
Welcome to Pathophysiology Department of Pathophysiology Liaoning Medical College.

Pathophysiology, diagnosis and clinical management
Bert Bammens UZ Leuven KU Leuven
Electrolyte disturbances
1
HYPOKALEMIA and K+ DEPLETION HYPERKALEMIA
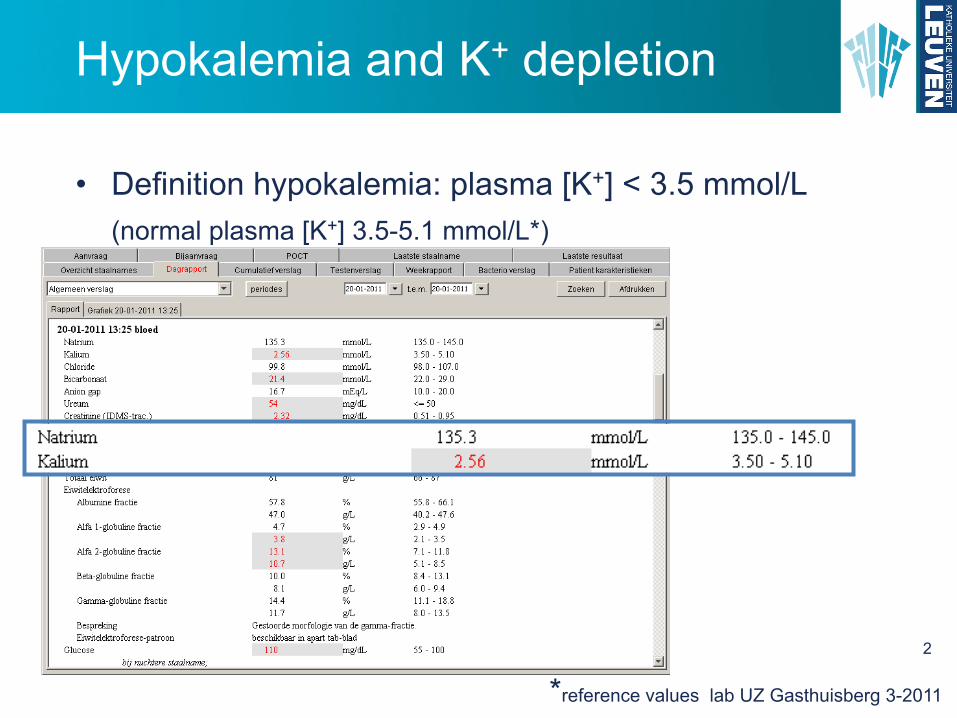
*reference values lab UZ Gasthuisberg 3-2011
Hypokalemia and K+ depletion
2
• Definition hypokalemia: plasma [K+] < 3.5 mmol/L
(normal plasma [K+] 3.5-5.1 mmol/L*)

Hypokalemia and K+ depletion
3
• Definition K+ depletion: negative (external) K+ balance
• Relationship plasma [K+] and K+ balance not linear!

Hypokalemia: pathogenesis
4
LOW INTAKE
EXCESSIVE LOSSES
SHIFT TO INTRACELLULAR COMPARTMENT
K+ depletion
K+ depletion
not necessarily K+ depletion

Hypokalemia: pathogenesis
5
LOW INTAKE
Causes RARE in case of normal oral intake, except when combined
with
Renal K+ excretion can be reduced to 5 à 25 mmol/day! Adaptation to low K+ diet takes ± 14 days.
EXCESSIVE LOSSES
Kalium: fysiologie
K+ transport in nefronBIJ LAGE K+ INTAKE
PT en Lis van Henlereabsorptie
DCT, CNT, ICT, CCTreabsorptie
MCDbeperkte reabsorptie
15

Hypokalemia: pathogenesis
6
LOW INTAKE
Causes Parenteral feeding with insufficient amounts of K+
Geofagia: clay ingestion, clay binds K+ in gastrointestinal tract
cultural heritage vs. psychiatric eating disorder?

Hypokalemia: pathogenesis
7
EXCESSIVE LOSSES
Causes GASTRO-INTESTINAL
LOW gastro-intestinal losses: 20-50 mmol/L K+.
bv. diarrhea, enema, laxatives, cation exchangers low gastro-intestinal fistulisation/stoma, ileus villous adenoma VIPoma (vasoactive intestinal peptide) Particularly when long-lasting!

Hypokalemia: pathogenesis EXCESSIVE LOSSES
Causes GASTRO-INTESTINAL
HIGH (gastric) losses: only 5-10 mmol/L K+.
Gastric losses metabolic alkalosis à renal K+ loss volume contraction à aldosterone à renal K+ loss
Zuur-base: pathogenese/oorzaken
48
Oorzaken GASTRO-INTESTINAALINITIEREND: verlies van H+
braken van maagvocht, afzuigen van maagvocht, maagfistels
metabole alkalose met ECV contractie
Kalium: fysiologie
• Alkalose (metabool of respiratoir) = hogere pHà hogere intracellulaire pH principal cellsà actievere Na+-K+-ATPase en apicale K+-kanalenà meer K+ secretie
• Alkalose (metabool of respiratoir)à hogere flow door meer HCO3
-
à meer K+ secretie
DUS: beide renale effecten van alkaloseversterken effect op interne balans
Externe K+ balans
30
Kalium: fysiologie
• Mineralocorticoiden: aldosterone, DOCA (synth.)
4 effecten-Stimulatie Na+-K+-ATPase-Toename aantal Na+-K+-ATPase-Stimulatie ENaC-Stimulatie K+-kanalen
K+-secreterend effect van aldosterone werkt voornamelijk bij groot distaal Na+ aanbod!
Externe K+ balans
25
8
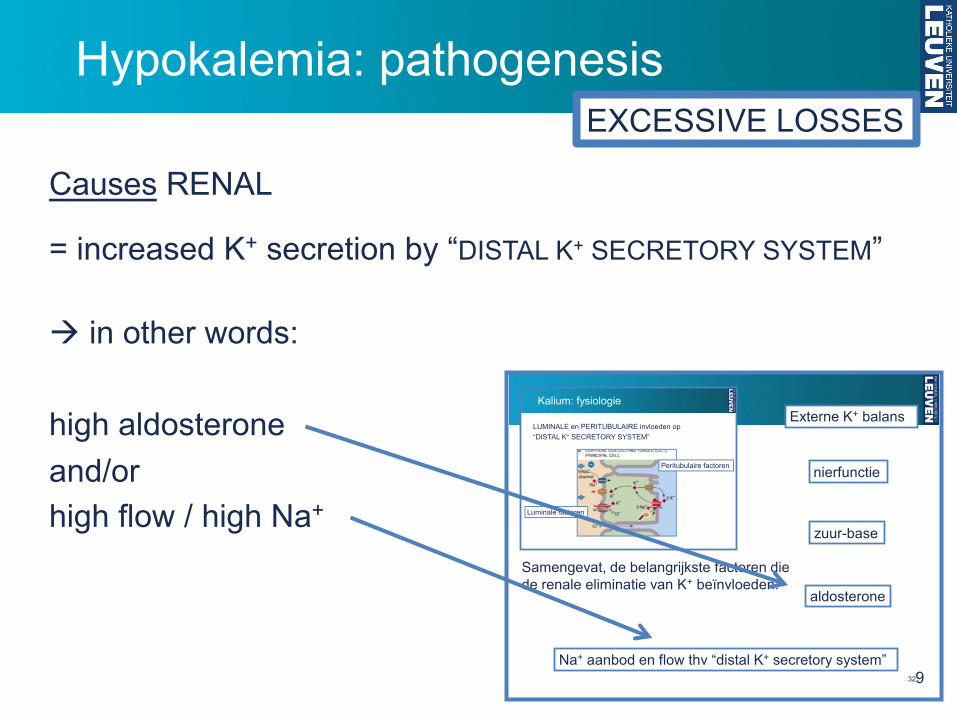
Hypokalemia: pathogenesis EXCESSIVE LOSSES
Causes RENAL
= increased K+ secretion by “DISTAL K+ SECRETORY SYSTEM”
à in other words: high aldosterone and/or high flow / high Na+
Kalium: fysiologie
LUMINALE en PERITUBULAIRE invloeden op “DISTAL K+ SECRETORY SYSTEM”
Luminale factoren
Peritubulaire factoren
Na+ aanbod en flow thv “distal K+ secretory system”
aldosterone
zuur-base
nierfunctie
Samengevat, de belangrijkste factoren die de renale eliminatie van K+ beïnvloeden:
Externe K+ balans
329

Hypokalemia: pathogenesis EXCESSIVE LOSSES
Causes RENAL
DIURETICS
carbo-anhydrase inhibitors (acetazolamide)
loop diuretics (furosemide, bumetanide)
thiazide diuretics (hydrochloorthiazide, chloortalidon)
osmotic diuretics
MECHANISM - Site of action = proximal à increased flow and Na+ delivery to
“DISTAL K+ SECRETORY SYSTEM” - Decrease of ECF volume stimulates RAAS à high aldosterone
inhibitie Na+ reabsorptiedoor blokkade Na+ transportin specifieke nefronsegmenten
DIURETICA
30
10
Hypokalemia: pathogenesis EXCESSIVE LOSSES
Causes RENAL
non-resorbable anions in glomerular filtrate
more Na+ retained in lumen of PT increased Na+ delivery to distal tubule
bv. HCO3
- in case of high gastro-intestinal losses in proximal RTA (type 2)
β-hydroxybutiric acid in diabetic keto-acidosis
Hippuric acid (toluene derivative) in glue addicts
11

Hypokalemia: pathogenesis EXCESSIVE LOSSES
Causes RENAL
Mineralocortoicoid excess (for other reasons than dehydration)
primary (hyper)aldosteronism (Conn’s syndrome) Cushing syndrome (glucocorticoid excess) licorice (glycyrrhetinic acid) secondary to renovascular disease secondary to stress (bv. post-surgery)
Na+ balans: RAAS
65
12

Hypokalemia: pathogenesis EXCESSIVE LOSSES
Causes RENAL
RENAL TUBULAR DEFECTS
Bartter’s syndrome (defect NKCC2 à mimics loop diuretics) Gitelman’s syndrome (defect NCC à mimics thiazide diuretics) RTA (type 1 and 2) Liddle’s syndrome
Liddle’s syndrome (autosomal dominant) Overexpression of ENac in principal cells
Na+ retention K+ secretion
Mimics primary aldosteronism with hypertension, hypokalemia and alkalosis, but NO increased renine or aldosterone levels (pseudo-aldosteronism)
13

Hypokalemia: pathogenesis EXCESSIVE LOSSES
Causes SWEATING, BURN WOUNDS
VERY RARE cause of hypokalemia, except when excessive and combined with low intake or other causes of excessive losses.
14
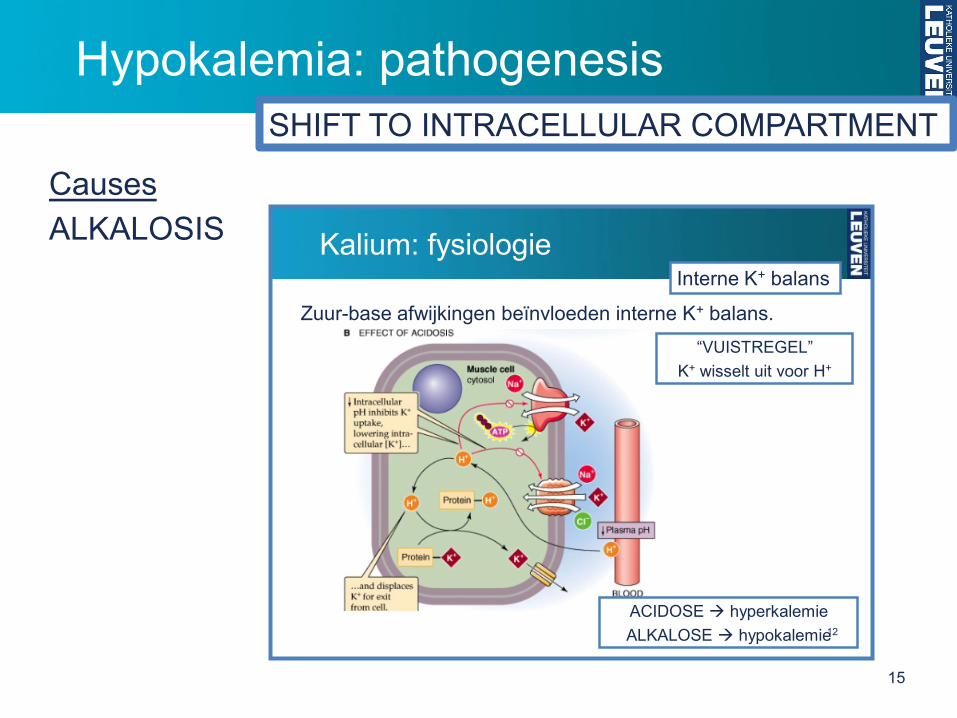
Hypokalemia: pathogenesis
Causes
ALKALOSIS
SHIFT TO INTRACELLULAR COMPARTMENT
Kalium: fysiologie
Zuur-base afwijkingen beïnvloeden interne K+ balans.“VUISTREGEL”
K+ wisselt uit voor H+
ACIDOSE à hyperkalemieALKALOSE à hypokalemie
Interne K+ balans
12
15

Hypokalemia: pathogenesis
Causes
GLUCOSE ± INSULIN
SHIFT TO INTRACELLULAR COMPARTMENT
Kalium: fysiologie
Insuline, β-adrenerge agonisten (adrenaline), aldosteronestimuleren Na+-K+-ATPase à K+ naar intracellulair
Interne K+ balans
11
16

Hypokalemia: pathogenesis
Causes
GLUCOSE + INSULIN = essential part of treatment of diabetic keto-acidosis
SHIFT TO INTRACELLULAR COMPARTMENT
Zuur-base: pathogenese/oorzaken
16
Oorzaken DIABETISCHE KETO-ACIDOSE K(ook hyperglycemie + osm.diurese)
tekort aan insuline therapie-stopintercurrerende ziekte die insuline-nood verhoogt
overmaat aan glucagon (door wegvallen inhibitie insuline)
hoger aanbod vrije vetzuren, aminozuren, glucoseaan lever vanuit vet- en spierweefsel
high anion gap METABOLE ACIDOSE
17

Hypokalemia: pathogenesis SHIFT TO INTRACELLULAR COMPARTMENT
Zuur-base: pathogenese/oorzaken
16
Oorzaken DIABETISCHE KETO-ACIDOSE K(ook hyperglycemie + osm.diurese)
tekort aan insuline therapie-stopintercurrerende ziekte die insuline-nood verhoogt
overmaat aan glucagon (door wegvallen inhibitie insuline)
hoger aanbod vrije vetzuren, aminozuren, glucoseaan lever vanuit vet- en spierweefsel
high anion gap METABOLE ACIDOSE
Dehydratatie: pathogenese
Renale oorzaken
Osmotische diurese: rijk aan “deeltjes”
glomerulair gefilterde abnormale osmolen
exogeen: mannitol, sorbitol…endogeen: glucose (ongecontroleerde diabetes)
ureum (hoog eiwit dieet, CNI)calcium (hypercalcemie)
primair waterverlies = hyperosmolaire dehydratatie
47 18
Causes
GLUCOSE + INSULIN = essential part of treatment of diabetic keto-acidosis

Hypokalemia: pathogenesis SHIFT TO INTRACELLULAR COMPARTMENT
Zuur-base: pathogenese/oorzaken
16
Oorzaken DIABETISCHE KETO-ACIDOSE K(ook hyperglycemie + osm.diurese)
tekort aan insuline therapie-stopintercurrerende ziekte die insuline-nood verhoogt
overmaat aan glucagon (door wegvallen inhibitie insuline)
hoger aanbod vrije vetzuren, aminozuren, glucoseaan lever vanuit vet- en spierweefsel
high anion gap METABOLE ACIDOSE
Dehydratatie: pathogenese
Renale oorzaken
Osmotische diurese: rijk aan “deeltjes”
glomerulair gefilterde abnormale osmolen
exogeen: mannitol, sorbitol…endogeen: glucose (ongecontroleerde diabetes)
ureum (hoog eiwit dieet, CNI)calcium (hypercalcemie)
primair waterverlies = hyperosmolaire dehydratatie
47
Hypokalemie: pathogenese/oorzakenTE GROOT VERLIES
Oorzaken RENAALDIURETICA
koolzuuranhydrase inhibitoren (acetazolamide)
lisdiuretica (furosemide, ethacrynezuur)
thiazide diuretica (hydrochloorthiazide, chloortalidon)
osmotische diuretica
MECHANISME- Door proximaal te werken, verhogen ze flow en Na+ aanbod thv
“DISTAL K+ SECRETORY SYSTEM”
- Door daling ECF volume, stimuleren ze aldosterone vrijzetting.
inhibitie Na+ reabsorptiedoor blokkade Na+ transportin specifieke nefronsegmenten
DIURETICA
30
19
Causes
GLUCOSE + INSULIN = essential part of treatment of diabetic keto-acidosis
Hypokalemia: pathogenesis SHIFT TO INTRACELLULAR COMPARTMENT
20
Causes
GLUCOSE + INSULIN = essential part of treatment of diabetic keto-acidosis
Risk of life threatening hypokalemia as a consequence of K+ shift to intracellular compartment in already K+ depleted patient (osmotic diuresis, non-resorbable anions).
Hypokalemia: pathogenesis
Causes
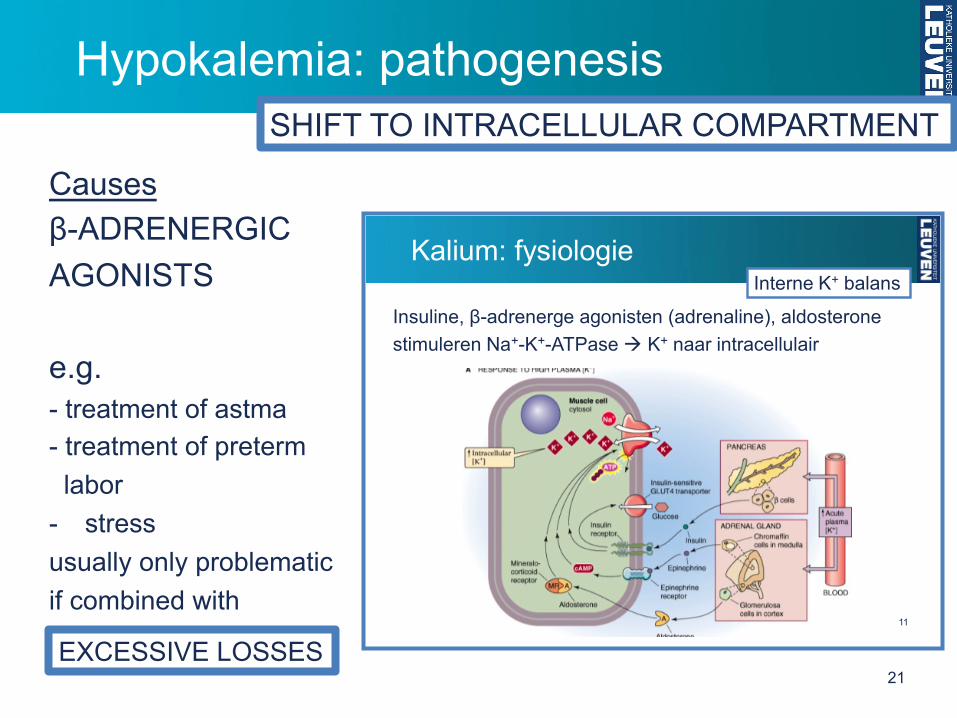
β-ADRENERGIC AGONISTS e.g. - treatment of astma - treatment of preterm labor - stress usually only problematic if combined with
SHIFT TO INTRACELLULAR COMPARTMENT
Kalium: fysiologie
Insuline, β-adrenerge agonisten (adrenaline), aldosteronestimuleren Na+-K+-ATPase à K+ naar intracellulair
Interne K+ balans
11
EXCESSIVE LOSSES 21
Hypokalemia: pathogenesis
Causes
FAMILIAL HYPOKALEMIC PERIODIC PARALYSIS
autosomal dominant defect of Ca2+ of Na+ channels in striated muscle cells (sometimes acquired form, e.g. associated with hyperthyroidism)
Attacks of painless muscle weakness, triggered by physical excercise, calory-rich meal (insuline+glucose)
Hypokalemia during attacks. Normal kalemia in-between attacks. (DD other forms of hypokalemic paralysis)
SHIFT TO INTRACELLULAR COMPARTMENT http://www.youtube.com/user/vlivings
22

Hypokalemia: pathogenesis
Causes
ANABOLIC CONDITIONS with INCREASED CELL GROWTH
uptake of K+ by “new” cells hypokalemia
e.g. treatment of anemia with Vit B12 of folic acid treatment of neurtropenia with GM-CSF
SHIFT TO INTRACELLULAR COMPARTMENT
23

Hypokalemia: pathogenesis
Causes
HIGH VOLUME TRANSFUSION OF RBC
Mechanisms - alkalosis due to preservative à hypokalemia - cold storage: Na+ K+ ATPase inhibited;
reactivation by warming à hypokalemia
SHIFT TO INTRACELLULAR COMPARTMENT
24

*reference values van lab UZ Gasthuisberg 3-2011
Hypokalemia: symptoms
25
• Definition hypokalemia: plasma [K+] < 3.5 mmol/L
(normal plasma [Na+] 3.5-5.1 mmol/L*)
• Symptoms usually only when [K+] < 3.0 mmol/L or in case of ACUTE onset.
Muscle weakness due to change of resting membrane potential (hyperpolarisation)
increased activation status of Na+ channels
Hypokalemia: symptoms
26
Muscle weakness
Striated muscle
decreased tendon reflexes paralysis (from lower limbs, through trunk to upper limbs)
rhabdomyolysis Smooth muscle nausea, anorexia abdominal distension and paralytic ileus bladder paralyse

Hypokalemia: symptoms
27
Muscle weakness Heart muscle
hyperpolarisation resting potential à increased excitability of normal pacemaker and ectopic ventricular pacemakers
prolonged action potential à slow ventricular repolarisation à prolonged relative refractory period
arrhythmias (ectopic pacemakers and reentry phenomena) VES, VFib…

Hypokalemia: symptoms
28
Muscle weakness Heart muscle
typical ECG changes ST depression, inversion T, U wave
Hypokalemia: symptoms
29
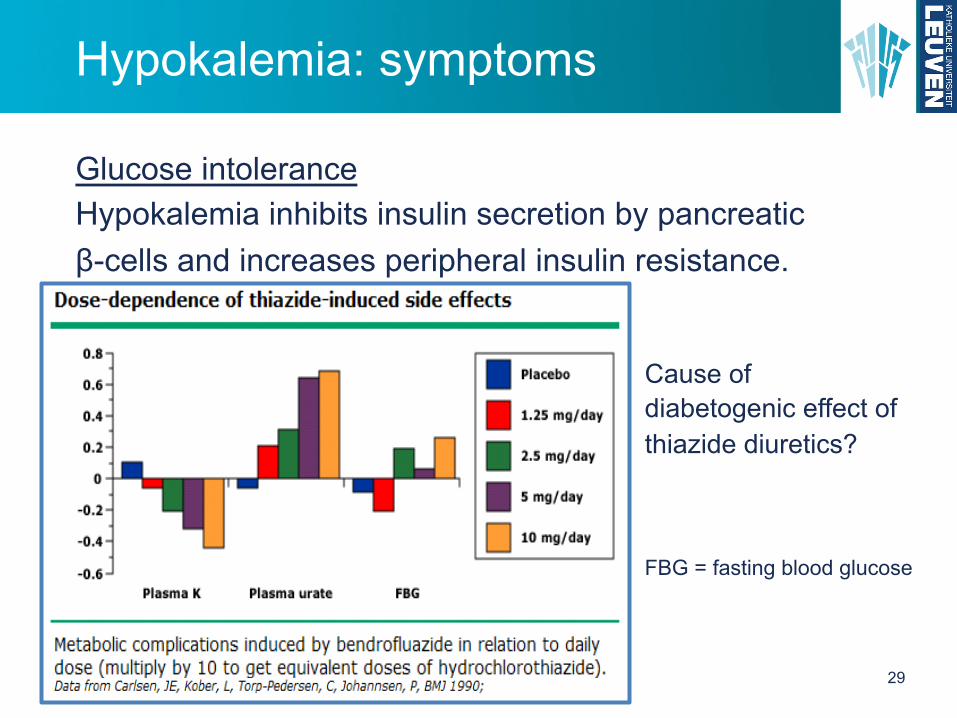
Glucose intolerance
Hypokalemia inhibits insulin secretion by pancreatic β-cells and increases peripheral insulin resistance.
Cause of diabetogenic effect of thiazide diuretics?
FBG = fasting blood glucose
Hypokalemia: symptoms
30
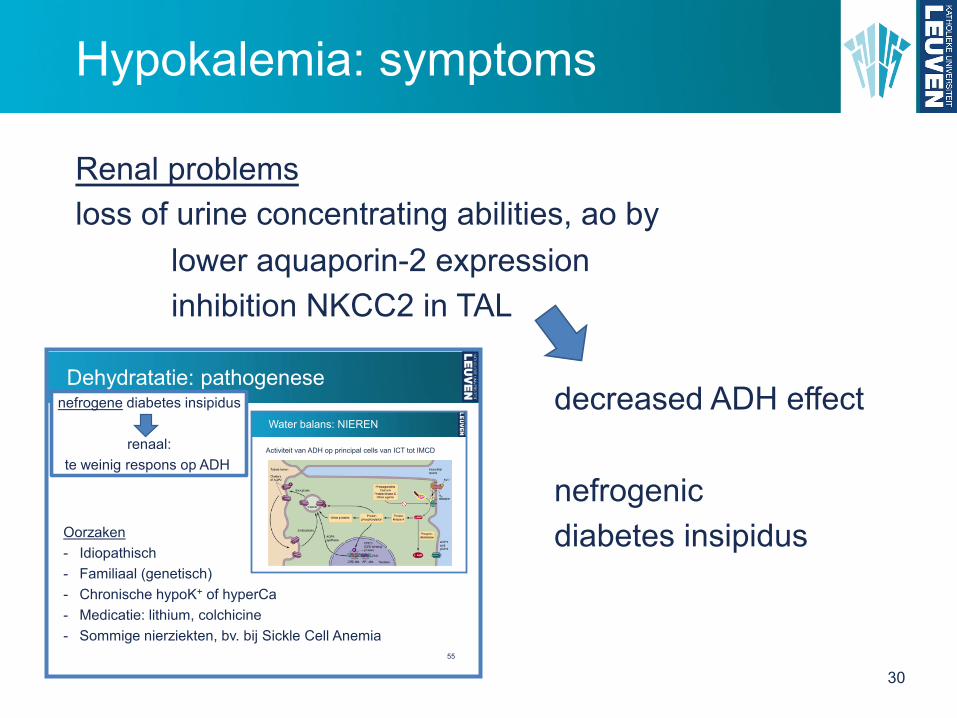
Renal problems loss of urine concentrating abilities, ao by
lower aquaporin-2 expression inhibition NKCC2 in TAL decreased ADH effect nefrogenic diabetes insipidus
Dehydratatie: pathogenese
Oorzaken- Idiopathisch- Familiaal (genetisch)- Chronische hypoK+ of hyperCa- Medicatie: lithium, colchicine- Sommige nierziekten, bv. bij Sickle Cell Anemia
nefrogene diabetes insipidus
renaal:te weinig respons op ADH
Activiteit van ADH op principal cells van ICT tot IMCD
Water balans: NIEREN
55

Hypokalemia: symptoms
31
Renal problems increased synthesis NH3, increased reabsorption HCO3
- alkalosis
Hypokalemia
• Door interne K+ balans: hypokaliemie à daling pHi
• à zelfde effect als bij chronische acidosevia (pHo en) pHi door stimulatie NHE3, electrogene H+
pomp, NBC, ammoniagene enzymes (glutaminase, PEPCK), Na/citraat cotransporterà niet-titreerbaar/titreerbaar zuur stijgt!
• K+ depletie stimuleert ook apicale K-H uitwisselaar in α-intercalated cells van ICT en CCT
(Omgekeerde effecten bij hyperkaliemie. Bovendien competitie K+ en NH4
+ voor Na/K/Cl cotransport in TAL à minder NH4+ accumulatie in
interstitium medulla)

Hypokalemia: symptoms
32
Renal problems vacuolisation tubular epithelial cells, interstitial edema interstitial nephritis
(acute and) chronic renal insufficiency

Hypokalemia: symptoms
33
Mental disturbances drowsiness, apathy, confusion, coma

Pathophysiology, diagnosis and clinical management
Bert Bammens UZ Leuven KU Leuven
Electrolyte disturbances
34
HYPOKALEMIA and K+ DEPLETION HYPERKALEMIA

*reference values van lab UZ Gasthuisberg 3-2011
Hyperkalemia
35
• Definition hyperkalemia: plasma [K+] > 5.0 mmol/L
(normal plasma [K+] 3.5-5.1 mmol/L*)
HIGH INTAKE
INSUFFICIENT (RENAL) ELIMINATION
SHIFT TO EXTRACELLULAR COMPARTMENT

Hyperkalemia: pathogenesis
36
HIGH INTAKE
Causes RARE with normal oral intake, except if combined with
thanks to early intracellular buffering followed by renal elimination.
INSUFFICIENT RENAL ELIMINATION
Kalium: fysiologie
Om extracellulaire [K+] constant te houden, is “opvang” vandeze externe kaliumbelasting nodig.
interne K+ balans = shift van K+ van extra- naar intracellulairsnel (< 1uur), “eerste opvang” voor 4/5 van K+ belasting
externe K+ balans = eliminatie van K+ uit het lichaamtrager (uren)
90-95% renaal5-10% gastrointestinaal (+ zweet)
K+ intake kan aanzienlijk groter zijn dan hoeveelheid extracellulair K+.
10

Hyperkalemia: pathogenesis
37
HIGH INTAKE
Causes Parenteral: (too fast) infusion of K+ containing substances (= iatrogenic hyperkalemia, cave renal insufficiency)
bv. kalium penicilline glucion®

Hyperkalemia: pathogenesis
38
INSUFFICIENT RENAL ELIMINATION
Causes
= insufficient K+ secretion by “DISTAL K+ SECRETORY SYSTEM”
In other words: renal insufficiency and/or low aldosterone and/or low flow / low Na+ delivery
Kalium: fysiologie
LUMINALE en PERITUBULAIRE invloeden op “DISTAL K+ SECRETORY SYSTEM”
Luminale factoren
Peritubulaire factoren
Na+ aanbod en flow thv “distal K+ secretory system”
aldosterone
zuur-base
nierfunctie
Samengevat, de belangrijkste factoren die de renale eliminatie van K+ beïnvloeden:
Externe K+ balans
32
Hyperkalemia: pathogenesis
39
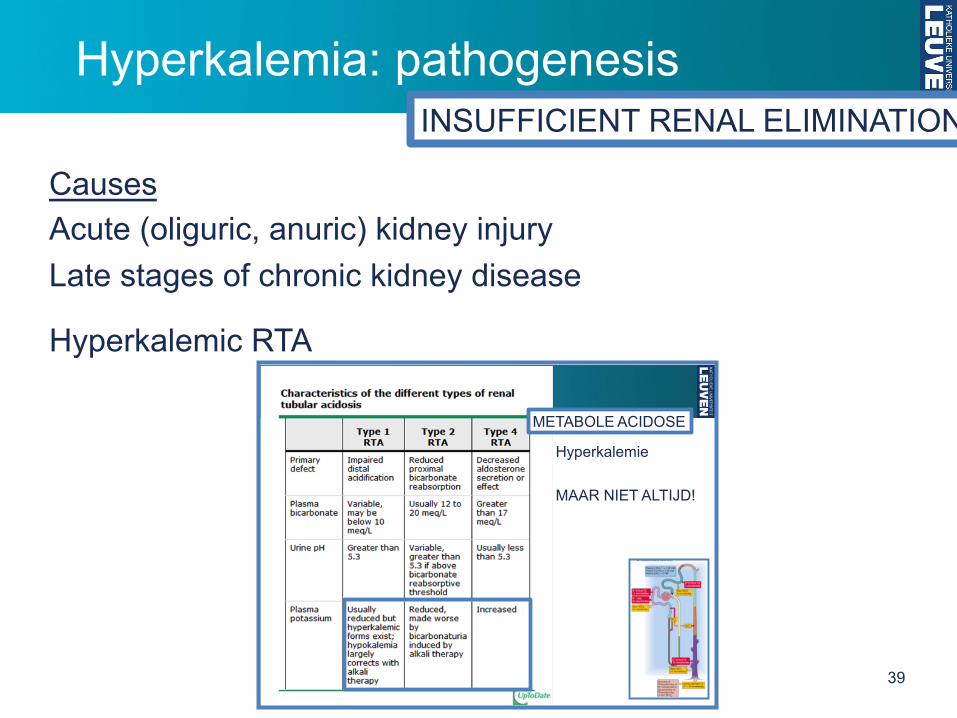
INSUFFICIENT RENAL ELIMINATION
Causes Acute (oliguric, anuric) kidney injury Late stages of chronic kidney disease
Hyperkalemic RTA
42
Hyperkalemie
MAAR NIET ALTIJD!
METABOLE ACIDOSE
Hyperkalemia: pathogenesis
40
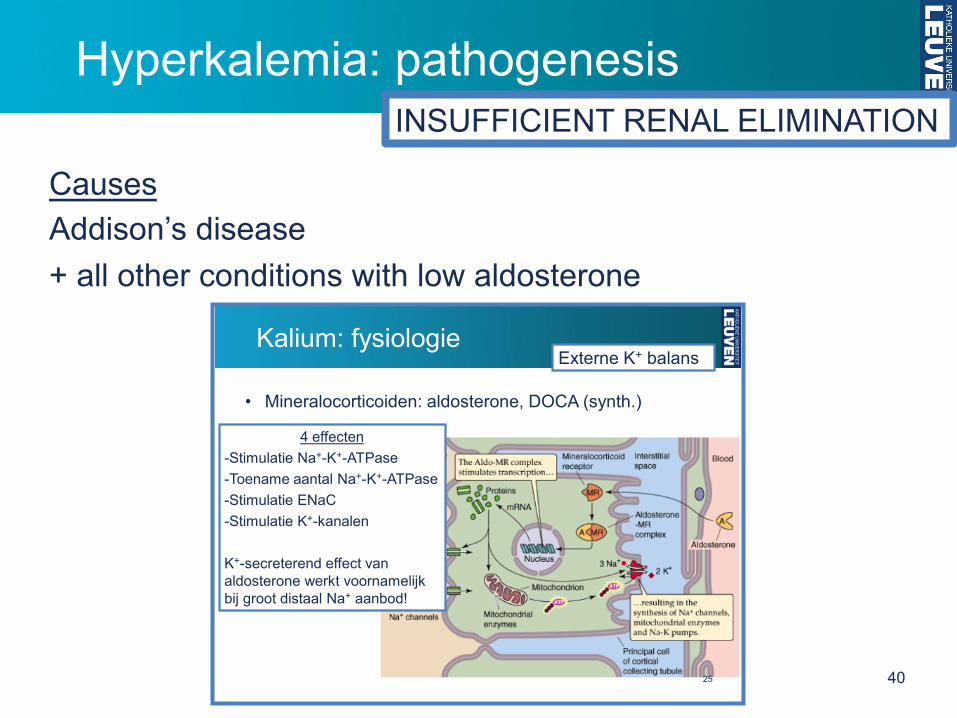
INSUFFICIENT RENAL ELIMINATION
Causes Addison’s disease + all other conditions with low aldosterone Kalium: fysiologie
• Mineralocorticoiden: aldosterone, DOCA (synth.)
4 effecten-Stimulatie Na+-K+-ATPase-Toename aantal Na+-K+-ATPase-Stimulatie ENaC-Stimulatie K+-kanalen
K+-secreterend effect van aldosterone werkt voornamelijk bij groot distaal Na+ aanbod!
Externe K+ balans
25
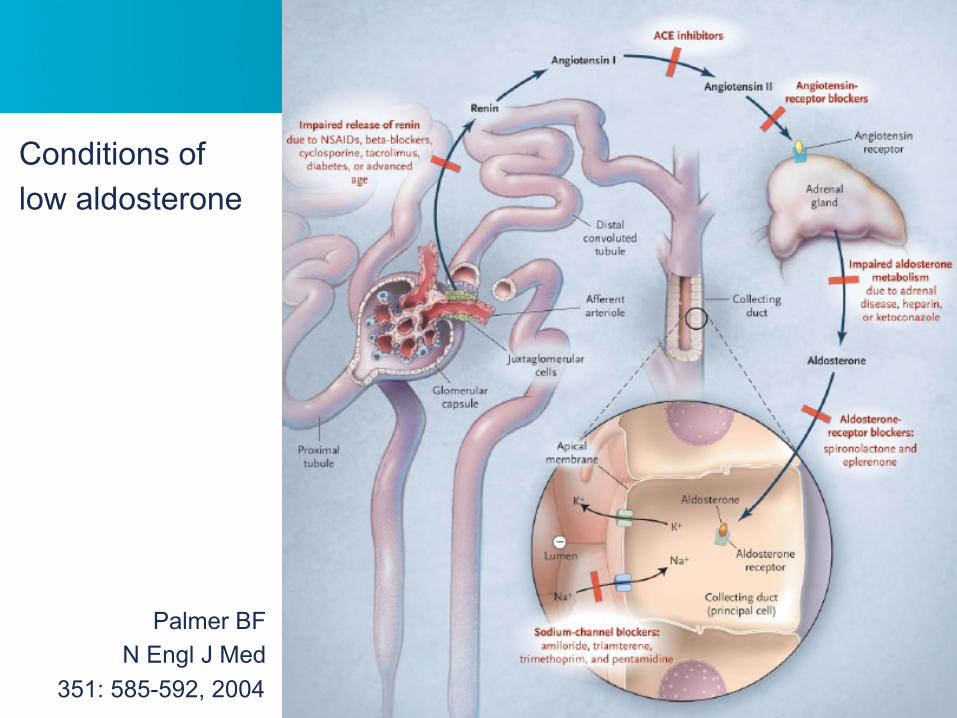
41
Conditions of low aldosterone
Palmer BF N Engl J Med
351: 585-592, 2004

Hyperkalemia: pathogenesis
42
INSUFFICIENT RENAL ELIMINATION
Causes Dehydration with low effective circulating volume
low flow and low Na+ delivery to “DISTAL K+ SECRETORY SYSTEM”
Kalium: fysiologie
• Hogere flow in lumen à K+ in lumen laag à gradientapicaal principal cells hoog à hogere K+ secretie
• Hogere flow in lumen à hoger Na+ aanbod distaalà stimulatie Na+-K+-ATPase à meer K+ secretie
Externe K+ balans
22
• Hoger Na+ in lumen à Na+ opname via ENaCà apicaal membraan depolariseert à electrische gradientstimuleert K+ secretie
• Laag Na+ in lumenà hyperpolarisatieà minder K+ secretie
• Idem bij blokkade ENaCdoor amiloride (diureticum)
Kalium: fysiologieExterne K+ balans
23

Hyperkalemia: pathogenesis
43
INSUFFICIENT RENAL ELIMINATION
Causes USUALLY MULTI-CAUSALITY!
e.g. heart failure patient with chronic use of ACE-inhibitor and spironolactone, getting dehydrated due to intercurrent illness.
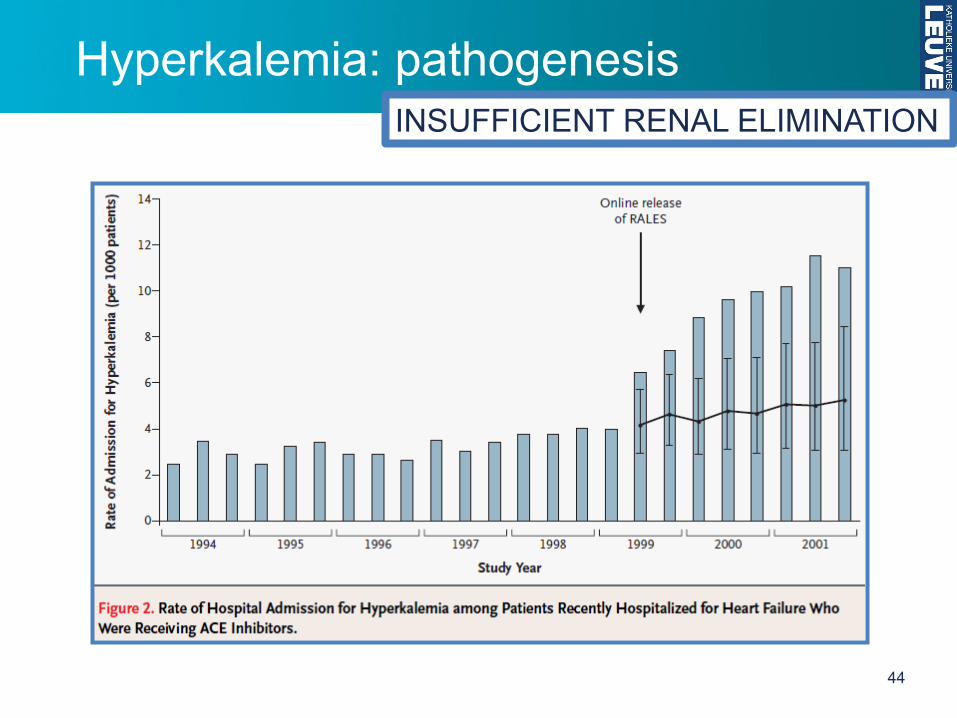
Hyperkalemia: pathogenesis
44
INSUFFICIENT RENAL ELIMINATION

Hyperkalemia: pathogenesis
45
INSUFFICIENT RENAL ELIMINATION

Hyperkalemia: pathogenesis
46
Causes ACIDOSIS
SHIFT TO EXTRACELLULAR COMPARTMENT
Kalium: fysiologie
Zuur-base afwijkingen beïnvloeden interne K+ balans.“VUISTREGEL”
K+ wisselt uit voor H+
ACIDOSE à hyperkalemieALKALOSE à hypokalemie
Interne K+ balans
12

Hyperkalemia: pathogenesis
47
Causes INSULIN RESISTANCE or LACK of INSULIN
SHIFT TO EXTRACELLULAR COMPARTMENT
Kalium: fysiologie
Insuline, β-adrenerge agonisten (adrenaline), aldosteronestimuleren Na+-K+-ATPase à K+ naar intracellulair
Interne K+ balans
11

Hyperkalemia: pathogenesis
48
Causes INSULIN RESISTANCE = why patients with or diabetic keto-acidosis may present LACK of with hyperkalemia INSULIN (despite K+ depletion)
SHIFT TO EXTRACELLULAR COMPARTMENT
Hypokalemie: pathogenese/oorzaken
OorzakenGLUCOSE + INSULINE TOEDIENING= essentieel bij behandeling diabetische keto-acidose
DUS risico op levensbedreigende hypokalemiedoor shift van K+ naar intracellulair bij patiënten dievaak reeds een K+ depletie hebben ontwikkeld!
SHIFT NAAR INTRA-CELLULAIR
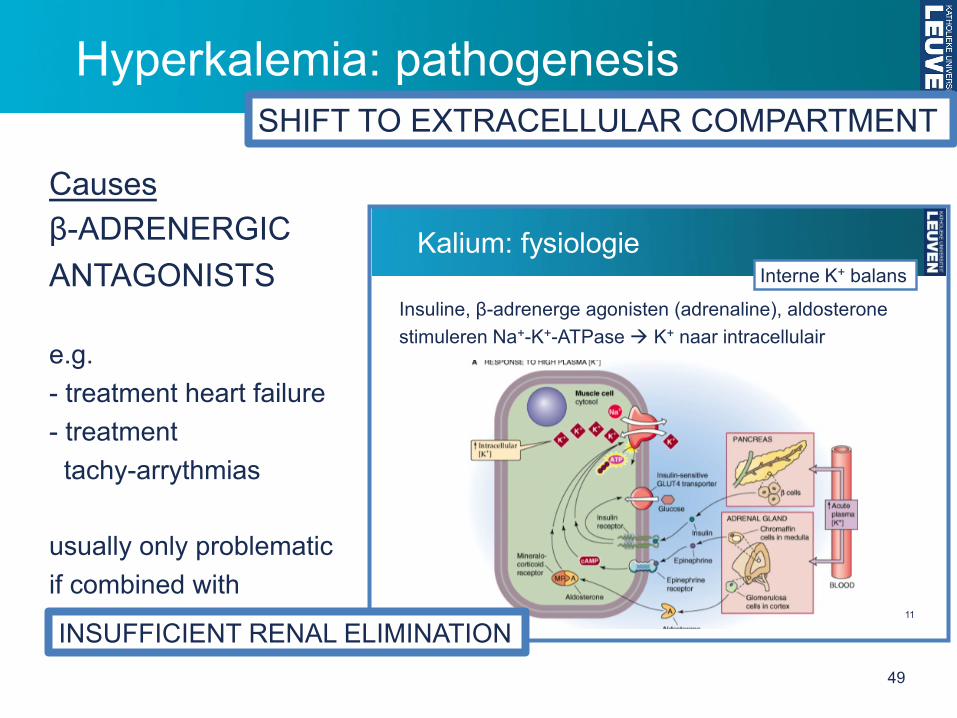
Hyperkalemia: pathogenesis
49
Causes β-ADRENERGIC ANTAGONISTS e.g. - treatment heart failure - treatment tachy-arrythmias usually only problematic if combined with
SHIFT TO EXTRACELLULAR COMPARTMENT
Kalium: fysiologie
Insuline, β-adrenerge agonisten (adrenaline), aldosteronestimuleren Na+-K+-ATPase à K+ naar intracellulair
Interne K+ balans
11
INSUFFICIENT RENAL ELIMINATION

Hyperkalemia: pathogenesis
50
Causes CELL- or TISSUE INJURY
bv. intravascular hemolysis tumorlysis syndrome physical exercise crush syndrome
SHIFT TO EXTRACELLULAR COMPARTMENT

Hyperkalemia: pathogenesis
51
Causes PSEUDOHYPERKALEMIA K+ leaves cells after blood sample has been taken
e.g. traumatic venipuncture long interval between sampling and analysis thrombocytosis or leucocytosis (release during clotting)
hereditary spherocytosis (temperature dependent K+ leakage)
SHIFT TO EXTRACELLULAR COMPARTMENT

Hyperkalemia: pathogenesis
Causes
FAMILIAL HYPERKALEMIC PERIODIC PARALYSIS
usually autosomal dominant defect of Na+ channels striated muscle cells
Attacks of painless paralysis, sometimes triggered by cold, recovery after physical excercise, fasting, ingestion of K+
Slight hyperkalemia during attacks (or normal [K+]) Normokalemia in-between attacks.
SHIFT TO EXTRACELLULAR COMPARTMENT
52
*reference values van lab UZ Gasthuisberg 3-2011
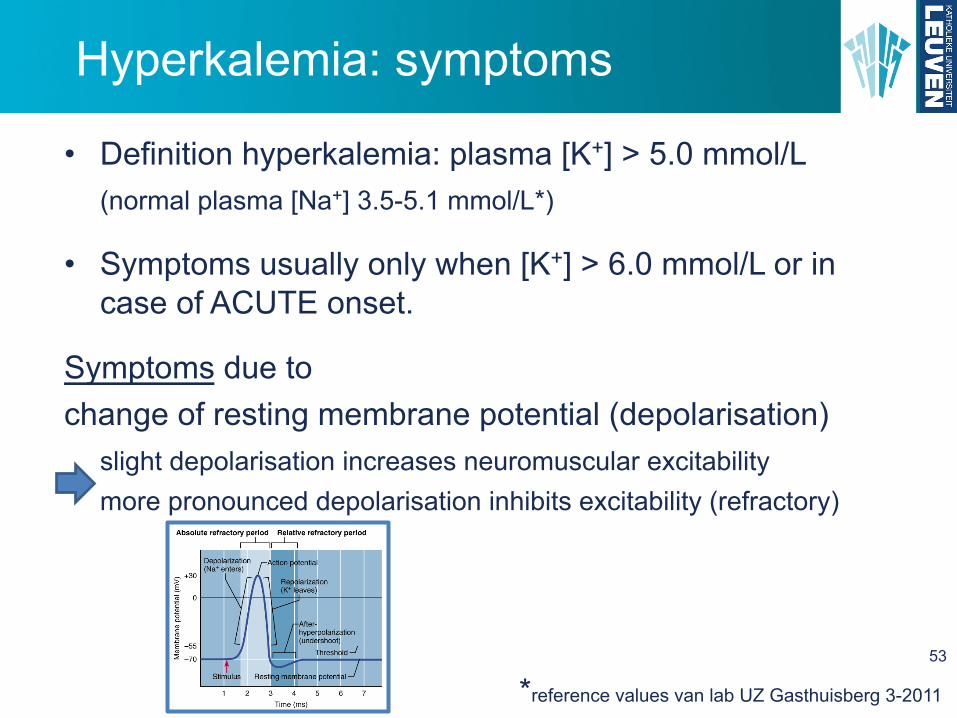
Hyperkalemia: symptoms
53
• Definition hyperkalemia: plasma [K+] > 5.0 mmol/L
(normal plasma [Na+] 3.5-5.1 mmol/L*)
• Symptoms usually only when [K+] > 6.0 mmol/L or in case of ACUTE onset.
Symptoms due to change of resting membrane potential (depolarisation)
slight depolarisation increases neuromuscular excitability more pronounced depolarisation inhibits excitability (refractory)

Hyperkalemia: symptoms
54
Muscle weakness
Striated muscle
muscle weakness paralysis (lower limbs, through trunk up to upper limbs)

Hyperkalemia: symptoms
55
Heart muscle
depolarisation resting potential à decreased excitability normal pacemaker more ectopic ventricular pacemakers
arrhytmias (ectopic pacemakers and reentry phenomena) VES, VFib…
Hyperkalemia: symptoms
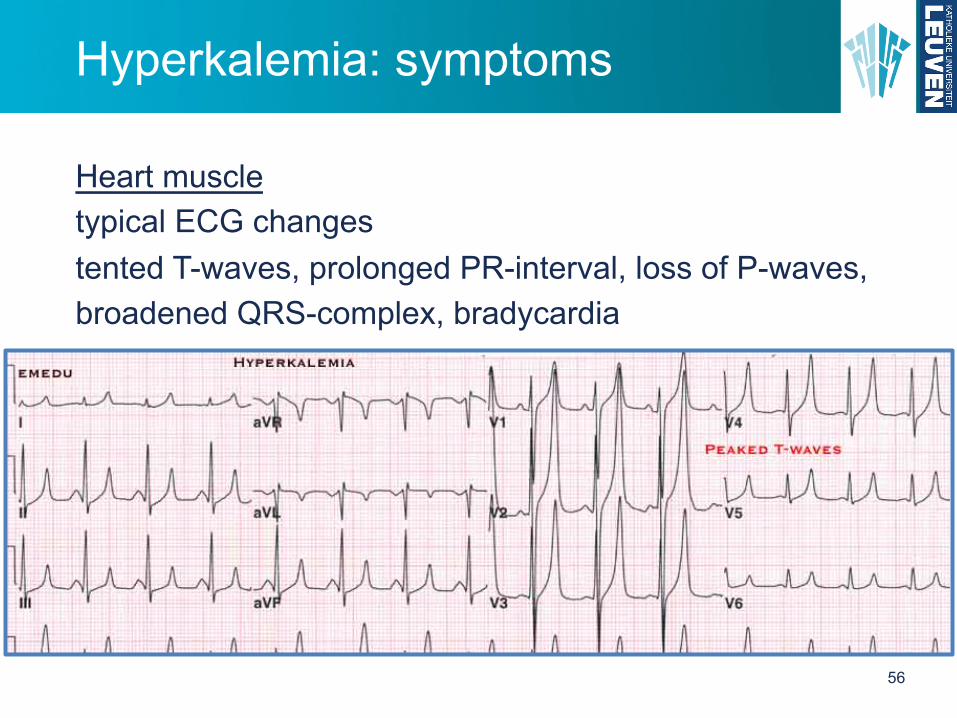
56
Heart muscle
typical ECG changes tented T-waves, prolonged PR-interval, loss of P-waves, broadened QRS-complex, bradycardia
Hyperkalemia: symptoms
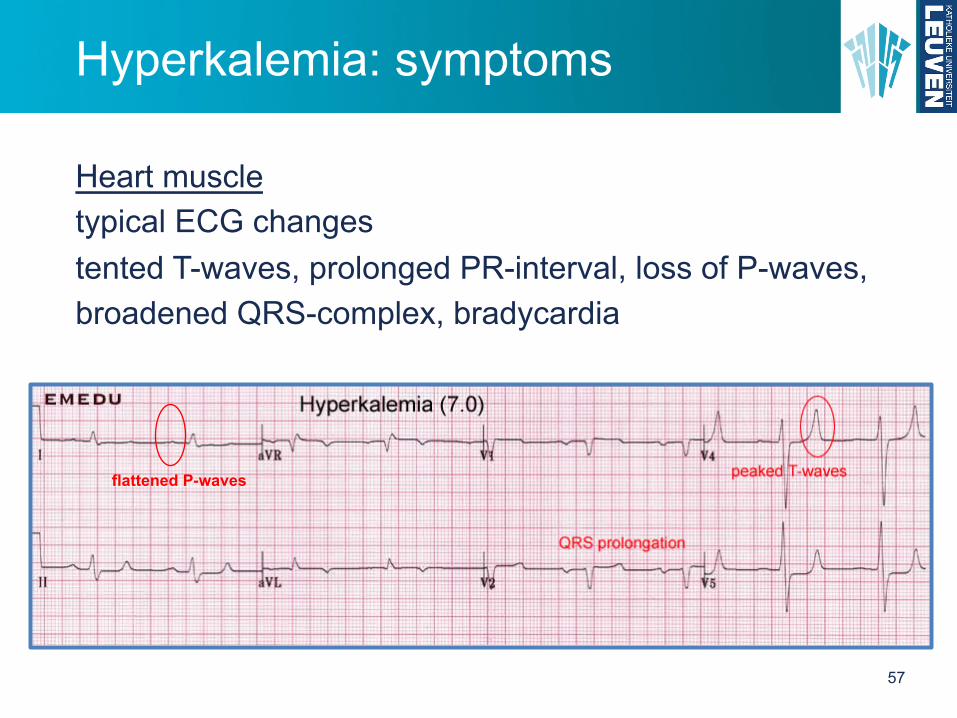
57
flattened P-waves
Heart muscle
typical ECG changes tented T-waves, prolonged PR-interval, loss of P-waves, broadened QRS-complex, bradycardia

Hyperkalemia: symptoms
58
Heart muscle
typical ECG changes

Hyperkalemia: symptoms
59
Renal problems decreased NH3 synthesis, decreased reabsorption HCO3
- acidosis
Hypokalemia
• Door interne K+ balans: hypokaliemie à daling pHi
• à zelfde effect als bij chronische acidosevia (pHo en) pHi door stimulatie NHE3, electrogene H+
pomp, NBC, ammoniagene enzymes (glutaminase, PEPCK), Na/citraat cotransporterà niet-titreerbaar/titreerbaar zuur stijgt!
• K+ depletie stimuleert ook apicale K-H uitwisselaar in α-intercalated cells van ICT en CCT
(Omgekeerde effecten bij hyperkaliemie. Bovendien competitie K+ en NH4
+ voor Na/K/Cl cotransport in TAL à minder NH4+ accumulatie in
interstitium medulla)
Hypokalemia
• Door interne K+ balans: hypokaliemie à daling pHi
• à zelfde effect als bij chronische acidosevia (pHo en) pHi door stimulatie NHE3, electrogene H+
pomp, NBC, ammoniagene enzymes (glutaminase, PEPCK), Na/citraat cotransporterà niet-titreerbaar/titreerbaar zuur stijgt!
• K+ depletie stimuleert ook apicale K-H uitwisselaar in α-intercalated cells van ICT en CCT
(Omgekeerde effecten bij hyperkaliemie. Bovendien competitie K+ en NH4
+ voor Na/K/Cl cotransport in TAL à minder NH4+ accumulatie in
interstitium medulla)

Hyperkalemia: symptoms
60
Mental disturbances drowsiness, apathy, confusion, coma
Hyperkalemia: treatment
61
Indication depends on severity of symptoms. But actively look for symptoms if >6 mmol/L. Ca2+ to “stabilize” the membrane of cardiac muscle cells Insulin + glucose Bicarbonate Beta-2-adrenergic agonists Diuretics (loop and thiazide) Rehydration Dialysis Resins (cation exchangers)


















