pathogenesis, treatment, and prevention of pneumococcal pneumonia

of 14
Transcript of pathogenesis, treatment, and prevention of pneumococcal pneumonia
-
8/13/2019 pathogenesis, treatment, and prevention of pneumococcal pneumonia
1/14
Seminar
www.thelancet.com Vol 374 October 31, 2009 1543
Pathogenesis, treatment, and prevention of pneumococcal
pneumoniaTom van der Poll, Steven M Opal
Pneumococcus remains the most common cause of community-acquired pneumonia worldwide.Streptococcus pneumoniaeis well adapted to people, and is a frequent inhabitant of the upper airways in healthy hosts.This seemingly innocuous state of colonisation is a dynamic and competitive process in which the pathogen attemptsto engage the host, proliferate, and invade the lower airways. The host in turn continuously deploys an array of innateand acquired cellular and humoral defences to prevent pneumococci from breaching tissue barriers. Discoveries intoessential molecular mechanisms used by pneumococci to evade host-sensing systems that are designed to contain thepathogen provide new insights into potential treatment options. Versatility of the genome of pneumococci and thebacterias polygenic virulence capabilities show that a multifaceted approach with many vaccine antigens, antibioticcombinations, and immunoadjuvant therapies will be needed to control this microbe.
IntroductionNearly a century ago, Sir William Osler proclaimedStreptococcus pneumoniae (or pneumococcus) as thecaptain of all the men of death.1This statement remainsas true today as it was then. Severe community-acquiredpneumonia is the most common cause of death frominfection in developed countries, and the pneumococcusis the most frequent cause of lower respiratory tractinfection. We can now control many other respiratorypathogens of man reasonably well (eg, influenza,pertussis, tuberculosis, and Haemophilus influenzae), yetpneumococcus remains the main cause of community-acquired pneumonia worldwide.1
Reasons for the success of this obligate human
pathogen are becoming increasingly apparent as thebasic pathogenic mechanisms of pneumococcalpneumonia are discovered. This pathogen causes at least12 million infant deaths every year worldwide.2,3 Theyearly death toll attributable to pneumococci in patientswith AIDS and other immunocompromised states,elderly people, and those with comorbid illnesses isdiffi cult to quantify, but probably exceeds the infantmortality rate.
Advances in comparative genomics and insights intoinnate and acquired immune-signalling mechanismscould provide new treatment options for pneumococcaldisease.28 We focus on the clinical outcomes after theinitial hostpathogen interaction when S pneumoniae
first reaches the airways and invades the lowerrespiratory tract.
EpidemiologyS pneumoniae is a common inhabitant of the upperrespiratory tract, existing mainly as a commensalbacterium along with other co-resident microorganismsidentified on the respiratory epithelium. Aftercolonisation by one of 91 presently recognised serotypes,a new strain eliminates other competing pneumococcalserotypes, and persists for weeks (in adults) or months(in children), usually without any adverse sequelae. Thiscarrier state maintains the organism within human
populations, and induces some acquired B-cell-mediatedimmunity to reinfection.3,4Genetic and epidemiological evidence show that one of
two survival strategies account for the success ofS pneumoniae. Specific clones are selected with either aninvasive pneumococcal diseasephenotype or a persistentcolonisation phenotype with low risk of tissue invasion.Success of the phenotype of invasive pneumococcaldisease depends on its capacity for rapid disease inductionand effi cient person-to-person spread by coughing. Bycontrast, the non-invasive phenotype uses various surfaceadhesins, immune evasion strategies, and secretorydefences such as IgA1 protease and inhibitors ofantibacterial peptides to help with long-term carriage
within the nasopharynx.5
Persistent carriage ofpneumococci allows for low-level and longlastingtransmission, thereby retaining non-invasive strains inhuman populations. Defects in host defences can alterthis hostpathogen interaction and allow strains of lowvirulence to invade the immunocompromised host.57
The pneumococcus is mainly transmitted by directcontact with contaminated respiratory secretions betweenhousehold members, infants, and children. Pneumococciare generally not regarded as highly contagious, andrespiratory isolation of patients who are infected in thecommunity or hospital settings is rarely indicated.However, a large, community-wide outbreak of serotype 5pneumococci in Vancouver, Canada,9 showed that
potential exists for epidemic spread of S pneumoniae
Lancet2009; 374: 154356
See Commentpage 1485
Centre for Infection and
Immunity Amsterdam, Centre
for Experimental and Molecular
Medicine, Academic Medical
Centre, University of
Amsterdam, Amsterdam,
the Netherlands
(Prof T van der Poll MD); and
Infectious Disease Division,
Warren Alpert Medical School,
Brown University, Providence,RI, USA(Prof S M Opal MD)
Correspondence to:
Prof Tom van der Poll, Academic
Medical Centre, University of
Amsterdam, Meibergdreef 9,
1105 AZ Amsterdam,
the Netherlands
Search strategy and selection criteria
We searched Medline and PubMed in English with the search
terms pneumococci, Streptococcus pneumoniae,
pneumococcal pneumonia, community acquired
pneumonia, and pneumococcal pathogenesis for reports
relating to pneumococcal pneumonia published in the past
10 years until January, 2009. We reviewed the publications
and searched the reference lists of identified articles for older
reports we judged to be of major importance.
-
8/13/2019 pathogenesis, treatment, and prevention of pneumococcal pneumonia
2/14
Seminar
1544 www.thelancet.com Vol 374 October 31, 2009
within urban neighbourhoods. Similar small-scaleoutbreaks have been reported in day-care centres, jails,military bases, and mens shelters.1012Airway colonisationby pneumococci is readily detectable in about 10% ofhealthy adults. 2040% of healthy children are carriers,and more than 60% of infants and children in day-care
settings can be carriers.3,8
Most people colonised with S pneumoniae have onlyone serotype at a time, although simultaneous carriageof more than one serotype is possible.13 Duration ofpneumococcal colonisation in an individual is highlyserotype-specific. 14 Recent acquisition of an invasiveserotype is more important as a determinant ofsubsequent risk of invasive pneumococcal disease thanis duration of colonisation or specific clonal genotype. 15Results of studies of the conjugate seven-valentpneumococcal vaccine in children suggest that thehumoral immune response can reduce risk ofserotype-specific disease, decrease likelihood oftransmission in vaccine recipients, and even reduce
transmission risk between non-immunised siblings andadults (ie, herd immunity).3,16
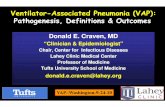
Incidence of invasive pneumococcal disease(ie, bacterial pneumonia and bacteraemia) varies sub-stantially by age, genetic background, socioeconomicstatus, immune status, and geographical location. In alarge US epidemiological survey in 1999, overallincidence in children older than 5 years was 987 per100 000 per year. By 2005, the same survey showed thatincidence had reduced by 75% to 234 per 100 000 peryear. This change was largely attributable to reducedrates of infection with serotypes contained in thepneumococcal conjugate vaccine17 (figure 1). This
decreased overall incidence was accompanied by a smallrise in invasive pneumococcal disease from non-vaccineserotypes.18This pattern seems to be continuing and hasprompted a renewed interest in other vaccineformulations. Incidence rates can be as high as 441 casesper 100 000 per year in isolated Indigenous populationssuch as Alaskan Eskimos, Aboriginal Australians, andthe Maoris of New Zealand.19
Other recognised risk factors for invasive pneumo-coccal disease in children and adults include asplenia,alcoholism, diabetes mellitus, age greater than 65 years,underlying lung disease, severe liver disease, influenzaand probably other respiratory viruses, immunoglobulinand complement deficiencies, and other immuno-compromised states, including HIV infection. Crowding,recent acquisition of a virulent strain, poverty, cigarette
smoking, proton pump inhibitors,20
and other riskfactors probably contribute to pneumococcal disease(panel).3,14 Antecedent respiratory infections and recentexposure to antibiotics seem to be additional risk factorsfor colonisation of airways and invasive pneumococcaldisease. Antibiotic-induced alterations in competinginhibitory bacteria (-haemolytic streptococci inparticular), release of viral enzymes (eg, influenzaneuraminidase) that promote adherence,3 and hostinflammation-induced expression of pneumococcalinvasion receptors on host cells, such as platelet-activatingfactor receptor21and CD14,22contribute to pneumococcalcolonisation and invasion.
Genetics and virulence of S pneumoniaeKnowledge of genomes of many invasive andnon-invasive strains of S pneumoniae enable detailedcomparative analyses.2329 The pneumococcal genomehas between 2 million and 21 million basepairs,dependent on strain virulence (figure 2). It is a covalentlyclosed, circular DNA structure often accompanied bysmall cryptic plasmids. The guaninecytosine content ofS pneumoniaeDNA (397%) is lower than that of manyother bacterial pathogens. One of the originalpneumococcal genomes to be sequenced, strain TIGR4,23has 2236 open reading frames of which two-thirds haveassigned roles for their predicted gene products. Another16% of open reading frames generate conserved,
hypothetical proteins of unknown function. About20% exist only in S pneumoniae.23
The genome contains a core set of 1553 genes that areessential for viability.2429An additional 154 genes form thecomplement of bacterial genes that collectively contributeto virulence (the virulome), and 176 genes activelymaintain a non-invasive phenotype. Pneumococci havean unusually large number of insertion sequences,accounting for up to 5% of the entire genome. Somestrains contain conjugative transposons within theirgenomes that mediate antibiotic resistance. Muchplasticity exists within the S pneumoniaegenome, with upto 10% variation between strains. The genome is replete
19980
50
100
150
200
250 PCV-7 vaccineintroduced
Age
-
8/13/2019 pathogenesis, treatment, and prevention of pneumococcal pneumonia
3/14
Seminar
www.thelancet.com Vol 374 October 31, 2009 1545
with many copies of direct-repeat DNA elements thatprovide recombination hotspots for genetic variability.23
Pneumococci express the most diverse array ofsubstrate transport, and use systems known to humanpathogens.23,24Specific ATP-binding cassette transportersimport carbon or aminoacid substrates and export outersurface adhesins, degradation enzymes, or capsularsynthetic components. These transporters are also
essential for genetic competence (ability to take uphomologous strands of naked DNA), for nutrientacquisition, and as effl ux pumps to resist antibiotics.23Pneumococci have much genetic space for capsularpolysaccharide synthesisthe most important virulencefactor for this organism.5 Phase variation arises withmolecular switches at promoter regions of open readingframes for major surface antigens.23 Pneumococciregulate the amount of capsular material producedduring colonisation and invasion. Transparent (thin)capsules are favoured in early colonisation, whereasopaque (thick) capsules are favoured during invasion toresist complement-mediated opsonophagocytosis.3,5
Pneumococci cluster virulence genes into smalldefined sequences within the genome known as regionsof diversity. These regions distinguish invasive fromnon-invasive strains. At least 13 such regions are identi-
fied in pneumococci, many of which carry the geneticsignatures of pathogenicity islands.25,28 Non-virulentstrains exist even within the same capsular serotypethat contain some but not all elements of the entirepneumococcal virulome.5,2931 Pneumococci have anarray of two-component sensor-kinase signal systemsthat recognise environmental cues (eg, cell density,substrate availability, and microbial competitors) andalter their genetic programmes in response. Thesesystems direct the synthesis of bactericins 32 (bacterialpeptides that kill other related bacteria), competencegenes for genetic recombination, biofilm formation,33and virulence expression.5,33 Pneumococcal virulencehas been acquired by horizontal transmission from
other pathogens during the evolutionary past.34
Evidence of continuing evolution through the acquisi-tion of new antibiotic resistance genes and virulencetraits is shown in pneumococci and other gram-positivebacterial pathogens, such as group A streptococci,35Staphylococcus aureus,36and Clostridium diffi cile.37
Pneumococcal virulence factorsTable 1 shows a summary of virulence traits identified inpneumococci.3849An array of virulence factors needs tobe expressed in a coordinated way for tissue invasion tobe successful (phenotype for invasive pneumococcaldisease). The most important virulence determinants
Panel: Risk factors for pneumococcal pneumonia and
invasive pneumococcal disease
Definite risk factors* (high risk)
Younger than 2 years or older than 65 years
Asplenia or hyposplenia
Alcoholism
Diabetes mellitus
Antecedent influenza
Defects in humoral immunity (complement or
immunoglobulin)
HIV infection
Recent acquisition of a new virulent strain
Probable risk factors (moderate risk)
Genetic polymorphisms (eg, complement, MBL, IRAK-4,
Mal, MyD88)
Isolated populations
Poverty, crowding, low pneumococcal vaccine use
Cigarette smoking
Chronic lung disease
Severe liver disease
Other antecedent viral infections
Poor mucociliary function
Possible risk factors (low risk)
Recent exposure to antibiotics
Defects in cellular immunity and neutrophil defects
Diminished cough reflex, aspiration pneumonitis
Proton-pump inhibitors and other gastric-acid inhibitors
Large organism burden in upper airways
Childhood day care
MBL=mannose binding lectin. IRAK=interleukin I receptor associated kinase.
Mal=Myeloid differentiation primary response factor 88 adaptor like.*Many clinical
studies. Some clinical and laboratory studies. Few clinical studies.
RDs
700000
800000
9000001000000
11000001200000
1300000
1400000
1500000
1600000
1700000
1800000
19000002
000
000
2100000 1
600000
500000
400000
300000
200000100000
Point of origin ofreplication
GCskew
Distinct tovirulent strains
IS and
repetitiveelements
Figure :Genomic structure of Streptococcus pneumoniaeTIGR4
RDs=regions of diversity. GC skew=difference in guanine (G)cytosine (C) ratio from GC average of pneumococcal
genome. IS=insertion sequence elements. Adapted from Tettelin, et al23with permission from the AAAS.
-
8/13/2019 pathogenesis, treatment, and prevention of pneumococcal pneumonia
4/14
Seminar
1546 www.thelancet.com Vol 374 October 31, 2009
include the antiphagocytic and adherence properties ofcapsular polysaccharides, adherence factors, invasiongenes, iron and other heavy-metal transporters, oxidativestress protection, host-defence evasion, pneumolysinproduction, bacteriocin production, and quorum sensingand biofilm formation (figure 3).5,3849
Virulence expression varies with tissue site andpopulation density. Sessile pneumococci residing insidebiofilms are more able to induce meningitis and
pneumonia but have less capacity to disseminate in bloodthan do those unattached and not inside biofilms. Bycontrast, free-living, unattached (or planktonic) bacteriaare more likely to induce bacteraemic infection, but areless successful in causing pneumonia.33Many virulencefactors probably contribute to invasive pneumococcaldisease in people, but unequivocal evidence exists onlyfor pneumococcal capsulesthe target of present vaccineformulations.
Pneumococcal capsular antigen is the most importantvirulence determinant for pneumococci in experimentaland clinical studies.38 The capsule is crucial duringcolonisation, invasion, and dissemination from the
respiratory tract. It prevents mechanical clearance bymucous secretion38 and helps with transit of theorganism to the epithelial surface. Capsularpolysaccharide is highly negatively charged and stericallyinhibits the interaction between phagocytic CR3receptors to iC3b, and between Fc receptors to the Fccomponent of IgG fixed to pneumococci.38,39 Pneumo-coccal capsules also restrict autolysis and reduceexposure to several antibiotics.3,5
Pneumococcal exotoxin-pneumolysin is expressed byalmost all invasive strains of S pneumoniae. Thispore-forming cytotoxin is released during autolysis as asoluble monomer that oligomerises on host membranes.Pneumolysin is lytic to host cells if suffi cient amounts ofit are generated. The toxin has many other pathologicaleffects, including its ability to inhibit ciliary action ofepithelial cells, activate CD4+ T cells, impair respiratoryburst of phagocytic cells, induce production ofchemokines and cytokines, stimulate complementfixation, and activate inflammation.7,40 Pneumolysin-negative mutants of S pneumoniaeare much less likely toproduce lethal pulmonary infections than are wild-type
Mechanism of action Level ofevidence*
Polysaccharide capsule5,6,38,39 Prevents mucosal clearance, antiphagocytic, sterically inhibits complement andimmunoglobulin-binding to host receptors
4+
Pneumolysin7,40 Cytolytic, TLR4 ligand, induces ciliostasis, impairs respiratory burst, activates complement,cytokine, chemokine production
3+
Pneumococcal surface protein A41 Blocks C3b binding to factor B, binds to epithelial membranes 2+
Pneumococcal surface protein C; also known ascholine binding protein A42,43
Binds factor H and blocks C3b fixation, binds to human polymeric immunoglobulinreceptor during invasion
2+
Cell wall polysaccharide5 Activates complement, pro-inflammatory 1+
Pneumococcal surface antigen A5,22,25 Mediates metal ion uptake (zinc and manganese), protects against oxidant stress, bindsto GlcNac-Gal
12+
Lipoteichoic acid44 Binds to PAFR, TLR2 ligand, proinflammatory 2+
Autolysin5 Releases peptidoglycan, teichoic acid, pneumolysin other intracellular contents 2+
Hyaluronate lyase45 Degrades hyaluronan in the extracellular matrix 1+
Enolase5 Binds to fibronectin in host tissues 1+
Sortase A46 Links surface proteins to cell wall 1+
Pili47 Pilion cell surface inhibits phagocytosis, promotes invasion 1+
Pneumococcal adhesion and virulence48 Binds to plasminogen within host tissues 1+
Pneumococcal iron acquisition A and iron uptake A5 ABC transporters that acquire iron for bacterial growth and virulence 1+
Bacteriocin5 Inhibits bacterial competition, might have other cytotoxic actions 2+
Neuraminidase45 Contributes to adherence, removessialic acids on host glycopeptides and mucin to expose binding sites
1+
Biofilm and competence33 Biofilm organisms upregulate CSP; competence genes contribute to pneumonia andmeningitis
2+
IgA protease5 Degrades human IgA1 12+
Phosphorylcholine44 Binds to PAFR on human epithelial cells 2+
Pneumococcal serine-rich repeat protein25 Surface adhesion, binds to platelet surface and promotes tissue invasion 2+
Pneumococcal choline binding protein A49 Low manganese-induced protein, unknown function but important in lungs and blood 12+
1+=one or few animal studies. 2+=some evidence from s everal animal studies. 3+=confirmed in several animal studies. 4+=confirmed in people. TLR=toll-like receptor.
C3b=complement component 3b. GlcNac-Gal=N-acetylglucosamine-beta-(1-4)-galactose disaccharide. ABC=ATP-binding cassette. CSP=competence-stimulating peptide.
PAFR=platelet-activating factor receptor.
Table :Known virulence factors in Streptococcus pneumoniaeinfection
-
8/13/2019 pathogenesis, treatment, and prevention of pneumococcal pneumonia
5/14
Seminar
www.thelancet.com Vol 374 October 31, 2009 1547
pneumococci.5,40 Figures 3 and 4 show the role of thistoxin and other virulence factors during invasion.
Mechanisms of host recognitionPattern-recognition receptors are key components of theinnate immune system.50,51 They recognise conservedmotifs expressed by pathogens that are referred to aspathogen-associated molecular patterns. Several of thesereceptors contribute to initiation of an effective, innateimmune response to the pneumococcus (figure 4).C-reactive protein, an acute-phase protein, functions as apattern-recognition receptor for S pneumoniae. It bindsphosphorylcholine in the pneumococcal cell wall andactivates complement.52 In animal models,53 humanC-reactive protein protects against lethal infection withS pneumoniaeinfection, and in man probably contributes
to host defence during bacteraemic pneumonia.S pneumoniae uses the host-derived receptor forplatelet-activating factor to cross from lung tissue intoblood. This receptor recognises the phosphorylcholinedeterminant of its natural human ligandplatelet-activating factor. Pneumococci express phosphorylcholinein their cell wall that binds to this receptor, initiatingbacterial uptake.54 In mice deficient in this receptor,pneumococcal growth is impaired, bloodstream invasionis reduced, and survival is improved.21,55 The dendriticcell-specific intercellular adhesion molecule (ICAM-3-grabbing nonintegrin [DC-SIGN] homologueSIGN-related 1 [SIGNR1]) is a C-type lectin implicated incapture of capsular polysaccharides from S pneumoniae
by marginal-zone macrophages.56
Although SIGNR1 isnot usually expressed by alveolar macrophages,SIGNR1-/- mice are highly susceptible to pneumococcalinfection and do not clear S pneumoniaefrom their lungsor blood.57 SIGNR1 probably restricts bacterial growthduring pneumococcal pneumonia with presentation ofpneumococcal antigens to B cells by SIGNR1 onmarginal-zone splenic macrophages. Antiphosphoryl-choline IgM antibodies resulting from this presentationassist in clearance of pneumococci from the lung.57,58
Macrophage receptor with collagenous structure(MARCO) is a class A scavenger receptor expressed onalveolar macrophages that is able to bind and internaliseS pneumoniae in vitro. MARCO-/- mice have a greatly
reduced resistance against pneumococcal pneumonia,with accelerated growth of pneumococci and increasedmortality.59Toll-like receptors (TLRs) have a central role aspattern-recognition receptors in initiation of cellular innateimmune responses because they can detect many microbialpathogens at either the cell surface or in lysosomes andendosomes.50,51TLR2 is generally thought to be the mostimportant pattern-recognition receptor for gram-positivepathogens (ie, peptidoglycan, lipoteichoic acid, andbacterial lipopeptides), but its importance for pneumococciis not fully understood. S pneumoniaecell-wall componentsare recognised by TLR2,6064but TLR4 is the receptor for theproinflammatory effects of pneumolysin.6567Unexpectedly,
when many different types of TLR-deficient mice werestudied to investigate which of these receptors was mostessential to detect and defend against pneumococci, onlyTLR9-/- mice were highly susceptible to lethal infection.TLR9 detects bacterial DNA and seems to be essentialfor effective phagocytosis and killing of pneumococci bylung macrophages.68
Intracellular signalling elements of the TLR system areessential for defence against pneumococcal pneumoniain experimental systems. Mice deficient in the commonTLR-adaptor protein myeloid-differentiation primary-response protein 88 (MyD88) are very susceptible topneumococcal pneumonia, probably in part as a result ofimpaired innate immune activation by interleukin 1 andinterleukin 18.6971The clinical relevance of these findingsaccords with the discovery of children with a geneticdeficiency for MyD88 or interleukin 1 receptor-associatedkinase 4 (IRAK4), a kinase acting directly downstreamfrom MyD88, who are especially susceptible to invasivepneumococcal disease.72,73Additionally, a single nucleotide
IgA1
protease
PavA
Eno
NanA
PsrP
Pneumocin
Extracellular toxins and enzymes
Pneumolysin
Degradesextracellularmatrix
PAF receptorbinding,inflammation
Anticomplement,invasion factors
LTA
PspC
PspA
PsaA
Pili
Metal binding transporters
PiaA/PiuA Intracellular
space
Periplasmicspace
Peptidoglycancell wall
Polysaccharide
capsule
Surfaceadhesins
Cps
Hyl LytA
StrA
Figure :Virulence factors of pneumococcus
PsaA=pneumococcal surface antigen A. PiaA/PiuA=pneumococcal iron acquisition and uptake.
PsrP=pneumococcal serine-rich repeat protein. NanA=neuraminidase. Eno=enolase. PavA=pneumococcal
adhesion and virulence. LytA=autolysin. StrA=sortase A. Hyl=hyluronate lyase. LTA=lipoteichoic acid.
PspC=pneumococcal surface protein C. PspA=pneumococcal surface protein A. Cps=polysaccharide capsule.
PAF=platelet-activating factor.
-
8/13/2019 pathogenesis, treatment, and prevention of pneumococcal pneumonia
6/14
Seminar
1548 www.thelancet.com Vol 374 October 31, 2009
polymorphism in the TLR-adaptor-protein Mal affectshost defence against S pneumoniae in people.74CD14 isanother crucially important pattern-recognition receptor.22CD14-/- mice are strongly protected against disseminationof S pneumoniaefrom the respiratory tract,22suggestingthat pneumococci specifically use CD14 in thebronchoalveolar compartment to spread.
Pneumococci are slowly killed inside phagolysosomes,especially if poorly opsonised,75and this process mightprovide an opportunity for viable organisms or theirbacterial products to escape from early phagosomes andinvade the cytosol. Within the intracellular space,pneumococci can be recognised by various cytoplasmic
pattern-recognition receptors. Nucleotide-binding oligo-merisation domain protein (NOD2) recognises muramyldipeptide, a common fragment of bacterial peptido-glycan, in the cytosol.50,76Additionally, bacterial infectionleads to activation of caspase-1 by a protein complexcalled inflammasome.77Inflammasome regulates activityof caspase-1, an enzyme responsible for secretion ofthree major host-defence cytokinesinterleukin 1,interleukin 18, and interleukin 33. However, caspase-1-/-mice seem to tolerate pneumococcal pneumonia.68Thus, the clinical implications of NOD2 andinflammasomes in pneumococcal infections in peopleremain unclear.
ImmunologyRespiratory epithelial cells not only provide the mucociliarycarpet to continually remove potential pathogens from thelower airways, but also actively respond to the presence ofpathogens. Respiratory epithelium releases variousmediators such as cytokines, chemokines, and anti-microbial peptides (eg, lysozyme, defensins, andcathelicidins), contributing to innate immunity againstpneumococci.78Transgenic mice that overexpress nuclearfactor inhibitor B- (IB-) and block nuclear factor B(NFB) nuclear translocation within epithelial cells have areduced ability to clear pneumococci from the airways.79Alveolar lining cells produce a pneumococcal-bindingprotein known as surfactant protein-D (SP-D). Micedeficient in this surfactant protein have a decreasedcapacity for clearance of pneumococci and are prone to
disseminated infection.80
Alveolar macrophages represent the first phagocyticdefence in the lungs and can phagocytise and kill lownumbers of pneumococci.75,81When large numbers ofpneumococci are introduced into the lower airways,neutrophils are recruited and they become the mainphagocytic cells in the acutely inflamed lung. Alveolarmacrophages are then relegated to clearing apoptoticneutrophils.82 They also undergo apoptosis duringpneumococcal pneumoniamacrophage apoptosishelps with killing of phagocytised S pneumoniae83andkeeps pneumococcal invasion into the bloodstream toa minimum.66,81
Neutrophils predominate within cellular infiltrates in
pneumococcal pneumonia. The conventional notion ofneutrophil migration with selectin-mediated rolling and2-integrin-mediated tight adhesion to the endotheliumdoes not apply to pneumococcal pneumonia.842-integrin-deficient mice show normal neutrophiltraffi cking into lung tissue after infection withS pneumoniae.85Another host-derived, soluble adhesionmolecule known as galectin-3 has been implicated as amajor neutrophil recruitment signal in pneumococcalpneumonia.86Galectin-3-/- mice with S pneumoniaehaveaccelerated lung infection, with early disseminateddisease.87 Additionally, galectin-3 augments neutrophilphagocytosis and exerts bacteriostatic effects onS pneumoniae.
chemokines also promote an influx of neutrophilsinto lung tissue during pneumococcal pneumonia,88whereas reactive oxygen species derived fromnicotinamide adenine dinucleotide phosphate (NADPH)oxidase restrict neutrophil reflux.89 Moreover, pneumo-cocci produce chemotactic factors such as N-formyl-methionyl-leucyl-phenylalanine and pneumolysin thathelp with neutrophil recruitment.8890The net effect to ahost of neutrophil influx in pneumococcal pneumoniacan be good or bad, dependent on the virulence of thepathogen. Antineutrophil antibody treatment resulted inwidespread infection and increased mortality withserotype 3 pneumococci.91 Depletion of neutrophils
MARCO
PneumolysinCD14
LTA
LTATLR2
ChoP
S pneumoniae
MDP-PG NOD 2
p65 p50
IkB
NFkB
p300p65 p50
PAFR G-protein
Nucle
arme
mbran
e
TLR4
TIR
TLR9
MyD88
Cytokine genes, acute phase proteins
BacterialDNA
EndosomalvacuoleCell
membrane
Figure : Pattern-recognition signalling receptors and pathways in pneumococcal infection
S pneumoniaeis recognised as a pathogen in the lung by several toll-like receptors ( TLRs), including TLR2 (with
pneumococcal lipoteichoic acid [LTA] as its major ligand), TLR4 (recognises pneumolysin), and TLR9 (within
endosomes; interacts with bacterial DNA). Macrophage receptor with collagenous structure (MARCO) expressed
by alveolar macrophages contributes to innate immune response in lungs. PAFR is shown as a pattern-recognition
receptor because it recognises pneumococcal phosphorylcholine and LTA, thereby contributing to tissue invasion.
(Soluble) cluster-determining (CD) 14 probably further helps S pneumoniaeinvade from the airways into blood.
Within cytoplasm, the muramyl dipeptide component of pneumococcal peptidoglycan (MDP-PG) is recognised by
nucleotide-binding oligomerisation domain (NOD-2) and can activate host defence and inflammation.
ChoP=phosphorylcholine. PAFR=platelet-activating factor receptor. TIR=toll-interleukin-1 receptor domain.
MyD88=myeloid differentiation primary response protein-88. NFB=nuclear factor B. IB=inhibitor B.
-
8/13/2019 pathogenesis, treatment, and prevention of pneumococcal pneumonia
7/14
Seminar
www.thelancet.com Vol 374 October 31, 2009 1549
worsened outcomes in those with a high infectious doseof serotype 4 S pneumoniae, but not in those with a lowinoculum.92 By contrast, neutrophil depletion in micewith a serotype 8 strain improved survival and resulted inreduced bacteraemia.93 Pneumococcal pneumonia isuncommon in adults with isolated neutropenia andwithout other concomitant immune defects.
The greatly increased frequency of pneumococcalpneumonia in patients with AIDS attests to the protectiverole of CD4+ T cells in resistance to pneumococci.S pneumoniae elicits an early accumulation of T cells inlung infection94,95a response that is dependent onpneumolysin. MHCII-/- mice have a pronounced deficiency
in CD4+ T cells and are highly susceptible to pneumococcalpneumonia.95 T cells make up only 2% of circulating Tcells but are present in increased concentrations inrespiratory tissues. Pneumococcal pneumonia is associatedwith an increase in T-cell subsets in lung tissues.96,97V4T cell-/- mice are very susceptible to pneumococci andshow reduced traffi cking of neutrophils into lung tissue.96 T cells also contribute to the resolution phase ofS pneumoniae infection.97 Natural killer T cells have acrucially important role in defence against pneumococcalpneumonia.98Treatment of mice with -galactosylceramide,which specifically activates V14+ natural killer T cells,improves clearance of pneumococci.99
Clearance of pneumococci from the circulation stronglydepends on opsonisation by complement componentsand phagocytosis by myeloid cells.1,3 Disruption of thecommon C3 pathway profoundly impairs resistance topneumococci.85 Of the three complement cascades(classic, alternative, and mannose-binding lectinpathways), the classic pathway has been identified asmost important in host defence against pneumococci. 100Natural IgM antibodies contribute to innate immuneresponses through activation of the classical complementpathway.100Antibody-independent activation of the classicpathway also arises through SIGNR1,101 C-reactiveprotein,52and serum amyloid P.102
Recognition of pneumococci by immune cells withinthe respiratory tract generates an array of proinflammatoryand anti-inflammatory cytokines. Some of these cytokinesplay a pivotal part in innate defence against pneumococci.Tumour necrosis factor (TNF) is of particularimportance because its inhibition or elimination greatlyhelps with growth and dissemination of pneumococci103an effect mainly mediated by the type I TNF receptor. 104Interleukin 1 seems to have a similar yet less important protective role.70Inhibition of both TNF and interleukin 1renders animals very susceptible to pneumococcalpneumonia and other types of bacterial infections.70,105Other proinflammatory cytokines that are important for
Endothelium
Pneumococcus
AMTLRs
MARCOPAFR
CD14
PMN influx
C5a chemokines,galectin-3, Ply, fMLP
Host defenceIL1, TNF, IL18,
C, TF, AMPs, SP-D
A
Lung
interstitium
Air spaces(alveolus) PMN
efflux
sCD14, PAFR
Invasion
IgM, IgG, C,CRP, SAP
H2O
B
Pneumococcus
Capillary
Alveoli
Figure :Major pathological events in invasive pneumococcal pneumonia
(A) Pneumococci that enter lower airways are recognised by pattern-recognition receptors, including toll-like receptors (TLRs; on epithelial cells and alveolar macrophages) and macrophage receptor
with collagenous structure (MARCO; on alveolar macrophages). At low infectious doses, epithelial cells and alveolar macrophages can clear S pneumoniaewithout help from recruited neutrophils, in
part by release of protective inflammatory mediators such as interleukin 1 (IL 1), tumour necrosis factor ( TNF ), interleukin 18 (IL 18), complement products (C), surfactant protein-D (SP-D), and
antimicrobial peptides (AMPs). These mediators continue to have a role after infection with a high infectious dose, whereby polymorphonuclear cells (PMN) are recruited by chemoattraction through
various mediators including C5a, and galectin-3, and pneumococcal products such as pneumolysin (Ply) and formyl-methionine-leucine-phenylalanine (fMLP). (B) If alveolar defence mechanisms are
overwhelmed by multiplication of pneumococci, invasion of S pneumoniaeinto the bloodstream takes place, helped by platelet-activating factor receptor (PAFR) and (soluble) CD14 (sCD14). In the
bloodstream, several host proteins contribute to host defence including natural IgM antibodies, C, C reactive protein (CRP), and serum amyloid (SAP). TF=tissue factor. AM=alveolar macrophage.
-
8/13/2019 pathogenesis, treatment, and prevention of pneumococcal pneumonia
8/14
Seminar
1550 www.thelancet.com Vol 374 October 31, 2009
defence against pneumococci are interleukin 6 andinterleukin 18,71,106whereas the anti-inflammatory cytokineinterleukin 10 impairs defence mechanisms during bothprimary and postinfluenza pneumococcal pneumonia.98
Surprisingly, interferon inhibits antibacterial defencein models of either primary or postinfluenza pneumo-coccal pneumonia,91,107 possibly because this cytokinedecreases the capacity of alveolar macrophages to killS pneumoniae.91 Other investigators108,109 have reportedwidely disparate results with blockers of interferon .Interleukin 12, a prominent inducer of interferon , hasbeen reported to either enhance109or have no effect77onhost defence against pneumococcal pneumonia. Together,these studies show that cytokine-mediated enhancementof lung inflammation improves outcomes for animalswith S pneumoniae pneumonia, although interferon might worsen outcomes.
S pneumoniae pneumonia results in activation ofnuclear factor B within the lungs.110 Inhibition ofnuclear factor B activation increases lethality andenhances bacterial growth in animal models of infectionwith S pneumoniae.79,111A role for adequate activation ofthis factor in defence against pneumococci in people issupported by the association between commonpolymorphisms in the inhibitor B genes NFKBIAandNFKBIE, and increased susceptibility to invasivepneumococcal disease.112 Extensive cross-talk existsbetween the coagulation system and the innate immunesystem in response to microbial infection.113 Thesesystems simultaneously activate and collaborate tocontain and eradicate localised infection.114 Pneumo-coccal pneumonia is associated with both intrapulmonaryand systemic activation of the coagulation systema
response initiated by tissue factor.115,116
Anticoagulanttreatment with recombinant tissue-factor pathwayinhibitor, activated protein C, or antithrombin greatlyrestricts lung coagulopathy in pneumococcal pneumoniain animals.117 Infusion of recombinant human-activatedprotein C improves 28 day mortality in patients withsevere sepsis and reduces the high likelihood of dying. 116This beneficial effect was most evident in a subgroup ofpatients who had pneumococcal pneumonia.116Figure 5shows the host responses within the lung induced byS pneumoniae.
Clinical featuresPneumococcal pneumonia usually presents as typical,
acute community-acquired pneumonia. It generallybegins with a mild upper-airway irritation attributableto a respiratory viral infection. When pneumococci aredeposited into the lower airways they are usually expelledby mucociliary clearance, cough, antimicrobial peptides,and local innate immune defences. Should thesesystems fail to eliminate the pathogen, systemicinflammation ensues with characteristic signs andsymptoms of bacterial pneumonia.1,3 Onset of severeillness is abrupt, and develops with a shaking chill,fever, malaise, cough, and dyspnoea. The cough becomesproductive with purulent sputum, sometimes withbrownish or blood-tinged sputum with respirophasicchest pain and progressive dyspnoea. Left untreated,
this toxic illness can progress to acute respiratory failure,septic shock, multiorgan failure, and death withinseveral days from onset.
Figure 6 shows typical radiographic findings in anelderly patient with bacteraemic pneumococcalpneumonia. Resolution of radiographic findings for thisillness is slow, with abnormal findings in half of patientsup to 6 weeks after symptom onset.118 Need for andclinical usefulness of routine follow-up radiographs afteruncomplicated pneumococcal pneumonia is questionableand no longer recommended.119121 Recurrent ornon-resolving pneumonia in the same anatomicallocation is suggestive of a possible endobrochial lesion.
A B
C D
Figure : Typical radiographic findings in pneumococcal pneumonia
This previously healthy woman aged 73 years presented to hospital with bacteraemic multilobar left-sided
pneumococcal pneumonia (A). 5 days later, the infiltrate worsened (B) despite appropriate therapy (ceftriaxone
and clarithromycin) for this penicillin-susceptible strain ofS pneumoniae. By day 10, chest radiograph (C) shows a
parapneumonic effusion, extensive consolidation, and areas of focal cavitation. A chest CT image on day 12 (D)
confirms cavitation and consolidation with air bronchograms. The patient slowly recovered with antimicrobial
therapy alone and had a chest radiogram after 2 months that was clear apart from minor parenchymal scarring in
the left lower lobe.
-
8/13/2019 pathogenesis, treatment, and prevention of pneumococcal pneumonia
9/14
Seminar
www.thelancet.com Vol 374 October 31, 2009 1551
Recurrent pneumococcal pneumonia in differentbronchopulmonary segments should prompt a searchfor an underlying immunocompromised state. HIVinfection, congenital or acquired B-cell disorders, andciliary dyskinesia are common concerns in patientsyounger than 18 years, and multiple myeloma and otherymphoreticular disorders are suspected in patients olderthan 65 years.118
Clinical presentation of pneumococcal pneumoniamight not be typical in some vulnerable patients, anddiagnosis can be diffi cult. Invasive pneumococcal diseasecan be subtle in its early phases in neonates, elderlypeople, severely immunocompromised patients, asplenichosts, and in various concomitant co-morbid illnesses.118,122Patients can present with extrapulmonary symptoms(meningitis, overwhelming sepsis, pericarditis, peri-
tonitis, mastoiditis, and endocarditis) before showingevidence of bacterial pneumonia.
DiagnosisDiagnostic methods for pneumococcal pneumonia havenot changed appreciably since Pasteur and Sternbergfirst isolated S pneumoniaein 1881, and Christian Gramused his famous stain to reveal pneumococci under themicroscope in 1886 (figure 7). Pneumococci grow readilyon blood agar plates in a CO incubator at 37C.S pneumoniae colonies are haemolytic and oftenumbilicate because of autolysis. Cultures from sputum,blood, and other tissue sites should be obtained beforeempirical antibiotic therapy is started.118
Two innovations for rapid diagnosis of pneumococcaldisease are now available and can be quite useful. Thefirst is urinary antigen detection of the C polysaccharidefrom the pneumococcal cell wall by an immunochromato-graphy assay. This test compares favourably with cultureand gram stain for detection of invasive pneumococcaldisease.123 The assay is most sensitive in severepneumococcal disease and bacteraemia, and can befalsely negative in early pneumococcal infection. Thisassay is especially useful in patients from whom clinicianshave diffi culty getting an adequate sputum sample, andin those who have already begun antibiotic treatmentbefore cultures were obtained. The urinary antigenremains positive for weeks after onset of severe
pneumococcal pneumonia. Major drawbacks of thisassay are an inability to acquire antimicrobialsusceptibility data from this test, and loss of sensitivitywith mild infections. The second is the many non-cultureassays based on nucleic acids for pneumococcalpneumonia that are now available or in develop-ment. They are rapid and highly specific, withS pneumoniae-specific DNA sequences as targets fordetection assays.124,125 To distinguish pneumococcalcolonisation from infection remains a challenge. Perhapsthese rapid diagnostic techniques will be useful formaking management decisions about patients withpneumococcal infections in the future.
TreatmentThe initial, uniform activity of penicillin againstS pneumoniaeresulted in this antibiotic being treatmentof choice for community-acquired pneumonia since thelate 1940s.1 Penicillin-resistant strains of S pneumoniae
were first noted in the mid 1970s and resistant cloneshave now spread worldwide.1,118,126Penicillin resistance isrelated to structurally modified penicillin-bindingproteins of S pneumoniae. These modified bindingproteins allow peptidoglycan synthesis despite thepresence of penicillin. This resistance mechanism canoften be overcome with high doses of penicillin. Presentclinical laboratory standards that define the minimuminhibitory concentration for susceptibility, intermediateresistance, and high-level resistance to penicillin varysomewhat by region (table 2).118,120,121
Non-meningeal S pneumoniae strains expressingintermediate and even high-level resistance to penicillincan still be treated with high-dose, -lactam antibiotics
(penicillins, or second or third generation cephalo-sporins).121,126,127 Meningitis attributable to S pneumoniaewith even intermediate resistance to pneumococcinecessitates use of other agents to assure a successfuloutcome.118Table 2 provides the present recommendedtreatment regimens and comparisons between theBritish,120 European,121 and American118 guidelines forcommunity-acquired pneumonia and specific types ofS pneumoniaeinfections.
Antimicrobial resistance of pneumococci tomacrolides,128 fluoroquinolones,129vancomycin,126 trime-thoprim, 118 and various other antimicrobial agents isincreasingly recognised worldwide.126,127When feasible,
m
10 200
Figure : Classic gram stain findings in acute pneumococcal pneumonia
Note numerous lancet-shaped gram-positive diplococci and neutrophilic cellular infiltrate. Pneumococci as
diplococci (arrows). (High power magnification under oil immersion 1000.)
-
8/13/2019 pathogenesis, treatment, and prevention of pneumococcal pneumonia
10/14
Seminar
1552 www.thelancet.com Vol 374 October 31, 2009
S pneumoniae strains isolated from patients who aresuffi ciently ill to need hospital admission shouldundergo sensitivity testing because susceptibilities to
standard agents are no longer assured.126
This testing isespecially important in assessment of blood orcerebrospinal fluid isolates, and in geographical areaswhere resistance to standard antibiotics is a knownproblem.
Much controversy exists about the advisability of useof combination therapy with a -lactam and eithera macrolide or respiratory fluoroquinolone forbacteraemic pneumococcal pneumonia. Results ofseveral retrospective and small prospective studies130132show a possible survival advantage with combinationtherapy, even when the pneumococcal isolate issusceptible to -lactams. Some form of in-vivo synergymight exist, or combination therapy might treat some
unrecognised co-pathogens not covered by -lactams(eg, Mycoplasma pneumoniae, Chlamydophila spp, orother untypical pathogens). Macrolides and perhapseven fluoroquinolones might limit excessive host-derived inflammatory reactions to severe pneumococcalpneumonia. 130132 In a laboratory study,133 researchersreported improved outcomes and reduced lunginflammation when inhibitors of bacterial proteinsynthesis (clindamycin or azithromycin) were added toampicillin for postinfluenza pneumococcal pneumonia.These protein inhibitors might reduce synthesis ofmicrobial mediators that contribute to lung inflam-mation. Convincing clinical evidence from large
numbers of people to show that combination therapy isbetter than monotherapy is highly desirable. Individualdecisions about dual therapy for severe invasive
pneumococcal disease presently rest on available butinsuffi cient clinical information.Early intervention with effective antimicrobial agents
provides a substantial survival advantage in severepneumococcal pneumonia. Antibiotics should be startedas soon as possible (01 mg/L (S), 0110 mg/L (I), and >14 mg/L
(R); ERS 20 (R); ATS 20 g/mL (S), 24 g/ml (I), 8 g/ml (R). For meningeal isolates: ATS
-
8/13/2019 pathogenesis, treatment, and prevention of pneumococcal pneumonia
11/14
Seminar
www.thelancet.com Vol 374 October 31, 2009 1553
compromised patients, and in infants younger thanage 2 yearsprecisely those at greatest risk for severepneumococcal disease.
The covalently linked polysaccharide-protein conjugatepneumococcal vaccine has been in use for almost 10 yearsand was very successful16,17 (figure 1). The seven-valentconjugate vaccine (Prevenar; Wyeth) is approved for usemainly in children younger than 2 years, and for childrenyounger than 5 years with high-risk conditions. Thisvaccine targets the pneumococcal serotypes 4, 6B, 9V, 14,18C, 19F, and 23F. These seven serotypes are responsiblefor 80% of pneumococcal infections in children living indeveloped countries. The vaccine is highly immunogenicin young children because it is T cell-dependent andovercomes the intrinsic loss of immunogenicity topolysaccharide vaccines within the first 2 years of life. 16
This vaccine has reduced incidence of invasivepneumococcal disease in children in the USA youngerthan 1 year by 82%.17One of the most remarkable attributesof the pneumococcal conjugate vaccine has been thedegree of herd immunity it generates. Frequency ofinvasive pneumococcal disease infection in non-vaccinatedsiblings and even adult contacts has declinedsubstantially.16,134,135 Young children are the primaryreservoir for pneumococcal colonisation in people, andthus elimination of the carrier state in children reducesrisk of transmission to the rest of the population.
Despite the effectiveness of the conjugate vaccine,disturbing patterns are developing in the epidemiologyof pneumococcal disease that threaten the long-term
benefits of the vaccine. Invasive disease attributable tonon-vaccine serotypes of S pneumoniae has greatlyincreased.18 Vaccine-induced anticapsular antibodiesrestrict access of vaccine-associated serotypes to thehuman upper airways. This niche is now available tonon-vaccine pneumococcal serotypes or otheroropharyngeal pathogens such as Staphylococcusaureus.1618 Vaccine replacement by non-virulentserotypes would be acceptable, but virulent, non-vaccineserotypes can also replace vaccine serotypes of pneumo-cocci.3,136,137Capsular switching probably arises throughtransformation of capsular genes from one serotype toanother.18,138140 Such events could arm an intrinsicallyvirulent strain of S pneumoniaepreviously encapsulated
with a vaccine-related serotype with a new antigenicpolysaccharide coat to avoid vaccine-induced immunerecognition.
Analysis of patterns of serotype replacement over timeafter widespread institution of the seven-valent conjugatevaccine is needed. An expanded conjugate vaccineincluding serotypes not covered in the present vaccinemight be useful. Serotype 19A S pneumoniaeis a specificconcern.136 This serotype has expanded greatly sinceintroduction of the conjugate pneumococcal vaccine,138,139and has much virulence potential as a pulmonary andextrapulmonary pathogen. Moreover, it has the propensityto acquire multiple drug-resistance genes, complicating
antimicrobial therapy against this organism.139,140 Othervaccine approaches include development of vaccinesagainst many, highly conserved, immunogenic proteinantigenseg, adhesins, pneumolysin, invasion proteins,and transport proteins.5
ConclusionsThe pneumococcus fascinates immunologists, yetfrustrates clinicians and public-health offi cials attemptingto control it. Although the human respiratory tract hasmany local and systemic immune defences, a range ofpneumococcal virulence factors work together to causeinvasive disease. The capacity of S pneumoniaeto resistantimicrobial agents and escape immune defences showsthat control of this pathogen will not be easy to achieve.Thus a multifaceted approach with new generation
vaccines, novel antimicrobial therapies, and improvedadjuvant treatments will be needed.
Contributors
Both authors contributed equally to this Seminar.
Conflicts of interest
We declare that we have no conflicts of interest.
References1 Watson DA, Musher DM, Jacobson JW, Verhoef J. A brief history
of the pneumococcus in biomedical research: a panoply ofscientific discovery. Clin Infect Dis1993; 17:91324.
2 Berkley JA, Lowe BS, Isaiah MP, et al. Bacteremia among childrenadmitted to a rural hospital in Kenya. N Engl J Med2005;352:3947.
3 Bogaert D, de Groot R, Hermans R. Streptococcus pneumoniaecolonisation: the key to pneumococcal disease.Lancet Infect Dis2004; 4: 14454.
4 Weinberger DM, Dagan R, Givon-Lavi N, et al. Epidemiologicevidence for serotype-specific acquired immunity topneumococcal carriage.J Infect Dis2008; 197:151118.
5 Kadioglu A, Weiser JN, Paton JC, Andrew PW. The role ofStreptococcus pneumoniaevirulence factors in host respiratorycolonization and disease. Nature RevMicrobiol 2008; 6:288301.
6 Orihuela CJ, Gao G, Francis KP, et al. Tissue-specificcontributions of pneumococcal virulence factors to pathogenesis.
J Infect Dis2004; 190:166169.
7 Zhang Q, Bagrade L, Bernatoniene J, et al. Low CD4 T cellimmunity to pneumolysin is associated with nasopharyngealcarriage of pneumococci in children.J Infect Dis2007;195: 1194202.
8 Dudley S, Ashe K, Winther B, Hendley JO. Bacterial pathogens ofotitis media and sinusitis: Detection in the nasopharynx withselective agar media.J Lab Clin Med2001; 138:33842.
9 Romney MG, Hull MW, Gustafson R, et al. Large communityoutbreak of Streptococcus pneumoniaeserotype 5 invasive infection inan impoverished, urban population. Clin Infect Dis2008; 47:76874.
10 Cherian T, Steinhoff MC, Harrison LH, et al. A cluster of invasivepneumococcal disease in young children in child care.JAMA1994;271:69597.
11 Hoge CW, Reichler MR, Dominguez EA, et al. An epidemic ofpneumococcal disease in an overcrowded, inadequately ventilatedjail. N Engl J Med1994; 331:64348.
12 Crum NF, Wallace MR, Lamb CR, et al. Halting a pneumococcalpneumonia outbreak among United States Marine Corps trainees.Am J Prev Med2003; 25:10711.
13 Hare KM, Morris P, Smith-Vaughan H, Leach AJ. Random colonyselection versus colony morphology for detection of multiplepneumococcal serotypes in nasopharyngeal swabs.Pediatr Infect Dis J2008; 27: 17880.
14 Smith T, Lehmann D, Montgomery J, et al. Acquisition andinvasiveness of different serotypes of Streptococcus pneumoniaeinyoung children. Epidemiol Infect1993; 111:2739.
-
8/13/2019 pathogenesis, treatment, and prevention of pneumococcal pneumonia
12/14
Seminar
1554 www.thelancet.com Vol 374 October 31, 2009
15 Brueggemann AB, Griffi ths DT, Meats E, et al. Clonal relationshipsbetween invasive and carriage Streptococcus pneumoniaeandserotype- and clone specific differences in invasive disease potential.
J Infect Dis2003, 187: 142432.16 Miller EV, Watt JP, Bronsdon MA, et al. Indirect effect of 7-valentpneumococcal conjugate vaccine on pneumococcal colonizationamong unvaccinated household members. Clin Infect Dis2008;47:98996.
17 Centers for Disease Control and Prevention. Invasive pneumococcaldisease in children 5 years after conjugate vaccine introductioneight states, 19982005. MMWRMorb Mortal Wkly Rep2008;57: 14448.
18 Hicks LA, Harrison LH, Flannery B, et al. Incidence ofpneumococcal disease due to non-pneumococcal conjugate vaccine(PCV7) serotypes in the United States during the era of widespreadPCV7 vaccination 19982004.J Infect Dis2007; 196: 134654.
19 Bruce MG, Deeks SL, Zulz T, et al. International circumpolarsurveillance system for invasive pneumococcal disease, 19992005.Emerg Infect Dis2008; 14:2533.
20 Gulmez SE, Holm A, Frederiksen H, et al. Use of proton pumpinhibitors and the risk of community-acquired pneumonia:a population-based case-control study. Arch Intern Med 2007;167:95055.
21 van der Sluijs KF, van Elden LJR, Nijhuis M, et al. Involvement ofthe platelet activating factor receptor in host defense againstStreptococcus pneumoniaeduring postinfluenza pneumonia.Am J Physiol Lung Cell Mol Physiol2005; 290: L19499.
22 Dessing MC, Knapp S, Florquin S, et al. CD14 facilitates invasiverespiratory tract infection by Streptococcus pneumoniae.Am J Respir Crit Care Med2007; 175:60411.
23 Tettelin H, Nelson KE, Paulsen IT, et al. Complete genome sequenceof a virulent isolate of Streptococcus pneumoniae.Science2001; 293:498506.
24 Lanie JA, Ng WL, Kazmierczak KM, et al. Genome sequence ofAverys virulent serotype 2 strain D39 of Streptococcus pneumoniaeand comparison with that of unencapsulated laboratory strain R6.
J Bacteriol2007; 189:3851.
25 Obert C, Sublett J, Kaushal D, et al. Identification of a candidateStreptococcus pneumoniaecore genome and regions of diversitycorrelated with invasive pneumococcal disease. Infect Immun2006;
74:476677.26 Hava DL, Camilli A. Large-scale identification of serotype 4
Streptococcus pneumoniae virulence factors. Mol Microbiol2002;45:1389406.
27 Orihuela CJ, Radin JN, Sublett JE, et al. Microarray analysis ofpneumococcal gene expression during invasive disease.Infect Immun2004; 72:558296.
28 Williams SP, Tait-Kamradt AG, Norton JE, et al. Nucleotidesequence changes between Streptococcus pneumoniaeR6 and D39strains determined by an oligonucleotide hybridization DNAsequencing technology.J Microbiol Methods2007; 70:6574.
29 Bijlsma JJ, Burghout P, Kloosterman TG, et al. Development ofgenomic array footprinting for identification of conditionallyessential genes in Streptococcus pneumoniae.Appl Environ Microbiol2007; 73: 151424.
30 Brown JS, Gilliland SM, Spratt BG, Holden DW. A locus containedwithin a variable region of pneumococcal pathogenicity island 1contributes to virulence in mice. Infect Immun2004; 72:158793.
31 Silva NA, McCluskey J, Jefferies JMC, et al. Genomic diversitybetween strains of the same serotype and multilocus sequence typeamong pneumococcal clinical isolates. Infect Immun2006;74:351318.
32 Dawid S, Roche A, Weiser J. The blp bacteriocins of Streptococcuspneumoniaemediate intraspecies competition both in vitro and invivo. Infect Immun2007; 75:44551.
33 Ogglioni MR, Trappetti C, Kadioglu A, et al. Switch from planktonicto sessile life: a major event in pneumococcal pathogenesis.Mol Microbiol2006; 61:1196210.
34 Martin-Galiano AJ, Wells JM, de la Campa AG. Relationshipbetween codon biased genes, microarray expression values andphysiological characteristics of Streptococcus pneumoniae.Microbiol2004; 50:231325.
35 Aziz RK, Kotb Malak. Rise and persistence of global M1T1 clone ofStreptococcus pyogenes. Emerg Infect Dis2008; 14: 151117.
36 Moran GJ, Krishnadasan A, Gorwitz RJ, et al. Methicillin-resistantS aureusinfections among patients in the emergency department.N Engl J Med2006; 355:66574.
37 Kelly CP, LaMont JT. Clostridium diffi cilemore diffi cult than ever.N Engl J Med 2008; 359:193240.
38 Nelson A, Roche AM, Gould JM, et al. Capsule enhancespneumococcal colonization by limiting mucus-mediated clearance.Infect Immun2007; 75:8390.
39 Hammerschmidt S, Wolff S, Hocke A, et al. Illustration ofpneumococcal polysaccharide capsule during adherence andinvasion of epithelial cells. Infect Immun2005; 73:465367.
40 Hirst RA, Kadioglu A, OCallaghan C, Andrew PW. The role ofpneumolysin in pneumococcal pneumonia and meningitis.Clin Exp Immunol 2004; 138:195201.
41 Rosenow C, Ryan P, Weiser JN, et al. Contribution of novelcholine-binding proteins to adherence, colonization andimmunogenicity of Streptococcus pneumoniae. Mol Microbiol1997;25:81929.
42 Iannelli F, Chiavolini D, Ricci S, et al. Pneumococcal surfaceprotein C contributes to sepsis caused by Streptococcus pneumoniaein mice. Infect Immun 2004; 72:307780.
43 Quin LR, Carmicle S, Dave S, et al. In vivo binding of complementregulator factor H by Streptococcus pneumoniae.J Infect Dis2005;192:19962003.
44 Weidenmaier C, Peschel A. Teichoic acids and related cell-wallglycopolymers in Gram-positive physiology and host interactions.Nature Rev Microbiol2008; 6:27687.
45 Jedrzejas MJ. Pneumococcal virulence factors: structure andfunction. Microbiol Mol Biol Rev 2001; 65:187207.
46 Paterson GK, Mitchell TJ. The role of Streptococcus pneumoniaesortase A in colonization and pathogenesis. Microbes Infect2006;8: 14553.
47 Rosch JW, Mann B, Thornton J, et al. Convergence of regulatorynetworks on the pilus locus of Streptococcus pneumoniae.Infect Immun2008; 76:318796.
48 Holmes A, McNab R, Millsap KW, et al. The pavA gene ofStreptococcus pneumoniaeencodes a fibronectin-binding protein thatis essential for virulence. Mol Microbiol 2001; 41:1395408.
49 Glover DT, Hollingshead SK, Briles DE. Streptococcus pneumoniae
surface protein pcpA elicits protection against lung infection andfatal sepsis. Infect Immun 2008; 76:276776.
50 Akira S. Uematsu S, Takeuchi O. Pathogen recognition and innateimmunity. Cell2006; 124:783801.
51 Beutler B, Jiang Z, Georgel P, et al. Genetic analysis of hostresistance: toll-like receptor signaling and immunity at large.Annu Rev Immunol2006; 24:35389.
52 Suresh MV, Singh SK, Ferguson DA Jr, Agrawal A. Role of theproperty of C-reactive protein to activate the classical pathway ofcomplement in protecting mice from pneumococcal infection.
J Immunol2006; 176: 436974.
53 Suresh MV, Singh SK, Ferguson DA Jr, Agrawal A. HumanC-reactive protein protects mice from Streptococcus pneumoniaeinfection without binding to pneumococcal C-polysaccharide.
J Immunol2007; 178: 115863.
54 Cundell DR, Gerard NP, Gerard C, et al. Streptococcus pneumoniaeanchor to activated human cells by the receptor forplatelet-activating factor. Nature1995; 377:43538.
55 Rijneveld AW, Weijer S, Florquin S, et al. Improved host defenseagainst pneumococcal pneumonia in platelet-activating factorreceptor-deficient mice.J Infect Dis2004; 189:71116.
56 Kang YS, Kim JY, Bruening SA, et al. The C-type lectin SIGN-R1mediates uptake of the capsular polysaccharide ofStreptococcus
pneumoniaein the marginal zone of mouse spleen.Proc Natl Acad Sci USA2004; 101:21520.
57 Koppel EA, Wieland CW, van den Berg VC, et al. Specific ICAM-3grabbing nonintegrin-related 1 (SIGNR1) expressed by marginalzone macrophages is essential for defense against pulmonaryStreptococcus pneumoniaeinfection. Eur J Immunol 2005;35: 296269.
58 Koppel EA, Litjens M, van den Berg VC, et al. Interaction ofSIGNR1 expressed by marginal zone macrophages with marginalzone B cells is essential to early IgM responses against Streptococcus
pneumoniae.Mol Immunol2008; 45:288187.
-
8/13/2019 pathogenesis, treatment, and prevention of pneumococcal pneumonia
13/14
Seminar
www.thelancet.com Vol 374 October 31, 2009 1555
59 Arredouani M, Yang Z, Ning Y, et al. The scavenger receptorMARCO is required for lung defense against pneumococcalpneumonia and inhaled particles.J Exp Med2004; 200:26772.
60 Knapp S, Weiland CW, van t Veer C, et al. Toll-like receptor 2 playsa role in the early inflammatory response to murine pneumococcalpneumonia but does not contribute to antibacterial defense.
J Immunol 2004; 172:313238.
61 Mogensen TH, Paludan SR, Kilian M, Ostergaard L. LiveStreptococcus pneumoniae, Haemophilus influenzae,and Neisseriameningitidisactivate the inflammatory response through Toll-likereceptors 2, 4, and 9 in species-specific patterns.J Leukoc Biol2006;80:26777.
62 Khan AQ, Chen Q, Wu ZQ, et al. Both innate immunity and type 1humoral immunity to Streptococcus pneumoniaeare mediated byMyD88 but differ in their relative levels of dependence on toll-likereceptor 2.Infect Immun2005; 73: 298307.
63 Seo HS, Michalek SM, Nahm MH. Lipoteichoic acid is important ininnate immune responses to gram-positive bacteria.Infect Immun2008; 76:20613.
64 Moore LJ, Pridmore AC, Dower SK, Read RC. Penicillinenhances the toll-like receptor 2-mediated proinflammatoryactivity of Streptococcus pneumoniae.J Infec t Dis 2003;188: 104048.
65 Malley R, Henneke P, Morse SC, et al. Recognition of pneumolysinby Toll-like receptor 4 confers resistance to pneumococcal infection.Proc Natl Acad Sci USA2003; 100: 196671.
66 Srivastava A,Henneke P, Visintin A, et al. The apoptotic response topneumolysin is Toll-like receptor 4 dependent and protects againstpneumococcal disease. Infect Immun2005; 73:647987.
67 Lee KS, Scanga CA, Bachelder EM, et al. TLR2 synergizes with bothTLR4 and TLR9 for induction of the MyD88-dependent spleniccytokine and chemokine response to Streptococcus pneumoniae.Cell Immunol2007; 245:10310.
68 Albiger B, Dahlberg S, Sandgren A, et al. Toll-like receptor 9 acts atan early stage in host defence against pneumococcal infection.Cell Microbiol 2007; 9:63344.
69 Albiger B, Sandgren A, Katsuragi H, et al. Myeloid differentiationfactor 88-dependent signalling controls bacterial growth duringcolonization and systemic pneumococcal disease in mice.Cell Microbiol2005; 7:160315.
70 Rijneveld AW, Florquin S, Branger J, et al. TNF-alphacompensates for the impaired host defense of IL-1 type Ireceptor-deficient mice during pneumococcal pneumonia.
J Immunol2001; 167:524046.
71 Lauw FN, Branger J, Florquin S, et al. IL-18 improves the earlyantimicrobial host response to pneumococcal pneumonia.
J Immunol2002; 168:37278.
72 Von Bermuth H, Picard C, Zhongbo J, et al. Pyogenic bacterialinfections in humans with MyD88 deficiency. Science2008;321: 69196.
73 Ku CL, von Bernuth H, Picard C, et al. Selective predisposition tobacterial infections in IRAK-4-deficient children: IRAK-4-dependentTLRs are otherwise redundant in protective immunity.
J Exp Med2007; 204: 240722.
74 Khor CC, Chapman SJ, Vannberg FO, et al. A Mal functionalvariant is associated with protection against invasive pneumococcaldisease, bacteremia, malaria and tuberculosis. Nat Genet2007;39:52328.
75 Gordon SB, Irving GR, Lawson RA, Lee ME, Read RC. Intracellulartraffi cking and killing of Streptococcus pneumoniaeby humanalveolar macrophages are influenced by opsonins.Infect Immun2000; 68:228693.
76 Opitz B, Pschel A, Schmeck B, et al. Nucleotide-bindingoligomerization domain proteins are innate immune receptors forinternalized Streptococcus pneumoniae.J Biol Chem2004;279: 3642632.
77 Ogura Y, Sutterwala FS, Flavell RA. The inflammasome: first line ofthe immune response to cell stress. Cell2006; 126:65962.
78 Bals R, Hiemstra PS. Innate immunity in the lung: how epithelialcells fight against respiratory pathogens. Eur Respir J 2004;23:32733.
79 Quinton LJ, Jones MR, Simms BT, et al. Functions and regulation ofNF-kappaB RelA during pneumococcal pneumonia.
J Immunol2007; 178: 1896903.
80 Jounblat R, Clark H, Eggleton P, et al. The role of surfactantprotein D in the colonisation of the respiratory tract and onsetof bacteraemia during pneumococcal pneumonia. Respir Res
2005; 6:126.81 Dockrell DH, Marriott HM, Prince LR, et al. Alveolar macrophageapoptosis contributes to pneumococcal clearance in a resolvingmodel of pulmonary infection.J Immunol2003; 171:538088.
82 Knapp S, Leemans JC, Florquin S, et al. Alveolar macrophages havea protective antiinflammatory role during murine pneumococcalpneumonia. Am J Respir Crit Care Med2003; 167:17179.
83 Marriott HM, Hellewell PG, Cross SS, et al. Decreased alveolarmacrophage apoptosis is associated with increased pulmonaryinflammation in a murine model of pneumococcalpneumonia.J Immunol2006; 177:648088.
84 Mizgerd JP, Meek BB, Kutkoski GJ, et al. Selectins and neutrophiltraffi c: marginat ion and Streptococcus pneumoniae-inducedemigration in murine lungs.J Exp Med1996; 184: 63945.
85 Rijneveld AW, de Vos AF, Florquin S, Verbeek JS, van der Poll T.CD11b limits bacterial outgrowth and dissemination during murinepneumococcal pneumonia.J Infect Dis2005; 191:175560.
86 Sato S, Ouellet N, Pelletier I, et al. Role of galectin-3 as an adhesion
molecule for neutrophil extravasation during streptococcalpneumonia.J Immunol2002; 168:181322.
87 Farnworth SL, Henderson NC, Mackinnon AC, et al. Galectin-3reduces the severity of pneumococcal pneumonia by augmentingneutrophil function. Am J Pathol2008; 172:395405.
88 Gauthier JF, Fortin A, Bergeron Y, et al. Differential contribution ofbacterial N-formyl-methionyl-leucyl-phenylalanine and host-derivedCXC chemokines to neutrophil infiltration into pulmonary alveoliduring murine pneumococcal pneumonia.Infect Immun2007; 75:536167.
89 Marriott HM, Jackson LE, Wilkinson TS, et al. Reactive oxygenspecies regulate neutrophil recruitment and survival inpneumococcal pneumonia. Am J Respir Crit Care Med2008;177:88795.
90 Fillion I, Ouellet N, Simard M, et al. Role of chemokines andformyl peptides in pneumococcal pneumonia-inducedmonocyte/macrophage recruitment.J Immunol2001;166:735361.
91 Sun K, Metzger DW. Inhibition of pulmonary antibacterial defenseby interferon-gamma during recovery from influenza infection.Nat Med2008; 14:55864.
92 Garvy BA, Harmsen AG. The importance of neutrophils inresistance to pneumococcal pneumonia in adult and neonatal mice.Inflammation1996; 20:499512.
93 Marks M, Burns T, Abadi M, et al. Influence of neutropenia on thecourse of serotype 8 pneumococcal pneumonia in mice.Infect Immun2007; 75:58697.
94 Kadioglu A, Gingles NA, Grattan K, et al. Host cellular immuneresponse to pneumococcal lung infection in mice.Infect Immun2000; 68:492501.
95 Kadioglu A, Coward W, Colston MJ, Hewitt CR Andrew PW.CD4-T-lymphocyte interactions with pneumolysin and pneumococcisuggest a crucial protective role in the host response topneumococcal infection. Infect Immun2004; 72:268997.
96 Nakasone C, Yamamoto N, Nakamatsu M, et al. Accumulation ofgamma/delta T cells in the lungs and their roles inneutrophil-mediated host defense against pneumococcal infection.
Microbes Infect2007; 9:25158.97 Kirby AC, Newton DJ, Carding SR, Kaye PM. Pulmonary dendritic
cells and alveolar macrophages are regulated by gamma delta Tcells during the resolution of S pneumoniae-induced inflammation.
J Pathol2007; 212:2937.
98 van der Sluijs KF, van Elden LJ, Nijhuis M, et al. IL-10 is animportant mediator of the enhanced susceptibility to pneumococcalpneumonia after influenza infection.J Immunol 2004; 172:760309.
99 Kawakami K, Yamamoto N, Kinjo Y, et al. Critical role of Valpha14+natural killer T cells in the innate phase of host protection againstStreptococcus pneumoniaeinfection. Eur J Immunol 2003;33:332230.
100 Brown JS, Hussell T, Gilliland SM, et al. The classical pathway isthe dominant complement pathway required for innate immunityto Streptococcus pneumoniaeinfection in mice.Proc Natl Acad Sci USA2002; 99:1696974.
-
8/13/2019 pathogenesis, treatment, and prevention of pneumococcal pneumonia
14/14
Seminar
101 Kang YS, Do Y, Lee KH, et al. A dominant complement fixationpathway for pneumococcal polysaccharides initiated by SIGN-R1interacting with C1q. Cell2006; 125:4758.
102 Yuste J, Botto M, Bottoms SE, Brown JS. Serum amyloid P aidscomplement-mediated immunity to Streptococcus pneumoniae.PLoS Pathog2007; 3: 120819.
103 van der Poll T, Keogh CV, Buurman WA, Lowry SF. Passiveimmunization against tumor necrosis factor-alpha impairs hostdefense during pneumococcal pneumonia in mice.Am J Respir Crit Care Med1997; 155:60308.
104 Kerr AR, Irvine JJ, Search JJ, et al. Role of inflammatory mediatorsin resistance and susceptibility to pneumococcal infection.Infect Immun2002; 70:154757.
105 Opal SM, Cross AS, Jhung J, et al. Potential hazards of combinationimmunotherapy in the treatment of experimental sepsis.
J Infect Dis1996; 173:141521.
106 van der Poll T, Keogh CV, Guirao X, et al. Interleukin-6gene-deficient mice show impaired defense against pneumococcalpneumonia.J Infect Dis1997; 176:43944.
107 Rijneveld AW, Lauw FN, Schultz MJ, et al. The role ofinterferon-gamma in murine pneumococcal
pneumonia.J Infect Dis2002; 185:9197.108 Rubins JB, Pomeroy C. Role of gamma interferon in thepathogenesis of bacteremic pneumococcal pneumonia.Infect Immun1997; 65: 297577.
109 Yamamoto N, Kawakami K, Kinjo Y, et al. Essential role for the p40subunit of interleukin-12 in neutrophil-mediated early hostdefense against pulmonary infection with Streptococcus
pneumoniae: involvement of interferon-gamma.Microbes Infect2004; 6:124149.
110 Amory-Rivier CF, Mohler J, Bedos JP, et al. Nuclear factor-kappaBactivation in mouse lung lavage cells in response to Streptococcus
pneumoniaepulmonary infection. Crit Care Med2000;28:324956.
111 Sha WC, Liou HC, Tuomanen EI, Baltimore D. Targeted disruptionof the p50 subunit of NF-kappa B leads to multifocal defects inimmune responses. Cell1995; 80:32130.
112 Chapman SJ, Khor, CC, Vannberg FO, et al. IkappaB geneticpolymorphisms and invasive pneumococcal disease.Am J Respir Crit Care Med2007; 176: 18187.
113 Levi M, Opal SM. Coagulation abnormalities in critically ill patients.Crit Care2006; 10:22228.
114 Opal SM. The host response to endotoxin, anti-LPS strategies andthe management of severe sepsis. Int J Med Microbiol 2007;297:36577.
115 Rijneveld AW, Weijer S, Bresser P, et al. Local activation of thetissue factor-factor VIIa pathway in patients with pneumonia andthe effect of inhibition of this pathway in murine pneumococcalpneumonia. Crit Care Med2006; 34: 172530.
116 Laterre PF, Garber G, Levy H, et al. Severe community-acquiredpneumonia as a cause of severe sepsis: data from PROWESS study.Crit Care Med2005; 33:95261.
117 Choi G, Hofstra JJ, Roelofs JJ, et al. Antithrombin inhibitsbronchoalveolar activation of coagulation and limits lung injuryduring Streptococcus pneumoniae pneumonia in rats.Crit Care Med2008; 36: 20410.
118 Mandel LA, Wunderink RG, Anzueto A, et al. The InfectiousDisease Society of America/American Thoracic Society consensusguidelines on the management of community-acquired pneumoniain adults. Clin Infect Dis2007; 44 (suppl):2772.
119 Bruns AHW, Oosterheert JJ, Prokop M, et al. Patterns ofresolution of chest radiograph abnormalities in adults hospitalizedwith severe community-acquired pneumonia. Clin Infect Dis2007;45:98391.
120 British Thoracic Society. BTS guidelines for the management ofcommunity-acquired pneumonia in adults. Thorax2001;56(suppl 4):164.
121 European Respiratory Society task force in collaboration withESCMID. Guidelines for the management of adult lower respiratorytract infections. Eur Respir J2005; 26:113880.
122 Opal SM. Splenectomy and splenic dysfunction. In: Infectiousdiseases. 2nd edn. J Cohen J, Powderly W, eds. Edinburgh: Mosby,Times-Mirror International Publishers, 2004: 114550.
123 Boulware DR, Daley CL, Merrifield C, Hopewell PC, Janoff EN.Rapid diagnosis of pneumococcal pneumonia among HIV-infectedadults with urine antigen detection.J Infect Dis2007; 55:30009.
124 Yang S, Lin S, Khalil A, et al. Quantitative PCR assay using sputumsamples for rapid diagnosis of pneumococcal pneumonia in adultemergency department patients.J Clin Microbiol2005; 43:322126.
125 Abdeldaim GMK, Strlin K, Olcn P, et al. Toward a quantitativeDNA-based definition of pneumococcal pneumonia: a comparisonof Streptococcus pneumoniaetarget genes, with special reference tothe Spn9802 fragment. Diag Microbiol Infect Dis2008; 60:14350.
126 Yu VL, Chiou CC, Feldman C, et al. An international prospectivestudy of pneumococcal bacteremia: correlation with in vitroresistance, antibiotics administered, and clinical outcome.Clin Infect Dis2003; 37:23037.
127 Pallares R, Capdevila O, Linares J, et al. The effect of cephalosporin
resistance on mortality in adult patients with nonmeningealsystemic pneumococcal infections. Am J Med2002; 113:12026.
128 Lonks JR, Garau J, Gomez L, et al. Failure of macrolide antibiotictreatment in patients with bacteremia due to erythromycin-resistantStreptococcus pneumoniae. Clin Infect Dis2002; 35: 55664.
129 Davidson R, Cavalcanti R, Brunton JL, et al. Resistance tolevofloxacin and failure of treatment of pneumococcal pneumonia.N Engl J Med2002; 346:74750.
130 Baddour LM, Yu VL, Klugman KP, et al. Combination antibiotictherapy lowers mortality among severely ill patients withpneumococcal bacteremia. Am J Respir Crit Care Med2004;170:44044.
131 Waterer GW, Somes GW, Wunderink RG. Monotherapy may besuboptimal for severe bacteremic pneumococcal pneumonia.Arch Intern Med2001; 161: 183742.
132 Martinez JA, Horcajada JP, Almela M, et al. Addition of a macrolideto a -lactam-based empirical antibiotic regimen is associated withlower in-hospital mortality for patients with bacteremicpneumococcal pneumonia. Clin Infect Dis2003; 36:38995.
133 Karlstrom A, Boyd KL, English BK, McCullers A. Treatment withprotein synthesis inhibitors improves outcomes of secondarybacterial pneumonia after influenza.J Infect Dis 2009; 199: 31119.
134 Flannery B, Heffeman RT, Harrison LH, et al. Changes in invasivepneumococcal disease among HIV-infected adults living in the eraof childhood pneumococcal immunization. Ann Intern Med2006;144:19.
135 Musher DM. Pneumococcal vaccinedirect and indirect (herd)effects. N Engl J Med 2006; 354:152228.
136 Albrich WC, Baughman W, Schmotzer, Farley MM. Changingcharacteristics of invasive pneumococcal disease in metropolitanAtlanta, Georgia after introduction of a 7-valent conjugate vaccine.Clin Infect Dis2007; 44: 156976.
137 Nahm MH, Lin J, Finkelstein JA, Pelton SI. Increase in theprevalence of the newly discovered pneumococcal serotype 6C inthe nasopharynx after introduction of pneumococcal conjugatevaccine.J Infect Dis 2009; 199:32025.
138 Ongkasuwan J, Valdez TA, Hulten KG, et al. Pneumococcalmastoiditis in children and the emergence of multidrug-resistantserotype 19A isolates. Pediatrics2008; 122:3439.
139 Mufson MA, Stanek RJ. Bacteremic pneumococcal pneumonia inone American City: a 20-year longitudinal study, 19781997.Am J Med1999; 107 (suppl):3443.
140 Brueggemann AB, Pai R, Crook DW, Beall B. Vaccine escaperecombinants emerge after pneumococcal vaccination in the UnitedStates. PloS Pathog 2007; 3: e168.


















