
PARTNERS - IIX Foundation...Low-income and rural women, in particular, are disproportionately...
60
Transcript of PARTNERS - IIX Foundation...Low-income and rural women, in particular, are disproportionately...


Copyright@ImpactInvestmentExchange(IIX)AsiaPte.Ltd.
2
Copyright@ImpactInvestmentExchange(IIX)AsiaPte.Ltd.
Allrightsreserved
Thispublicationmaybereproducedinwholeor inpartforeducationalornon-profitpurposeswithoutspecial permission from the copyright holder, provided that the source is acknowledged. ImpactInvestment Exchange (IIX) would appreciate receiving a copy of any publication that uses thispublicationasasource.
No use may be made of this publication for resale or any other commercial purposes whatsoeverwithoutpriorpermission,withastatementofpurposeandextentofreproduction,shouldbeaddressedtoDurreenShahnaz,founderandCEOofIIX.

Copyright@ImpactInvestmentExchange(IIX)AsiaPte.Ltd.
3
PARTNERS
ThisreportwasdevelopedbyImpactInvestmentExchange(IIX)AsiaPte.Ltd.andfundedbyMedtronicFoundation.
IMPACTINVESTMENTEXCHANGE(IIX)
IIXisaglobalorganizationdedicatedtobuildingamoreinclusiveworldasthefoundationforsustainablepeace.Wedothisbychangingfinancialsystemsandinnovatingsolutionsforwomenempowerment,climateaction,andcommunityresilience.Overthepastdecade,wehavebuilttheworld’slargestcrowdfundingplatformforimpactinvesting(ImpactPartners),createdinnovative
financialproductssuchastheWomen'sLivelihoodBond,operatedaward-winningenterprisetechnicalassistanceprogramssuchasIIXACTS,andestablishedanImpactInstitutefortrainingandeducation.Todate,ourworkhasspanned40countries,unlockednearly$75millionofprivatesectorcapital,avoidedover850,000tonnesofcarbonandimpactedover23millionlives.IIXhasreceivednumerousawardsfor
itsworkincludingtheOsloBusinessforPeaceAward,the‘NobelPrizeforBusiness.’
TheMedtronicFoundationisfocusedonexpandingaccesstoqualitychronicdiseasecareamongunderservedpopulationsworldwide,aswellassupportinghealthinitiativesincommunitieswhere
Medtronicemployeesliveandgive.MedtronicFoundation’sphilanthropicworkistheembodimentoftheMedtronicMissiontoalleviatepain,restorehealthandextendlife.MedtronicFoundationis
committedtoaddressinghealthissuesfortheunderservedandrecognizethattodosoiscomplexandrequirespartnership.MedtronicFoundation’sworkisgroundedintheadvancementoftheGlobal
SustainableDevelopmentGoals(SDGs).MedtronicFoundationbelievesthatbytheworldcommunity–bothpublicandprivatesectors–pullingtogetherwecanmultiplyourcollectiveactionsandstrengths
towardsharedpursuitofglobalgood.MedtronicInc.isthesolefunderofMedtronicFoundation.
Copyright@ImpactInvestmentExchange(IIX)AsiaPte.Ltd.
4
TableofContentsLISTOFACRONYMS..............................................................................................................................5LISTOFTABLESANDFIGURES..............................................................................................................6EXECUTIVESUMMARY..........................................................................................................................7ACKNOWLEDGEMENTS........................................................................................................................9IIX’SWOMEN’SHEALTHPRINCIPLES..................................................................................................13METHODOLOGYTONARROWDOWNFOCUSAREASFORTHEWHB................................................16CRITERIA1:TARGETISSUEAREAS.......................................................................................................17CRITERIA2:TARGETSEGMENTOFTHEHEALTHCONTINUUM..........................................................26CRITERIA3:TARGETSTATES...............................................................................................................30BLUEPRINTOFTHEWOMEN’SHEALTHBOND..................................................................................38ILLUSTRATIVECASES..........................................................................................................................45WOMEN’SHEALTHIMPACTASSESSMENTTOOLKIT.........................................................................50CALLTOACTION.................................................................................................................................56REFERENCES.......................................................................................................................................57

Copyright@ImpactInvestmentExchange(IIX)AsiaPte.Ltd.
5
LISTOFACRONYMS
• AHRQ:AgencyforHealthcareResearchandQuality(AHRQ)
• ACA:AffordableCareAct
• ACS:AmericanCancerSociety
• CA:California
• CDC:CentreforDiseaseControlandPrevention(CDC)
• CMS:CentreforMedicareandMedicaid(CMS)
• FPL:FederalPovertyLevel
• GIIN:GlobalImpactInvestmentNetworks
• HEDIS:HealthcareEffectivenessDataandInformationSet
• HPV:HumanPapillomavirus
• MN:Minnesota
• NCQA:NationalCommitteeforQualityAssurance
• NY:NewYork
• NYP:NewYork-Presbyterian
• ICHOM:InternationalConsortiumofHealthOutcomesMeasurement
• IOM:InstituteofMedicine
• IRIS:ImpactReportingandInvestmentStandards
• IIX:ImpactInvestmentExchange
• UN:UnitedNations
• SDG:SustainableDevelopmentGoal(s)
• SDH:SocialDeterminantsofHealth
• US/USA:UnitedStatesofAmerica
• USAID:UnitedStatesAgencyforInternationalDevelopment
• WHB:Women’sHealthBond
• WHO:WorldHealthOrganization
• WOC:WomenofColor
Copyright@ImpactInvestmentExchange(IIX)AsiaPte.Ltd.
6
LISTOFTABLESANDFIGURESTABLESTABLE1:LISTOFINTERVIEWEES……………….……………………….……………………….………….…………….10TABLE 2: KEY CHALLENGES AND UNDERFUNDED AREAS FACED BY UNDERSERVEDWOMEN INTERMSOFCANCERPREVENTION,EARLYDETECTIONANDTREATMENT……………….…………………18TABLE3:COMPARINGBREASTANDCERVICALCANCERFUNDINGBASEDONACSGRANTS……….20TABLE4:CERVICALCANCERINCIDENCEANDMORTALITYRATEACROSSETHNICGROUPS…….….20TABLE 5: KEY CHALLENGES AND UNDERFUNDED AREAS FACED BY UNDERSERVEDWOMEN INTERMSOFAFFORDABILITYANDQUALITYOFMATERNALHEALTH……………………………….……….…21TABLE6:POSITIVESCREENINGCRITERIAFORTARGETSTATES….…………….………………….…………..33TABLE7:ABSOLUTENEED–SUMMARYOFKEYSTATISTICS….…………….………………………………..…34TABLE8:ACUITYNEED–SUMMARYOFKEYSTATISTICS….……………………………………………………..35TABLE9:COMPARITIVEANALYSISOFPOTENTIALBONDSTRUCTURES…….…………….……………….44FIGURESFIGURE1:PATIENT-CENTEREDECOSYSTEMMAPPINGFOCUSEDONWOMEN…………………………..10FIGURE2:FACTORSINCLUDEDINDETERMININGPATIENT-CENTEREDCARE…………………………….14FIGURE3:METHODOLOGYOVERVIEWANDALIGNMENTWITHWOMEN’SHEALTHPRINCIPLES….16FIGURE4:WHBFOCUSONWOMEN-SPECIFICCANCERS…….…………….……………………………………..17FIGURE5:FIVEYEARESTIMATESOFBREASTCANCERMORTALITYRATES…………………………….….19FIGURE6:WHBFOCUSONMATERNALHEALTHANDREPRODUCTIVERIGHTS………………………….21FIGURE7:PREVENTABILTYOFMATERNALMORTALITYBASEDONTIMEOFDEATHINRELATIONTOPREGNANCY……..……….………………………….…………….………………………….…………….……………….23FIGURE8:LEADINGUNDERLYINGCAUSEOFPREGNANCY-RELATEDDEATHS,BYRACE/ETHINICITY..….…………….………………………….…………….………………………….…………….………….24FIGURE9:DISPARITIESINCONTRACEPTIONUSEANDABORTIONACCESS……………………………….25FIGURE10:QUANTIFYINGCONTRACEPTIVEUSEBASEDONRACEANDETHNICITY……………………25FIGURE11:LEVELSOFHEALTHCARESYSTEMANDCONTINUUMOFCARE……………………………….26FIGURE12:RIPPLEEFFECTOFREACTIVEHEALTHCARE…….…………….………………………………………27FIGURE13:DISTRIBUTIONOFPREVENTABILITYAMONGPREGNANCYRELATEDDEATHS…………..28FIGURE14:WHBAPPROACHTOEMBRACEPROACTIVECAREACROSSTHECONTINUUM…………..29FIGURE15:EXPLORINGTHEINTERESTININVESTINGINWOMEN’SHEALTH–THEINTERSECTIONOFTHEINNOVATIVEFINANCEANDGENDER-LENSMOVEMENTS…….…………….………………………..31FIGURE16:TAPPINGINTOTHEIMPACTINVESTINGMOVEMENTTOFINANCEHEALTHCARE……..32FIGURE17:ESTIMATEDUNDOCUMENTEDPOPULATION(2014)….….…………….………………………….36FIGURE18:ESTIMATEDNUMBEROFWOMENWHOAREUNINSURED(2014)…….…………….…………36FIGURE19:MAPPINGUNINTENDEDPREGNANCYRATEPER1000WOMEN,15–44…………………….37FIGURE20:DESIGNINGTHEBLUEPRINTOFTHEBOND……………………………………………………………39FIGURE21:OUTLINEOFSUSTAINABILITYBONDMECHANISM…………………………………………………40Figure22:OUTLINEOFSOCIALIMPACTBONDS………………………………………………………………………41Figure23:OUTLINEOFTHEHUMANITYBOND………………………………………………………………………..42FIGURE24:OUTLINEOFGAVIBONDMECHANISM…………………………………………………………………..43FIGURE25:5-YEARROADMAPFORWOMEN’SHEALTHBONDSERIES……………………………………….45FIGURE26:ILLUSTRATIVEEXAMPLEOFTHEWOMEN’SHEALTHBONDFORACS………………..…….47FIGURE27:ILLUSTRATIVEEXAMPLEOFTHEWOMEN’SHEALTHBONDFORTHEMOTHER’SCENTER………………………………………………………………………………………………………………………………49Figure28:IIXSUSTAINABILITYPYRAMIDTM…………………………………….……………………………………….51FIGURE29:KEYCHALLENGESINMEASURINGIMPACTTHROUGHTHELENSOFIMPROVINGHEALTHCAREFORUNDERSERVEDWOMEN….………………………………….……………………………………53FIGURE30:FIVESTAGEPROCESSOFMEASURINGIMPACT….…………………………………………………..53

Copyright@ImpactInvestmentExchange(IIX)AsiaPte.Ltd.
7
EXECUTIVESUMMARY
Women’sHealthMatters
IIXandIIXFoundationUSAbelievenowomenshouldbedeniedhealth access because of financial or social barriers. IIX hasspent thepastdecadeusing its expertise in innovative financeto empowermillions of underservedwomen across theworld.IIXandIIXFoundationUSAarenowbuildingonthismovementto bring underserved women in the United States to theforefront of financial markets through the Women’s HealthBond (WHB). TheWHB embraces IIX’smission to connect thebackstreetsofunderservedcommunitiestotheWallStreetsoftheworldbyensuringwomenhavebetteraccesstohealthcarethatisaffordable,inclusiveandpatient-centric.
This feasibility study report developed by Impact InvestmentExchange (IIX) is the first phase of designing an innovativefinancialmechanism,theWHB,basedonasystematicreviewofkey barriers to patient-centered health care, health needs ofwomen in the United States and investment drivers that canhelp scale up potential solutions. The report will lay thefoundation for the second phase of the work, which entailsdeveloping a series ofBonds that are equipped to unlock newsourcesofinvestmentcapitaltodriveforwardpatient-centeredoutcomes for underserved women in the United States. TheWHBseries isexpected tounlock$100millionovera five-yeartimeframewithagoaltoimpact2millionwomen.
Low-income and rural women, in particular, aredisproportionatelyimpactedbythelackofaccesstoaffordablehealthcare.Womentendtohavemorecontactwithhealthcaresystems, greater needs during childbearing years, and asprimarycaregiversmoreinterfacewithhealthcareprovidersonbehalfofothers.Thismakesitimperativetoensureallwomen,regardlessof their socio-economicbackground,haveaccess toquality health care. For the purposes of the feasibility study,underservedwomenincludeoneormoreofthefollowing:
• Womenlivingbelow200%oftheFederalPovertyLevel• Womenlivinginruralcommunities• Womenofcolor(WOC),ethnicminorities• Other women that are traditionally excluded from the
health care system (undocumented, uninsured, non-Englishspeaking,etc.)

Copyright@ImpactInvestmentExchange(IIX)AsiaPte.Ltd.
8
NavigatingtheReport:KeyFindingsandSectionOverviews
Keyfindingsfromthereporthavebeensummarizedbelow:
• IIX Principles for AdvancingWomen’s Health:Aspartof the feasibility study, the IIX teamhasconducted+40stakeholderinterviewsandanextensivefieldvisittolearnaboutkeychallengesonthe ground based on insights from industry experts, frontline health workers and patientsthemselves.ThisprocesshasledIIXtodevelopthreeguidingprinciplestoensuretheeffectivenessof theWomen’s Health Bond in creating a demonstrable positive impact on women’s health: (i)patient-centered–embracingsixcoredimensionsofhealth:access,affordability,equity,efficiency,qualityand responsiveness; (ii) proactive– redefining thenarrative from reactivehealth care thatsolelyfocusesontreatmenttoproactivehealthcarethatalsofocusesonprevention;and(iii)usingpositiveincentivestolinkimpacttocapitalmobilized.
• DefinedtheneedforaninnovativefinancialstructuresuchastheWHBandnarroweddownthefocus areas: TheWHBwill focus on women-specific cancers such as breast and cervical cancer,maternal health (prioritizing initiatives that also target mothers at risk of heart disease anddiabetes)andreproductiverights.TheWHBwillprioritizeinitiativesfocusedondeliveringproactivehealthcareviapreventionandearlydetectionorbyreducingdelaystotreatmentwiththeobjectiveto savemore lives today and reduce future outlays of costs to patients and providers. The threestates that IIXwill focuson for the initial tranchesof theBond includeCalifornia (CA),Minnesota(MN)andNewYork(NY).Thedecision-makingprocesstonarrowdownthefocusareasfortheWHBinitiativeisfurtheroutlinedinthe‘Methodology’sectionofthereport.
• AssessedthestructuresofthreedifferentinnovativefinancialmechanismsinthecontextoftheWHB: The IIX team has reviewed three potential structures for theWomen’s Health Bond, andbasedonfindingstodate,hasdeterminedthataHumanityBondstructurewillbethemostsuitable.Thestructureiswellsuitedtouseablendedfinanceapproachbyusingexistingconcessionalcapitalfrom the philanthropic or public sectors to unlock upfront funding from private sector investors.Upfrontfundingcanbeusedbynon-profitstomagnifyhealthcareoutcomesatagreaterpaceandscale by funding proactive and time-sensitive initiatives while also reducing long-term costsassociated with reactive health care. An overview of the Bond structures considered and anillustrativecaseoftheproposedmechanismisfurtheroutlinedinthereport.
• NeedformeasurementandtheIAtoolkit:Thefieldvisitswerealsousedtoassesscurrentgapsinthemeasurementofhealthcareoutcomes,whichrevealedaseverelackofpatients’voicesinwhatgetsmeasuredandadisproportionatefocusonvolumeofcare(oroutputs)insteadofvalueofcare(oroutcomes).Toaddressthis,IIXhasalsodevelopedaWomen’sHealthImpactAssessmentToolkitdesignedtocomplementtheBond.TheWomen’sHealthImpactAssessmentToolkithasbeenbuiltbasedonIIX’s+9yeartrackrecordofconducting+130impactassessmentsacrosstheworldusingitsproprietary framework – the IIX Sustainability PyramidTM. The Toolkit is outlined in brief in thereportandfurtherdetailedinaseparateguidelinedocumentandspreadsheetthatwillbepublishedalongwiththisreport.

Copyright@ImpactInvestmentExchange(IIX)AsiaPte.Ltd.
9
ACKNOWLEDGEMENTS
IIXandMedtronicFoundation
This publication was prepared under the overall direction and guidance of Prof. Durreen Shahnaz,FounderandCEOof Impact InvestmentExchange (IIX) and IIXFoundationUSA.Colleagues from theMedtronicandMedtronicFoundationprovidedvalue input, includingOmar Ishrak,CEOofMedtronic,PaurviBhatt,PresidentofMedtronicFoundationandAnneKatherineWales,MedtronicFoundation.
Women’sHealthBondTaskForce
TheWomen’s Health Bond Task Force is comprised of a distinguished group of health care industryleaders, impact investing sector, corporations, philanthropic organizations, policymakers, and otherorganizationswithacommongoaltocreatehealthcareequalityforwomenintheUnitedStates.Themissionofthisuniquegroupofhigh-levelexpertswithon-the-groundexperienceandperspectivesistoinformandstrengthentheWomen’sHealthBondInitiativeledbyImpactInvestmentExchange(IIX)andsupportedbytheMedtronicFoundation.MembersoftheWomen’sHealthBondTaskForceinclude:
HealthcareExperts
Ms.ElanaAbraham-CorporateTreasurer,TheMountSinaiHealthSystemMr.OmarIshrak–CEO,MedtronicMs.KrisKim-ExecutiveVicePresident,NortheastRegion,AmericanCancerSocietyMs. Mary Manning - Division Director Health Promotion/Chronic Disease, Minnesota Department ofHealthDr.RuthSaber-Founder,TaraHealthFoundationMs.AstaSorensen-SocialScientist,RTIInternationalMs.JeanLimTerra-StrategicAdvisor,CorporateAffairs,GileadSciencesMs.PamelaZeller–President,ZellerSolutionsFinance/ImpactInvestingExperts
Mr.AntonyBugg-Levine-CEO,Non-ProfitFinanceFundMs.CynthiaCalderon-ManagingDirector,SmallWorldGroupIncubatorMr.PaulTregidgo-AdvisoryCouncil,CentreforFinancialInclusionAcademia
Prof.PaulBrest,DirectoroftheLawandPolicyLab,StanfordUniversityProf.CatherineClark-FacultyDirector,CenterfortheAdvancementofSocialEntrepreneurship(CASE),DukeUniversity’sFuquaSchoolofBusinessProf.KatherineKlein-ViceDean,WhartonSocialImpactInitiative,UniversityofPennsylvaniaStrategicPartnerships
Mr.GeorgeGreen-Founder,PluribusCapitalManagementMr.EdwardHartman-Co-Founder,LegalZoomMs.KalpanaRaina-ManagingPartner,252Solutions,LLCMr.AlanSeem-CorporateLawPartner, JonesDay;MemberofBoardofTrusteeofCaliforniaPacificMedicalCenterFoundation

Copyright@ImpactInvestmentExchange(IIX)AsiaPte.Ltd.
10
Ms.SharmilaMonaSinha-Trustee,SmithCollegeMr.JoesphYurcik-COO&CFO,TheaterMania.com
Interviewees
As part of the feasibility study, IIX interviewed + 40 health care experts and industry leaders ininnovativefinance,maternalhealth,reproductivehealthandwomen-specificcancers.Figure1outlinestheecosystemmappingcreatedby IIX, takingapatient-centeredapproachthatplacedwomenatthecenterofthehealthcareequation.Table1providesalistofintervieweeswhocontributedvaluableinputtothefeasibilitystudy:
FIGURE1:PATIENT-CENTEREDECOSYSTEMMAPPINGFOCUSEDONWOMEN
TABLE1:LISTOFINTERVIEWEES
Individual(s) Organization
JanetteFlint,ExecutiveDirectorNourbeseFlint,PolicyDirector
BlackWomenforWellness
LaceyClarke,DirectorofPolicyCommunityHealthCareAssociationofNewYorkState
JulieHammerman,BoardInvestmentCommitteeJulieRabinovitz,PresidentandCEO
EssentialHealthAccess
SarahVerbiest,DirectorTheNationalPreconceptionHealthandHealthCareInitiative
DianaRamos,MedicalDirectorforReproductiveHealthRitaSinghal,MedicalDirector(former)
LosAngelesCountyDepartmentofPublicHealth
JanMalcolm,CommissionerMaryManning,DivisionDirectorJoanBrandt,DivisionDirectorSusanCastellano,MaternalandChildHealthDirector
MinnesotaDepartmentofHealth
Women
Individual Non-profit For-profit For-Profit/NonProfit Government
MedicalSpecialists
Navigators
HomeCareProviders
PrimaryCareProviders
RuralClinics
Hospitals
CriticalAccessHospitals
ResearchInstitutions
PharmaceuticalCompanies
Foundations
Advocates
Medical&ProfessionalAssociations
CommunityBasedOrganizations
InsuranceAgenciesAuditors
Note: Many organizations, particularly enablers, playmultipleroleswithinthehealthcareecosystem.
MedicalDeviceProviders
Women-CentricApproachtoEcosystemMappingForthepurposeoftheWHB,womenarepositionedatthecenteroftheecosystemmapping.Inparticular,theWHBfocusesonunderservedwomen.ThisapproachisinlinewithIIX’smissiontotakeapatient-centered,gender-lensapproachtodevelopingtheWHB.
FrontlineHealthWorkersIndividualsdirectlyinteractingwithpatientstoprovideortofacilitatehealthcare.
EnablersOrganizationthatequipthehealthcaresystemtooperatebyprovidingfinancing,accesstoinformation,skillsdevelopmentservices,medicalsuppliesandequipment,etc.
HealthCareProvidersOrganizationsandinstitutionsthatprovidehealthcare.Thesecanrangefromlarge,usuallyurban,hospitalstosmallruralclinics.
RegulatorsActorsinchargeofestablishingtheguidelinesforhowandwhenhealthcareisprovided,andthosewhomonitorcompliancewiththoseguidelines.Thisgroupincludeslocal,stateandfederallevelpolicymakersaswell.
DESCRIPTION
Legislatures(Local/State/National)
FederallyQualified
HealthClinics
FinancialInstitutions
Agencies&Departments
(Local/State/National)
HealthcareSystems

Copyright@ImpactInvestmentExchange(IIX)AsiaPte.Ltd.
11
JanetOlstad,AssistantDirector
AvivaGoldstein,DirectorofDevelopmentDeborahKaplan,AssistantCommissioner
NewYorkCityDepartmentofHealth
MarilynKacica,MedicalDirectorKristineMesler,AssociateBureauDirectorWendyShaw,AssociateDirectorLaurenTobias,Director
NewYorkStateDepartmentofHealth,DivisionofFamilyHealth,ChildandAdolescentHealth
KarenPaolinelli,President CaliforniaAssociationofRuralHealthClinics
RickPotter,ExecutiveVicePresidentandCOO HealthServicesAdvisoryGroup
ClareBradley,SeniorVicePresidentandCMOTheodoreWill,CEO
IPRO
LeslieMcGowan,CEO LivingstonCommunityHealthCenter
SusanBradley,PresidentandCEOJuliaHejl,DirectorofDevelopmentAndreaLeti,ChiefDevelopmentOfficerLindaPahl,CFOJorgeTapia,DevelopmentAssociateBessWalkes,VicePresidentofDevelopment
PlannedParenthoodLACounty
GloriaMartinez,ChiefofStaff PlannedParenthoodNorthernCalifornia
EricStockton,HealthProgramManager,CommunityInvestmentMollyTheobald,Director,CommunityInvestment
AppalachianRegionalCommission
RachelWick,SeniorProgramOfficer BlueShieldofCaliforniaFoundation
CarlinaHansen,SeniorProgramOfficer CaliforniaHealthCareFoundation
TammyJohnson,SeniorDonorRelationsOfficerRosemaryVeniegas,SeniorProgramOfficer,Health
CaliforniaCommunityFoundation
SarojSedalia,Advisor–RabinMartin MerckforMothers
SommerBazuro,BoardMemberSusanJacobson,ManagerofBusinessandCommunityDevelopmentLindaTantawi,CEOKomenFoundation,GreaterNYC
SusanKomenFoundation
DeannaLarson,CEO AveraeCare
MichaelChinnavaso,CampaignDirector,CancerCenterKarenJeu,PresidentCeciliaThomas,Manager,CommunityHealthPrograms
CaliforniaPacificMedicalCenterFoundationandSutterHealth
ElanaAbraham,DirectorofSpecialProjects,Finance Mt.Sinai
AndresNieto,Director,CommunityHealthOutreach&MarketingVictoriaSchlegel,DirectorofCorporateandFoundationRelationsKarenSchmitt,ExecutiveDirector
NewYorkPresbyterian

Copyright@ImpactInvestmentExchange(IIX)AsiaPte.Ltd.
12
KariVredenburg,BusinessDevelopment
BrittanyPampuch,MedtronicLabs Medtronic
DavidHiggins,HeadofImpactInvesting JohnsonandJohnson
BarbaraLevy,VicePresidentforHealthPolicyAmericanCollegeofObstetricsandGynecologists
DianaRamos,ACOGFellowAmericanCollegeofObstetricsandGynecologists,California
AlisonTeitelbaum,ExecutiveDirector AmericanHealthQualityAssociation
KarenPaolinelli,President CaliforniaAssociationofRuralHealthClinics
LouiseMcCarthy,PresidentandCEO CommunityClinicAssociationofLACounty
KrisKim,ExecutiveVicePresident AmericanCancerSociety
ShobhaKrishnan,PresidentandFounderGlobalInitiativeAgainstHPVandCervicalCancer
PatriciaHeinrich,ExecutiveDirectorEmmaSmizik,AssociateProjectDirector
NationalInstituteforChildren'sHealthQuality
ChristineMorton,ProgramManager CaliforniaMaternalQualityCareCollaborative
HopeYates,DirectorofStrategyandCommunications ColombiaUniversity'sDepartmentofOB/GYN
AlinaSalganicoff,VicePresidentandDirectorofWomen’sHealthPolicy
KaiserFoundation
PeterSchafer,DirectorNewYorkAcademyofMedicine,CenterforHealthPolicyandPrograms
JenniferGriffin,ResearchEpidemiologist RTIInternational,CenterforGlobalHealth
MichaelTrisolini,SeniorDirectorRTIInternational,HealthCareQualityandOutcomesProgram
SamanthaSommerness,ClinicalAssistantProfessor UniversityofMinnesota,SchoolofNursing


Copyright@ImpactInvestmentExchange(IIX)AsiaPte.Ltd.
14
IIX’SWOMEN’SHEALTHPRINCIPLES
ThepurposeofthissectionistodefinethethreeprinciplesthatguidedthedevelopmentofthisreportandtheImpactAssessmenttoolkit:(i)PatientCentered;(ii)Proactive;and(iii)PositiveIncentives.
Principle1:Patient-CenteredCare
DefiningPatient-CenteredCare:Forthepurposesofthisreport,patient-centeredcarewillrefertotheInstitute of Medicine definition: ‘Providing care that is respectful of and responsive to patientpreferences, needs and values, ensuring patient values guide all clinical decisions’i. The objective oftaking a patient-centered approach is to improve trust, experience and outcomes of underservedwomenimpactedandtoenhancethequalityofthehealthsystem.
Why: There is a need to have patients at the center of the health care solution design process.Particularly,thevoicesofunderservedwomenaretypicallynotreflectedinhowhealthcareisdeliveredorhow‘success’or‘progress’getsmeasured.Assuch,themajorityofhealthsolutionsorinterventionstendtofocusonaccessibility,mortalityorcoveragewithlimitedconsiderationofdeeperelementssuchas health equity, patient satisfaction, ability to pay and other factorswherein social determinants ofhealtharetakenintoconsideration.
What:IIXhasusedtheframeworkoutlinedinFigure2toadoptpatient-centeredapproachbothinthedesign of theWHB and in the development of theWomen’sHealth ImpactAssessment Toolkit. Thefollowingsectionoutlineseachofthesixcorefacetsofpatient-centeredcare:
FIGURE2:FACTORSINCLUDEDINDETERMININGPATIENT-CENTEREDCARE
• Access:Accessreferstoimprovedproximity(orgeographicavailability);improvedsystemcapacity(havingadequatestaffwithrequiredskills,havingadequateequipment);andimprovedconnectivity(provisionofconsistentservicesandwhomthepatienttrustsi.e.buildsapersonalrelation).
• Affordability: Affordability refers to improved ability to pay for health; improved coverage oralternativemeanstopayforhealthcare;andreducedproblemaggravationduetodelayedhealthcare.
• Efficiency: Efficiency refers to improved cost effectiveness or reduced wastage or resources,increased organizational productivity and increased use of technology or data to drive improvedoutcomesand/orbetterresourceuse.
RESPONSIVENESS EFFICIENCY
EQUITY
ACCESS
QUALITY AFFORDABILITY
PATIENTCENTERED
CARE

Copyright@ImpactInvestmentExchange(IIX)AsiaPte.Ltd.
15
• Equity: Equity refers to increased health equality or reduced discrimination based on race orethnicity; increasedautonomyorappropriatenessofcarebasedonpatient’spersonalandculturalpreferences;andincreasedpatientsatisfaction(feelingofbeingtreatedwithdignityandempathy).
• Quality:Improvedeffectivenessrelatedtoreducedmorbidity,reducedmortality,improvedqualityof life, improved functional status of patient, etc.; improved patient safety (through clinicalappropriateness and adequate adherence to best practice structures/processes); and improvededucation/awarenessofpatientsonhealthcarerisksandrights.
• Responsiveness:Improvedtimeliness/promptnessofcare,shiftfromreactivetoproactivecareandimprovedclinicaloutcomesduetopromptcare;increasedclarity,completenessandconfidentialityofcommunicationinaneasytounderstandandactionablemanner;andimprovedcoordinationofcare(includingbetterpatientnavigation).
Principle2:Proactive
Why:Underservedwomentendtobemorereactivewiththeirhealthcare,typicallyseekingtreatmentonlyaftertheissuehasadvanced.Reflectiveofthis,mosthealthcareinterventionsandmeasurementtoolsfocusmostlyontreatment.
What: IIXrecommendsshiftingtowardsamoreproactiveapproachofdesigningsolutions,measuringimprovementinoutcomesandallocatingcapitaltoscaleinterventionsby:
• Expanding thecapital, time,andother resourcesallocated towardsprevention,earlydetectionorreduceddelaysbetweendiagnosisandtreatment.
• Conducting regular impactmonitoringand reportingusinganadaptivemanagementapproach toholdhealthcareprovidersorenablersmoreaccountabletobothpatientsandfunders.
• Engagingpatients directly to validate thehealthoutcomes theyhave experienced, potentially bydigitalizingtheimpactassessmentdatacollectionandverificationprocess.
Principle3:PositiveIncentives
Why:Thereisaneedtorefocuscapitaldeployedonthevalueofcarecreated,notthevolumeofcaredelivered. Many funding programs use negative incentives to penalize different groups for non-performancesuchasbyreducingfinancialreturnsorcuttingofffuturefundingstreams.
What: IIX recommends using positive incentives to accelerate the pace and scale of high-impactsolutionsthatwillimprovehealthoutcomesforunderservedwomenby:
• Designing an innovative financialmechanism that rewards investors for supportingwomen’shealthandcreates‘additionality’byunlockingnewsourcesofcapitalthatwouldotherwisenothave been allocated for this purpose.Thiscould involve (i)usingablendedfinanceapproachofconcessionary funding fromphilanthropic or public sector actors to leverage in or de-risk privatesectorinvestments;or(ii)offeringprivatesectorinvestorsafinancialreturninadditiontothesocialreturnsgenerated.The‘Blueprint’sectionofthisreportoutlineshowtheWHBcanachievethis.
• Linking impact achieved with capital mobilized. IIX’s impact assessment toolkit marries thecreationoftangibleimpactonunderservedwomenwiththeWHB’sabilitytomobilizeandallocatecapitaleffectively.Bylinkingfundingtooutcomesinsteadofoutputs,IIXusespositiveincentivestoshift the focus from volume of care to value of care. The ‘Women’s Health Impact AssessmentToolkit’sectionofthisreportfurtherdetailshowtheWHBcanadoptthisapproach.

Copyright@ImpactInvestmentExchange(IIX)AsiaPte.Ltd.
16
METHODOLOGYTONARROWDOWNFOCUSAREASFORTHEWHBThepurposeof this section is tooutline thekeycriteriaused tonarrowdown the focusareas for theWHB. Given the complexity of the US health care system, IIX took amulti-dimensional approach tonarrowdownthefocusoftheWHBtospecificissues,segmentsofthehealthcarecontinuumandstates.EachcriterionisalignedwithoneoftheWomen’sHealthPrinciplesdescribedintheprevioussection.
FIGURE3:METHODOLOGYOVERVIEWANDALIGNMENTWITHWOMEN’SHEALTHPRINCIPLES
Criteria1–PotentialtoImpactUnderservedWomenusingaPatient-CenteredApproach:WhileIIXrecognizesthathealthequityisimportantforthecommunityasawhole,thepurposeoftheWomen’sHealth Bond is to mobilize capital to drive improved health outcomes for women in particular.Additionally, IIX focused on issues that required additional funding to shift towards providingunderservedwomenwithmore inclusive, patient-centered care. As such, IIX has narrowed down thefocus areas of the Bond towomen-specific cancers (breast and cervical cancer)maternal health andreproductivehealth.
Criteria 2 – Potential of Intervention to Create Effective Outcomes by Embracing a ProactiveApproach:While all initiatives will be assessed on a case-by-case basis for their potential to impactunderserved women, the WHB will prioritize initiatives that advance proactive health care, supportpreventativemeasures,advanceearlydetectionandreducetimetotreatment.Thekeyfocuswillbetosupportprogramsthatcanmagnifyimpactatthesamecostorachievethesameimpactatalowercostoverthelongrun.
Criteria 3 – Potential for an Innovative Financial Mechanism to Unlock Capital using PositiveIncentives:Aspartofthefeasibilitystudy,IIXidentifiedstatesthathadacombinationoftwofactors(i)demand for capital, i.e. presence of innovative health care providers with solutions that neededadditional capital at an increasedpaceand scale; and (ii) supplyof capital, i.e. ability tobring innewinvestors from the private sector into the health care equation based on key investment drivers. Assuch,IIXhasnarroweddownthetargetstatesoftheBondtoCalifornia,NewYorkandMinnesota.
The following section outlines each of these key criteria sequentially althoughmany sub-factorswere assessed in parallel andplayedan influencing roleon eachother in order todetermine thefinalsetofnarroweddownfocusareasinaholisticmanner.
KeyCriteria
1PotentialtoImpactUnderservedWomenusingaPatientCentered
Approach
1aWomenspecificissues
1bIssuesimpactingunderservedcommunities
2PotentialofInterventiontoCreateEffectiveOutcomesbyEmbracingaProactive
Approach
2aAbilitytosavemorelivestodaybyimprovingqualityandaccess
2bAbilitytolowerfutureoutlaysofcosttoimproveaffordability
3PotentialforanInnovativeFinancialMechanismtoUnlockCapitalusingPositive
Incentives
3aNeedandfeasibilityofmobilizingalternativesourcesofcapital
3bNeedandfeasibilitytoabsorbanddeploymission-drivencapital
TargetIssueArea1.MaternalHealth(prenatal/postpartumcareand
reproductivejustice)2.Women-SpecificCancers(cervicalcancerand
breastcancer)
TargetStates1.California(highnumberoflow-incomewomen)2.NewYork(highnumberoflow-incomewomen)
3.Minnesota(highdisparities)
TargetSegmentofHealthcareContinuum1.Prevention(low-incomewomentendtobemore
reactivewiththeirhealthcare)2.EarlyDetectionandReducedDelaystoTreatment(relativelylargefundinggaps)
NARROWEDDOWNFOCUSAREASOFTHEWOMEN’SHEALTHBOND
KEY CRITERIA ALIGNED WITHWOMEN’SHEALTHPRINCIPLES
SUB-FACTORSCONSIDERED

Copyright@ImpactInvestmentExchange(IIX)AsiaPte.Ltd.
17
CRITERIA1:TARGETISSUEAREAS
OVERVIEWOFWOMEN-SPECIFICCANCERS
IIXfollowedatwo-prongedapproachtoassessingchallengesfacedbyunderservedwomenasitrelatesto access, affordability and quality of women-specific cancers: (i) primary data collected through in-person and remote interviews,meetings and field visits – an important step to understandpriorities,acuityof need, and to identifypotential projects that are addressing the issue andwork towards theinitial shortlist of initiatives; and (ii) secondary data collected through desktop research, reviews ofofficial publications and reports, with key insights validated or verified during the field visits. Assummarizedinthecontextsection,IIXiscurrentlyexploringtwokeyareasundercancerasoutlinedinFigure4:
FIGURE4:WHBFOCUSONWOMEN-SPECIFICCANCERS
WOMEN-SPECIFICCANCER:BREASTCANCERANDCERVICALCANCER
Cancer is the second leading causeofdeathofwomen in theUnitedStates, killingone in every fourwomen.iiResearchindicatesthatbreastcancerhasthehighestincidenceofcancersaffectingwomen.iiiAlthoughrelatively lessprevalent,cervicalcancer isanotherwomen-specificcancerthatwasexploredaspartofthefeasibilitystudy.While93%ofcervicalcancersare‘preventable’,ivthediseaseisnotbeingadequatelypreventedintheUnitedStates,particularlyamonglowincomeandruralcommunitieswhotypically have lower awareness of the broader benefits of the HPV vaccination and / or associateencouragingthevaccinationwithpromotingpromiscuity.
KEYCHALLENGESBASEDONSTAKEHOLDERINTERVIEWS
Basedonstakeholder interviewsconductedwith frontlinehealthexperts in the field,TableXoutlinesunderfundedareasthataddtochallengesfacedbyunderservedwomenthroughthe lensesofaccess,affordability,andqualityforbreastandcervicalcancer.
• Vaccinationforcervicalcancer• Earlydetectionandreduceddelaystotreatmentforbreastandcervicalcancer
Prevention EarlyDetection Treatment Recovery

Copyright@ImpactInvestmentExchange(IIX)AsiaPte.Ltd.
18
TABLE2:KEYCHALLENGESANDUNDERFUNDEDAREASFACEDBYUNDERSERVEDWOMENINTERMSOFCANCERPREVENTION,EARLYDETECTIONANDTREATMENT
Cancers Prevention(CervicalCancer)
EarlyDetection(Breast/CervicalCancer)
Treatment(Breast/CervicalCancer)
Affordability Women18-26whoarenotinsuredarenotcoveredfortheHPVvaccine
Screening for both breastand cervical cancers arecovered by manyinsurance programs butcanstillbeoutofreachforuninsured women. TheCDC has implementedpublicly funding programsfor each state to coveralmostwomen, regardlessof insurance, but use oftheseprogramsbyeligiblepatientsislow,largelyduetoawarenessandaccess.
Co-payscanbeexpensive,and multiple doctors (andmultipleco-pays)areoftenrequired.Most advocates ornavigators,whohelpguidea patient through thepayment and treatmentsystems, are not coveredby insurance.This impactsthe affordability oftreatmentfortheprovider,who often choose to notoffertheseservices.
Cervical cancerprevention,andearlydetectionand treatment forbreastandcervicalcancer,requiremultipleprovidervisits.Thesetransportationcosts,aswellaschildcareneededduringthesevisits,arenotcovered.
Quality Quality barriers forprevention of cervicalcancerarenotsignificant.
Limited availability ofproviders that women arecomfortable with (femaledoctors, nurses of thesame ethnicity) candecrease patient qualityand exacerbate issues oftrust in the system,particularlyamongwomenofcolor.
Lack of coordination ontreatment, and lack ofpatientadvocatescanleadtosuboptimaltreatment.
Healthcare institutionsandproviders,particularlythosein rural communities, can suffer from a lack of trainingamong the care givers or a lack of the appropriatemedicalequipment.
Access Lack of awareness, fromboth theguardianandthepediatrician, that theHPVvaccine is covered byinsuranceforminors.
Conflicting information,among both patients andservice providers, aboutthe recommendedfrequency of screeningscanleadtolapsedvisits.
The system for care andinsurance can be overlyconfusing for patients, forthose with low literacy orwho speak English as asecondlanguage.
Scarcity of service providers and institutions, particularly in rural areas, mean thatwomencanbeprohibitivelyfarfromhealthcareservices

Copyright@ImpactInvestmentExchange(IIX)AsiaPte.Ltd.
19
ADDITIONALINSIGHTSFROMSECONDARYRESEARCH
BREASTCANCER
MainBarriers toEarlyDetection:Thetotalcostofillnessforbreastcancerhasbeenestimatedtobe$3.8 billion, of which $1.8 billion represents medical care costs.vMammography can improve earlydetectionbyasmuchas15-35%andreducethecostoftreatmentsignificantly.viCostcanactasabarrierto53%oflow-incomewomenfromaccessingpreventiveorearlydiagnosticservicesandismoreacuteamonguninsuredgroups.viiIncomehasbeenobservedtobestronglyassociatedwithbreastcancercareandsurvivalintheU.S.IntheUSwomenwithprivatehealthinsurancearemorelikelytoreceivebettercare than those women with arguably less adequate coverage such as that provided through theMedicaidprogramsofmanystates,orthosewithnocoverage.
OtherSocialDeterminants:Althoughlow-incomeleveland/oralackofhealthinsuranceisusuallyoneof the key reasons for breast cancer screening disparities in the U.S., other factors play a role,particularly for underservedwomen.viiiEven amongwomen between 40-64with insurance, only 68%hadarecentmammogram.Otherbarrierstomammographyscreeningmayinclude:ix
• Lackofausualhealthcareprovider• Lackofarecommendationfromaprovidertogetmammographyscreening• Loweducationlevel• Lackofawarenessofbreastcancerrisksandscreeningmethods• Lackofchildcare• Lackofsickleaveorunabletomisswork• Fearofbadnewsorpainfromtheprocedure• MorerecentmigrationtotheU.S.(bornoutsidetheU.S./livingintheU.S.forlessthan10years)• Culturalandlanguagedifferences
Racialdisparities:Blackwomenaremorelikelytocontractbreastcancerandare43%morelikelytodiefromit;Figure5providesinsightsfromthreecitiesinthetargetstatesx:
FIGURE5:FIVEYEARESTIMATESOFBREASTCANCERMORTALITYRATES
CERVICALCANCER
Barriers to Prevention and Early Detection: Althoughbreast cancer is higher in incidence, it is stillmoresignificantly funded thancervical cancer.Breastcancer receives themost fundingpernewcase($2,956) and the most funding relative to each death ($13,452) than any other cancer.x To further
FIGURE32:FIVEYEARESTIMATESOFBREASTCANCERMORTALITYRATESLOSANGELES(1990–2014)
NEWYORK(1990–2014)
MINNEAPOLIS(1990–2014)

Copyright@ImpactInvestmentExchange(IIX)AsiaPte.Ltd.
20
illustrate this, Table 3 compares American Cancer Society breast cancer grants with cervical cancergrantsxi:
TABLE3:COMPARINGBREASTANDCERVICALCANCERFUNDINGBASEDONACSGRANTS
CancerType NumberofGrants GrantAmounts
Breastcancer 162 $91,422,750
Cervicalcancer 22 $9,337,128
SocialDeterminantsandOther InfluencingFactors:Lessthan1/3oflow-incomewomengetregularpap smears.xiiWomen frommedically underserved populations aremore likely to be diagnosedwithlate-stagecervicalthatmighthavebeentreatedmoreeffectivelyorcuredifdiagnosedearlier.Financial,physical, and cultural beliefs are also barriers that prevent individuals or groups from obtainingpreventative care.xiii This is aggravated by the fact that the HPV vaccination is associated withencouraging promiscuity and there is, therefore, a cultural and ‘mind-set’ barrier that may preventyoungwomenfromcompletingthedosageseries.Additionally,youngmenaretypicallynottargetedbycervicalcancerawarenessoreducationcampaigns.
RacialDisparities:Thecervicalcancermortalityrateforblackwomenwas10.1per100,000.xivForwhitewomen, it is 4.7 per 100,000.xvHispanic/Latino women, however, have the highest cervical cancerincidencerate.WhitewomenlivinginAppalachiasufferadisproportionatelyhigherriskfordevelopingcervical cancer than other white women. Incidence and death rates for cervical cancer are shown inTable4xvi:
TABLE4:CERVICALCANCERINCIDENCEANDMORTALITYRATEACROSSETHNICGROUPS
Racial/EthnicGroup IncidenceRate MortalityRate
AfricanAmerican 11.4 4.9
Asian/PacificIslander 8.0 2.4
Hispanic/Latino 13.8 3.3
White 8.5 2.3
Statisticsarefor2000-2004,age-adjustedtothe2000U.S.standardmillionpopulation,andrepresentthenumberofnewcasesofinvasivecancer(1)anddeaths(2)peryearper100,000women.

Copyright@ImpactInvestmentExchange(IIX)AsiaPte.Ltd.
21
OVERVIEWOFMATERNALHEALTHANDREPRODUCTIVERIGHTS
The Women’s Health Bond will prioritize maternal health care in recognition that the ability forunderservedwomentomanagetheir fertilityaswellas thehealthof themselvesandtheirbabies isabasichumanright.IIXfollowedatwo-prongedapproachtoassessingchallengesfacedbyunderservedwomen as it relates to access, affordability and quality of maternal care: (i) primary data collectedthrough in-personandremote interviews,meetingsandfieldvisits–an importantsteptounderstandpriorities,acuityofneed,toidentifypotentialprojectsthatareaddressingtheissueandworktowardstheinitialshortlistofinitiatives;and(ii)secondarydatacollectedthroughdesktopresearch,reviewsofofficial publications and reports, with key insights validated or verified during the field visits. Assummarizedinthecontextsection,IIXiscurrentlyexploringtwokeyareasundermaternalhealth:
FIGURE6:WHBFOCUSONMATERNALHEALTHANDREPRODUCTIVERIGHTS
KEYCHALLENGESBASEDONSTAKEHOLDERINTERVIEWS
Basedon stakeholder interviewsconductedwith frontlinehealthexperts in the field,Table5outlinesunderfunded areas that add to challenges faced by underserved women through the lenses ofaffordabilityandqualityformaternalhealth.
TABLE5:KEYCHALLENGESANDUNDERFUNDEDAREASFACEDBYUNDERSERVEDWOMENINTERMSOFAFFORDABILITYANDQUALITYOFMATERNALHEALTH
MaternalHealth andReproductiveRights
Prevention EarlyDetection Treatment
Affordability - TitleX fundingprovidedfunding for familyplanning services for lowincome women (andmen), primarily throughPlanned Parenthood. Thisfunding is likely to be cutor eliminated, impactingnearly 1millionwomen inCaliforniaalone.- Medicaid will cover
- Women below thepoverty line can struggleto cover co-pays that areusually required for pre-natal visits. Co-pays canrange from $20-$100,depending on the clinicand the insuranceprovider.Multiplevisits,asrecommended for pre-natal care, can mean
- Patient advocates,doulas,etc.arenotalwayscoveredbyinsurance- Follow up visits formothers may not becovered, nor may chronicconditions developedduring or exacerbated bypregnancy – the threebiggestissuescontributingto escalating maternal
Prevention EarlyDetection Treatment Recovery
• Improvingqualityofprenatalandpostpartumcare• Advancingreproductiverights

Copyright@ImpactInvestmentExchange(IIX)AsiaPte.Ltd.
22
chronic conditions thatimpact fertility andmaternal health, butclinicians may not haveproper incentives in termsofreimbursementtoordertestsorprovidetreatmentacross specialties ortreatment needs with afocus on healthy plannedpregnancies.
significantco-paycosts.- Working women,particularlythoselivingfarfrom service providers,have an opportunity costfor pre-natal visits due tolost work. This loss ofincome, inaddition to thefees of the visits, maymake pre-natal visitsinaccessibleduetocost.
mortality include heartdisease, hypertension andhemorrhage.
Quality - Clinicians do not treatwomen of childbearingage with fertility andconceptioninmindLack of awareness ofimpact of chronicconditions (diabetes,hypertension, etc.) onfetaldevelopment- Reimbursement policies(as above) may impactscreening and treatmentprovidedoremphasized
- In ruralareas, theremaynotbetrainedclinicianstoaddress pre-natal needsand coordinate withtreatment for chronicconditions- Evenwhen clinicians areappropriatelytrained, lackofoperationalfundingcanlead to sub-par facilitiesand lack of appropriatemedicalequipment.
- More than 60% of U.S.hospitals perform fewerthan 1000 deliveries peryear. Lower volumehospitals have beenshown to have highermaternal and neonatalmorbidityandmortality.- Without an advocate,women/families may nothave adequateinformation tounderstanding options—there can be a lack ofcoordination betweenclinicians- Clinicians may not workwith women to addresspostpartumhealthneeds
Access - Maternal Health andFamily Planning (MHFP):most low-income womenreceive family planningand maternal healthservices through PlannedParenthood(0.8outof1.1million in California).Cancellation of Title Xfunding (“Affordability”)means that women willhave to seek other clinicsfortheseservices- There can be severestigma against familyplanning, so even incircumstances where thewomanmayhavephysical
-Over one third of lowincome and/orunderserved women donot see a doctor in thefirsttrimester-Lack of awareness ofimpact of behaviors andchronicconditionsonfetaldevelopment-Clinics that offer pre-natal services can bedifficult to find,particularlyinruralareas.
-Obstetric departments inrural hospitals are closingatanalarmingrate.Today,only46%ofruralhospitalshave been able to retainobstetrics services. Thiscanbefurtherexacerbatedforwomenlookingforcarewithin a particularinsurance system, or for aclinicthattreatsuninsuredpatients.-Both patients and careproviderscandemonstratealackofknowledgeontheneed for frequent andsustained post-partumcare.

Copyright@ImpactInvestmentExchange(IIX)AsiaPte.Ltd.
23
access to reproductiveservices there may beculturalandsocialbarrierspreventingtheiraccess.- Pre-conception (PC): isdependent on awarenessand capability ofclinicians. This oftenrequires sustainedlifestyle changes for thepatient, which requirefrequent follow ups fromtheprovider.
- Navigating the “system” can be difficult—understandingprenatalvisits,laboranddelivery,optionsforcomplications,etc.Thisisparticularlytrueforwomenwith low literacy, or who speak English as a secondlanguage.- Transportation logistics (duration, distance, childcare,medical companion) are a significant barrier for pre-natal, labor and delivery, and post-partum access tocare.Evenifcostwerenotanissue,whichitoftenis,thephysicalbarriercanbeenoughtopreventapatientfromobtainingcare.
ADDITIONALINSIGHTSFROMSECONDARYRESEARCH
MATERNALHEALTH
TheUnitedStatessawa26.6% increase inmaternaldeathsfrom2000 to2014, according toa recentstudy published inObstetrics & Gynecology.xviiIn contrast, maternal mortality rates in other similarlydeveloped nationsdecreased dramatically during this same period.xviiiLack of adequate prenatal andpostpartumcarearecontributingfactorstotheriseinmortality.Motherswhodonotreceiveprenatalcarearethreetimesmorelikelytogivebirthtoalowweightbaby;theirbabyisfivetimesmorelikelytodie.xixCertainnewscastsclaimeverywomanwhodies inchildbirth in theU.S.,anestimated70morecomeclose.xxSocialdeterminantscanfurtheraffecttheoutcomeofprenatalorpost-partumcare.Forinstance,motherswho live in poverty are 3 timesmore likely to have depression than thosewhodonot.xxi
Additionally,between58%–66%(averaging60%)ofpregnancy-relateddeathsarepreventablebasedontimeofdeathinrelationtopregnancy(Figure7).xxiiFederalandstatefundingshowonly6%ofblockgrantsfor"maternalandchildhealth"actuallygotothehealthofmothers.xxiiiIntheU.S,somedoctorsenteringthegrowingspecialtyofmaternal-fetalmedicinewereabletocompletethattrainingwithouteverspendingtimeinalabor-deliveryunit.xxiv
FIGURE7:PREVENTABILTYOFMATERNALMORTALITYBASEDONTIMEOFDEATHINRELATIONTOPREGNANCY
FIGURE28:PREVENTABILITYOFDEATHBASEDONTIMEOFDEATHINRELATIONTOPREGNANCY1

Copyright@ImpactInvestmentExchange(IIX)AsiaPte.Ltd.
24
Considerableracialdisparitiesinpregnancy-relatedmortalityexist.AccordingtotheCDC,during2011–2013,thepregnancy-relatedmortalityratioswerexxv:
• 12.7deathsper100,000livebirthsforwhitewomen.• 43.5deathsper100,000livebirthsforblackwomen.• 14.4deathsper100,000livebirthsforwomenofotherraces.
Thismeansblackwomenareatespeciallyhighrisk,beingthreetofourtimesmorelikelytodieduringpregnancyorchildbirththanwhitewomen.Causesofpregnancy-relateddeathdifferbyrace(Figure8),whichhighlightsuniqueopportunitiesforprevention.xxvi
FIGURE8:LEADINGUNDERLYINGCAUSEOFPREGNANCY-RELATEDDEATHS,BYRACE/ETHINICITY
REPRODUCTIVERIGHTS
Thecostofunintendedpregnancies:Almosthalf(45%or2.8million)ofallpregnanciesintheUnitedStates are unintended, with nearly 5% of reproductive-agewomen having an unintended pregnancyeachyear.xxviiThecostofunintendedpregnanciestotheUSeconomyisestimatedtobe$21billionperyear.xxviiiOnly26%ofwomen inneedofpublicly fundedcontraceptives receivetheseservices,.18%ofwomen at risk of unintended pregnancy use contraceptives inconsistently/ incorrectly, and 10% ofwomendonotusecontraception.xxix
RacialDisparities:Womenofcolor(particularlyblackorHispanicwomen)andundocumentedwomenaredisproportionatelyunlikelytousecontraceptivesduetothreereasons:(i)providerbias:withintheblack community many patients experience negative patient-provider experiences; (ii) trust incontraceptiveoptions:biascombinedwithahistoryofforcedsterilizationandcoercionfostersdistrustin the health care system specifically for women of color; (iii) immigration status: undocumentedimmigrantsmaynothaveaccess to the financial resources to access contraceptives, even thosewhohavegainedlegalstatusmustwaitfiveyearsbeforereceivingMedicaidcoverage.xxx
DisparitiesincontraceptionusearemappedoutbelowinFigure9andFigure10:
FIGURE27:LEADINGUNDERLYINGCAUSESOFPREGNANC-RELATEDDEATHS,BYRACE-ETHNICITY1

Copyright@ImpactInvestmentExchange(IIX)AsiaPte.Ltd.
25
FIGURE9:DISPARITIESINCONTRACEPTIONUSEANDABORTIONACCESS
FIGURE10:QUANTIFYINGCONTRACEPTIVEUSEBASEDONRACEANDETHNICITY
RepercussionsofCutstoTitleXFunding:DefundingofTitleXwillmeanthelossofnearly$300Mforfamilyplanningandhealthscreening for4millionpeople,mostofwhomare low-income.xxxiBetween2006 and 2010, a total of 43 million women aged 15 to 44 years reported having received familyplanning or a related medical service in the past 12 months.xxxii Approximately half of the 18% ofwomenwho received such careat a clinicdid soat aTitleX–funded clinic.xxxiiiUseofTitleX clinics ismorecommonamongwomenwholiveinanonmetropolitanareaorareblack,Hispanic/Latina,belowthepovertylevel,oruninsured.xxxiv
FIGURE30:DISPARITIESINCONTRACEPTIONUSEANDABORTIONACCESS
FIGURE31:QUANTIFYINGCONTRACEPTIVEUSEBASEDONRACEANDETHNICITY1

Copyright@ImpactInvestmentExchange(IIX)AsiaPte.Ltd.
26
CRITERIA2:TARGETSEGMENTOFTHEHEALTHCONTINUUM
The second criterion is to ensure that theWHB takes a proactive approach to delivering care and isequipped to improve efficiency or effectiveness across the continuum of care (Figure 20) at threedistinctlevels:
1. Patient Level (main priority): Improving access, affordability and quality of health care,enhancinginclusivenesstodrivehealthequityandtimelinessofcare
2. Provider Level: Improving outcomes achieved by shifting to patient-centered care, achievingsamelong-termoutcomesatreducedcost
3. SystemLevel:Improvingcost-efficiency,reducingpressureoncapacity,shiftingtovalue-basedcarefromvolume-basedcare
Figure 11 provides an overview of the continuum of care overlaid with the levels of the health caresystem:
FIGURE11:LEVELSOFHEALTHCARESYSTEMANDCONTINUUMOFCARE
Thefollowingsectionwillexplorehowinterventionscan:
1. Improve effectiveness:Theabilitytoachieveimprovedhealthcareoutcomesinasustainablemanner
2. Improve efficiency: The ability to achieve the same outcomes while reducing the resources(time,money,talent)requiredoverthelong-term
SocialDeterminantsofHealthandRepercussionsofReactiveHealthCare
ImpactofSocialDeterminantsofHealthonLow-Income,Minority,RuralandWomenofColor
Based on interviews with patient advocates and frontline health workers, a common trend thatemergedwasthatlow-income,minorityandruralwomenalltendtobemorereactivewiththeirhealthcare.Expertssuggestthisispartlyduetosocialdeterminantsofhealth(SDH)whicharedefinedastheconditionsinwhichpeopleareborn,grow,work,live,andage,andthewidersetofforcesandsystemsshaping the conditions of daily life (WHO). These forces and systems include economic policies andsystems, development agendas, social norms, social policies and political systems. Women living inpoverty, women with lower education levels, women that struggle to navigate the system due tolanguagebarrierstypicallyaremorereactivewiththeirhealthcare.Womenofcolor,regardlessoftheirsocio-economicstatus,tendtohavelowertrustinthesystemandtherebyavoidavailingofhealthcare
PatientLevel
ProviderLevel
SystemLevel
Prevention EarlyDetection Treatment Recovery
Leve
lsofH
ealth
careSystem
ContinuumofCare

Copyright@ImpactInvestmentExchange(IIX)AsiaPte.Ltd.
27
services until the issue has progressed to an advanced stage. Finally, research shows costs can be abarrierforbothinsuredanduninsuredwomenxxxv:
• 52%ofuninsuredwomenand13%ofinsuredwomenpostponepreventativeservicesbecauseofcost
• 50%ofuninsuredwomenand13%of insuredwomenskiprecommendedmedicaltestsduetocosts.
RepercussionsofReactiveHealthCareAcrosstheSystem
The repercussions ofwomenbeing reactivewhen seeking health care have a ripple effect across thehealth care systemas outlinedbelow (Figure 12).As such, a reactive approach to health care canbebothexpensiveandsomewhatineffectiveatachievingsustainableoutcomes.
FIGURE12:RIPPLEEFFECTOFREACTIVEHEALTHCARE
ProactiveBreastandCervicalCancerMeasures:
• Cervical cancer: Vaccines are available to help prevent infection by certain types ofHPV andsome of the cancers linked to those types. As of 2017, Gardasil 9® is the only HPV vaccineavailableintheUnitedStates.Gardasil9helpspreventinfectionby4typesofHPV(16,18,6and11),plus5otherhighrisktypes:31,33,45,52and58.xxxviTogetherthesetypescauseabout90%ofcervicalcancers(aswellasmanyothercancersoftheanus,penis,vagina,vulvaandthroat).Anotherwell-provenway toprevent cervical cancer is tohave testing (screening) to findpre-cancers before they can turn into invasive cancer.xxxviiThe Pap test (or Pap smear) and thehumanpapillomavirus(HPV)testareusedforthis.
• Breastcancer:Preventionofbreastcancer ismostly linkedto lifestylechanges,healthierdietsand preventative surgery. Different tests can be used to detect breast cancer early includingmammograms,breastultrasounds,breastMRIscans,newerbreastimagingtestsandbiopsy.
AbilitytoEnhanceOutcomes:
While the cervical cancer vaccination has a proven ability to improve outcomes (by completelyeliminatingtheriskofmortality),earlydetectionofbreastcancer ismorecomplex.Data fromclinicaltrials ofmammography showed it reduces themortality rate from breast cancer by at least 15% forwomen in their 40s and by at least 20% for older women.xxxviiiHowever, it is important to note thatresearch indicatesthatwhile5 in1,000womendieofbreastcancerwithoutavailingofscreening, thenumberisonlyreducedby4in1,000womenforwomenwhoarescreened.xxxixThesocialandfinancialcostoffalsepositivesindicatesincreasedneedtoimprovequalityofscreeningtools.
PatientLevel
ProviderLevel
SystemLevel
Lowerprobabilityofsuccessfuloutcomesandreducedqualityoflife,higherlong-termcosts(treatmentistypicallymoreexpensivethanprevention)
Increasedpressureoncapacity,highercomplexityandresourceintensivenessofinterventionsrequiredtoachievethesameoutcomes
Higherpressureonthesystemduetolongerperiodsoftreatment,higherhealthcarecoststobeabsorbedatthestateandnationallevel

Copyright@ImpactInvestmentExchange(IIX)AsiaPte.Ltd.
28
AbilitytoReduceLongTermCosts:
• Patientlevel:California,MinnesotaandNewYorkprovidefreebreast/cervicalcancerscreeningfortheuninsured/underinsured.However,thisrequireswomentobeeligible(low-incomestatusdependentonstateregulations).Italsorequireswomentobeawareoftheprogram,applyforeligibility, andbeable tonavigate/access theproviderand/or reimbursement systemwhich istypicallywhyallunderservedwomendonotbenefitfromtheseprograms.
• Provider/Systemlevel:Theannualnationalcostsavingsforearlydiagnosisofbreastcancerisestimatedtobe$1,562millionandforcervicalcancertobe$221million.xl
• Additionalconsiderations:Whilethemajorityoffundingisfocusedoncancertreatment,thereisrelativelylowerfundingavailableforpreventionandearlydetection.Forinstance,theNationalCancer Institutebudget for2012-13 reflected$1.3billion for treatmentversus$232million forprevention.xli
ProactiveMaternalHealthCareMeasures:
• Nearly60%ofpregnancy-relateddeathsareestimatedaspreventable(Figure13).xlii
• The two primary causes of death are cardiovascular disease and other medical non-cardiovascular disease, indicating potential issues related to prenatal health or preventabledisease.xliii
• Uninsuredwomenuse fewerpreventive servicesandaremore likely todelay carebecauseofcost.xliv
• Additionally, access to improved reproductive health services can help prevent unintendedpregnancies–overhalfofallpregnanciesintheUnitedStatesareunintended.xlv
FIGURE13:DISTRIBUTIONOFPREVENTABILITYAMONGPREGNANCYRELATEDDEATHS
AbilitytoEnhanceOutcomes:
Inordertotrulyprovidemotherswithproactivematernalhealthservices,womenmusthaveaccesstoand a longitudinal relationship with a primary care physician who understands a woman's individual
FIGURE22:DISTRIBUTIONOFPREVENTABILITYAMONGPREGNANCYRELATEDDEATHS
Copyright@ImpactInvestmentExchange(IIX)AsiaPte.Ltd.
29
health needs at each stage of her life, access to subspecialists who are properly trained to care forwomenhavinghigh-riskpregnanciesorprovidethedistinctperspectiveofpediatricianstreatingyoungwomenorgeriatricianstreatingolderwomen.Assuch,accesstopreventativecareisnotsufficientandthereneedstobeanadequatefocusonimprovingoutcomesachievedinsteadofvolumeofservices.
AbilitytoReduceLong-TermCosts:
• Patient Level: Apart fromdirect cost savings,which is critical to uninsuredmothers, patientsalsoexperienceindirectcostsavingsfromimprovedqualityoflifeandproductivity.
• Provider/SystemLevel:xlvi
• Prenatal care: The cost of caring for babies who weigh less than 1,140 grams (2.5pounds)atbirthisestimatedtobeanaverage$140,000perpatient,bringingtheannualcostofneonatal intensivecare intheUnitedStatestoatotalof$1.5billion.Foreverydollar spentonprenatal care, $3.38 is saved in the costof caring for low-birth-weightinfants.
• ReproductiveHealth:Totalpublicexpenditureonunintendedpregnanciesisestimatedtobe$21billionperannum.
Conclusion
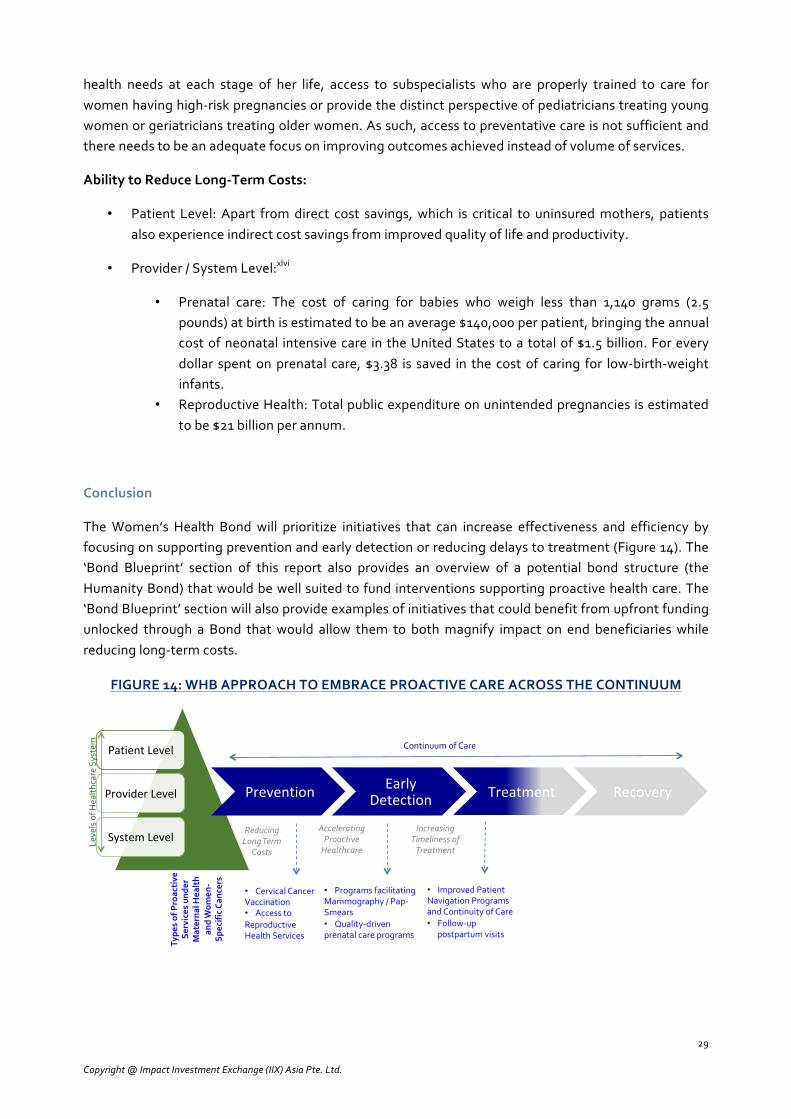
TheWomen’s Health Bond will prioritize initiatives that can increase effectiveness and efficiency byfocusingonsupportingpreventionandearlydetectionorreducingdelaystotreatment(Figure14).The‘Bond Blueprint’ section of this report also provides an overview of a potential bond structure (theHumanityBond)thatwouldbewellsuitedtofundinterventionssupportingproactivehealthcare.The‘BondBlueprint’sectionwillalsoprovideexamplesofinitiativesthatcouldbenefitfromupfrontfundingunlocked through a Bond thatwould allow them to bothmagnify impact on end beneficiarieswhilereducinglong-termcosts.
FIGURE14:WHBAPPROACHTOEMBRACEPROACTIVECAREACROSSTHECONTINUUM
PatientLevel
ProviderLevel
SystemLevel
Prevention EarlyDetection Treatment Recovery
Leve
lsofH
ealth
careSystem
ContinuumofCare
• CervicalCancerVaccination• AccesstoReproductiveHealthServices
• ProgramsfacilitatingMammography/Pap-Smears• Quality-drivenprenatalcareprograms
• ImprovedPatientNavigationProgramsandContinuityofCare• Follow-up
postpartumvisits
Type
sofProac
tive
Se
rvices
und
er
Materna
lHea
lth
andWom
en-
Spec
ificCa
ncers
IncreasingTimelinessofTreatment
AcceleratingProactiveHealthcare
ReducingLongTerm
Costs

Copyright@ImpactInvestmentExchange(IIX)AsiaPte.Ltd.
30
CRITERIA3:TARGETSTATES
The final criterion explores the potential of selected states to align with two factors (i) demand forcapital,i.e.presenceofinnovativehealthcareproviderswithsolutionsthatareequippedtoeffectivelyabsorbanddeploycapital;and(ii)supplyofcapital,i.e.abilitytobringinnewinvestorsfromtheprivatesector into the health care equation based on key investment drivers. Thiswill lay the foundation tocreateaninnovativefinancialmechanismusingpositiveincentivestounlocknewsourcesofcapitalforwomen’s health at the pace and scale required. The following section outlines a series of questionsassessed as part of the feasibility study to support the decision-making process to narrow down thethreetargetstatesofCalifornia,MinnesotaandNewYork.
Question 1:Are there fundinggaps forwomen’shealth care in theUnitedStates indicating thatcurrentsourcesofcapitaldonotsufficientlyaddresskeyissuesfacedbyunderservedwomenatthepaceandscalerequired?
PUBLICSECTORANALYSIS
HealthcarespendinghasoutpacedthegrowthoftheUSeconomy,outlinedinFigure8.Inadditiontopolicychanges, federal, state,and localbudgetsarebeing furthersqueezedbydemographicchangesandausteritymeasures.Annualhealthcosts for low incomecommunitiesareexpectedtogrowat3%peryear,comparedto0.5%peryearfortherestofthepopulation.xlviiFunding lossesfromchangestotheAffordableCareAct (ACA) could total $172Bbetween 2020-2026xlviii; solutionsmust look beyondonly increasing insurancecoverage to funding initiatives thatwilldeliverpatient-centeredcare that isaffordable,accessibleandcommittedtoimprovequalityofoutcomes.
SPOTLIGHT:INSIGHTSFROMSTAKEHOLDERINTERVIEWS
Accordingtostakeholderinterviews,thetopthreelimitationsofrelyingonpublicsectorfunding(eitherfromthefederalandstatelevel)are:
! Unreliable: Stakeholders interviewed indicated relying solely onpublic sector funding canbeunreliable in the event of policy changes, particularly for organizations focused onmaternalhealth.
! Limited Links to Impact:Stakeholders interviewedindicatedlimitedlinkagesbetweenpublicsectorfundingreceivedandoutcomesachieved,orpatient-centeredapproachadopted.
! Limited Leverage: Stakeholders interviewed indicated there are limited mechanisms usingpublicsectorfundingtoeffectivelycatalyzeadditionalcapitalwhichwillhelptomultiplyimpactachievedatagreaterpaceandscale.
PHILANTHROPICSECTORANALYSIS
Philanthropicfundingforhealthcare,whichwillbeexpectedtomakeupforshortfalls inpublicsectorfunding,accountsforjust$5billionofthetotal$3.3trillionspentannuallyonhealthcareintheUnitedStates (2013).xlixThe total value of grants directed towards women’s and girls’ health issues in theUnitedStateswaslimitedto$520million(2013)butisnotablyonanupwardtrend.l

Copyright@ImpactInvestmentExchange(IIX)AsiaPte.Ltd.
31
SPOTLIGHT:INSIGHTSFROMSTAKEHOLDERINTERVIEWS
Accordingtostakeholderinterviews,thetopthreelimitationsofrelyingonphilanthropicare:
! Time Consuming: Stakeholders interviewed indicated that to mobilize philanthropic grantstheymust investasignificantamountoftimeandresourcestofund-raiseupfrontandthentoreportonoutputsduringthe lifeofthegrant.Thistakesawayresourcesfromfocusingontheactualwork.
! One-off Grants: Stakeholders interviewed indicated that themajorityof philanthropic actorstend to provide one-off grants with narrowly defined focus areas as opposed to multi-yearsupportwhichwouldallowrecipientstheflexibilitytofocusonsustainingimpactandachievinglong-termoutcomes.
! LimitedLeverage:Stakeholdersinterviewedindicatedthattherearelimitedmechanismsusingphilanthropicsectorfundingtoeffectivelycatalyzeadditionalcapitalwhichwillhelptomultiplyimpactachievedatagreaterpaceandscale.
Question2:Istherepotentialtounlocknewsourcesofcapital,particularlyfromtheprivatesector,to advance health care for underserved women using blended finance or innovative financialmechanisms?
Theconclusionfromtheanalysisofpublicandphilanthropiccapital is that itwillbe imperativetotapinto the~$85 trillion capitalmarkets tomobilizeadditional capital from theprivate sector toaddressfunding gaps that the public and philanthropic sector are not expected to be able to support at therequiredpaceandscale. Theabilityoftheprivatesectortoaddressthesegapsandsupportaproductsuch as a Women’s Health Bond with dual social and financial goals is assessed based on theintersectionoftwomovements:(i)InnovativeFinance;and(ii)GenderLensInvesting.
FIGURE15:EXPLORINGTHEINTERESTININVESTINGINWOMEN’SHEALTH–THEINTERSECTIONOFTHEINNOVATIVEFINANCEANDGENDER-LENSMOVEMENTS
Growinginnovativefinancemovement(risingtrendsintheblendedfinanceandimpactinvestingspacefocusedonhealth)
Growinginterestininvestinginwomen
(risingtrendsingenderlens
investingandbringingwomen
intocapitalmarkets)
InvestinginWomen’sHealth

Copyright@ImpactInvestmentExchange(IIX)AsiaPte.Ltd.
32
GROWINGINNOVATIVEFINANCEMOVEMENT
The innovative finance movement has rapidly evolved over the past decade to bring private sectorcapital into thesustainabledevelopmentequation.Oneof thechannelsof innovative finance, impactinvesting, refers to investmentswith the intention to generate dual social and financial returns. Theestimatedmarketsizeis$228billionli.5%oftotalimpactinvestingmarketsizefocusedonhealthcareinvestmentsindicatingatotalvalueof$11.4billion(Figure16)lii.49%ofimpactinvestorshavehealthasoneoftheirfocussectorsliii.
FIGURE16:TAPPINGINTOTHEIMPACTINVESTINGMOVEMENTTOFINANCEHEALTHCARE
GROWINGINTERESTININVESTINGINUNDERSERVEDWOMEN
Thereisagrowinginterestacrosstheworldfromtheprivatesectortoinvestinwomenempowermentandfromthephilanthropicsectortofundinitiativesfocusedongenderequality.Thisservesasthebasisforanopportunitytostructurean innovativefinancialmechanismthat leveragesexistingcapital fromphilanthropicactorstounlockupfrontfundingfromtheprivatesector.
Additionally, there is an increasing focus around gender equality and empowerment in the UnitedStates, further indicating there will be market interest in participating in innovative financialmechanismsfocusedon improvingthe livesofunderservedwomen.This issupportedbythegrowingrecognition thatempoweringwomenwithaffordable,qualityhealthcareshouldbeviewedasabasichumanright,notaprivilegecontingentonthewomen’ssocio-economicstatus.OnereasonforgrowinginterestininvestinginwomeninAmericaiswomen’srateofparticipationinthelabormarketrosefrom34% in 1950 to 57% in2016,puttingmorewealth in thehandsofwomenwho in turn invest inotherwomen.livBetween2010and2015,privatewealthheldbywomengrewfrom$34trillionto$51trillion.lvWomen’s wealth also rose as a share of all private wealth from 28% to 30% and by 2020 they areexpectedtohold$72trillion,32%ofthetotal.lvi
Othermovementssuchas#MeTooand#BlackLivesMatterhave furtherbuiltmomentumfor fundinginitiativesthatempowerwomenandinparticular,thatfocusonaddressingtheneedsofmarginalizedcommunitiesorsegmentsofthepopulationthathavefaceddiscrimination.
Source:GIIN2018

Copyright@ImpactInvestmentExchange(IIX)AsiaPte.Ltd.
33
Question3:Whichstateshavesupportiveecosystemsforaninnovativefinancialmechanism,bothintermsofpresenceofapipelineofhighimpactinitiativestoabsorbanddeploycapitalandfromaregulatoryperspective?
Table6outlines thekeypositive screening criteria thatplayeda role indetermining the feasibilityoffocusingthefirsttranchesoftheWomen’sHealthBondonCalifornia,MinnesotaandNewYork:
TABLE6
Source:MinnesotaHealthScoreCard,Availableat:https://mnbp.com/wp-content/uploads/2015/02/MBP_HealthScorecard.pdf
POSITIVESCREENINGCRITERIAFORTARGETSTATES
CALIFORNIA
Supportiveenvironmentforgenderlensinvestingandwomen’sreproductiverights:
-Californiahasastronghistoryofsupportingwomen’srightsandbuildinganinclusivecommunitythatembracesundocumentedwomen.
-Assuch,whenassessingthefeasibilityoftheWomen’sHealthBondfromthedemandsideoftheequation,Californiahasarelativelystrongerpipelineofhigh-impactinitiativesthatcanpotentiallyabsorbanddeploycapitaltoprovideunderservedwomenwithaccesstoaffordable,qualityhealthcare.-Whenassessingthesupplysideoftheequation,therearealargenumberoflocalfoundationsinterestedinsupportingwomen’shealth(refertotheecosystemmappingsectioninthisdocumentforalistofecosystemactorsidentifiedthatarebasedinCA).Thesefoundationscanserveaspotentialpartnersinblendedfinancialvehiclesthatusegrantcapitaltoleverageprivatesectorinvestments.
NEWYORK
Previoustrackrecordsupportinginnovativefinancialmechanismsandrelativelygreaterunderstandingofimpactinvestingamongphilanthropicfunders:
-NewYorkwashometothefirstSocialImpactBondintheUnitedStates,focusedonreducingrecidivisminRiker’sIsland.AlthoughtheBonditselfwasnotsuccessful,itlaidthefoundationforinvestorinterestinalternativevehiclesforfundingpressingsocialissues.-Additionally,NewYorkservesastheheadquartersforanumberoffoundationsthathavesupportedtheimpactinvestingspaceinthepast,includingtheRockefellerFoundationwhichcoinedtheterm‘impactinvesting’in2008.-Assuch,thereisarelativelystrongerunderstandingofinnovativefinanceascomparedtootherstates,increasingthelikelihoodofsuccessforinitialtranchesoftheBondiftheyarefocusedonNewYork.
MINNESOTA
Stronglinksbetweenhealthcaresectorandgrowthofthestateeconomyandhighlevelofprivatesectorinvolvementinthesectorincreasesthelikelihoodoflocalinvestorparticipationandcorporatesupport:
-Thehealthcaresector,vitaltothestate’seconomy,accountsforalargeandgrowingportionoftheemploymentbase;16ofthestate’stop50employersarehealthcarecompanies,whichrepresent32%ofMinnesota’sjobs.-Healthcareprovidersaloneemployedmorethan16%oftheworkforcein2010andareoneoftheeconomy’sfastest-growingsegments.-Throughitsactiveinvolvementandleadershiponhealthcareissues,theprivatesectorhascreatedastrongfoundationforcollaborationwiththestateandauniqueplatformfromwhichtoeffectchange.Thisincreasesthelikelihoodoflocalinvestorsandlocalcorporatesbasedinthestatetoparticipateinthebondissuance.

Copyright@ImpactInvestmentExchange(IIX)AsiaPte.Ltd.
34
Question4:Instateswhereaninnovativefinancialmechanismisexpectedtobefeasible,isthereaclear need to mobilize capital, both in terms of absolute need and acuity of need (focusing onwomen-specificcancers,maternalhealthandreproductiverights)?
The final question will reassess the ability of the Bond to achieve desired outcomes in target statesdeterminedasfeasiblebyreviewingkeystatisticsrelatedtobothabsoluteneedandacuityofneed interms of the specific health issues narrowed down as part of the first criteria –maternal health andwomen-specificcancers.
Table 7 summarizes the key statistics related to absolute need of underserved women in the threetargetstates.
TABLE7:ABSOLUTENEED–SUMMARYOFKEYSTATISTICS
KeyIndicator California Minnesota NewYork
#ofwomen(age18andolder) 15,283,600 2,132,700 8,042,900
%womenbelowpovertyline 14% 10% 13%
#womenbelowpovertyline 2,139,704 213,270 1,045,577
%womenreportingpoorhealth 20% 20% 21%
#womenreportingpoorhealth 3,056,720 426,540 1,689,009
#ofcriticalaccesshospitals 34 78 18
#ofruralhealthclinics 280 89 9
#offederallyqualifiedhealthclinics 194 16 65
#ofwomenwithouthealthinsurance 1,776,848 249,391 710,436
% of women not seeing doctor due to
cost
(inthelast12months)
20%
White:17%
Black:23%
Hispanic:26%
18%
White:15%
Black:-
Hispanic:26%
17%
White:15%
Black:23%
Hispanic:33%
Sources:USCensusReports2017,KaiserFamilyFoundationStateProfilesforWomen’sHealth,Statistica
Table 8 summarizes the key statistics related to acuity needof in the three target states in termsofwomen-specificcancersandmaternalhealth.

Copyright@ImpactInvestmentExchange(IIX)AsiaPte.Ltd.
35
TABLE8:ACUITYOFNEED–SUMMARYOFKEYSTATISTICS
KeyIndicators California Minnesota NewYork
BreastCancerIncidence(per100,000women) 118.7 130.9 132.3
BreastCancerDeaths(per100,000women) 20 17 19.2
CervicalCancerIncidence(per100,000women) 6.9 4.8 7.3
CervicalCancerDeaths(per100,000women) 2.3 1.3 2.4
CervicalCancerScreening(%ofwomenaged18–44) 79.6% 81.1% 78.4%
LowBirthWeight
7%White:6%Black:12%Hispanic:
7%
6%White:6%Black:9%Hispanic:6%
8%White:6%Black:12%Hispanic:8%
MaternalMortality(deathsper100,000births) 4.5 13 20.6
PostpartumDepression (%ofwomenwitha recentlivebirth)
13% 9% 12.2%
DedicatedHealthCareProvider(%ofwomenaged18–44)
71.7% 72.4% 80%
Alcohol During Pregnancy (% of pregnant womenaged18–44)
7.6% 5.4% 8.3%
NoPostpartumVisit (%ofwomenwitharecentlivebirth)
12.5% 9.1% 8.9%
Sources:USCensusReports2017,KaiserFamilyFoundationStateProfilesforWomen’sHealth,Statistica
OTHERKEYFACTORSTOASSESSABSOLUTEANDACUITYOFNEEDINTARGETSTATES
Besides focusing on absolute number of low-incomewomen or rural communities, other key factorsmapped as part of the analysis including number of undocumented women, uninsured women andwomenofcolor.
Undocumentedwomen:Figure17mapstheundocumentedpopulationintheUnitedStates.
Keyinsight:Californiahasbyfarthelargestnumberofundocumentedimmigrants(about2.3millionin2014).About six-in-ten undocumented immigrants live in California, andNewYork (twoof theWHBtargetstates)andinFlorida,Illinois,NewJerseyandTexas.lvii

Copyright@ImpactInvestmentExchange(IIX)AsiaPte.Ltd.
36
FIGURE17:ESTIMATEDUNDOCUMENTEDPOPULATION(2014)
Uninsuredwomen:Figure18mapstheuninsuredpopulationintheUnitedStates.
Keyinsight:CaliforniaandNewYorkarebothrankedinthetoptenprioritystatesintermsofabsolutenumberofuninsuredorunderinsuredwomen.lviii
FIGURE18:ESTIMATEDNUMBEROFWOMENWHOAREUNINSURED(2014)
Ethnic/racialdiversity:Majorityofunderservedwomenareexpectedtobenon-whites.BothNewYorkandCaliforniafeatureamongthegivemostdiversecountiesintheU.S.,whichinclude:lix
• Queens County, New York (27.6% white/non-Latino, 17.7% African American, 0.3% NativeAmerican,22.8%AsianAmerican,27.5%Latino,and4%other)
• Alameda County, California (34.1% white/non-Latino, 12.2% African American, 0.3% NativeAmerican,25.9%AsianAmerican,22.5%Latino,and5.1%other)
• Solano County, California (40.8% white/non-Latino, 14.2% African American, 0.5% NativeAmerican,14.3%AsianAmerican,24%Latino,and6.2%other)

Copyright@ImpactInvestmentExchange(IIX)AsiaPte.Ltd.
37
SpotlightonAbsoluteNeedofReproductiveRights:Figure19mapstheunintendedpregnancyrateintheUnitedStates.lxCaliforniaandNewYork ranked in the toptenprioritystates in termsofabsolutenumberofwomeninneedofreproductiveservices.lxi
FIGURE19:MAPPINGUNINTENDEDPREGNANCYRATEPER1000WOMEN,15-44
Spotlight on Minnesota: Minnesota consistently performs well across various national healthperformancescorecards.However,notallwomenresidinginthestateareequallylikelytobereflectedintheserankingsbecausethestatehassomeofthe largestracial,ethnicandgeographic inequities inhealth status and incidence of chronic disease in the country particularly among undocumentedcommunities.Keystatisticsincludelxii:
• Minnesota’s foreign-born population is increasing faster than the national average, tripling since1990whilethenationalaveragehasonlydoubled.Onlyaboutone-thirdofMinnesota’simmigrantswereborninLatinAmerica,comparedtomorethanhalfofimmigrantsnationally.Similarly,oneinfiveMinnesotaimmigrantswereborninAfrica,comparedtoonly4%nationally.TheTwinCities,inparticular,ishometoarelativelylargeAmericanIndianpopulation,includingmembersoftheLittleEarthofUnitedTribesandShakopeeMdewakantonSiouxcommunities.lxiii
• Asian immigrants tended tohavehigheroutcome ratesacrossmultiplemeasuresandgeographicareas. In fact,Vietnamese immigrantshadthehigheststatewiderateforoptimaldiabetescareofany racialorethnicgroup. In theWestMetroRegion,64percentofVietnamese immigrantswerereceivingsuchcare.TherewasoneexceptiontothesehigherratesamongAsianimmigrants:thoseborn inLaos.Theygenerallyhad lowerhealth careoutcomes thanotherAsian-bornpatientsandotherpatientsingeneral.lxiv
• Womenof color inMinnesotaare less likely to receivepreventivecare,more likely to suffer fromserious illnesses and have less desirable health outcomes, and less likely to receive clinically-necessary procedures and services. Racial and ethnic disparities accounted for an estimated $60billioninexcesshealthcarecostsin2009.lxv
As such,Minnesota is currently being considered as a potential focus state for theWomen’s HealthBond,eventhoughitdoesnothavethesamescaleofissuesasothertargetstates.


Copyright@ImpactInvestmentExchange(IIX)AsiaPte.Ltd.
39
BLUEPRINTOFTHEWOMEN’SHEALTHBOND
Thepurposeofthissectionistooutlinethedecision-makingprocessbehindthedesignoftheWomen’sHealthBondandreviewpotentialinnovativestructuresthatmaybesuitable.Toaddressthisquestion,IIXadoptedathree-stageanalysisasoutlinedinFigure20anddescribedindetailbelow:
FIGURE20:DESIGNINGTHEBLUEPRINTOFTHEBOND
Whatistheexpectedprofileofrelevanthealthcareentities?
Relevanthealthcareentitiesforthisanalysisneedtomeetthreemaincriteria:
(i) Clearfocusontargetingunderservedwomen
(ii) Existinginitiativesthataddressthechallengesfacedbythesewomen
(iii) Clearneedforadditional/alternativesourcesofcapital
Based on the aforementioned criteria, relevant health care entities are typically non-profit initiativeswhichindicatestheneedtomobilizeacombinationofdebtandgrantcapital(non-profitentitiescannotabsorbequitycapitalorvariantsofthesame).Theexpectedprofileandneedsofthesenon-profitsvary:
- 501c3entities (eg:BlackWomenforWellness),professionalassociations (eg:AmericanCollegeofObstetrics and Gynecologists) and national level voluntary health organizations (eg: AmericanCancer Society) that run innovative patient-centered programs and need more flexible fundingoptionstoenhancethepaceandscaleoftheirimpactonunderservedwomen.
- Hospitals thathavean innovativenew initiative that isunequipped to tap into traditional fundingsourcesfromeitherthecapitalmarketsorfromfederalorstatelevelgrants(eg:BuildingaMother’sCenterbyNewYorkPresbyterian).
- FederallyQualifiedHealthClinicsandCommunityHealthClinicsthatdonotbenefitfromthecapitalmarketsatthesamelevelaslargehospitals.However,theseentitiescanonlyabsorbasmallportionofcapitalperyearwhichmaymandatethattheybeaggregatedintoaportfolio.
Whatarethefundingbarriersthattheseentitiesfaceandwhichofthese
canbeaddressedbyinnovativefinancialmechanismsuchasa
Women’sHealthBond
Whatbondstructureswouldbemostsuitabletounlocktherighttypeofblendedcapitaltoenabletheseentitiestocreatedemonstrable
outcomesonunderservedwomen
FundingBarriersFacedbyEntities
TypeofFundingaBondcanUnlock
Targetunderserved
women
Haveinitiativesthat
addresschallengesidentified
Needadditional/alternativesourcesofcapital
PotentialBond
Mechanism
Whatistheprofileofhealthcareentitiesbasedon(i)abilitytotargetunderservedwomen;(ii)existing
initiativesaddressingchallenges;(iii)needforadditionalcapital

Copyright@ImpactInvestmentExchange(IIX)AsiaPte.Ltd.
40
Whatarethekeyfundingbarriersfacedbytheseentities?
Based on stakeholder interviewswith potential recipients of funding, IIX has identified the followingfundingbarriersthattheWomen’sHealthBondwouldneedtoaddress:
(i) Time Consuming: Long process to solicit grants from philanthropic funders and resource-intensivereporting
(ii) One-offGrants:Grantsareoftennotmulti-yearresultinginlimitedfocusonlong-termprogramperformance
(iii) LimitedLinkstoImpact:Fewcontractslinkcapitalmobilizedwithforward-looking,outcomes-focusedM&E
(iv) Limited Leverage: Limited ability for current funding to catalyze new sources of capital, nomultipliereffect
(v) Unreliable:Fundingfrompoliticalsourcesinparticulartendtobeunreliableandcontingentonpolicychanges
Whatinnovativebondstructureswouldbemostsuitable?
IIXisexploringavarietyofinnovativefinancialmechanismswhiledesigningtheWomen’sHealthBondas outlinedbelow.The following sectionwill provide anoverviewof howeach structureworks and acomparativeanalysistodefinethemechanismthatwouldbemostsuitedtofundhealthcareentitiesinthe United States. The unique merits and drawbacks of each of the different structures have beendiscussedwithTaskForcemembers,healthcareexpertsandpotentialentitiesthatwillbe included intheBondtosolicitdiversefeedbackanddrawarangeofperspectives.
PotentialStructure1:SustainabilityBond
Aninnovativedebtsecuritythatmobilizesinvestmentcapitalfromtheprivatesectorandisrepaidbyapoolofborrowersachievingdualsocialandfinancialreturns
FIGURE21:OUTLINEOFSUSTAINABILITYBONDMECHANISM
SUSTAINABILITYBOND
PRIVATESECTORINVESTORS
BANKINGPARTNERS LEGALPARTNERSPORTFOLIOMANAGER
ANDLEADSTRUCTURER
GUARANTEEPARTNER(FOUNDATION/GOVERNMENT)
FINANCIALLYSUSTAINABLEIMPACT
ENTERPRISE
FINANCIALLYSUSTAINABLEIMPACT
ENTERPRISE
FINANCIALLYSUSTAINABLEIMPACT
ENTERPRISE
FIGURE33:OUTLINEOFSUSTAINABILITYBONDMECHANISM
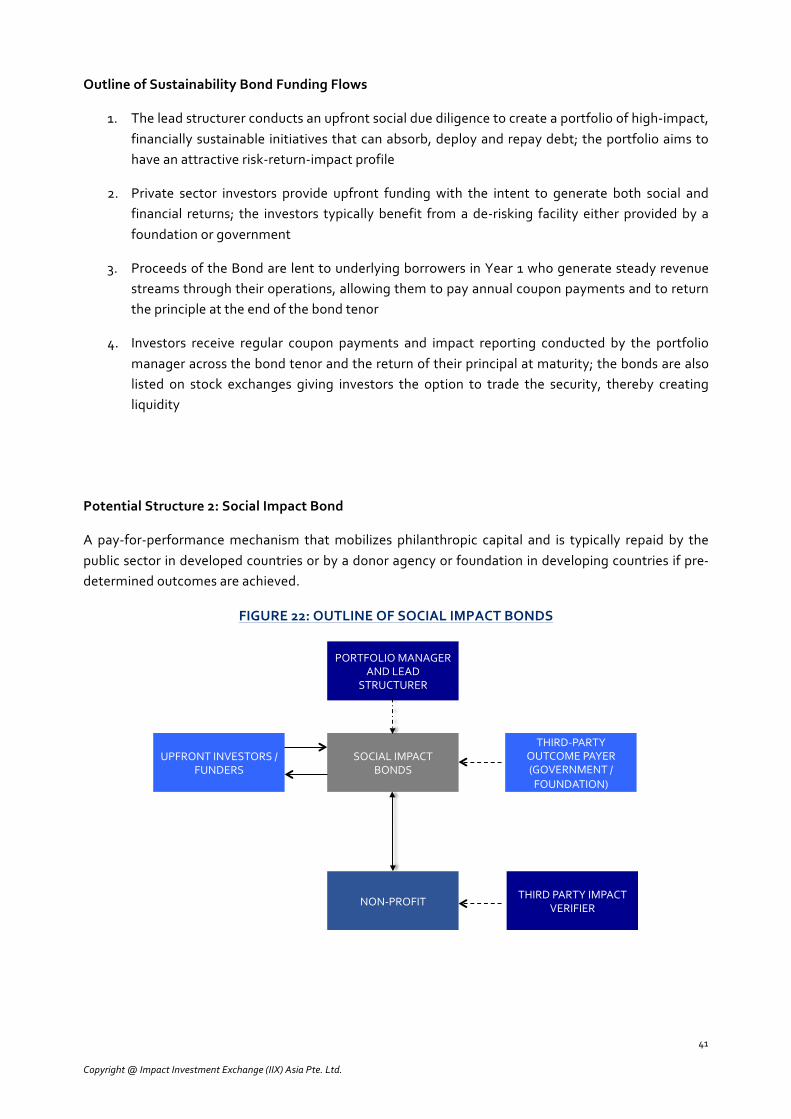
Copyright@ImpactInvestmentExchange(IIX)AsiaPte.Ltd.
41
OutlineofSustainabilityBondFundingFlows
1. Theleadstructurerconductsanupfrontsocialduediligencetocreateaportfolioofhigh-impact,financiallysustainable initiativesthatcanabsorb,deployandrepaydebt;theportfolioaimstohaveanattractiverisk-return-impactprofile
2. Private sector investors provide upfront funding with the intent to generate both social andfinancial returns; the investors typically benefit froma de-risking facility either providedby afoundationorgovernment
3. ProceedsoftheBondarelenttounderlyingborrowersinYear1whogeneratesteadyrevenuestreamsthroughtheiroperations,allowingthemtopayannualcouponpaymentsandtoreturntheprincipleattheendofthebondtenor
4. Investors receive regular coupon payments and impact reporting conducted by the portfoliomanageracrossthebondtenorandthereturnoftheirprincipalatmaturity;thebondsarealsolisted on stock exchanges giving investors the option to trade the security, thereby creatingliquidity
PotentialStructure2:SocialImpactBond
A pay-for-performancemechanism thatmobilizes philanthropic capital and is typically repaid by thepublicsectorindevelopedcountriesorbyadonoragencyorfoundationindevelopingcountriesifpre-determinedoutcomesareachieved.
FIGURE22:OUTLINEOFSOCIALIMPACTBONDS
SOCIALIMPACTBONDS
UPFRONTINVESTORS/FUNDERS
PORTFOLIOMANAGERANDLEAD
STRUCTURER
THIRD-PARTYOUTCOMEPAYER(GOVERNMENT/FOUNDATION)
NON-PROFITTHIRDPARTYIMPACT
VERIFIER
FIGURE35:OUTLINEOFSOCIAL/DEVELOPMENTIMPACTBONDS

Copyright@ImpactInvestmentExchange(IIX)AsiaPte.Ltd.
42
OutlineofSocialImpactBondFundingFlows
1. Theleadstructureridentifiesanon-profitthatisaddressingaparticularsocialprobleminacost-effectivemannerandassesseswhetherathird-partyoutcomepayer (government/foundation)will experienceclear cost savingsand therebybewilling to repay investors if the interventionsuccessfullyachievespre-determinedoutputs/outcomes
2. Investors/funders (typically philanthropic in nature although theoretically, this could includetraditionalprivatesectorinvestors)provideupfrontfundingto‘buy’thebonds
3. Proceedsofthebondareusedtoscalenon-profitinterventions
4. Athird-partyimpactverifierassesseswhetherpredeterminedoutputs/outcomesaremet
5. If the resultsarepositive the third-partyoutcomepayer repays theupfront investors/-funderstheirprincipalplusacoupon(theamountofthecouponmayvarybasedonthelevelofimpactachieved).
PotentialStructure3:HumanityBond
Ahybridoftheprevioustwostructures,theHumanityBondcombinestheabilitytouseblendedfinanceto bring in upfront funding from private sector actors similar to the Sustainability Bond whilemaintaining a commitment to achieving patient-centered outcomes and linking impact to capitalmobilizedsimilartoSocialImpactBonds.Thestructureisbestsuitedforproactivehealthcareinitiatives(particularlypreventionorservices the reducethedelayto treatment) that requireupfront fundingtoaddresshealthissuesatagreaterpaceandscale–thisallowshealthcareproviderstomagnifyimpactorsavemore lives todaywhile effectively lowering future costsoutlays.Themechanicsof theBondaredescribedbelow:
FIGURE23:OUTLINEOFTHEHUMANITYBOND
HUMANITY BOND PRIVATE SECTOR INVESTORS
BANKING PARTNERS LEGAL PARTNERS LEAD STRUCTURER
ULTIMATE PAYER (FOUNDATION)
NON-PROFIT OR IMPACT
ENTERPRISE
NON-PROFIT OR IMPACT
ENTERPRISE
NON-PROFIT OR IMPACT
ENTERPRISE
FIGURE37:HUMANITYBONDMECHANISM

Copyright@ImpactInvestmentExchange(IIX)AsiaPte.Ltd.
43
OutlineofHumanityBondFundingFlows1. The lead bond structurer (or portfolio manager) conducts an upfront social due diligence to
createaportfolioofpatient-centered,time-sensitiveinitiativesthatwouldbenefitfromupfrontfundingbyincreasingtheirimpacttodayandreducingcostoutlaysinthefuture.
2. Privatesectorimpactinvestorsprovideupfrontfundingwiththeintenttogeneratebothsocialandfinancialreturns.
3. ProceedsoftheBondareusedtoscaleupandacceleratetime-sensitive initiativesbythepre-selectednon-profitsorimpactenterprises.
4. Athird-party‘ultimatepayer’repaysthebondthroughpre-committedfundingstreams.Thisistypically an organization with vested interest in improving health outcomes for women (forinstance,afoundation,corporateCSRarmorgovernmentbody).
5. Investorsreceiveregularimpactreportingconductedbytheportfoliomanageracrossthebondtenorandthereturnoftheirprincipalatmaturity.
TheHumanityBond followsa similar structureas ‘GAVI’bonds. Issuedbytheinternationalfinancefacilityfor immunization(IFFIm),GAVIbondshaveraised+US$6.5billiontodatefromcapitalmarketinvestors upfront; the repayment is secured against committed pledges for future donations fromgovernmentssuchastheUK,Japan,andFrance.lxviWiththeproceeds,theGlobalAllianceforVaccinesandImmunizations(GAVI)hasbeenabletoconductlarge-scalevaccinationprograms,savingmorelivesthan could be achieved by spreading these programs over time. In this case, the governments arerepaying the bond which means these bonds are considered low-risk, low-return investment gradebonds.FitchRatings,Moody's InvestorServiceandStandard&Poor'shaveratedIFFImasAA/Aa1/AAandcouponsvarybasedoncurrency(average~2%).lxvii
FIGURE24:OUTLINEOFGAVIBONDMECHANISM
KeyInsight:CustomizationfortheWHB
IfthehumanitybondstructureistobeadaptedfortheWHB,itispossibletohaveafoundationortheCSRarmofacorporaterepaytheinvestorsinsteadofagovernment.Thebenefitofusingthisstructureinsteadofatraditionalgrantistheabilityforthefoundationtounlocklarge-scalecapitalinYear1andthenrepaythebondovertime.Thiswillhelpacceleratetheachievementofoutcomesandisbestsuitedto initiatives focused on prevention and early detection that typically are more cost effective thantreatment. It isalsoaneffectiveway tobringnewactors fromtheprivate sector into theU.S.healthcare equationwhichwill have a ripple effect of galvanizing anew set of stakeholders invested in thestrengtheningthehealthcaresystemandcommittedtoempoweringunderservedwomen.
ComparativeAnalysis
Basedonthefollowingcomparativeanalysisofthethreepotentialbondstructures,theHumanityBondisthemostsuitablefortheWomen’sHealthBondduetotheclearalignmentwithIIX’sthreeprinciples–patient-centered,proactiveandpositiveincentives.
IssuerofGAVIBonds
CapitalMarketInvestors
VaccinationPrograms
Beneficiaries Beneficiaries Beneficiaries
GAVIBonds
$$$
$$$$$$$$$
GovernmentDonors
FIGURE38:OUTLINEOFGAVIBONDMECHANISM

Copyright@ImpactInvestmentExchange(IIX)AsiaPte.Ltd.
44
TABLE9
HUMANITYBOND:PUTTINGWOMENFRONTANDCENTEROFCAPITALMARKETS
It is imperative to put women front and center of capital markets by developing more innovativefinancialinstrumentsthatgobeyondphilanthropyandtrulymakethecaseforinvestinginwomenforamore resilient, equitable future. It is also important to create a financial instrument that balances astrong commitment to outcomes with the ability to bring new private sector investors into thehealthcareequationintheUnitedStatestocomplement(notreplace)currentphilanthropicefforts.TheHumanityBondisdesignedtoachievethisinthreeways:• Bringing in new private sector capital to invest inwomen and creating liquidity:Social Impact
Bondsshifttheentirefinancialrisktoinvestors;ifoutcomesarenotmetbytheentityreceivingthecapital investors are not repaid – as such, this tends to attract philanthropic investors such asfoundations.TheHumanityBondisdesignedtogobeyondphilanthropicfundersbecausetheentirefinancialriskisnotshiftedtotheinvestors–investorsarepaidtheirprincipalbackregardlesstherebyunlockingnewsourcesofcapitalatamuchlargerscalefromtraditionalprivatesector investors(asseeninthecaseoftheGAVIBondsonPage43).Additionally,theHumanityBondcanbelistedonastock exchange, which will create liquidity for investors as well as transparency of results for allstakeholders involved. This is an important step towards having more gender-lens investmentproductsonthemarketthattrulybuildthecaseforinvestinginwomenintheUnitedStates.
• Incentivizing social outcomes and ensuring commitment to transparent, accountable results:The Humanity Bond rewards both investors and the entities (who are actually responsible for
COMPARATIVEANALYSISOFPOTENTIALBONDSTRUCTURES
SUSTAINABILITYBOND
KeyFeatures
-Effectivelyengagesmultiplestakeholders
-Aggregatesapoolofentitiestocreateanattractiveportfolio
-Idealforprivateinvestment
-Suitableformission-drivenfor-profitandfinanciallysustainablenon-profitentities
-Outcomesmeasuredpre-emptivelyandreportedacrossbondtenor
-Canbelistedonastockexchangetoallowforliquidity
Drawbacks
-Requiresfinanciallysustainableentitieswithclearborrowingneedsandrepaymentability
-CapitalmarketsintheUnitedStateshighlyefficientsowillnotbenefitlargefinanciallysustainablenon-profitsorsmallfor-profits
SOCIALIMPACTBOND
KeyFeatures
-Bringsinmultiplestakeholdersfrompublicandphilanthropicsector
-Linksoutcomesachievedtorepaymenttoinvestors
-Idealforunlockingphilanthropiccapital
-Suitablefornon-profitentitieswiththird-partyoutcomepayer
Drawbacks
-Shiftsentirefinancialrisktoinvestors;thiscreatesatendencytobringincapitalthatwouldhavebeenusedforphilanthropicpurposesanywayresultinginlimitedadditionalityandliquidity
-Relativelyexpensivetomeasureandverifyimpact;takesaretrospectiveapproachtomeasuingresults
HUMANITYBOND
KeyFeatures
-AlignmentwithPrinciple1"PatientCentered":Ensuresupfrontsocialduediligenceonunderlyingentitiestoassessandprojectpatient-centeredoutcomesandongoingreportingofimpactachievedtotherebyensuringtransparencyandaccountabilitytobothpatientsandinvestors
-AlignmentwithPrinciple2"Proactive":Idealforscalingpreventiveorearlydetectioninitiativesthatsavemorelivestodayandreducelargeroutlaysofcosttomorrow
-AlignmentwithPrinciple3"PositiveIncentives":Leveragesphilanthropiccapitaltounlocklarge-scaleinvestmentfromprivatesectoractorsthatwouldnothaveparticipatedotherwise,therebyachievingamultipliereffect.Doesnotshifttheentirefinancialriskofachievingsocialoutcomestoprivatesectorinvestors(i.e.doesnotusenegativeincentives

Copyright@ImpactInvestmentExchange(IIX)AsiaPte.Ltd.
45
creating outcomes)with a potential ‘upside’ or share in the coupon payment if the outcomes aremet.This isauniquewaytousepositive incentives toencourageacommitment tocreatingsocialoutcomesamongallpartiesinvolved(insteadofonlypenalizinginvestorsifoutcomesarenotmet).Additionally,theentitieswillgothroughasocialduediligenceusingtheImpactAssessmentToolkitdescribedinthenextsectionbeforereceivingtheinvestment–thiswillensureimpactcreatedwillbeassessedupfront,projectedinaforwardlookingwaywithcleartargetsandthenreportedonacrossthelifeofthebond(notjustattheendofthebondtenor)tocreatetransparency.
• Enhancingefficiency and supportingproactivehealthcare interventions:Finally,theprojectwillensurethatinitiativesthatbenefitmorefromfundingtodayratherthanfundingspreadovertimeareprioritized.Thiswillbeassessedbothfromacostperspective(consideringhowmuchwillbesavedbyspendingonprevention/earlydetectioninsteadofexclusivelyontreatment)andfromanimpactperspective(abilitytosavemorelivesandreducemorbidityormortalityifweinvesttodayinsteadofprovidinggrantsoveranumberofyears).Acceleratingaccess toupfront fundingwillalsohelp theentities receiving the capital to create internal efficiencies instead of constantly fundraising ordesigning new programs every year, which is a time, capital and resource intensive process thatdetractsorganizationsfromfocusingoncreatingpatient-centeredoutcomes.
NEXTSTEPS:WOMEN’SHEALTHBONDSERIES
Basedonfindingsfromthefeasibilitystudy,IIXwillissueaseriesofWomen’sHealthBondswithagoaltomobilize$100millionoverthenext~5years.Thiswillalloweachbondtofocusonasinglestatewhichwillreduceadministrativecostsandcomplexityofdealingwithnuancedregulatoryrequirementslinkedto financial securities that vary based on states. Smaller bond sizes also are alignedwith findings onfunding needs of individual entities that range from$1million to $20million. Each of the bondswillfocusononeofIIX’stargetconditions:women-specificcancers,maternalhealthorreproductiverights.Over time, bonds issued will evolve based on learnings from previous issuances to either scale upexistinginitiativesinnewcounties,bringsuccessfulinterventionstonewormorecomplexstates,widenthebreadthofissuesacrossthehealthcarecontinuumorintroduceothercomplexitiesinthestructureto magnify the impact on women or to makemore efficient use of the capital mobilized. The nextsectionincludesexamplesofpotentialinitiativesthatcouldbenefitfromaninnovativebond.
FIGURE25:5-YEARROADMAPFORWOMEN’SHEALTHBONDSERIES
ILLUSTRATIVECASESThe following section outlines two illustrative case of how the Humanity Bond mechanism can becustomizedfortheWomen’sHealthBond:
• Case1:AmericanCancerSocietyHPVVACandSustainabilityInitiative• Case2:TheMother’sCenteratColumbiaUniversityIrvingMedicalCenter
SummaryofPotentialThematicFocusAreas:
FIGURE39:FIVEYEARROADMAPFORWOMEN’SHEALTHBONDSERIES
PrenatalCare PostpartumCare ReproductiveJustice BreastCancer CervicalCancer
2018 2019 2020 2021 2022
• ConductFeasibilityStudy• CreateIAToolkit• GalvanizeEcosystemto
SupportPhase2• StructurethefirstWHBin
theseriesandplacewithinvestors
Continuedimpactassessment,monitoringandreportingtoinvestorsandotherstakeholdersusingIAToolkit
• RevisefeasibilitystudyforWHB2
• StructureWHB2andplacewithinvestors
• RevisefeasibilitystudyforWHB3
• StructureWHB3andplacewithinvestors
• RevisefeasibilitystudyforWHB4
• StructureWHB4andplacewithinvestors
• RevisefeasibilitystudyforWHB5
• StructureWHB5andplacewithinvestors

Copyright@ImpactInvestmentExchange(IIX)AsiaPte.Ltd.
46
Case1:AmericanCancerSocietyHPVVACandSustainabilityInitiativeACS InitiativeGoals:ACSproposestolaunchitsHPVVACprogramwiththedualgoalsto(i)eradicatecervical cancer inMNover the courseof 10yearsbasedon the successof itspilotproject; and (ii) tocreatesustainabilityinACS’sownoperations,enablingittoscaleupandreplicatetheprograminotherstatesgoingforward.PilotProjectOverview: TheACSHPVVACsPilotProjectaimed to increaseHPVvaccination rates foradolescents nationwide, with a focus on adolescents ages 11 to 12, through improved providerawareness and education and improved system-wide processes. The project expanded theAmericanCancerSociety’sexistingcancerpreventionandearlydetection interventionswithFederallyQualifiedHealthCareCenters (FQHCs)andCommunityHealthCenters (CHCs).Theprojectmodel centeredonAmericanCancerSociety(ACS)primarycarestafftoworkwithpartnerFQHCstowardincreasingHPVvaccination rates. All partner FQHCs were given an upfront grant along with technical assistance tosupport staff training, modify their electronic health records and implement four core interventionstrategies to increase HPV vaccination rates in their target communities: (i) client reminders; (ii)providerprompts;(iii)standingorders;and(iv)providerassessmentandfeedback.AlignmentwithIIXPrinciplestoAdvanceWomen’sHealthPatientCenteredCare–TheexpectedhealthoutcomesoftheACSinitiativeinclude:
TheNeedforUpfrontFundingtoAdoptaProactiveApproach:• Theprimarypurposeof the fundingwillbetosupportpreventionofcervicalcancerby improving
HPVvaccination initiationandcompletionratesandearly detectionbysupportingpapsmearsorreducing time to treatment. Part of the proceeds will be used to build awareness among rural,undocumentedandwomenofcolorthattendtobemorereactivewiththeirhealthcare.UpfrontfundingwillhelptoacceleratewidespreadadoptionoftheHPVvaccine inMNwiththebenefitofsavingmorelivestodayandreducinghigherfuturecostsassociatedwithtreatment.
• Additionally,thefundingwillhelpallowIIXtoprovideACSwithadvisorysupporttobuildtheirowninternal sustainability to roll out similar proactive health programs in a more cost-effective,sustainablemannergoing forward.Thisbenefitwill be to reduce thepressureof fundraisingandprogram management costs in the future, allowing ACS to deliver services in a more scalablemanner.
BondMechanismOutline:ThefollowingillustrativeexampleoutlineshowtheWomen’sHealthBondcanusetheHumanityBondstructuretosupporttheACSinitiative,usingpositiveincentivestomobilize$10millionofupfrontcapitalfromprivatesectorinvestors.
Responsiveness:Improvingtimelinessofcarebyincreasingcapacityof
FQHCtoeffectivelyscreenforcervicalcancer
Access:ImprovingproximityofHPVvaccinationservicesforruralwomen;
providingvaccinationservicesforadolescents(bothyounggirlsandyoungboys)
Efficiency:ImprovingACS’sownsustainabilityoverthelongrun;improvingFQHC
efficiencybyupdatingelectronichealthrecords,etc.Equity:Increasingawarenessofcervicalcancerrisksamongat-risksgroups,
prioritizingundocumentedwomen,womenofcolorandethnicminoritiesQuality:ReducingcervicalcancermortalityratesinMNbyincreasingHPV
vaccinationrates(bothinitiationandcompletion)Affordability:ProvidinggrantsupporttoFQHCtoensuretheservices/training
arenotcostprohibitiveorexclusivetohigherincomegroups
ACCESS
QUALITY AFFORDABILITY

Copyright@ImpactInvestmentExchange(IIX)AsiaPte.Ltd.
47
FIGURE26:ILLUSTRATIVEEXAMPLEOFWOMEN’SHEALTHBONDFORAMERICANCANCERSOCIETYHPVVACANDSUSTAINABILITYINITIATIVE
1. IIX designs mechanics of Women’s Health Bond for ACS and conducts upfront social due
diligencetoassesspatient-centeredoutcomesonunderservedwomenandestimateprojectedimpactthatcanbeachievedacrossthebondtenor;
2. Privatesectorimpactinvestorsprovideupfrontfundingof~$10millionbybuyingtheWomen’sHealthBond;
3. Proceedsof thebondaredistributedtoAmericanCancerSocietyto (i) rolloutcervicalcancerprograminMN;and(ii)tobuildinternalsustainabilityofACSoverthelifeoftheBond;
4. IIXverifiesandreportsimpactachievedonunderservedwomenacrossthelifeoftheBond;5. Athird-partyultimatepayer–potentiallytheCSRarmofacorporatewithoperationsinMN–
repaysthebondthroughpre-committedfundingstreamsattheendofthebondtenor;6. Investorsreceivethe$10millionprincipalatmaturity.Anycoupontobepaidtoinvestorswillbe
determined when developing the bond based on efficiencies created (improved patient-centeredoutcomes for the samecostor increasedcost-efficiencies)and timevalueofmoney(based on cost of proactive prevention and early detection are lower than cost of reactivetreatment).
AMERICANCANCERSOCIETY
Objective1:Reducingcervicalcancermortalityamong
underservedwomeninMN
Objective2:ImprovingACS’sownsustainabilityinthe
long-run
IMPACTINVESTMENT
EXCHANGE(IIX)
ULTIMATEPAYER
PRIVATESECTORINVESTORS
1
2
3
5
6
4
HUMANITYBOND
Ongoingimpactassessmentandreporting
Bonddesignandadvisory
Upfront$10millioninvestmentmobilizedinYear1
Repaymentofcapitalattheendofbondtenor(eg:Year5)
Fundusedtoscaleupproactive,time-sensitiveinitiatives

Copyright@ImpactInvestmentExchange(IIX)AsiaPte.Ltd.
48
Case2:TheMothersCenteratColumbiaUniversityIrvingMedicalCenter
Themajorityofwomen(estimatedat85%inNewYorkState)thatexperienceamaternaldeathhaveanidentifiable risk factor with an average number of 2.5 risk factors permaternal death. Non-Hispanicblackwomenare3-4xmorelikelytoexperienceamaternaldeaththanwhitewomennationally,and12xmorelikelyinNewYorkCity.
TheMothersCenteratColumbiaUniversityIrvingMedicalCenterisafirst-of-its-kindspacededicatedtomoms at increased risk for maternal morbidity and mortality. Over 25% of the patients seen byphysicians since2013havehadcardiacdiseaseduringpregnancy;over 18%haveaplacentaldisorderputtingthematsignificantriskofpostpartumhemorrhage;and10%haveaneurologicdisorder.Inthenewcenter, physicians fromacross 16 specialties at themedical centerwill be able to comeTOTHEPATIENTattheMothersCentersothatmomcanmoreeasilyaccessallofthecaresheneedsforasafepregnancyanddeliveryandherphysicianscanmoreeasilycollaborate.
The Center aims to improve maternal health outcomes through multidisciplinary collaboration ofspecialties,healthpromotionefforts,andfollow-upcareincluding:- Optimizedhealthatconceptionforwomenwithexistingmedicalorsurgicalconditions(well-
managedhypertension,diabetes,otherchronicdisease)- Reducedseveremorbidity(bloodtransfusionsandadmissionstoICU)andmortalitythroughrisk
identificationandmitigationaswellasregionalization- Postpartumfollowuptoensurethatwomenwhoexperiencedcomplicationsduringpregnancyhave
accesstothecaretheyneedtomitigatetheirfuturerisk(heartattack,stroke,diabetes).- Increasednutritionandmentalhealthsupportforourmomsfacingahigh-riskpregnancytoreduce
gestationaldiabetes,diabetes,obesity,andantepartum/postpartumdepression.
AlignmentwithIIXWomen’sHealthPrinciples:
PatientCenteredCare–Selectedhealthoutcomesoftheinitiativeinclude:
Responsiveness:Improvingcoordinationofcarethroughmultidisciplinary
careformomswithacuteorchronicmedicalandsurgicalconditions
Access:Improvingproximityandreduceddelaysbyprovidingmotherswith
accesstophysiciansfromacross16specialtiesatthemedicalcenter
Efficiency:Maintainingadatabaseandpopulateresearchconductedbythecenteraroundpregnancy-relatedriskfactors(diabetes,heart-disease,etc.)Equity:TargetbeneficiariesincludealargecommunityfromtheDominicanRepublic,andat-risk,underservedmothersfromacrossNewYorkQuality:Activepreconceptioncounselingandpost-partumfollow-upcare;reducedseveremorbidityandmortalitythroughriskidentification/mitigationAffordability:Supportslow-incomewomen(approximately50%ofpatients
servedhaveinsurancethroughMedicaid)
PatientCenteredOutcomesNYPMaternalHealthInitiative
ACCESS
QUALITY AFFORDABILITY

Copyright@ImpactInvestmentExchange(IIX)AsiaPte.Ltd.
49
TheNeedforUpfrontFundingtoAdoptaProactiveApproach:
UpfrontfundingwillallowtheMother’sCenterto:- Include supporting services (such as the focus on diabetes and heart disease) to mitigate risks
associatedwithpregnancy;- Reducehigherfuturecostsassociatedwithdelaystotreatmentorlackofadequateearlydetection;- Improve patient quality of life and reduce maternal morbidity and mortality by addressing
preventableissuesattheonset;and- Accelerate funding to the Center to reduce ongoing pressure of fundraising or dependency on
unreliableorinconsistentfunding.
BondMechanismOutline:ThefollowingillustrativeexampleoutlineshowtheWomen’sHealthBondcanusetheHumanityBondstructuretosupporttheinitiative,usingpositiveincentivestomobilizeupto~$5millionofupfrontcapitalfromprivatesectorinvestors.Foundationsplayingtheroleoftheultimatepayer inthepilottrancheoftheprogramcanhelpbuildatrackrecordoftangibleoutcomesandclearcost savings,making a case for public sector actors such as the state government to come in as theultimatepayerinfollowingissuancesoflargersize.
FIGURE27:ILLUSTRATIVEEXAMPLEOFWOMEN’SHEALTHBONDFORTHEMOTHER’SCENTER
1. IIXdesignsmechanicsofWomen’sHealthBondfortheMother’sCenterandconductsupfrontsocialduediligencetoassesspatient-centeredoutcomesonunderservedwomenandestimateprojectedimpactthatcanbeachievedacrossthebondtenor;
2. Privatesector impact investorsprovideupfrontfundingof~$5millionbybuyingtheWomen’sHealthBond;
3. Proceeds of the bond are distributed to theMother’s Center to scale up thematernal healthinitiativefocusedonsupportingunderservedwomeninthecommunity;
4. IIXverifiesandreportsimpactachievedonunderservedwomenacrossthelifeoftheBond;5. Athird-partyultimatepayer–potentiallyafoundationwithvestedinterestinwomen’shealthin
NY–repaysthebondthroughpre-committedfundingstreamsattheendofthebondtenor;6. Investorsreceivethefullprincipalbackatmaturity.Anycoupontobepaidtoinvestorswillbe
determined when developing the bond based on efficiencies created (improved patient-centeredoutcomesforthesamecostorincreasedcost-efficiencies)andtimevalueofmoney.
THEMOTHER’SCENTERATCOLUMBIAUNIVERSITYIRVINGMEDICALCENTER
BONDMANAGER(IIX)
ULTIMATEPAYER
PRIVATESECTORINVESTORS
1
2
3
5
6
4
HUMANITYBOND
Ongoingimpactassessmentandreporting
Bonddesignandadvisory
Upfront~$5millioninvestmentmobilizedinYear1
Repaymentofcapitalattheendofbondtenor(eg:Year5)
Fundusedtoscaleupproactive,time-sensitiveinitiatives


Copyright@ImpactInvestmentExchange(IIX)AsiaPte.Ltd.
51
WOMEN’SHEALTHIMPACTASSESSMENTTOOLKIT
TOOLKITOVERVIEW
Mission andObjectives:TheoverarchingmissionoftheWomenHealthImpactAssessmentToolkitistolinkinvestmentinhealthcareandthecreationofpatient-centeredoutcomeswithafocusonwomen.The toolkitwill alsocomplement IIX'sWomen'sHealthBondby facilitating theupfrontmeasurementandongoingmonitoringofresultsachieved.
Inparticular,theToolkithasthreekeyobjectives:
• To provide patients, particularly underserved women, with a voice in the health care system bydesigningatoolkitthatmeasureswhatmattersmosttothem
• To systematically enable health care providers or programs to transcend the boundaries ofmeasuringoutputs(orvolumeofcare)tomeasuringoutcomes(orvalueofcare)
• Tounlockcapitalfromprivatesectorinvestorsandscalehealthcareprogramsthatembracesixcoredimensionsofhealthoutcomes:access,affordability,efficiency,equity,qualityandresponsiveness.
Toolkit Design and Users: TheWomen’sHealth ImpactAssessmentToolkithasbeenbuiltbasedonIIX’s+9yeartrackrecordofconducting+130impactassessmentsacrosstheworldusingitsproprietaryframework – the IIX Sustainability PyramidTM (Figure 28). The IIX Sustainability PyramidTM, marriesimpactcreationwiththefinancialhealthoftheenterpriseandassesseschangestooutcomesachieved.This analytical approach balances the social science need to demonstrate effectiveness with incisiveanalysis to improve social initiatives. The objective of the framework is to provide a valuable tool inhelping enterprises understand their impact value chain and identifyingways to deepen their impactcreation by analyzing its relevance to intended beneficiaries, the efficiency of this undertaking, theeffectiveness of its approach, and the viability of its impact creation over time. Additionally, theframework is designed to equip investors or funders to make an educated investment or capitalallocationdecisionsthatcanleadtooptimizedimpactgeneration.
FIGURE28:IIXSUSTAINABILITYPYRAMIDTM
TheToolkithasbeencustomizedforwomen'shealthintheUnitedStatesbasedonfindingsfromIIX'sfeasibility study to design theWomen's Health Bond to ensure the Toolkit takes a patient-centered
HealthcareEnterprise
PatientCenteredOutcomes
Access,Affordability,QualityEfficiency,Equity,Responsiveness
PatientCenteredOutcomes
(Quality,Affordability,AccessEquity,Efficiency,Responsiveness)
FinancialViability
SustainableImpact(Systemic/National/GlobalGoals)
Mission
E
HealthcareEntity

Copyright@ImpactInvestmentExchange(IIX)AsiaPte.Ltd.
52
approachand isdesignedtomeasurehealthoutcomesthatmattermosttounderservedwomen.ThisapproachisfurtherdetailedintheIIXWomen’sHealthImpactAssessmentToolkit(guidelinesandexcelspreadsheet)thatwillbepublishedseparatelyandmadepubliclyavailablealongwiththisreport.
The Toolkit is comprised of 100 indicators: 60 generic indicators linked to access, affordability,efficiency, equity, quality and responsiveness and 40 condition-specific indicators linked to breastcancer,cervicalcancer,maternalhealthandreproductiverights–thefourfocusareasoftheWomen’sHealthBond.Sourcesfortheindicatorsincludeasystematicreviewandadaptationofmetricsfromthefollowing sources in addition to indicators shared by healthcare providers, practitioners and clinicsinterviewed:
• Agency for Healthcare Research andQuality(AHRQ)
• AmericanCancerSociety
• CentersforDiseaseControlandPrevention(CDC)
• CentersforMedicareandMedicaidServices(CMS)
• National Center for BiotechnologyInformation
• NationalQualityMetricsClearingHouse
• Network for Regional HealthcareImprovement
• Global Impact Investment Network (GIIN)IRISmetrics
• GuttmacherInstitute
• Healthcare Effectiveness Data andInformation Set (HEDIS) (under NationalCommitteeforQualityAssurance(NCQA))
• HenryJKaiserFamilyFoundation
• International Consortium of HealthOutcomesMeasurement(ICHOM)
• MaternalandChildHealthBureau
• OrchidHealthInternational
• Santilli&Vogenberg
• Saver&Martin
• TheCommonwealthFund
• TheLeapFrogGroup
• United Nations Sustainable DevelopmentGoals
• United States Agency for InternationalDevelopment (USAID) – MEASUREEvaluation
• US Department of Health and HumanSciences
• US National Library of Medicine (NationalInstitutesofHealth)
• WorldHealthOrganization(WHO)
EXPECTEDUSERSOFTHEIMPACTASSESSMENT(IA)TOOLKIT
IIXenvisionstheToolkittobeusedbytwomaingroups:
• Health care providers (demand-side of the capital equation): with the objective to improvepatient outcomes, increase healthworker productivity, enhance systemic efficiency, reduce costsandmobilizeadditionalcapital;and
• Funders or investors (supply-side of the capital equation): with the objective to benchmarkperformance,understandeffectiveness in termsofvalueofcare insteadofvolumeofcareand tomakemoreinformedcapitalallocationdecisions
KEYCHALLENGESIDENTIFIED
Sevenmainchallengesrelatedtomeasuringhealthoutcomeshavebeenidentifiedbasedoninterviewswithindustryexperts,healthcarepractitionersandpatientadvocates.Figure29providesabreakdownof the responses from interviews and surveys conducted as a part of the feasibility study (~60respondents).‘Lackofinclusionofpatientvoices/opinions'wasidentifiedasthemostsignificantbarrier,followedby‘focusonvolumeofcareinsteadofvalueofcare'and‘retrospectiveapproachtomeasuringresults'.

Copyright@ImpactInvestmentExchange(IIX)AsiaPte.Ltd.
53
FIGURE29:KEYCHALLENGESINMEASURINGIMPACTTHROUGHTHELENSOFIMPROVINGHEALTHCAREFORUNDERSERVEDWOMEN
WHBTOOLKITIMPACTMEASUREMENTAPPROACH
This section outlines the five-phase approach tomeasuring impact using the toolkit [Figure 30] thatseeks to address the aforementioned challenges by embedding the three IIX’s Women’s HealthPrinciples.
FIGURE30:FIVESTAGEPROCESSOFMEASURINGIMPACT
Phase1:DefiningScopeofUpfrontSocialDueDiligenceandStakeholderMapping
The first phase involves adopting a patient-centered approach from the onset of the impactassessmentinlinewithPrinciple1.Keyactivitiesinclude:
Lackofinclusionofpatientvoices/
opinions31%
Focusonvolumeorcareinsteadofvalue
ofcare24%
Retrospectiveapproachto
measuringresults17%
Limitedconsiderationof
socialdeterminantsofhealth
11%
Lowtransparencyandlow
accountability11%
Impactmeasurementviewedasacost-
center6%
Phase1 Phase2 Phase3 Phase4 Phase5
DefiningScopeofUpfrontSocialDueDiligenceandStakeholderMapping
UseIIXSustainabilityPyramidTMtoDetermineSocialValueGenerated
MobilizeCapitalBasedonEstimatedSocialReturnonInvestment
OngoingMeasurement,ReportingandAdaptiveManagement
ImpactVerificationwithPatientEngagementandSystematicReview
Principle1:Patient-Centered
Principle2:Proactive
Principle3:PositiveIncentives

Copyright@ImpactInvestmentExchange(IIX)AsiaPte.Ltd.
54
• DefiningScopeofSocialDueDiligence:Itisimportanttodeterminethescopeoftheassessmentupfront (whether the assessment is for a single entity looking tomobilize additional capital or agroupofentities,agroupofinitiativesunderalargerumbrellaorganizationoronaspecificprogramrun by a single organization), the impact goals or priorities of the user (whether it is aninvestor/funderortheorganizationitself)andtheresourcesavailabletoconducttheassessment(toensureifwhatisbeingproposedisfeasible).
• StakeholderMapping:Stakeholdersaredefinedaspeopleororganizationsthatexperiencechangeas a result of thework of the entity being analyzed. In the case of this Toolkit, IIX recommendsprioritizing underserved women as the key stakeholder, particularly for outcomes such asaffordability, quality, and equity. Secondary stakeholders could include the entity/health careprovider or enabler themselves particularly for outcomes such as efficiency, responsiveness oraccess. IIXrecommendsonlyincludingstakeholdersthatexperiencematerialchangeasaresultoftheactivitiesoftheenterprise.
Phase2:UseIIXSustainabilityPyramidTMtoDetermineSocialValueGenerated
The next step involves using the IIX Sustainability Pyramid to determine the social value generatedusingaproactiveapproachtoestimatingfuturevaluegeneratedbasedonretrospectiveanalysisoftheentityinlinewithPrinciple2.Keyactivitiesinclude:
• Followingthestep-by-stepinstructionsintheprevioussectiontousethePyramidtodeterminethesocial value generated by the entity being analyzed. This includes data collection to create abaselineofsocialvaluegeneratedandthenusingaproactive,forward-lookingapproachtomeasureandprojectthechangetheentitywillmakeiftheyreceiveadditionalfunding.
• Atthisstage,usersshouldalsoassesshowmuchoftheentity’simpactisattributedtopreventionorearly detection as opposed to treatment. A cost-benefit analysis can be conducted to determinewhethermorecapitalisrequiredtosupportmoreproactiveinitiativesthatwillcreatelargerimpactorsavemorelivestoday(duetoprevention)and/orpotentiallysavelargercostoutlaysinthefuture(associatedwithtreatment).
Phase3:MobilizeCapitalBasedonEstimatedSocialReturnonInvestment
Thethirdphase involvesmobilizingcapitalbasedontheestimatedSROIorsocialvaluegeneratedbythecompany.TheobjectiveistoensuretheentityhasapositiveincentivetomeasureitsimpactinlinewithPrinciple3.Inadditiontodecidinghowmuchcapitaltoallocatetowardstheentity,therearetwootherfactorsthat investors/fundersshouldconsiderduringthisphasetounderstandhowcatalyticthecapitalprovidedisandhoweffectivelyitisbeingusedtomagnifyimpact:
• Leverage:The leveragefactorreferstohowmuchadditionalcapital isunlockedasaresultofthefundingprovided.Forexample,ifupfrontgrantfundingof$1,000,000isprovidedbyafoundationtostructureaBondthatthenmobilizes$100,000,000theleveragefactoris10X(forevery$1ofgrantcapital,$10ofinvestmentcapitalismobilized).

Copyright@ImpactInvestmentExchange(IIX)AsiaPte.Ltd.
55
• Additionality:Additionality is definedas theabilityof the capital tobring innewactors into theequation thatwould not have otherwise participated or to use the capital to fund initiatives thatwould not otherwise move forward at the required pace and scale to achieve a certain level ofimpact.Forexample,followingonthesamecaseasabove,iftheinvestorsintheBondareprivatesector, traditional investors instead of the foundation arm of a large bank, then there is greater‘additionality’becausetheseactorswouldnothaveotherwisefundedwomen’shealthwhereasthefoundationwouldhavelikelyprovidedthesameamountoffundingforasimilarpurposeanyway.
Phase4:OngoingMeasurement,ReportingandAdaptiveManagement
This phase recognizes the dynamic nature of impact assessments and suggests conducting proactivemeasurement,reportingandmanagementinlinewithPrinciple2.Keyactivitiesinclude:
• OngoingMeasurementandReporting:IIXrecommendsconductingongoingimpactmeasurementonaregularbasis.Whilethisistypicallydoneonaquarterlybasis,thefrequencycanbeadjustedbytheuserbasedonresourcesavailableandtheexpectednatureofchangecreatedbytheentitybeinganalyzed.Thiswillallowtheusertoproactivelyidentifyanydeviationfromprojections.InthecaseofinnovativefinancialmechanismssuchasBonds,IIXrecommendsprovidinginvestors/funderswithsemi-annualupdatesontheimpactperformance;highlightinganydeviationsfromprojectionsandsubsequentchangetheSROIforecastedwillensuretransparencyofresults.
• AdaptiveManagement:IIXrecommendsproactivelyaddressinganydeviationsfromresultstotaketherecommendedcourseofactiontoensuretheultimateoutcomesarestillmet.Assuch,usersareencouragedtoworkwiththeentitytoadapttheapproachasrequiredbytracingbackthroughtheimpactvaluechaindescribedinthePyramid.Theobjectiveofthisexercise istounderstandwhichactivities are causing the deviations and identifying how they can be re-adjusted in a feasiblemannertoensurethefinalsocialvaluegeneratedismaintainedasmuchaspossible.
Phase5:ImpactVerificationwithPatientEngagementandSystematicReview
Thefinalphaseinvolvesre-integratingthepatient’svoiceintotheequationthroughasystematicimpactverificationandreviewprocessinlinewithPrinciple1.Keyactivitiesinclude:
• ImpactVerification:Asapartoftheongoingreportingprocess,IIXrecommendsgoingbeyondself-reportingby theentityandengagingdirectlywith theendbeneficiary. In thecaseof thisToolkit,thiswouldentailconductingstakeholderinterviewswithunderservedwomentodetermine,intheiropinion, howmuch change (positive, negative, intentional, unintentional) has been experienced.Going forward, IIX recommends harnessing the power of technology to gather information anddigitalizing the impact assessment process to include the voice of the patients, which will bothfacilitatereal-timedatasharingintheimmediatetermandreducecostsinthelongterm.
• Systematic Review: Finally, users are encouraged to conduct a systematic review of the impactassessmentwith the entity receiving the funding at the end of the funding period. Thiswill helpsharelessonslearned,understandwhatworkedandwhatdidn’tandcreatemorepatient-centeredprogramsgoingforwardthatfocusonthevalueofcareinsteadofthevolumeofcare.


Copyright@ImpactInvestmentExchange(IIX)AsiaPte.Ltd.
57
REFERENCES
iWilkerson,L.,Fung,C.,May,W.andElliott,D.(2018).AssessingPatient-centeredCare:OneApproachtoHealthDisparitiesEducation.[online]Availableat:https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2847105/iiCentersforDiseaseControlandPrevention.(2018).FromtheCDC-LeadingCausesofDeathbyRace/Ethnicity,Females-US.[online]Availableat:https://www.cdc.gov/women/lcod/2015/race-ethnicity/index.htmiiiGis.cdc.gov.(2018).USCSDataVisualizations.[online]Availableat:https://gis.cdc.gov/Cancer/USCS/DataViz.htmlivCentersforDiseaseControlandPrevention.(2018).CDCVitalsign:CervicalCancerisPreventable.[online]Availableat:https://www.cdc.gov/vitalsigns/cervical-cancer/index.htmlvCentersforDiseaseControlandPrevention.(2018).CancerPreventionandControl.[online]Availableat:https://www.cdc.gov/cancer/index.htmviCentersforDiseaseControlandPrevention.(2018).CancerPreventionandControl.[online]Availableat:https://www.cdc.gov/cancer/index.htmviiCentersforDiseaseControlandPrevention.(2018).CancerPreventionandControl.[online]Availableat:https://www.cdc.gov/cancer/index.htmviiiKevinM.Gorey,Ph.D.,M.S.W.,aNancyL.Richter,M.S.W.,bIsaacN.Luginaah,Ph.D.,cCarolineHamm,M.D.,dEricJ.Holowaty,M.D.,eGuangYongZou,Ph.D.,fandMadhanK.Balagurusamy,M.Sc.(2015).BreastCanceramongWomenLivinginPoverty.Availableat:https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4500640/ixKomenFoundation(2018).Comparingbreastcancerscreeningratesamongdifferentgroups.Availableat:https://ww5.komen.org/BreastCancer/DisparitiesInBreastCancerScreening.htmlxBreastCancerResearchFoundation(2018).Availableat:https://www.bcrf.org/disparity-map[Accessedon29May2018]xiAmericanCancerSocietyOfficialWebsite(2018).Availableat:https://www.cancer.org/research/currently-funded-cancer-research/grants-by-cancer-type.html[Accessedon29May2018]xiiNationalCancerInstitute(2018).StateCancerProfiles.Availableat:https://statecancerprofiles.cancer.gov/risk/index.php?topic=vaccine&risk=v71&sex=2&type=risk&sortVariableName=default&sortOrder=default#results[Accessedon29May2018]xiiiAmericanCancerSocietyOfficialWebsite(2018).Availableat:https://www.cancer.gov/about-nci/organization/crchd/cancer-health-disparities-fact-sheet#q2[Accessedon29May2018]xivAmericanCancerSocietyOfficialWebsite(2018).Availableat:https://www.cancer.gov/about-nci/organization/crchd/cancer-health-disparities-fact-sheet#q2[Accessedon29May2018]xvAmericanCancerSocietyOfficialWebsite(2018).Availableat:https://www.cancer.gov/about-nci/organization/crchd/cancer-health-disparities-fact-sheet#q2[Accessedon29May2018]xviAmericanCancerSocietyOfficialWebsite(2018).Availableat:https://www.cancer.gov/about-nci/organization/crchd/cancer-health-disparities-fact-sheet#q2[Accessedon29May2018]xviiMarianF.MacDorman,Ph.D.1,EugeneDeclercq,Ph.D.2,HowardCabral,Ph.D.3,andChristineMorton,Ph.D.4(2016).IstheUnitedStatesMaternalMortalityRateIncreasing?DisentanglingtrendsfrommeasurementissuesShorttitle:U.S.MaternalMortalityTrends.Availableat:https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5001799/pdf/nihms810951.pdfxviiiUNICEF(2018).UNICEFDataMaternalMortality.Availableat:http://data.unicef.org/topic/maternal-health/maternal-mortality/[Accessedon18April2018]xixNPRnews(2018).ForEveryWomanWhoDiesInChildbirthInTheU.S.,70MoreComeClose.[online]Availableat:http://www.wbur.org/npr/607782992/for-every-woman-who-dies-in-childbirth-in-the-u-s-70-more-come-close

Copyright@ImpactInvestmentExchange(IIX)AsiaPte.Ltd.
58
xxNPRnews(2018).ForEveryWomanWhoDiesInChildbirthInTheU.S.,70MoreComeClose.[online]Availableat:http://www.wbur.org/npr/607782992/for-every-woman-who-dies-in-childbirth-in-the-u-s-70-more-come-closexxiAnnals.org.(2018).Error|AmericanCollegeofPhysicians.[online]Availableat:http://annals.org/aim/fullarticle/2682682/women-s-health-policy-united-states-american-college-physicians-positionhttp://annals.org/aim/fullarticle/2682682/women-s-health-policy-united-states-american-college-physicians-positionxxiiReviewtoActionofficialwebsite(2018).Availableat:http://www.reviewtoaction.org/[Accessed17April2018].xxiiiNPRandProPublica(2017).Availableat:http://www.wbur.org/npr/528098789/u-s-has-the-worst-rate-of-maternal-deaths-in-the-developed-worldxxivProPublica(2017).Availableat:https://www.propublica.org/article/die-in-childbirth-maternal-death-rate-health-care-systemxxvCenterforDiseaseControlofficialwebsite(2018).Availableat:https://www.cdc.gov/[Accessed9April2018]xxviReviewtoActionofficialwebsite(2018).Availableat:http://www.reviewtoaction.org/[Accessed6April2018].xxviiReproductiveHealthInvestorAlliance(2017).USReproductiveHealthInvestmentCase.Availableonline:https://tarahealthfoundation.org/wp-content/uploads/2017/03/RHIA_InvestmentCase.pdf[Accessed6April2018].xxviiiReproductiveHealthInvestorAlliance(2017).USReproductiveHealthInvestmentCase.Availableonline:https://tarahealthfoundation.org/wp-content/uploads/2017/03/RHIA_InvestmentCase.pdf[Accessed6April2018].xxixReproductiveHealthInvestorAlliance(2017).USReproductiveHealthInvestmentCase.Availableonline:https://tarahealthfoundation.org/wp-content/uploads/2017/03/RHIA_InvestmentCase.pdf[Accessed6April2018].xxxReproductiveHealthInvestorAlliance(2017).USReproductiveHealthInvestmentCase.Availableonline:https://tarahealthfoundation.org/wp-content/uploads/2017/03/RHIA_InvestmentCase.pdf[Accessed6April2018].xxxiOfficeofPopulationAffairs(2017).TitleXFamilyPlanningAnnualReport2016Summary.Availableonline:https://www.hhs.gov/opa/sites/default/files/OPA-FPAR-Infographic.pdfxxxiiOfficeofPopulationAffairs(2017).TitleXFamilyPlanningAnnualReport2016Summary.Availableonline:https://www.hhs.gov/opa/sites/default/files/OPA-FPAR-Infographic.pdfxxxiiiOfficeofPopulationAffairs(2017).TitleXFamilyPlanningAnnualReport2016Summary.Availableonline:https://www.hhs.gov/opa/sites/default/files/OPA-FPAR-Infographic.pdfxxxivOfficeofPopulationAffairs(2017).TitleXFamilyPlanningAnnualReport2016Summary.Availableonline:https://www.hhs.gov/opa/sites/default/files/OPA-FPAR-Infographic.pdfxxxvHenryJKaiserFamilyFoundation(2017).Women’sHealthInsuranceCoverage.Availableat:https://www.kff.org/womens-health-policy/fact-sheet/womens-health-insurance-coverage-fact-sheet/xxxviAmericanCancerSocietyOfficialWebsite(2018).Availableat:https://www.cancer.gov/about-cancer/causes-prevention/risk/infectious-agents/hpv-vaccine-fact-sheet[Accessedon29May2018]xxxviiAmericanCancerSocietyOfficialWebsite(2018).Availableat:https://www.cancer.gov/about-cancer/causes-prevention/risk/infectious-agents/hpv-vaccine-fact-sheet[Accessedon29May2018]xxxviiiKevinC.Oeffinger,MD,ElizabethT.H.Fontham,MPH,DrPH,RuthEtzioni,PhD,AbbeHerzig,PhD,JamesS.Michaelson,PhD,Ya-ChenTinaShih,PhD,LouiseC.Walter,MD,TimothyR.Church,PhD,ChristopherR.Flowers,MD,MS,SamuelJ.LaMonte,MD,AndrewM.D.Wolf,MD,CarolDeSantis,MPH,JoannieLortet-Tieulent,MSc,KimberlyAndrews,DeanaManassaram-Baptiste,PhD,DebbieSaslow,PhD,RobertA.Smith,PhD,OtisW.Brawley,MD,andRichardWender,MD(2015).BreastCancerScreeningforWomenatAverageRisk:2015GuidelineUpdatefromtheAmericanCancerSociety.Availableat:https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4831582/xxxixHardingCenterforRiskLiteracy,2014xlHardingCenterforRiskLiteracy,2014xliAWorldWithoutCancer,2014

Copyright@ImpactInvestmentExchange(IIX)AsiaPte.Ltd.
59
xliiMaternalMortalityReviewandReviewtoAction–supportedbyMerckforMothers(2017).BuildingU.S.CapacitytoReviewandPreventMaternalDeaths.Availableat:https://www.cdcfoundation.org/sites/default/files/upload/pdf/MMRIAReport.pdfxliiiAnnalsofInternalMedicine-HilaryDaniel,BS;ShariM.Erickson,MPH;SueS.Bornstein,MD;fortheHealthandPublicPolicyCommitteeoftheAmericanCollegeofPhysicians(2018).Women'sHealthPolicyintheUnitedStates:AnAmericanCollegeofPhysiciansPositionPaper.Availableat:http://annals.org/aim/fullarticle/2682682/women-s-health-policy-united-states-american-college-physicians-positionxlivAnnalsofInternalMedicine-HilaryDaniel,BS;ShariM.Erickson,MPH;SueS.Bornstein,MD;fortheHealthandPublicPolicyCommitteeoftheAmericanCollegeofPhysicians(2018).Women'sHealthPolicyintheUnitedStates:AnAmericanCollegeofPhysiciansPositionPaper.Availableat:http://annals.org/aim/fullarticle/2682682/women-s-health-policy-united-states-american-college-physicians-positionxlvReproductiveHealthInvestorAlliance(2017).USReproductiveHealthInvestmentCase.Availableonline:https://tarahealthfoundation.org/wp-content/uploads/2017/03/RHIA_InvestmentCase.pdf[Accessed6April2018].xlviJamesW.Henderson,Ph.D.(1994).TheCostEffectivenessofPrenatalCareAvailableat:https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4193436/xlviiArabellaAdvisors(2013).HealthPhilanthropy.Availableat:http://www.gih.org/files/FileDownloads/Health_Philanthropy_New_Players_and_Approaches_November_2013.pdfxlviiiTheCommonWealthFund–SaraR.Collins(2017).WhatArethePotentialEffectsoftheGraham-CassidyACARepeal-and-ReplaceBill?PastEstimatesProvideSomeClues.Availableat:http://www.commonwealthfund.org/publications/blog/2017/sep/potential-effects-of-graham-cassidyxlixFoundationCenterOfficialWebsite(2018).Availableat:http://data.foundationcenter.org/#/fc1000/subject:health/all/total/list/2012[Accessedon10April2018]lFoundationCenterOfficialWebsite(2018).Availableat:http://data.foundationcenter.org/#/fc1000/population_group:women_girls/nationwide/total/trends:amount/2012[Accessedon10April2018]liGlobalImpactInvestingNetwork(2018).AnnualImpactInvestingSurvey.Availableat:https://thegiin.org/assets/2018_GIIN_Annual_Impact_Investor_Survey_webfile.pdfliiGlobalImpactInvestingNetwork(2018).AnnualImpactInvestingSurvey.Availableat:https://thegiin.org/assets/2018_GIIN_Annual_Impact_Investor_Survey_webfile.pdfliiiGlobalImpactInvestingNetwork(2018).AnnualImpactInvestingSurvey.Availableat:https://thegiin.org/assets/2018_GIIN_Annual_Impact_Investor_Survey_webfile.pdflivBostonConsultingGroup(2018).Availableat:https://www.lgbco.com/sites/default/files/2018-07/Wealth%20Briefing%2025.07.18.pdflvBostonConsultingGroup(2018).Availableat:https://www.lgbco.com/sites/default/files/2018-07/Wealth%20Briefing%2025.07.18.pdflviBostonConsultingGroup(2018).Availableat:https://www.lgbco.com/sites/default/files/2018-07/Wealth%20Briefing%2025.07.18.pdflviiUSCensusReports2017,KaiserFamilyFoundationStateProfilesforWomen’sHealth,Statistica,PewResearchCenter:(Availableathttp://www.pewhispanic.org/interactives/unauthorized-immigrants/)[AccessedonApril112018]

Copyright@ImpactInvestmentExchange(IIX)AsiaPte.Ltd.
60
lviiiUSCensusReports2017,KaiserFamilyFoundationStateProfilesforWomen’sHealth,Statistica,PewResearchCenter:(Availableat:http://www.pewhispanic.org/interactives/unauthorized-immigrants/)[AccessedonApril112018]lixAvailableat:https://imgur.com/cQWZfwA[AccessedonJune122018]lxReproductiveHealthInvestorAlliance(2017).USReproductiveHealthInvestmentCase.Availableonline:https://tarahealthfoundation.org/wp-content/uploads/2017/03/RHIA_InvestmentCase.pdf[Accessed6April2018].lxiReproductiveHealthInvestorAlliance(2017).USReproductiveHealthInvestmentCase.Availableonline:https://tarahealthfoundation.org/wp-content/uploads/2017/03/RHIA_InvestmentCase.pdf[Accessed6April2018].lxiiMNCommunityMeasurement(2014).2014HealthEquityofCareReport.Availableat:http://mncm.org/wp-content/uploads/2015/01/2014-MN-Community-Measurement-Health-Equity-of-Care-Report.pdflxiiiMNCommunityMeasurement(2014).2014HealthEquityofCareReport.Availableat:http://mncm.org/wp-content/uploads/2015/01/2014-MN-Community-Measurement-Health-Equity-of-Care-Report.pdflxivMNCommunityMeasurement(2014).2014HealthEquityofCareReport.Availableat:http://mncm.org/wp-content/uploads/2015/01/2014-MN-Community-Measurement-Health-Equity-of-Care-Report.pdflxvMNCommunityMeasurement(2014).2014HealthEquityofCareReport.Availableat:http://mncm.org/wp-content/uploads/2015/01/2014-MN-Community-Measurement-Health-Equity-of-Care-Report.pdflxviTheVaccinationAllianceOfficialWebsite(2018).Availableat:https://www.gavi.org/funding/iffim/[AccessedonMay292018]lxviiTheVaccinationAllianceOfficialWebsite(2018).Availableat:https://www.gavi.org/funding/iffim/[AccessedonMay292018]


















