Partners Demonstration Project - HIV self testing update - Feb 2015
Upload
hivstorgCategory
view
3download
1
PARTNERS DEMONSTRATION PROJECT
Acceptability and Uptake ofHIV-1 Self-Testing among Individuals using
Pre-Exposure Prophylaxis in KenyaAn ancillary study to the Partners Demonstration Project
Jared Baeten MD PhDUniversity of Washington
Bill & Melinda Gates Foundation Meeting on Self-TestingFebruary 2015

Outline
• Goals and status of the Partners Demonstration Project
• Implementation and preliminary findings from the HIV-1 self-testing ancillary study within the Partners Demonstration Project

Partners Demonstration Project
• The Partners Demonstration Project is an open-label, prospective interventional study of ART and PrEP for HIV prevention among heterosexual HIV serodiscordant couples
• The project is being conducted at 4 clinical care sites: Kisumu & Thika in Kenya and Kabwohe & Kampala in Uganda
• The overall goal is to evaluate, using implementation science methods, a scalable delivery system for PrEP and ART for HIV prevention in couples

PrEP as a bridge to ART • For couples initiating ART at enrollment, PrEP is offered
through 6 months, then stopped:
• For couples in which the infected partner delays or declines ART, PrEP is continued until 6 months after ART initiation:
• This strategy is supported by mathematical modeling as potentially highly effective and cost-effective (Hallett et al. PLoS Med 2011; Ying et al. CROI 2015, abstract #1106)
ART
PrEP Stop
ART
PrEP Stop
ART delayed……………..

Results: Participant Characteristics• Between Nov 2012 and Aug 2014, 1013 couples were
enrolled. Characteristics are consistent with elevated HIV risk: Characteristic % or median (IQR)
Gender, HIV- partner 33% female / 67% male
Age Median 30 years (IQR 26-36), with 20% <25 years
No children with study partner 56%
Unprotected sex in the prior month 65%
CD4 count, HIV+ partner Median 436 (IQR 272-638),with 41% >500 cells/µL
Plasma HIV RNA, HIV+ partner Median 37,095 (IQR 7058-104,462),with 41% >50,000 copies/mL

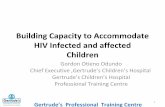
HIV incidence
0
1
2
3
4
5
6
EXPECTED
• Based on the risk profile of enrolled couples, nearly 40 HIV infections are expected to date. However, only 2 incident HIV transmissions have been observed, a 96% reduction.
N=39.7 infectionsincidence = 5.2
(95% CI 3.7-6.9)
OBSERVED
N=2 infectionsincidence = 0.2
(95% CI 0.0-0.9)
IRR observed vs. expected = 0.04
(95% CI 0.01-0.19)or a
96% reduction (95% CI 81-99%)
P<0.0001

HIV-1 self-testing in a PrEPdemonstration project: rationale
• HIV-1 testing is integral to PrEP delivery – for persons who acquire HIV-1 while on PrEP, prompt testing and discontinuation of PrEP may reduce the risk of antiretroviral resistance
• Self-testing for HIV-1 for persons on PrEP could provide an efficient method to identify new infections between in-clinic tests and reduce PrEP exposure among persons who acquire HIV-1 in spite of PrEP without increasing PrEP clinical delivery costs and participant burden– Plus, frequent HIV-1 testing itself may have behavioral benefits
in terms of risk reduction and PrEP adherence

HIV-1 self-testing in a PrEPdemonstration project: aims
1. Evaluate acceptability and uptake of HIV-1 self-testing among HIV-1 uninfected persons in HIV-1 serodiscordant relationships receiving PrEP.
2. Evaluate the performance of HIV-1 self-testing when used by HIV-1 uninfected persons receiving PrEP.
3. Explore the barriers and challenges to self-testing among HIV-1 uninfected persons receiving PrEP.

HIV-1 self-testing in a PrEPdemonstration project: setting
• Setting: Thika, Kenya site (a couples-oriented HIV prevention, care, and research center), conducting the Partners Demonstration Project

HIV-1 self-testing in a PrEPdemonstration project: mechanics
• HIV-1 self-testing is integrated with Partners Demonstration Project: – scheduled clinic visits occur quarterly and OraQuick self-
testing has been inserted between clinic visits to increase frequency of HIV-1 testing:
• Partners Demonstration Project – Months 1, 3, 6, 9, 12, 15, 18, 21, 24 after enrollment
• HIV-1 self-testing: – Months 2, 4, 5, 7, 8, 10, 11, 13, 14, 16, 17, 19, 20, 22, 23 after
enrollment
• Result: HIV-1 testing can occur monthly (as it was in the clinical trials of PrEP), without monthly clinic visits

HIV-1 self-testing in a PrEPdemonstration project: key elements
• Key elements of implementation: – informed consent– training in test execution
and observed episode of testing
– pictorial information sheet – 24 hour helpline for
counseling and questions http://www.oraquick.com/What-is-OraQuick/How-Oral-Testing-Works
Swabbing procedure Interpretation of results
Non-reactive
Reactive

HIV-1 self-testing in a PrEPdemonstration project: data collection
• Number of tests performed
• Ease of performing the test
• Confidentiality of test results
• Sharing of self test kits
• Use of the 24 hour helpline
• Preference oral versus finger prick for testing
• Preference self testing versus provider testing

HIV-1 self-testing in a PrEPdemonstration project: results
HIV uninfected partners at Thika siteN=332
self‐testing study initiated November 2013
Enrolled – 220 Ineligible – 88 Pending – 24
• Not on PrEP• Declined PrEP• Stopped PrEP• Seroconverter• Pregnant• Declined self‐testing =5
Reasons for declining self-testing: not wanting to do testing alone, already goes for monthly rapid testing at VCT

Results: Follow-up Data
Description NTotal number of self tests dispensed 1190Proportion of expected tests reported as used 96 %
Ngure et al R4P Oct 2014 and updated to January 2015

Results : Test Performance
• 79.6% of participants report conducting HIVST at least once & 93.0% reported using the kit was easy.
• 19.2% reported that they self-test when they opened a new bottle of PrEP—but most did self-testing at a different time.
– Often to have partner present (or not present), generally same day or within a few days
• 56.7% self-tested alone and 41.1% study partner was present
• 52.5% shared their HIVST results with study partner, while 44.0% did not share the results with anyone.
• 95% of participants did not use the help line

Results: Qualitative• Quotes from 4 focus group discussions conducted so far:
– Reduced anxiety• “Every day, every time thinking to yourself, “How will it be when I go back there
[clinic]? When you test yourself, you know your status, you relax”
– Testing alone versus with others: • “Sometimes I call my husband. Like the last time I tested, I called my husband
and told him “Come you see mine is okay until now “.• “Like me, I hide myself… (All the participants laugh) I go to the bedroom.”
– Remembering to test: • “I put a reminder on my phone.” • “What makes me remember is putting it together with these medication
(Truvada).”

Results: Counselor Observations• Self testing is empowering
• Majority report that the self testing is easy to perform and does not require the presence of the health provider.
• The new technology is exciting, real time and efficient as it enables them to learn their status in their homes and at their own convenience.
• A number of clients report getting support from their partners during the procedure.
• It is the most preferred choice for testing in that there is no blood sample required to perform the test.
• It reduces anxiety associated with 3-monthly waiting for testing.

HIV-1 self-testing in a PrEPdemonstration project: summary
• HIV-1 self-testing appears to be an acceptable and feasible adjunct to PrEPdelivery among high-risk Kenyan HIV-1 serodiscordant couples
• Continuing work will provide increased sample size, costing analyses, continued exploration of positive/negative experiences with testing

The Partners Demonstration Project is made possible by the United States National Institutes of Health, the Bill and Melinda Gates Foundation, and the generoussupport of the American people through the United States Agency for International Development. The contents are the responsibility of the University of Washington andstudy partners and do not necessarily reflect the views of any of the study sponsors or the United States Government.
Investigative Team– University of Washington: Jared Baeten (protocol chair), Connie Celum (protocol chair), Renee Heffron
(project director), Deborah Donnell (statistician), Ruanne Barnabas, Justin Brantley, Benjamin Browning-Roberts, Lynn Harr, Harald Haugen, Lara Kidoguchi, Toni Maddox, Susan Morrison, Jennifer Morton, Kelly Moutsos, Andrew Mujugira, Caitlin Scoville, Bettina Shell-Duncan, Kathy Thomas, Kerry Thomson
– Kabwohe, Uganda (KCRC): Steven Asiimwe, Edna Tindimwebwa, Elioda Tumwesigye– Kampala, Uganda (Makerere University): Elly Katabira, Nulu Bulya– Kisumu, Kenya (KEMRI): Elizabeth Bukusi, Josephine Odoyo– Thika, Kenya (KEMRI/JKUAT): Nelly Mugo, Kenneth Ngure– MGH/Harvard University: Jessica Haberer, David Bangsberg, Norma Ware, Monique Wyatt – Johns Hopkins University: Craig Hendrix, Mark Marzinke– Fred Hutchinson Cancer Research Center: Dara Lehman– DF/Net Research (data management); Gilead Sciences (PrEP donation)
Project participantsFunders
– NIH (R01MH095507, R01MH100940, R01MH101027, R21AI104449, R21TW009908, K99/R00HD076679)– Bill & Melinda Gates Foundation (OPP1056051, OPP47674)– USAID (AID-OAA-A-12-00023)
Partners Demonstration Project