Patophysiology of blood and lymph circulation in lower extremities Assoc. prof. Jana Plevkova MD,...
64
Patophysiology of blood and lymph Patophysiology of blood and lymph circulation in lower extremities circulation in lower extremities Assoc. prof. Assoc. prof. Jana Plevkova MD, PhD Jana Plevkova MD, PhD 20 20 12 12 Department of Pathophysiology Department of Pathophysiology Jessenius Faculty of Medicine in Martin Jessenius Faculty of Medicine in Martin
-
Upload
leonard-pitts -
Category
Documents
-
view
218 -
download
1
Transcript of Patophysiology of blood and lymph circulation in lower extremities Assoc. prof. Jana Plevkova MD,...

Patophysiology of blood and lymph Patophysiology of blood and lymph circulation in lower extremities circulation in lower extremities
Assoc. prof. Assoc. prof. Jana Plevkova MD, PhD Jana Plevkova MD, PhD 20 201212
Department of Pathophysiology Department of Pathophysiology Jessenius Faculty of Medicine in MartinJessenius Faculty of Medicine in Martin

Blood circulation is sophisticated system which Blood circulation is sophisticated system which conduct the blood from the heart and lungs into conduct the blood from the heart and lungs into
the tissuesthe tissues- it's main function is to provide suitable - it's main function is to provide suitable metabolic supply to the cells /oxygen, metabolic supply to the cells /oxygen,
substrates/, aw well as the cleavage of metabolic substrates/, aw well as the cleavage of metabolic products from the tissueproducts from the tissue
vessels – resistance, capacity, capillary vessels – resistance, capacity, capillary network, other specific vascular structures network, other specific vascular structures
high pressure / low pressure part of circulationhigh pressure / low pressure part of circulation regional specific circulations regional specific circulations

Arterial system of lower extremitiesArterial system of lower extremities
source :http://education.yahoo.com/reference/gray/subjects/subject/157

Principles of blood flowPrinciples of blood flow
science discipline analyzing the flow of the science discipline analyzing the flow of the blood within the circulation blood within the circulation
P. .r4
8..l Q – blood flowP – pressure gradient between two different points of the tube /vessel/r – vessel diameterl – vessel length - blood viscosity
Q

Arterial system of lower extremitiesArterial system of lower extremities
-a part of high pressure circulation -a part of high pressure circulation
Energy of the heart ejection /systolic effort/ continues into Energy of the heart ejection /systolic effort/ continues into 1)1) frontal pressure, responsible for the forward movement frontal pressure, responsible for the forward movement
of the blood within the vessel of the blood within the vessel 2)2) lateral pressure affecting the wall of the artery causing lateral pressure affecting the wall of the artery causing
it's distension, giving the base for the pulse wave it's distension, giving the base for the pulse wave laminar flowlaminar flow (flow within individual layers smoothly gliding (flow within individual layers smoothly gliding
one on another one on another ))- This mutual gliding is responsible for the tangential - This mutual gliding is responsible for the tangential
tension among the layers and most external layer and tension among the layers and most external layer and endothelium, as well endothelium, as well (shear stress)(shear stress)

shear stressshear stress – – this mechanism is able to influence some this mechanism is able to influence some of the regulatory and secretory functions of the of the regulatory and secretory functions of the endothelium endothelium
Turbulent flow Turbulent flow within the blood stream could be within the blood stream could be physiological only at the sites of wide vessels physiological only at the sites of wide vessels
- aortal arc, pulmonary artery, site of the vessel aortal arc, pulmonary artery, site of the vessel branching, sudden bending of the vessel branching, sudden bending of the vessel
Predisposition for turbulent blood flowPredisposition for turbulent blood flow
-- wide vessel wide vessel -- sudden change of the diametersudden change of the diameter- high blood flow velocity - high blood flow velocity - - low blood viscositylow blood viscosity -- uneven endothelial surfaceuneven endothelial surface

The blood flow in the arteries has three phases, due to The blood flow in the arteries has three phases, due to elastic properties of the veselastic properties of the vesssel wall el wall
1st phase – forward movement of the blood caused 1st phase – forward movement of the blood caused by ventricular contraction – systolic ejection. by ventricular contraction – systolic ejection. Vessel wall is distended during this phase, because Vessel wall is distended during this phase, because of lateral pressure applied onto the vessel wall of lateral pressure applied onto the vessel wall
2nd phase is characterized by return of the distended 2nd phase is characterized by return of the distended vessel diameter into the former size – elastic recoil vessel diameter into the former size – elastic recoil the flow is directed to the beds with low resistancethe flow is directed to the beds with low resistance
3rd phase of the diastolic period – the flow is directed 3rd phase of the diastolic period – the flow is directed forward againforward again

Regulation of the blood flow in lower extremitiesRegulation of the blood flow in lower extremities Relative constant pressure gradient – diving pressure is Relative constant pressure gradient – diving pressure is
constant, so regulation is secured predominantly by the constant, so regulation is secured predominantly by the change of vessel resistance – change of vessel diameter change of vessel resistance – change of vessel diameter
1.1. myogenic (Bayliss regulation)myogenic (Bayliss regulation)2.2. metabolic (autoregulation)metabolic (autoregulation) lactic acid, lactic acid, COCO22, H, H++, K, K++, adenosin , adenosin
3.3. other humoral factors other humoral factors (catecholamine, histamine, (catecholamine, histamine, acetylcholine, angiotensin)acetylcholine, angiotensin)
4.4. nerve regulationnerve regulation - - sympathetic fibers sympathetic fibers

Endothelium – is not only a mechanical barrier
It has high metabolic activity, participates in vessel reactivity, regulation of thrombogenesis, influences the functions of circulating cells
Endothelial surface – 500 - 1000 m2 – contact surface for the mediation of „signals“ between circulating cells and intimal surface
It seems to be the largest endocrine organ /1500g/
Metabolic and secretoric systems influence mainly vessel tone therefore resistance and blood flow
Physiological tendency to vasodilatation

Endothelial vasodilators
production of NO – from L arginine by NO synthasis – enzymatic process, new molecule of NO is released into the smooth muscle cells layer beneath the endothelium – activation of guanylatcyclase - production of cGMP leads to relaxation of muscle cells and thus to vasodilatation
production of NO is responsible for permanent „natural“ tendency to vasodilatation in arterial system
production of NO is stimulated by – shear stress, platelets derived molecules like (ATP, ADP, serotonin), vessel distention – flow dependent dilatation
NO is dominant vasodilator in basal conditions endothelium produce also other vasoactive substances like -
PGI2 (prostacyclin) PGE2, PGD2

Endothelial vasoconstrictors
endothelins, tromboxan A2, nonstable endoperoxides, and molecules of local RAA system
Endothelins (1, 2, 3) – group of peptides containing 21 AA, derived from molecule of proendothelin, which is fragmented to active molecules
ETA a ETB receptors – vasoconstricting response, long lasting effects involve proliferative effects on smooth muscle cells within the vessel wall

Endothelial dysfunction
Functional changes of the endothelial cells
predominance for production of vasoconstricting mediators
increased production of cytokines increased permeability for plasmatic proteins and
lipoproteins predominance of procoagulating processes increased production of CAM molecules

Pathogenesis of diseases of arterial system of lower Pathogenesis of diseases of arterial system of lower extremitiesextremities
Diseases with different ethiology may have the same, Diseases with different ethiology may have the same, or very similar signs and symptomsor very similar signs and symptoms
- So it is not correct to talk about „arterial occlusion“ So it is not correct to talk about „arterial occlusion“ onlyonly
Ischemia of lower extremitiesIschemia of lower extremities- acuteacute – sudden onset of ischemic attac /dangerous, – sudden onset of ischemic attac /dangerous,
bc of the risk of the lost of the extremity/bc of the risk of the lost of the extremity/- chronicchronic – long lasting ischemization, trophic – long lasting ischemization, trophic
changes...changes...
- Degenerative processes - atherosclerosis /ATS/- Degenerative processes - atherosclerosis /ATS/- Aneurysmal arterial disease- Aneurysmal arterial disease- Inflammation and thrombosis - Inflammation and thrombosis - Vasospastic disease- Vasospastic disease

Atherosclerosis obliterans Atherosclerosis obliterans Risk factorsRisk factors
fatty and cholesterol containing diet fatty and cholesterol containing diet
less fruits/vegetable/fibless fruits/vegetable/fiberer diet diet
hypercholesterolaemiahypercholesterolaemia
smokingsmoking
hypertensionhypertension
low concetration of HDLlow concetration of HDL
+ family history for CVS diseases+ family history for CVS diseases
obesityobesity
increased fibrinogene levelincreased fibrinogene level
male sexmale sex

(Atherosclerosis obliterans - ASO)(Atherosclerosis obliterans - ASO)
ppatogenesis of ATS – response of the vessel wall to atogenesis of ATS – response of the vessel wall to injuryinjury
1.1. functional changes of endothelial cells functional changes of endothelial cells
2.2. deposition of lipid particles into the vessel wall with deposition of lipid particles into the vessel wall with subsequent reaction – creation of fibromuscular plaquesubsequent reaction – creation of fibromuscular plaque
3.3. chemotactic activity of monocytes – fagocythosis of lipid chemotactic activity of monocytes – fagocythosis of lipid particles of macrophages (foam cells) particles of macrophages (foam cells) lipid plaque lipid plaque
Formation of ATS plaques of different size and position in Formation of ATS plaques of different size and position in the arterial systthe arterial systeem of lower extremitiesm of lower extremities

ConsequencesConsequences
turbulent flowturbulent flow at the site of the plaque location at the site of the plaque location
presence of the plaque may lead to presence of the plaque may lead to „serious“ stenosis limiting the „serious“ stenosis limiting the
blood flow blood flow
damage of the vessel wall due to plaque may lead to weakening of damage of the vessel wall due to plaque may lead to weakening of
media and formation of aneurysmamedia and formation of aneurysma
bleeding into the plaque with possibility for formation of bleeding into the plaque with possibility for formation of false false
aneurysmaaneurysma
dysrupture of the plaque with subsequent thrombosis of the artery dysrupture of the plaque with subsequent thrombosis of the artery
abruption of the plaque and embolization of those fragments into abruption of the plaque and embolization of those fragments into
more peripheral circulation more peripheral circulation
acute or chronic ischemiacute or chronic ischemizzation of extremityation of extremity

Arterial aneurysmsArterial aneurysms
http://www.daviddarling.info/encyclopedia/A/aneurysm.html
http://images.rheumatology.org/viewphoto.php?imageId=2861575&albumId=75674

Arterial aneArterial aneuurysms – rysms – llocalized dilatation of the vessel wallocalized dilatation of the vessel wall
1)1) True aneurysms True aneurysms – c– coonsist of all three layers of arterial wall, nsist of all three layers of arterial wall, usually has fusiform or circumferential shape, the underlying usually has fusiform or circumferential shape, the underlying condition for such a dilatation is weakening of the vessel condition for such a dilatation is weakening of the vessel wall due to some pathological process – mainly ATS wall due to some pathological process – mainly ATS
The damage of the vessel wall with weakening of media could be The damage of the vessel wall with weakening of media could be
acquiredacquired (atherosclerosis, inflammation, toxic ifl.) or (atherosclerosis, inflammation, toxic ifl.) or inheritedinherited (syndroms with weak connective tissue like s (syndroms with weak connective tissue like syy. . Marfan)Marfan)
2)2) FFalse aneurysms alse aneurysms – – extra vascular accumulation of blood with disruption, two or all three vascular layers the wall of the aneurysms is formed by thrombus and adjacent tissues, or adventitia
False aneurysms is usually consequence of trauma, or , or complication of ATS plaquecomplication of ATS plaque

http://medical-dictionary.thefreedictionary.com/false+aneurysm

Whatever the cause, the aneurysm becomes Whatever the cause, the aneurysm becomes progressively larger !progressively larger !
tension within the vessel wall is directly influenced by the tension within the vessel wall is directly influenced by the diameter and the lateral blood pressure diameter and the lateral blood pressure
localized dilatation of the vessel at the site of aneurysms localized dilatation of the vessel at the site of aneurysms leads to increase of diameter and therefore enhance the leads to increase of diameter and therefore enhance the tension within the vessel wall, what again may enhance it´s tension within the vessel wall, what again may enhance it´s enlargement enlargement
Consequences Consequences IIschemia below the location of aneurysmaschemia below the location of aneurysma Acute thrombosis at the site of aneurysmaAcute thrombosis at the site of aneurysma Dysrupture of aneurysmaDysrupture of aneurysma Embolization of the thrombus into the more peripheral Embolization of the thrombus into the more peripheral
circulation circulation

Inflamatory diseases – Thrombangitis obliteransInflamatory diseases – Thrombangitis obliterans
Burger´s diseaseBurger´s disease
Inflammatory disease of small peripheral arteriesInflammatory disease of small peripheral arteries
chronic inflammatory processchronic inflammatory process inflammation is localized at the intima of affected inflammation is localized at the intima of affected
vessels, and thrombosis is just a secondary vessels, and thrombosis is just a secondary consequence of itconsequence of it
affected vessels are prone to vasospasm affected vessels are prone to vasospasm affected are mainly tibial and plantar arteries affected are mainly tibial and plantar arteries

Etiopathogenesis of the disease is unknown Etiopathogenesis of the disease is unknown
affected population - men 20 – 40 yrs, smokers, affected population - men 20 – 40 yrs, smokers, autoimmunityautoimmunity
Disease has three stagesDisease has three stages
1)1) inflammatory and spastic phase (phlebitis inflammatory and spastic phase (phlebitis ssaltans, altans, migrans)migrans)
2)2) obliterative phase with symptoms and obliterative phase with symptoms and signs of signs of ischemia ischemia
3)3) gangrenegangrene


Vasospastic diseasesVasospastic diseases
Attacks of sudden constrictions of small diameter arteries Attacks of sudden constrictions of small diameter arteries and arterioles of upper and also lower extremities, and arterioles of upper and also lower extremities, commonly fingers, sometimes toescommonly fingers, sometimes toes
Raynaud disease – Raynaud disease – primary vasospastic without any primary vasospastic without any obvious or clear cause, most affected are young ladiesobvious or clear cause, most affected are young ladies
Raynaud phenomenon – Raynaud phenomenon – syndrome, secondary problem syndrome, secondary problem usually linked with systemic collagen diseases, usually linked with systemic collagen diseases, autoimmune diseases, toxic influences, long lasting autoimmune diseases, toxic influences, long lasting vibration exposition, ...vibration exposition, ...

Raynaud disease Raynaud disease
In spite the cause is unknown, there was identified hypetrophy In spite the cause is unknown, there was identified hypetrophy of myoepithelial cells, which participate in regulation of of myoepithelial cells, which participate in regulation of blood supply to the capillary bed and hyperplastic changes blood supply to the capillary bed and hyperplastic changes of a-v- anastomosesof a-v- anastomoses
cold or emotional stimulus is usually the provoking factor, cold or emotional stimulus is usually the provoking factor, leading to severe vasoconstriction, blood is redirected leading to severe vasoconstriction, blood is redirected through a-v anastomoses into the venous system, while the through a-v anastomoses into the venous system, while the capillaries are compromisedcapillaries are compromised
Typical three phaTypical three phasicsic color changes of the skin, color changes of the skin, changes are always symetricchanges are always symetric
a)a) sudden pallor (dogiti mortui)sudden pallor (dogiti mortui)b)b) followed by cyanosisfollowed by cyanosisc) c) finally redness caused by reactive hyperaemiafinally redness caused by reactive hyperaemia

Raynaud phenomenonRaynaud phenomenon
It is only a sign (manifestation/ of other It is only a sign (manifestation/ of other primarily well defined diseaseprimarily well defined disease
Example: systemic lupus erythematodes, Example: systemic lupus erythematodes, primary pulmonary hypertension, soprimary pulmonary hypertension, someme endocrine disorders – myxedema-, exposition to endocrine disorders – myxedema-, exposition to vibrations, intoxication with ergot (claviceps vibrations, intoxication with ergot (claviceps purpurea)purpurea)
Symptoms are asymetric, affected persons are Symptoms are asymetric, affected persons are both men and women both men and women

All mentioned diseases may lead to acute or chronic All mentioned diseases may lead to acute or chronic progressive obliteration of the vessel lumen. progressive obliteration of the vessel lumen.
Obliteration of the lumen increases the vessel Obliteration of the lumen increases the vessel resistance.resistance.
Increased resistance means - decreased blood Increased resistance means - decreased blood supply supply to the to the affected region with a possibility of affected region with a possibility of ischemia. ischemia.

http://lifeinthefastlane.com/2011/01/cardiovascular-curveball-012/
http://www.bellevuepodiatrist.com/raynauds-phenomenon-red-white-and-blue-toes/

Occlusive arterial diseaseOcclusive arterial disease
Chronic occlusive arterial diseaseChronic occlusive arterial disease ischemia as a result of ischemia as a result of arterial obstructionarterial obstruction
Obstructive arterial lesions occur more frequently in the lowerObstructive arterial lesions occur more frequently in the lower extremities than in the upper extremities.Obstruction extremities than in the upper extremities.Obstruction influencing the blood flow to lower extremities is usually influencing the blood flow to lower extremities is usually localised. at:localised. at:
- aortoiliac level- aortoiliac level
- femoropopliteal level- femoropopliteal level
- popliteo-tibial level- popliteo-tibial level

DevelopmentDevelopment
- - arterial lumen is progressively narrowedarterial lumen is progressively narrowed resistance resistance to blood flowto blood flowblood flow to the tissue below the lesionblood flow to the tissue below the lesion is reduced is reduced tendency to tissue ischemia tendency to tissue ischemia
- - vessel lumen must be reduced by approximately 50% invessel lumen must be reduced by approximately 50% in diameter or 75% in crossectional area to produce clinicallydiameter or 75% in crossectional area to produce clinically significant interference with blood flowsignificant interference with blood flow
- - in combination (stenosis occurring in sequence), less in combination (stenosis occurring in sequence), less significant lesions can seriously impair blood flowsignificant lesions can seriously impair blood flow

At the site of stenosis and below the stenosis we can see At the site of stenosis and below the stenosis we can see changes of the blood flow likechanges of the blood flow like
- acceleration of the blood flow at the site of stenosisacceleration of the blood flow at the site of stenosis- turbulent blood flow below the stenosis with recirculation of turbulent blood flow below the stenosis with recirculation of
the blood, whirls (murmors present above the affected the blood, whirls (murmors present above the affected vesselvessel
- poststenotic dilatation with possibility for thrombogenesispoststenotic dilatation with possibility for thrombogenesis
Stenosis less than 75% of crossectional area is not compromising blood flow during the rest condition, but during the physical exercise – it could interfere with the blood supply leading to ischemia

Example for Example for stenosis occurring in sequence, less stenosis occurring in sequence, less significant lesions can seriously impair blood flowsignificant lesions can seriously impair blood flow
When small nonsignificanWhen small nonsignificantt st steenosis may lead to nosis may lead to ischemia?ischemia?
During physical exerciseDuring physical exercise ( (OO2 2 requirements, requirements, vasodilatation in working muscle, decrease of vasodilatation in working muscle, decrease of driving pressure)driving pressure)
During elevation of the extremityDuring elevation of the extremity (no hydrostatic (no hydrostatic effect supporting the blood supply)effect supporting the blood supply)

Intensity of ischemic damage depends on –Intensity of ischemic damage depends on –
the site /level/ of the vessel occlusion the site /level/ of the vessel occlusion – aortoilic, – aortoilic, femoropopliteal, popliteotibial levelfemoropopliteal, popliteotibial level
extent and seriousness of stenosisextent and seriousness of stenosis time course of occlusion development /acute vs. time course of occlusion development /acute vs.
chronic/chronic/ presence and quality of collateral circulation presence and quality of collateral circulation Collateral circulation is unique and important Collateral circulation is unique and important
compensatory mechanism of long lasting, compensatory mechanism of long lasting, progressively worsening ischemia. Increased progressively worsening ischemia. Increased resistance of affected arteries is responsible for resistance of affected arteries is responsible for „opening“ of collateral circulation. Mainly „opening“ of collateral circulation. Mainly muscular arterial branches could be base for muscular arterial branches could be base for collateral circulation. collateral circulation.

Symptoms and signs of occlusive arterial diseaseSymptoms and signs of occlusive arterial disease
chronic course - usually ATS chronic course - usually ATS claudicatio intermittens claudicatio intermittens pain at rest pain at rest no pulse no pulse postural chpostural chaanges of the skin colornges of the skin color temperature gradient bellow and above stanosis temperature gradient bellow and above stanosis neurologic symptoms – paresthesisneurologic symptoms – paresthesis trophic changes of the skin, hair, nailstrophic changes of the skin, hair, nails atrophic muscles and soft tissuesatrophic muscles and soft tissues ulceration and gangrene – ulceration and gangrene – (dry, wet)(dry, wet)

Symptoms and signs of occlusive arterial diseaseSymptoms and signs of occlusive arterial disease
acute course – thrombosis, embolisation, traumaacute course – thrombosis, embolisation, trauma
dominant severe ischemic paindominant severe ischemic pain no pulseno pulse distal part below the stenosis is paledistal part below the stenosis is pale temperature gradienttemperature gradient decreased filling of superficial venous system decreased filling of superficial venous system no trophic changes – thno trophic changes – theere is no time for their re is no time for their
developmentdevelopment

Occlusive arterial disease in patients with DMOcclusive arterial disease in patients with DM
macroangiopathymacroangiopathy – ATS – ATS (in DM patients is accelerated(in DM patients is accelerated))- hypertensionhypertension- hyperlipidaemia and dyslipidaemiahyperlipidaemia and dyslipidaemia- impaired nutrition of vessel wall because of dysfunction of vasa impaired nutrition of vessel wall because of dysfunction of vasa
vasorumvasorum
microangiopathymicroangiopathyDamage of small diameter arteries and capillaries by Damage of small diameter arteries and capillaries by
generaliezed chronic complication of DM generaliezed chronic complication of DM
endothelial damage endothelial damage (diffusion of glucose into the cells, change into (diffusion of glucose into the cells, change into sorbitol, endothelial swelling – endothelial dysfunction....)sorbitol, endothelial swelling – endothelial dysfunction....)
In this group of patients – ischemic problems with lower In this group of patients – ischemic problems with lower extremities are very common, shifted to „younger“ extremities are very common, shifted to „younger“ age, and are usually complicated by immunodeficiency age, and are usually complicated by immunodeficiency and metabolic disorder /worse healing of wounds/and metabolic disorder /worse healing of wounds/

http://www.surgery.usc.edu/divisions/vas/legpainandlowerextremityarterialdisease.html

Venous system of lower extremitiesVenous system of lower extremities
http://www.chivatechnique.com/veins.php

Blood flow in veins – lower extremitiesBlood flow in veins – lower extremities
vis a tergovis a tergo – rest of left ventricle ejection energy – rest of left ventricle ejection energy vis a frontevis a fronte – suction of right atrium caused by up – suction of right atrium caused by up
and down movement oand down movement off AV junction AV junction negative thoracic pressure during inspirationnegative thoracic pressure during inspiration craniocaudal movement ocraniocaudal movement off diaphragm diaphragm corresponding changes of abdominal pressurecorresponding changes of abdominal pressure horizontal body positionhorizontal body position rhythmic compression and decompression of deep rhythmic compression and decompression of deep
venous system by muscles /walking/venous system by muscles /walking/ valvesvalves plantar venous mechanismplantar venous mechanism ppulsation of commitant arteriesulsation of commitant arteries

Venous system of lover extremities Venous system of lover extremities
superficial venous system (10% of venous returs)deep venous system (90% of venous return)system of perforating veins Physiological pattern of venous return from lower extremity:


Function of the valvesFunction of the valves
If the valves are working properly:If the valves are working properly: they completely prevent pervasion of the blood from deep they completely prevent pervasion of the blood from deep
into superficial system into superficial system they redirect central blood flow within the deep system they redirect central blood flow within the deep system they prevent retrograde blood flow from the upper level, if they prevent retrograde blood flow from the upper level, if
once the blood was ejected by muscle pump to upper level. once the blood was ejected by muscle pump to upper level. During the muscle relaxation they completely prevent During the muscle relaxation they completely prevent backward blood flow to more distal levels. backward blood flow to more distal levels.

TrombophlebitisTrombophlebitis
Pathological process affecting mainly superficial venous Pathological process affecting mainly superficial venous
system. Primary affection is system. Primary affection is inflammationinflammation of spa. vein by of spa. vein by the process spreading from the surrounding tissue the process spreading from the surrounding tissue
Creation of thrombus is usually secondary phenomenon Creation of thrombus is usually secondary phenomenon superimposed to inflammation. superimposed to inflammation.
Thrombus is fixed to the vein wall by fibrin connections Thrombus is fixed to the vein wall by fibrin connections between the thrombus and inflamed vessel wall. The between the thrombus and inflamed vessel wall. The process is usually localized to the site of inflammation, no process is usually localized to the site of inflammation, no or minimal systemic symptoms, only local signs of or minimal systemic symptoms, only local signs of inflammation. inflammation.
No risk of emboli, b/c the thrombus if fixed onto the vein wall, No risk of emboli, b/c the thrombus if fixed onto the vein wall, and as well is localized within the superficial system.and as well is localized within the superficial system.

Deep venous thrombosis DVTDeep venous thrombosis DVT
- - intravital coagulation of the blood inside the intravital coagulation of the blood inside the vesselsvessels
- physiological mechanisms against thrombosis- physiological mechanisms against thrombosis continual blood flowcontinual blood flow intact endothelium intact endothelium balance in production of pro and anti coagulating balance in production of pro and anti coagulating
factors factors
Impairment of those three mechanisms , known as Impairment of those three mechanisms , known as
VirchowVirchow´s´s trias trias has crucial role in pathogenesis of has crucial role in pathogenesis of DVT. DVT.

Predisposing factors for DVTPredisposing factors for DVT history of DVT history of DVT immobilizationimmobilization (slowness of venous return from (slowness of venous return from
LE DK)LE DK) senior agesenior age (polymorbidity, dehydration, change (polymorbidity, dehydration, change
of rheologic properties of the blood)of rheologic properties of the blood) obesity, malignityobesity, malignity (production of pro (production of proccoagulating oagulating
factors)factors) heart failure, decompensation (heart failure, decompensation (venous congestion venous congestion
in backward failure)in backward failure) surgical procedures, traumasurgical procedures, trauma (release of tissue (release of tissue
tromboplastin)tromboplastin) pregnancy, puerperium, abortion pregnancy, puerperium, abortion (occlusion of (occlusion of
pelvic veins by pregnant uterus, enhanced pelvic veins by pregnant uterus, enhanced coagulation, tissue of trophoblast)coagulation, tissue of trophoblast)

PathogenesisPathogenesis
Slowing of the blood flow during immobilization, or in Slowing of the blood flow during immobilization, or in case of procoagulative status the blood there is a case of procoagulative status the blood there is a possibility of deposition of small amounts of fibrin at possibility of deposition of small amounts of fibrin at the site of vein valves the site of vein valves
The fibrin deposition is growing progressively by The fibrin deposition is growing progressively by apposition of „new“ fibrin fibers and platelets apposition of „new“ fibrin fibers and platelets trapped into the fibrin matrix – formation of trapped into the fibrin matrix – formation of thrombus thrombus
The thrombus is a serious occlusion, which impairs or The thrombus is a serious occlusion, which impairs or completely blocks the venous return through the completely blocks the venous return through the affected deep vein affected deep vein

http://www.jaapa.com/cvi-and-pad-a-review-of-venous-and-
arterial-disease/article/136677/
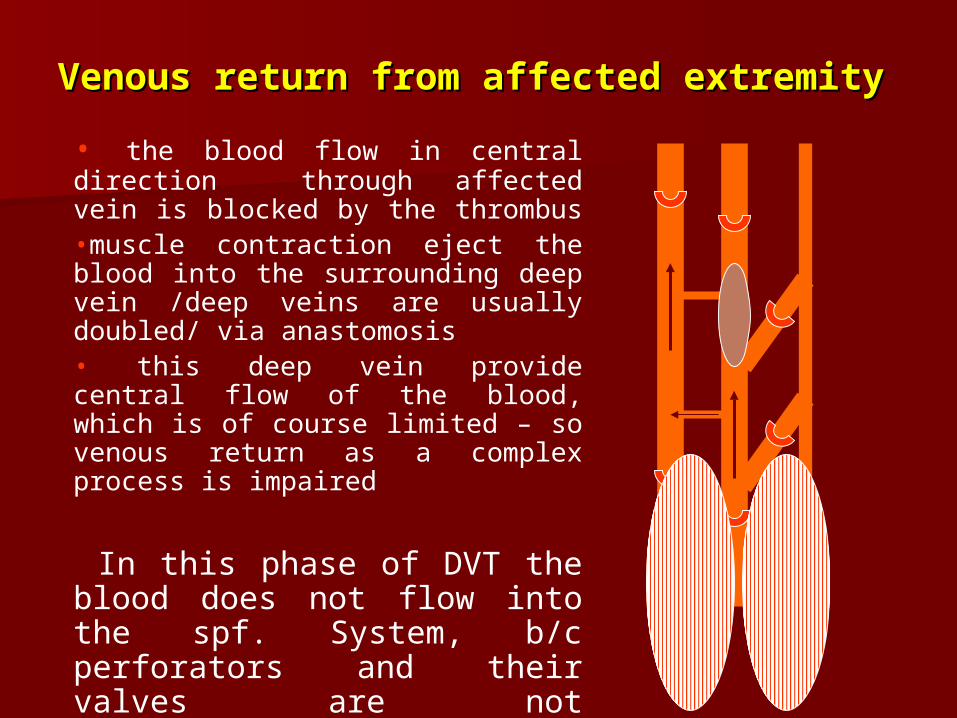
Venous return from affected extremityVenous return from affected extremity
• the blood flow in central direction through affected vein is blocked by the thrombus •muscle contraction eject the blood into the surrounding deep vein /deep veins are usually doubled/ via anastomosis• this deep vein provide central flow of the blood, which is of course limited – so venous return as a complex process is impaired
In this phase of DVT the blood does not flow into the spf. System, b/c perforators and their valves are not affected/destroyed, YET.

Venous return in a stage of recanalisation Venous return in a stage of recanalisation
Muscle contraction ejects the blood into three directions •through partially recanalized vein upwards• through anastomosis into surrounding deep vein •through perforating veins /which valves are destroyed/not working / into the spf. system.
During muscle relaxation – spf. veins are emptying only partially into the deep veins, with sudden balancing of the pressure in both systems.Blood is cumulating in spf. veins – leading to permanent hypertension in spf. system and recanalized part of deep venous system.

Venous return after total recanalisation
Total recanalisation means healing of the vein, desobliteration, Total recanalisation means healing of the vein, desobliteration, consequence of this process unfortunately is fibrotisation, or consequence of this process unfortunately is fibrotisation, or destruction of the valves.destruction of the valves.
During muscle contraction the blood from deep vein is ejected into three directions
-to SPF veins b/c of insufficient valves of perforating veins-to SPF veins b/c of insufficient valves of perforating veins-to central direction through recanalised vein upwards-to central direction through recanalised vein upwards -to central direction through surrounding deep vein-to central direction through surrounding deep vein Muscle relaxation: tendency for downward blood flow with rise Muscle relaxation: tendency for downward blood flow with rise
of pressure in deep system, therefore emptying of spf. veins of pressure in deep system, therefore emptying of spf. veins which had to be enhanced by the „suctionwhich had to be enhanced by the „suction“ “ of negative of negative pressure is limited pressure is limited

http://www.nlm.nih.gov/medlineplus/ency/imagepages/2549.htm

ConsequencesConsequences
physiological pattern of venous return is affectedphysiological pattern of venous return is affected onset of hypertension in spf. system and retrograde onset of hypertension in spf. system and retrograde
venostasis venostasis
Venous congestion – consequence for the capillary Venous congestion – consequence for the capillary
balancebalance Congestion leads toCongestion leads to- rise of hydrostatic pressure at the venous end of the rise of hydrostatic pressure at the venous end of the
capillary capillary - hypoxic damage to the endothelial cellshypoxic damage to the endothelial cells- increase of capillary permeabilityh and therefore increase of capillary permeabilityh and therefore
transudation of fluids into the pericapillary spacetransudation of fluids into the pericapillary space

Symptoms and signs of DVTSymptoms and signs of DVT
- Depends on the level of deep system which is Depends on the level of deep system which is altered by thrombosis, crural thrombosis – pain, altered by thrombosis, crural thrombosis – pain, asymetric edema, fever – not so severe symptomsasymetric edema, fever – not so severe symptoms
Ileofemoral levelIleofemoral level- severe painsevere pain- edema, feeling of „heavy“ leg, edema, feeling of „heavy“ leg, - dilatation of superficial veinsdilatation of superficial veins- skin is stretched, pale or cyanotic /according the skin is stretched, pale or cyanotic /according the
progress of disease/progress of disease/- phlegmasia alba/coerulea dolensphlegmasia alba/coerulea dolens- always fever, shivering, general symptoms, always fever, shivering, general symptoms,
restlessness, anxietyrestlessness, anxiety

VaricesVarices Cyllindric or saccular dilatation of spf. veins usually linked with relative valve Cyllindric or saccular dilatation of spf. veins usually linked with relative valve
insufficiency insufficiency Primary varicesPrimary varicesSecondary varicesSecondary varices
Primary varicesPrimary varices genetic predisposition, inherited insufficiency of connective tissue, abnormal genetic predisposition, inherited insufficiency of connective tissue, abnormal
collagen moleculle, collagen moleculle, The vein´s wall is weakened because of abnormal connective tissue, less tonus of The vein´s wall is weakened because of abnormal connective tissue, less tonus of
muscular layer muscular layer passive dilatation of the vein passive dilatation of the vein
Supporting risk factorsSupporting risk factors repeated increases of the pressure in spf. veinsrepeated increases of the pressure in spf. veins long lasting sitting, or standing without muscle contractions, obesity, pregnancylong lasting sitting, or standing without muscle contractions, obesity, pregnancy

Secondary varicesSecondary varices
Always as a consequence of DVT, and valve Always as a consequence of DVT, and valve damagedamage
– – dilatation of vein enhances more and more dilatation of vein enhances more and more relative insufficiency of the valves in perforating relative insufficiency of the valves in perforating and spf. Veinsand spf. Veins
Muscle contraction ejects the blood upwards, but Muscle contraction ejects the blood upwards, but also into the spf. system, what is not also into the spf. system, what is not physiological - spf. venous hypertension physiological - spf. venous hypertension
http://www.chivatechnique.com/veins.php
ChChronic venous insufficiencyronic venous insufficiency
CHVI – due to inappropriate venous return form the lover CHVI – due to inappropriate venous return form the lover extremity as a consequence of severe impairment of extremity as a consequence of severe impairment of hemodynamic mechanisms of venous return itself, is always hemodynamic mechanisms of venous return itself, is always linked with hypertension in spf. systemlinked with hypertension in spf. system
Venous hypertension in lover extremitiesVenous hypertension in lover extremitiesRetrograde venostasis with simultaneous imbalance of Retrograde venostasis with simultaneous imbalance of
hydrostatic pressures within the capillary –hydrostatic pressures within the capillary – Starling Starling mechanismmechanism
transudation of fluids into IST space transudation of fluids into IST space edema edema endothelial hypoxic damageendothelial hypoxic damage increase of capillary permeabilityincrease of capillary permeability transudation of proteins, RBC into he IST spacetransudation of proteins, RBC into he IST space fibrotic processes within IST spacefibrotic processes within IST space

Symptoms and signs of CHVISymptoms and signs of CHVI
pain – pain – venous claudicationvenous claudication, improves during , improves during elevation of extremityelevation of extremity
edema edema induration and thickness of subcutaneous tissueinduration and thickness of subcutaneous tissue hyperpigmentation of the skin – hyperpigmentation of the skin – caused by caused by
hemosiderine from RBC trapped and destroyed hemosiderine from RBC trapped and destroyed within the tissue within the tissue
trophic changestrophic changes (sclerosis of the skin, (sclerosis of the skin, ulcerations, scars after ulcers healing) – edema ulcerations, scars after ulcers healing) – edema and fibrotisation limit transport of oxygen and and fibrotisation limit transport of oxygen and substrates to the tissues, that´s why we have substrates to the tissues, that´s why we have trophic changestrophic changes
ulcus crurisulcus cruris
http://meded.ucsd.edu/clinicalimg/extremities_venous_insuf4.htm

http://www.oculusis.com/mexico/is/varicose/varicose2.php

LymphedemaLymphedema
Lymphatic system provide filtration of the
blood, participates in immune reaction
and production and outflow of lymph is a
part of Starling balance.
Lymphedema – edema of the tissue due to
impaired production and/or outflow of the
lymph.
http://www.healingdaily.com/exercise/rebounding-for-detoxification-and-health.htm

LymphedemaLymphedema - - no painno pain - in this case the fluid contains considerable - in this case the fluid contains considerable
amount of proteinsamount of proteins
Dysfunction of lymphatic system could be: Dysfunction of lymphatic system could be:
inheritedinherited (inherited hypoplasia of lymphatic capillaries and (inherited hypoplasia of lymphatic capillaries and vessels – Sy. Nonne – Milroy) , vessels – Sy. Nonne – Milroy) , lymphedema is usually lymphedema is usually symmetric, affecting both extremities, in kidssymmetric, affecting both extremities, in kids
acquiredacquired ((obstruction of lymphatic vessels or nodes by obstruction of lymphatic vessels or nodes by tumor, scar tissue, parasites, external compression, etctumor, scar tissue, parasites, external compression, etc), ), lymphedema is usually asymmetric, mainly adultslymphedema is usually asymmetric, mainly adults

Mechanisms involvedMechanisms involved
1)1) static insufficiency of lymph. system –static insufficiency of lymph. system – decrease decrease of the transport capacity of the normal ly. of the transport capacity of the normal ly. system, volume of produced lymph within the system, volume of produced lymph within the tissue is normal /block of ly. flow/tissue is normal /block of ly. flow/
2)2) dynamic insufficiency of lymph. systemdynamic insufficiency of lymph. system – – ly. ly. system is intact, but is not able to drain lymph system is intact, but is not able to drain lymph from the tissue, because of overproduction of from the tissue, because of overproduction of the lymphthe lymph
- localized regional inflammation - localized regional inflammation
- venous congestion- venous congestion

Lymphedema is chronic progressive Lymphedema is chronic progressive pathological processpathological process
- accumulation of the protein molecules within the accumulation of the protein molecules within the tissuetissue
- eedema (osmotic action of proteins)dema (osmotic action of proteins)- chronic inflammationchronic inflammation- fifibrosisbrosis ConsequenceConsequence: f: fibibrotic obliteration of ly. Vessels rotic obliteration of ly. Vessels
and/or nodesand/or nodes decreased transport capacity decreased transport capacity leading to total block of lymphatic flowleading to total block of lymphatic flow
–– onset of blisters in affected areaonset of blisters in affected area– – repeated inflammations of the skin and repeated inflammations of the skin and
subcutaneous structures subcutaneous structures – – hyperkeratosis and papilomatosis of the skinhyperkeratosis and papilomatosis of the skin

Signs and symptomsSigns and symptoms
soft edema of the extremity, dough like consistence soft edema of the extremity, dough like consistence touching or pressing with the finger can make several touching or pressing with the finger can make several
hollows, with slow alignmenthollows, with slow alignment edema progressively gets more solid, creates folding edema progressively gets more solid, creates folding typically it is not painful typically it is not painful pallor, cold extremity, because of compromising of pallor, cold extremity, because of compromising of
„normal“ blood supply „normal“ blood supply lymph edema could crate bizalymph edema could crate bizarrrree shapes, leading to shapes, leading to
deformation of affected part of the body deformation of affected part of the body Long lasting lymphedema could lead to secondary skin Long lasting lymphedema could lead to secondary skin
affection like repeated inflammations caused by affection like repeated inflammations caused by spteptococcus sp., or trophic changes spteptococcus sp., or trophic changes

http://www.medsci.org/v07p0353.htm