Pathophysiology, diagnosis and clinical management ... Bammens Sodium.pdf · Electrolyte...
55
Electrolyte disturbances Pathophysiology, diagnosis and clinical management Hyponatremia Hypernatremia Bert Bammens UZ Leuven KU Leuven 1
Transcript of Pathophysiology, diagnosis and clinical management ... Bammens Sodium.pdf · Electrolyte...

Electrolyte disturbances
Pathophysiology, diagnosis and clinical management
Hyponatremia Hypernatremia
Bert Bammens UZ Leuven KU Leuven
1

Hyponatremia
• Definition: plasma [Na+] < 135 mmol/L
(normal plasma [Na+] 135-145 mmol/L*)
*reference values van lab UZ Gasthuisberg 3-2011
2

Hyponatremia
• Definition: plasma [Na+] < 135 mmol/L
(normal plasma [Na+] 135-145 mmol/L*)
• Up to 30% hospitalized patients • 15-20% emergency room admissions
• Often iatrogenic
*reference values van lab UZ Gasthuisberg 3-2011
3

Hyponatremia: pathogenesis
hypo-osmolar hyponatremia
hyperosmolar hyponatremia
iso-osmolar hyponatremia
STEP 1: measure plasma osmolality! (normal plasma osmolality 275-295 mOsm/kg*)
*reference values van lab UZ Gasthuisberg 3-2011
4
Hyponatremia: pathogenesis iso-osmolar hyponatremia
= PSEUDO-HYPONATREMIA [Na+] in plasma water is normal . Osmolality (= concentration of osmoles in plasma water) is normal. BUT Fraction plasma water of total volume is lower than normal, due to increased fraction of lipids and/or proteins.
5

Hyponatremia: pathogenesis iso-osmolar hyponatremia
= PSEUDO-HYPONATREMIA Causes hyperlipidemia: hypertriglyceridemia excess abnormal protein: Morbus Kahler/Myeloma
Volume en osmolaliteit: fysiologie
• Osmolaliteit (mOsm/kg) – Osmolariteit (mOsm/L) = concentratie opgeloste stoffen in vloeistof
• De osmotische (on)evenwichten stellen zich in obvconcentraties van osmolen in WATER
• Water = 93% van totaal plasma volume(7% = lipiden en proteinen)
[Na+ ]plasma=142 mmol/L
(142/0.93)
[Na+ ]plasmaWATER=154 mmol/L6

Hyponatremia: pathogenesis iso-osmolar hyponatremia
7
Turchin et al. N Engl J Med
349: 1465-1469, 2003

Hyponatremia: pathogenesis iso-osmolar hyponatremia
8
[Na+ ]plasma=142 mmol/L [Na+ ]plasmaWATER=154 mmol/L
(154 x 0.93) (77 x 2)
diluted [Na+ ]plasmaWATER=77 mmol/L
“flame photometry”
and “indirect potentiometry”

Hyponatremia: pathogenesis iso-osmolar hyponatremia
9
[Na+ ]plasma=111,6 mmol/L [Na+ ]plasmaWATER=120 mmol/L
(120 x 0.93) (60 x 2)
diluted [Na+ ]plasmaWATER=60 mmol/L
“flame photometry”
and “indirect potentiometry”
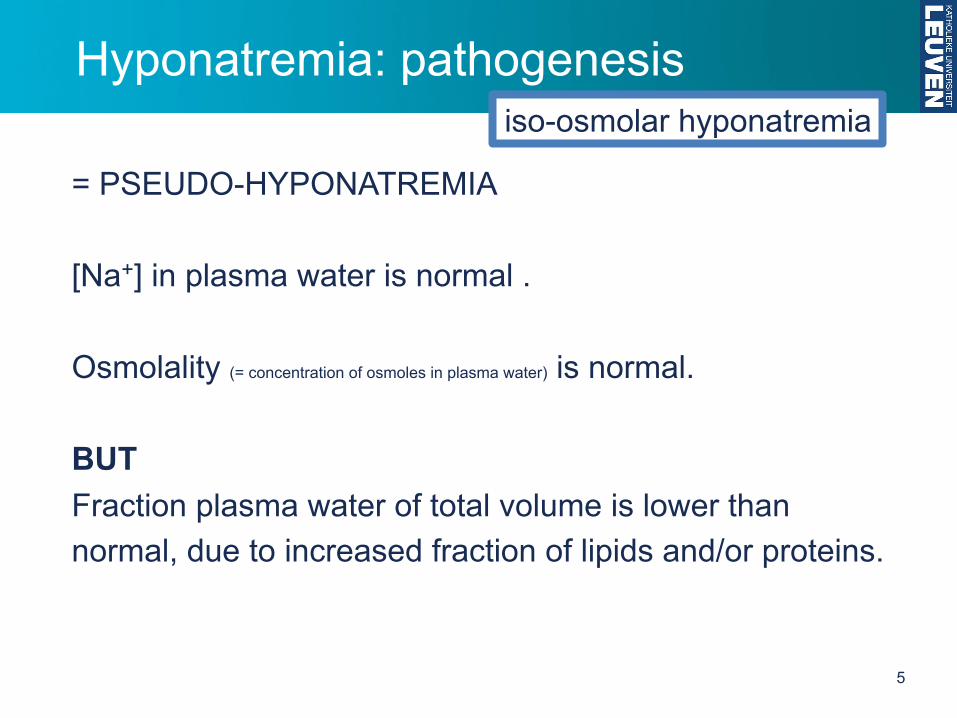
Hyponatremia: pathogenesis iso-osmolar hyponatremia
10
[Na+ ]plasma=142 mmol/L
(154 x 0.93)
[Na+ ]plasmaWATER=154 mmol/L
“direct potentiometry”

Hyponatremia: pathogenesis
= translocation HYPONATREMIA “Abnormal” osmoles in ECF cause high osmolality. Water moves from intra- to extra-cellular compartment. Plasma [Na+] decreases.
hyperosmolar hyponatremia
11

Hyponatremia: pathogenesis
= translocation HYPONATREMIA
Causes hyperglycemia (uncontrolled diabetes: glucose becomes an effective osmole)
mannitol, sorbitol, contrast dyes glycine (transurethral prostate/bladder procedures)
high “osmolar gap”
hyperosmolar hyponatremia
Water balans: regeling osmolaliteit
*referentiewaarden van labo UZ Gasthuisberg 3-2011
• Normale plasma osmolaliteit: 275-295 mOsm/kg*
• Meting in het labo• Schatting obv berekening
2 (Na+ + K+) + ureum + glucose - 10
2 (Na+) + ureum + glucose
2 (Na+)
6 18
6 18
Na+, K+: mEq/L ureum, glucose: mg/dL
12

Hyponatremia: pathogenesis
= translocation HYPONATREMIA
Causes hyperglycemia each 100 mg/dL [glucose] higher than 100 mg/dL 1.0-1.6 mmol/L lower plasma [Na+]
hyperosmolar hyponatremia
13

Hyponatremia: pathogenesis
STEP 2: measure urine osmolality! primary polydipsia, beer drinkers hyponatremia Kidneys do what they need to do! (= maximal free water excretion) BUT water intake higher than maximal diluting capacity
urine osmolality ≤ 100 mOsm/kg
14
hypo-osmolar hyponatremia

Hyponatremia: pathogenesis
STEP 2: meet urine osmolality! primary polydipsia, beer drinkers hyponatremia normal: elimination ± 600 mOsm per day normal: maximally diluted urine 30 mOsm/kg*
max 20 L urine per day
urine osmolality ≤ 100 mOsm/kg
*usually somewhat higher, so max diuresis somewhat lower
15
hypo-osmolar hyponatremia

Hyponatremia: pathogenesis
STEP 2: meet urine osmolality! beer drinkers potomania: low osmolar intake elimination < 250 mOsm per day maximally diluted urine 30 mOsm/kg*
max 8.3 L urine per day
urine osmolality ≤ 100 mOsm/kg
16
hypo-osmolar hyponatremia
*usually somewhat higher, so max diuresis somewhat lower

Hyponatremia: pathogenesis
STEP 2: measure urine osmolality! STEP 3: measure urine [Na+]
urine osmolality > 100 mOsm/kg
hypo-osmolar hyponatremia
17
urine [Na+] ≤ 30 mmol/L urine [Na+] > 30 mmol/L

urine [Na+] ≤ 30 mmol/L urine osmolality > 100 mOsm/kg
Hyponatremia: pathogenesis hypo-osmolar hyponatremia
STEP 4: assess ECF volume!
Extracellulaire overhydratatie: symptomen
Cardiovasculaire symptomenin geval van overvulling van plasma-compartiment
• gestuwde halsvenenverhoogde centraal veneuze druk (CVD)positief hepatojugulair reflux (HJR)
26
Extracellulaire overhydratatie, oedeem
• Definitie oedeem: excessieve opstapeling van vocht in interstitieel compartiment (+- transcellulair)
• Anasarca = gegeneraliseerd oedeem
2
Dehydratatie: symptomen
Interstitiële symptomen
• droge huid zonder turgorstaande of traag verstrijkende huidplooi
• droge tong, overlangse plooien, zwart-bruin beslag
• ingevallen ogen
62
Cardiovasculaire symptomenin geval van ondervulling van plasma-compartiment(dus meer bij iso-osmolaire dehydratatie)
• platgevallen halsvenenverlaagde centraal veneuze druk (CVD)
Dehydratatie: symptomen
66
Cardiovasculaire symptomenin geval van ondervulling van plasma-compartiment(dus meer bij iso-osmolaire dehydratatie)
• lage bloeddruk, orthostatische hypotensie• compensatoire tachycardie• hoofdpijn, beter bij neerliggen• zwakte, vermoeidheid, apathie• shock
Dehydratatie: symptomen
Na+ balans: regeling volume
• Naast Na+ balans, zijn voor volume- en bloeddrukregeling ook hartritme, slagvolume en vasculaire tonus belangrijk.
Belangrijke verschillen
regeling ECF volume regeling osmolaliteit
Registratie van… effectief circulerend volume plasma osmolaliteit
Sensoren carotis, aorta, aff. arteriool, atria osmoreceptoren hypothalamus
Efferent signaal RAAS, sympathicus, ADH, ANP ADH dorst
Effector korte termijn: hart, bloedvaten nieren hersenenlange termijn: nieren
Effect korte termijn: bloeddruk water excretie water intakelange termijn: Na+ excretie
Water en Na+ balans: fysiologie
67
18

Hyponatremia: pathogenesis
HYPERVOLEMIA heart failure, liver cirrhosis, nephrotic syndrome Na+ retention + non-osmotic stimulation of ADH release
free water retention hyponatremia
Hartsdecompensatie
Daling hartdebiet of shunting van deel van debiet
Effectief circulerend volume daalt
Na+ retentie
Oedeem: oorzaken toename veneuze drukstijging ECF
(toename arteriële druk)
4 parallelle efferente“effector pathways”
corrigeren afwijking van effectief circulerend volume
Na+ balans
http://www.heartfailurematters.org/EN/Animation/Pages/animation_2.aspx
9
Levercirrose
- Veneuze outflow vv. hepaticae is verstoord door fibroseà toename splanchnisch bloedvolume en portale hypertensieà ascites vocht
- Daling effectief circulerend volume à Na+ retentie- Hogere concentratie en langere werking
aldosterone- Hypo-albuminemie door verminderde
synthese
Oedeem: oorzaken toename veneuze drukstijging ECF
(toename arteriële druk)stoornis van
differentieel oncotische druk
21
Verlaging plasma oncotische druk
Hypo-albuminemie door- Eiwit tekort in voeding (kwashiorkor)- Slechte gastro-intestinale eiwit opname- Tekort in albumine synthese (leverpathologie)- Eiwitverlies (nefrotisch syndroom, protein-loosing
enteropathy, eiwitrijk ascitesvocht, brandwonden)
Vocht naar interstitium à effectief circulerend volume daalt à Na+ retentie
Oedeem: oorzaken stoornis vandifferentieel oncotische druk
18
19
urine [Na+] ≤ 30 mmol/L urine osmolality > 100 mOsm/kg
hypo-osmolar hyponatremia

Hyponatremia: pathogenesis
HYPERVOLEMIA heart failure, liver cirrhosis, nephrotic syndrome As a consequence of Na+ retention
Hartsdecompensatie
Daling hartdebiet of shunting van deel van debiet
Effectief circulerend volume daalt
Na+ retentie
Oedeem: oorzaken toename veneuze drukstijging ECF
(toename arteriële druk)
4 parallelle efferente“effector pathways”
corrigeren afwijking van effectief circulerend volume
Na+ balans
http://www.heartfailurematters.org/EN/Animation/Pages/animation_2.aspx
9
Levercirrose
- Veneuze outflow vv. hepaticae is verstoord door fibroseà toename splanchnisch bloedvolume en portale hypertensieà ascites vocht
- Daling effectief circulerend volume à Na+ retentie- Hogere concentratie en langere werking
aldosterone- Hypo-albuminemie door verminderde
synthese
Oedeem: oorzaken toename veneuze drukstijging ECF
(toename arteriële druk)stoornis van
differentieel oncotische druk
21
Verlaging plasma oncotische druk
Hypo-albuminemie door- Eiwit tekort in voeding (kwashiorkor)- Slechte gastro-intestinale eiwit opname- Tekort in albumine synthese (leverpathologie)- Eiwitverlies (nefrotisch syndroom, protein-loosing
enteropathy, eiwitrijk ascitesvocht, brandwonden)
Vocht naar interstitium à effectief circulerend volume daalt à Na+ retentie
Oedeem: oorzaken stoornis vandifferentieel oncotische druk
18
20
urine [Na+] ≤ 30 mmol/L urine osmolality > 100 mOsm/kg
hypo-osmolar hyponatremia
urine [Na+] ≤ 30 mmol/L

Hyponatremia: pathogenesis
HYPOVOLEMIA
+ HYPOTONIC SUBSTITUTION!
free water loss = hyperosmolar dehydration
loss of water and Na+ = iso-osmolar dehydration
21
urine [Na+] ≤ 30 mmol/L urine osmolality > 100 mOsm/kg
hypo-osmolar hyponatremia

Hyponatremia: pathogenesis
HYPOVOLEMIA (hypovolemic) shock hyponatremia iso-osmolar fluid loss, but non-osmotic stimulation of ADH release free water retention hyponatremia
Dehydratatie: pathogenesegelijkmatig verlies water en Na+
= iso-osmolaire dehydratatieVerlies van bloed of plasma
= rechtstreeks verlies uit extra-cellulaire ruimte= per definitie iso-osmolair
ENKEL ECF volume daalt, want geen osmotische gradiënt
39
Ernstige daling effectief circulerend volume (5-10%)/ hypotensie( 1% voor osmolaliteit)
• Via baroreceptoren sinus caroticus• Drempel voor ADH secretie daalt• Helling van ADH vs. osmolaliteit-curve stijgt
• bv. hemorragische shockhypovolemische shock
Water balans: NIEREN
22
urine [Na+] ≤ 30 mmol/L urine osmolality > 100 mOsm/kg
hypo-osmolar hyponatremia

Hyponatremia: pathogenesis
Causes: 2 categories heart failure hyperosm. dehydr. + hypotonic subst. liver cirrhosis iso-osm. dehydr. + hypotonic subst. nephrotic syndrome hypovolemic shock HYPERVOLEMIA HYPOVOLEMIA
IN BOTH CATEGORIES: LOW EFFECTIVE CIRCULATING VOLUME!
23
urine [Na+] ≤ 30 mmol/L urine osmolality > 100 mOsm/kg
hypo-osmolar hyponatremia

urine [Na+] > 30 mmol/L urine osmolality > 100 mOsm/kg
Hyponatremia: pathogenesis hypo-osmolar hyponatremia
STEP 4: diuretics OR renal insufficiency?
24

urine [Na+] > 30 mmol/L urine osmolality > 100 mOsm/kg
Hyponatremia: pathogenesis hypo-osmolar hyponatremia
STEP 4: diuretics OR renal insufficiency?
YES!
25
Dehydratatie: pathogenese
Diuretica
thiazide diuretica
LET WEL! Diuretica kunnen ook voor hypotoon vochtverlies zorgen endus resulteren in hyper-osmolaire dehydratatie (lisdiuretica)
primair Na+ verlies= hypo-osmolaire dehydratatie
Ook de variabele inname van water en zouten bepaaltmee het uiteindelijke klinische beeld (hypo-, iso-, hyper-osmolair)
60

urine [Na+] > 30 mmol/L urine osmolality > 100 mOsm/kg
Hyponatremia: pathogenesis hypo-osmolar hyponatremia
STEP 4: diuretics OR renal insufficiency?
YES! acute or chronic renal insufficiency
26
Nierinsufficiëntie
Daling maximaal mogelijke Na+ en water excretie
Stijging ECF als intake Na+ en water > excretie
Oedeem: oorzaken toename veneuze drukstijging ECF
(toename arteriële druk)
13
Nierinsufficiëntie
Perfusiestoornis in zieke glomeruli
Stimulatie vrijzetting renine
Na+ retentie
Oedeem: oorzaken toename veneuze drukstijging ECF
(toename arteriële druk)
Daling effectief circulerend volume à vrijzetting renine
• via stimulatie sympathisch zenuwstelsel• via verminderd aanbod NaCl aan macula densa
(“NaCl sensor”)• via baroreceptor functie
afferente arteriool“Externe” invloed op RPF en GFR
• Angiotensine II– Constrictie arteria renalis en arteriolen: efferent > afferent à
daling RPF > GFR– Contractie mesangiale cellen à Kf daalt à GFR daalt– Verhoogde gevoeligheid van TG feedback à GFR daalt– Daling bloedflow in medulla
• Sympathisch zenuwstelsel: norepinephrine– Constrictie arteriolen: efferent > afferent à daling RPF > GFR– Vrijzetting Renin uit granulaire cellen
Autoregulatie
• Juxtaglomerulair apparaat: 2 feedbacksystemen
LOKAAL: TUBULOGLOMERULAIRE FEEDBACK– Hoger aanbod vocht en NaCl aan macula densa (Na/K/2Cl symporter)
– Constrictie afferente arteriool– Daling glomerulaire filtratie van nefron
SYSTEMISCH: RENINE RELEASE– Daling druk in renale arterie– Baroreceptor in afferente arteriool registreert– Vrijzetting Renine uit granulaire cellen– Angiotensinogeen à Angiotensine I à Angiotensine II– Systemische vasoconstrictie
Autoregulatie
• Juxtaglomerulair apparaat: 2 feedbacksystemen
LOKAAL: TUBULOGLOMERULAIRE FEEDBACK– Hoger aanbod vocht en NaCl aan macula densa (Na/K/2Cl symporter)
– Constrictie afferente arteriool– Daling glomerulaire filtratie van nefron
SYSTEMISCH: RENINE RELEASE– Daling druk in renale arterie– Baroreceptor in afferente arteriool registreert– Vrijzetting Renine uit granulaire cellen– Angiotensinogeen à Angiotensine I à Angiotensine II– Systemische vasoconstrictie
Na+ balans: RAAS
14
Overmatige intake van water
Geeft enkel aanleiding tot oedeemvorming indien geenwater excretie mogelijk is: anurie of oligurie.
Is meestal iatrogeen.
Oedeem: oorzaken toename veneuze drukstijging ECF
(toename arteriële druk)
17

urine [Na+] > 30 mmol/L urine osmolality > 100 mOsm/kg
Hyponatremia: pathogenesis hypo-osmolar hyponatremia
STEP 4: diuretics OR renal insufficiency?
NO!
STEP 5: assess ECF volume!
27
Extracellulaire overhydratatie: symptomen
Cardiovasculaire symptomenin geval van overvulling van plasma-compartiment
• gestuwde halsvenenverhoogde centraal veneuze druk (CVD)positief hepatojugulair reflux (HJR)
26
Extracellulaire overhydratatie, oedeem
• Definitie oedeem: excessieve opstapeling van vocht in interstitieel compartiment (+- transcellulair)
• Anasarca = gegeneraliseerd oedeem
2
Dehydratatie: symptomen
Interstitiële symptomen
• droge huid zonder turgorstaande of traag verstrijkende huidplooi
• droge tong, overlangse plooien, zwart-bruin beslag
• ingevallen ogen
62
Cardiovasculaire symptomenin geval van ondervulling van plasma-compartiment(dus meer bij iso-osmolaire dehydratatie)
• platgevallen halsvenenverlaagde centraal veneuze druk (CVD)
Dehydratatie: symptomen
66
Cardiovasculaire symptomenin geval van ondervulling van plasma-compartiment(dus meer bij iso-osmolaire dehydratatie)
• lage bloeddruk, orthostatische hypotensie• compensatoire tachycardie• hoofdpijn, beter bij neerliggen• zwakte, vermoeidheid, apathie• shock
Dehydratatie: symptomen
Na+ balans: regeling volume
• Naast Na+ balans, zijn voor volume- en bloeddrukregeling ook hartritme, slagvolume en vasculaire tonus belangrijk.
Belangrijke verschillen
regeling ECF volume regeling osmolaliteit
Registratie van… effectief circulerend volume plasma osmolaliteit
Sensoren carotis, aorta, aff. arteriool, atria osmoreceptoren hypothalamus
Efferent signaal RAAS, sympathicus, ADH, ANP ADH dorst
Effector korte termijn: hart, bloedvaten nieren hersenenlange termijn: nieren
Effect korte termijn: bloeddruk water excretie water intakelange termijn: Na+ excretie
Water en Na+ balans: fysiologie
67

Hyponatremia: pathogenesis
HYPOVOLEMIA
Dehydratatie: pathogenese
Renale salt-wastingVermogen van nieren om zout te reabsorberen(vnl. proximale tubulus) schiet tekort.
- Chronische nierinsufficiëntie en (te) strikt zoutarm dieet(vooral bij nieraandoeningen met sterk tubulo-interstitiële aantasting)
- Herstelfase na acute tubulus necrose, niertransplantatie- Herstelfase na opheffen van chronische urinewegobstructie
“post-obstructieve polyurie”
primair Na+ verlies= hypo-osmolaire dehydratatie
5828
urine [Na+] > 30 mmol/L urine osmolality > 100 mOsm/kg
hypo-osmolar hyponatremia

Hyponatremia: pathogenesis
Dehydratatie: pathogenese
Ziekte van AddisonBijnierschorsinsufficiëntie:te weinig glucocorticoidente weinig mineralocorticoiden
primair Na+ verlies= hypo-osmolaire dehydratatie
Na+ reabsorptie bevorderen
Aldosterone werkt op PRINCIPAL CELLS van
CORTICAL COLLECTING DUCT
daling GFRmeer ADH
Netto meer verlies van zoutdan van water!
5929
urine [Na+] > 30 mmol/L urine osmolality > 100 mOsm/kg
hypo-osmolar hyponatremia
HYPOVOLEMIA

Hyponatremia: pathogenesis
EUVOLEMIA
Causes • hormonal disturbances leading to increased ADH
without osmotic stimulus: glucocorticoid deficiency (Addison’s disease) hypothyroidism
• Syndrome of Inappropriate AD(H secretion): SIAD(H)
30
urine [Na+] > 30 mmol/L urine osmolality > 100 mOsm/kg
hypo-osmolar hyponatremia

Hyponatremia: pathogenesis
EUVOLEMIA glucocorticoid deficiency stimulation CRH co-secretion of ADH
Dehydratatie: pathogenese
Ziekte van AddisonBijnierschorsinsufficiëntie:te weinig glucocorticoidente weinig mineralocorticoiden
primair Na+ verlies= hypo-osmolaire dehydratatie
Na+ reabsorptie bevorderen
Aldosterone werkt op PRINCIPAL CELLS van
CORTICAL COLLECTING DUCT
daling GFRmeer ADH
Netto meer verlies van zoutdan van water!
5931
urine [Na+] > 30 mmol/L urine osmolality > 100 mOsm/kg
hypo-osmolar hyponatremia

Hyponatremia: pathogenesis
EUVOLEMIA hypothyroidism lower cardiac output and GFR secretion of ADH (hemodynamic stimulus)
32
urine [Na+] > 30 mmol/L urine osmolality > 100 mOsm/kg
hypo-osmolar hyponatremia
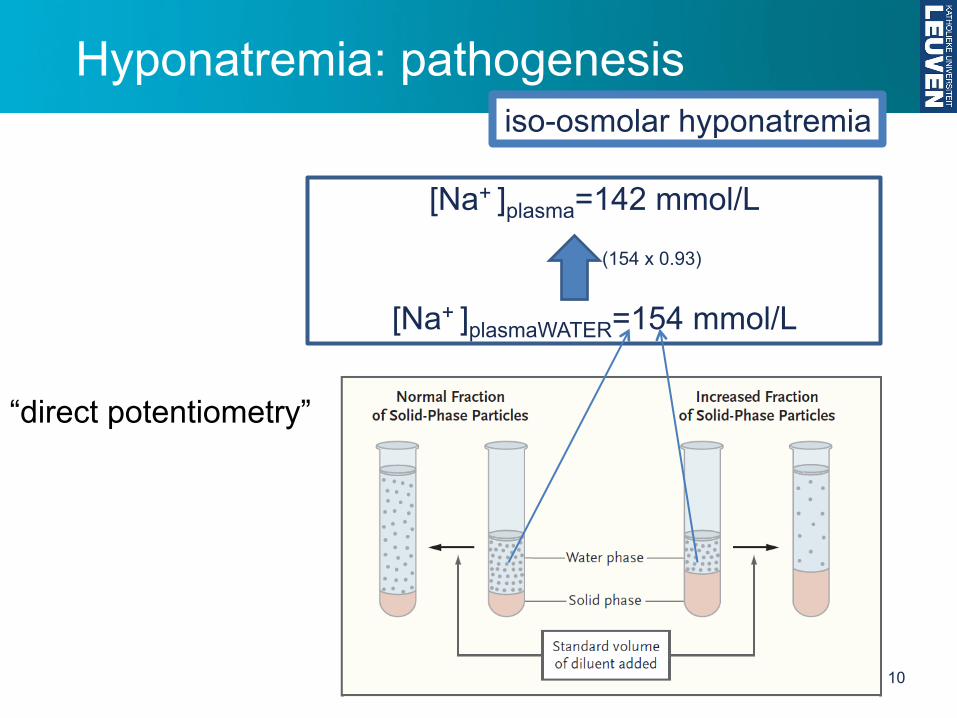
Hyponatremia: pathogenesis
EUVOLEMIA SIADH (Schwartz-Bartter syndroom) excess ADH free water retention, intra- and extra-cellular distribution Increase of ECF stimulates Na en water excretion ECF volume restored (euvolemia) reinforces hyponatremia
urine osmolality meestal > 300 mOsm/kg plasma urinezuur meestal < 4 mg/dL
33
urine [Na+] > 30 mmol/L urine osmolality > 100 mOsm/kg
hypo-osmolar hyponatremia

urine [Na+] > 30 mmol/L urine osmolality > 100 mOsm/kg
hypo-osmolar hyponatremia
NEW!!!
Hyponatremia: pathogenesis

urine [Na+] > 30 mmol/L urine osmolality > 100 mOsm/kg
hypo-osmolar hyponatremia
Hyponatremia: pathogenesis
Causes: 2 categories renal salt-wasting glucocorticoid deficiency Addison’s disease hypothyroidism
SIAD(H) HYPOVOLEMIA EUVOLEMIA
Hyponatremia: pathogenesis
36
urine [Na+] > 30 mmol/L urine osmolality > 100 mOsm/kg
hypo-osmolar hyponatremia
diuretics OR renal insufficiency? YES!
NO!

*reference values van lab UZ Gasthuisberg 3-2011
Hyponatremia: symptoms
37
• Definition: plasma [Na+] < 135 mmol/L
(normal plasma [Na+] 135-145 mmol/L*) • Serious trouble: [Na+] < 125 mmol/L
symptoms as a consequence of - osmotic watertransfer to intra-cellular compartment (brain) - additional symptoms of over- or dehydration
NOTE: pseudohyponatremia: no symptoms hyperosmolar hyponatremia: watertransfer to extra-cellular compartment

*reference values van lab UZ Gasthuisberg 3-2011
Hyponatremia: symptoms
38
• Definition: plasma [Na+] < 135 mmol/L
(normal plasma [Na+] 135-145 mmol/L*) • Serious trouble: [Na+] < 125 mmol/L
ACUTE changes, more risk of symptoms In case of gradual change of natremia
Na+, K+ and organic osmoles leak from brain cells
less swelling

Hyponatremia: symptoms
39
symptoms of brain edema, high intracranial pressure
e.g. bradypnea (Cheyne-Stokes-ademhaling)

Treat the cause! Reduction of free water intake (take volume status into acount) SIAD(H) - reduction of free water intake - (hypertonic) NaCl ± loop diuretic - ureum therapy (induce osmotic diuresis) - demeclocycline, lithium (inhibition of ADH) - vaptans
Hyponatremia: treatment
40

FAST correction, only in ACUTE hyponatremia 1-2 mmol/L per hour to 120 mmol/L, then max. 0.5 mmol/L per hour
SLOW correction in case of gradual change of natremia. If too fast à risk of central pontine myelinolysis < 0.5 mmol/L per hour (< 12 mmol/L per day)
paraparesis, ataxia, coma
Hyponatremia: treatment
41

Hyponatremia
42
Spasovski et al. Nephrol Dial Transplant
29 (Suppl 2): i1-i39, 2014

“new” vs. “old”
Immediate treatment (before diagnostic work-up) ACUTE hyponatremia SERIOUS symptoms
Spasovski et al. Nephrol Dial Transplant 29 (Suppl 2): i1-i39, 2014
NEW?

“new” vs. “old”
“position switch”

Hyponatremia: assessing ECF
121 consecutive hyponatremia cases
Diagnostic and therapeutic work-up by - medical students using “physiology-based” algorithm
intervention - senior intensive care doctor
comparator - senior endocrinologist
golden standard
Fenske et al. Am J Med 123: 652-657, 2010

Hyponatremia: assessing ECF
Diagnostic agreement with golden standard: intervention 71% comparator 32%
Diagnostic accuracy:
intervention 86% comparator 48%
(95% when “measuring” rather than “assessing” ECF)
Fenske et al. Am J Med 123: 652-657, 2010

Electrolyte disturbances
Pathophysiology, diagnosis and clinical management
Hyponatremia Hypernatremia
Bert Bammens UZ Leuven KU Leuven
47

Hypernatremia
• Definition: plasma [Na+] > 145 mmol/L
(normal plasma [Na+] 135-145 mmol/L*)
• Serious trouble: [Na+] > 160 mmol/L
symptoms as a consequence of - osmotic watertransfer to extra-cellular compartment (brain) - additional symptoms of over- or dehydration *reference values van lab UZ Gasthuisberg 3-2011
48

Hypernatremia
• Definition: plasma [Na+] > 145 mmol/L (normal plasma [Na+] 135-145 mmol/L*)
• Serious trouble: [Na+] > 160 mmol/L
ACUTE changes, more risk of symptoms In case of gradual change of natremia intra-cellular osmolality increases due to “idiogenic osmoles” less cell shrinking *reference values van lab UZ Gasthuisberg 3-2011
49

Hypernatremia: symptoms
50
symptoms of brain cell shrinking
subarachnoidal or intracerebral bleeding
hallucinations, delirium, lethargy, coma, convulsions
hemiparesis

Hypernatremia: pathogenesis
high free water loss
low free water intake
high Na+ intake
51
(relative to water intake)

(relative to water intake)
Hypernatremia: pathogenesis high Na+ intake
52
RARE! OFTEN IATROGENIC! Causes infusion of hypertonic solutions (NaCl, NaHCO3) salt instead of sugar in milk formulations

Hypernatremia: pathogenesis low free water intake
53
Dehydratatie: pathogenese
Niet-renale oorzaken
Te lage water innamefalend dorstcentrumbaby’s (bv. verwaarlozing)onbewuste patiënten
Te veel (vrij) water verliesbrakenosmotische diarree: laxativa, lactase-deficiëntiezweten (igv koorts, hoge omgevingstemperatuur, inspanningen)brandwonden
primair waterverlies = hyperosmolaire dehydratatie
44
high free water loss

Hypernatremia: pathogenesis low free water intake
54
high free water loss
Dehydratatie: pathogenese
Renale oorzaken
Osmotische diurese: “solute diuresis”excessief waterverlies, rijk aan “deeltjes”
Diabetes insipidus: “water diuresis”excessief waterverlies, arm aan “deeltjes”urine meer gedilueerd dan nodig
primair waterverlies = hyperosmolaire dehydratatie
Renale fysiologie kan zorgen voor…
…dilutie tot 10x de plasma-osmolaliteit (30 mOsm)…concentratie: tot 4x de plasma-osmolaliteit (1200 mOsm)
Water balans: NIEREN
46
+ loop diuretics

Treat the cause! Increase free water intake (take volume status into account) Diabetes insipidus
- Central: ADH-analogue - Nefrogenic: treat the cause, thiazide
Hypernatremia: treatment
55