PATHOLOGY LABORATORY MANUAL · Web viewDifferentiate acute versus chronic anemia of blood loss....
24
GOALS AND OBJECTIVES: Upon completion of this section, the student will be able to: 1. Describe clinical presentation, common symptoms and physical examination findings in patients with anemia. 2. Generate a differential diagnosis for an anemia case, based on laboratory findings as well as peripheral blood smear examination. 3. Identify the most common pathologic (abnormal) red blood cell morphologies. 4. Describe the pathophysiology of the main types of anemia (hemolytic and anemia of acute blood loss). 5. Differentiate acute versus chronic anemia of blood loss. 6. Recognize that in acute blood loss anemia, the main goal is to restore intravascular volume (not RBCs). 7. Describe in detail all the laboratory tests available in clinical laboratories to further diagnose the etiology of a specific anemia case. 8. Discuss the genetic and clinical features of sickle cell anemia and known complications. 9. Discuss hemostasis . 10. Describe clinical presentation, common symptoms and physical examination findings in patients with bleeding disorders. 11. Define the diagnostic approach to follow when evaluating a bleeding patient. 12. Identify the most common laboratory tests used for the diagnosis of bleeding disorders. 13. Describe the clinical presentation, common symptoms and physical examination findings in patients with thrombotic microangiopathic disorders. 14. Define the diagnostic approach to follow when evaluating a patient with a thrombotic microangiopathic disorder. 15. Recognize the most common laboratory tests used for the diagnosis of a thrombotic microangiopathic disorder. MANDATORY READING: 1. Robbins Pathologic Basis of Disease (9 th edition) a. Anemias of blood loss, page 631 b. Hemolytic Anemias (Hereditary Spherocytosis, Glucose-6-Phospate Dehydrogenase deficiency and Sickle cell anemia), pages 631-638. c. Immunohemolytic anemias, pages 643-644 d. Hemorrhagic diathesis related to abnormalities in clotting factors (The factor VIII-vWF Complex, Von Willebrand disease, Hemophilia A and Hemophilia B), pages 661-663 e. Bleeding disorders: Hemorrhagic diatheses (Bleeding disorders caused by vessel wall abnormalities, bleeding related to reduced platelet number: thrombocytopenia, chronic immune thrombocytopenic purpura (ITP), acute immune thrombocytopenic purpura, drug-induced thrombocytopenia, HIV CPC #2, INSTRUCTOR HANDOUT HEM-ONC 1
Transcript of PATHOLOGY LABORATORY MANUAL · Web viewDifferentiate acute versus chronic anemia of blood loss....

GOALS AND OBJECTIVES:
Upon completion of this section, the student will be able to:
1. Describe clinical presentation, common symptoms and physical examination findings in patients with anemia. 2. Generate a differential diagnosis for an anemia case, based on laboratory findings as well as peripheral blood
smear examination. 3. Identify the most common pathologic (abnormal) red blood cell morphologies. 4. Describe the pathophysiology of the main types of anemia (hemolytic and anemia of acute blood loss).5. Differentiate acute versus chronic anemia of blood loss.6. Recognize that in acute blood loss anemia, the main goal is to restore intravascular volume (not RBCs).7. Describe in detail all the laboratory tests available in clinical laboratories to further diagnose the etiology of a
specific anemia case. 8. Discuss the genetic and clinical features of sickle cell anemia and known complications.9. Discuss hemostasis.10. Describe clinical presentation, common symptoms and physical examination findings in patients with bleeding
disorders. 11. Define the diagnostic approach to follow when evaluating a bleeding patient.12. Identify the most common laboratory tests used for the diagnosis of bleeding disorders. 13. Describe the clinical presentation, common symptoms and physical examination findings in patients with
thrombotic microangiopathic disorders.14. Define the diagnostic approach to follow when evaluating a patient with a thrombotic microangiopathic disorder.15. Recognize the most common laboratory tests used for the diagnosis of a thrombotic microangiopathic disorder.
MANDATORY READING: 1. Robbins Pathologic Basis of Disease (9th edition)
a. Anemias of blood loss, page 631b. Hemolytic Anemias (Hereditary Spherocytosis, Glucose-6-Phospate Dehydrogenase deficiency and Sickle cell
anemia), pages 631-638.c. Immunohemolytic anemias, pages 643-644 d. Hemorrhagic diathesis related to abnormalities in clotting factors (The factor VIII-vWF Complex, Von Willebrand
disease, Hemophilia A and Hemophilia B), pages 661-663e. Bleeding disorders: Hemorrhagic diatheses (Bleeding disorders caused by vessel wall abnormalities, bleeding
related to reduced platelet number: thrombocytopenia, chronic immune thrombocytopenic purpura (ITP), acute immune thrombocytopenic purpura, drug-induced thrombocytopenia, HIV associated thrombocytopenia, thrombotic microangiopathies, bleeding disorders related to defective platelet functions), pages 656-661
f. Bilirubin and Bile formation (Ch. 18): pages 852-853
2. Lecture notes:a) Anemia II Online Module/Lectures (Dr. Cannaday)b) Coagulation Online Module/Lectures (Dr. Cannaday)
3. Mandatory Paper: A blood mystery. The New England Journal of Medicine. Novemeber 5, 2009; 361:1887-94. Adam Cuker,M.D., Jean M. Connors,M.D., Joel T.Katz, M.D., Bruce D. Levy,M.D., and Joseph Loscalzo,M.d.,Ph.D.
CPC #2, INSTRUCTOR HANDOUT
HEM-ONC
1

Case #1: “A 52-year-old woman with increasing fatigue” AUTOIMMUNE IDIOPATHIC HEMOLYTIC ANEMIA
CLINICAL HISTORY: This is a 52-year-old African American woman who reports a 2-months history of increasing fatigue, as well as dyspnea upon exertion. Review of systems reveals some bilateral ankle swelling as well. The patient otherwise denies any significant past medical history. Her vital signs are as follows: Temp 98.1 F, Pulse 106/min and blood pressure 140/78 mmHg. Physical examination is significant for mildly jaundiced sclera and mucosal pallor.
Cardiopulmonary exam shows systolic murmur at the apex, cardiomegaly, inspiratory rales over both lung bases and 2+ pitting edema in her ankles. A complete blood count is drawn and the results reveal the following:
Test Result Reference range
White blood cells (leukocyte count) 11.0 4.8-10.8 thou/uL
Hemoglobin 5.2 12-16g/dL
Hematocrit 18 36-47%
Mean Corpuscular Volume (MCV) 100 81-99 fl
Mean Corpuscular Hemoglobin (MCH) 34 27-31 pg
Mean Corpuscular Hemoglobin Concentration (MCHC) 38 32-36 g/dL
Red Cell Distribution Width (RDW) 15 11.5-14.5%
Platelet count 230 130-400 thou/uL
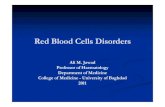
Peripheral Blood smear (see image below)
2

References (from mandatory readings) for this case
a. Lecture: Anemia II Online Module/Lectures (Dr. Cannaday), Wednesday July 26th, 8-9:30 amb. Lecture: Immunohematology Lecture (Dr. Linz), Tuesday, August 1, 9-10 amc. Robbins Pathologic Basis of Disease (9th edition), Hemolytic Anemias, Hereditary Spherocytosis, Glucose-6-Phospate
Dehydrogenase deficiency: pages 631-634, Immunohemolytic anemias, pages 643-644 and Bilirubin and Bile formation (Ch. 18): pages 852-853
Clinical Features and Pathophysiology relevant from this clinical history
1. What do the constellation of symptoms of dyspnea on exertion, rales heard at lower lung bases, heart murmur, cardiomegaly and 2+ edema indicate or point to? Why is the patient presenting with this? Congestive heart failure, this is a result from severe chronic anemia
2. How would you characterize this anemia? Severe, normocytic normochromic, likely hemolytic (based on jaundice and sphereocytes on PBS)
3. What does the mild jaundiced sclera indicate and what labs could help support your suspicion? Hemolysis; can do LDH levels and indirect bilirubin, both of which will be elevated
4. Briefly illustrate bilirubin metabolism and how jaundice is produced: Bilirubin metabolism and elimination: (1) Normal bilirubin production from heme (0.2 to 0.3 gm/day) is derived primarily from the breakdown of senescent circulating erythrocytes. (2) Extrahepatic bilirubin is bound to serum albumin and delivered to the liver. (3) Hepatocellular uptake and (4) glucuronidation in the endoplasmic reticulum generates bilirubin monoglucuronides and diglucuronides, which are water soluble and readily excreted into bile. (5) Gut bacteria deconjugate the bilirubin and degrade it to colorless urobilinogens. The urobilinogens and the residue of intact pigments are excreted in the feces, with some reabsorption and excretion into urine. Unconjugated (indirect) bilirubin is insoluble and not excreted in the urine, hence causes jaundice.
3

5. What is the expected life span of a red blood cell? How is that affected in hemolytic anemia? 100-120 days; reduced to 30-40 days
6. What do you expect with a patient who is presenting with acute intravascular hemolysis? (mention at least 3): Hemoglobinemia, hemoglobinuria, hemosidreinuria, low/depleted haptoglobin levels, oxidization of excess free hemoglobin into methemoglobin
7. What do you expect from a patient presenting with extravascular hemolysis? Possibly just a drop in hemoglobin and splenomegaly
8. List causes of hemolytic anemia (organize by mechanism, e.g. RBC structure vs hemoglobinopathies etc.). List as many causes and specific diseases as you can:
o Problem Intrinsic to RBC Hemoglobinopathies
e.g. HbS causing Sickle Cell Anemia Thalassemia (presenting with severe and significant hemolysis)
e.g. β–thalassemia major RBC Membrane Defects
e.g. Hereditary Spherocytosis, Elliptocytosis, Stomatocytosis
4
Cannaday, Rania A., 06/18/19,
Yun, this question maybe good for a matching or drop and drag etc.

RBC Enzyme Defect e.g. G-6-PD deficiency, Pyruvate Kinase deficiency
Paroxysmal Nocturnal Hemoglobinuria- PNH (acquired d/o)
o Problem Extrinsic to RBC Immunohemolytic Anemia Microangiopathic Hemolytic Anemia- MAHA
Vessel is diseased or mechanical injury through an artificial heart valve Parasites
e.g. Malaria 9. Based on the clinical information given above (including laboratory findings and peripheral
blood smear), which hemolytic anemias can you exclude, which are unlikely and why? (make 2 lists of “excluded” and “unlikely” and list reasons next to each): Excluded list: Sickle cell anemia (no sickle cells, presents in childhood), Thalassemia (microcytic anemia, also should present in childhood if causing severe hemolysis like beta thalassemia major), MAHA like TTP (no thrombocytopenia, fever, neurological symptoms, no schistocytes), DIC (no thrombocytopenia, no bleeding or coagulopathy), Malaria (no fever). Unlikely list: PNH (no evidence of thrombosis), Vessel damage (no clinical clues to point to it)
10. Based on the clinical information given above (including laboratory findings and peripheral blood smear), which causes of hemolytic anemias would you include in your differential diagnosis? Entities causing RBC membrane defects like Hereditary Spherocytosis and also immunohemolytic anemia. Can consider entities causing RBC enzyme defects like G-6-PD deficiency (although presence of spherocytes do not favor this diagnosis).
Laboratory Questions:
11. What further laboratory tests would you order in this patient to confirm hemolytic anemia and what do you expect for each value (mention at least 4)?: Reticulocyte (calculate retic index) will be high >3%, LDH- will be high, bilirubin (indirect)- will be high, haptoglobin- will be low, Urine analysis (UA)- to check for presence of hemoglobinuria, hemosidreinuria
12. What further laboratory tests would you order to further narrow down your differential diagnosis from the question above? For HS: osmotic fragility test, flow cytometry and mutational analysis. For immune mediated: direct and indirect antiglobulin test, cold agglutinin titer, complement levels. For G6PD deficiency: G6PD screen/quantitative assay; also use PBS with bite cells or crystal violet to see Heinz bodies
13. Describe how a direct and indirect antiglobulin tests are performed: General Principal: DAT to check for antibodies that are directly attached to the RBC; answers the question “is there an autoantibody”?! IAT checks for antibodies in the serum and can identify types.
5

14. In what entities do you expect to see a positive DAT (hint: check Immunohematology lecture by Dr. Linz): Autoimmune diseases, immunohemolytic anemia, transfusion reactions, hemolytic disease of the newborn
15. What is cause of the slight increase in MCHC (hint: look at the PBS)? Spherocytes have less volume therefore the mean corpuscular volume concentration will be increased
16. List mutations in which red blood cell membrane skeletal proteins are most commonly responsible for causing hereditary spherocytosis? Ankyrin, Spectrin, Band 3 and Band 4.2
17. List the function of G-6-PD enzyme in the normal healthy state: This enzyme maintains adequate intracellular “reduced glutathione” pools and therefore has a role to defend against oxidative injury
Microscopic questions:
18. Describe the red blood cells on the PBS: Some normochromic, normocytic red blood cells, many spherocytes, evidence of reticulocytes
19. What term is used to describe the “color” of red blood cells on PBS, when there is an increase in reticulocytes? Polychromasia
20. The spleen acts as a testing ground of red blood cell flexibility and variability. The spleen also has a trapping/filtering function, which allows it to remove RBC inclusions and denatured hemoglobin within red blood cells. Name an RBC inclusion and denatured hemoglobin substance and which diseases are they associated with: Howell Jolly bodies (HS) and Heinz bodies (G6PD deficiency)
21. In which other disease entity are spherocytes seen (in addition to hereditary spherocytosis)? Immunohemolytic anemia
6

Additional laboratory findings:
Further laboratory testing is obtained. Reticulocyte index is >3% and LDH/indirect bilirubin are elevated, all indicating hemolysis. For practical purposes, DAT and presence of warm or cold antibody should be done immediately. The blood bank reports a DAT positive for anti-IgG and negative for anti-C3. A cold agglutinin titer was low. The patient is diagnosed with a “warm antibody” autoimmune idiopathic hemolytic anemia (AIHA) and immediate intervention with immunosuppressive therapy is started. Red blood cell transfusion is a consideration. Splenectomy can be done in cases refractive to treatment.
7

Case #2: “A 29 yo Asian man with significant blood loss after an MVA” ACUTE BLOOD LOSS ANEMIA
CLINICAL HISTORY: A 29-year-old Asian man is brought into the emergency department by an ambulance after sustaining significant blood loss in a motor vehicle accident (MVA) from a deep laceration to his left thigh. EMT personnel have applied pressure to the wound and started saline drip intravenously. The patient’s vital signs in the field were as follows: Temperature 98.0 F, Pulse 120/min, BP 108/62 mmHg, respiratory rate 22/min. In the ED, the patient appears pale and anxious. He is breathing rapidly. He is otherwise awake, oriented and answering questions. He denies any significant past medical history or drug allergies. A second set of vitals are done supine and show the following: Pulse 130/min, BP 100/54 mmHg, respiratory rate 24/min. Upon sitting up, the patient feels very faint and repeat BP is now 60/40 mmHg. At this point, a second IV line is started with infusion of lactate ringer at maximum rate. Simultaneously, blood is drawn for a STAT type and crossmatch for 4 Units of red blood cells, and CBC/coagulation profile is ordered. The patient’s vitals are now monitored continuously and surgery is consulted.
References (from mandatory readings) for this case
a. Robbins Pathologic Basis of Disease (9th edition), Anemias of Blood Loss: page 631
Clinical Features relevant from this clinical history:
1. What is the principal cause of this patient’s symptoms (i.e. pale, anxious, low blood pressure, faint etc. hint: it is not simply RBC loss…)? Loss of intravascular volume
2. What are the terminal consequences of acute massive blood loss in a bleeding patient? Cardiovascular collapse, shock (shutting down of organs e.g. anuria etc.) and ultimately death.
3. What is the term given for his blood pressure findings? Orthostatic hypotension4. Is it more beneficial to immediately give this patient a red blood cell transfusion, or intravenous
fluids? In acute blood loss, the main goal is to RESTORE INTRAVSCULAR VOLUME, so give IV fluids first.
Laboratory and Pathophysiology Questions:
5. What do you expect to see for the white blood cell count and platelet count as the patient recovers from blood loss? Leukocytosis and thrombocytosis, respectively
6. Describe the red blood cells on PBS for a patient at the time of bleeding? Initially, the red blood cells are normochromic and normocytic
7. How will the PBS change as the patient recovers from the bleeding? And why? There will be an increase in reticulocytes as the bone marrow compensates to make more red blood cells. Low oxygen, triggers increase in erythropoietin
8. What % reticulocytes do you expect in a patient, 5-7 days after acute massive hemorrhage? 10-15% 9. How is the anemia of acute blood loss different from the anemia of chronic blood loss? Acute blood
loss will have hemodilution with low hematocrit due to the shift of water from interstitial space to restore intravascular volume. Also early there is normocytic, normochromic RBCs. Later there is reticulocytosis. Anemia of chronic blood loss will cause loss and depletion of iron stores and result in iron deficiency anemia
8

Two Bonus Questions:
10. The patient’s blood type returns O negative and during surgical intervention he needs to get an RBC transfusion. The blood bank has all blood types except for O negative RBCs. Which RBC type would you transfuse to this patient, given O negative is not available? O positive
11. The bone marrow response to acute blood loss is slow but circulating red blood cells can quickly compensate by increasing their transfer of oxygen to tissues. Which way do you expect the hemoglobin-oxygen dissociation curve to shift to (right or left?) and what do you expect to happen to the levels of 2,3-diphosphoglycerate (increase or decrease) Hint: check RBC physiology handout? Right shift. 2,3-DPG will increase to help unload more oxygen
9

Case #3: “An 8-year-old African American boy coming to the ER” SICKLE CELL ANEMIA WITH ACUTE CHEST SYNDROME
CLINICAL HISTORY: This is an 8-year-old African American boy who is brought to the emergency department with severe pain in his back and chest. He was brought in by his summer camp manager and his parents have not yet arrived. He is in severe pain and is unable to answer most of your questions. He did not bring any medications to the camp nurse on his arrival to the camp. Vital signs: Temperature 100.9 F, Pulse 115/min, BP 118/68 mmHg, Oxygen saturation 89% on 2L nasal cannula. His physical examination reveals that he is in moderate distress and in visible pain. He is curled up on the bed grimicing and moaning. His respiratory exam is signficant for shallow inspiration, mildly decreased breath sounds bilaterally but with no wheezes, rales, or rhonchi. Lastly, abdominal examination reveals mild splenomegly. Relevant labortory data show Hemoglobin: 5.8 g/dL, Hematocrit: 19% and Mean Corpuscular Volume (MCV): 75 µm3.
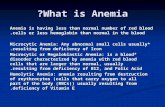
Peripheral Blood smear (see image below)
References (from mandatory readings) for this case
a. Lecture: Anemia II Online Module/Lectures (Dr. Cannaday), Wednesday July 26th, 8-9:30 amb. Robbins Pathologic Basis of Disease (9th edition), Sickle cell Anemia: pages 635-638
Clinical Features relevant from this clinical history
1. What is the most likely cause (pathophysiology) of the boy’s chest pains? Ischemia of post capillary tissue due to sickling of red blood cells in low oxygen tension
2. Why is there splenomegaly on physical exam? Hemolysis causes increase in erythropoiesis and extramedullary hematopoiesis causing splenomegaly
3. What crisis has been described in children due to the big spleen? Splenic sequestration crisis
10

4. Do you expect to see splenomegaly in an adult patient with sickle cell disease? And what is the term used to describe the spleen in the adult patient: No. Autoinfarction occurs. Terms: autosplenectomy or functional asplenia
5. What are the consequences of functional asplenia: Predisposition to infections by encapsulated microorganisms
6. How will this patient be managed immediately and long term? Patient is unstable with acute chest syndrome and needs emergent exchange transfusion. Other measures would be hydration and pain control. Look for infection and treat accordingly. Long term management with folic acid and hydroxyurea.
7. If untreated, what are the consequences of acute chest syndrome? Vicious cycle of hypoxemia, more sickling and eventually death
8. What do you expect to see on chest x-ray of a patient with acute chest syndrome? New pulmonary infiltrates
9. Aplastic crisis can occur in patients with chronic hemolytic anemia such as sickle cell disease. What is the name of the infectious agent? Parvovirus B19
10. What is the life span of sickled red blood cells? 10-20 days11. List some triggers of sickle cell disease crises: Hypoxemia, dehydration, infections, acidosis,
increased altitude, pregnancy or sometimes no trigger is found12. How does hydroxyurea work? Increases HbF and a tetramer ααβsγ forms- does not
polymerize, therefore protective and decrease in vaso-occulsive crisis has been shown
Additional laboratory findings:
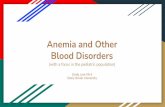
Hemoglobin electrophoresis would be done to establish the diagnosis of sickle cell disease- below is an example of what this patient’s would look like (lane 6) if performed:
Laboratory Questions:
13. How much HbA versus HbS does a patient with genotype SS has? HbA: 0. HbS: 76-98%14. How much HbA versus HbS does a patient with genotype AS has? HbA: 60%. HbS: 35-40%15. When a patient with sickle cell disease (genotype SS) receives an exchange transfusion, how
low do you want to reduce their HbS levels to? 30-40%
Microscopic questions:
11

16. What is the cellular defect seen in the atypical red blood cells on the PBS and what is the result of the mutation? Point mutation in the beta-globin chain, glutamic acid to valine point mutation
17. Besides sickle cells seen on PBS, what else do you expect to see? Target cells, nucleated red blood cells, Howell-Jolly bodies, reticulocytosis (polychromasia), nucleated RBC
12

Case #4: “A 65 yo Caucasian man with bruising and severe arm pain” ACQUIRED HEMOPHILIA- FACTOR VIII INHIBITOR
CLINICAL HISTORY: This is a 65-year-old Caucasian man who comes to clinic today for bruising and severe right arm pain for the past day. His past medical history is significant for hypertension that is controlled with HCTZ (hydrochlorothiazide), non-insulin dependent diabetes mellitus, for which he takes glyburide. The remainder of his ROS is negative. Vital signs show the following: Temperature 99.0 F, Pulse 94/min, BP 135/86 mmHg. Physical examination is significant for ecchymoses over his right shoulder, triceps and forearm with tenderness and swelling in his forearm.Laboratory Data:
Test Result Reference range
White blood cells (leukocyte count) 12.0 4.8-10.8 thou/uL
Hemoglobin 13.2 12-16g/dL
Hematocrit 40 36-47%
Mean Corpuscular Volume (MCV) 92 81-99 fl
Red Cell Distribution Width (RDW) 15 11.5-14.5%
Platelet count 280 130-400 thou/uL
PT 12.1 <14 sec
INR 1.0 <1.3sec
PTT 76 22-35sec
References (from mandatory readings) for this case
a. Lecture: Coagulation Online Module/Lectures (Dr. Cannaday), Friday July 28th, 8-11 amb. Robbins Pathologic Basis of Disease (9th edition): Hemophilia: pages 662-663
Clinical Features relevant from this clinical history:
1. Based on the clinical presentation and laboratory findings, how would you approach the differential diagnosis in this patient? Bleeding with ecchymoses, high PTT, normal PT. No evidence of thrombocytopenia.
2. What is your differential diagnosis for increased PTT? Hemophilia A, hemophilia B, severe vWB disease, type 3, use of heparin, Factor inhibitor or antibody
3. Which entities within your differential diagnosis list are unlikely and why? Hemophilia A/B should be childhood diagnoses; also vWB disease type 3 would have presented perhaps earlier in life. Heparin use is not mentioned in the history.
13

Laboratory Questions:
4. How is Partial Thromboplastic Time test performed and what does it assess? In the laboratory, activate factor XII by adding glass beads in the test tube and measure the time (in seconds) it takes to form a clot. PTT asscess functionality of factors in the intrinsic (XII, XI, IX, VIII) and common (X, V, II, I) pathways. If any of the above factors are deficient or defective, then the time to make a clot will be prolonged
5. Which medication is PTT used to monitor? Use to monitor heparin. Heparin binds and enhances activity of anti-thrombin III (which blocks coagualtion by inhibiting thrombin, and factors X, XII, XI and IX)
6. How is Prothrombin Time test performed and what does it assess? In the laboratory, activate factor VII by adding exogenous tissue factor and measure the time (in seconds) it takes to form a clot. PT asscess functionality of factors in the extrinsic (VII) and common (X, V, II, I) pathways. If any of the above factors are deficient or defective, then the time to make a clot will be prolonged
7. Which medication is PT used to monitor? Use to monitor warfrin. Warfrin is a vitamin K antagoinist and blocks factors II, VII, IX, and X. Factor VII has the shortest half life, and therefor PT is used to monitor warfrin (rather than PTT). INR is a standardization of PT which is used clinically
8. List all Vitamin K dependant factors: Coagulation factors II, VII, IX, and X. Anti-coagulation proteins: Protein C and Protein S
9. What additional laboratory tests is needed when PTT is prolonged and how is it performed? If PT or PTT or both are prologned, a mixing study will be performed by the lab. Patient’s sample is mixed with normal plasma (which contains all the factors); if PT or PTT corrects, then the patient has a factor defiecincy; if it does not correct, then the patient has a factor inhibitor
Additional laboratory and imaging studies:
A “mixing study” using a 1:1 dilution of patient plasma with pooled normal plasma is performed and does not show correction of the prolonged PTT. An assay for von Willebrand disease is negative. The patient is diagnosed with a factor inhibitor (factor VIII). A CT scan of the right shoulder and arm shows a large hematoma. The patient is treated with factor inhibitor coagulant complex FEIBA. FEIBA stands for “Factor Eight Inhibitor Bypassing Agent” and contains Factors X and II. Factor II is prothrombin. So, by giving those factors, you bypass the inhibitor by stimulating coagulation at a point lower on the cascade than Factor VIII. Surgery is consulted for surgical intervention to relieve the compartment syndrome.
14

Case 5: “A 5-year-old Caucasian boy with multiple bruises”
VON WILLEBRAND DISEASE TYPE 3
CLINICAL HISTORY: This is a 5-year-old boy with multiple bruises, purpura and small hematoma around his thigh, who is coming in with his mother for a follow up visit on previously drawn labs.
References (from mandatory readings) for this case
a. Lecture: Coagulation Online Module/Lectures (Dr. Cannaday), Friday July 28th, 8-11 amb. Robbins Pathologic Basis of Disease (9th edition), Von Willebrand Disease: pages 661-662 and Hemophilia: pages 662-663
Clinical Features relevant from this clinical history:
1. Given the patient’s bleeding symptoms, what 2 entities were in your differential diagnosis when you ordered the labs (given that child abuse was ruled out)? Hemophilia (A or B) and Von Willebrand Disease (severe subtype such as subtype 3)
2. What clues in the case above (mention at least 2) lead you to suspect large vessel bleed? Purpura and hematoma (no petechiae which indicate small vessel bleed)
3. What skin manifestation does small vessel bleed lead to: Petechiae, also purpura- seen with thrombocytopenia
4. List 2 types of Hemophilia and the associated factor deficiency: Hemophilia A- factor VIII deficiency and Hemophilia B- factor B deficiency
5. List the 3 main types of Von Willebrand Disease and whether mutations cause quantitative or qualitative defects in vWF. Comment on the severity of bleeding for each type: Type 1 (quantitative, mild to moderate), Type 2A (qualitative, mild to moderate), Type 3 (quantitative, severe)
6. In Hemophilia A, the amount of factor VIII determines the severity of the bleeding symptoms. Summarize the bleeding tendencies depending on the factor VIII levels:Severity of Disease:
o <1% of factor: present with severe bleedingo Up to 5%: modeate bleeding tendencyo >5%: mild bleeding tendency
Additional laboratory findings: Further laboratory testing shows his vWF antigen is essentially zero, while factor VIII level is 6%. Platelet count is within normal limits.
Laboratory Questions:
7. Which type of Von Willebrand’s disese does this boy most likely have? Type 38. What would you expect to see for his PT and PTT values: Normal PT and increased PTT9. What would you expect for his Ristocetin induced platelet aggregation study: No aggregation 10. Explain the results of the PT and PTT for this type of Von Willebrand Disease: PTT is prolonged
because essentially you have very little vWF which stabilizes Factor VIII- this in turn leads to factor VIII being degraded and essentially “deficient”, hence PTT is prolonged. PT is not affected.
15

Case #6: “A 32 year old Asian American woman with difficulty moving her tongue” TTP
CLINICAL HISTORY: This is a 32-year-old Asian American woman who comes in to the emergency room with difficulty moving her tongue, difficulty speaking and intermittent numbness of her legs for the last two days. Physical exam reveals a temperature of 100.5 and is notable for a positive neurological exam. A STAT CBC comes back with a low hemoglobin, low hematocrit and low platelet count. WBC is within normal limits.
References (from mandatory readings) for this case
a. Lecture: Coagulation Online Module/Lectures (Dr. Cannaday), Friday July 28th, 8-11 amb. Robbins Pathologic Basis of Disease (9th edition), Thrombotic microagniopathies: pages 659-660
Clinical Features relevant from this clinical history:
1. Given the clinical presentation of neurological symptoms and low grade fever along with anemia and thrombocytopenia, which life threatening disease, do you suspect? TTP.
2. What other diagnoses can present with neurological symptoms and anemia (mention 2)? HUS and B12 deficiency anemia
3. What is the underlying mechanism of thrombocytopenia and hemolytic anemia in TTP? TTP: deficiency of ADAMTS-13. This enzyme cuts vWF ultra-large multimers into smaller units; otherwise, they are very thrombogenic and platelets get consumed with them and form intravascular thrombi (hence the thrombocytopenia). Also these thrombi in the microvasculature cause damage to the passing by red blood cells, resulting in their fragmentation and destruction (hemolysis).
4. What is the underlying mechanism of thrombocytopenia and hemolytic anemia in HUS? HUS- E Coli O157:H7 produces “Shiga-like toxin”, which causes platelet activation and aggregation, causing intravascular microthrombi (consume platelets) and damage RBCs (hemolysis).
5. What is the classic clinical presentation for TTP? HUS? TTP: pentad of thrombocytopenia, hemolytic anemia, renal failure, fever, neurological symptoms. HUS: thrombocytopenia, hemolytic anemia, renal failure
6. How will you treat this patient? Emergent exchange transfusion (plasmaphresis)
Laboratory Questions:
7. Which set of labs will you order to work the patient up? Order bilirubin (↑ in hemolysis), LDH (↑ in hemolysis), haptoglobin (↓ in hemolysis), urine to evaluate for hemoglobinuria and hemosiderinuria, get peripheral blood smear (schistocytes), DAT aka Coombs test (negative) and renal function tests.
8. What do you expect to see on the PBS? Normocytic and normochromic red blood cells with schistocytes (RBC fragments); reticulocytosis
16

1) What is the cellular defect in a sickle cell red blood cell?(A) *A point mutation in the beta-globin chain(B) A defect in a component of the cell membrane skeletal proteins(C) Decreased synthesis of the alpha-globin chain(D) Lack of an erythrocyte enzyme
2) What is the most likely casue for chest pain in a sickle cell disease patient with acute chest syndrome?(A) Thrombosis of the coronary artery(B) Severe esophageal vasospasm(C) *Ischemia of post capillary tissue (D) Anxiety attack from being homesick
3) What is the most immediate and life saving step in managing a patient with acute chest syndrome?(A) Give Folic Acid(B) Give Hydoxyurea(C) *Do an exchange transfusion(D) Give pain medications
4) The sickle cell disease patient may experience all of the following complications from his or her underlying disease, except:
(A) *Psychosis(B) Vasoocculsive crises(C) Stroke(D) Priapism(E) Decreaesd vision
1) A2) C3) C4) A
ANSWERS TO SELF REVIEW QUESTIONS ON HANDOUT
SELF REVIEW QUESTIONS (ANSWERS AT THE END OF HANDOUT)
17