
PATHOKINESIOLOGICAL ASSESSMENT AND REHABILITATION …
45
Transcript of PATHOKINESIOLOGICAL ASSESSMENT AND REHABILITATION …


OUTLINE
• GAIT• GAIT PROBLEMS• ASSESSMENT• REHABILITATION
GAIT AND TYPES OF GAIT
GAIT: Manner of walking/ Manner in which walking is performed.
Types
Quadripedal
Digitigrade
Unguligrade
Bipedal
Plantigrade.
The ability to walk upright is the defining characteristic of man. The human gait is bipedal and plantigrade.

GAIT CYCLE


EVENTS AND DETERMINANTS OF HUMAN GAITSEvents
Control of Forward Movement during deceleration at the end of swing phaseShock Absorption at Heel StrikePropulsion duriing Push Off, When the Centre of Mass (Gravity) is propelled upward and forward.
DeterminantsPelvic Rotation in Horizontal Plane
Pelvic Tilt in Frontal PlaneKnee FlexionControl of the Knee-Ankle-Foot MotionLateral Pelvic Movement.

NORMAL GAIT TO SHOW PELVIC ROTATION, TILT AND LATERAL MOVEMENT

GAIT ANALYSES [TOOLS FOR ASSESSMENT]Gait analysis:• Clinical Evaluation• Individual History• Physical Examination• Functional and Aesthetic Assessment.
• Observatory Gait Analysis• Gait Laboratory Technology; Gait problems/ abnormalities can be more precisely
examined through the use of Gait Laboratories.• EMG activities of muscles• Force plates• Instrumented Shoes and kinematic evaluation of the lower limbs
A proper clinical evaluation should always precede any gait laboratory assessment.

NORMAL GAIT

CAUSES OF ABNORMAL GAITS
Broad DivisionsA. Neuromuscular
A.Injury to the central or pripheral nervous system- results in changes in muscle tone and motor control
B. MusculoskeletalA.Hip Knee, Foot and Ankle patologiesB.Liomb Length discrepancyC.Skeletal abnormalties
C. Isolated Motor Weakness Gait Problems

NEUROMUSCULAR AETIOLOGIES
Hemiplegic gait: Results from Cerebrovascular Disease.• Abnormal arm position and swing• Extensor synergy (extension, adduction, internal rotation of the hip) • Slow with decrease in step length, increase in stance phase with
circumduction to allow to allow toe clearance
Flexor Synergy gait: Less common, eliminates ambulation potential
Spactic gait: Results from injury to CNS that affects motor tone.• Scissoring of lower limbs from overactivity of hip adductors with • Associated tiptoeing.

Parkinsonian/Festinating Gait: Results from Parkinson’s Disease – Lesion of the basal ganglia affecting motor control and function bilaterally.• Trunk is flexed forward• Slow and shuffling• Rapid steps• Subject may have difficulties with stops and turns.
Ataxic gait: Injury to the cerebellum and/or its pathway afeecting coordination and precision movement. Or Sensory deficit of lower limb. Characterised by
• Unsteady /staggering gait with • broad standing base.• Slapping of feet• Loss of propioceptive feed back causes individual to look at their feet

PARKINSONIAN/FESTINATING POSTURE/GAIT

MUSCULOSKELETAL AETIOLOGIES
• Hip Pathology• Osteoarthritis, Avascular Necrosis of Head of Femur..
• Knee Pathology• Osteoarthritis, Infection as in Septic arthritis, Synovitis, Meniscial
tear. Loose body, fracture.may result in Antalgic Gait.• Injuries to P cruciate L, Lateral collateral ligament, Posterior joint
capsule and popliteus tendon may result in Varus thrust Gait.• Injury to ACL result in Quadriceps Avoidance Gait. In order to
decrease or avoid the stress tendency to anterior subluxation of the tibia (which the ACL prevents) by decreasing the stride length and avoiding knee flexion during the mid stance phase..• Knee Flexion contracture result in Toe Walking or Steppage Gait
MUSCULOSKELETAL AETIOLOGY CONTD.
Foot and Ankle Pathology
Trauma, inflammatory disorder, plantar fascitis,, degenerative disorders of the foot and ankle, forefoot and hind foot pathologies may result in various forms of antalgic gait.
Leg Length Discrepancy (LLD): LLD can relative (apparent) or true (real).
Relative LLD may result from Scoliosis and Contractures of the Hip, Knee and Ankle.
True LLD results from asymmetry in lengths of pelvis, femur or tibia.
In either case LLD can result in Pelvic Obliquity (Tilt), decreased hip/knee flexion, ankle plantar flexion and/or hyper pronation- ipsilateral to shortened side.
In LLD of less than 1.27cm ,in addition to the pelvic drop , during the entire stance phase, there is apparent elevation of the shoulder on the opposite side (swing side) and exaggerated flexion of the Hip/Knee and Plata flexion of the ankle on ipsilateral side.
LLD can result in Tiptoeing Gait.

Skeletal Abnormality
Equine Gait may result from:
Untreated Congenital Equinus/ Equinovalrus
Paralysis of the peroneals
Characteristics: High Steps on toes or on Clubbed Foot
High Steps on dorsum of affected foot/feet.
Waddling Gait;
Coxa vara
Double Congenital Displacement/Dislocation of the Hip.
Characteristics: Gaits iwhich feet are wide apart resembling that of a duck.

ISOLATED MOTOR WEAKNESS GAIT PROBLEMS
Gluteus Medius or Tredelenburg gait: Paralysis/ Paresis of hip abductors.-G Medius..
Characteristic (Cxt): Leaning of trunk to the affected side
Gluteus Maximus (Lurch) Gait: Weakness of G. Maximus
Cxt: Trunk is thrown bacward after hee stike
Hip Flexors Weakness Gait: Paresis of hip flexors.
Cxt : Backward trunk lurch towards unaffected side from push off to mid swing.
Quadriceps Weakness Gait;
Affected knee is locked in hyper extentsion at heel stike. Some subjects place their hand on the thigh at heel strike. Excessive heelstrike in fast walking.

Steppage /Foot Drop/ Slap Foot gait: Results from ankle dorsiflexors weakness
Cxts: • Losses of heel strike, plantar flexion control, • decreased/eccentric control of dorsiflexion, • Toes clearance ensured by compensatory exaggerated hip and knee flexions
Gastrosoleus Weakness Gait: This may result from weakness of gastrosoleus , unrepaired rupture of Tendo Archilles resulting in
• Loss of ankle dorsifexion control• Delayed heel-off, and decreased push-off,• Lag of forward movement of the unaffected side during push off• Shortening of stride of the unaffected side• Reduced ground reaction and knee buckling

ABNORMAL GAIT - LURCHING AND ANTALGIC
Abnormal gait1

QUADRICEPS WEAKNESS GAIT (R)

HELICOPOD GAIT/MILD HEMIPLEGIC

QUADRICEPS WEAKNESS GAIT ( R)
QUADRICEPS WEAKNESS GAIT ®

MULTI-COMPLICATED- QUADRICEPS WEAKNESS ( R), FOOT DROP-GASTROSOLEUS( R), FOOT-KNEE PRONATION ( R), GLUTEUS MEDIUS/MAXIMUS (L)
CLINICAL GAIT ANALYSISThe process by which quantitative information is collected to aid in understanding the
etiology of gait abnormalities and in treatment decision-making (Davis, 2002)
• Observation as clients ambulates into the room/cubicle/gymn
• Individual History• Physical Examination
• Specific Tests. [eg for knee pathologies]• Functional and aesthetic assessment
Visual Observation
Objective Evaluation• Observatory Gait Analysis [OGA]
Gait characteristics using walk way
GAIT LABORATORY TECHNOLOGY
Electromyography with Multichannel SystemPolarised Light Goniometry [Polgon]Electrogoniometry [Elgon]Force Plate walkwayTelemetry System with Instrumented Shoes.BTS G-Walk System

ELECTROMYOGRAPHY

MOTION LABORATORY [KINETIC AND KINEMATIC ASSESSMENTS]
GAIT ASSESSMENT
• Kinematic Assessment• OGA• POLGON• ELGON• BTS G-WALK SYSTEM
• Kinetic Assessment• FORCE PLATE WALK WAY• INSTRUMENTED INSOLE [SHOE]

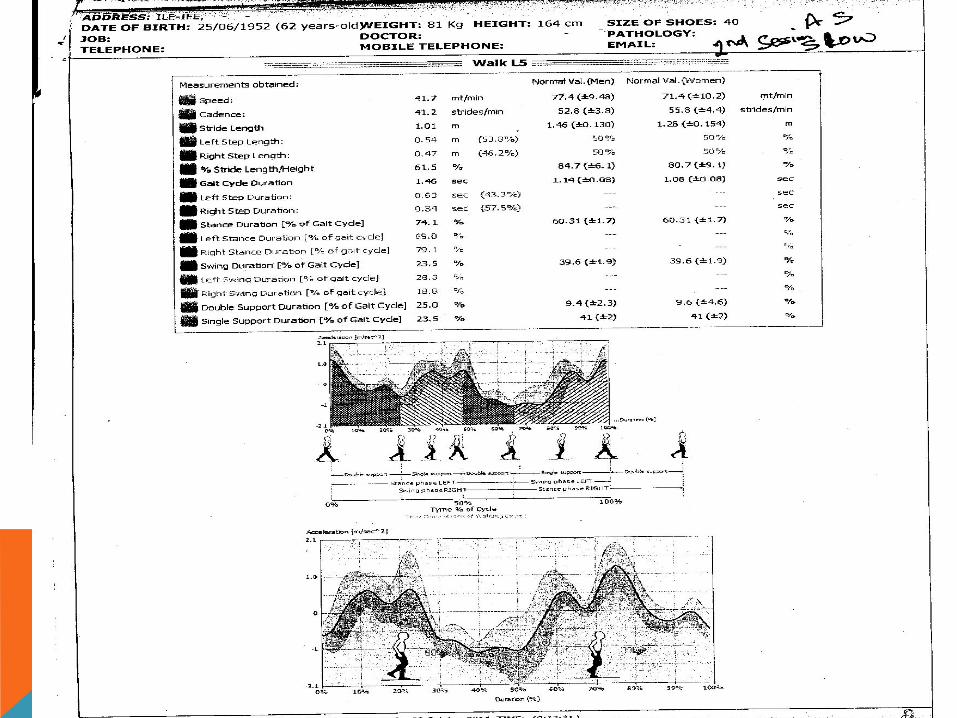
OBSERVATIONAL GAIT ANALYSISWalkwayTreadmillGait Characteristics
CadenceSpeedStride LengthStep LengthStep WidthFoot AngleAsymmetry…….






REHABILITATION
• What is Rehabilitation?• A cooperative effort…..
• Who are team members?• ………………patient/client most important.
• Who needs rehabilitation.• ………..clients from prison, mental care, drug addiction, injury,
illnesses..

REHABILITATION
Assessment/Evaluation
It is impotant to determine the aetiology
Education and Counseling
Intervention§ Pain/Orthopaedic§ Support ( Splinting, Bracing, …)§ Unloading of joints – Use of Walking Aids§ Corrective Approaches (including Surgery)§ Progressive and selective Strengthening Exercises§ Neurologic
§ Neurologic Approaches /Neurorehabilitation
REHABILTATION CONTD
Stepping Test using the Forward Upward Leading Step Test (FULST) .Strengthening Exercises to the antigravity muscles/physiologic lower limb extensors may include:
Stepping Exercises with • Back packs (with regulated weights)• Ankle weigths

FOLLOW UP
Home Programme with tele-prompting

REFERENCES
Buriamoh-Igbo L.A., Olaogun M.O.B., Jubril A.M. (1996): Measurement of ground-foot reaction force to determine gait asymmetry using a computer-based telemetry system. Rehabilitation R & D Progress Reports. 52-53
Davis R.B., Õunpuu S., DeLuca P.A., Romness M.J. (2002): Clinical Gait Analysis and Its Role in Treatment Decision-Making. Orthopaedics & Sports. http://www.medscape.com/viewarticle/440148.
Faivre A., Dahan M., Parratte B., Monnier G. (2004): Instrumented shoes for pathological gait assessment. Mechanics Research Communications. 31; 627–632.
Hausdorf J.M., Ladin F.Z., Wei J.Y., Footswitch system for measurement of the temporal parameters of gait. J Biomech., 28 (3) (1995), 347-51.
.

REFERENCES CONTINUEDMorris S.J., Paradiso J.A. (2003): A Compact Wearable Sensor Package for
Clinical Gait Monitoring, Offspring: 1 (1) 7-15.
Malanga G and Delisa JA (1998); Gait Analysis in the Science of Rehabilitation; RRDS, pp 1-10
Olaogun MOB(1996); Pathokinesiology; JNMRT. Vol. 1 No.2 pp 28-30.
Olaogun MOB, Abereoje OK, Obajuluwa VA (1989); Forward Upward Leading Step Test for the Clinica Evaluation of Locomotor Ability; Clinical Rehabilitation; 3, 41-45.
Oyebisi T.O., Kehinde L.O., Buraimoh-Igbo L.A. and Olaogun M.O.B (1994). Computer based Data Acqising System for Ground Foot Forces in pathologic Gait. J.Comp. Science and its Application Vol. 6, No 1,1-15.
Wertsch J.J., Webster J.G., Tompkins W.J. (1992): A portable insole plantar pressure measurement system. Journal of Rehabilitation Research and Development ; 29 (1) 13-18.

THANK YOU


















