Pathophysiology of Hydrops Fetalis
10
Pathophysiology of Hydrops Fetalis Michael Apkon Hydrops fetalis occurs when the rate of interstitial fluid production by capillary ultrafiltration exceeds the rate of interstitial fluid return to the circulation via lymphatic vessels. Developmental differences in the microcirculation and lymphatic system of the fetus, as compared with mature subjects, renders the fetus susceptible to interstitial fluid accumulation. These differences include greater capillary permeability, more compliant interstitial compartment, and greater influence of venous pressures on lymphatic return. The balance between interstitial fluid production and removal is most commonly disrupted as a consequence of homeostatic mechanisms serving to preserve adequate systemic delivery of metabolic substrate when cardiocirculatory function is impaired. The pathophysiology of two conditions of impaired cardiocirculatory function, atrial tachycardia and severe anemia, serve as examples of the mechanisms by which these homeostatic mechanisms perturb the balance of interstitial fluid movement. Copyright 1995 by W.B. Saunders Company H ydrops fetalis, the excessive accumulation of interstitial fluid in the fetus, is a condi- tion that results in considerable rates of morbidity and mortality. The list of abnormalities associated with hydrops is protean, encompassing congenital malformations, infections, tumors, and acquired disorders. Although many disorders have a clear association with hydrops fetalis, in many cases, the actual cause of excessive fluid accumulation remains obscure. One might consider interstitial fluid to be a transudate of plasma, which, via lymphatic vessels, is eventually returned to the vascular space (Fig 1). Accordingly, hydrops may be considered a result of an imbalance between the rate of interstitial fluid formation and the rate at which this fluid is returned to the circu- lation. Thus, hydrops might result from any con- dition that accelerates the rate of transudation from the vascular space or delays the return of lymph to the circulation. This disrupted balance of fluid accumulation and clearance from the in- terstitial space may represent a primary distur- bance in the mechanisms governing fluid flux, as in the case of lymphatic malformations. More frequently, however, the balance of fluid move- ment is disrupted as a consequence of compen- satory mechanisms invoked by the fetus to pre- serve adequate delivery of oxygen and other vital suhstrates to the tissues in the face of impaired cardiocirculatory function. One approach in planning a rational diagnostic and therapeutic strategy in hydrops fetalis is to consider the pathophysiological basis of interstitial fluid ac- cumulation. Therefore, the author will develop a physiological framework to examine the factors governing fluid movement between the vascular and interstitial spaces and will explore, in partic- ular, the unique features of the fetal microcir- culation that facilitates fluid movement in utero. Additionally, the article discusses the compen- satory mechanisms that preserve adequate oxy- gen and nutrient delivery to the tissues at the expense of increased interstitial fluid accumu- lation. Finally, the pathophysiological mecha- nisms in two experimental models of hydrops fe- talis will be considered. Regulation of Fluid Movement Between Vascular and Interstitial Spaces Transcapillary Filtration The rate of interstitial fluid formation is deter- mined by the balance of forces governing water movement across the capillary endothelium, as originally described by Starling I (Fig 1). The driving forces for water extravasation from the vascular space is the hydrostatic pressure within the capillary (Pc) and the colloid oncotic pressure of the interstitial fluid (a'i). Similarly, the forces driving the return of water from the interstitial From the Division of Critical Care, Departmentof Yale University School of Medicine, New Haven, CT. Address reprint requeststo Michael Apkon, MD, PhD, Department of Pediatrics, Yale UniversitySchool of Medicine, PO Box 208064, New Haven, CT 06520-8064. Copyright 1995 by W.B. Saunders Company 0146-0005/95/1906-0009505.00/0 Seminars in Perinatology, Vol 19, No 6 (December), 1995: pp 437-446 437
-
Upload
drsunilpawar -
Category
Documents
-
view
434 -
download
2
Transcript of Pathophysiology of Hydrops Fetalis

Pathophysiology of Hydrops Fetalis Michael Apkon
Hydrops fetalis occurs when the rate of interstitial fluid production by capillary ultrafiltration exceeds the rate of interstitial fluid return to the circulation via lymphatic vessels. Developmental differences in the microcirculation and lymphatic system of the fetus, as compared with mature subjects, renders the fetus susceptible to interstitial fluid accumulation. These differences include greater capillary permeability, more compliant interstitial compartment, and greater influence of venous pressures on lymphatic return. The balance between interstitial fluid production and removal is most commonly disrupted as a consequence of homeostatic mechanisms serving to preserve adequate systemic delivery of metabolic substrate when cardiocirculatory function is impaired. The pathophysiology of two conditions of impaired cardiocirculatory function, atrial tachycardia and severe anemia, serve as examples of the mechanisms by which these homeostatic mechanisms perturb the balance of interstitial fluid movement. Copyright �9 1995 by W.B. Saunders Company
H ydrops fetalis, the excessive accumulation of interstitial fluid in the fetus, is a condi-
tion that results in considerable rates of morbidity and mortality. The list of abnormalities associated with hydrops is protean, encompassing congenital malformations, infections, tumors, and acquired disorders. Although many disorders have a clear association with hydrops fetalis, in many cases, the actual cause of excessive fluid accumulation remains obscure. One might consider interstitial fluid to be a transudate of plasma, which, via lymphatic vessels, is eventually returned to the vascular space (Fig 1). Accordingly, hydrops may be considered a result of an imbalance between the rate of interstitial fluid formation and the rate at which this fluid is returned to the circu- lation. Thus, hydrops might result from any con- dition that accelerates the rate of transudation from the vascular space or delays the return of lymph to the circulation. This disrupted balance of fluid accumulation and clearance from the in- terstitial space may represent a primary distur- bance in the mechanisms governing fluid flux, as in the case of lymphatic malformations. More frequently, however, the balance of fluid move- ment is disrupted as a consequence of compen- satory mechanisms invoked by the fetus to pre- serve adequate delivery of oxygen and other vital suhstrates to the tissues in the face of impaired cardiocirculatory function. One approach in planning a rational diagnostic and therapeutic strategy in hydrops fetalis is to consider the pathophysiological basis of interstitial fluid ac- cumulation. Therefore, the author will develop
a physiological framework to examine the factors governing fluid movement between the vascular and interstitial spaces and will explore, in partic- ular, the unique features of the fetal microcir- culation that facilitates fluid movement in utero. Additionally, the article discusses the compen- satory mechanisms that preserve adequate oxy- gen and nutrient delivery to the tissues at the expense of increased interstitial fluid accumu- lation. Finally, the pathophysiological mecha- nisms in two experimental models of hydrops fe- talis will be considered.
Regulat ion o f Fluid Movement Between Vascular and Interstitial Spaces
Transcapillary Filtration
The rate of interstitial fluid formation is deter- mined by the balance of forces governing water movement across the capillary endothelium, as originally described by Starling I (Fig 1). The driving forces for water extravasation from the vascular space is the hydrostatic pressure within the capillary (Pc) and the colloid oncotic pressure of the interstitial fluid (a'i). Similarly, the forces driving the return of water from the interstitial
From the Division of Critical Care, Department of Yale University School of Medicine, New Haven, CT. Address reprint requests to Michael Apkon, MD, PhD, Department of Pediatrics, Yale University School of Medicine, PO Box 208064, New Haven, CT 06520-8064. Copyright �9 1995 by W.B. Saunders Company 0146-0005/95/1906-0009505.00/0
Seminars in Perinatology, Vol 19, No 6 (December), 1995: pp 437-446 437

4 8 8 Michael Apkon
Artery O 0
0 0 0 0
0 O 0 0 r
Interstitium (Pi)
o o 0
Capillary (Pc)
Vein L
o 000 ~176 o o
o
Oo~C ~176 o o
Lymphatic
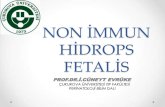
Figure 1. Interstitial fluid balance. Interstitial fluid is formed by ultrafiltration of plasma at the capillary. Capillary ultrafiltration is driven by the difference between capillary (Pc) and interstitial (Pi) hydrostatic pressures. Fluid reabsorption by the capillary is driven by the difference between the capillary 0re) and interstitial (Tri) colloid oncotic pressures, measures of the concentrations of oncotically active molecules, or, the reflection coefficient, and Lp, the hydraulic permeability, are intrinsic properties of the capillary wall that characterize the efficacy of such driving forces to produce water flux (.Iv). Interstitial fluid is returned to the circulation via the lymphatic system. The outflow pressure of the lymphatic pressure is the venous pressure. The "manometers" indicate the relative pressures in each compartment.
space to the intravascular space is the hydrostatic pressure of the intersti t ium (Pi) and the plasma colloid oncotic pressure (a'D. The colloid oncotic pressure in the vascular and interstitial spaces depends on the concentra t ion of osmotically ac- tive particles in the compar tment , and the efficacy with which oncotic pressure differences influence water movement depends on the extent to which movement of osmotically active molecules across the capillary is restricted (as described by ~, the colloid osmotic reflection coefficient). The less permeable the endothel ium is to a particular molecule (ie, the higher the tr), the greater the effect o f colloid oncotic pressure differences. A corollary of this relation is that a more permeable endothel ium will allow a grea ter solute flux to accompany, via solvent drag, water movement . The net rate of fluid movement depends on the capillary surface area and its hydraulic conduc- tivity (Lp). The produc t o f capillary surface area and hydraulic conductivity, re fe r red to as the capillary filtration coefficient (CFC) provides a measure of units o f volume translocated per unit time per millimeters of mercury driving force. Thus, Jv, the fluid flux across the capillary, may be described by the following equation:
Jv = CFC(Ap - ~A~r)
where Ap is the net hydrostatic pressure gradient (Pc - Pi) and ATr is the colloid osmotic pressure gradient between the capillary and interstitial fluid (Trc - 7ri).
Several features of the fetal microcirculation may facilitate transcapillary water movement compared with adult subjects. 2 First, fetal cap- illaries appear to be more permeable to plasma proteins, resulting in a lower reflection coeffi- cient for oncotically active solute. The effect of this enhanced solute permeabili ty is that for any given solute concentrat ion difference across the capillary endothel ium, the colloid oncotic pres- sure difference will drive water less effectively f rom the interstitium to the vascular space. Thus, transcapillary flux and the distribution of body water will be less sensitive to alterations in plasma or interstitial colloid osmotic pressure. This, in part, explains the finding that plasma prote in re- duction in chronically ins t rumented fetal sheep does not affect body water content. 3 Second, the capillary filtration coefficient is fivefold higher than that of adults. The increased capillary fil- tration coefficient in the fetus results in an in-

Pathophysiology of Hydrops 4 3 9
creased water flux for a given driving force. Third, the interstitial space of the fetus is more compliant than that of more mature subjects. That is to say, that the interstitial space of the fetus is capable of receiving a greater amount o f fluid with a smaller increase in the interstitial hy- drostatic pressure. Because it is the interstitial hydrostatic pressure that opposes the capillary hydrostatic pressure and drives water f rom the capillary, a given increase in capillary hydrostatic pressure may result in greater interstitial fluid accumulation before it is checked by a corre- sponding increase in interstitial hydrostatic pres- sure.
In the short term, facilitated transcapillary flow has important consequences in blood vol- ume regulation. For example, transcapillary flow from the interstitium is likely an import mecha- nism restoring blood volume after acute hem- orrhage. MeUander and others 4'5 have shown that in adult cats, acute hemorrhage induces altera- tions in microcirculatory pressures, which results in reabsorption rather than filtration by the cap- illaries. This "autotransfusion" probably con- tributes to restoring the blood volume and preserving cardiac output. In adult sheep, res- toration of full blood volume after a 30% hem- orrhage requires 24 to 48 hours. 6 In contrast, full blood volume of fetal sheep is restored over 3 to 4 hours. 7 The more rapid recovery of blood volume in the fetal subjects is consistent with a greater capillary filtration coefficient and a greater interstitial compliance. Similarly, facili- tated transcapillary flow contributes to blood volume regulation during blood volume expan- sion. For example, saline infusion results in blood volume expansion. However, this expansion is transient as fluid redistributes across the capil- lary. In adult sheep, 30% of administered saline remains in the vascular space 30 minutes after infusion. In fetal sheep, in contrast, only 6% of the infused saline remains in the vascular space, s This suggests that for a given amount of fluid added to or retained by the fetus, a smaller frac- tion will reside in the vascular space and a larger fraction will reside in the interstitial space.
Lymphatic Return
Enhanced capillary filtration of water to the in- terstitial space predicts that lymphatic flow in the fetus must be increased also. Indeed, Brace et al 9A~ have shown that the thoracic duct lymph
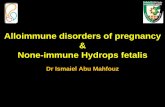
flow (normalized for body mass) in fetal sheep is four to five times greater than those o f adult sheep. In addition to differences in lymphatic ca- pacity between fetal and mature subjects, there are differences in the regulation of lymphatic flow. For example, lymphatic flow rates depend on the outflow pressure for the lymphatic system, which is the venous pressure (Fig 2). In mature subjects, lymphatic flow is relatively constant until the outflow pressure increases to approximately 8 mm Hg. At greater pressures, lymphatic flow falls and eventually ceases when the outflow pressure nears 25 mm Hg. In contrast, fetal lym- phatic flow begins to decrease when the outflow pressure is greater than 0 mm Hg and ceases when the outflow nears 10 mm Hg. Because the normal fetal central venous pressure is typically greater than 0 mm Hg, basal lymph flow is limited in the normal fetus and is expected to be limited fur ther whenever central venous pressure in- creases. The factors governing lymphatic flow through abnormal lymphatic structures are more poorly understood.
Circulatory Failure as a Cause o f Hydrops
Although increases in capillary permeability, de- creases in plasma colloid oncotic pressure, and impaired lymphatic function may each contribute to interstitial fluid accumulation in the hydropic fetus, circulatory dysfunction with associated in- creases in venous pressures may be a more com- mon mechanism causing noninunune hydrops. ~ ~~ 4 Elevation in venous pressure is a manifestation of several of the normal homeostatic mechanisms that preserve organ perfusion in the face of a critical imbalance between the supply and de- mand for oxygen and other vital nutrients. An understanding of the pathophysiology of hydrops under such conditions of supply-demand imbal- ance requires examination o f the determinants o f substrate delivery to the tissues as well as an understanding of the homeostatic mechanisms contributing to elevations o f venous pressures.
Circulatory Failure as an Imbalance Between Substrate Supply and Metabolic Demand
Adequate delivery of metabolic substrate to the tissues depends not only on the overall cardiac output , the concentrat ion o f substrate within the

4 4 0 Michael Apkon
A
, r
.c:_ E
E
t~
0
Q. E
._1
0.31 , , ,
iiiiiiiiiiiii!iiiiiiiiiiiiiiiiiiiiiiiiiiiiiiii !
0.2
0.1
0 k- -20
. 0 ~ 1 7 6 . . . . . . . . . . . . . . . . . . . . . .
iiiiiii!i!iiiiii iiiiiiii!!i ili
. . . . . . . . . . . ~ 1 7 6 , . . . - . . . . . . . . - . . . . . . . . . . . ,
i I [ l I I I [
Fetal
Adult
/ -10 0 10 20
Outflow pressure (mmHg)
30 40
Figure 2. Left thoracic duct lymph-flow in ovine fetus and adult. Measure- ments were made in animals with chronically implanted lymphatic and vascular catheters. The normal lym- phatic outflow pressure is the central venous pressure which is typically 3 to 4 mm Hg in the ovine fetus. Data are mean -+2 X SE. (Re- printed with permission. 2)
blood and the appropriateness of the distribution of blood flow among various organs, but also on the metabolic demands of the tissue. Table 1 lists examples of clinical conditions that have been associated with nonimmune hydrops and that may decrease cardiac output or increase the de- mand for blood flow. Conditions are grouped according to the primary mechanism by which supply-demand imbalance occurs. Recall that
cardiac output is the product of heart rate and stroke volume. Furthermore, stroke volume is determined by the degree of cardiac filling (ie, the end diastolic volume) and the effectiveness of contraction (ie, the ejection fraction). Thus deficiencies in heart rate, cardiac filling, or con- tractile function could impair cardiac output.
Impairment of cardiac filling may result from an inadequate intravascular volume, an impedi-
Table 1. Causes of Supply-Demand Imbalance for Metabolic Substrate Delivery
Disturbance Mechanism Examples
Decreased cardiac output
Increased demand for flow
Inadequate cardiac filling
Inadequate or impeded ejection
Inadequate heart rate Decreased oxygen content Maldistribution of flow Increased metabolic rate
Decreased ventricular compliance, pericardial effusion, tachyarrythmias, hemorrhage, hepatitis or peritonitis causing extravasation of fluid from vascular space
Myocarditis, myocardial infarction, asphyxia, polycythemia, premature closure of the ductus arteriosus, valve dysfunction
Congenital heart block Anemia, bypoxemia Arteriovenous malfornaation Thyrotoxicosis
Modified with permission) 8

Pathophysiology of Hydrops 441
ment to venous return, or to a decrease in ven- tricular compliance. A relative deficiency in in- travascular volume may exist as a consequence of either fluid loss f rom the vascular space or from an increase in vascular capacity. Fluid may be lost f rom the vascular space to the interstitial space if capillary filtration increases as a result of either an increase in capillary permeability or a decrease in plasma colloid oncotic pressure as discussed previously. Alternatively, blood may be lost f rom the vascular space as a result of fetal- maternal or twin-twin transfusion. Fur thermore , fetal hemorrhage (ie, intracranial hemorrhage) causes blood loss f rom the vascular space.
Even when intravascular volume is normal, cardiac filling will be diminished if venous return is impeded. Pericardial effusions, cardiac tumors, and subendocardial fibroelastosis each decrease the effective ventricular compliance, resulting in a smaller end diastolic ventricular volume for a given venous pressure. Tachyarrhythmias also impart an impediment to cardiac filling by lim- iting the duration of diastole.
Given adequate cardiac filling, ejection of blood may be impaired by depressed cardiac muscle function as may occur f rom in utero myocarditis, myocardial infarction or hypoxemia. Moreover, ejection may be impaired when ven- tricular outflow is impeded. Thus, valvular mal- formations such as calcified aortic valve or ab- normalities of the puimonic valve compromise the ability of the ventricle to eject. Premature closure of the ductus arteriosus might also be expected to compromise right ventricular ejec- tion by forcing the total right ventricular output to be ejected through the high vascular resistance of the fetal pulmonary circulation. In fetal lambs, acute ductal occlusion caused a decrease in right ventricular output (RV), increases in RV systolic and diastolic dimensions, and tricuspid valve re- gurgitation) 5 Interestingly, premature closure of the foramen ovale may also create a relative de- ficiency in RV function by necessitating that the RV discharge the total systemic venous re turn as right to left transatrial flow is b locked) 6
Decreases in the concentrat ion of metabolic substrate, particularly oxygen, in the blood cre- ates a requirement for more blood flow to pro- vide a constant amount of substrate delivery. Thus, decreases in hemoglobin concentrat ion or in hemoglobin saturation result in less oxygen delivery per unit of blood and hence a demand
for increased flow. Maldistribution of blood flow, as might occur in the presence of an arteriove- nous malformation, also creates a need for in- creased total blood flow because a port ion of the total cardiac output is distributed to provide ex- cessive flow to some tissues at the expense o f flow to o ther tissues. Finally, increases in meta- bolic rate, as may occur in metabolic disturbances such as thyrotoxicosis, must be met by increases in substrate delivery.
In the fetus as well as the mature subject, a number of homeostatic responses are activated locally and systemically by inadequate cardiac output. 17.18 In addition to their beneficial effects, these compensatory mechanisms may also be maladaptive in so far as they contr ibute to fluid retent ion by the fetus and extravasation o f fluid from the vascular space, thereby contributing to the development of hydrops.
Compensatory Mechanisms
Local and systemic cardiovascular regulation preserves homeostasis via three mechanisms. First, local mechanisms enhance the efficiency of oxygen extraction and use by the tissues. Second, systemic and local mechanisms act together to redistribute blood flow to more metabolically ac- tive organs such as the brain and heart. Third, systemic mechanisms act to enhance cardiac out- put by augmenting blood volume and myocardial performance.
Local mechanisms enhance the efficiency o f oxygen extraction in part by recruiting previously closed capillaries. 19 In adult subjects, capillary recrui tment allows enhanced oxygen extraction by increasing surface area for oxygen diffusion, by decreasing the distance between the capillary and tissue, and by increasing the transit time o f blood cells within the tissues. It is not known to what extent the capillary bed of the fetus is fully recruited at rest or if capillary recrui tment is an important homeostatic mechanism during de- velopment.
At times o f insufficient cardiac output for metabolic demands, flow is redistributed by a combination o f local and systemic mechanisms. Many organs are able to locally regulate their blood flow by varying the resistance of the con- ducting vessels. This regulation occurs as a result of metabolic feedback from the tissues to the conducting vessels and by direct effects of per- fusion pressure and blood flow on the blood ves-

442 Michael Apkon
sels themselves. As organs differ in their ability to regulate flow in this manner , local mechanisms will serve to redistribute blood flow to those or- gans with more potent autoregulat ion. Systemic mechanisms involving neural and humeral factors also serve to redistr ibute b lood flow. Specifically, stimulation of the sympathetic nervous system via activation of low pressure atrial stretch re- ceptors and arterial ba rorecep tors results in pe- r ipheral vasoconstriction. Similarly, plasma con- centrations of vasopressin, angiotensin II , and other neuroendocr ine factors are increased and cause arteriolar constriction. As vascular beds differ in their sensitivity to sympathetic stimula- tion, blood flow is redistr ibuted to those tissues with a lower sensitivity such as the heart and brain. In chronically ins t rumented fetal sheep, it has been possible to show that these mechanisms function during gestation. The ba ro recep to r re- flex, for example, a measure of autonomic ner- vous system function, is active throughout the second half of gestation, 2~ although the sensitivity of the reflex to changes in mean arterial blood pressure seems to increase with age. I t is also possible to show increases in fetal plasma con- centrations of no rep inephr ine , renin, and vaso- pressin in response to circulatory stress such as hemorrhage. 7'21 That these mechanisms are im- por tan t to cardiovascular homeostasis is sup- por ted by the finding that blockade of angioten- sin I I (whose formation is stimulated by increased plasma renin activity) or vasopressin activity magnifies the decrease in fetal mean arterial pressure that occurs with hemorrhage . 22 The net effect o f these regulatory mechanisms in the fetus is that during times of circulatory stress such as hypoxia or hemorrhage , b lood flow and oxygen delivery to the brain, heart , and adrenal glands are preserved at the expense of that to the kidney, gut, and m u s c l e . 23'24
The same systemic mechanisms that serve to redistribute flow also act to enhance cardiac out- put by augmenting blood volume and myocardial performance. For example, renal arteriolar va- soconstriction decreases renal perfusion. How- ever, glomerular filtration may be maintained by selective constriction of the efferent arteriole. 25 The kidney responds to this decrease in perfusion by increasing the proximal reabsorpt ion o f the glomerular filtrate. Additionally, vasopressin acts to increase water reabsorpt ion and angiotensin I I stimulates aldosterone release f rom the adrenal
cortex, which in turn promotes sodium reab- sorption. The effect o f these responses is that fluid is re tained by the kidneys, in p a r t aug- ment ing the circulating blood volume.
Blood volume may also be augmented if trans- capillary hydrostatic forces are altered to favor fluid reabsorpt ion f rom the interstitium. Mean capillary pressure could decrease as a direct result o f decreases in arterial or venous pressures. Al- ternatively, mean capillary pressure could de- crease even though arterial pressure is increased if the arterial pressure is dissipated by arteriolar constriction, as occurs with sympathetic nervous system stimulation. I t is likely that enhancement in transcapillary reabsorpt ion by these mecha- nisms contributes to the restoration of fetal blood volume af ter a c u t e hemorrhage . 26"27
Increases in blood volume result in increases in myocardial filling as blood is distributed among different compar tments (ie, arteries, capillaries, veins, and cardiac chambers) according to the relative compliance and capacitance of each compar tment . Even if blood volume is not in- creased, myocardial filling can be increased by redistributing blood a m o n g these various com- partments. The venous system has a large capac- itance that is regulated by the sympathetic ner- vous system. Increases in sympathetic tone cause venoconstriction, which increases venous pres- sures and redistributes blood f rom the veins to the heart. Such increases in fetal venous pressure have been shown dur ing circulatory stress such as hypoxia. 2s
Increases in myocardial filling are translated to increases in cardiac output because of the Frank- Starling mechanism, 29 which relates changes in end-diastolic fiber length to changes in stroke volume. The te rm preload reserve has been used to describe the augmentat ion in cardiac output that may be obtained with increases in myocardial filling. In the fetal lamb, as in the adult, increases in mean atrial pressure or end-diastolic pressure result in increases in right and left ventricular output 3~ (Fig 3). However, the increase in ven- tricular ou tput for a given increase in filling pressure is substantially diminished at filling pressures grea ter than approximately 3 to 8 m m Hg. Whether or not the Frank-Starling mecha- nism provides preload reserve in the fetus de- pends on the normal mean atrial pressure relative to this inflection point in the output-pressure re- lationship. I t appears, at least in fetal lambs, that

Pathophysiology of Hydrops 4 4 3
1.5
Figure 3. Ventricular stroke volume as a function of mean atrial pressure. These com- posite left (LV) and fight ventricular (RV) function curves measured in ovine fetuses were obtained by measuring stroke volumes during rapid blood rein- fusion after phlebotomy. Lines represent the "best fits" to the rising and pla- teau segments of the curve. (Reprinted with permission? ~)
e j
I
o., // /
i t t
0
. . - - - - - RV
_._...-- LV
i I J * i i I i * * , I
5 10 15 Mean atrial pressure (torr)
normal mean atrial pressures are sufficiently high that preload reserve is limited.
Maladaptive Effects of Compensatory Mechanisms
Although the compensa tory mechanisms dis- cussed previously preserve balance between substrate supply and demand, at least in the most metabolically active tissues, homeostasis occurs at the expense o f increased venous pressures, impaired organ funct ion, and ulti- mately interstitial fluid accumulat ion. Eleva- tion in venous pressures has been shown in human I~'s~ and lamb s436 fetuses with hydrops secondary to impaired circulatory funct ion. Increases in venous pressure may con t r ibu te to interstitial fluid accumulat ion by two mecha- nisms, as discussed previously: (1) increasing the mean capillary hydrostat ic pressure, caus- ing increased capillary fi l tration and, (2) in- creasing the outflow pressure for lymphatic re turn , causing a decrease in lymphatic flow. Even if venous pressures are not increased, mean capillary pressures can be increased as a result of local and systemic compensa to ry mechanisms for insufficient circulation. For example, precapil lary vasodilation could ele- vate mean capillary pressure by be t t e r trans- mitting arteriolar pressure to the capillaries and could recrui t previously closed capillaries, cont r ibut ing to an increase in capillary filtra-
t ion surface area. Increases in venous resis- tance that are p ropor t iona te ly grea ter than in- creases in ar ter iolar resistance will also increase mean capillary pressure. These increases in mean capillary pressure are maladaptive in that they result in extravasat ion o f fluid f rom the vascular space and interstitial fluid deposi t ion. Such decreases in b lood volume have been shown exper imenta l ly in fetal lambs dur ing cir- culatory stress such as occurs in fetal hyp- oxia.2S, s7
In addition to alterations in hydrostatic pres- sure, colloid oncotic pressure has also been sug- gested to be altered as a consequence of circu- latory compromise. In adults, for example, venous congestion and decreased hepatic per- fusion have been suggested to impair synthesis of albumin, ss the predominant oncotically active plasma protein. Moreover, hepatic synthetic function may be fur ther reduced by increased extramedullary hematopoeisis in response to chronic fetal hypoxia.
Increases in capillary permeabi l i ty could also contr ibute to increased transcapillary fluid movement at times o f c i rcula tory compromise . Capillary permeabil i ty may increase as a result o f hypoxia- induced endothel ia l injury. Alter- natively, capillary permeabil i ty may be modu- lated by circulat ing n e u r o h o r m o n a l factors re- leased via homeosta t ic mechanisms or by the host defense against infection. For example,

4 4 4 Michael Apkon
atrial natr iuret ic factor, released in response to atrial distension, may directly increase cap- illary permeabili ty. 39
Experimental Models of Hydrops Fetalis
Atrial Tachycardia
Recogni t ion o f in t rau ter ine supraventr icular tachycardia as a cause of nonimmune hydrops suggested that hydrops might be c rea ted in ex- perimental subjects by atrial pacing. Stevens et al 4~ adapted the chronically instrumented fetal lamb preparat ion to electrically pace the left atrium for prolonged periods of time. Atrial pac- ing at 300 bpm resulted in evidence of fluid ac- cumulation in all animals studied: 1 of 13 study animals developed massive edema (hydrops)~ Ev- idence of fluid accumulation was not observed in a set o f control animals that did not receive atrial pacing.
It is likely that these pathological changes re- sult f rom the decrease in cardiac output that ac- companies rapid atrial pacing. In this regard, it is important to distinguish between the conse- quences o f abnormal rhythms with rapid atrial rates, and the consequences o f tachycardia per se. Anderson et al have distinguished between the effects of sinus tachycardia and rapid atrial pacing in chronically catheterized fetal lambs. 41'42 In fetal lambs, increases in spontaneous heart rate were accompanied by increases in right ven- tricular end-diastolic dimension and output at a constant stroke volume, but decreases in left ventricular end-diastolic dimension and stroke volume; left ventricular output also increased. However, when the heart rate was increased by atrial pacing, a decrease in stroke volume and end-diastolic dimension was observed for both ventricles. Interestingly, ventricular output only decreased significantly in the ventricle ipsilateral to the paced atrium. The alterations in myocar- dial filling appear to result f rom an inadequate diastolic intervalbecause the rate-related changes were reversed during test beats introduced at longer interbeat intervals. One reason tha t the cardiac output is bet ter preserved during spon- taneous tachycardia is because the mechanisms that normally accelerate the heart beat, such as the sympathetic nervous system, also augment cardiac filling (by increasing venomotor tone) and the force o f contraction.
Given the decrease in cardiac output during pacing, it is not surprising that the arterial Po~ decreases somewhat f rom approximately 18 to 15 mm Hg. Decreases in arterial Po2 were not observed in similar experiments by Gest et a lY It seems unlikely that this modest degree of hyp- oxia resulted in increases in capillary permeability because plasma protein, albumin, and Na § con- centrations do not change significantly with pac- ing. Gest et a135 measured the turnover rate of radiolabeled albumin in the plasma and found no evidence for increased capillary permeability.
Stevens et al 4~ found that the histopathology of those fetuses who had received atrial pacing suggested that edema formation is a result of ve- nous congestion: many animals had cardiomegaly or hepatomegaly. Elevations in inferior vena cava pressure were showed directly in the study by Gest et al. 35 Interestingly, the increase in venous pressures does not necessarily reflect an increase in total blood volume. Plasma volume may ac- tually decrease somewhat with a constant red blood cell volume. This suggests that the com- pensatory mechanisms preserving tissue perfu- sion during tachycardia redistribute the blood between the various vascular spaces and redis- tribute fluid f rom the vascular to the interstitial space. Furthermore, increases in venous pressure must reflect increases in venomotor tone and de- creased venous compliance. This does not mean that fluid accumulation by the fetus does not take place. Rather, it suggests that if fluid retention occurs it is poorly effective at increasing blood volume and restoring circulatory function.
The elevation in venous pressure contributes to edema not only by forcing fluid from the vas- cular space, but also by impeding the re turn of fluid via the lymphatics. Gest et a143 found that if the thoracic duct lymph flow in fetal lambs was collected against a pressure equal to the baseline central venous pressure, then electrically induced tachycardia caused a 50% increase in lymph flow. If, however, the lymph flow outlet pressure was increased to a pressure equal to the venous pres- sures measured during atrial pacing, then lymph flow decreased to baseline rates. Thus it appears that in tachyarrhythmia-induced hydrops, edema formation results from (1) increases in microcir- culatory pressure resulting f rom increased ven- omotor tone a n d / o r decreased ventricular com- pliance, and (2) impairment o f lymphatic flow resulting f rom increased venous pressure. Inter-

Pathophysiology of Hydrops 4 4 5
estingly, electrically induced tachycardia is par- ticularly well suited for examining the time course for the development and reversal of hydrops, be- cause the circulatory disturbance can be initiated and terminated instantaneously. Hydrops ap- pears to develop within several hours to a few days after initiating pacing, and many o f the cir- culatory disturbances are rapidly reversible after returning to sinus rhythm. 34's6
Anemia
Anemia as a result of alloimmunization, hemor- rhage, or red blood cell dyscrasia is a common cause of hydrops. Recently, Blair et al have suc- cessfully produced anemia-associated hydrops in fetal lambs by partial exchange transfusion. 44 This experimental model is beginning to provide im- portant insight into the pathogenesis of fluid ac- cumulation during anemia. As in electrically in- duced tachycardia, hydrops in anemia seems to be associated with an increase in venous pressure. Plasma colloid oncotic pressure increased some- what in all the anemic animals, suggesting that extravasation of fluid from the vascular space oc- curs in anemia as well as in electrically induced tachycardia. It is unlikely that these alterations in oncotic forces contribute to water accumula- tion in anemia, however, because the observed increase in plasma oncotic pressure would be ex- pected to impede water loss to the interstitium. Interestingly, the likelihood o f developing hy- drops was related to the rapidity with which ane- mia was produced.
S u m n l a l ~
Interstitial fluid accumulates in the fetus when- ever the rate of fluid extravasation f rom the vas- cular space is greater that the rate at which fluid is re turned to the venous system by the lym- phatics. The fetus is particularly susceptible to such interstitial fluid accumulation by virtue of developmental differences that facilitate fluid extravasation and cause lymphatic re turn to be more potently influenced by lymphatic outflow pressure. The delicate balance between fluid en- try and egress from the interstitium can be easily upset as a result of normal homeostatic mecha- nisms that preserve organ nourishment in the face of circulatory insufficiency. Given the num- ber of independent parameters that determine
the rates o f transcapillary fluid movement, it is not surprising that hydrops is a common conse- quence of many different disease processes. Even if one considers hydrops to be most commonly a consequence of circulatory insufficiency, the specific entities leading to circulatory compro- mise are numerous. Understanding the physiol- ogy of interstitial fluid accumulation and the pathophysiology o f specific diseases aids in the advancement of diagnostic and therapeutic ap- proaches to prenatal care. The challenge o f fu- ture investigations is to develop therapeutic strategies aimed not only at reversing the under- lying disease, but also to ameliorate the conse- quences o f interstitial fluid accumulation.
References
1. Starling EH: On the absorption of fluids from the con- nective tissue spaces. J Physiol 19:312-326, 1896
2. Brace RA: Fluid distribution in the fetus and neonate, in Polin RA, Fox WW (eds): Fetal and Neonatal Physi- ology. Philadelphia, PA, Saunders, 1992, pp 1288-1298
3. Moise AA, Gest AI,, Weickmann PH, et al: Reduction in plasma protein does not affect body water content in fetal sheep. Pediatr Res 29:623-626, 1991
4. Mellander S and Lewis DH: Effect of hemorrhagic shock on the reactivity of resistance and capacitance vessels and on capillary filtration transfer in cat skeletal muscle. Circ Res 13:105-118, 1963
5. Maspers M, BjornbergJ, Grande P-O, et al: Sympathetic alpha-adrenergic control of large-bore arterial vessels, arterioles and veins, and of capillary pressure and fluid exchange in whole-organ cat skeletal muscle. Acta Physiol Scand 138:509-521, 1990
6. GrimesJM, Buss LA, Brace RA: Blood volume restitution after hemorrhage in adult sheep. AmJ Physio1253:R541- 544, 1987
7. Brace RA, Cheung CY: Fetal cardiovascular and endo- crine responses to prolonged fetal hemorrhage. Am J Physiol 251 :R417-424, 1986
8. Brace RA: Fetal blood volume responses to intravenous saline solution and dextran. Am J Obstet Gynecol 147: 777-781, 1983
9. Brace RA, Valenzuela GJ: Effects of outflow pressure and vascular volume loading on thoracic duct lymph flow in adult sheep. Am J Physiol 258:R240-244, 1990
10. Brace RA: Effects of outflow pressure on fetal lymph flow. Am J Obstet Gynecol 160:4944497, 1989
11. Kleinman CS, Donnerstein RL, De Vore GR, et al: Fetal echocariography for evaluation of in utero congestive heart failure: A techniques for study of nonimmune hy- drops. N EnglJ Med 306:568-575, 1982
12. Weiner CP: Umbilical pressure measurement in the eval- uation of nonimmune hydrops fetalis. Am J Obstet Gy- necol 168:817-823, 1993
13. Allan LD, Crawford DC, Sheridan R, et al: Aetiology of non-immune hydrops: The value of echocardiography. BrJ Obstet Gynaecol 93:223-225, 1986

446 Michael Apkon
14. Holzgreve W, Curry CJR, Golbus MS, et al: Investigation of nonimmune hydrops fetalis. AmJ Obstet Gyneco1150: 805-812, 1984
15. Tulzer G, Gudmundsson S, Rotondo KM, et al: Acute fetal ductal occlusion in lambs. Am J Obstet Gynecol 165:775-778, 1991
I6. Coulson CC, KullerJA: Nonimmune hydrops fetalis sec- ondary to premature closure of the foramen ovale. Am J Perinatol 11:439-440, 1994
17. Morin FC, Weiss KI: Response of the fetal circulation to stress, in Polin RA, Fox WW (eds): Fetal and Neonatal Physiology, Philadelphia, PA, Saunders, 1992, pp 620- 628
18. Lister G, Apkon M, Fahey JT: Shock, in Emmanoulides TA, Riemenschneider TA, Allen HD, Gutgesell HP (eds): Heart Disease in Infants, Children, and Adolescents, ed 5. Baltimore, MD, Williams and Wilkins, 1994, pp 1725- 1746
19. Duling BR, Klitzman B: Local control of microvascular function: Role in tissue oxygen supply. Annu Rev Physiol 42:373-382, 1980
20. Shinebourne EA, Vapaavuori EK, Williams RL, et al: De- velopment of baroreflex activity in unanesthetized fetal and neonatal lambs. Circ Res 31:710-718, 1972
21. Brace RA, Cheung CY: Fetal blood volume restoration following rapid fetal hemorrhage. Am J Physiol 259: H567-573, 1990
22. Iwamoto HS, Rudolph AM: Role of renin-angiotensin system in response to hemorrhage in fetal sheep. Am J Physiol 240:H848-854, 1981
23. Cohn HE, Sacks EJ, Heymann MA, et al: Cardiovascular responses to hypoxemia and acidemia in fetal lambs. Am J Obstet Gynecol 120:817-824, 1974
24. ItskovitzJ, Goetzman BW, Rudolph AM: Effects of hem- orrhage on umbilical venous return and oxygen delivery in fetal lambs. AmJ Physiol 242:H543-548, 1982
25. RobillardJE, Weitzman RE, Burmeister L, et al: Devel- opmental aspects of the renal response to hypoxia in the lamb fetus. Circ Res 48:128-138, 1981
26. Brace RA: Fetal blood volume responses to acute fetal hemorrhage. Circ Res 52:730-734, 1983
27. Brace RA: Fetal blood volume responses to fetal hae- morrhage: Autonomic nervous contribution. J Dev Physiol 9:97-103, 1987
28. Brace RA, Cheung CY: Role of catecholamines in me-
diating fetal blood volume decrease during acute hypoxia. AmJ Physiol 253:H927-932, 1987
29. Frank O: On the dynamics of cardiac muscle. Am Heart J 58:467-478, 1959
30. Kirkpatrick SE, Pitlick PT, NaliboffJ, et al: Frank-Starling relationship as an important determinant of fetal cardiac output. AmJ Physiol 231:495-500, 1976
31. Gilbert RD: Control of fetal cardiac output during changes in blood volume. AmJ Physio1238:H80-86, 1980
32. Relier MD, Morton MJ, Reid DL, et al: Fetal lamb ven- tricles respond differently to filling and arterial pressures and to in utero ventilation. Pediatr Res 22:621-626, 1987
33. Johnson P, Sharland G, Allan LD, et al: Umbilical venous pressure in nonimmune hydrops fetalis: Correlation with cardiac size. Am J Obstet Gynecol 167:1309-1313, 1992
34. Nimrod C, Davies D, Harder J, et al: Ultrasound evalu- ation of tachycardia-induced hydrops in the fetal lamb. AmJ Obstet Gynecol 157:655-659, 1987
35. Gest AL, Hansen TN, Moise AA, et al: Atrial tachycardia causes hydro ps in fetal lambs. Am J Physiol 258:H 1159- 1163, 1990
36. Gest AL, Martin CG, Moise AA, et al: Reversal of venous blood flow with atrial tachycardia and hydrops in fetal sheep. Pediatr Res 28:223-226, 1990
37. Brace RA: Fetal blood volume responses to acute fetal hypoxia. AmJ Obstet Gynecol 155:889-893, 1986
38. Dunn GD, Hayes P, Breen KJ, et al: The liver in congestive hear failure: A review. AmJ Med Sci 265:174-189, 1973
39. ValentinJ-P, RibsteinJ, Mimran A: Effect ofnicardipine and atriopeptin on transcapillary shift of fluid and pro- teins. AmJ Physiol 257:R174-179, 1989
40. Stevens DC, Hilliard JK, Schreiner RL, et al: Supraven- tricular tachycardia with edema, ascites, and hydrops in fetal sheep. Am J Obstet Gynecol 142:316-322, 1982
41. Anderson PAW, Killman AP, Mainwaring RD, et al: In utero right ventricular output in the fetal lamb: The effect of heart rate. J Physiol 387:297-316, 1987
42. Anderson PAW, Glick KL, Killam AP, et al: The effect of heart rate on in utero left ventricular output in the fetal sheep. J Physiol 372:557-573, 1986
43. Gest AL, Bair DK, Vander Straten MC: Thoracic duct lymph flow in fetal sheep with increased venous pressure from electrically induced tachycardia. Biol Neonate 64: 325-330, 1993
44. Blair DK, Vander Straten MC, Gest AL: Hydrops in fetal sheep from rapid induction of anemia. Pediatr Res 35: 560-564, 1994