
Patients with abnormal liver function test - … · 30 iu/l...
18
Patients with abnormal liver function test พญ. พนิดา ทองอุทัยศรี Liver function tests (LFTs) ที่ใช้ในทางคลินิก เป็นการตรวจ liver biochemical tests 1-2 บ่ง บอกความผิดปกติที่เกิดขึ ้นในตับ ประกอบด้วย 2 ส่วนหลักได้แก่ 1. การตรวจเอ็นไซม์ตับ (enzyme tests) เป็น markers ของ liver injury ได้แก่ 1.1 เอ็นไซม์ที่บ่งบอกการอักเสบของเซลล์ตับ (hepatocellular injury) ได้แก่ serum aminotransferases ประกอบด้วย alanine aminotransferase (ALT หรือ เดิมเรียกว่า serum glutamic-pyruvic transaminase หรือ SGPT) และ aspartate aminotransferase (AST หรือเดิมเรียกว่า serum glutamic-oxaloacetic transaminase หรือ SGOT) 1.2 เอ็นไซม์ที่บ่งบอกภาวะ cholestasis หรือโรคของระบบท่อน ้ าดีได้แก่ alkaline phosphatase (ALP) และ gamma glutamyl transpeptidase (GGT) 2. การตรวจการทางานของตับ (tests of liver function) ได้แก่ serum albumin, prothrombin time (PT) และ serum bilirubin Markers ของ hepatocellular injury Markers ของ hepatocellular injury หรือ necrosis ได้แก่ serum aminotransferases 1-2 โดยทั่วไป ALT ส่วนใหญ่มาจาก cytosol ของเซลล์ตับ ในขณะที่ AST สร้างจากเซลล์ตับมาจาก cytosol (ร้อยละ 20) และ mitochondria (ร้อยละ 40) 3 AST มีความจาเพาะในการวินิจฉัยโรคตับ น้อยกว่า ALT เนื่องจากมาจากหลายอวัยวะได้แก่ กล้ามเนื ้อ 4 กล้ามเนื ้อหัวใจ ไต สมอง ตับอ่อน ปอด เม็ดเลือดแดงและเม็ดเลือดขาว เป็นต้น 1-3 ทั ้ง ALT และ AST ถูกการกาจัดออกจากกระแส เลือดโดย reticuloendothelial system ทั ้งนี ้ half-life ของ ALT ในเลือดประมาณ 47 ชั่วโมง และ ของ total AST 17 ชั่วโมง และ mitochondrial AST 87 ชั่วโมง 3 โดยทั่วไป range ของค่าปกติของ ALT และ AST มาจาก mean ± 2 standard deviations ของคนที่คาดว่าปกติ ดังนั ้นประมาณร้อยละ 2.5 ของคนปกติอาจมี LFTs ผิดปกติได้ 4 ค่า upper limit ของ ALT และ AST ยังมีข้อโต้แย้งกันและมีความแตกต่างกันในแต่ละแห่ง 5-6 โดยส่วนใหญ่ กาหนดค่าสูงสุดไม่เกิน 40 IU/L แต่ใน guideline บางประเทศกาหนดค่า ALT ปกติในผู้ชายไม่เกิน
Transcript of Patients with abnormal liver function test - … · 30 iu/l...

Patients with abnormal liver function test
พญ. พนดา ทองอทยศร
Liver function tests (LFTs) ทใชในทางคลนก เปนการตรวจ liver biochemical tests1-2 บงบอกความผดปกตทเกดขนในตบ ประกอบดวย 2 สวนหลกไดแก
1. การตรวจเอนไซมตบ (enzyme tests) เปน markers ของ liver injury ไดแก
1.1 เอนไซมทบงบอกการอกเสบของเซลลตบ (hepatocellular injury) ไดแก serum aminotransferases ประกอบดวย alanine aminotransferase (ALT หรอเดมเรยกวา serum glutamic-pyruvic transaminase หรอ SGPT) และ aspartate aminotransferase (AST หรอเดมเรยกวา serum glutamic-oxaloacetic transaminase หรอ SGOT)
1.2 เอนไซมทบงบอกภาวะ cholestasis หรอโรคของระบบทอน าดไดแก alkaline phosphatase (ALP) และ gamma glutamyl transpeptidase (GGT)
2. การตรวจการท างานของตบ (tests of liver function) ไดแก serum albumin, prothrombin time (PT) และ serum bilirubin
Markers ของ hepatocellular injury
Markers ของ hepatocellular injury หรอ necrosis ไดแก serum aminotransferases1-2 โดยทวไป ALT สวนใหญมาจาก cytosol ของเซลลตบ ในขณะท AST สรางจากเซลลตบมาจาก cytosol (รอยละ 20) และ mitochondria (รอยละ 40) 3 AST มความจ าเพาะในการวนจฉยโรคตบนอยกวา ALT เนองจากมาจากหลายอวยวะไดแก กลามเนอ4 กลามเนอหวใจ ไต สมอง ตบออน ปอด เมดเลอดแดงและเมดเลอดขาว เปนตน1-3 ทง ALT และ AST ถกการก าจดออกจากกระแสเลอดโดย reticuloendothelial system ทงน half-life ของ ALT ในเลอดประมาณ 47 ชวโมง และของ total AST 17 ชวโมง และ mitochondrial AST 87 ชวโมง3
โดยทวไป range ของคาปกตของ ALT และ AST มาจาก mean ± 2 standard deviations ของคนทคาดวาปกต ดงนนประมาณรอยละ 2.5 ของคนปกตอาจม LFTs ผดปกตได4 คา upper limit ของ ALT และ AST ยงมขอโตแยงกนและมความแตกตางกนในแตละแหง5-6 โดยสวนใหญก าหนดคาสงสดไมเกน 40 IU/L แตใน guideline บางประเทศก าหนดคา ALT ปกตในผชายไมเกน
30 IU/L และผหญงไมเกน 19 IU/L6 เนองจากขอมลทางระบาดวทยาพบวาผทมคา ALT สงเกนกวาคาดงกลาวจะมโอกาสเสยชวตมากกวา
บางกรณตรวจวดระดบ ALT และ AST อาจมคาสงหรอต าลวง โดยทไมมความผดปกตทตบเชน ผปวยทกนยา erythromycin และ para-aminosalicylic acid ถาตรวจวด aminotransferase โดย colorimetric tests ซงเปนเทคนคเกาจะมคาสงลวง ผปวยโรคไตวายทใช SMA-12/60 autoanalyser หรอจาก uremic toxin จะท าใหคา ALT และ AST ต ากวาความเปนจรง7 ในผปวย Crohn's disease อาจมคา ALT ต ากวาความเปนจรง เปนตน
Markers ของ cholestasis
ALP และ GGT เปน markers ของ cholestasis ทงน ALP มาจากตบและกระดกเปนสวนใหญ ทอนๆมาจากล าไสเลก ไต หรอ รก ดงนนในวยทก าลงเจรญเตบโต ม ALP สงจากกระดก ในหญงตงครรภ อาจสงจากรก รวมกบม hypermetabolic state และในผปวยโรคไตวาย ม ALP สงจาก intestinal ALP isoenzyme เปนตน ดงนนถาม GGT รวมสงดวยชวยบงบอกวา ALP มาจากตบหรอทอน าด1-3 และควรอดอาหารกอนตรวจ เนองจากอาหารไขมนอาจท าให ALP สงได การตรวจอนๆเพอสนบสนนวา ALP สงจากตบไดแก electrophoresis โดยใช polyacrylamide gel หรอ sepharose และ 5'-nucleotidase เปนตน โดยทวไป half-life ของ ALP ในเลอดประมาณ 5-7 วน ในการ clearance ขนกบการท างานของตบและการขบออกทางทอน าด
ภาวะทท าให serum ALP ต าไดแก congenital hypophosphatasia, hypothyroidism, pernicious anemia, fulminant Wilson's disease, zinc deficiency, congenital hypophosphatemia และ progressive familial intrahepatic cholestasis1-2
ในกรณท GGT สงอยางเดยวโดยทไมไดเปนโรคตบและ LFTs อนๆปกต เชนถาดมแอลกอฮอล 3 drinks ตอวนขนไป ในชวงเวลา 2-3 สปดาหกอนตรวจเลอด อาจพบ GGT สงได ทงนเนองจาก half-life ของ GGT ในเลอดนาน 26 วน GGT ทสงจงกลบมาปกตใน 8 สปดาห8
ดงนนอาจใช GGT เปน marker วาผปวยยงดมสราหรอเครองดมทมแอลกอฮอล และในผปวยทกนยา phenobarbital และ phenytoin (dilantin) จะม GGT สงไดแตมกไมเกน 2 เทา9
Markers ของ synthetic function
Albumin โดยปกตตบสราง albumin 12 กรมตอวน ถาการท างานของตบลดลงไมมาก หรอมการสญเสย albumin จากภาวะตางๆ ในระยะแรกตบกสามารถ compensate โดยสราง albumin เพมเปน 2 เทาของภาวะปกตได โดยทวไป 2 ใน 3 ของ albumin ในรางกายอยท

extravascular, extracellular space ซงมการแลกเปลยนกบในเลอด และ half-life ของ albumin ในเลอดนานประมาณ 20 วน ดงนนระดบ albumin ในเลอดขนกบอตราการสรางและ plasma volume
ในผปวยโรคตบแขง ตบจะสราง albumin ลดลง ประกอบกบมภาวะการขาดสารอาหารรวมกบมการเสย albumin มาใน ascites ท าใหเกดภาวะ hypoalbuminemia ในทางตรงขามผปวยโรคตบแขงมกม serum globulin สงขนเชอวาอาจเกดจากม transient bacteremia ดงนนใน LFTs จงพบลกษณะ reverse albumin/globulin (A/G) ratio คา serum globulin ทสงในผปวยโรคตบมกจะ nonspecific ยกเวนใน autoimmune hepatitis พบ serum IgG สง10 และใน primary biliary cirrhosis (PBC) พบ serum IgM สง11 เปนตน
ในกรณท serum albumin ต าเพยงอยางเดยว โดยท LFTs อนปกต ใหสงสยภาวะอนทไมไดเกดจากโรคตบกอนเชน proteinuria, acute หรอ chronic inflammatory state เชน burns, trauma และ sepsis ซงภาวะเหลานสามารถกดการสราง albumin นอกจากนพบใน active rheumatic disorders, severe end-stage malnutrition และในภาวะตงครรภ เปนตน1-3
Coagulation factors โดยสวนใหญ coagulation factors ตางๆสรางจากตบ (ยกเวน factor VIII และ von Willebrand factor (vWF) สรางจากผนงเสนเลอด) ไมวาจะเปน fibrinogen, vitamin K-dependent factors (prothrombin, factors VII, IX, และ X) และ factor V ทงน factor VII ม half-life สนทสด ตามดวย factors X และ IX ดงนนจงใชคา prothrombin time (PT) เพอวดการท างานของตบ บอกความรนแรงและพยากรณโรค อยางไรกตามผปวยทม prolonged PT อาจเกดจากการท างานของตบลดลงหรอจากภาวะ cholestatic liver disease ได การแยก 2 ภาวะดงกลาวโดยฉด vitamin K 10 มลลกรมตอวน ทาง subcutaneous หรอ intravenous นาน 3 วน ถาเปนจาก cholestasis จะสามารถ correct PT ทผดปกตได นอกจากนการวด factor V ในเลอดอาจจะชวยแยก 2 ภาวะ ดงกลาวได1-3 เนองจาก factor V ไมไดเปน vitamin K-dependent ดงนนถาม factor V ต ารวมดวย นาจะเกดจากการท างานของตบลดลง นอกจากน factor V ยงชวยบอกพยากรณโรคได เชนใน fulminant hepatic failure ถา factor V นอยกวารอยละ 20 ของปกต เปนตวบอกวา poor prognosis ควรรบท า liver transplantation
การทม prolonged PT อาจพบไดในภาวะอนๆเชน disseminated intravascular coagulation, inherited deficiencies of coagulation factors และยาบางอยางท antagonize prothrombin complex เปนตน ส าหรบ international normalized ratio (INR) เปนตวบงชระดบของ coagulopathy ดกวา PT เนองจากมการ standardized value ท าใหลดการคลาดเคลอนของคา PT และสามารถน ามาใชในการบอกพยากรณโรคได12-14
Serum bilirubin ไดจากการสลาย heme ซงมาจากการแตกตวของเมดเลอดแดงเปนสวนใหญ ทงน unconjugated bilirubin ทไดจะเขาสตบและ conjugated กบ glucuronic acid เปลยนเปน

เปน conjugated bilirubin ซงละลายน าไดและขบทางน าด โดยทวไป hyperbilirubinemia อาจเกดจาก overproduction หรอความผดปกตในการ uptake, conjugation, หรอ excretion ถาความผดปกตเกดขนทตบท าใหไมสามารถขบ conjugated bilirubin ออกทางน าดได conjugated bilirubin จงถกกรองออกทางปสสาวะสามารถตรวจพบจาก dipstick test
เมอตรวจพบ isolated hyperbilirubinrmia ตองดวาเปน unconjugated หรอ conjugated bilirubin ทสง ถาเปน unconjugated hyperbilirubinemia เกดจาก overproduction เชน hemolysis ทงทเปน inherited disorders เชน spherocytosis, sickle cell anemia, pyruvate kinase และ glucose-6-phosphate dehydrogenase deficiency เปนตน หรอเกดจาก acquired hemolytic disorders เชน microangiopathic hemolytic anemia, hemolytic-uremic syndrome, paroxysmal nocturnal hemoglobinuria และ immune hemolysis เปนตน ซง serum total bilirubin มกไมเกน 5 mg/dL และอาจ confirm โดยการตรวจ reticulocyte count หรอ haptoglobin นอกจากน unconjugated hyperbilirubinemia อาจเกดจากความผดปกตท hepatic uptake/conjugation ของ bilirubin เชน Gilbert's disease, Crigler-Najjar syndrome และยาเชน rifampicin และ probenecid เปนตน1-3
ภาวะ isolated conjugated hyperbilirubinemia พบใน 2 inherited conditions ซงพบไมบอยไดแก Dubin-Johnson syndrome และ Rotor syndrome1-3 ในผปวย hepatocellular diseases หรอภาวะ cholestasis จะม serum bilirubin สงได โดยมสดสวนของ conjugated bilirubin มากกวา unconjugated bilirubin และม LFTs อนๆผดปกตรวมดวย
แนวทางในการ approach ผปวยทม abnormal LFTs
การแปลผล LFTs มขอจ ากดหลายอยาง และความไวและความจ าเพาะในการวนจฉยโรคตบไมดนก ผปวยโรคตบในระยะแรกมกไมมอาการผดปกตและอาจตรวจไมพบความผดปกตใน LFTs ได 15 เชน ผปวยทเปนพาหะของไวรสตบอกเสบบ ผปวยโรคตบแขงระยะเรมแรก ฯลฯ หรอถามความผดปกตทระบบอนอาจจะตรวจพบ LFTs ผดปกตได เชนภาวะ hemolysis พบวาม serum bilirubin สง การตรวจ AST สงอยางเดยวอาจจะมาจากกลามเนอตางๆรวมถงกลามเนอหวใจ หรอ ALP สงอาจมาจากกระดก รก (placenta) ล าไส หรอโรคของตอมไธรอยด17-18 ฯลฯ
ดงนนในการแปลความหมาย LFTs จงตองอาศยขอมลการซกประวต และตรวจรางกายอยางละเอยด 1-2 เชน อาการและอาการแสดงของโรคตบ ตาเหลองตวเหลอง ไข คลนไส อาเจยน ปวดทอง คนตามตว ปสสาวะเขม อจจาระสซดลง บวม เบออาหาร น าหนกลด ประวตการดมสรา การใชยา รวมถงสมนไพร ลกกลอน ยาชด ความเสยงตอไวรสตบอกเสบเชน รบเลอด การสกเจาะ

ผวหนง การฉดสารเสพตด เพศสมพนธ รวมถงอาการผดปกตของระบบอนๆและโรคประจ าตวเชน โรคหวใจ เบาหวาน autoimmune diseases อนๆ ฯลฯ โรคตบในครอบครว การตรวจรางกาย หา stigmata ของโรคตบเชน spider nevi, palmar erythema, gynecomastia, caput medusae, parotid gland enlargement, testicular atrophy, Dupuytren's contractures ฯลฯ และทกระบบอยางละเอยด หลงจากนนประมวลขอมลทงหมด แลวแปลผลวาความผดปกตของ LFTs นาจะเกดจากสาเหตใด แลวจงสงตรวจพเศษอนๆ การตรวจทางรงส ตลอดจนการตรวจชนเนอตบ19 เพอใหไดวนจฉยและใหการรกษาไดถกตองและเหมาะสม
การแปลผล LFTs ประกอบ 3 ขนตอน
ขนตอนท 1 ลกษณะ pattern ของ LFTs (hepatocellular, cholestasis หรอ mixed)
ขนตอนท 2 คนหาสาเหต
ขนตอนท 3 ประเมนพยากรณโรค (prognosis)
ขนตอนท 1 ลกษณะ pattern ของ LFTs
Patterns บงบอก hepatocellular หรอ parenchymatous disease คอ ALT และ AST สง และ patterns บงบอก cholestatic liver disease คอ ALP และ GGT สง และการแบงระดบของคาทวดไดเปน 3 ระดบ1 (ตารางท 1) ซงอาจชวยในการวนจฉยแยกโรคได
ตารางท 1 ระดบของ LFTs ทผดปกต (x จ านวนเทาของ upper limit of normal)1
Enzyme Measured สงเลกนอย สงปานกลาง สงมาก
Aspartate or alanine aminotransferase <2-3× 2-3 to 20× >20×
Alkaline phosphatase <1.5-2× 1.5-2 to 5× >5×
Gamma glutamyl transpeptidase <2-3× 2-3 to 10× >10×
ในบางครงพบความผดปกตทง 2 patterns ใหดวา marker ตวไหนทสงเดนมากกวา โดยการดสดสวน ALT (จ านวนเทาทมากกวา upper limit of normal) หารดวย ALP (จ านวนเทาทมากกวา upper limit of normal) ถาเปน parenchymatous disease มคามากกวา 5, mixed pattern อยระหวาง 2-5 และ cholestatic liver disease นอยกวา 2 20
แผนภมท 1 สดสวน ALT (จ านวนเทาทมากกวา upper limit of normal) หารดวย ALP (จ านวนเทาทมากกวา upper limit of normal) ในการแยกภาวะ parenchymatous disease, mixed pattern และ cholestatic liver disease

เชน ผปวยรายทหนงตรวจพบ ALT 800 U/L (upper normal limit ไมเกน 40 U/L) และ ALP 160 (upper normal limit ไมเกน 80 U/L) ดงนนเมอค านวณสดสวน ALT 800/40 หารดวย ALP 160/80 เทากบ 10 ดงนน LFTs ทผดปกตเกดจาก parenchymatous disease ผปวยรายท 2 พบ ALT 1200 U/L และ ALP 800 U/L ดงนนเมอค านวณสดสวน ALT 1200/40 หารดวย ALP 800/80 เทากบ 3 (อยระหวาง 2 ถง 5) แสดงวา LFTs ทผดปกตเปน mixed ทง hepatocellular และ cholestasis และผปวยรายท 3 พบ ALT 120 U/L และ ALP 400 U/L ดงนนเมอค านวณสดสวน ALT 120/40 หารดวย ALP 400/80 เทากบ 0.6 (นอยกวา 2) นาจะมาจากภาวะ cholestatic liver disease เปนตน
ขนตอนท 2 คนหาสาเหต
Parenchymatous disease
ระดบของ ALT ทสง อาจชวยบอกสาเหตได โดยเฉพาะถาสงมากกวา 20 เทาขนไปหรอมากกวา 1000 U/L พบใน acute viral hepatitis เชน เอ บ ซ ด และอ ควรสง anti-HAV IgM ในรายทสงสย acute viral hepatitis A, anti-HBc IgM และ HBsAg ใน acute viral hepatitis B หรอ HBV reactivation ในรายทสงสย acute viral hepatitis C บางครงการตรวจ anti-HCV อาจไมพบใน 2 สปดาหแรก ในรายทสงสยอาจสงตรวจ HCV PCR เปนตน นอกจากนแลวอาจเกดจากยาหรอ toxins ตางๆ โดยทวไปผลของยาทมตอตบแบงเปน 2 อยางคอ predictable และ unpredictable (idiosyncratic) ในกลมท predictable มกเกยวของกบขนาดยา (dose-dependent) และเกดไดกบทก

คน เชน acetaminophen hepatotoxicity ในคนทกน paracetamol overdose ในการณ idiosyncratic จะไมเกยวกบขนาดยา เกดกบคนบางกลมเชน ผปวยทไดรบยา antituberculosis drugs และ NSAIDs21 ส าหรบ toxins ทท าใหเกดภาวะนไดแก vinyl chloride, herbal preparations ทมสวนประกอบ pyrrolizidine alkaloids (Jamaica bush tea) และเหด Amanita phalloides หรอ verna เปนตน ภาวะ ischemic hepatitis (shock liver) หรอ hypoxic hepatitis 22-23 เชน cardiac arrest หรอ severe heart failure เปนตน ภาวะนม lactate dehydrogenase (LDH) ในเลอดสงมากรวมดวย พยากรณโรคขนกบสาเหตและการรกษาแกไขภาวะทเปนสาเหตและรกษา hemodynamic กลบมาปกตไดเรว LFTs มกกลบมาปกตไมเกนสปดาห นอกจากนอาจพบในผปวย autoimmune hepatitis ทมาดวย fulminant hepatitis ซงพบไมบอยแตม poor prognosis24 หรอผปวยทมาดวย acute liver failure และม AST/ALT มากกวา 4 และ ALP/bilirubin นอยกวา 2 ใหคดถงภาวะ fulminant Wilsonian hepatitis25-26
ถา ALT และ AST สงปานกลาง เกดจากหลายสาเหต อาจเปน acute viral hepatitis ทเอนไซมตบสงไมมาก หรอเปน chronic hepatitis ถาเอนไซมสงนานกวา 6 เดอน ( แผนภมท 2) สาเหตอาจเกดจากไวรสตบอกเสบบ ซ หรอ coinfection ทงนระดบ aminotransferase อาจสงตลอดเวลา หรอเปนบางชวงเวลา ถาตรวจพบ HBsAg-positive ใหสง HBeAg และ anti-HBe และ HBV DNA viral load เพมเตม ใน HBeAg –positive chronic hepatitis B (CHB) พจารณารกษาเมอ HBV DNA มากกวา 105 copies/mL หรอ 20,000 IU/mL ส าหรบ HBeAg –negative CHB พจารณาเรมรกษาเมอ HBV DNA มากกวา 104 copies/mL หรอ 2,000 IU/mL และควรท า liver biopsy กอนรกษาโดยเฉพาะอยางยงใน HBeAg –negative CHB27 กรณทพบ anti-HCV-positive ควรสง HCV RNA viral load และ HCV genotype และควรท า liver biopsy กอนรกษาโดยเฉพาะ genotype 128
ใน alcoholic hepatitis ระดบ AST สงมากกวา ALT 2 เทาขนไป แต AST มกสงไมเกน 500 IU/L และ ALT มกสงไมเกน 300 IU/L1-3 สาเหต chronic hepatitis ทเปน non-virus และ non-alcohol ไดแก ใน nonalcoholic fatty liver disease (NAFLD) มกพบในคนอวนหรอทม ภาวะ metabolic syndrome และตอง exclude สาเหตอน โดยทวไป ALT/AST มากกวา 129 และถาสงสย hepatitis จากยาใหหยดยาและตดตาม ALT และ AST ใน Wilson’s diseaseใหสงสยภาวะนในผปวยโรคตบอายนอยกวา 40 ป ทไมไดมสาเหตจากไวรสตบอกเสบและสรา ควรตรวจตาเพอหา Kayser-Fleischer (KF) ring และสงตรวจ serum ceruloplasmin ถาผลไมแนชดใหตรวจ 24-hour urine copper ถามากกวา 100 mcg/day ชวยในการวนจฉย และอาจจะตรวจยนยนดวย liver biopsy และวด quantitative copper มากกวา 250 mcg/gm ของ dry weight 30-31 ใน autoimmune hepatitis (AIH) พบในผหญงมากกวาชาย ตรวจเลอดพบ immunoglobulin G (IgG) สงรวมกบ autoantibodies

ตางๆ ไดแก antinuclear antibody (ANA), anti–smooth muscle antibody (ASMA) ซงใหผลบวกใน type 1 AIH และอาจท า liver biopsy เพอชวยยนยนการวนจฉย สวน type 2 และ type 3 AIH พบ anti–liver-kidney microsomal antibody (anti–LKM-1) และ antibodies against soluble liver antigen (anti-SLA) ตามล าดบ32-33
ผปวยทสงสย hereditary hemochromatosis (HHC) มอาการเหนอยงาย ผวคล า ปวดขอ (arthropathy) เบาหวาน ตรวจรางกายพบ มผวสคล า (skin bronzing หรอ hyperpigmentation) จากธาตเหลกและสารเมลานนสะสมทผวหนง หวใจโต (dilated cardiomyopathy) ตบโต ตรวจหา serum transferrin saturation ซงค านวณโดย total serum iron หารดวย serum iron ferritin คณดวย 100 ถามากกวา 45% ใหสงสยภาวะน ใหสง serum ferritin concentration เพมเตม ถามากกวา 400 ng/mL ในผชายและมากกวา 300 ng/mL ในผหญง จะชวยสนบสนนการวนจฉยโรคน หลงจากนนควรท า liver biopsy และหา hepatic iron index (hepatic iron concentration (micromoles/gram dry weight) หารดวยอาย ) ใน homozygous HHC มคามากกวา 1.9 และควรตรวจ genetic study และตรวจ screening ในครอบครว34 อยางไรกตามภาวะ HHC พบนอยในคนไทย สวนใหญมกจะเปน secondary hemochromatosis เชนใน thalassemia, hemolysis, ดมสรา หรอเคยรบเลอดจ านวนมากและเปนเวลานาน
ในกลมท ALT สงเลกนอย เกดไดจากหลายสาเหตไมจ าเพาะ ทงจาก chronic viral หรอ nonviral hepatitis ดงทกลาวขางตน รวมถงใน early cirrhosis ซงมกพบ AST มากกวา ALT
Cholestatic liver disease
ถาตรวจพบ ALP สง ควร confirm วา ALP มาจากตบโดยดท GGT สงดวย สาเหตอาจมาจากภาวะ extrahepatic และ intrahepatic cholestasis หรอเกดจากการทมกอนในตบ (space occupying lesion) ซงไปกดเบยดและ/หรอม invasion ท small, intrahepatic bile ducts เชน ฝทตบ มะเรงตบเชน hepatocellular carcinoma, peripheral type ของ cholangiocarcinoma และ metastasis CA ฯลฯ หรออาจเปนกอนจาก benign tumor เชน hemangioma, hepatic adenoma, focal nodular hyperplasia ฯลฯ นอกจากน ALP ทสงมาก (มากกวา 1,000 U/ L หรอมากกวา 6 เทาของคาปกต) มกเกดจาก infiltrative lesions เชน granulomatous diseases, amyloidosis, sarcoidosis, infiltrating tumors และ fungal infections3 ซงใน malignant infiltration ม LDH สงรวมดวย
สาเหต extrahepatic cholestasis ไดแก นวในทอน าด ในกรณ acute biliary tract obstruction ใน 24-48 ชวโมงแรกอาจพบ serum aminotransferase สง (มากกวา 300 IU/L) และลดลงอยางรวดเรว หลงจากนน serum ALP และ biliribin จงขนสงตาม35 ทงนเนองจาก ALP สราง

จาก bile duct epithelium เมอเกดภาวะ cholestasis จงใชเวลาในการสรางและหลง ALP ออกมา ดงนน ALP จงขนสงชากวา serum aminotransferase มะเรงทอน าด (cholangiocarcinoma) หรอ periampullar cancers อนๆเชน pancreatic cancer, gallbladder cancer และ duodenal cancer จาก ampullary cancer รวมทง malignancy อนๆหรอตอมน าเหลองกดทบทอน าดบรเวณ porta hepatits ซงผปวยอาจมอาการตาเหลองตวเหลองได หรออาจไมมอาการตาเหลองตวเหลองกได เชนใน focal intrahepatic ductal obstruction หรอม partial extrahepatic duct obstruction เปนตน โรค primary sclerosing cholangitis (PSC) พบนอยในคนไทย ผปวยมาดวยคนเปนๆหายๆ หรอ ascending cholangitis ตรวจเลอดพบ perinuclear antineutrophil cytoplasmic antibodies (p-ANCA) สง และเมอท า endoscopic retrograde cholangiography (ERCP) หรอ magnetic resonance cholangiography (MRCP) พบ intra- และ extrahepatic bile-duct strictures และ dilations (bead-like appearance) นอกจากน biliary dilatation อาจเกดจาก secondary sclerosing cholangitis จากสาเหตอน
ภาวะ intrahepatic causes เชน ยา เชน anabolic และ contraceptive steroids, chlorpromazine, imipramine, tolbutamide, sulindac, cimetidine, erythromycin estolate, trimethoprim-sulfamethoxazole, penicillin based antibiotics รวมถงยาชด ยาลกกลอน หรอสมนไพรหลายอยาง, ภาวะ sepsis, การให parenteral nutrition ฯลฯ และในผหญงวยกลางคน มอาการคนตามตวเปนๆหายๆ มไขมนในเลอดสง (hypercholesterolemia) ตบโต และ serum globulin สงโดยเฉพาะ IgM ใหคดถงโรค primary biliary cirrhosis (PBC) ควรสงตรวจ antimitochondrial antibodies (AMA) และตรวจชนเนอตบเพอยนยนการวนจฉย
ในผปวยทมคา ALP และ GGT ทสง ควรสงตรวจ U/S upper abdomen (แผนภมท 2) ถาพบวามกอน ในตรวจ อาจสงตรวจ CT หรอ MRI abdomen เพมเตมหรอตรวจชนเนอตบ ถา U/S upper abdomen พบ intrahepatic ducts dilatation ควรท า ERCP เพอหาสาเหตและใหการรกษา หรอ CT abdomen ในกรณทสงสยวามการกดเบยดทอน าดจากอวยวะอนๆ ในกรณ severe biliary obstruction เปนเวลานาน เมอแกไขภาวะดงกลาวโดยใส stent หรอ drainage โดย percutaneous หรอการผาตด เพอใหน าดไหลผานลงมาได ในชวง 2-3 วนแรก serum bilirubin จะลดลงอยางรวดเรว หลงจากนนเขาส slow phase ซงอาจจะใชเปนสปดาหจงกลบลงมาปกต เนองจาก delta-bilirubin จบกบ serum albumin (half-life 20 วน) ใชเวลา clearance นานกวา bilirubin-glucuronide เรยกภาวะนวา “delta-bilirubin phenomenon” ในกรณท U/S ไมพบกอนและไมพบ intrahepatic ducts dilatation อาจเกดจาก intrahepatic cholestasis ดงทกลาวขางตน หรอจาก infiltrative lesion หรอจาก partial extrahepatic duct obstruction

แผนภมท 2 แนวทางการ approach ผปวยทม ALP สง1
ในผปวยมะเรงอนๆอาจม ALP สงโดยทไมมความผดปกตทตบ เชน ในผปวยมะเรงปอดบางราย ม ALP ทสง ทงทไมมความผดปกตทตบและกระดก ซง ALP เปนชนด Regan ALP isoenzyme มลกษณะทางเคมตางจาก hepatic ALP isoenzyme และใน Hodgkin's disease และ renal cell carcinoma อาจม hepatic ALP isoenzyme สงโดยทไมไดท าใหเกดพยาธสภาพในตบโดยตรง แตเปนผลมาจาก nonspecific hepatitis เรยกภาวะนวา “bystander phenomenon”1
LFTs ผดปกต ทเกดจากสาเหตนอกตบ

ในกรณทสงสยวา LFTs ทผดปกต เกดจากสาเหตนอกตบ (ตารางท 2) การตรวจพเศษเพมเตมเพอชวยยนยนการวนจฉย ตารางท 2 สาเหตนอกตบ (Nonhepatic causes) ทท าให LFTs ผดปกต36
Test สาเหต Discriminating tests
albumin ต า Protein-losing enteropathy Serum globulins, alpha1-antitrypsin clearance
Nephrotic syndrome Urinalysis, 24-hr urinary collection for protein
Congestive heart failure Cardiac examination, two-dimensional echocardiogram
AST สง Myocardial infarction CK-MB, troponin, ECG
Muscle disorders CK, ESR
ALP สง Bone disease GGT, serum leucine aminopeptidase, 59-nucleotidase
Pregnancy GGT, 59-nucleotidase, hCG in serum and urine
Malignant tumor Alkaline phosphatase electrophoresis
Bilirubin สง Hemolysis Reticulocyte count, peripheral smear, LDH, haptoglobin
Sepsis Clinical setting, blood cultures
Ineffective erythropoiesis Peripheral smear, urine bilirubin, hemoglobin electrophoresis, bone marrow aspiration and biopsy
Shunt hyperbilirubinemia Clinical setting
PT สง Antibiotic use, anticoagulant use, steatorrhea, dietary
Response to vitamin K

deficiency
CK, creatine kinase; ECG, electrocardiogram; ESR, erythrocyte sedimentation rate; hCG, human chorionic gonadotropin; LDH, lactate dehydrogenase
ขนตอนท 3 ประเมนพยากรณโรค (prognosis)
หลงจากวนจฉยสาเหตโรคตบแลว ในผปวยโรคตบควรประเมนความรนแรงของโรคเพอบอกพยากรณโรค ตลอดจนปองกนและรกษาภาวะแทรกซอนทเกดขน การประเมนความรนแรงของโรคตบแขงโดยทวไปใช Modified Child-Turcotte-Pugh prognostic classification (ตารางท 3) ค านวณจาก 5 parameters ไดแก encephalopathy, ascites, bilirubin, albumin และ prothrombin time โดยแบงเปน 3 ระดบไดแก A (คะแนน 5-6), B (คะแนน 7-9) และ C (คะแนน 10-15) ตารางท 3 Modified Child-Turcotte-Pugh prognostic classification
parameters points
1 2 3
Encephalopathy (grade) 0 1-2 3-4
Ascites None Slight Moderate
Bilirubin (mg/dL) 1-2 2-3 >3
Albumin (g/dL) >3.5 2.8-3.5 <2.8
Prolonged prothrombin time (sec) หรอ INR
1-4 < 1.7
5-6 1.7-2.3
>6 > 2.3
นอกจากนประเมนความรนแรงของโรคตบ ทนยมใชแพรหลายในปจจบนคอ Model for End-stage Liver Disease. (MELD)37-39 ค านวนจาก
Model for End-stage Liver Disease (MELD) Scoring Equation[*]
MELD score for TIPS = 0.957 × loge(creatinine [mg/dL]) + 0.378 × loge(bilirubin [mg/dL]) +
1.120 × loge(INR) + .643 (cause of liver disease)[†]
MELD score for liver transplantation[‡] = 0.957 × loge(creatinine [mg/dL]) + 0.378 × loge(bilirubin [mg/dL]) + 1.120 × loge(INR) + .643
INR, international normalized ratio; TIPS, transjugular intrahepatic portosystemic shunt.
* Laboratory values less than 1.0 are set at 1.0. The maximum serum creatinine level considered in the MELD score equation is 4.0 mg/dL.
† 0 if cholestatic or alcoholic liver disease, and 1 if other liver disease.
‡ Multiply by 10 and round to the nearest whole number.
หรอเขาไปท http://www.unos.org/resources/MeldPeldCalculator.asp?index=98 ทงนถาคะแนนยงมากโอกาสเสยชวตสง ถาผปวยไมมขอหาม ควรรบสงตอเพอเตรยมตวท า liver transplantation
Direct quantitative testing ของ hepatocyte function
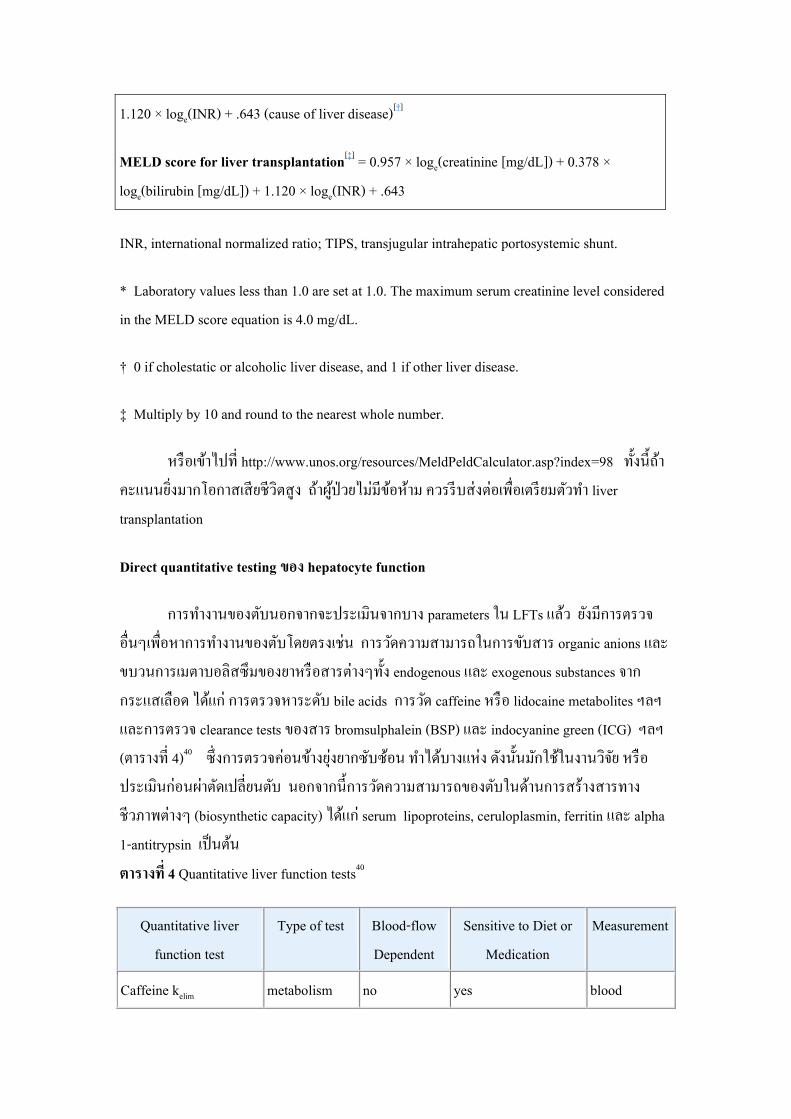
การท างานของตบนอกจากจะประเมนจากบาง parameters ใน LFTs แลว ยงมการตรวจอนๆเพอหาการท างานของตบโดยตรงเชน การวดความสามารถในการขบสาร organic anions และขบวนการเมตาบอลสซมของยาหรอสารตางๆทง endogenous และ exogenous substances จากกระแสเลอด ไดแก การตรวจหาระดบ bile acids การวด caffeine หรอ lidocaine metabolites ฯลฯ และการตรวจ clearance tests ของสาร bromsulphalein (BSP) และ indocyanine green (ICG) ฯลฯ (ตารางท 4)40 ซงการตรวจคอนขางยงยากซบซอน ท าไดบางแหง ดงนนมกใชในงานวจย หรอประเมนกอนผาตดเปลยนตบ นอกจากนการวดความสามารถของตบในดานการสรางสารทางชวภาพตางๆ (biosynthetic capacity) ไดแก serum lipoproteins, ceruloplasmin, ferritin และ alpha 1-antitrypsin เปนตน ตารางท 4 Quantitative liver function tests40
Quantitative liver function test
Type of test Blood-flow Dependent
Sensitive to Diet or Medication
Measurement
Caffeine kelim metabolism no yes blood
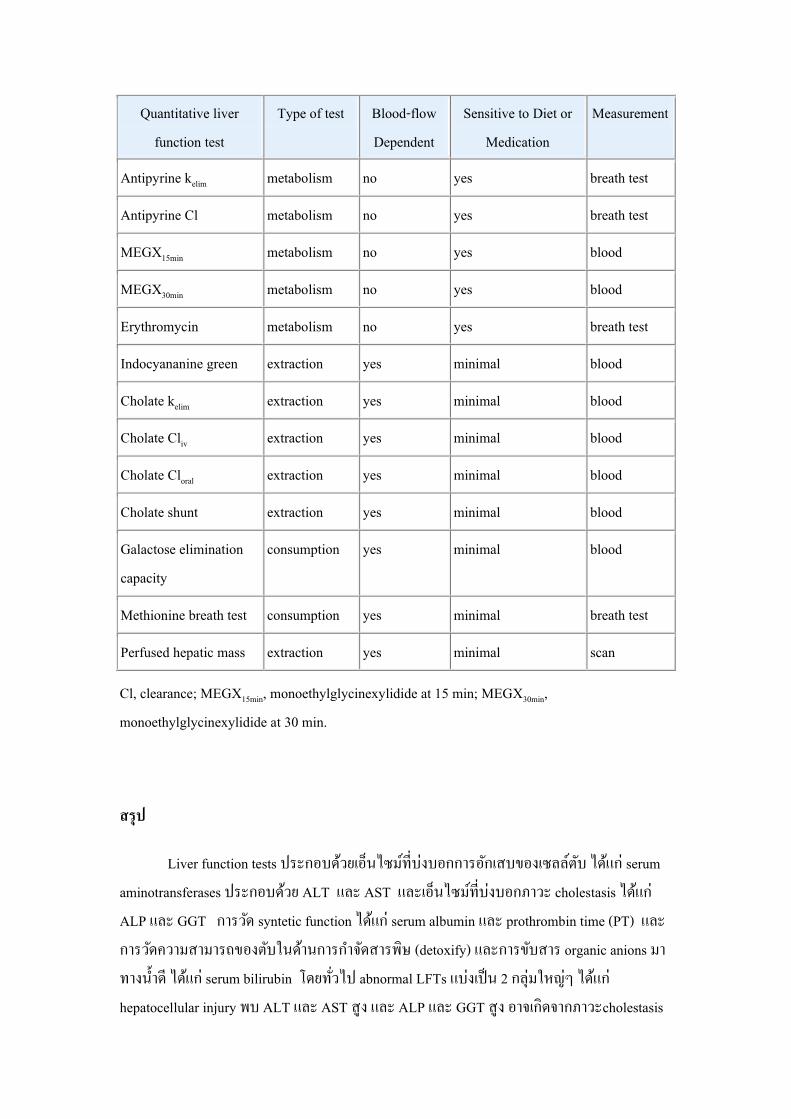
Quantitative liver function test
Type of test Blood-flow Dependent
Sensitive to Diet or Medication
Measurement
Antipyrine kelim metabolism no yes breath test
Antipyrine Cl metabolism no yes breath test
MEGX15min metabolism no yes blood
MEGX30min metabolism no yes blood
Erythromycin metabolism no yes breath test
Indocyananine green extraction yes minimal blood
Cholate kelim extraction yes minimal blood
Cholate Cliv extraction yes minimal blood
Cholate Cloral extraction yes minimal blood
Cholate shunt extraction yes minimal blood
Galactose elimination capacity
consumption yes minimal blood
Methionine breath test consumption yes minimal breath test
Perfused hepatic mass extraction yes minimal scan
Cl, clearance; MEGX15min, monoethylglycinexylidide at 15 min; MEGX30min, monoethylglycinexylidide at 30 min.
สรป
Liver function tests ประกอบดวยเอนไซมทบงบอกการอกเสบของเซลลตบ ไดแก serum aminotransferases ประกอบดวย ALT และ AST และเอนไซมทบงบอกภาวะ cholestasis ไดแก ALP และ GGT การวด syntetic function ไดแก serum albumin และ prothrombin time (PT) และการวดความสามารถของตบในดานการก าจดสารพษ (detoxify) และการขบสาร organic anions มาทางน าด ไดแก serum bilirubin โดยทวไป abnormal LFTs แบงเปน 2 กลมใหญๆ ไดแก hepatocellular injury พบ ALT และ AST สง และ ALP และ GGT สง อาจเกดจากภาวะcholestasis
กอนทตบหรอ infiltrative diseases ในการแปรผล LFTs ตองอาศยขอมลหลายอยางประกอบทงจากประวต การตรวจรางกาย อยางละเอยด การตรวจพเศษเพมเตม รวมทงการท า liver biopsy อาจชวยบอกสาเหตและความรนแรงของการอกเสบ และพงผดในตบได
เอกสารอางอง
1. Ahmed A., Keeffe EB. Liver Chemistry and Function Tests. In: Feldman M, Friedman LS, Brandt LJ, ed. Feldman: Sleisenger & Fordtran's Gastrointestinal and Liver Disease, 8th ed. Philadelphia: Saunders Elsevier, 2006:1575-86.
2. Green RM, Flamm S. AGA technical review on the evaluation of liver chemistry tests. Gastroenterology 2002;123:1367-84.
3. Giannini EG, Testa R, Savarino V. Liver enzyme alteration: a guide for clinicians. CMAJ. 2005 ;172:367-79.
4. Nathwani, RA, Pais, S, Reynolds, TB, Kaplowitz, N. Serum alanine aminotransferase in skeletal muscle diseases. Hepatology 2005; 41:380-2.
5. Kakumu S. Is mortality from liver disease associated with normal serum aminotransferase concentrations? Nat Clin Pract Gastroenterol Hepatol. 2004;1:22-3
6. Prati D, Taioli E, Zanella A, et al. Updated definitions of healthy ranges for serum alanine aminotransferase levels. Ann Intern Med. 2002 ;137:1-10
7. Fabrizi, F, Lunghi, G, Finazzi, S, et al. Decreased serum aminotransferase activity in patients with chronic renal failure: Impact on the detection of viral hepatitis. Am J Kidney Dis 2001; 38:1009-15.
8. Moussavian, SN, Becker, RC, Piepmeyer, JL, et al. Serum gamma-glutamyl transpeptidase and chronic alcoholism. Influence of alcohol ingestion and liver disease. Dig Dis Sci 1985; 30:211-4.
9. Keeffe EB, Sunderland MC, Gabourel JD: Serum gamma-glutamyl transpeptidase activity in patients receiving chronic phenytoin therapy. Dig Dis Sci 1986; 31:1056-61.
10. Czaja AJ. Autoimmune liver disease. Curr Opin Gastroenterol. 2008;24:298-305. 11. Hirschfield GM, Heathcote EJ. Primary biliary cirrhosis: the future. Clin Liver Dis.
2008;12:473-9.

12. Tripodi, A, Chantarangkul, V, Primignani, M, et al. The international normalized ratio calibrated for cirrhosis (INR(liver)) normalizes prothrombin time results for model for end-stage liver disease calculation. Hepatology 2007; 46:520-7.
13. Bellest, L, Eschwege, V, Poupon, R, et al. A modified international normalized ratio as an effective way of prothrombin time standardization in hepatology. Hepatology 2007; 46:528-34.
14. Kovacs MJ, Wong A, MacKinnon K, et al. Assessment of the validity of the INR system for patients with liver impairment. Thromb Haemost. 1994;71:727-30.
15. Pratt, DS, Kaplan, MM. Evaluation of abnormal liver-enzyme results in asymptomatic patients. N Engl J Med 2000; 342:1266-71.
16. Nyblom H, Berggren U, Balldin J, et al. High AST/ALT ratio may indicate advanced alcoholic liver disease rather than heavy drinking. Alcohol Alcohol 2004; 39:336-9.
17. Huang, MJ, Liaw, YF. Clinical associations between thyroid and liver diseases. J Gastroenterol Hepatol 1995; 10:344-50.
18. Saha, B, Maity, C. Alteration of serum enzymes in primary hypothyroidism. Clin Chem Lab Med 2002; 40:609-11.
19. Sorbi, D, McGill, DB, Thistle, JL, et al. An assessment of the role of liver biopsies in asymptomatic patients with chronic liver test abnormalities. Am J Gastroenterol 2000; 95:3206-10.
20. Comar KM, Sanyal AJ. Abnormal liver function tests. In: Weinstien WM, Hawkey CJ, Bosch J, eds. Cilnical gastroenterology and hepatology. 1st ed. Elsevier Mosby, 2005: 105-10.
21. Lee WM. Drug-induced hepatotoxicity. N Engl J Med 2003;349:474-85. 17. 22. Henrion, J, Schapira, M, Luwaert, R, et al. Hypoxic hepatitis: clinical and hemodynamic
study in 142 consecutive cases. Medicine (Baltimore) 2003; 82:392-406. 23. Seeto RK, Fenn B, Rockey DC. Ischemic hepatitis: clinical presentation and
pathogenesis. Am J Med 2000;109:109-13. 24. Kessler WR, Cummings OW, Eckert G, Chalasani N, Lumeng L, Kuo PY. Fulminant
hepatic failure as the initial presentation of acute autoimmune hepatitis. Clin Gastroenterol Hepatol 2004;2:625-31.
25. Shaver, WA, Bhatt, H, Combes, B. Low serum alkaline phosphatase activity in Wilson's disease. Hepatology 1986; 6:859-63.

26. Berman, DH, Leventhal, RI, Gavaler, JS, et al. Clinical differential of fulminant Wilsonian hepatitis from other causes of hepatic failure. Gastroenterology 1991; 100:1129-34.
27. Lok AS, McMahon BJ. Chronic hepatitis B. Hepatology. 2007;45:507-39 28. Asian Pacific Association for the Study of the Liver (APASL) Hepatitis C Working
Party, McCaughan GW, Omata M, Amarapurkar D, et al.Asian Pacific Association for the Study of the Liver consensus statements on the diagnosis, management and treatment of hepatitis C virus infection. J Gastroenterol Hepatol. 2007;22:615-33.
29. Khashab MA, Liangpunsakul S, Chalasani N. Nonalcoholic fatty liver disease as a component of the metabolic syndrome. Curr Gastroenterol Rep. 2008;10:73-80.
30. Roberts EA, Schilsky ML. A practice guideline on Wilson disease. Hepatology 2003;37:1475-92.
31. Ala A, Walker AP, Ashkan K, Dooley JS, Schilsky ML. Wilson's disease. Lancet 2007; 369: 397-408.
32. Dite P, Novotny I, Trna J, Sevcikova A. Autoimmune pancreatitis. Best Pract Res Clin Gastroenterol. 2008;22:131-43.
33. Czaja AJ. Autoimmune liver disease. Curr Opin Gastroenterol. 2008;24:298-305. 34. U.S. Preventive Services Task Force. Screening for hemochromatosis: recommendation
statement. Ann Intern Med. 2006;145:204-8. 35. Nathwani, RA, Kumar, SR, Reynolds, TB, Kaplowitz, N. Marked elevation in serum
transaminases: an atypical presentation of choledocholithiasis. Am J Gastroenterol 2005; 100:295-8.
36. Gopal DV, Rosen HR. Abnormal findings on liver function tests: interpreting results to narrow the diagnosis and establish a prognosis. Postgrad Med 2000;107:100-14
37. Kamath PS, Kim WR; Advanced Liver Disease Study Group.The model for end-stage liver disease (MELD). Hepatology. 2007;45:797-805.
38. Cholongitas, E, Marelli, L, Shusang, V, et al. A systematic review of the performance of the model for end-stage liver disease (MELD) in the setting of liver transplantation. Liver Transpl 2006; 12:1049-61.
39. Hoefs JC, Chen PT, Lizotte P. Noninvasive evaluation of liver disease severity. Clin Liver Dis. 2006;10:535-62
40. Fogden E, Neuberger J. Alternative medicines and the liver. Liver Int 2003; 23: 213-20



















