2-5 mg/kg/dose (start QHS, increase to three times a day over several days; max daily dose 60 mg/kg/day or 3 g/day)
– May cause somnolence, dizziness, ataxia, tremor, blurred vision, dry mouth
– Gabapentin has been found to be helpful for extreme irritability in brain-injured children (sometimes requires high doses)
Adjuvant Analgesics: Ketamine
Ketamine is an N-methyl-D-aspartate (NMDA) receptor antagonist and blocks transmission of pain signals
Inhibits the pain wind-up phenomenon, reducing opioid tolerance and opioid-induced hyperalgesia
– May reduce opioid consumption by up to 30%
Adverse effects involve CNS (hallucinations, anxiety, dizziness) and GI (nausea, vomiting) symptoms
Oral dosing: 0.5-1 mg/kg q8-12 hours
Can also be given as an infusion 0.1-0.2 mg/kg/hr
Regional Anesthetic Techniques
Epidural catheter (temporary or tunneled)– Intermittent bolus, continuous infusion, patient-controlled
– Local anesthetics, opioids, clonidine, ketamine
Intraspinal catheter (usually implantable device)
Peripheral nerve blocks (single injection or tunneled catheter)
Benefits: reduce need for opioids, allow for pain relief without sedation
Burdens: require specialized care for insertion and maintenance, can become dislodged, side effects
Questions, Comments or Suggestions? I’m all ears…..
Resources
• Initiative for Pediatric Palliative Care (http://ippcweb.org/index.asp)
• End-of-Life Nursing Education Consortium (ELNEC) http://www.aacn.nche.edu/elnec
• End of Life/Palliative Education Resource Center (EPERC) www.eperc.mcw.edu/
• American Academy of Hospice and Palliative Medicine: www.aahpm.org/
• Children’s Hospitals and Clinics of Minnesota Pediatric Pain Master Class
– http://www.childrensmn.org/services/painpalliativecare/
– http://www.room217.ca/downloads/Pain_Management_in_Pediatric_Palliative_Care.pdf
• WHO guidelines (http://whqlibdoc.who.int/publications/2012/9789241548120_Guidelines.pdf)
• International Association for the Study of Pain (http://www.iasp-pain.org//AM/Template.cfm?Section=Home)
– Pediatric Pain Management article (http://www.iasp-pain.org/AM/Template.cfm?Section=Home&Template=/CM/ContentDisplay.cfm&ContentID=12197)
Bibliography
1. American Academy of Pediatrics Committee on Bioethics and Committee on Hospital Care. (2000). Palliative Care for Children. Pediatrics, 106(2), 351 - 357.
2. Billings, J. (2011). The End of Life Meeting in Intensive Care: Part II: Family Centered Decision Making. Journal of Palliative Medicine, 10 - 23.
3. Billings, J. (2011). The End-of-Life Family Meeting in Intensive Care Part I: Indications, Outcomes, and Family Needs. Journal of Palliative medicine, 14(9), 1042 -1063.
4. DeLisser, H. (2010). How I Conduct the family Meeting to Discuss the Limitation of Life-sustaining Interventions: a Recipe for Success. Blood, 116(10), 1648 - 1654.
5. Ullrich C, M. R. (2013). Pediatric Palliative Care Research Comes of Age: What We Stand to Learn from Children with Life Threatening Illness. Journal of Palliative Medicine, 16(4), 1 - 3.
| 66

From: Cultural Relevance in End-of-Life Care http://ethnomed.org/clinical/end-of-life/cultural-relevance-in-end-of-life-care
1
Kagawa-Singer & Blackhall’s ABCD Cultural Assessment Model
Kagawa-Singer and Blackhall developed a cultural assessment mnemonic approach to assess the degree of cultural adherence to help avoid stereotyping and decrease the risk of miscommunication (Kagawa-Singer & Backhall, 2001). The ABCD cultural assessment is outlined below:
Relevant Information Questions and Strategies for the Health Care Provider
Attitudes of parents and families: • What attitudes does this ethnic /cultural
group in general – and the patient and family in particular – have about truth telling with regard to diagnosis and prognosis?
• What is their general attitude towards discussion of death and dying?
• Do they have positive or negative attitudes about particular aspects of care?
• Increase one’s knowledge about the values, beliefs, and attitudes of the cultural group most frequently seen in your practice.
• Determine the patient and family’s perception of an illness: “What does your illness/sickness mean to you?”
• Determine if the patient uses traditional healing practices and for what problems.
• Determine if the patient or family has positive or negative attitudes about a particular aspect of care being addressed, such as advance directives.
Beliefs: • What are the patient’s and family’s
religious and spiritual beliefs, especially relating to the meaning of death and dying, the afterlife, and miracles?
• “Spiritual or religious strength sustain many people in times of distress. What is important for me to know about your faith or spiritual needs?”
• “How can we support your needs and practices?”
• “Where do you find your strength to make sense of what is happening to you?”
Context: • Determine the historical and political
context of the patient’s and family’s lives, including place of birth, refugee or immigrant status, poverty, experience with discrimination, health disparities, language spoken, and degree of integration within their ethnic community and the degree of assimilation into Western culture.
• “Where were you born and raised?” • “How long have you lived in the United
States?” What has your experience been since coming to the U.S. (or the city)?”
• “How has your life changed since coming to the U.S.?”
• “What language are you most comfortable using when talking about your health care?”
• “What were other important times in your life that might help us better understand your situation?”
Decision-making style: • What is the general decision-making style
of the cultural group and specifically of the patient and family?
• Is the emphasis on the individual decision-making process or the family decision-making process?
• “How are decisions about health care made in your family?”
• “Who is the head of the family?” • “Is there anyone else I should talk to in
your family about your condition?”

From: Cultural Relevance in End-of-Life Care http://ethnomed.org/clinical/end-of-life/cultural-relevance-in-end-of-life-care
2
Environment: • What resources and support are available
to the patient and family? • What resources are available to assist the
health care provider to interpret the significance of the patient’s culture?
• Identify community resources that may be of assistance to the health care provider and the patient and family, such as translators, health care workers from the same community as the patient, community associations, religious leaders, and healers.
Kagawa-Singer, M., & Backhall, L. (2001). Negotiating cross-cultural issues at end of life. Journal of American Medical Association, 286(3001), 2993-.

For personal use. Only reproduce with permission from The Lancet Publishing Group.
THE LANCET • Vol 358 • July 28, 2001 335
CORRESPONDENCE
US drug policy
Sir—I object to your glib indictmenton US drug policy in your March 31editorial.1 The USA had experiencewith harm-reduction drug policy inthe late 1970s. 13 states legalised ordecriminalised marijuana. Thenumber of drug arrests fell. Someleaders in the White House openlyused cocaine, and others supportedits legalisation. Drug use in youngpeople reached a high in around1978.
Rigorous enforcement efforts, user accountability, widespreadprevention, and treatment led tostriking reductions in use. Dailymarijuana use among high schoolseniors dropped from 10·7 % in 1978to 1·9% in 1992,2 as did bingedrinking of alcohol. Unfortunately,our current times are remiscent of the1970’s, but overall restrictive drug policy has been effective.3,4
As drug legalisation advocacy groups have gained strength fromwealthy benefactors since 1992, drug use began to increase. Thecountry lacked focus on drug policy, and the Clinton admin-istration was quite lax on the issue. More recently, leadership forDrug Czar helped to refocus theissue.
Eight states have passed medicalmarijuana legislation. Drug legal-isation campaigns have been waged inseveral states. The Michigan PersonalResponsibility Amendment, whichfailed, sought to make personal useand possession of three marijuanaplants and three ounces of driedmarijuana legal for bona fide seriousand debilitating medical disorders,with the direct consultation of aphysician, and the same amount legalfor any adult aged 21 years or older.However, the amendment alsolimited use of asset forfeiture only toprevention programmes, domesticviolence, or drug, alcohol, or tobaccoawareness. Furthermore, it limitedcauses of action for restitution forloss, disability, or injury that as aresult of someone’s long termsubstance abuse.
The California ballot initiative,Proposition 36, will allow up to only30 days in jail for offenders beyondthe first and second offence.Everything from videotaped treat-ment programmes to internet chatrooms for addicts can qualify for a share of tax dollars. Proposition36 specifically prohibits any of the proposed funding for drug testing, choosing instead to trust drug addicts to hold themselves
accountable; prohibits payment forany treatment longer than 12 months,even though extended treatment isfrequently the most effective approachfor many long-term addicts; does notprovide funding for treatmentprogrammes to help addicts inCalifornia prisons; and wouldundermine California’s highlyeffective individualised addictiontreatment.
More treatment capacity is neededbut should be coupled withenforcement efforts to prevent repeatjail sentences. Drug screening, appliedcarefully as it is in business, couldgreatly reduce drug use in schools.Drug prevention efforts need to bemore widely aimed at at-risk childrenand the general population andfamilies need to be empowered andeducated.
Drug abuse is a public-health and asocial menace. Few other health issuespose such dire and broad-reachingsocial threats. We must be firm but compassionate; forgiving, butunyielding in our pursuit of restrictivedrug policy.
Eric A VothInstitute on Global Drug Policy, Box 11298, St Petersburg, FL 33733, USA
1 Editorial. Rethinking America’s “War OnDrugs” as a public-health issue. Lancet2001; 357: 971.
2 Johnston LD, O’Malley PM, Bachman JG.Monitoring the future survey. NationalInstitute on Drug Abuse, NIH publication00-4690, 2000.
3 DuPont RL, Voth EA. Drug legalization, harm reduction, and drugpolicy. Ann Intern Med 1995; 123:461–65.
4 Voth EA, Levitsky M. Contemporary drugpolicy. Northwest University J Int Policy2000; 21: 17–22.
Proposed definitions forterminal sedation
Sir—Although sedation for symptomrelief for terminally ill patients hasbeen a focus of medical study, theinterpretation of research findings isdifficult because of the confusingterminology.1,2
Many existing reports stress twofactors as the core nature ofsedation:2–4 the presence of intractableor severe distress refractory tostandard palliative treatment; and theuse of sedative medications with the primary aim of relieving severe symptoms by reduction inconsciousness. Thus, to clarify theessential nature of sedation, wepropose the term palliative sedation therapy defined as use ofsedative medications to relieveintractable and refractory distress by
reduction in patient consciousness. In this definition, the patientsdetermine whether their symptoms are intractable, but they must be refractory to standard palliativetreatment established for eachsymptom.
There are large inconsistencies inthe definition of degrees and duration of sedation and pharmacologicalproperties of medications used(pharmacologically effective to relieveunderlying suffering or not), targetsymptoms, and target patients. We propose to handle theseinconsistencies as subcategories ofpalliative sedation therapy.
For degree of sedation, duration,and pharmacological properties ofmedications, we classify sedation intomild to deep, intermittent tocontinuous, and primary to secondarysubgroups, respectively. Mild sedationis to maintain consciousness so thatpatients can communicate withcaregivers, whereas deep sedation isalmost or complete unconsciousness.Intermittent sedation is to providesome periods when patients are alert,and continuous sedation is tocontinue to alter a patient’sconsciousness until they die. Primarysedation is achieved by sedativemedications that have not beenproven to be pharmacologicallyeffective to relieve underlying distress,and secondary sedation is to allowreduced consciousness accompaniedwith pharmacologically effectivemedications for the relief ofunderlying symptoms.
Target symptoms are clarified asbased on standard diagnostic criteriasuch as sedation for pain and sedationfor delirium. To clarify targetpopulations, the general conditionsare described using rating methods forterminal patients,5 or as the presenceor absence of vital organ failure, suchas sedation for terminally ill cancerpatients with a palliative prognosticindex score of 6 or more.
By use of these definitions, sedationcan be expressed as a combination offive subcategories. Thus, terminalsedation in many reports3 can bedescribed as primary-continuous-deepsedation for physical or psychologicaldistress in patients with vital-organfailure. Opioid dose escalation forsevere pain that induces somnolence,not deemed as a type of sedation bymany practitioners,1 can be expressedas secondary-mild sedation for pain inpatients without vital-organ failure,including intermittent-continuoussubtypes of sedation.
We believe that these clarifications of terminology will contribute to

For personal use. Only reproduce with permission from The Lancet Publishing Group.
336 THE LANCET • Vol 358 • July 28, 2001
CORRESPONDENCE
HPS is caused by increased intrapulmonary vasodilatation andshunting, which is thought to bemediated by the excess production ofthe potent vasodialator nitric oxide.2,3
At high altitude, the pulmonaryvasculature is subjected to mildhypoxia, which results in pulmonaryvasoconstriciton.4 Although thepathophysiological mechanism thatleads to the low freqency of HPS inDenver and Salt Lake City is unknown,we speculate that it is related to thegreater degree of pulmonary vasocon-striction that occurs at high altitude.
*J F Trotter, T Box, M Heneghan, R Shrestha *University of Colorado Health Sciences Center,4200 E 9th Avenue, B-154, Denver, CO 80262,USA; LDS Hospital, Salt Lake City, UT; DukeUniversity Medical Center, Durham, NC; andUniversity of North Carolina Hospitals, ChapelHill, NC
1 Fallon MB, Abrams GA. Hepatopulmonarysyndrome. Curr Gastroenterol Rep 2000; 2:40–45.
2 Cremona G, Higenbottam TW, Mayoral V,et al. Elevated exhaled nitric oxide inpatients with hepatopulmonary syndrome.Eur Respir J 1995; 8: 1883–85.
3 Rolla G, Brussino L, Colagrande P, et al.Exhaled nitric oxide and impairedoxygenation in cirrhotic patients before andafter liver transplantation. Ann Intern Med1998; 128: 375–78.
4 Naeije R. Pulmonary circulation at high altitude. Respiration 1997; 64: 429–34.
Hepatopulmonarysyndrome in transplantcentres at differentaltitudes
Sir—Hepatopulmonary syndrome(HPS) is seen in up to 15% of patientswith end-stage liver disease.1 Thedefining features of HPS are hypoxia, chronic liver disease andintrapulmonary shunting in theabsence of cardiopulmonary disease.
After moving from a low-altitudetransplant centre (Durham, NC) to a high-altitude transplant centre(Denver, CO), one of us (JT) noted astriking reduction in the number ofHPS patients. As a result, we reviewedthe frequency of HPS at the twohighest-altitude US transplant centres(Denver and Salt Lake City, UT)compared with two low-altitudetransplant centres in NC.
The number of patients with HPSwho underwent or were listed for livertransplantation during the tenure ofeach researcher at the respectiveinstitutions was recorded. Theproportion of patients with HPS wascalculated relative to the total numberof patients listed for transplant ortransplanted. The altitude of eachcentre (in m above sea level) is: Denver1609; Salt Lake City 1280; Durham120; and Chapel Hill 153. Thefrequency of HPS for the the two high-altitude transplant centres is one per762 (0·13%), and 12 per 850 (1·4%)for the low-altitude centres (p<0·05).
Serious adverse events associated with yellowfever 17DD vaccine in Brazil: a report of twocases—In this Article by Pedro Vasconcelos andcolleagues (July 14, p 91), the labels on thepanels of figure 1 (p 93) were incorrect. A and Bshould be swapped, as should C and D, and E and F.
DEPARTMENT OF ERRORAntihypertensive drug helps prevent strokerecurrence—In this News item by James Butcher(June 23, p 2030), the third paragraph shouldhave read “6105 patients were randomised in172 centres in ten countries. The researchersrandomised patients to a perindopril-basedregimen (4 mg) or placebo. Blood-pressurerecordings in the active treatment group were9/4 mm Hg (systolic/diastolic) lower than in theplacebo group: there was a 28% risk reductionfor stroke during the 4 years of follow up. Bloodpressure was 12/5 mm Hg lower in patients whoreceived combination treatment with perindoprilplus indapamide (2·0 or 2·5 mg), with a 43%risk reduction for stroke.”
improving the accuracy and depth ofthe discussion in this area.We thank Janet Hardy for helpful comments.
*Tatsuya Morita, Satoru Tsuneto, Yasuo Shima
*Seirei Hospice, Seirei Mikatabara Hospital,Shizuoka 466-8558, Japan; HospiceYodogawa Christian Hospital, Osaka; andPalliative Care Unit, National Cancer CentreHospital East, Chiba(e-mail: [email protected])
1 Hardy J. Sedation in terminally ill patients.Lancet 2000; 356: 1866–67.
2 Quill TE, Byock IR. Responding tointractable terminal suffering: the role ofterminal sedation and voluntary refusal offood and fluids. Ann Intern Med 2000; 132:402–14.
3 Chater S, Viola R, Paterson J, Jardis V.Sedation for intractable distress in thedying: a survey of experts. Palliat Med1998; 12: 255–69.
4 Morita T, Tsunoda J, Inoue S, Chihara S.Do hospice clinicians sedate patientsintending to hasten death? J Palliat Care15: 20–23: 1999.
5 Vigano A, Dorgan M, Buckingham J, Bruera E, Suarez-Almazor ME. Survivalprediction in terminal cancer patients: asystematic review of the medical literature.Palliat Med 2000; 14: 363–74.
Comeback of Anophelesfunestus in SahelianSenegal
Sir—Before 1970, Anopheles funestusand A gambiae s l. were the two mainmalaria vectors in the whole of Senegal.After the 1970s’ droughts, A funestusdisappeared from the northen part ofthis country along the Senegal riversystem, as well as from the marshyareas of the Niayes located along theAtlantic Coast, 50 km north of Dakar.The absence of this vector species wasfollowed by a striking decrease (>80%)of malaria prevalence and incidence.1,2
However in November 1999, A funestus was reported again in asurvey made in Keur-Mbaye village,near Richard-Toll town in the Senegalvalley. A funestus accounted for 14·3%of the anopheline species collectedduring human landing captures (558specimens per person for every 10nights) and for 77·9% by pyrethrumindoor-spraying collections (tenhouses). In comparison, A gambiae s laccounted for only 10% in spraycollections and the non-vector A wellcomei for 51% (on human baits).Only a few A pharoensis were caught.Therefore, A funestus seemed to be the
dominant species in this area where ithas been absent for nearly 30 years.
In the Niayes, where A funestus wasthe dominant species before 1970, afterwhich it disappeared, this species wasstill absent in 1999.
In this part of Africa, where rainfallvaries greatly each year, the pluviometrywas average in 1998 and 1999, with laterains in October, 1999. Rainfall doesnot seem to have led to the comebackof A funestus. However, all along theSenegal River many developmentprojects have been carried out since theedification of the Manantali dam inMali and the antisalt dam of Diama inthe lower part of the Senegal River.
We strongly suspect that environ-mental changes, mainly due to thedevelopment of irrigation systems, havecreated favourable conditions for thereestablishment of A funestus. At theopposite in the Niayes areas, thatbecame unsuitable to A funestus sincethe 1970s’ droughts, the environmenthas not changed and A funestus is stillabsent.
Senegalese health services are awareof the risk from the re-establishment ofA funestus and a surveillance system isbeing set up to prevent an increase ofmalaria incidence.
*L Konate, A Diop, N Sy, M N Faye, Y Deng, A Izri, O Faye, J Mouchet*University of Dakar, Senegal; and UniversityParis 13, France, IRD, 75480 Paris, France
1 Faye O, Gaye O, Fontenille D, et al.sécheresse et la baisse du paludisme dans lesNiayes, Sénégal. Cahiers Santé 1995; 5:299–305.
2 Mouchet J, Faye O, Julvez J, Manguin S.Drought and malaria retreat in the Sahel, west Africa. Lancet 1996; 348:1735–36.
The idea and the experiment—In this Corresp-ondence letter by Henry Gans (Jan 13, p 148),the address listed should have been “522Colorado Avenue, Stuart, FL 34994, USA”.

Evidence for Improving Palliative Care at the End of Life:A Systematic ReviewKarl A. Lorenz, MD, MSHS; Joanne Lynn, MD, MA, MS; Sydney M. Dy, MD; Lisa R. Shugarman, PhD; Anne Wilkinson, MS, PhD;Richard A. Mularski, MD, MSHS, MCR; Sally C. Morton, PhD; Ronda G. Hughes, RN, MHS, PhD; Lara K. Hilton, BA;Margaret Maglione, PhD; Shannon L. Rhodes, MS; Cony Rolon, BA; Virginia C. Sun, BS, MSN; and Paul G. Shekelle, MD, PhD
Background: Many persons and their families are burdened byserious chronic illness in late life. How to best support quality of lifeis an important consideration for care.
Purpose: To assess evidence about interventions to improve pallia-tive and end-of-life care.
Data Sources: English-language citations (January 1990 to Novem-ber 2005) from MEDLINE, the Database of Abstracts of Reviews ofEffects, the National Consensus Project for Quality Palliative Carebibliography, and November 2005 to January 2007 updates fromexpert reviews and literature surveillance.
Study Selection: Systematic reviews that addressed “end of life,”including terminal illness (for example, advanced cancer) andchronic, eventually fatal illness with ambiguous prognosis (for ex-ample, advanced dementia), and intervention studies (randomizedand nonrandomized designs) that addressed pain, dyspnea, depres-sion, advance care planning, continuity, and caregiving.
Data Extraction: Single reviewers screened 24 423 titles to find6381 relevant abstracts and reviewed 1274 articles in detail toidentify 33 high-quality systematic reviews and 89 relevant inter-vention studies. They synthesized the evidence by using the Grad-ing of Recommendations, Assessment, Development, and Evalua-tion (GRADE) classification.
Data Synthesis: Strong evidence supports treating cancer pain withopioids, nonsteroidals, radionuclides, and radiotherapy; dyspnea
from chronic lung disease with short-term opioids; and cancer-associated depression with psychotherapy, tricyclics, and selectiveserotonin reuptake inhibitors. Strong evidence supports multi-component interventions to improve continuity in heart failure.Moderate evidence supports advance care planning led by skilledfacilitators who engage key decision makers and interventions toalleviate caregiver burden. Weak evidence addresses cancer-relateddyspnea management, and no evidence addresses noncancer pain,symptomatic dyspnea management in advanced heart failure, orshort-acting antidepressants in terminal illness. No direct evidenceaddresses improving continuity for patients with dementia. Evidencewas weak for improving caregiver burdens in cancer and wasabsent for heart failure.
Limitations: Variable literature indexing for advanced chronic illnessand end of life limited the comprehensiveness of searches, andheterogeneity was too great to do meta-analysis.
Conclusion: Strong to moderate evidence supports interventions toimprove important aspects of end-of-life care. Future researchshould quantify these effects and address the generalizability ofinsights across the conditions and settings of the last part of life.Many critical issues lack high-quality evidence.
Ann Intern Med. 2008;148:147-159. www.annals.orgFor author affiliations, see end of text.
Americans struggling with symptoms and disability of-ten die of chronic illness, and improving care during
this period is important (1, 2). About 30% of Medicare’sexpenditures arise in patients’ last year of life, and outlayswill increase as the population ages (3). Hospices servemost Americans dying of cancer and 10% of all others (3).More than 25% of hospitals had palliative care services in2003 (4). Even with growing specialization in palliativemedicine and geriatrics, generalist physicians will providemost services.
People tend to follow characteristic patterns of clinicaland functional decline as they approach the end of life.The clinical course exemplified by cancer often ends withobvious decline in the last weeks or months (5). In con-trast, organ system failure tends to cause long-term lack ofreserve and intermittent serious exacerbations, making thetiming of death unpredictable (6, 7). A third group markedby frailty and often dementia usually declines slowly (6–8,8) (Appendix Figure, available at www.annals.org). Orga-nizing our report around these 3 common trajectories, wesystematically reviewed the literature to address the follow-ing questions posed by the American College of PhysiciansClinical Efficacy Assessment Subcommittee:
1. What are the critical elements for clinicians to ad-dress when caring for persons coming to the end of life?
2. What do definitions of the end of life suggest aboutidentifying patients who could benefit from palliative ap-proaches?
3. What treatment strategies work well for pain, dys-pnea, and depression?
4. What elements are important in advance care plan-ning for patients coming to the end of life?
See also:
PrintRelated article. . . . . . . . . . . . . . . . . . . . . . . . . . . . . 141Summary for Patients. . . . . . . . . . . . . . . . . . . . . . . I-42
Web-OnlyAppendix TablesAppendix FigureCME quizConversion of graphics into slidesAudio summary
Annals of Internal Medicine Clinical Guidelines
© 2008 American College of Physicians 147

5. What elements of collaboration and consultation areeffective in promoting improved end of life care?
6. What elements of assessment and support are effectivefor serving caregivers, including family, when patients arecoming to the end of life?
METHODS
ObjectivesWe reviewed evidence for the National Institutes of
Health (NIH) State-of-the-Science Conference on Improv-ing End-of-Life Care in December 2004 and updated itthrough November 2005 to support guideline develop-ment by the American College of Physicians. In addressingthe 6 questions posed by this report, we focused on theclinical problems and literature related to pain, dyspnea,and depression; advance care planning; continuity; andcaregiver concerns because they are especially important topatients and families (9). We focused on cancer, chronicheart failure, and dementia to illustrate differences in pa-tient and caregiver experiences in the 3 characteristic tra-jectories of clinical and functional decline (5–8).
Literature SearchNational Library of Medicine librarians searched
MEDLINE for English-language publications (January1990 to April 2004), and 1 reviewer used the Database ofAbstracts of Reviews of Effects to search for reviews oncancer, congestive heart failure (CHF), and dementia. Weadded citations identified by the National ConsensusProject for Quality Palliative Care (10). An advisory paneland peer reviewers suggested additional references untilSeptember 2004. We updated the original search strategythrough November 2005 and further updated the litera-ture to January 2007 by using the American Academy ofHospice and Palliative Medicine literature surveillance (forexample, Fast Article Critical Summaries for Clinicians inPalliative Care) and the Annual Update (available at www.aahpm.org/membership/pcfacs.html). We did not searchgray literature because it did not contribute to a recentreview of the effectiveness of palliative care teams (11).
Literature Selection and AbstractionEight reviewers familiar with palliative care formed
topic-oriented, 2-person teams. We accepted English-language publications from the United States, Canada,Western Europe, Australia, and New Zealand. We in-cluded studies about the definition of end-of-life care. Ad-vance care planning reports had to address process or out-comes for patients and families (not just clinicians).Continuity publications had to address relationships withproviders over time (12). Informal caregiving articles ex-cluded bereavement. We described spiritual care outcomeswhen reported with emotional well-being. We rejectedstudies that addressed only surgery, chemotherapy, radio-therapy, stents, lasers, and similar technical interventionsor if they reported only physiologic, laboratory, or radio-logic outcomes. We characterized articles by research de-
sign quality, study population, settings, intervention, andoutcomes. Studies addressing several topics are included ineach topic’s section.
Several methods reduced bias and enhanced accuracy,and 1 reviewer screened each citation. Two experts in sys-tematic reviews conducted a structured, implicit evaluationof the quality of reviews. For intervention studies, eachreviewer completed a training set, and 1 principal investi-gator reviewed a random subset from each reviewer’s cita-tions and double-reviewed outlier sets. Reviewers discusseduncertain decisions, and we abstracted full articles inteams, coming to consensus after independent review. Twoprincipal investigators reviewed abstractions from articles,and we used piloted, standard forms throughout.
Data AnalysisThe variety of outcome measures and study designs
required qualitative synthesis of the evidence. We evaluatedthe strength of evidence related to each of the 6 questionsfor each of the 3 clinical and functional trajectories (forexample, cancer, CHF, and dementia) (5–8). We discussspecific interventions only for reports not previously cov-ered in high-quality reviews. We rated the study design,quality, consistency, and directness in each domain accord-ing to the Grading of Recommendations, Assessment, De-velopment, and Evaluation (GRADE) system, yielding rat-ings of the strength of evidence of high, moderate, low, orvery low (13). In each area, we rated the overall evidencebased on unique studies within each domain, qualitativelytaking into account studies addressed by several reviews.
Role of the Funding SourceThe Agency for Healthcare Research and Quality
(AHRQ) and the National Institute of Nursing Researchfunded our initial systematic review. An advisory groupfrom the National Institute of Nursing Research shapedour initial aims and review priorities. We complied withthe methodological standards of the AHRQ and the Na-tional Institutes of Health Office of Medical Applicationsof Research (available at www.ahrq.gov/clinic/epcsums/eolsum.htm) (14). The funding sources played no role inthe analysis of the data or decision to submit this materialfor publication. We produced this updated report undercontract to the American College of Physicians Clinical Ef-ficacy Assessment Subcommittee. This research did not in-volve human participants.
RESULTS
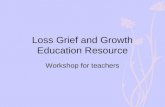
Literature FlowThe April 2004 search identified 24 423 titles, from
which we identified 6381 potentially relevant abstracts andthen 1274 potentially relevant articles. Accepted articlesincluded 95 systematic reviews and 109 reports of inter-ventions. The November 2005 update identified an addi-tional 944 titles, including 8 systematic reviews and 19reports of interventions. After November 2005, expertsources added an additional 3 systematic reviews and 3
Clinical Guidelines Evidence for Improving Palliative Care at the End of Life
148 15 January 2008 Annals of Internal Medicine Volume 148 • Number 2 www.annals.org

interventions. This report includes 33 high-quality system-atic reviews and 89 intervention reports (Figure). Appen-dix Tables 1 to 5 (available at www.annals.org) providedetails about the literature cited.
What Are the Critical Issues for Clinicians to Addresswhen Caring for Persons Nearing the End of Life?
Expert opinion and qualitative research have charac-terized priority concerns for patients in late life (15–19).One national survey defined whether patients, caregivers,and providers have similar concerns (15), and an after-death survey evaluated whether health care achieves theseends (20). Important topics include preventing and treat-ing pain and other symptoms, supporting families andcaregivers, ensuring continuity, making informed deci-sions, attending to emotional well-being (including spiri-tual concerns), sustaining function, and surviving longer.The studies addressed various illnesses and settings, show-ing that dying patients and their families generally sharethese concerns.
What Do Definitions of End of Life Suggest aboutIdentifying Patients Who Could Benefit from PalliativeApproaches?
The literature used various approaches to identify pa-tients at the end of life. Some used clinician assessment of“active dying” or “patient readiness,” but no precise defi-nitions or performance characteristics of these terms havebeen published. Many studies used specified clinical char-acteristics, survival prediction rules, or physician judgment(21). Although prognostic tools usefully characterize sub-populations (for example, heart failure), many patientswith fatal conditions have substantial probabilities for 2- or6-month survival, even in their last week of life (6, 7).Patients with metastatic cancer, who have an estimated10% or greater chance of dying within 6 months, are morelikely to prefer to avoid resuscitation, even when survivalwas much less likely than they acknowledged (22). Thus,clinicians might define the end of life as having a fatalcondition, risking death with the next exacerbation, or be-
Figure. Study flow diagram.
*From the American Academy of Hospice and Palliative Medicine Fast Article Critical Summaries for Clinicians in Palliative Care and Annual Updates,November 2006 to January 2007. †Some reviews and interventions were relevant to more than 1 domain.
Clinical GuidelinesEvidence for Improving Palliative Care at the End of Life
www.annals.org 15 January 2008 Annals of Internal Medicine Volume 148 • Number 2 149

ginning to acknowledge the seriousness of the situation(23). Asking clinicians “Would it be a surprise if this pa-tient were to die within 6 months?” is being used widelybut also has had no rigorous testing (24). The studies em-phasize that acknowledging death risk is important for de-cision making. Waiting for near-certainty would fail toidentify most dying people, so palliative approaches needto be regularly incorporated for people living with seriousillnesses.
What Treatment Strategies Work Well for Pain,Dyspnea, and Depression?Pharmacologic and Complementary and Alternative MedicineTreatments for Pain
Nine systematic reviews focused on pain (25–33), ofwhich 4 addressed cancer pain (26, 27, 30, 31) (Table andAppendix Table 1), and several addressed pharmacologicand complementary and alternative medicine treatments(28–31). Our update identified reviews of the efficacy ofopioids in noncancer pain (32) and local anesthetics forneuropathic pain (33).
A methodologically robust review of cancer pain eval-uated patients in randomized trials receiving nonsteroidals,breakthrough medications, spinal and other adjuvants,opioid trials, chemotherapeutic agents, external-beamradiation and radionuclides, alternative medicine, andbisphosphonates (for metastatic bone pain or painful com-plications, and most studies of breast cancer and also somestudies including myeloma). Seventeen studies generallysupported the use of nonsteroidals, opioids, bisphospho-nates, and radiotherapy or radiopharmaceuticals. Heteroge-neity of study design barred comparisons of specific opioidsor opioid delivery strategies. The review also affirmed theeffectiveness of neurolytic celiac plexus block for pain reliefin visceral cancer (26). Two reviews found insufficient evi-dence on exercise or acupuncture (30, 31), and 2 reviews ofcomplementary and alternative medicine approaches foundvarying effects, which were partly attributed to study heter-ogeneity and small numbers of participants (28, 29).
We identified 24 additional studies (of 23 pain inter-ventions) (34–57) (Appendix Table 5). Most focused oncancer or cancer-predominant populations. Ten trials wererandomized or controlled, with 9 targeting opioid delivery(36, 43, 44, 49, 50, 52–54, 56, 57) and 1 evaluatingbisphosphonates (55). Others studies addressed heteroge-neous interventions (for example, reflexology, aroma-therapy, massage, exercise, and toileting) (38–40, 47).Randomized or controlled trials of pharmacologic or com-plementary and alternative medicine approaches added lit-tle to published systematic reviews.
Care Delivery Interventions for Pain
Among systematic reviews and meta-analyses of pain,1 provided a meta-analysis of the effects of palliative careteams on pain (25) and 2 focused on the clinical organiza-tion of services (27, 29). Few studies in the review of multi-
disciplinary teams addressed hospital-based palliative careconsultation services, whereas the rest addressed non-specialist physicians and nurses working in hospitals, nurs-ing homes, and home settings. The review identified 43studies, including 6 randomized studies (25). Twenty stud-ies of team interventions found palliative care to be betterthan usual care (effect size, 0.13 [95% CI, 0.11 to 0.63]).A review of supportive services for cancer (27) included 27reports that addressed pain, many of which overlappedwith the previous review. Mixed evidence supported clini-cal pathways, patient education, and massage.
Of the 24 additional studies of pain, we identified 9intervention studies about service delivery (34, 35, 37, 41,42, 45, 46, 48, 51), of which 4 were randomized, con-trolled trials (RCTs). Informal caregivers of patients receiv-ing intensive palliative home nursing care just before deathrated the patient’s pain as alleviated in after-death surveys(2.52 vs. 3.00 on a 4-point scale; P � 0.050) (41, 42).A cluster-randomized trial of hospital-based palliative carecollaborating with community-based primary care provid-ers did not improve the European Organization for Re-search and Treatment of Cancer Quality-of-Life Question-naire C30 pain scores (45). Compared with the positivefindings of the review of multidisciplinary teams (25), 1study randomly assigned outpatient clinics for palliativecare team consultation. Participants with chronic obstruc-tive pulmonary disease (COPD), CHF, and cancer (50intervention, 40 control) had no benefit on several painitems (from the Brief Pain Inventory) (37). Another inter-vention provided quality-of-life feedback to clinicians dur-ing a visit and did not change pain on the Short Form-36Health Survey (48).
Strong evidence from consistent randomized trialssupports treating cancer pain with nonsteroidals, opioids,radionuclides, and radiotherapy. Less consistent evidencesupports the use of bisphosphonates for pain. Weak evi-dence, mostly from nonrandomized designs in cancer-predominant populations, supports multidisciplinary teams.No evidence addressed pain management in advancedheart failure or dementia. Although a recent review dem-onstrated the efficacy of opioids for noncancer pain (32),opioid use is controversial in noncancer pain (58).
Palliative care services are becoming common, al-though their effectiveness is not well tested. Small studiessuggest that pain is common and severe in advanced non-cancer conditions (59, 60). Thus, research priorities shouldaddress pain in advanced noncancer conditions and servicedelivery strategies generally.
Pharmacologic and Complementary and Alternative MedicineTreatments for Dyspnea
Seven systematic reviews addressed dyspnea (27, 28,61–65), of which 3 addressed COPD (62, 64, 65) and 3addressed mixed diseases (28, 61, 63) (Table and Appen-dix Table 1). Twelve additional reports of interventions
Clinical Guidelines Evidence for Improving Palliative Care at the End of Life
150 15 January 2008 Annals of Internal Medicine Volume 148 • Number 2 www.annals.org

included dyspnea evaluation (37, 41, 42, 45, 46, 48, 57,66–70) (Table and Appendix Table 5). Four reviews fo-cused on pharmacology (61, 63–65), and a review of com-plementary and alternative medicine included several stud-ies with dyspnea outcomes (28).
One review identified 34 randomized trials of oxygenfor COPD, cancer, and CHF. Nine trials addressed the useof oxygen for long-term relief, with mixed results. Twentyof 22 studies in COPD showed either improved enduranceor reduced dyspnea with oxygen for short-term relief withexercise. Three small studies in cancer showed improve-ment, although 1 found oxygen equivalent to room air(63). A review of randomized trials testing at least 4 weeksof rehabilitation for COPD identified 12 trials with re-duced dyspnea (effect size, 0.62 [CI, 0.35 to 0.89]). Lower-extremity training enhanced effective rehabilitation (62).
A review of opioids for dyspnea in advanced lung dis-ease identified 18 double-blind, randomized studies.Twelve trials addressed COPD, and 2 addressed cancer.Meta-analysis of 13 studies showed benefit (effect size,
�0.31 [CI �0.50 to �0.13]). Nebulized and oral opioidswere equivalent. Constipation, nausea, and vomiting werethe most common side effects. Four studies measured ar-terial blood gases, and 9 measured oxygen saturation. Onestudy found a significant but clinically trivial increase inPCO2 during treatment with dihydrocodeine (61). Of theother relevant reviews, 1 review of 33 unique RCTs dem-onstrated the effectiveness of �-agonists (65). Few studiesof theophylline evaluated dyspnea as an outcome (64), andweakly designed complementary and alternative medicinestudies demonstrated conflicting results (28).
Twelve additional studies (11 unique interventions)explored treatments for dyspnea, and these studies focusedon several diseases in which dyspnea is prominent (37, 41,42, 45, 46, 48, 57, 66–70). Three studies (2 RCTs) fo-cused on cancer (46, 48, 66), and 2 more RCTs focused oncancer-predominant hospice patients (41, 42, 45). TwoRCTs targeted heart failure (67, 70) and COPD, respec-tively (68, 69), and 1 controlled clinical trial targeted all 3conditions (37).
Table. Summary of Systematic Reviews and Additional Intervention Studies of Palliative and End-of-Life Care*
Domain Literature Identified† Summary of Evidence and GRADE Rating‡
SymptomsPain 9 systematic reviews (25–33) and 24
reports of interventions (34–57)Strong evidence supports approaches to treating cancer pain with
nonsteroidals, opioids, radionuclides, and radiotherapy. Less consistentevidence supports use of bisphosphonates for pain or painfulcomplications (for example, fracture). Weak evidence supportsmultidisciplinary teams. No evidence addressed pain management inadvanced heart failure or dementia.
Dyspnea 7 systematic reviews (27, 28, 61–65) and12 reports of interventions (37, 41, 42,45, 46, 48, 57, 66–70)
Strong evidence supports treating dyspnea with �-agonists and opioiduse in COPD, although these trials are small and short in duration.Weak evidence supports opioid use for relieving dyspnea in cancer.Strong evidence supports pulmonary rehabilitation and oxygen forimproving symptoms during short-term exercise in COPD. Evidence foroxygen use in cancer is weak, and few studies address it. Weakevidence supports care delivery interventions for dyspnea. No evidenceaddressed symptomatic dyspnea management in advanced heartfailure.
Depression 4 systematic reviews (26, 27, 30, 71) and9 reports of interventions (35, 37,39–42, 72–74)
Strong evidence supports psychotherapy, as well as tricyclicantidepressants and SSRIs, for depression treatment in cancer.
Advance care planning 9 systematic reviews (25, 29, 75–81) and32 reports of interventions (35, 82–112)
Moderate evidence supports multicomponent interventions to increaseadvance directives; however, such studies seldom measure clinicallyimportant outcomes. Recent research supports care planning throughengaging values, involving skilled facilitators, and focusing on keydecision makers (for example, patients, caregivers, and providers).
Continuity 9 systematic reviews (25, 27, 29,113–118) and 12 reports ofinterventions (103, 104, 112, 119–127)
Moderate evidence supports multidisciplinary interventions that targetcontinuity to affect utilization outcomes. Evidence is strong forreducing readmissions in heart failure, but insufficient evidence wasavailable for other conditions. Successful interventions involvedmultidisciplinary teaming, addressed patient needs across settings andover time, and facilitated communication by personal andtechnological means.
Caregiver burdens 8 systematic reviews (25, 27, 29,129–133) and 19 reports ofinterventions (103, 104, 134–150)
Weak to moderate evidence suggests that caregiver interventions,especially when comprehensive and individually targeted, can improvevarious measures of caregiver burden, although effect sizes are small.Moderate evidence suggests that palliative care interventions improvecaregiver satisfaction. Existing research has focused on dementia and,to a lesser extent, cancer.
* COPD � chronic obstructive pulmonary disease; GRADE � Grading of Recommendations, Assessment, Development, and Evaluation; SSRIs � selective serotoninreuptake inhibitors.† Appendix Tables 1 to 5 (available at www.annals.org) describe details of individual studies and the overlap of studies included in the various systematic reviews.‡ The GRADE standards rate evidence by considering 4 attributes of available literature: study design, study quality, consistency or similarity in the results of studies, anddirectness or relevance of the findings (13).
Clinical GuidelinesEvidence for Improving Palliative Care at the End of Life
www.annals.org 15 January 2008 Annals of Internal Medicine Volume 148 • Number 2 151

Additional studies tested various clinical interventions.Two studies focused on oxygen and morphine in cancerand COPD (66, 68), 1 evaluated acupuncture in COPD(69), and 2 assessed exercise and inspiratory muscle train-ing for CHF (67, 70). Two of these studies were random-ized. In the first 33 nonhypoxemic patients (31 with ad-vanced lung cancer), oxygen did not improve 6-minutewalk distance, dyspnea, or fatigue (66). A randomized,double-blind, placebo-controlled crossover study of mor-phine in 48 patients, 42 of whom had COPD, showed lessdyspnea on a visual analogue scale, both in the morning(�6.6 mm [CI, �1.6 mm to �11.6 mm) and in theevening (�9.5 mm [CI, �3.0 mm to �16.1 mm), as wellas improved sleep (1 vs. 8 dyspnea-related awakenings).Despite routine use of laxatives, constipation worsened,and 1 patient discontinued morphine because of sedation.Patients had no adverse respiratory outcomes (68).
Care Delivery Interventions for Dyspnea
A review of supportive cancer services identified manystudies, but only 6 measured dyspnea. Two randomizedtrials showed improvement with nurse-led patient trainingin coping techniques, including relaxation (27).
The 6 additional intervention studies of dyspnea thataddressed care delivery interventions evaluated 5 servicedelivery models (37, 41, 42, 45, 46, 48). Of the random-ized studies, 1 project randomly assigned 2 general medi-cine clinics to palliative care interventions for chronic lungdisease and CHF (85% of patients with dyspnea). Inter-vention patients were more often breathing comfortably(odds ratio, 6.07 [CI, 1.04 to 35.56]), and physical limi-tations due to dyspnea improved for intervention patientsand worsened among control patients (37). Facilitatedpatient–provider communication did not improve physicalsymptoms (48). Two randomized interventions, 1 of inten-sive palliative home nursing care just before death fromcancer and another of consultation with community-basedproviders for patients with cancer, showed no impact ondyspnea, although evaluation of dyspnea was very limited(41, 42, 45).
Strong evidence from consistent, high-quality RCTssupports treating dyspnea with �-agonists, and strong evi-dence from small but high-quality RCTs of short durationsupports opioid use in COPD. Weak evidence supportsopioid use for relieving dyspnea in cancer. Strong evidencefrom consistent, moderate-quality RCTs supports pulmo-nary rehabilitation, and consistent evidence from RCTssupports the use of oxygen for improving symptoms duringshort-term exercise in COPD. Evidence for oxygen use incancer is weak, and few studies address it. Weak evidencefrom few studies with mixed results support care deliveryinterventions for dyspnea. No evidence addressed symp-tomatic dyspnea management in advanced heart failure.Strengthening the evidence base for dyspnea management
in cancer and heart failure is particularly critical becausedyspnea is common in these conditions.
Pharmacologic and Complementary and Alternative MedicineTreatments for Depression
Four reviews addressed depression or mood, and allfocused on cancer (26, 27, 30, 71) (Table and AppendixTable 1). We identified an additional 9 reports about in-terventions to improve depression or mood (35, 37, 39–42, 72–74) (Table and Appendix Table 5). Reviews ofguided imagery and exercise identified a few studies withmixed results on mood in cancer (30, 71).
One methodologically robust review identified 11controlled trials of antidepressants and 1 trial of pain anddepression treatment in cancer. Tricyclic antidepressantsand selective serotonin reuptake inhibitors were uniformlyeffective, given sufficient treatment duration (that is, �6weeks). This review also found strong, consistent efficacyfrom RCTs of various psychosocial interventions (that is,education, cognitive and noncognitive behavioral therapy,informational interventions, and individual and group sup-port) (26).
Nine additional reports (8 interventions, including 3randomized trials focused on care delivery innovations) ad-dressed depression or existential well-being (35, 37, 39–42, 72–74). Seven of these focused on cancer, and only 2focused on noncancer populations (37, 72). Of those ad-dressing clinical interventions, 3 addressed aromatherapy(39, 40, 73), and 1 addressed antidepressants and anti-psychotics in inpatients with dementia (72).
Care Delivery Interventions for Depression
A review of supportive cancer care identified studiesthat addressed social and spiritual support. Among diversestudies examining depression outcomes, behavioral inter-ventions were generally effective, but evidence was mixedabout delivery system interventions (27).
Four additional interventions reported service innova-tions (35, 37, 41, 42). Of these, a randomized trial ofpalliative outpatient care for previously treated patientswith depression found no effect on depression, althoughspiritual well-being (evaluated with a 20-item scale) improvedonly for intervention patients (37). Two methodologicallylimited randomized trials of a portable health record andintensive home care support, mostly of patients with cancerwho were very near death, did not change depression (35,41, 42). A before-and-after study of “dignity therapy,”which included psychotherapy and facilitated life recall,improved both existential and emotional well-being (74).
When depression has been identified, strong evidencefrom several high-quality RCTs supports psychosocial in-terventions to treat depression in cancer. Although derivedfrom fewer studies, RCTs consistently support tricyclic anti-depressants and selective serotonin reuptake inhibitors fortreating depression in cancer when treatment lasts 6 weeks
Clinical Guidelines Evidence for Improving Palliative Care at the End of Life
152 15 January 2008 Annals of Internal Medicine Volume 148 • Number 2 www.annals.org

or longer. Critical gaps include that the evidence base doesnot address late-stage cancer (for example, terminal care) ordelivery system changes. Existing evidence does not sup-port palliative care delivery interventions. No evidence ad-dressed depression management in advanced heart failureor dementia.
What Issues Are Important in Advance Care Planning forPatients Approaching the End of Life?
Nine systematic reviews addressed establishing goals ofcare and advance care planning (25, 29, 75–81), and 32additional reports addressed interventions to improve ad-vance care planning (35, 82–112) (Table and AppendixTables 1 and 2). An older review (10 randomized trials)found inconclusive evidence for whether conveying badnews improved short-term patient knowledge, psychologi-cal adjustment, and satisfaction (75). One review con-cluded that multicomponent interventions yield more ad-vance directives than limited strategies do. An older reviewmeasured similar conclusions (76), and 10 RCTs since1997 compared advance directive delivery methods (79).Seven studies (4 RCTs) evaluated effective outcomes ofadvance care planning: None found harms, and 2 werepositive (78). A systematic review of factors influencingdeath at home found 58 observational studies, and theexpression and recording of preferences for dying at homewas strongly associated with that outcome in the 15 high-est-quality studies (80). A recent review found that patientand surrogate preferences were often concordant (an aver-age of 68% in 16 studies involving 19 526 paired re-sponses) (81).
Two reviews addressed utilization outcomes. Nurse-facilitated decision making; ethics consultation; and family,provider, and patient communication interventions re-duced end-of-life care use in intensive care (77). A meta-analysis of palliative care teams’ effects identified 9 mostlyobservational studies that suggested more frequent death athome with palliative care (effect size, 0.28 [CI, 0.11 to0.71]). The significance of this effect, however, dependedon inclusion of the National Hospice Study, a large dem-onstration of hospice care from 25 years ago, which maynot reflect current practices (25).
We found 32 additional studies (30 interventions,with 13 randomized trials) related to goals of care andadvanced care planning (35, 82–112). Four studies ad-dressed relatively healthy outpatients; 15 addressed unspec-ified illnesses mostly in high-intensity settings; and the re-mainder addressed CHF, COPD, dementia, AIDS, anddialysis. Interventions in the highest-quality designs (RCTsor controlled clinical trials with randomization by provideror site) tested multidisciplinary decision making in a nurs-ing home (86, 93), advance care planning workbook (94),peer mentoring (95), ethics team consultation (103, 104),preoperative structured care planning (98), nursing homequality improvement (105), and the effects of directives onmutual understanding (87). Several RCTs focused on ap-
proaches to increasing advance directive completion or sur-rogate–patient understanding (82, 89, 97, 107, 111, 112).
Six of the randomized studies tested skilled facilitatorsor goals clarification (86, 93, 94, 98, 103, 104). A study of198 nursing home residents used goals-oriented interviewswith conclusions communicated to nursing home physi-cians to increase hospice use from 1% to 20% (P � 0.001)(86). Documented treatment limitations and preference-concordant care increased for patients served by socialworkers experientially trained in care planning (93). Ethicsteam consultation reduced days in the intensive care unit(ICU) (�1.44 days; P � 0.03), hospital (�2.95 days, P �0.01), and ventilator (�1.7 days; P � 0.03) without re-ducing length of life (103, 104). For patients with AIDS, avalues-oriented program facilitated by social work (“YourLife, Your Choices” workbook) improved rates of physi-cian discussion (64% vs. 38%; P � 0.001), living wills(48% vs. 23%; P � 0.001), and patient–provider andpatient–caregiver understanding (94). A manual (“Re-specting Choices”) and nurse facilitator successfully pro-moted understanding among patients preparing for cardiacsurgery (98). A controlled, quality improvement interven-tion in nursing homes increased hospice enrollment, painmanagement orders, and in-depth discussions about pallia-tive care (105). Two nonrandomized, quality improvementinterventions showed substantial effects with structured or-ders for dying hospitalized patients (110) and implement-ing a clinical pathway (109).
Moderate evidence suggests that multicomponent in-terventions increase advance directives. Although thesestudies seldom measure clinically important end points,expressed preferences are associated with death at home inobservational studies. Recent research suggests that engag-ing values; involving skilled facilitators; and including pa-tients, caregivers, and providers can increase the rates andeffectiveness of communication about late-life goals andadvance care planning. Many studies focused on settings inwhich a wide spectrum of serious conditions is typicallyrepresented (for example, ICU, hospital, and nursinghome), underscoring that palliative care approaches aregenerally effective when patients are living with serious ill-nesses.
What Opportunities for Collaboration and ConsultationAre Effective in Promoting Improved End-of-Life Care?
Nine systematic reviews addressed continuity (25, 27,29, 113–118), including 1 largely subsumed by more re-cent reviews (115) and 1 discussed in the previous section(25) (Table and Appendix Table 1). One review focusedon cancer, 2 on COPD, 3 on CHF, and 2 on palliative orend-of-life care. Our review identified 11 additional inter-vention studies (103, 104, 112, 119–127) (Table and Ap-pendix Table 4).
A review of case management in end-of-life care iden-tified 4 RCTs, with 2 that evaluated utilization, havingmixed effects (29). A review of improved coordination for
Clinical GuidelinesEvidence for Improving Palliative Care at the End of Life
www.annals.org 15 January 2008 Annals of Internal Medicine Volume 148 • Number 2 153

supportive cancer care identified 9 RCTs of portablerecords (mostly negative) or palliative care–home care co-ordination (with mixed effects for patient, caregiver, andutilization) (27). A review of nurse care management forCOPD found 9 RCTs, with 1 reporting reduction in re-admission (113). A review and meta-analysis of intensivein-home support from respiratory care nurses teamed withhospital support for COPD (7 RCTs) showed reducedhospital days and costs but unchanged readmissions (114).
For CHF, a review identified 29 RCTs of multidisci-plinary teams after hospitalization, which always reducedhospitalizations with team follow-up (relative risk, 0.81[CI, 0.71 to 0.92]) or enhanced self-care (relative risk, 0.73[CI, 0.57 to 0.93]). Telephone contact and advice reducedheart failure but not all-cause hospitalizations (116). An-other review (15 RCTs) focused on interventions to reduceutilization or improve patient outcomes. Both reviewsfound improvement in half of the studies examining qual-ity of life or functional status (116, 118). By pooling qual-ity-of-life scores for 6 RCTs, 1 study reported a statisticallysignificant improvement with after-hospital disease man-agement (26% vs. 14%; P � 0.01) (117). Although studiestypically excluded terminally ill persons, trials enrolled pa-tients with advanced illness and substantial mortality rates(that is, approximately 5% to 20% 6- to 12-month mor-tality rates).
Twelve additional reports (11 interventions) addressedmanagement and informational and relational aspects ofcontinuity (103, 104, 112, 119–127). These reports in-clude 3 RCTs or controlled clinical trials addressing heartfailure (120, 122, 125) and 7 RCTs or controlled clinicaltrials (of 6 interventions) addressing mixed or other condi-tions, including frailty (103, 104, 112, 123, 124, 126,127). Two were discussed in the previous section (103,104). Intensive medication counseling in stable heart fail-ure improved adherence and decreased edema and dyspnea(125). Results of 2 studies, 1 that used a nurse care man-ager and telephonic monitoring linked to an electronicscale and 1 that implemented a critical pathway for heartfailure with staff education, video teleconferencing, and ahospital-based quality improvement program, were mixed(120, 122). Two RCTs provided team-based home care forfrail elderly patients and thereby maintained function(123, 124). Three RCTs used care managers among seri-ously ill patients at risk for hospitalization. One trial re-duced readmissions among at-risk inpatient discharges; aclinical pathway reduced admissions among residents withpneumonia; and palliative case managers increased advancedirectives and lowered utilization (112, 126, 127).
In summary, moderate evidence supports the ability ofmultidisciplinary interventions that target continuity to af-fect outcomes of utilization in advanced illness. Strong ev-idence derived from many high-quality RCTs shows thatreducing readmissions and other inappropriate utilizationin advanced heart failure is possible, and the evidence ismore consistent among more comprehensive and multidis-
ciplinary approaches. Fewer robust studies addressed otherspecific conditions. Weak evidence addressed cancer(mostly in the palliative care literature), and no direct evi-dence was found for dementia. Successful interventionsused multidisciplinary teams involving nurses and socialservices, ensured continuity across settings, and facilitatedcommunication. Better understanding of how health caresystems can improve continuity in cancer and dementia isneeded. Multiple complex transitions are common in theseand other advanced illnesses (128).
What Aspects of Assessment and Support Are Effectivefor Serving Caregivers, Including Family, When PatientsAre Approaching the End of Life?
Eight systematic reviews (25, 27, 29, 129–133) and19 intervention trials (103, 104, 134–150) addressed care-giver outcomes (Table and Appendix Tables 1 and 3). Anolder review of 4 RCTs found that palliative care improvedcaregiver satisfaction (129). A meta-analysis found no over-all benefit of palliative care teams (effect size, 0.16 [CI,�0.14 to 0.48]) in 13 mostly nonrandomized studies (25).A review of supportive cancer care (22 interventions, 5randomized trials) identified 3 studies reporting improvedcaregiver satisfaction (27). A review of end-of-life careidentified 5 randomized studies evaluating family or care-giver satisfaction with palliative care, with several reportinghigh satisfaction but only 1 demonstrating improvement(29).
A meta-analysis of caregiving for frail elderly patientswith dementia found benefits in 11 intervention studies(effect size, 0.26 [CI, 0.15 to 0.37]) (130). Two partiallyoverlapping and less complete reviews about dementiafound no benefit for caregiver interventions (131, 132).A meta-analysis of 6 dementia outcomes (with 4 to 45randomized, before-and-after studies and 1 to 11 random-ized studies of long-term follow-up, depending on out-come) showed reduced symptoms in the care recipient inthe short term, as well as reduced caregiver burden anddepression, improved caregiver ability and knowledge, andlonger follow-up studies (133). Two reviews found indi-vidual and multicomponent interventions more effectivethan group or single-component strategies (130, 133).
Nineteen additional studies (9 interventions, plus theseveral interventions and 6 sites in the REACH [Resourcesfor Enhancing Alzheimer’s Caregiver Health] project) as-sessed caregiver satisfaction or burden in end-of-life care(103, 104, 136–150). Five interventions focused on can-cer, and 4 focused on palliative care or mixed populations.Interventions included case management, palliative careand advance care planning, care coordination, telephonesupport, and problem-solving interventions for cancer.
The SUPPORT (Study to Understand Prognoses andPreferences for Outcomes and Risks for Treatment) RCTprovided improved information and communication forinpatients with poor prognoses, which improved caregiversatisfaction with communication (136, 137). In a study of
Clinical Guidelines Evidence for Improving Palliative Care at the End of Life
154 15 January 2008 Annals of Internal Medicine Volume 148 • Number 2 www.annals.org

patients with cancer who were randomly assigned to com-prehensive palliative care or telephone palliative care sup-port, patient and caregiver satisfaction with care was highin both groups (135). A cluster-randomized trial of hospi-tal-based palliative consultations for community oncologypatients and providers was associated with improved after-death satisfaction for family members (138, 139). Ran-domized ICU ethics consultations were regarded favorablyby 87% of patients, caregivers, physicians, and nurses (103,104). Satisfaction was high and did not differ amonggroups in an RCT of a nursing home advance directiveprogram (“Let Me Decide” booklet) (149).
The REACH project (available at www.edc.pitt.edu/reach/abstract.html) is a multisite project that uses com-mon measures and procedures to test diverse interventionsfor dementia caregivers. Interventions included variousskills training, emotional and behavioral assistance, in-home support, and enhanced technologies. The effect ofthe 9 interventions on caregiver burden (pooled result fromthe Revised Memory and Behavior Problems Checklist, a0- to 96-point scale that summarizes 24 problem behaviorsand accounts for the caregiver bother associated with each)was small but significant (�1.40; P � 0.022). With re-spect to depression, only 1 REACH site reported improve-ment in the Center for Epidemiologic Studies DepressionScale. The site used family therapy combined with a com-puter support system that facilitated connections to localresources and family conferencing (141, 142, 145–148).
In summary, weak to moderate evidence suggests thatcaregiver interventions, especially when comprehensive andindividually targeted, can relieve burden, although effectsizes are generally small. Moderate evidence suggests thatpalliative care interventions improve satisfaction. Becauseexisting research focuses on dementia, evidence is moderatein dementia and weak in cancer. No evidence addressedcaregivers in heart failure. Addressing these deficits in care-giver research is critical because of the growing role offamily caregivers for an increasing number of persons at theend of life.
DISCUSSION
We identified 33 systematic reviews and 89 reports ofinterventions from approximately 25 000 total citationsrelevant to improving the care of pain, dyspnea, and de-pression; advance care planning; care continuity; and care-giving. Most palliative and end-of-life care research ad-dressed populations with cancer or advanced unspecifiedillness in which cancer is common. Other than the litera-ture on cancer, much of this research focused on patientswith advanced rather than terminal illness. Our evidencebase for improving dyspnea and continuity of care andaddressing caregiving burdens relies (to a large degree) onsuch indirect evidence. Most of the evidence base arisesfrom studies of 1 setting of care, and few reports addressnursing homes.
We found strong evidence for many pharmacologictreatments for cancer pain. Strong evidence supports�-agonists, morphine, pulmonary rehabilitation, and oxy-gen for symptomatic care of COPD, and opioid use isweakly supported for cancer dyspnea. Antidepressants havestrong support for treating depression. Strong evidencesupports the use of multidisciplinary interventions to en-hance continuity and reduce inappropriate utilization.Weak to moderate evidence suggests that multifaceted, in-dividually targeted caregiver programs can relieve burden.
We found weak evidence for the effectiveness of spe-cific palliative service delivery innovations for managingpain and dyspnea, and we found no evidence that theyimprove depression. We found no evidence addressingpain management in advanced noncancer conditions, andinsufficient evidence addressing dyspnea in cancer andheart failure. We identified research priorities about short-acting antidepressants and caregiving challenges in popula-tions other than patients with dementia.
A recent systematic review found symptoms to becommonplace in late life across conditions (151). Becauseour review shows that treatment is effective, assessment andfollow-up of pain, dyspnea, and depression are clinical pri-orities. Palliative care teams may be effective because theyensure symptom screening, treatment, and follow-up.Symptom research priorities include evaluation and man-agement of pain in noncancer conditions, dyspnea in can-cer, depression in late life (for example, short-acting anti-depressants), and symptoms in the cognitively impaired.
Given the lack of patient- and family-centered mea-sures (152), older research has focused on legal, adminis-trative, and utilization outcomes of advance care planning.However, more recent research emphasizes broader inter-ventions—including trained facilitators, involving keydecision makers, and addressing care across settings. Recentliterature has focused on special settings (for example, ICUor nursing home). Research should evaluate advance careplanning in various conditions (for example, outpatientswith advanced heart failure) and across settings.
Palliative care trials that have improved continuity didnot compare various approaches. Heart failure research af-firms the effectiveness of comprehensive interventions thatensure comprehensive support across time and settings.Such research has targeted utilization, with less attention topatient- and family-centered outcomes. Care coordinationand continuity become especially difficult at the end of lifewhen the patient faces complex transitions. For example,25% of Oregonians use 3 or more settings during their last4 weeks of life (128).
Most studies about caregiving focused on dementia,with some on cancer. Individual interventions yieldedlarger treatment effects, yet group interventions predomi-nate in the literature. Multicomponent interventions showmore consistent improvement in caregiver burden, al-though the effect size is generally small. Future research
Clinical GuidelinesEvidence for Improving Palliative Care at the End of Life
www.annals.org 15 January 2008 Annals of Internal Medicine Volume 148 • Number 2 155

should compare alternative strategies and include othercommon patient conditions.
Limitations of our review include that much of theliterature relevant to these domains and the care of patientswith advanced illness does not have a common keyword orindexing term. We dealt with this challenge by conductingdisease-specific supplemental searches, but we may havemissed relevant citations. Our study did not address certaindomains (for example, spiritual support or bereavement) ortechnical interventions (for example, palliative surgery); fu-ture reviews will have to address these topics.
In summary, our systematic review identified interven-tions that could generate substantial improvement in theend-of-life experience. For example, the evidence base forimproving cancer pain makes failing to relieve pain clearlyunjustifiable (2). Although we address important researchgaps, the rapid aging of our population makes implemen-tation of current knowledge crucial in order to assure thehighest possible quality of care throughout the lifespan.
From Veterans Affairs Greater Los Angeles Healthcare System, Los An-geles, California; Southern California Evidence-based Practice Centerand RAND Health, Santa Monica, California; Johns Hopkins Univer-sity, Baltimore, Maryland; Agency for Healthcare Research and Quality,Bethesda, Maryland; City of Hope, Duarte, California; and Center forHealth Research, Kaiser Permanente Northwest, Portland, Oregon.
Disclaimer: The views expressed herein do not represent the views of theU.S. Department of Veterans Affairs, Agency for Healthcare Researchand Quality (AHRQ), or National Institute of Nursing Research.
Grant Support: The National Institute of Nursing Research and theAgency for Healthcare Research and Quality (grant no. 290-02-0003)provided funding for this project. Dr. Lorenz was supported by a Veter-ans Affairs Health Services Research & Development Service Career De-velopment Award, and Dr. Dy was supported by a K07 award from theNational Cancer Institute (K07-CA096 783).
Potential Financial Conflicts of Interest: Grants received: K.A. Lorenz(Amgen).
Requests for Single Reprints: Karl A. Lorenz, MD, MSHS, Division ofGeneral Internal Medicine, Veterans Integrated Palliative Program, Vet-erans Affairs Greater Los Angeles Healthcare System, 11031 WilshireBoulevard, Code 111-G, Los Angeles, CA 90073; e-mail, [email protected].
Current author addresses are available at www.annals.org.
References1. Field MJ, Cassel CK, eds. Approaching Death: Improving Care at the End ofLife. Washington, DC: National Academies Pr; 1997.2. Adams K, Corrigan JM, eds. Priority Areas for National Action: TransformingHealth Care Quality. Washington, DC: National Academies Pr; 2003.3. Hogan C, Lunney J, Gabel J, Lynn J. Medicare beneficiaries’ costs of care inthe last year of life. Health Aff (Millwood). 2001;20:188-95. [PMID:11463076]4. Morrison RS, Maroney-Galin C, Kralovec PD, Meier DE. The growth ofpalliative care programs in United States hospitals. J Palliat Med. 2005;8:1127-34. [PMID: 16351525]5. Teno JM, Weitzen S, Fennell ML, Mor V. Dying trajectory in the last year of
life: does cancer trajectory fit other diseases? J Palliat Med. 2001;4:457-64.[PMID: 11798477]6. Fox E, Landrum-McNiff K, Zhong Z, Dawson NV, Wu AW, Lynn J.Evaluation of prognostic criteria for determining hospice eligibility in patientswith advanced lung, heart, or liver disease. SUPPORT Investigators. Study toUnderstand Prognoses and Preferences for Outcomes and Risks of Treatments.JAMA. 1999;282:1638-45. [PMID: 10553790]7. Knaus WA, Harrell FE Jr, Lynn J, Goldman L, Phillips RS, Connors AF Jr,et al. The SUPPORT prognostic model. Objective estimates of survival for seri-ously ill hospitalized adults. Study to understand prognoses and preferences foroutcomes and risks of treatments. Ann Intern Med. 1995;122:191-203. [PMID:7810938]8. Lunney JR, Lynn J, Foley DJ, Lipson S, Guralnik JM. Patterns of functionaldecline at the end of life. JAMA. 2003;289:2387-92. [PMID: 12746362]9. Patrick DL, Curtis JR, Engelberg RA, Nielsen E, McCown E. Measuring andimproving the quality of dying and death. Ann Intern Med. 2003;139:410-5.[PMID: 12965967]10. The National Consensus Project for Quality Palliative Care. Accessed atwww.nationalconsensusproject.org on 28 February 2006.11. Cook AM, Finlay IG, Edwards AG, Hood K, Higginson IJ, Goodwin DM,et al. Efficiency of searching the grey literature in palliative care. J Pain SymptomManage. 2001;22:797-801. [PMID: 11532593]12. Haggerty JL, Reid RJ, Freeman GK, Starfield BH, Adair CE, McKendry R.Continuity of care: a multidisciplinary review. BMJ. 2003;327:1219-21. [PMID:14630762]13. Atkins D, Best D, Briss PA, Eccles M, Falck-Ytter Y, Flottorp S, et al.;GRADE Working Group. Grading quality of evidence and strength of recom-mendations. BMJ. 2004;328:1490. [PMID: 15205295]14. Lorenz KA, Lynn J, Morton SC, Dy SM, Shugarman LM, Wilkinson A,et al. Methodological approaches for a systematic review of end-of-life care. JPalliat Med. 2005;8 Suppl 1:S4-11. [PMID: 16499467]15. Steinhauser KE, Christakis NA, Clipp EC, McNeilly M, McIntyre L, Tul-sky JA. Factors considered important at the end of life by patients, family, phy-sicians, and other care providers. JAMA. 2000;284:2476-82. [PMID: 11074777]16. Hanson LC, Danis M, Garrett J. What is wrong with end-of-life care?Opinions of bereaved family members. J Am Geriatr Soc. 1997;45:1339-44.[PMID: 9361659]17. Singer PA, Martin DK, Kelner M. Quality end-of-life care: patients’ per-spectives. JAMA. 1999;281:163-8. [PMID: 9917120]18. Wenrich MD, Curtis JR, Ambrozy DA, Carline JD, Shannon SE, RamseyPG. Dying patients’ need for emotional support and personalized care fromphysicians: perspectives of patients with terminal illness, families, and health careproviders. J Pain Symptom Manage. 2003;25:236-46. [PMID: 12614958]19. Teno JM, Clarridge B, Casey V, Edgman-Levitan S, Fowler J. Validation ofToolkit After-Death Bereaved Family Member Interview. J Pain Symptom Man-age. 2001;22:752-8. [PMID: 11532588]20. Teno JM, Clarridge BR, Casey V, Welch LC, Wetle T, Shield R, et al.Family perspectives on end-of-life care at the last place of care. JAMA. 2004;291:88-93. [PMID: 14709580]21. Lorenz K, Lynn J, Morton SC, Dy S, Mularski R, Shugarman L, et al.End-of-Life Care and Outcomes. Evidence Report/Technology Assessment no.110. Rockville, MD: Agency for Healthcare Research and Quality; 2004.22. Weeks JC, Cook EF, O’Day SJ, Peterson LM, Wenger N, Reding D, et al.Relationship between cancer patients’ predictions of prognosis and their treat-ment preferences. JAMA. 1998;279:1709-14. [PMID: 9624023]23. The National Institutes of Health State-of-the-Science Conference Statementon Improving End-of-Life Care. Bethesda, MD: National Institutes of Health;2004. Accessed at http://consensus.nih.gov/2004/2004EndOfLifeCareSOS024htmlhtm on 4 March 2007.24. Thomas K. Caring for the Dying at Home: Companions on the Journey.Abingdon, UK: Radcliffe Medical Pr; 2004.25. Higginson IJ, Finlay IG, Goodwin, DM, Cook AM, Edwards AG, HoodK, et al. The role of palliative care teams: systematic review of their effectivenessand cost-effectiveness. Report to Wales Office of Research and Development ofthe National Assembly of Wales. London: King’s College; 2000.26. Carr D, Goudas L, Lawrence, D, Pirl W, Lau J, DeVine, D, et al. Man-agement of Cancer Symptoms: Pain, Depression, and Fatigue. Summary. Evi-dence Report/Technology Assessment no. 61. Rockville, MD: Agency forHealthcare Research and Quality; 2002. Accessed at www.ahrq.gov/clinic/epcsums/csympsum.htm on 5 July 2007. AHRQ publication no. 02-E031.
Clinical Guidelines Evidence for Improving Palliative Care at the End of Life
156 15 January 2008 Annals of Internal Medicine Volume 148 • Number 2 www.annals.org

27. Gysels M, Higginson IJ. Improving Supportive and Palliative Care for Adultswith Cancer: Research Evidence. London: National Institute for Clinical Excel-lence; 2004. Accessed at www.nice.org.uk/pdf/csgspresearchevidence.pdf on 5July 2007.28. Pan CX, Morrison RS, Ness J, Fugh-Berman A, Leipzig RM. Complemen-tary and alternative medicine in the management of pain, dyspnea, and nauseaand vomiting near the end of life. A systematic review. J Pain Symptom Manage.2000;20:374-87. [PMID: 11068159]29. Wilson DM. Systematic Review of End of Life Care, Health Canada. Edm-onton, Alberta, Canada: Univ of Alberta; 2004.30. Knols R, Aaronson NK, Uebelhart D, Fransen J, Aufdemkampe G. Physicalexercise in cancer patients during and after medical treatment: a systematic reviewof randomized and controlled clinical trials. J Clin Oncol. 2005;23:3830-42.[PMID: 15923576]31. Lee H, Schmidt K, Ernst E. Acupuncture for the relief of cancer-relatedpain—a systematic review. Eur J Pain. 2005;9:437-44. [PMID: 15979024]32. Furlan AD, Sandoval JA, Mailis-Gagnon A, Tunks E. Opioids for chronicnoncancer pain: a meta-analysis of effectiveness and side effects. CMAJ. 2006;174:1589-94. [PMID: 16717269]33. Tremont-Lukats IW, Challapalli V, McNicol ED, Lau J, Carr DB. Systemicadministration of local anesthetics to relieve neuropathic pain: a systematic reviewand meta-analysis. Anesth Analg. 2005;101:1738-49. [PMID: 16301253]34. Jack B, Hillier V, Williams A, Oldham J. Hospital based palliative care teamsimprove the symptoms of cancer patients. Palliat Med. 2003;17:498-502.[PMID: 14526882]35. Latimer EJ, Crabb MR, Roberts JG, Ewen M, Roberts J. The Patient CareTravelling Record in palliative care: effectiveness and efficiency. J Pain SymptomManage. 1998;16:41-51. [PMID: 9707656]36. Mercadante S, Fulfaro F, Casuccio A. A randomised controlled study on theuse of anti-inflammatory drugs in patients with cancer pain on morphine therapy:effects on dose-escalation and a pharmacoeconomic analysis. Eur J Cancer. 2002;38:1358-63. [PMID: 12091067]37. Rabow MW, Dibble SL, Pantilat SZ, McPhee SJ. The comprehensive careteam: a controlled trial of outpatient palliative medicine consultation. Arch InternMed. 2004;164:83-91. [PMID: 14718327]38. Simmons SF, Ferrell BA, Schnelle JF. Effects of a controlled exercise trial onpain in nursing home residents. Clin J Pain. 2002;18:380-5. [PMID: 12441832]39. Soden K, Vincent K, Craske S, Lucas C, Ashley S. A randomized controlledtrial of aromatherapy massage in a hospice setting. Palliat Med. 2004;18:87-92.[PMID: 15046404]40. Wilkinson S, Aldridge J, Salmon I, Cain E, Wilson B. An evaluation ofaromatherapy massage in palliative care. Palliat Med. 1999;13:409-17. [PMID:10659113]41. Grande GE, Todd CJ, Barclay SI, Farquhar MC. A randomized controlledtrial of a hospital at home service for the terminally ill. Palliat Med. 2000;14:375-85. [PMID: 11064784]42. Grande GE, Todd CJ, Barclay SI, Farquhar MC. Does hospital at home forpalliative care facilitate death at home? Randomised controlled trial. BMJ. 1999;319:1472-5. [PMID: 10582932]43. Sittl R, Griessinger N, Likar R. Analgesic efficacy and tolerability of trans-dermal buprenorphine in patients with inadequately controlled chronic pain re-lated to cancer and other disorders: a multicenter, randomized, double-blind,placebo-controlled trial. Clin Ther. 2003;25:150-68. [PMID: 12637117]44. Smith TJ, Staats PS, Deer T, Stearns LJ, Rauck RL, Boortz-Marx RL, etal.; Implantable Drug Delivery Systems Study Group. Randomized clinical trialof an implantable drug delivery system compared with comprehensive medicalmanagement for refractory cancer pain: impact on pain, drug-related toxicity, andsurvival. J Clin Oncol. 2002;20:4040-9. [PMID: 12351602]45. Jordhøy MS, Fayers P, Loge JH, Ahlner-Elmqvist M, Kaasa S. Quality oflife in palliative cancer care: results from a cluster randomized trial. J Clin Oncol.2001;19:3884-94. [PMID: 11559726]46. Sarna L. Effectiveness of structured nursing assessment of symptom distress inadvanced lung cancer. Oncol Nurs Forum. 1998;25:1041-8. [PMID: 9679262]47. Stephenson NL, Weinrich SP, Tavakoli AS. The effects of foot reflexologyon anxiety and pain in patients with breast and lung cancer. Oncol Nurs Forum.2000;27:67-72. [PMID: 10660924]48. Detmar SB, Muller MJ, Schornagel JH, Wever LD, Aaronson NK. Health-related quality-of-life assessments and patient-physician communication: a ran-domized controlled trial. JAMA. 2002;288:3027-34. [PMID: 12479768]49. Bruera E, MacEachern T, Ripamonti C, Hanson J. Subcutaneous morphine
for dyspnea in cancer patients. Ann Intern Med. 1993;119:906-7. [PMID:8215003]50. Bruera E, Palmer JL, Bosnjak S, Rico MA, Moyano J, Sweeney C, et al.Methadone versus morphine as a first-line strong opioid for cancer pain: a ran-domized, double-blind study. J Clin Oncol. 2004;22:185-92. [PMID:14701781]51. McDonald MV, Pezzin LE, Feldman PH, Murtaugh CM, Peng TR. Canjust-in-time, evidence-based “reminders” improve pain management amonghome health care nurses and their patients? J Pain Symptom Manage. 2005;29:474-88. [PMID: 15904750]52. Marinangeli F, Ciccozzi A, Leonardis M, Aloisio L, Mazzei A, Paladini A,et al. Use of strong opioids in advanced cancer pain: a randomized trial. J PainSymptom Manage. 2004;27:409-16. [PMID: 15120769]53. Grosset AB, Roberts MS, Woodson ME, Shi M, Swanton RE, Reder RF,et al. Comparative efficacy of oral extended-release hydromorphone and imme-diate-release hydromorphone in patients with persistent moderate to severe pain:two randomized controlled trials. J Pain Symptom Manage. 2005;29:584-94.[PMID: 15963867]54. Mercadante S, Villari P, Ferrera P, Casuccio A. Addition of a second opioidmay improve opioid response in cancer pain: preliminary data. Support CareCancer. 2004;12:762-6. [PMID: 15206014]55. Rodrigues P, Hering F, Campagnari JC. Use of bisphosphonates can dra-matically improve pain in advanced hormone-refractory prostate cancer patients.Prostate Cancer Prostatic Dis. 2004;7:350-4. [PMID: 15534620]56. Benıtez-Rosario MA, Feria M, Salinas-Martın A, Martınez-Castillo LP,Martın-Ortega JJ. Opioid switching from transdermal fentanyl to oral metha-done in patients with cancer pain. Cancer. 2004;101:2866-73. [PMID:15529307]57. Mazzocato C, Buclin T, Rapin CH. The effects of morphine on dyspnea andventilatory function in elderly patients with advanced cancer: a randomized dou-ble-blind controlled trial. Ann Oncol. 1999;10:1511-4. [PMID: 10643545]58. Martell BA, O’Connor PG, Kerns RD, Becker WC, Morales KH, KostenTR, et al. Systematic review: opioid treatment for chronic back pain: prevalence,efficacy, and association with addiction. Ann Intern Med. 2007;146:116-27.[PMID: 17227935]59. Levenson JW, McCarthy EP, Lynn J, Davis RB, Phillips RS. The last sixmonths of life for patients with congestive heart failure. J Am Geriatr Soc. 2000;48:S101-9. [PMID: 10809463]60. Lynn J, Ely EW, Zhong Z, McNiff KL, Dawson NV, Connors A, et al.Living and dying with chronic obstructive pulmonary disease. J Am Geriatr Soc.2000;48:S91-100. [PMID: 10809462]61. Jennings AL, Davies AN, Higgins JP, Gibbs JS, Broadley KE. A systematicreview of the use of opioids in the management of dyspnoea. Thorax. 2002;57:939-44. [PMID: 12403875]62. Salman GF, Mosier MC, Beasley BW, Calkins DR. Rehabilitation forpatients with chronic obstructive pulmonary disease: meta-analysis of randomizedcontrolled trials. J Gen Intern Med. 2003;18:213-21. [PMID: 12648254]63. Booth S, Wade R, Johnson M, Kite S, Swannick M, Anderson H; ExpertWorking Group of the Scientific Committee of the Association of PalliativeMedicine. The use of oxygen in the palliation of breathlessness. A report of theexpert working group of the Scientific Committee of the Association of PalliativeMedicine. Respir Med. 2004;98:66-77. [PMID: 14959816]64. Ram FS, Jardin JR, Atallah A, Castro AA, Mazzini R, Goldstein R, et al.Efficacy of theophylline in people with stable chronic obstructive pulmonarydisease: a systematic review and meta-analysis. Respir Med. 2005;99:135-44.[PMID: 15715180]65. Shukla VK, Chen S, Boucher M, Mensinkai S, Dales R. Long-acting B2-agonists for the maintenance treatment of chronic obstructive pulmonary diseasein patients with reversible and non-reversible airflow obstruction: a systematicreview of clinical effectiveness. Technology report no. 65. Ottawa, Ontario, Can-ada: Canadian Coordinating Office for Health Technology Assessment; 2006.66. Bruera E, Sweeney C, Willey J, Palmer JL, Strasser F, Morice RC, et al. Arandomized controlled trial of supplemental oxygen versus air in cancer patientswith dyspnea. Palliat Med. 2003;17:659-63. [PMID: 14694916]67. Weiner P, Waizman J, Magadle R, Berar-Yanay N, Pelled B. The effect ofspecific inspiratory muscle training on the sensation of dyspnea and exercise tol-erance in patients with congestive heart failure. Clin Cardiol. 1999;22:727-32.[PMID: 10554688]68. Abernethy AP, Currow DC, Frith P, Fazekas BS, McHugh A, Bui C.Randomised, double blind, placebo controlled crossover trial of sustained release
Clinical GuidelinesEvidence for Improving Palliative Care at the End of Life
www.annals.org 15 January 2008 Annals of Internal Medicine Volume 148 • Number 2 157

morphine for the management of refractory dyspnoea. BMJ. 2003;327:523-8.[PMID: 12958109]69. Lewith GT, Prescott P, Davis CL. Can a standardized acupuncture tech-nique palliate disabling breathlessness: a single-blind, placebo-controlled crossoverstudy. Chest. 2004;125:1783-90. [PMID: 15136391]70. Gottlieb SS, Fisher ML, Freudenberger R, Robinson S, Zietowski G, AlvesL, et al. Effects of exercise training on peak performance and quality of life incongestive heart failure patients. J Card Fail. 1999;5:188-94. [PMID: 10496191]71. Roffe L, Schmidt K, Ernst E. A systematic review of guided imagery as anadjuvant cancer therapy. Psychooncology. 2005;14:607-17. [PMID: 15651053]72. Sultzer DL, Gray KF, Gunay I, Wheatley MV, Mahler ME. Does behav-ioral improvement with haloperidol or trazodone treatment depend on psychosisor mood symptoms in patients with dementia? J Am Geriatr Soc. 2001;49:1294-300. [PMID: 11890487]73. Wilcock A, Manderson C, Weller R, Walker G, Carr D, Carey AM, et al.Does aromatherapy massage benefit patients with cancer attending a specialistpalliative care day centre? Palliat Med. 2004;18:287-90. [PMID: 15198118]74. Chochinov HM, Hack T, Hassard T, Kristjanson LJ, McClement S, Har-los M. Dignity therapy: a novel psychotherapeutic intervention for patients nearthe end of life. J Clin Oncol. 2005;23:5520-5. [PMID: 16110012]75. Walsh RA, Girgis A, Sanson-Fisher RW. Breaking bad news. 2: Whatevidence is available to guide clinicians? Behav Med. 1998;24:61-72. [PMID:9695897]76. Hanson LC, Tulsky JA, Danis M. Can clinical interventions change care atthe end of life? Ann Intern Med. 1997;126:381-8. [PMID: 9054283]77. Baggs JG. End-of-life care for older adults in ICUs. Annu Rev Nurs Res.2002;20:181-229. [PMID: 12092510]78. Song MK. Effects of end-of-life discussions on patients’ affective outcomes.Nurs Outlook. 2004;52:118-25. [PMID: 15197360]79. Guo B, Harstall C. Advance Directives for End-of-Life Care in the Elderly—Effectiveness of Delivery Modes. Edmonton, Alberta, Canada: Alberta HeritageFoundation for Medical Research; 2004.80. Gomes B, Higginson IJ. Factors influencing death at home in terminally illpatients with cancer: systematic review. BMJ. 2006;332:515-21. [PMID:16467346]81. Shalowitz DI, Garrett-Mayer E, Wendler D. The accuracy of surrogatedecision makers: a systematic review. Arch Intern Med. 2006;166:493-7. [PMID:16534034]82. Anderson JP, Kaplan RM, Schneiderman LJ. Effects of offering advancedirectives on quality adjusted life expectancy and psychological well-being amongill adults. J Clin Epidemiol. 1994;47:761-72. [PMID: 7722589]83. Brumley RD, Enguidanos S, Cherin DA. Effectiveness of a home-basedpalliative care program for end-of-life. J Palliat Med. 2003;6:715-24. [PMID:14622451]84. Campbell ML, Guzman JA. Impact of a proactive approach to improveend-of-life care in a medical ICU. Chest. 2003;123:266-71. [PMID: 12527629]85. Campbell ML, Guzman JA. A proactive approach to improve end-of-life carein a medical intensive care unit for patients with terminal dementia. Crit CareMed. 2004;32:1839-43. [PMID: 15343010]86. Casarett D, Karlawish J, Morales K, Crowley R, Mirsch T, Asch DA.Improving the use of hospice services in nursing homes: a randomized controlledtrial. JAMA. 2005;294:211-7. [PMID: 16014595]87. Coppola KM, Ditto PH, Danks JH, Smucker WD. Accuracy of primarycare and hospital-based physicians’ predictions of elderly outpatients’ treatmentpreferences with and without advance directives. Arch Intern Med. 2001;161:431-40. [PMID: 11176769]88. Gillick M, Berkman S, Cullen L. A patient-centered approach to advancemedical planning in the nursing home. J Am Geriatr Soc. 1999;47:227-30.[PMID: 9988295]89. Heffner JE, Fahy B, Hilling L, Barbieri C. Outcomes of advance directiveeducation of pulmonary rehabilitation patients. Am J Respir Crit Care Med.1997;155:1055-9. [PMID: 9116986]90. Holzapfel L, Demingeon G, Piralla B, Biot L, Nallet B. A four-step protocolfor limitation of treatment in terminal care. An observational study in 475 inten-sive care unit patients. Intensive Care Med. 2002;28:1309-15. [PMID:12209282]91. Lilly CM, Sonna LA, Haley KJ, Massaro AF. Intensive communication:four-year follow-up from a clinical practice study. Crit Care Med. 2003;31:S394-9. [PMID: 12771590]92. Monteleoni C, Clark E. Using rapid-cycle quality improvement methodol-
ogy to reduce feeding tubes in patients with advanced dementia: before and afterstudy. BMJ. 2004;329:491-4. [PMID: 15331474]93. Morrison RS, Chichin E, Carter J, Burack O, Lantz M, Meier DE. Theeffect of a social work intervention to enhance advance care planning documen-tation in the nursing home. J Am Geriatr Soc. 2005;53:290-4. [PMID:15673354]94. Pearlman RA, Starks H, Cain KC, Cole WG. Improvements in advance careplanning in the Veterans Affairs System: results of a multifaceted intervention.Arch Intern Med. 2005;165:667-74. [PMID: 15795344]95. Perry E, Swartz J, Brown S, Smith D, Kelly G, Swartz R. Peer mentoring:a culturally sensitive approach to end-of-life planning for long-term dialysis pa-tients. Am J Kidney Dis. 2005;46:111-9. [PMID: 15983964]96. Ratner E, Norlander L, McSteen K. Death at home following a targetedadvance-care planning process at home: the kitchen table discussion. J Am GeriatrSoc. 2001;49:778-81. [PMID: 11454117]97. Schwartz CE, Wheeler HB, Hammes B, Basque N, Edmunds J, Reed G,et al.; UMass End-of-Life Working Group. Early intervention in planning end-of-life care with ambulatory geriatric patients: results of a pilot trial. Arch InternMed. 2002;162:1611-8. [PMID: 12123405]98. Song MK, Kirchhoff KT, Douglas J, Ward S, Hammes B. A randomized,controlled trial to improve advance care planning among patients undergoingcardiac surgery. Med Care. 2005;43:1049-53. [PMID: 16166875]99. Soskis CW. End-of-life decisions in the home care setting. Soc Work HealthCare. 1997;25:107-16. [PMID: 9313307]100. Stuart B, D’Onofrio CN, Boatman S, Feigelman G. CHOICES: promot-ing early access to end-of-life care through home-based transition management. JPalliat Med. 2003;6:671-83. [PMID: 14516514]101. Tolle SW, Tilden VP, Nelson CA, Dunn PM. A prospective study of theefficacy of the physician order form for life-sustaining treatment. J Am GeriatrSoc. 1998;46:1097-102. [PMID: 9736102]102. Weisbord SD, Carmody SS, Bruns FJ, Rotondi AJ, Cohen LM, ZeidelML, et al. Symptom burden, quality of life, advance care planning and thepotential value of palliative care in severely ill haemodialysis patients. NephrolDial Transplant. 2003;18:1345-52. [PMID: 12808172]103. Schneiderman LJ, Gilmer T, Teetzel HD, Dugan DO, Blustein J, Cran-ford R, et al. Effect of ethics consultations on nonbeneficial life-sustaining treat-ments in the intensive care setting: a randomized controlled trial. JAMA. 2003;290:1166-72. [PMID: 12952998]104. Schneiderman LJ, Gilmer T, Teetzel HD. Impact of ethics consultations inthe intensive care setting: a randomized, controlled trial. Crit Care Med. 2000;28:3920-4. [PMID: 11153636]105. Hanson LC, Reynolds KS, Henderson M, Pickard CG. A quality improve-ment intervention to increase palliative care in nursing homes. J Palliat Med.2005;8:576-84. [PMID: 15992199]106. Karel MJ, Powell J, Cantor MD. Using a values discussion guide to facil-itate communication in advance care planning. Patient Educ Couns. 2004;55:22-31. [PMID: 15476986]107. Gutheil IA, Heyman JC. Communication between older people and theirhealth care agents: results of an intervention. Health Soc Work. 2005;30:107-16.[PMID: 15974371]108. Treece PD, Engelberg RA, Crowley L, Chan JD, Rubenfeld GD, Stein-berg KP, et al. Evaluation of a standardized order form for the withdrawal of lifesupport in the intensive care unit. Crit Care Med. 2004;32:1141-8. [PMID:15190964]109. Bookbinder M, Blank AE, Arney E, Wollner D, Lesage P, McHugh M,et al. Improving end-of-life care: development and pilot-test of a clinical pathway.J Pain Symptom Manage. 2005;29:529-43. [PMID: 15963861]110. Bailey FA, Burgio KL, Woodby LL, Williams BR, Redden DT, KovacSH, et al. Improving processes of hospital care during the last hours of life. ArchIntern Med. 2005;165:1722-7. [PMID: 16087819]111. Heffner JE, Barbieri C. Effects of advance care education in cardiovascularrehabilitation programs: a prospective randomized study. J Cardiopulm Rehabil.2001;21:387-91. [PMID: 11767814]112. Engelhardt JB, McClive-Reed KP, Toseland RW, Smith TL, Larson DG,Tobin DR. Effects of a program for coordinated care of advanced illness onpatients, surrogates, and healthcare costs: a randomized trial. Am J Manag Care.2006;12:93-100. [PMID: 16464138]113. Taylor SJ, Candy B, Bryar RM, Ramsay J, Vrijhoef HJ, Esmond G, et al.Effectiveness of innovations in nurse led chronic disease management for patientswith chronic obstructive pulmonary disease: systematic review of evidence. BMJ.
Clinical Guidelines Evidence for Improving Palliative Care at the End of Life
158 15 January 2008 Annals of Internal Medicine Volume 148 • Number 2 www.annals.org

2005;331:485. [PMID: 16093253]114. Ram FS, Wedzicha JA, Wright J, Greenstone M. Hospital at home forpatients with acute exacerbations of chronic obstructive pulmonary disease: sys-tematic review of evidence. BMJ. 2004;329:315. [PMID: 15242868]115. Smeenk FW, van Haastregt JC, de Witte LP, Crebolder HF. Effectivenessof home care programmes for patients with incurable cancer on their quality oflife and time spent in hospital: systematic review. BMJ. 1998;316:1939-44.[PMID: 9641929]116. McAlister FA, Stewart S, Ferrua S, McMurray JJ. Multidisciplinary strat-egies for the management of heart failure patients at high risk for admission: asystematic review of randomized trials. J Am Coll Cardiol. 2004;44:810-9.[PMID: 15312864]117. Phillips CO, Wright SM, Kern DE, Singa RM, Shepperd S, Rubin HR.Comprehensive discharge planning with postdischarge support for older patientswith congestive heart failure: a meta-analysis. JAMA. 2004;291:1358-67.[PMID: 15026403]118. Windham BG, Bennett RG, Gottlieb S. Care management interventionsfor older patients with congestive heart failure. Am J Manag Care. 2003;9:447-59; quiz 460-1. [PMID: 12816174]119. Ahrens T, Yancey V, Kollef M. Improving family communications at theend of life: implications for length of stay in the intensive care unit and resourceuse. Am J Crit Care. 2003;12:317-23; discussion 324. [PMID: 12882061]120. Goldberg LR, Piette JD, Walsh MN, Frank TA, Jaski BE, Smith AL,et al.; WHARF Investigators. Randomized trial of a daily electronic home mon-itoring system in patients with advanced heart failure: the Weight Monitoring inHeart Failure (WHARF) trial. Am Heart J. 2003;146:705-12. [PMID:14564327]121. Gorski LA, Johnson K. A disease management program for heart failure:collaboration between a home care agency and a care management organization.Lippincotts Case Manag. 2003;8:265-73. [PMID: 14646784]122. Philbin EF, Rocco TA, Lindenmuth NW, Ulrich K, McCall M, JenkinsPL. The results of a randomized trial of a quality improvement intervention inthe care of patients with heart failure. The MISCHF Study Investigators. Am JMed. 2000;109:443-9. [PMID: 11042232]123. Mann WC, Ottenbacher KJ, Fraas L, Tomita M, Granger CV. Effective-ness of assistive technology and environmental interventions in maintaining in-dependence and reducing home care costs for the frail elderly. A randomizedcontrolled trial. Arch Fam Med. 1999;8:210-7. [PMID: 10333815]124. Melin AL, Bygren LO. Efficacy of the rehabilitation of elderly primaryhealth care patients after short-stay hospital treatment. Med Care. 1992;30:1004-15. [PMID: 1331632]125. Goodyer LI, Miskelly F, Milligan P. Does encouraging good complianceimprove patients’ clinical condition in heart failure? Br J Clin Pract. 1995;49:173-6. [PMID: 7547154]126. Loeb M, Carusone SC, Goeree R, Walter SD, Brazil K, Krueger P, et al.Effect of a clinical pathway to reduce hospitalizations in nursing home residentswith pneumonia: a randomized controlled trial. JAMA. 2006;295:2503-10.[PMID: 16757722]127. Coleman EA, Parry C, Chalmers S, Min SJ. The care transitions interven-tion: results of a randomized controlled trial. Arch Intern Med.2006;166:1822-8. [PMID: 17000937]128. Tolle SW, Tilden VP, Rosenfeld AG, Hickman SE. Family reports ofbarriers to optimal care of the dying. Nurs Res. 2000;49:310-7. [PMID:11093695]129. Wilkinson EK, Salisbury C, Bosanquet N, Franks PJ, Kite S, LorentzonM, et al. Patient and carer preference for, and satisfaction with, specialist modelsof palliative care: a systematic literature review. Palliat Med. 1999;13:197-216.[PMID: 10474707]130. Yin T, Zhou Q, Bashford C. Burden on family members: caring for frailelderly: a meta-analysis of interventions. Nurs Res. 2002;51:199-208. [PMID:12063419]131. Acton GJ, Winter MA. Interventions for family members caring for anelder with dementia. Annu Rev Nurs Res. 2002;20:149-79. [PMID: 12092509]132. Acton GJ, Kang J. Interventions to reduce the burden of caregiving for anadult with dementia: a meta-analysis. Res Nurs Health. 2001;24:349-60. [PMID:11746065]133. Sorensen S, Pinquart M, Duberstein P. How effective are interventions
with caregivers? An updated meta-analysis. Gerontologist. 2002;42:356-72.[PMID: 12040138]134. Hughes SL, Weaver FM, Giobbie-Hurder A, Manheim L, Henderson W,Kubal JD, et al.; Department of Veterans Affairs Cooperative Study Group onHome-Based Primary Care. Effectiveness of team-managed home-based primarycare: a randomized multicenter trial. JAMA. 2000;284:2877-85. [PMID:11147984]135. Hanks GW, Robbins M, Sharp D, Forbes K, Done K, Peters TJ, et al.The imPaCT study: a randomised controlled trial to evaluate a hospital palliativecare team. Br J Cancer. 2002;87:733-9. [PMID: 12232756]136. Baker R, Wu AW, Teno JM, Kreling B, Damiano AM, Rubin HR, et al.Family satisfaction with end-of-life care in seriously ill hospitalized adults. J AmGeriatr Soc. 2000;48:S61-9. [PMID: 10809458]137. A controlled trial to improve care for seriously ill hospitalized patients. Thestudy to understand prognoses and preferences for outcomes and risks of treat-ments (SUPPORT). The SUPPORT Principal Investigators. JAMA. 1995;274:1591-8. [PMID: 7474243]138. Ringdal GI, Jordhøy MS, Kaasa S. Family satisfaction with end-of-life carefor cancer patients in a cluster randomized trial. J Pain Symptom Manage. 2002;24:53-63. [PMID: 12183095]139. Ringdal GI, Ringdal K, Jordhøy MS, Ahlner-Elmqvist M, Jannert M,Kaasa S. Health-related quality of life (HRQOL) in family members of cancervictims: results from a longitudinal intervention study in Norway and Sweden.Palliat Med. 2004;18:108-20. [PMID: 15046407]140. Walsh SM, Schmidt LA. Telephone support for caregivers of patients withcancer. Cancer Nurs. 2003;26:448-53. [PMID: 15022976]141. Gitlin LN, Winter L, Corcoran M, Dennis MP, Schinfeld S, Hauck WW.Effects of the home environmental skill-building program on the caregiver-carerecipient dyad: 6-month outcomes from the Philadelphia REACH Initiative.Gerontologist. 2003;43:532-46. [PMID: 12937332]142. Gitlin LN, Belle SH, Burgio LD, Czaja SJ, Mahoney D, Gallagher-Thompson D, et al.; REACH Investigators. Effect of multicomponent interven-tions on caregiver burden and depression: the REACH multisite initiative at6-month follow-up. Psychol Aging. 2003;18:361-74. [PMID: 14518800]143. Smeenk FW, de Witte LP, van Haastregt JC, Schipper RM, BiezemansHP, Crebolder HF. Transmural care of terminal cancer patients: effects on thequality of life of direct caregivers. Nurs Res. 1998;47:129-36. [PMID: 9610646]144. Bucher JA, Loscalzo M, Zabora J, Houts PS, Hooker C, BrintzenhofeSzocK. Problem-solving cancer care education for patients and caregivers. CancerPract. 2001;9:66-70. [PMID: 11879281]145. Burgio L, Stevens A, Guy D, Roth DL, Haley WE. Impact of two psy-chosocial interventions on white and African American family caregivers of indi-viduals with dementia. Gerontologist. 2003;43:568-79. [PMID: 12937335]146. Burns R, Nichols LO, Martindale-Adams J, Graney MJ, Lummus A.Primary care interventions for dementia caregivers: 2-year outcomes from theREACH study. Gerontologist. 2003;43:547-55. [PMID: 12937333]147. Eisdorfer C, Czaja SJ, Loewenstein DA, Rubert MP, Arguelles S, MitraniVB, et al. The effect of a family therapy and technology-based intervention oncaregiver depression. Gerontologist. 2003;43:521-31. [PMID: 12937331]148. Mahoney DF, Tarlow BJ, Jones RN. Effects of an automated telephonesupport system on caregiver burden and anxiety: findings from the REACH forTLC intervention study. Gerontologist. 2003;43:556-67. [PMID: 12937334]149. Molloy DW, Guyatt GH, Russo R, Goeree R, O’Brien BJ, Bedard M,et al. Systematic implementation of an advance directive program in nursinghomes: a randomized controlled trial. JAMA. 2000;283:1437-44. [PMID:10732933]150. Cameron JI, Shin JL, Williams D, Stewart DE. A brief problem-solvingintervention for family caregivers to individuals with advanced cancer. J Psycho-som Res. 2004;57:137-43. [PMID: 15465067]151. Solano JP, Gomes B, Higginson IJ. A comparison of symptom prevalencein far advanced cancer, AIDS, heart disease, chronic obstructive pulmonary dis-ease and renal disease. J Pain Symptom Manage. 2006;31:58-69. [PMID:16442483]152. Mularski RA, Dy SM, Shugarman LR, Wilkinson AM, Lynn J, ShekellePG, et al. A systematic review of measures of end-of-life care and its outcomes.Health Serv Res. 2007;42:1848-70. [PMID: 17850523]
Clinical GuidelinesEvidence for Improving Palliative Care at the End of Life
www.annals.org 15 January 2008 Annals of Internal Medicine Volume 148 • Number 2 159

Current Author Addresses: Drs. Lorenz and Shekelle: Veterans AffairsGreater Los Angeles Healthcare System, 11301 Wilshire Boulevard,Code 111-G, Los Angeles, CA 90073.Dr. Lynn: Center for Medicare & Medicaid Services, Office of Standardsand Quality, 7500 Security Boulevard, Mail Stop S3-02-01, Baltimore,MD 21244-1850.Dr. Dy: Johns Hopkins Bloomberg School of Public Health, Room 609,624 North Broadway, Baltimore, MD 21205.Drs. Shugarman and Maglione, Ms. Hilton, Ms. Rhodes, Ms. Rolon,and Ms. Sun: RAND Corporation, 1776 Main Street, Santa Monica,CA 90401-3208.
Dr. Wilkinson: Western Australia Center for Cancer and Palliative Care,Edith Cowan University, Building 19, Churchlands Campus, PearsonStreet, Churchlands, WA 6018, Australia.Dr. Mularski: Center for Health Research, Kaiser Permanente North-west, 3800 North Interstate, WIN 1060, Portland, OR 97227.Dr. Morton: Research Triangle Institute, 3040 Cornwallis Road, POBox 12194, Research Triangle Park, NC 27709-2194.Dr. Hughes: Agency for Healthcare Research and Quality, John M.Eisenberg Building, 540 Gaither Road, Rockville, MD 20850.
Annals of Internal Medicine
www.annals.org 15 January 2008 Annals of Internal Medicine Volume 148 • Number 2 W-27

Appendix Figure. Trajectories of late-life illness.
Func
tion
Short Period of Evident Decline
Mostly cancer
Time
Death
Low
High
Func
tion
Long-Term Limitations with Intermittent Serious Episodes
Mostly heart and lung failure
Time
Time
Death
Low
High
Death
Func
tion
Prolonged Dwindling
Mostly frailty and dementia
Low
High
W-28 15 January 2008 Annals of Internal Medicine Volume 148 • Number 2 www.annals.org

For personal use. Only reproduce with permission from The Lancet Publishing Group.
THE LANCET Oncology Vol 4 May 2003 http://oncology.thelancet.com312
Opioids and sedative drugs are commonly used to controlsymptoms in patients with advanced cancer. However, it isoften assumed that the use of these drugs inevitably resultsin shortening of life. Ethically, this outcome is excused byreference to the doctrine of double effect. In this review, weassess the evidence for patterns of use of opioids andsedatives in palliative care and examine whether thedoctrine of double effect is needed to justify their use. Weconclude that patients are more likely to receive higherdoses of both opioids and sedatives as they get closer todeath. However, there is no evidence that initiation oftreatment, or increases in dose of opioids or sedatives, isassociated with precipitation of death. Thus, we concludethat the doctrine of double effect is not essential forjustification of the use of these drugs, and may act as adeterrent to the provision of good symptom control.
Lancet Oncol 2003; 4: 312–18
There is a widespread consensus that physicians have anethical obligation to relieve patients with advanced cancer ofpain and other distressing symptoms.1 However, opioids andsedatives—two vital classes of drugs for symptom control atthe end of life—have become tainted with the implicationthat they hasten death.
High profile court cases involving the legal or illegal use ofmorphine attract much attention.2,3 Billings and Block,described the use of a morphine drip (figure 1) as “sloweuthanasia”.4 And, in a statement about physician-assistedsuicide, the US Supreme Court described this treatment aspain relief that advances death. Wall believes these viewsperpetuate myths surrounding the use of morphine, despitethe fact that claims about its addictive potential and safetyhave now been successfully challenged. He concludes that “wemust help patients to be absolutely clear that their treatmentfor pain is just that, it is not an alternative route to an earlygrave”.5
Despite the progress that has been made in palliativemedicine with regards to symptom control, there are stillpatients who have symptoms that prove intractable, eitherbecause treatment is ineffective or the treatment itself isintolerable. The response in these circumstances is to usesedative medication to reduce the patient’s awareness of theirsymptoms and hence relieve distress. In addition to physicalsymptoms, mental syndromes such as agitated delirium,severe anxiety, and fear are also present near the end of life. Invery ill patients, delirium may prove to be untreatable, andthe patients’s energy and ability to concentrate may beinsufficient to cope with talking through their concerns. Inthis situation, sedation is also the therapeutic response.
The use of sedation at the end of life has attractedsuspicion in the same way that the use of opioids has done.
The practice has been dubbed slow euthanasia or terminalsedation;4 both these terms suggest that patients’ lives areshortened by treatment. Such use of opioids and sedatives canbe defended ethically on the basis of the doctrine of doubleeffect.6 The doctrine of double effect applies to a medicaltreatment if the following conditions are met:
� the treatment is potentially beneficial but may also haveharmful effects
� the clinician intends the beneficial effect but not theharmful effect, although the harmful effect may beforeseen
� the harmful effect is not necessary in order to achieve thebeneficial effect
� the symptoms are severe enough to constitute acompelling reason to expose the patient to the risk of aharmful outcome.However, critics of this argument say that it is too difficult
to know a person’s true intentions.7 The potential danger ofconceding to these criticisms is that effective symptomcontrol is withheld from dying patients for fear of accusationsof malpractice.
Personal view Opioids and sedatives
NS is the Head of Medicine and a Consultant in Palliative Medicineat St Christopher’s Hospice and a Honorary Senior Lecturer atKing’s College, London, UK. AT is a Consultant and Senior Lecturerin Palliative Medicine at Pilgrims Hospices, Margate, UK
Correspondence: Professor Nigel Sykes, St Christopher’s Hospice,Lawrie Park Road, London, SE26 6DZ, UK. Tel: +44 (0)208 768 4550. Fax: +44 (0)208 659 5051. Email: [email protected]
The use of opioids and sedatives at the end of life
Nigel Sykes and Andrew Thorns
Figure 1. Opioids and sedatives can be given in increasing doses at theend of life.

For personal use. Only reproduce with permission from The Lancet Publishing Group.
THE LANCET Oncology Vol 4 May 2003 http://oncology.thelancet.com 313
We aim to review current practices of opioid andsedative use, focusing particularly on evidence that life isshortened through use of these drugs.
OpioidsWe identified 17 studies which examined the use of opioidsat the end of life,8–24 and analysed them for patterns ofopioid use, types of opioid used, mean doses, and effect ofopioid use on survival.
The use of opioids in palliative care Opioids are commonly used in palliative care for thetreatment of pain,25 dyspnoea,26 and cough (figure 2).Higher doses of opioids are required in some clinicalsituations such as neuropathic pain, advancing disease,metabolic variation, and in younger patients.27 Such factorsmay explain some interindividual variation in theeffectiveness of opioids, but the use of adjuvant analgesicsand attention to non-physical factors, which may beexacerbating pain, need to be considered alongside doseescalation.
Inappropriate increases in opioid doses will probablyresult in myoclonus, hallucinations, and delirium. Althoughrespiratory depression is the most feared and often quotedside-effect of strong opioids, it occurs late because toleranceto the effects on respiration develops with chronic use.28
Fohr concluded that when opioids are used appropriatelyfor pain relief, the risk of respiratory depression is moremyth than fact.29 However, the risk remains real whenopioids are used inappropriately. Tolerance to the analgesiceffect of opioids does not seem to be a significant problem.27
Opinion is divided over the issue of increasing opioiddoses as symptoms increase and death approaches, becausestudying such circumstances is difficult. Those studieswhich have been published showed great variation inreported responses; probably due to differences indefinitions, patient groups, and timing of assessments. Painat the end of life is reported to occurr in up to 51% ofpatients, and dyspnoea is present in up to 38%. There issome evidence that pain becomes less over the last fewweeks of life, but dyspnoea is known to worsen.16,30
Opioid use at the end of lifeFrequency The reported frequency of opioid use in the last few days oflife varies from 25% to 99%.14,18 Generally, patients receivingcommunity palliative care seem to be given less opioids.Goldberg and colleagues reported that 66% of patientsbeing cared for at home received opioids compared with78% of hospice patients.19 Patients receiving conventionalcare (ie, care without specialist palliation) received lessopioids than either of the other two groups, possiblyconfirming the presence of anxieties among generalphysicians about their use. Mercadante reported aminimum use of opioids of 25% in his community group.18
He suggests that this low percentage is due to a wideselection of patients in contrast to studies in specialistpalliative-care units that treat more complex cases.McCormack, by contrast, found that 89% of patients
received opioids in his community group.20 This figure issimilar to other in-patient studies that showed 70–90% ofpatients received opioids.
Changes in doseStudies of dose alterations show great variation in themethods used. Different time periods have been analysed anddifferent percentage changes considered significant. Fourstudies showed an increase in the proportion of patientsreceiving opioids as death approached (table 1). Goldberg andcolleagues reported only minor changes in the proportion ofpatients receiving opioids near death, but in conventional-care patients the proportion dropped from 68% to 57%.19
Five studies reported that the mean dose also increasedover the last few weeks or days of life (table 2). Morita andcolleagues9 and Fainsinger and colleagues15 found a decrease inopioid dose during the last few days of life after an initialincrease. Furthermore, eight studies reported that somepatients required a marked increase in the last 24–48 hours oflife.9,11,12,14,16,17,21,22 The percentage of these patients variedconsiderably from occasional individuals21 to 32% (20% ofwhich received less than 25 mg of parenteral morphine perday)22 and 40%.17
Doses of opioids usedMean doses of opioid used at the time of death vary widelybetween studies: 52–659 mg14,21 with a weighted average of 192 mg. Patients in the USA and Canada reportedly receivehigher doses than elsewhere. These differences have beensuggested to be because of different rates of use of adjuvant
Personal viewOpioids and sedatives
Figure 2. Opioids are derived from opium poppies (P somniferum).
Table 1. Patients receiving strong opioids at study entryand before death
Patients receiving opioids Patients receiving opioids Refat start of study (%) before death (%)
42 87 9
61 89 12
69 66 1976 78
68 57
68 85 20

For personal use. Only reproduce with permission from The Lancet Publishing Group.
THE LANCET Oncology Vol 4 May 2003 http://oncology.thelancet.com314
analgesics, variations in psychological care, and differences inthe type of opioids used.31 In two studies by Fainsinger andcolleagues, there is a marked difference in mean opioiddose.14,15 This variation may be because of an increasedrotation between different opioids and the use of methadonesuppositories.
Types of opioids Morphine is by far the commonest strong opioid used instudies that report on the frequency of opioid use (table 3).
Effect on survivalFive studies have looked at the effect of opioid use on survival,although they used different methods.8,9,10,12,32 None of thestudies reported that opioids had shortened life. However, thisaspect does not seem to have been as frequently examinedwith opioids as it has been with sedatives.
Bercovitch and colleagues found no difference insurvival between patients receiving high doses and thosereceiving low doses.8 Furthermore, there were no cases ofrespiratory depression. Morita and colleagues found nosignificant difference in the survival of patients receivingdifferent doses of opioids.10 However, the studies comparingmean doses of opioids may be misleading because the rate ofchange of dose has been suggested to be a more importantfactor.28 We reported, however, that there was no significantdifference in the rate of increase in dose in relation tosurvival.12 In the same study, we also analysed thedistribution of large increases in opioid dose during the lastweek of life. We found that such increases were no morelikely to occur in the last 48 hours of life than earlier in thestudy period. Regnard and Badger compared patients whowere given a double dose of opioid at night with those whoreceived a single dose; they reported that those in the double
dose group were no more likely to die at night.32 Respiratorydepression seems to be an issue of concern only inexperimental situations.33
Guidelines for opioid use at the end of lifeGuidelines on the use of opioids in palliative care advocatethe careful titration of opioid according to the patient’s pain.They also offer reassurance that the appropriate use ofmorphine should not shorten life and that there is no reasonto withhold opioids in the last few days.34,35
The evidence we report in this review supports theseguidelines. Although studies generally report a gradualincrease in opioid dose up until the end of life, there is noapparent shortening of life when higher doses are used or, asreported by our study, when the rate of administration ofopioids is increased. Cases in which opioid doses given topatients increase substantially are rare even in specialistpalliative-care units where more difficult pain problems mayoccur. Clinicians who are treating patients that need largeincreases in opioid dose should be encouraged to seekspecialist help, particularly if the dose increases are greaterthan 100% per day or the clinician feels they risk shortening apatient’s life. This message is reinforced in the UK’s RoyalCollege of Physicians guidance information that remindsdoctors of the professional obligation to seek advice when thelimits of their skills have been reached.
SedationWe identified 17 studies (including 2 yet to be published by Morita and colleagues, and Scholes and colleagues,respectively) that addressed the use of sedatives in the care ofcancer patients in the final stages of life.10,14,22,36–47 In addition,we included a systematic review that analysed three studiespublished in Spanish.48
Definitions of sedationIn a survey of palliative physicians, Chater and colleaguesdefined sedation as “deliberately inducing and maintainingdeep sleep for the relief of intractable physical or mentalsymptoms”, but specified that their definition did notinclude the management of delirium.49 Only 40% ofrespondents agreed with this definition and there wereseveral alternative views. There is evidence that heavysedation is more likely to be used by physicians who are lessconfident in psychological care and have higher levels ofprofessional burnout.50
Personal view Opioids and sedatives
Table 2. Change in mean opioid dose in parenteralmorphine equivalents from study entry to death
Mean opioid dose Mean opioid dose before Refon entry to study (mg) death (mg)
49 139 9
42 55 12
125 460 13
493 659 14
184 180 15
45 75 24
Table 3. Percentage of patients given strong opioids at the end of life
Morphine Buprenorphine Tramadol Hydromorphone Methadone Diamorphine Other Ref
100 .. .. .. .. .. .. 8
77 20 .. .. .. .. .. 10
62 8 11 .. .. .. 10 11
59 .. .. 39 5 11 .. 14
57 .. .. 38 6 2 4 15
36 .. .. 22 11 .. 2 (oxycodone) 16
19 .. .. 14 8 .. 9 19
44 .. .. 9 1 .. .. 20
100 .. .. .. .. .. .. 24

For personal use. Only reproduce with permission from The Lancet Publishing Group.
THE LANCET Oncology Vol 4 May 2003 http://oncology.thelancet.com 315
Clearly, many, perhaps most, palliative physicians do notaim to induce deep sleep by use of sedative drugs in very illpatients, other than in a situation where the patientexperiences a catastrophic event, which is likely to cause animminent, distressing death.51 Instead, the sedative dose istitrated against the distress response, just as opioid doses aretitrated against a pain response. Sedation should be classedas adequate if distress is relieved and the patient remainsconscious. Sales described this approach as “proportional”,distinguishing it from the act of deliberately inducing deepsleep which he termed “sudden”.48 We have used these termsin the analysis of the studies in table 4. However, in somecases it is unclear which approach was used and we do notagree with Sales about the interpretation of some of thestudies. Also, few studies provide a definition of sedation,and the depth of sedation has either not been measured(many investigations are retrospective) or assessed in anobjective way to allow a comparison with other reports.
Definitions of symptomsPain, dyspnoea, and vomiting are fairly unequivocalsymptoms, but some studies use different terms, and othersymptoms can be harder to characterise. Existential or familialdistress is a fairly common reason for sedation in somecountries, notably Spain, but apparently entirely absent inothers.45 How much does this category overlap with what
another group has labelled mental anguish?39 Is theclassification the same as the restlessness reported by McIverand colleagues,37 or the same as what most others studiesdefine as delirium?
Some of these differences may be cultural, with identicalbehaviours given different interpretations in differentcountries. However, it has been suggested that some of thedifferences in perceived levels of existential distress may begenuine, and may be a reflection of the limited disclosure ofinformation about cancer, which is common in somecountries. The result of this practice may be a level ofpsychological distress that grows as the patient realises theseriousness of his or her condition through physicaldeterioration.45 Although there is general agreement about themost common indications for use of sedatives at the end oflife, such differences need to be explored further.
Patterns of sedative useTable 4 shows the frequency and length of sedative use invarious studies and table 5 describes the types of drug andindications for sedation. The prevalence of sedation varieswidely, from 1% to 88% among the populations analysed.This variation is partly due to differences in definitions ofsedation. Studies reporting a proportional use of sedationshow a mean use of 45%, whereas the small number ofstudies using so-called “sudden” sedation report a mean use
Personal viewOpioids and sedatives
Table 4. Characteristics of sedation used
Type of study n Type of care Mode of sedation Frequency of Length of sedative Survival Refsedation (%) use (days) (days)
Retrospective 209 Palliative-care unit Proportional 60 ·· Overlapping Kaplan-Meier 10curves
Retrospective 100 Palliative-care unit Proportional 16 ·· ·· 14
Prospective 50 Palliative-care unit Proportional 88 ·· ·· 22and hospital
Prospective 154 Home care Proportional 52 2* 25* (sedated) 3623* (non-sedated) (p=ns)
Prospective 20 Hospital Proportional 25 2·5 ·· 37
Retrospective 143 Palliative-care unit Proportional 48 3·9 ·· 38
Retrospective 115 Palliative-care unit Proportional 26 1·3 18·6 (sedated) 39and hospital 19·1 (non-sedated) (p=ns)
Retrospective 278 Palliative-care unit Sudden 1 1·5 ·· 40
Retrospective 76 Palliative-care unit Proportional 30 2·5 ·· 41
Prospective 157 Palliative-care unit Proportional 45 3 ·· 42
Prospective 401 Home and hospital ·· 7–60 ·· ·· 43Multicentre
Prospective Palliative-care unit Sudden 4–10 2·6 ·· 44Muticentre 150 and hospital
Prospective 387 Palliative-care unit Sudden 15–36 1·9–3·2 ·· 45Multicentre
Prospective 251 Palliative-care unit Proportional 28 5* 28·5 (sedated) 4624·7 (non-sedated) (p=ns)
Retrospective 237 Palliative-care unit Proportional 48 ·· 38·6 (sedated) 4714·2 (non-sedated) (p<0·001)
Retrospective 284 Palliative-care unit Proportional 22 2·5* (midazolam only) ·· †
Prospective 40 Palliative-care unit Proportional .. 2·8 (levomepromazine) ·· ‡1·0 (midazolam)
*Median; †Morita et al, unpublished data; ‡Scholes et al, unpublished data; ns, not significant.

For personal use. Only reproduce with permission from The Lancet Publishing Group.
THE LANCET Oncology Vol 4 May 2003 http://oncology.thelancet.com316
of 16%. It is fair to expect that sedation tounconsciousness is a less common procedurethan more moderate sedation.
Another influence on studies of sedation isthe type and geographical location of the unitswhere the studies were done. Units that havemore complex and challenging palliative-careproblems seem to use sedation more freelythan those that are less specialised. Thissituation was the case in Canada where thespecialist palliative-care unit had a sedationrate of 10% compared with 4% reported inother units.44 Similarly, in a UK hospice, 31%of patients experienced some degree ofsedation compared with only 21% of patientsin hospital.39 However, Peruselli and co-workers analysed data from at least 58different centres across Italy and reportedlarge differences in sedation frequency.43 Theseresults are likely to reflect differences in thedefinition of sedation by different doctors,rather than actual use of sedative drugs.Because of the variability inherent in this studyit is impossible to classify the mode of sedativeuse (table 4).
Fainsinger and colleagues found thatsedation was used more than twice as often ina Spanish palliative-care unit than in acomparable Israeli centres, with two SouthAfrican centres having values inbetween.45 Thisfinding raises the possibility that the triggersfor sedation are culturally determined.However, none of the uses of sedativesreported in this international multicentrestudy fell outside the range of values reportedfrom studies in English-speaking countries.
There is a general agreement across thestudies that a syndrome of delirium andagitation in an extremely ill patient withcancer is the most common indication forsedative use, with a weighted mean of 65%(table 5). After this, breathlessness is the nextmost frequent reason (weighted mean 26%).Pain, perhaps surprisingly, is a much lesscommon reason for sedation (weighted mean 14%).
The drugs used in this patient group varybetween countries, but midazolam was the mostcommon, used in 8 of the 13 studies thatreported medications, and was the second mostused sedative in three other studies.Psychotropic drugs are used frequently,sometimes in conjunction with benzo-diazepines. However, they are the mostfavoured drug category in only three reports—two citing haloperidol and the otherchlorpromazine. Given the inefficiency ofopioids as sedatives it is surprising to find theirinclusion—in one case at the top of the list—in
Personal view Opioids and sedatives
Table 5. Types of sedative used and the indications for sedation
Type of sedative Percentage Reason for Percentage of Refof patients sedation patients withtreated symptoms
Haloperidol 43 .. .. 10Midazolam 23 .. ..Hydroxyzine 15 .. ..
.. Delirium 63 14
.. Pain 37
Midazolam .. .. .. 22Clonazepam .. .. ..Lorazepam .. .. ..Diazepam .. .. ..
Diazepam .. Dyspnoea 41 36Chlorpromazine .. Pain 39Haloperido .. Delirium 14
.. Vomiting 6
Chlorpromazine 100 Dyspnoea 55 37.. Restlessness 45
Midazolam 55 Dyspnoea 49 38Morphine 55 Pain 39Haloperidol 33 Malaise 38Diazepam 15 Agitation 23Scopolamine 13 Nausea 10
Midazolam 80 Delirium 60 39Haloperidol 37 Mental anguish 27Levomepromazine 33 Pain 20Phenobarbitone 3 Dyspnoea 20
Midazolam 100 Delirium 100 40
Midazolam 91 Delirium 96 41Chlorpromazine 9 Dyspnoea 4Lorazepam 9 .. ..
Opioids 37 Delirium/ restlessness 42 42Midazolam 31 Dyspnoea 41Haloperidol 31 Pain 13Diazepam 13 Vomiting 1Scopolamine 10 Psychological distress 1
Midazolam 50 Delirium 91 44
Levomepromazine 30 Dyspnoea 9Lorazepam 10 .. ..Diazepam 10 .. ..
Midazolam 71 Delirium 61 45Haloperidol 9 Dyspnoea 26Lorazepam 8 Pain 7Phenobarbitone 3 Existential distress 7Levomepromazine 1
Haloperidol 50 Delirium 57 46Midazolam 24 Dyspnoea 23Morphine 13 Pain 10
Insomnia 7
Midazolam 82 .. .. 47Levomepromazine 22 .. ..Haloperidol 2 .. ..Phenobarbitone .. .. ..
Midazolam 100 Delirium 63 †.. Dyspnoea 44.. Pain 13.. Insomnia 13.. Myoclonus 5
Levomepromazine 50 Agitation 100 ‡Midazolam 50
† Morita et al, unpublished data; ‡ Scholes et al, unpublished data.

For personal use. Only reproduce with permission from The Lancet Publishing Group.
THE LANCET Oncology Vol 4 May 2003 http://oncology.thelancet.com 317
two studies from the Southeast Asia.38,46 Barbiturates andpropofol are reported as sedative drugs to be used as a lastresort.
Effect of sedation on survivalThe most important ethical question is whether the use ofsedatives shortens the life of terminally ill patients. A definitiveanswer to this question could only be obtained from arandomised controlled trial in which patients were randomlyallocated to sedation or non-sedation groups. But thissolution is ethically impossible.
Ten studies have estimated the average duration for whichsedation was used (table 4). The weighted mean durationfrom these studies is 2·8 days, a figure that could either implythat sedative use results in death within 72 hours, or thatsedation is used to control symptoms that occur as deathapproaches. To distinguish between these possibilities, fivestudies have reported the use of sedation in relation to survivalfrom admission to death for in-patient centres or fromcommencement of service involvement to death fordomiciliary-based teams (table 4). In each case survival ofpatients receiving sedation was not significantly different fromthat of patients who were not given sedatives, and in one casethere was a difference in favour of sedation.47 Patients whoreceived sedatives for over a week before death had bettersurvival than those who did not receive sedation; patients whohad only 2 or 3 days of sedatives had the same survival as thosewho never received sedation. This finding may be explainedby the role of delirium in initiating breakdown of care athome and consequent admission to a specialist palliative-careunit. Delirious patients would have been admitted at an earlierstage of their illness than those who did not experience thissyndrome before being close to death.
ConclusionSedatives are used commonly in patients with cancer at theend of life. In most cases they are not given with the intentionof inducing sleep. Instead, the dose is titrated against the reliefof a specific symptom, most often an agitated delirium, to thepoint where the symptom is adequately relieved. Theimpairment of consciousness is not an objective but anaccompaniment to the use of the medication, and varies in itsextent.
Sedation is generally used over a short period and most ofthe evidence suggests that in the context of specialist palliativecare it is not associated with shortening of life. Generally,sedative use is a response to symptoms that are part of the
dying process, and for the same reason are untreatable byother means. Thus, concerns about hydration and feedingthat have been raised are not generally relevant.52,53
Guidance Cherny and Portenoy have produced guidelines for the use ofsedatives for symptom control.1 Sedation should be usedappropriately for specified symptoms once therapeuticalternatives have been considered and found ineffective orinapplicable to the present situation. As agents of symptomcontrol, not of life shortening, sedative drugs should be givenin doses that are titrated against the response to balance reliefof symptoms with the distress they cause.
Benzodiazepines are the most favoured class of sedativesin palliative care worldwide. In particular, midazolam can beadministrated by continuous subcutaneous infusion, and hasanticonvulsant and muscle relaxant as well as anxiolyticproperties.54 The psychotropic drugs haloperidol, levo-mepromazine, and chlorpromazine may be more appropriatefor the specific management of delirium, but they can lowerthe fit threshold and may precipitate myoclonus in severely illpatients.55 Psychotropics can be used in combination withbenzodiazepines. Phenobarbitone and propofol have beenreported on a case-series basis to be of use in severe agitationwhich is unresponsive to other sedatives.56,57
The doctrine of double effectThe doctrine of double effect is used as an ethical justificationfor the specific risk of foreseeable life shortening as a result ofa medical treatment. However, we suggest that there is noevidence that the use of opioids or sedatives in palliative carerequires the doctrine of double effect as a defence. We havespecifically examined the role of this doctrine in relation tosymptom control and found that in 238 patients in a specialistpalliative-care unit (89% receiving strong opioids and 48%receiving sedation) there was no evidence that that thedoctrine needed to be invoked in relation to any morphinetherapy.12 In fact, the doctrine was only possibly relevant totwo patients who were treated with sedatives.47 In each case thecondition of the patient had already been noted to bedeteriorating and they were very disturbed.
Thus, although the doctrine is a valid ethical device, it is,for the most part, irrelevant to symptom control at the end oflife. To exaggerate its involvement perpetuates a myth thatsatisfactory symptom control at the end of life is inevitablyassociated with hastening death. The result can be a reluctanceto use medication to secure comfort and a failure to provideadequate relief to a very vulnerable group of patients.29
Conflict of interestNone declared.
References1 Cherny NI, Portenoy RK. Sedation in the management of refractory
symptoms: guidelines for evaluation and treatment. J Palliat Care1994; 10: 31–38.
2 Dyer C. Dr David Moor cleared of murder after giving a patient adose of diamorphine: British GP cleared of murder charge. Br Med J1999; 318: 1306.
3 Horton R. The real lessons from Harold Frederick Shipman. Lancet2001; 357: 82–83
4 Billings JA, Block SD. Slow euthanasia. J Palliat Care 1996; 12: 21–30.
Personal viewOpioids and sedatives
Search strategy and selection criteriaSearches of Medline, Embase, CancerLit, CINAHL, andCochrane databases were done with the search terms“palliative care”, “hospice”, “cancer”, “opioids”, “sedatives”,“euthanasia”, “ethics”, and “double effect”. Manual searchesof reference lists of articles were also done. The Halley StewartLibrary at St Christopher’s Hospice was also searched. Paperswere limited to detailed retrospective or prospective studies ofthe use of opioids or sedatives or both in the palliative care ofcancer patients. Only papers published in English wereselected.

For personal use. Only reproduce with permission from The Lancet Publishing Group.
THE LANCET Oncology Vol 4 May 2003 http://oncology.thelancet.com318
5 Wall PD. The generation of yet another myth on the use of narcotics.Pain 1997; 73: 121–22.
6 Latimer EJ. Ethical decision-making in the care of the dying and itsapplications to clinical practice. J Pain Symptom Manage 1991; 6:329–36.
7 Quill TE. The ambiguity of clinical intentions. New Eng J Med 1993;329: 1039–40.
8 Bercovitch M, Waller A, Adunsky A. High dose morphine use in thehospice setting: a database survey of patient characteristics and effecton life expectancy. Cance, 1999; 86: 871–77
9 Morita T, Ichiki T, Tsunoda J, et al. A prospective study on the dyingprocess in terminally ill cancer patients. Am J Hosp Palliat Care 1998;15: 217–22.
10 Morita T, Tsunoda J, Inoue S, Chihara S. Effects of high dose opioidsand sedatives on survival in terminally ill cancer patients. J PainSymptom Manage 2001: 21: 282–89.
11 Grond S, Zech D, Schug SA, et al Validation of World HealthOrganisation guidelines for cancer pain relief during the last days andhours of life. J Pain Symptom Manage 1991; 6: 411–22.
12 Thorns A, Sykes N. Opioid use in the last week of life andimplications for end of life decision-making. Lancet 2000; 356:398–99.
13 Brescia FJ, Portenoy RK, Ryan M, et al. Pain, opioid use and survivalin hospitalised patients with advanced cancer. J Clin Oncol 1992; 10:149–55.
14 Fainsinger R, Miller MJ, Bruera E. Symptom control during the lastweek of life on a palliative care unit. J Palliat Care 1991; 7: 5–11.
15. Fainsinger RL, Louie K, Belzie M, Bruera E. Decreased opioid dosesused in a palliative care unit. J Palliat Care 1996; 12: 6–9.
16 Coyle N, Adelhardt J, Foley KM, Portenoy RK. Character of terminalillness in the advanced cancer patient: pain and other symptomsduring the last four weeks of life. J Pain Symptom Manage 1990; 5:83–93.
17 Lichter I, Hunt E. The last 48 hours of life. J Palliat Care 1990; 6:7–15.
18 Mercadante S. Pain treatment and outcomes for patients withadvanced cancer who received follow up care at home. Cancer 1999;85: 18–58.
19 Goldberg RJ, Mor V, Wiemann M, et al. Analgesic use in terminalcancer patients: report from the national hospice study. J Chronic Dis1986; 39: 37–45.
20 McCormack A, Hunter-Smith D, Piotrowski ZH, et al. Analgesic usein home hospice patients. J Fam Pract 1992; 34: 160–164.
21 Boyd KJ. Short terminal admissions to a hospice. Palliat Med 1993; 7:289–94.
22 Turner K, Chye R, Aggarwal G, et al. Dignity in dying: a preliminarystudy of patients in the last three days of life. J Palliat Care 1996; 12:7–13.
23 Mercadante S, Dardanoni G, Salvaggio L, et al. Monitoring of opioidtherapy in advanced cancer pain patients. J Pain Symptom Manage1997; 13: 204–12.
24 Zech DFJ, Grond S, Lynch J, et al. Validation of World HeathOrganisation guidelines for cancer pain relief: a 10 year prospectivestudy. Pain 1995; 63: 65–76.
25 Ventafridda V, Tamburini M, Caraceni A, et al. A validation study ofthe WHO method for cancer pain relief. Cancer 1987; 59: 850–56.
26 Jennings AL, Davies AN, Higgins JPT, Broadley K. Opioids for thepalliation of breathlessness in terminal illness (Cochrane review). In:The Cochrane Library, Issue 4, 2001.
27 Mercadante S, Portenoy R. Opioid poorly responsive cancer pain. J Pain Symptom Manage 2001; 21: 144–50.
28 Walsh TD. Opiates and respiratory function in advanced cancer.Recent Results Cancer Res 1984; 89: 115–17.
29 Fohr SA. The double effect of pain medication: separating myth fromreality. J Palliat Med 1998: 1: 315–28.
30 Higginson I, McCarthy M. Measuring symptoms in terminal cancer:are pain and dyspnoea controlled? J R Soc Med, 1989; 82: 264–67.
31 Boisvert M, Cohen SR. Opioid use in advanced malignant disease:why do different centres use vastly different doses? A plea forstandardised reporting. J Pain Symptom Manage 1995: 10: 632–38.
32 Regnard C, Badger C. Opioids, sleep and the time of death. PalliatMed 1987; 1: 107–10.
33 Citron ML, Johnston-Early A, Fossieck BE, et al. Safety and efficacy ofcontinuous intravenous morphine for severe cancer pain. Am J Med1984; 77: 199–204.
34 World Health Organisation. Cancer Pain Relief. Geneva: WorldHealth Organisation, 1986.
35 Hanks GWF, de Conno F, et al. Morphine and alternative opioids incancer pain: the EAPC recommendations. Br J Cancer 2001; 84:587–93.
36 Ventafridda V, Ripamonti C, de Conno F, et al. Symptom prevalenceand control during cancer patients’ last days of life. J Palliat Care1990; 6: 7–11.
37 McIver B, Walsh D, Nelson K. The use of chlorpromazine forsymptom control in dying cancer patients. J Pain Symptom Manage1994; 9: 341–45.
38 Morita T, Inoue S, Chihara S. Sedation for symptom control in Japan:the importance of intermittent use and communication with familymembers. J Pain Symptom Manage 1996; 12: 32-–38.
39 Stone P, Phillips C, Spruyt O, Waight C. A comparison of the use ofsedative in a hospital support team and in a hospice. Palliat Med1997; 11: 140–44.
40 Fainsinger RL. Use of sedation by a hospital palliative care supportteam. J Pall Care 1998; 14: 51–54.
41 Fainsinger RL, Landman W, Hoskings M, Bruera E. Sedation foruncontrolled symptoms in a South African hospice. J Pain SymptomManage 1998; 16: 145–52.
42 Morita T, Tsunoda J, Inoue S, Chihara S. Do hospice clinicians sedate patients intending to hasten death? J Palliat Care 1999; 15:20–23.
43 Peruselli C, Di Giulio P, Toscani F, et al. Home palliative care forterminal cancer patients: a survey on the final week of life. Palliat Med1999; 13: 233–41.
44 Fainsinger RL, de Moissac D, Mancini I, Oneschuk D. Sedation fordelirium and other symptoms in terminally ill patients in Edmonton.J Palliat Care 2000; 16: 5–10.
45 Fainsinger R, Waller A, Bercovici M, et al. A multicentre internationalstudy of sedation for uncontrolled symptoms in terminally illpatients. Palliat Med 2000; 14: 257–65.
46 Chiu TY, Hu W-Y, Lue B-H, et al. Sedation for refractory symptomsof terminal cancer patients in Taiwan. J Pain Symptom Manage 2001;21: 467–72.
47 Sykes NP, Thorns A. Sedative use in the last week of life and theimplications for end of life decision-making. Arch Int Med 2003; 163:341–44.
48 Sales JP. Sedation and terminal care. Eur J Palliat Care 2001; 8:97–100.
49 Chater S, Viola R, Paterson J, Jarvis V. Sedation for intractabledistress in the dying: a survey of experts. Palliat Med 1998; 12:255–69.
50 Morita T, Akechi T, Sugawara Y, et al. Practices and attitudes ofJapanese oncologists and palliative care physicians concerningterminal sedation: a nationwide survey. J Clin Oncol 2002; 20: 758–64.
51 Stone P, Phillips C, Khullar M. Sedation in catastrophic incidents.Palliat Med 1997; 11: 253–54.
52 Craig GM. On withholding nutrition and hydration in the terminallyill: has palliative medicine gone too far? J Med Ethics 1994; 20:139–43.
53 Dunlop RJ, Ellershaw JE, Baines MJ, Sykes NP. On withholdingnutrition and hydration in the terminally ill: has palliative medicinegone too far? A reply. J Med Ethics 1995; 21: 141–43.
54 McNamara P, Minton M, Twycross RG. The use of midazolam inpalliative care. Palliat Med 1991; 5: 244–49.
55 Twycross RG, Lichter I. The terminal phase. In: Doyle D, Hanks G,MacDonald N (Eds). The Oxford Textbook of Palliative Medicine (2ndedition). Oxford: University Press, 1998; 976–92.
56 Truog RD, Berde CB, Mitchell C, Greir HE. Barbiturates in the careof the terminally ill. New Eng J Med 1992; 327: 1678–82.
57 Moyle J. The use of propofol in palliative medicine. J Pain SymptomManage 1995; 10: 643–46.
Personal view Opioids and sedatives