
Part 2 GCMAS symp Research & Motion Anal Ounpuu-Pierz hand ... · Pathomechanics of...
15
Motion analysis in understanding gait pathology, AACPDM 2013 Part 2 -1 Research Using Motion Analysis: Impact in Understanding Impact in Understanding Movement Pathology Sylvia Õunpuu, MSc Kristan Pierz, MD Center for Motion Analysis Connecticut Children’s Medical Center Introduction • Motion analysis techniques have been used to understand typical and pathological movement since the 1800’s • Computerized motion analysis moved this tool • Computerized motion analysis moved this tool from the research realm into routine clinical services in the 1980’s • The resulting documentation of movement has expanded to a wide variety of gait pathologies Outline • Review how motion analysis has improved our understanding of movement pathology that impacts children’s gait Charcot Marie Tooth – Charcot-Marie-Tooth – Myelomeningocele – Cerebral palsy • Natural progression • Prevalence of gait deviations • Classification/patterns • Skeletal modeling Objectives • At the end of this section, participants will be able to: – Describe how motion analysis has improved our understanding of the pathomechanics in a number understanding of the pathomechanics in a number of gait pathologies • most commonly inherited neurological Charcot-Marie-Tooth CMT most commonly inherited neurological disorder = de-myelination of large peripheral nerves • CMT is characterized by: • distal muscle weakness and imbalance • foot and ankle deformities • associated gait implications • impairment progression at varying rates Textbook gait description: • foot drop (excessive equinus) in swing phase • steppage (hyper- steppage (hyper flexion of knee and hip in swing) • circumduction and pelvic hiking in swing (Fenton, JOPA 1984) (Morrisy, Pediatric Orthopedics) (Vinci, Archives of Physical Medicine & Rehab 2002)
Transcript of Part 2 GCMAS symp Research & Motion Anal Ounpuu-Pierz hand ... · Pathomechanics of...
Motion analysis in understanding gait pathology, AACPDM 2013 Part 2 -1
Research Using Motion Analysis: Impact in UnderstandingImpact in Understanding
Movement PathologySylvia Õunpuu, MScKristan Pierz, MD
Center for Motion AnalysisConnecticut Children’s Medical Center
Introduction
• Motion analysis techniques have been used to understand typical and pathological movement since the 1800’s
• Computerized motion analysis moved this tool• Computerized motion analysis moved this tool from the research realm into routine clinical services in the 1980’s
• The resulting documentation of movement has expanded to a wide variety of gait pathologies
Outline
• Review how motion analysis has improved our understanding of movement pathology that impacts children’s gait
Charcot Marie Tooth– Charcot-Marie-Tooth– Myelomeningocele– Cerebral palsy
• Natural progression• Prevalence of gait deviations• Classification/patterns• Skeletal modeling
Objectives
• At the end of this section, participants will be able to:– Describe how motion analysis has improved our
understanding of the pathomechanics in a numberunderstanding of the pathomechanics in a number of gait pathologies
• most commonly inherited neurological
Charcot-Marie-ToothCMT
most commonly inherited neurological disorder = de-myelination of large peripheral nerves
• CMT is characterized by: • distal muscle weakness and imbalance• foot and ankle deformities• associated gait implications • impairment progression at varying rates
Textbook gait description:• foot drop (excessive
equinus) in swing phase
• steppage (hyper-steppage (hyperflexion of knee and hip in swing)
• circumduction and pelvic hiking in swing
(Fenton, JOPA 1984)(Morrisy, Pediatric Orthopedics)(Vinci, Archives of Physical Medicine & Rehab 2002)
Motion analysis in understanding gait pathology, AACPDM 2013 Part 2 -2
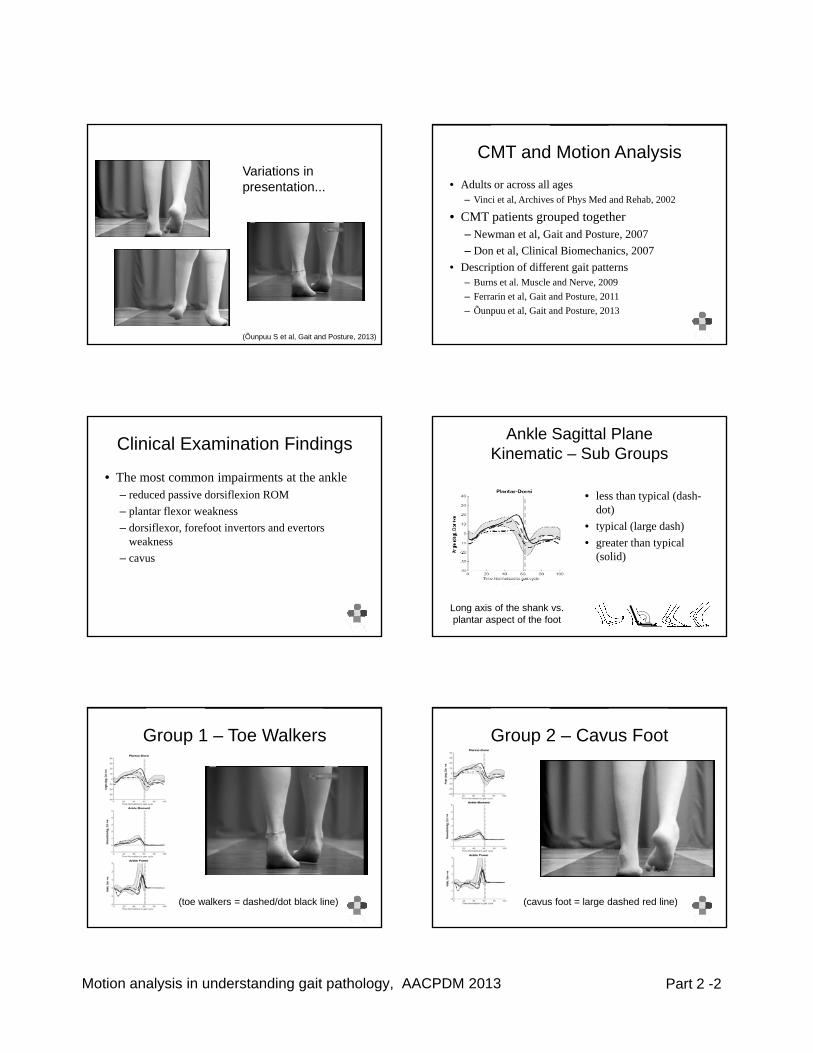
Variations in presentation...
(Õunpuu S et al, Gait and Posture, 2013)
CMT and Motion Analysis
• Adults or across all ages– Vinci et al, Archives of Phys Med and Rehab, 2002
• CMT patients grouped together– Newman et al Gait and Posture 2007– Newman et al, Gait and Posture, 2007– Don et al, Clinical Biomechanics, 2007
• Description of different gait patterns– Burns et al. Muscle and Nerve, 2009– Ferrarin et al, Gait and Posture, 2011– Õunpuu et al, Gait and Posture, 2013
Clinical Examination Findings
• The most common impairments at the ankle – reduced passive dorsiflexion ROM – plantar flexor weakness
dorsifle or forefoot in ertors and e ertors– dorsiflexor, forefoot invertors and evertors weakness
– cavus
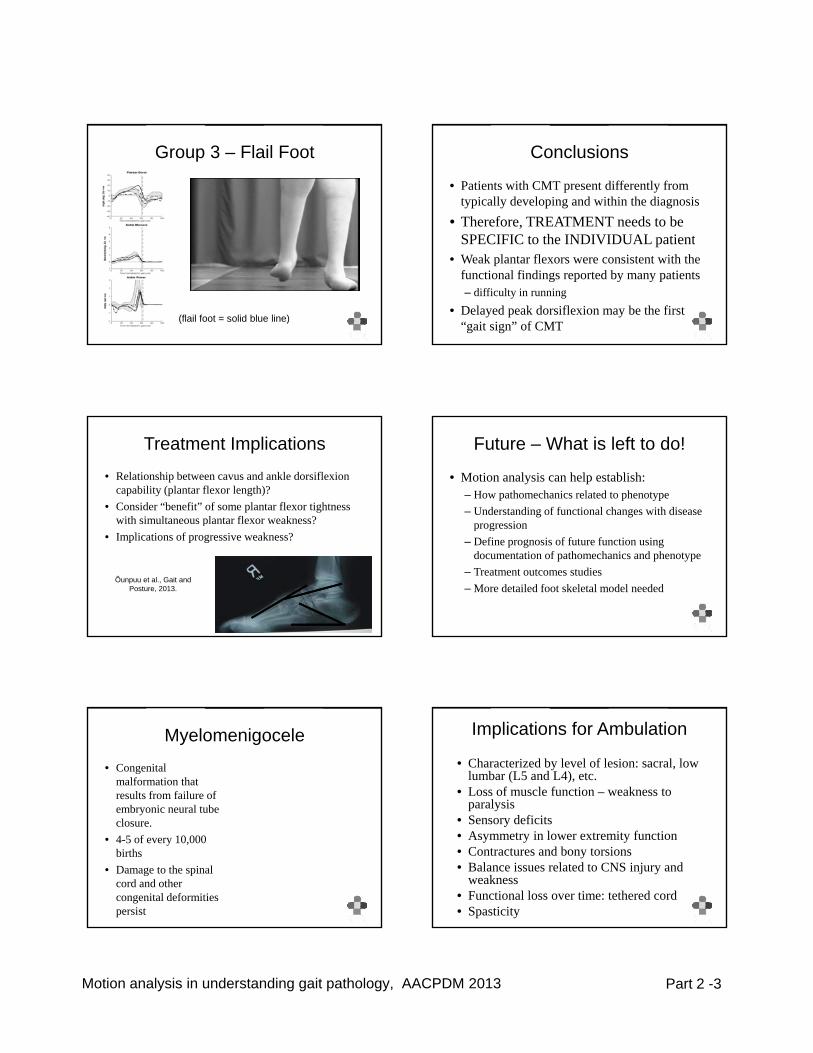
Ankle Sagittal Plane Kinematic – Sub Groups
• less than typical (dash-dot)
• typical (large dash)• typical (large dash) • greater than typical
(solid)
Long axis of the shank vs. plantar aspect of the foot
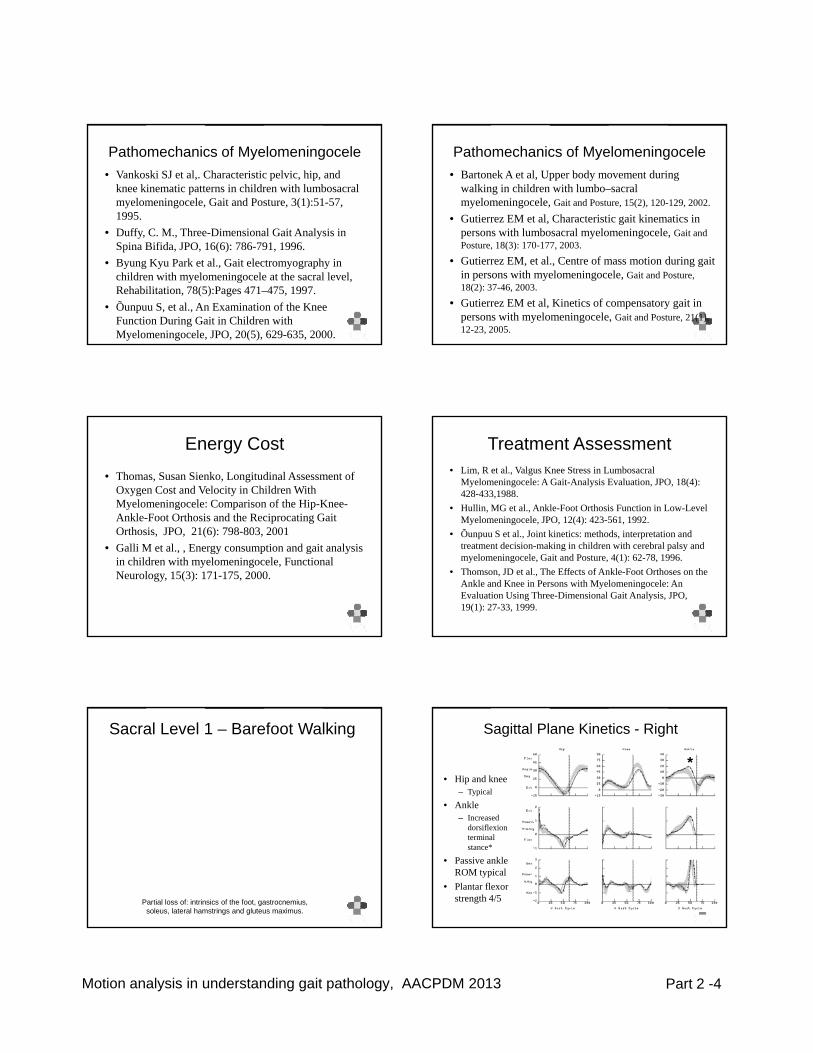
Group 1 – Toe Walkers
(toe walkers = dashed/dot black line)
Group 2 – Cavus Foot
(cavus foot = large dashed red line)
Motion analysis in understanding gait pathology, AACPDM 2013 Part 2 -3
Group 3 – Flail Foot
(flail foot = solid blue line)
Conclusions
• Patients with CMT present differently from typically developing and within the diagnosis
• Therefore, TREATMENT needs to be SPECIFIC h INDIVIDUAL iSPECIFIC to the INDIVIDUAL patient
• Weak plantar flexors were consistent with the functional findings reported by many patients – difficulty in running
• Delayed peak dorsiflexion may be the first “gait sign” of CMT
Treatment Implications
• Relationship between cavus and ankle dorsiflexioncapability (plantar flexor length)?
• Consider “benefit” of some plantar flexor tightness with simultaneous plantar flexor weakness?p
• Implications of progressive weakness?
Õunpuu et al., Gait and Posture, 2013.
Future – What is left to do!
• Motion analysis can help establish:– How pathomechanics related to phenotype– Understanding of functional changes with disease
progressionprogression– Define prognosis of future function using
documentation of pathomechanics and phenotype– Treatment outcomes studies– More detailed foot skeletal model needed
Myelomenigocele
• Congenital malformation that results from failure of embryonic neural tube closure.
• 4-5 of every 10,000 births
• Damage to the spinal cord and other congenital deformities persist
Implications for Ambulation
• Characterized by level of lesion: sacral, low lumbar (L5 and L4), etc.
• Loss of muscle function – weakness to paralysisS d fi it• Sensory deficits
• Asymmetry in lower extremity function• Contractures and bony torsions• Balance issues related to CNS injury and
weakness• Functional loss over time: tethered cord• Spasticity
Motion analysis in understanding gait pathology, AACPDM 2013 Part 2 -4
Pathomechanics of Myelomeningocele• Vankoski SJ et al,. Characteristic pelvic, hip, and
knee kinematic patterns in children with lumbosacral myelomeningocele, Gait and Posture, 3(1):51-57, 1995.
• Duffy C M Three-Dimensional Gait Analysis inDuffy, C. M., Three Dimensional Gait Analysis in Spina Bifida, JPO, 16(6): 786-791, 1996.
• Byung Kyu Park et al., Gait electromyography in children with myelomeningocele at the sacral level, Rehabilitation, 78(5):Pages 471–475, 1997.
• Õunpuu S, et al., An Examination of the Knee Function During Gait in Children with Myelomeningocele, JPO, 20(5), 629-635, 2000.
Pathomechanics of Myelomeningocele• Bartonek A et al, Upper body movement during
walking in children with lumbo–sacral myelomeningocele, Gait and Posture, 15(2), 120-129, 2002.
• Gutierrez EM et al, Characteristic gait kinematics in persons with lumbosacral myelomeningocele Gait andpersons with lumbosacral myelomeningocele, Gait and Posture, 18(3): 170-177, 2003.
• Gutierrez EM, et al., Centre of mass motion during gait in persons with myelomeningocele, Gait and Posture, 18(2): 37-46, 2003.
• Gutierrez EM et al, Kinetics of compensatory gait in persons with myelomeningocele, Gait and Posture, 21(1), 12-23, 2005.
Energy Cost
• Thomas, Susan Sienko, Longitudinal Assessment of Oxygen Cost and Velocity in Children With Myelomeningocele: Comparison of the Hip-Knee-Ankle-Foot Orthosis and the Reciprocating Gait Orthosis, JPO, 21(6): 798-803, 2001
• Galli M et al., , Energy consumption and gait analysis in children with myelomeningocele, Functional Neurology, 15(3): 171-175, 2000.
Treatment Assessment• Lim, R et al., Valgus Knee Stress in Lumbosacral
Myelomeningocele: A Gait-Analysis Evaluation, JPO, 18(4): 428-433,1988.
• Hullin, MG et al., Ankle-Foot Orthosis Function in Low-Level Myelomeningocele, JPO, 12(4): 423-561, 1992.
• Õunpuu S et al., Joint kinetics: methods, interpretation and treatment decision-making in children with cerebral palsy and myelomeningocele, Gait and Posture, 4(1): 62-78, 1996.
• Thomson, JD et al., The Effects of Ankle-Foot Orthoses on the Ankle and Knee in Persons with Myelomeningocele: An Evaluation Using Three-Dimensional Gait Analysis, JPO, 19(1): 27-33, 1999.
Sacral Level 1 – Barefoot Walking
Partial loss of: intrinsics of the foot, gastrocnemius, soleus, lateral hamstrings and gluteus maximus.
Sagittal Plane Kinetics - Right
• Hip and knee– Typical
• AnkleIncreased
*
– Increased dorsiflexion terminal stance*
• Passive ankle ROM typical
• Plantar flexor strength 4/5
Motion analysis in understanding gait pathology, AACPDM 2013 Part 2 -5
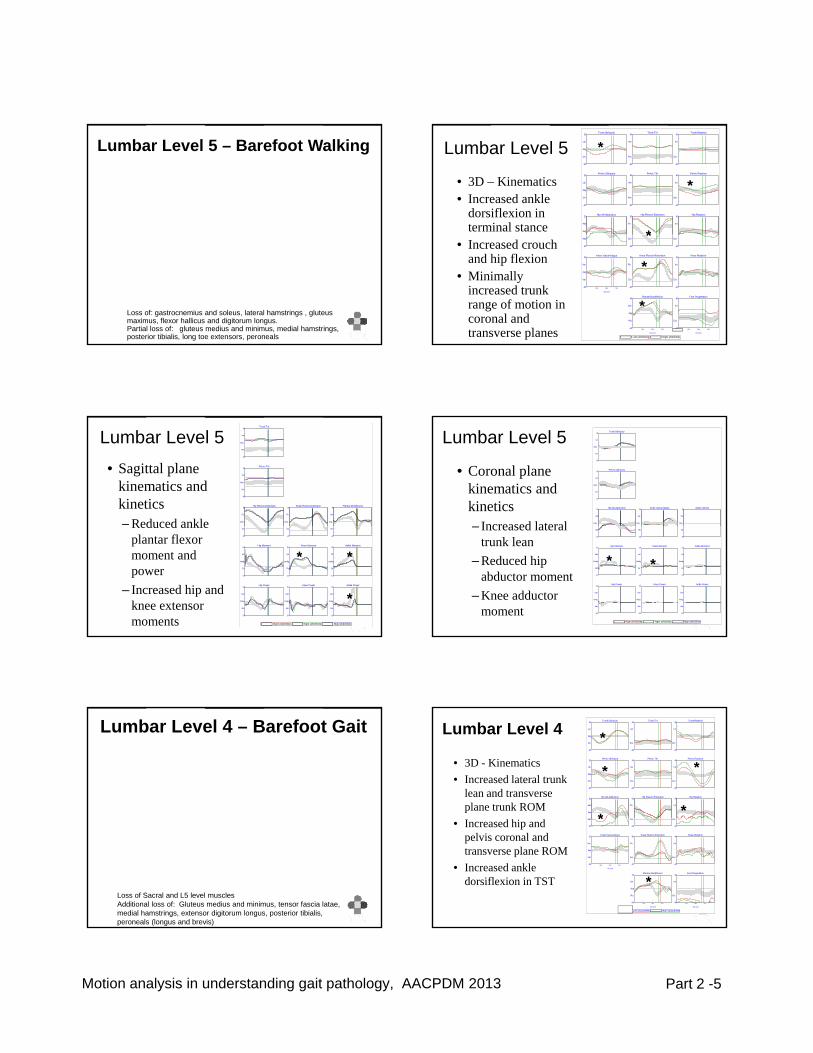
Lumbar Level 5 – Barefoot Walking
Loss of: gastrocnemius and soleus, lateral hamstrings , gluteus maximus, flexor hallicus and digitorum longus.Partial loss of: gluteus medius and minimus, medial hamstrings, posterior tibialis, long toe extensors, peroneals
Trunk Obliquity30
-30
Up
Dn
deg
Pelvic Obliquity20
-20
Up
Dn
deg
Hip Ab-Adduction20
Add
deg
Trunk Tilt40
-20
Ant
Pos
Pelvic Tilt40
-20
Ant
Pos
Hip Flexion-Extension60
Flx
Trunk Rotation40
-40
Int
Ext
Pelvic Rotation40
-40
Int
Ext
Hip Rotation40
Int
Lumbar Level 5
• 3D – Kinematics• Increased ankle
dorsiflexion in terminal stance *
*
*
214665 44 Left (4/9/2004) 214665 44 Right (4/9/2004)
-20
Abd
Knee Varus-Valgus
Gait Cycle
30
-30
Var
Val
deg
25% 50% 75%
-20
Ext
Knee Flexion-Extension80
-20
Flx
Ext
Plantar-Dorsiflexion
Gait Cycle
40
-40
Dor
Pla
deg
25% 50% 75%
-40
Ext
Knee Rotation40
-40
Int
Ext
Foot Progression
Gait Cycle
40
-40
Int
Ext
25% 50% 75%
• Increased crouch and hip flexion
• Minimally increased trunk range of motion in coronal and transverse planes
*
*
*
Trunk Tilt40
-20
Ant
Pos
Deg
Pelvic Tilt40
-20
Ant
Pos
Deg
Hip Flexion-Extension60
Flx
Deg
Knee Flexion-Extension80
Flx
Deg
Plantar-Dorsiflexion40
Dor
Deg
• Sagittal plane kinematics and kinetics– Reduced ankle
Lumbar Level 5
214665 41 Right (4/9/2004) 214665 42 Right (4/9/2004) 214665 44 Right (4/9/2004)
-20
Ext
Hip Moment2.0
-1.0
Ext
Flx
Nm/kg
Hip Power3.0
-2.0
Gen
Abs
W /kg
-20
Ext
Knee Moment2.0
-1.0
Ext
Flx
Nm/kg
Knee Power3.0
-2.0
Gen
Abs
W /kg
-40
Pla
Ankle Moment2.0
-1.0
Pfl
Dfl
Nm/kg
Ankle Power3.0
-2.0
Gen
Abs
W /kg
Reduced ankle plantar flexor moment and power
– Increased hip and knee extensor moments
* *
*
Trunk Obliquity30
-30
Up
Dn
Deg
Pelvic Obliquity20
-20
Up
Dn
Deg
Hip Ab-Adduction20
Add
Deg
Knee Varus-Valgus30
Var
Deg
Ankle Var/Val30
Var
Deg
• Coronal plane kinematics and kinetics
Increased lateral
Lumbar Level 5
214665 41 Right (4/9/2004) 214665 42 Right (4/9/2004) 214665 44 Right (4/9/2004)
-20
Abd
Hip Moment2.0
-1.0
Abd
Add
Nm/kg
Hip Power3.0
-2.0
Gen
Abs
W /kg
-30
Val
Knee Moment2.0
-1.0
Val
Var
Nm/kg
Knee Power3.0
-2.0
Gen
Abs
W /kg
-30
Val
Ankle Moment2.0
-1.0
Val
Var
Nm/kg
Ankle Power3.0
-2.0
Gen
Abs
W /kg
– Increased lateral trunk lean
– Reduced hip abductor moment
– Knee adductor moment
**
Lumbar Level 4 – Barefoot Gait
Loss of Sacral and L5 level musclesAdditional loss of: Gluteus medius and minimus, tensor fascia latae, medial hamstrings, extensor digitorum longus, posterior tibialis, peroneals (longus and brevis)
Trunk Obliquity30
-30
Up
Dn
deg
Pelvic Obliquity20
-20
Up
Dn
deg
Hip Ab-Adduction20
Add
deg
Trunk Tilt40
-20
Ant
Pos
Pelvic Tilt40
-20
Ant
Pos
Hip Flexion-Extension60
Flx
Trunk Rotation40
-40
Int
Ext
Pelvic Rotation40
-40
Int
Ext
Hip Rotation40
Int
Lumbar Level 4
• 3D - Kinematics• Increased lateral trunk
lean and transverse plane trunk ROM
*
*
*
*
*
221333 41 Left (2/21/2008) 221333 41 Right (2/21/2008)
-20
Abd
Knee Varus-Valgus
Gait Cycle
30
-30
Var
Val
deg
25% 50% 75%
-20
Ext
Knee Flexion-Extension80
-20
Flx
Ext
Plantar-Dorsiflexion
Gait Cycle
40
-40
Dor
Pla
deg
25% 50% 75%
-40
Ext
Knee Rotation40
-40
Int
Ext
Foot Progression
Gait Cycle
40
-40
Int
Ext
25% 50% 75%
• Increased hip and pelvis coronal and transverse plane ROM
• Increased ankle dorsiflexion in TST
*
*
Motion analysis in understanding gait pathology, AACPDM 2013 Part 2 -6
Trunk Tilt40
-20
Ant
Pos
Deg
Pelvic Tilt40
-20
Ant
Pos
Deg
Hip Flexion-Extension60
Flx
Deg
Knee Flexion-Extension80
Flx
Deg
Plantar-Dorsiflexion40
Dor
Deg
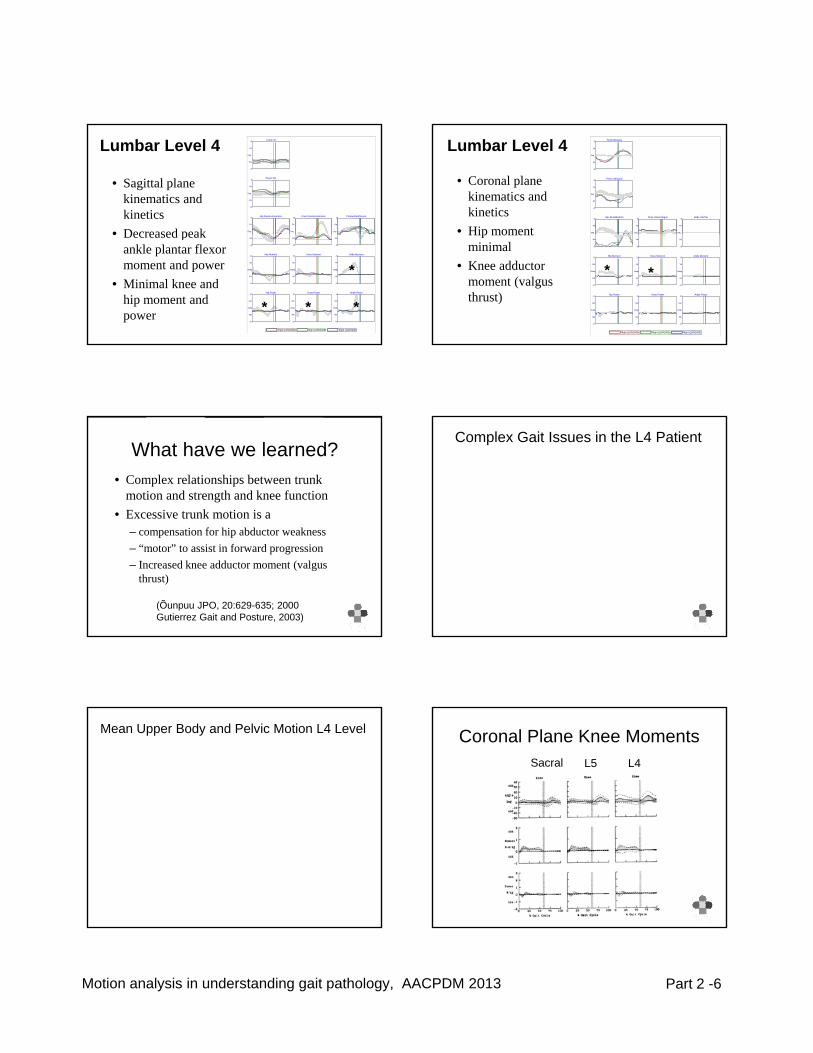
Lumbar Level 4
• Sagittal plane kinematics and kinetics
• Decreased peak
221333 29 Right (10/5/2005) 221333 29 Right (10/5/2005) 221333 29 Right (10/5/2005)
-20
Ext
Hip Moment2.0
-1.0
Ext
Flx
Nm/kg
Hip Power3.0
-2.0
Gen
Abs
W /kg
-20
Ext
Knee Moment2.0
-1.0
Ext
Flx
Nm/kg
Knee Power3.0
-2.0
Gen
Abs
W /kg
-40
Pla
Ankle Moment2.0
-1.0
Pfl
Dfl
Nm/kg
Ankle Power3.0
-2.0
Gen
Abs
W /kg
• Decreased peak ankle plantar flexor moment and power
• Minimal knee and hip moment and power
*
***
Lumbar Level 4
• Coronal plane kinematics and kinetics
• Hip moment
Trunk Obliquity30
-30
Up
Dn
Deg
Pelvic Obliquity20
-20
Up
Dn
Deg
Hip Ab-Adduction20
Add
Deg
Knee Varus-Valgus30
Var
Deg
Ankle Var/Val30
Var
Deg Hip moment minimal
• Knee adductor moment (valgus thrust)
221333 29 Right (10/5/2005) 221333 29 Right (10/5/2005) 221333 29 Right (10/5/2005)
-20
Abd
Hip Moment2.0
-1.0
Abd
Add
Nm/kg
Hip Power3.0
-2.0
Gen
Abs
W /kg
-30
Val
Knee Moment2.0
-1.0
Val
Var
Nm/kg
Knee Power3.0
-2.0
Gen
Abs
W /kg
-30
Val
Ankle Moment2.0
-1.0
Val
Var
Nm/kg
Ankle Power3.0
-2.0
Gen
Abs
W /kg
**
What have we learned?• Complex relationships between trunk
motion and strength and knee function• Excessive trunk motion is a
– compensation for hip abductor weakness – “motor” to assist in forward progression– Increased knee adductor moment (valgus
thrust)
(Õunpuu JPO, 20:629-635; 2000Gutierrez Gait and Posture, 2003)
Complex Gait Issues in the L4 Patient
Mean Upper Body and Pelvic Motion L4 Level Coronal Plane Knee MomentsSacral L5 L4
Motion analysis in understanding gait pathology, AACPDM 2013 Part 2 -7
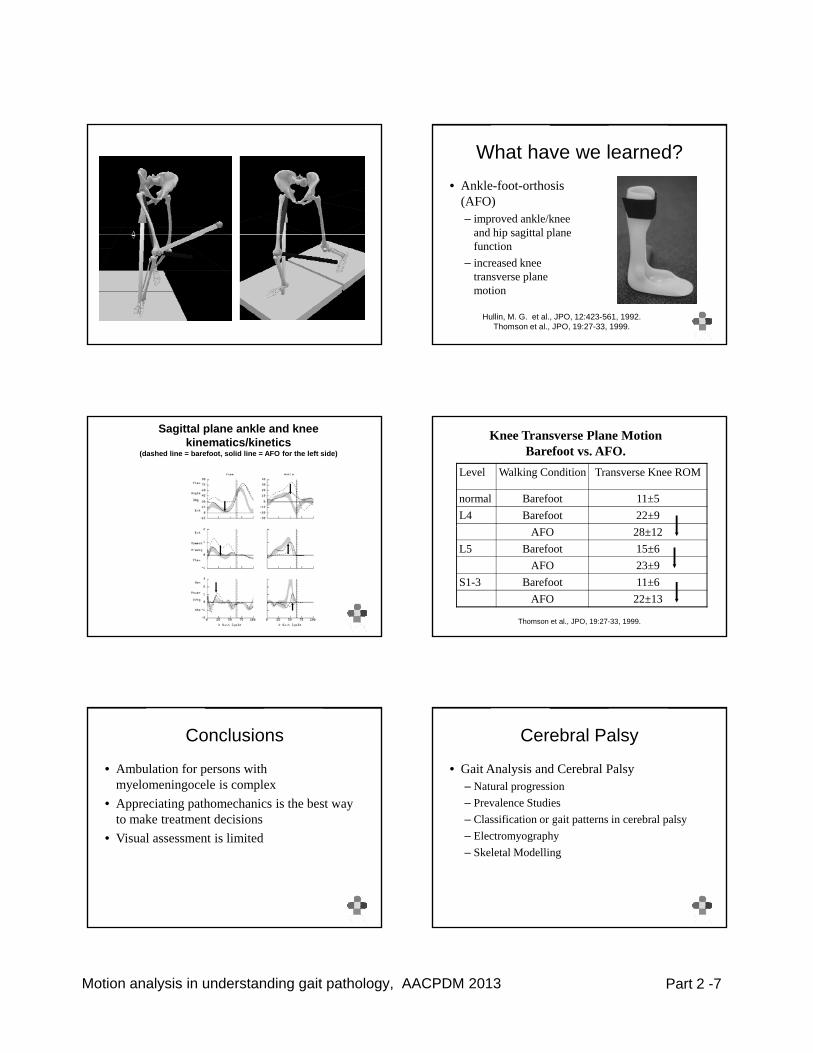
What have we learned?• Ankle-foot-orthosis
(AFO)– improved ankle/knee
and hip sagittal planeand hip sagittal plane function
– increased knee transverse plane motion
Hullin, M. G. et al., JPO, 12:423-561, 1992.Thomson et al., JPO, 19:27-33, 1999.
Sagittal plane ankle and knee kinematics/kinetics
(dashed line = barefoot, solid line = AFO for the left side)
Knee Transverse Plane Motion Barefoot vs. AFO.
Level Walking Condition Transverse Knee ROM
normal Barefoot 11±5L4 Barefoot 22±9
AFO 28±12L5 Barefoot 15±6
AFO 23±9S1-3 Barefoot 11±6
AFO 22±13
Thomson et al., JPO, 19:27-33, 1999.
Conclusions
• Ambulation for persons with myelomeningocele is complex
• Appreciating pathomechanics is the best way to make treatment decisionsto make treatment decisions
• Visual assessment is limited
Cerebral Palsy
• Gait Analysis and Cerebral Palsy– Natural progression– Prevalence Studies
Classification or gait patterns in cerebral pals– Classification or gait patterns in cerebral palsy– Electromyography– Skeletal Modelling
Motion analysis in understanding gait pathology, AACPDM 2013 Part 2 -8
Natural Progression and Motion Analysis
• Understanding the implications of not undergoing surgical intervention in children with cerebral palsy
• Required to interpret treatment results such as orthopaedic intervention
• Provide a justification for the importance of treatment
Johnson et al. Results
• 18 subjects with spastic diplegia, ranging in age from 4 to 14 years assessed at 32 months apart
• deterioration of gait stability evidenced by increases in double support and decreases in single support pp g ppwith time and growth (p < 0.05).
• kinematic analysis revealed a loss of excursion about the knee, ankle, and pelvis (p < 0.05).
• passive range-of-motion analysis revealed a decrease in the popliteal angle over time (p < 0.05).
Published Studies
• Johnson, David C.; Damiano, Diane L; Abel, Mark F. The Evolution of Gait in Childhood and Adolescent Cerebral Palsy, J Pediatr Orthop, 17:392-396, 1997
• Bell KJ, Õunpuu S, DeLuca PA, Romness MJ. pNatural Progression of Gait in Children with Cerebral Palsy. J Pediatr Orthop, 22:677-82, 2002
• Martin Gough, Linda C, Richard O Robinson, Adam P Shortland , Short-term outcome of multilevel surgical intervention in spastic diplegic cerebral palsy compared with the natural history, DMCN, 46(2): 91-97, 2004.
Gough et al, Results
• twelve patients (mean age 10 years) with no treatment (control group)
• showed a significant increase in minimum hip and knee flexion in stance 17 months after firstand knee flexion in stance 17 months after first gait analysis
Bell et al.
• 25 children with cerebral palsy• Two gait analyses an average of 4 years apart• No intervening surgery• Clinical Measures
– Statistically significant reductions in • popliteal angle• passive maximum ankle dorsiflexion
– No change in passive maximum hip internal/external ROM
Gait Changes:
• Functional Walkers (>81 cm/sec walking velocity)• Less Functional Walkers (<80 cm/sec)
Motion analysis in understanding gait pathology, AACPDM 2013 Part 2 -9
Conclusions• Functional Walkers
– Getting “stiffer”• Decreased knee flexion in swing• Decreased ankle, knee and hip range of motionp g
• Less Functional Walkers– Increased crouch
• Increased knee flexion and ankle dorsiflexion in stance
Conclusions
• ambulatory ability tends to worsen over time in children with spastic cerebral palsy
• outcome studies comparing postoperative gait with preoperative gait require thiswith preoperative gait require this understanding to interpret results
Future – What is left to do!
• Increase study numbers• Understand natural progression by GMFCS
level
Prevalence Studies
• Studies that help to define the characteristics/pathomechanics of a particular diagnostic group such as cerebral palsy
• Provides important information for counseling• Provides important information for counseling parents and patients with cerebral palsy
• Information about prognosis in terms of– possible treatment needs– future gait function
Prevalence of Gait Abnormalities in CP
• 492 patients with cerebral palsy• computerized motion analysis• prevalence of 14 specific gait abnormalities
l d d d b dwas evaluated and compared based on– involvement (hemiplegia, diplegia, or
quadriplegia)– age– history of previous lower extremity surgery
Wren et al. JPO, 2005
Prevalence of Gait Abnormalities in CP
• In hemiplegic, diplegic, and quadriplegic groups, more than 50% of patients had– stiff knee in swing
equinus– equinus– in-toeing
• In diplegic and quadriplegic groups, more than 50% of patients also had– increased hip flexion – crouch
Wren et al. JPO, 2005

Motion analysis in understanding gait pathology, AACPDM 2013 Part 2 -10
• In quadriplegic group, more than 50% of patients also had– Increased hip adduction
Prevalence of Gait Abnormalities in CP
Wren et al. JPO, 2005
• The likelihood of having stiff knee in swing, out-toeing, calcaneus deformity, and crouch increased with prior surgery.
• The likelihood of having rotational
Prevalence of Gait Abnormalities in CP
• The likelihood of having rotational malalignment of the leg (internal hip rotation with out-toeing), calcaneus, out-toeing, varus and valgus foot deformities, and hip internal rotation increased with age.
Wren et al. JPO, 2005
Understanding Gait Pathology
• Increased understanding of pathomechanics –causes of gait issues
• Increased understanding of appropriate treatment optionstreatment options
Causes of In-toeing Gait in Children with Cerebral Palsy
• 412 children with cerebral palsy (587 involved sides)
• Combination of motion analysis and clinical yassessment information
Rethlefsen, S et al., Causes of In-toeing Gait in Children with Cerebral Palsy, JBJS (Am), 88(10):2175-2180, 2006.
• Most common causes of in-toeing – internal hip rotation (322 of 587 sides) – internal tibial torsion (296 of 587 sides).
pes ar s contrib ted to in toeing of 35 of the– pes varus contributed to in-toeing of 35 of the eighty-two involved limbs of the patients with hemiplegia
– pes varus contributed to in-toeing in 42 of the 505 limbs of the patients with diplegia or quadriplegia
• 1/3 rd of children with CP have multiple causes of internal rotation
• Multiple causes of in-toeing were noted in 215 of the 587 involved limbsof the 587 involved limbs– bilateral involvement: 176 of the 505 limbs of the
patients with bilateral involvement – hemiplegic involvement : 39 of the 82 involved
limbs
Motion analysis in understanding gait pathology, AACPDM 2013 Part 2 -11
Causes of in-toeing
• Bilateral involvement: – internal hip rotation (288 of 505)– internal tibial torsion (261 of 505)
internal pel ic rotation (ninet t o of 505)– internal pelvic rotation (ninety-two of 505)• Hemiplegic involvement:
– internal tibial torsion (35 of 82)– pes varus (35-82)– internal hip rotation (34-82)– metatarsus adductus (20-82)
Conclusion
• 1/3 of children with CP have multiple causes of internal rotation
• Pes varus is common in hemiplegia and rare in children with bilateral involvementchildren with bilateral involvement
• Knowledge of possible causes helps direct clinical assessment and understanding
• Is critical to treatment decision making
Gait Classifications/Patterns in Cerebral Palsy
• Effort to develop a “typology” that differs from the present diagnostic system which classifies a cerebral palsy patient as either quadriplegic diaplegic or hemiplegic or morequadriplegic, diaplegic or hemiplegic or more recently GMFCS level.
• Typology based upon function at the joint level– Single joint – knee– Multiple joints – knee and ankle
• Motion analysis data based
Benefits of Classification/Patterns
• standardization of gait management/treatment• communication within and across professions
if organized based upon visually identifiable gait characteristics: crouch, equinus etc.
• must be:– Clinically meaningful categories– Related to specific impairments
• illustrative representation of characteristics for each pattern = clinically friendly
Initial Efforts• Wong MA, et al, Statistical analysis of gait
patterns of persons with cerebral palsy, Statistics in Medicine, 2(3), pages 345–354, July/September 1983.
• Kadaba M, et al., Gait pattern recognition in spastic diplegia. Dev Med Child Neurol. S33:28, 1991.
• Sutherland et al., Common gait abnormalities of the knee in cerebral palsy. Clin Orthop Relat Res, 139-47, 1993.
Gait Patterns in Hemiplegia• Winters T et al., Gait patterns in hemiplegia in
children and adults. JBJS (Am): 69 (A): 437-41, 1987.
• Hullin MG et al., Gait patterns in children with , phemiplegic spastic cerebral palsy, JPO, 5:247-51, 1996.
• Õunpuu S, DeLuca PA, Davis RB, Chapter 7: Gait Analysis, In Congenital Hemiplegia, Ed Brian Neville, Robert Goodman, Cambridge University Press, Suffolk, 81-97, 2000.
Motion analysis in understanding gait pathology, AACPDM 2013 Part 2 -12
Con’t
• Rodda J et al., Classification of gait patterns in spastic hemiplegia and spastic diplegia: a basis for a management algorithm, European Journal of Neurology 8: 98-108 2001of Neurology, 8: 98-108, 2001.
• Stebbins J et al., Gait classification in hemiplegic cerebral palsy based on EMG, Gait and Posture, 20:S2-3, 2004.
Classifications - Methodology
• Quality is limited:– Reliability– Validity
Arbitrar decisions– Arbitrary decisions– Adequate numbers– Sagittal plane focus
• Dobson, F et al., Gait classification in children with cerebral palsy: A systematic review, Gait and Posture, 25(1): 140-152, 2007.
Gait Patterns: Hemiplegia
• Provided frame work for thinking about hemiplegia as a continuum of increasing involvement with associated increasing requirements for treatmentrequirements for treatment
• 4 types – sagittal plane (Winter, 1987)• Kinetics and EMG (Hullin, 1996)• Addition of transverse plane (Õunpuu, 2000
and Rodda, 2001)• EMG alone (Stebbins, 2004)
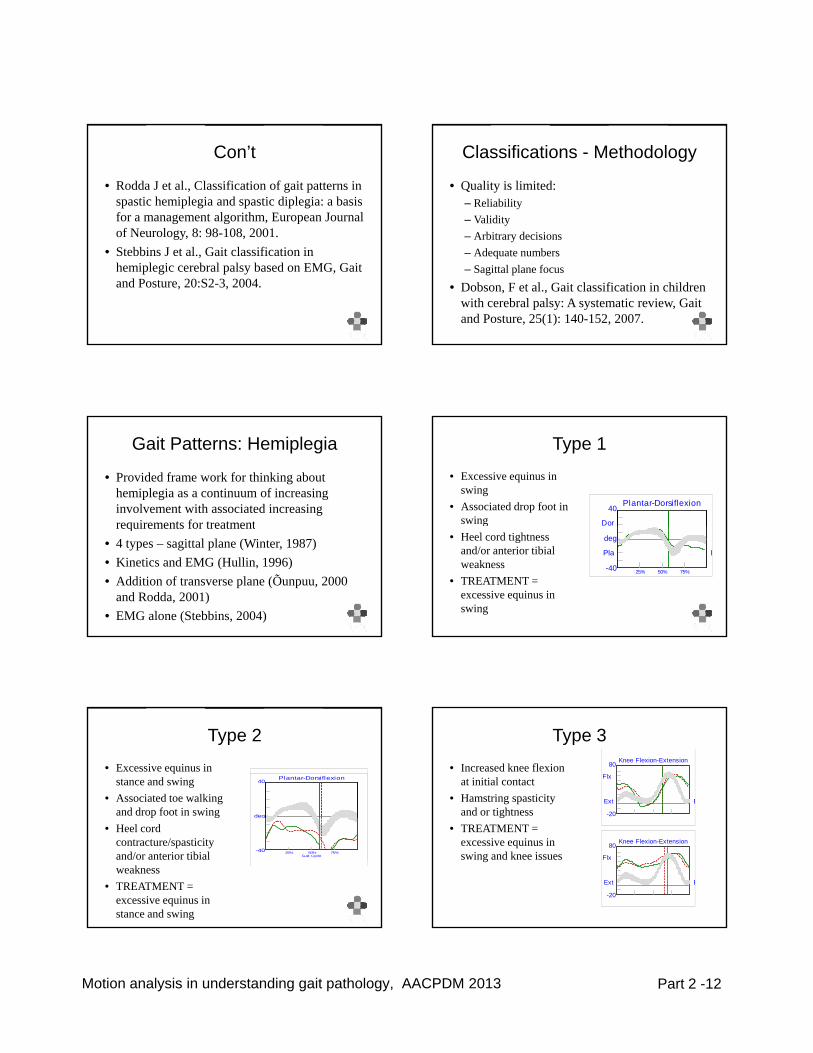
Type 1
• Excessive equinus in swing
• Associated drop foot in swing
Plantar-Dorsiflexion40
Dor g• Heel cord tightness
and/or anterior tibial weakness
• TREATMENT = excessive equinus in swing
-40
Pla
deg
25% 50% 75%
E
Type 2
• Excessive equinus in stance and swing
• Associated toe walking and drop foot in swing
Plantar-Dorsiflexion40
degp g• Heel cord
contracture/spasticity and/or anterior tibial weakness
• TREATMENT = excessive equinus in stance and swing
Gait Cycle-40
g
25% 50% 75%
Type 3
• Increased knee flexion at initial contact
• Hamstring spasticity and or tightness
Knee Flexion-Extension80
-20
Flx
Ext E
g• TREATMENT =
excessive equinus in swing and knee issues
Knee Flexion-Extension80
-20
Flx
Ext E
Motion analysis in understanding gait pathology, AACPDM 2013 Part 2 -13
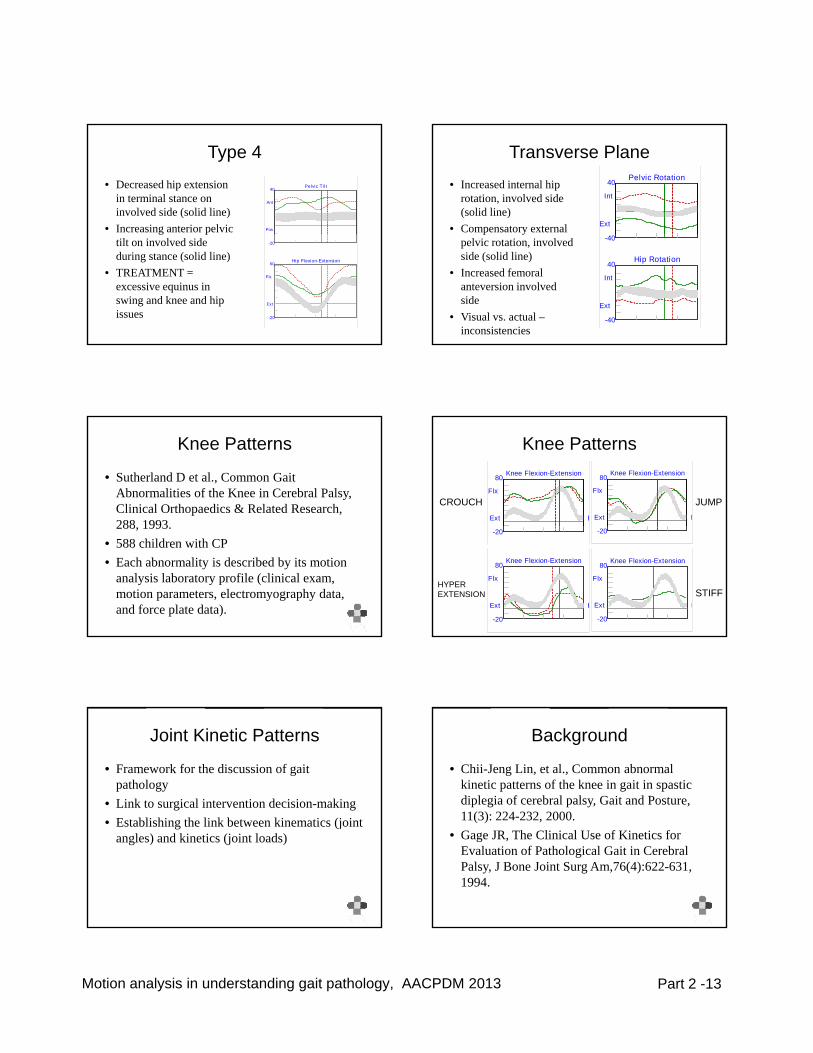
Type 4
• Decreased hip extension in terminal stance on involved side (solid line)
• Increasing anterior pelvic
Pelvic Til t40
Ant
Pos g ptilt on involved side during stance (solid line)
• TREATMENT = excessive equinus in swing and knee and hip issues
-20
Hip Flexion-Extension60
-20
Flx
Ext
Transverse Plane
• Increased internal hip rotation, involved side (solid line)
• Compensatory external
Pelvic Rotation40
Int
Ext p ypelvic rotation, involved side (solid line)
• Increased femoral anteversion involved side
• Visual vs. actual –inconsistencies
-40
Hip Rotation40
-40
Int
Ext
Knee Patterns
• Sutherland D et al., Common Gait Abnormalities of the Knee in Cerebral Palsy, Clinical Orthopaedics & Related Research, 288 1993288, 1993.
• 588 children with CP• Each abnormality is described by its motion
analysis laboratory profile (clinical exam, motion parameters, electromyography data, and force plate data).
Knee PatternsKnee Flexion-Extension80
Flx
Ext E
Knee Flexion-Extension80
Flx
Ext E
JUMPCROUCH
-20 -20
Knee Flexion-Extension80
-20
Flx
Ext E
Knee Flexion-Extension80
-20
Flx
Ext ESTIFF
HYPEREXTENSION
Joint Kinetic Patterns
• Framework for the discussion of gait pathology
• Link to surgical intervention decision-makingbli hi h li k b ki i (j i• Establishing the link between kinematics (joint
angles) and kinetics (joint loads)
Background
• Chii-Jeng Lin, et al., Common abnormal kinetic patterns of the knee in gait in spastic diplegia of cerebral palsy, Gait and Posture, 11(3): 224-232 200011(3): 224-232, 2000.
• Gage JR, The Clinical Use of Kinetics for Evaluation of Pathological Gait in Cerebral Palsy, J Bone Joint Surg Am,76(4):622-631, 1994.
Motion analysis in understanding gait pathology, AACPDM 2013 Part 2 -14
• “Double Bump” Ankle Pattern:– Kinematic and
kinetic (moment andkinetic (moment and power)
– Toe initial contact– Spasticity in ankle
plantar flexors
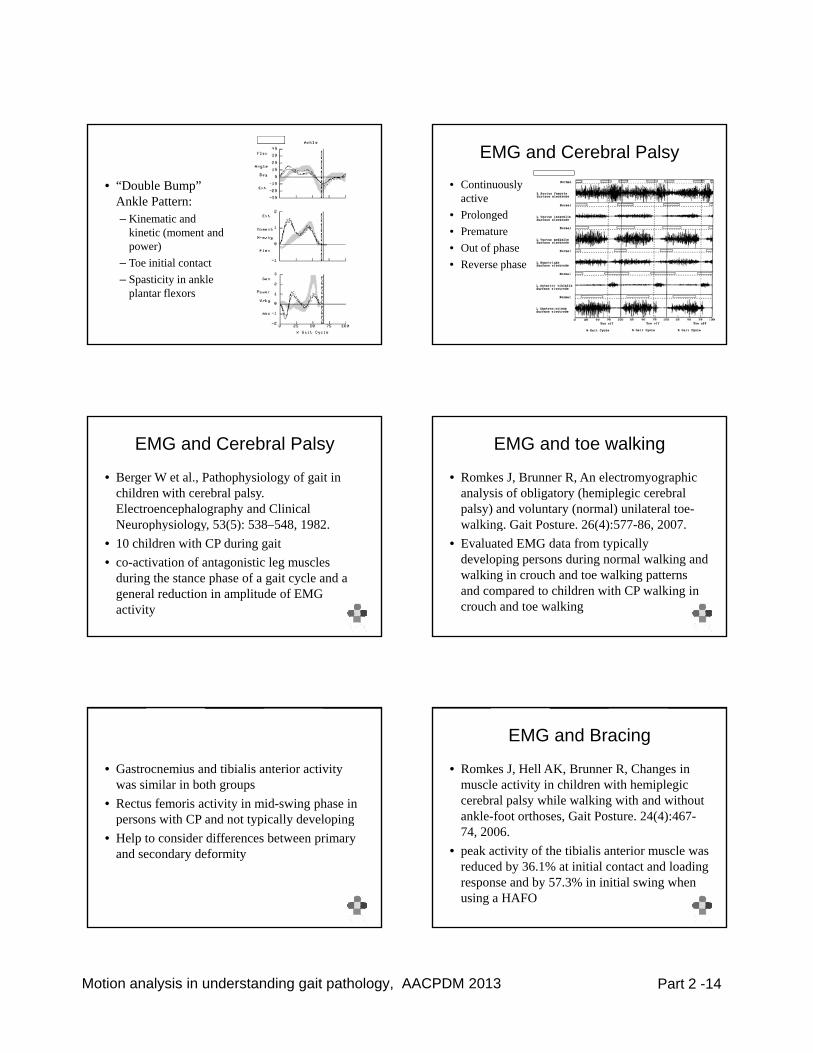
EMG and Cerebral Palsy
• Continuously active
• Prolonged• PrematurePremature• Out of phase• Reverse phase
EMG and Cerebral Palsy
• Berger W et al., Pathophysiology of gait in children with cerebral palsy. Electroencephalography and Clinical Neurophysiology 53(5): 538–548 1982Neurophysiology, 53(5): 538 548, 1982.
• 10 children with CP during gait• co-activation of antagonistic leg muscles
during the stance phase of a gait cycle and a general reduction in amplitude of EMG activity
EMG and toe walking
• Romkes J, Brunner R, An electromyographic analysis of obligatory (hemiplegic cerebral palsy) and voluntary (normal) unilateral toe-walking Gait Posture 26(4):577-86 2007walking. Gait Posture. 26(4):577-86, 2007.
• Evaluated EMG data from typically developing persons during normal walking and walking in crouch and toe walking patterns and compared to children with CP walking in crouch and toe walking
• Gastrocnemius and tibialis anterior activity was similar in both groups
• Rectus femoris activity in mid-swing phase in persons with CP and not typically developingpersons with CP and not typically developing
• Help to consider differences between primary and secondary deformity
EMG and Bracing
• Romkes J, Hell AK, Brunner R, Changes in muscle activity in children with hemiplegic cerebral palsy while walking with and without ankle-foot orthoses Gait Posture 24(4):467-ankle-foot orthoses, Gait Posture. 24(4):467-74, 2006.
• peak activity of the tibialis anterior muscle was reduced by 36.1% at initial contact and loading response and by 57.3% in initial swing when using a HAFO
Motion analysis in understanding gait pathology, AACPDM 2013 Part 2 -15
EMG and Treatment Planning
• Perry J et al., Preoperative and postoperative dynamic electromyography as an aid in planning tendon transfers in children with cerebral palsy. JBJS (Am), 59(4):531-537, 1977.
Motion Analysis - Skeletal Modeling• Peak Knee Flexion Deficit• Role of rectus femoris vs.
vastii• Other factors:
– Stance phase knee kinetics (increased knee extensor moment)
– Rotational deformity
• Simulation
Õunpuu S. et al., Gait and Posture, 5(3):211-216, 1997.Goldberg S R, et al., Journal of Biomechanics, 36, 1111-1116, 2003.Goldberg S R, Journal of Biomechanics, 39:689-698, 2006.
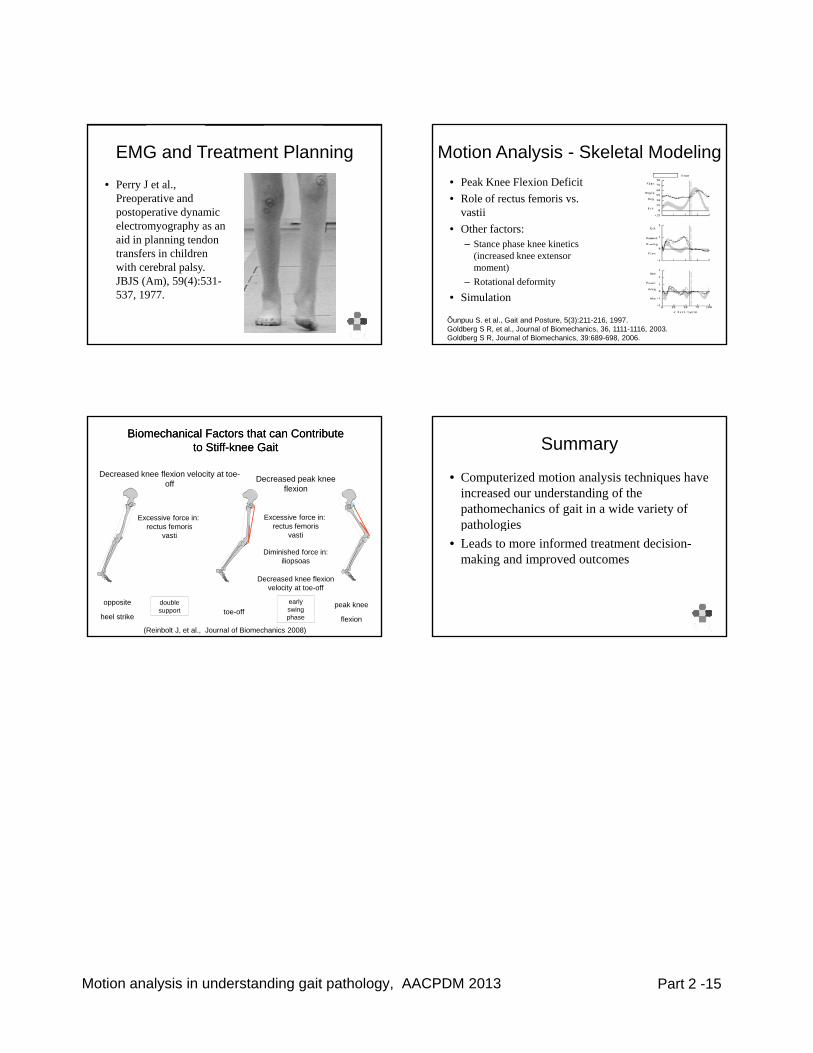
Decreased peak knee flexion
Decreased knee flexion velocity at toe-off
Excessive force in: rectus femoris
Excessive force in:rectus femoris
Biomechanical Biomechanical Factors Factors that can that can Contribute Contribute to to StiffStiff--knee knee GGait ait
double support
rectus femorisvasti
Diminished force in:iliopsoas
Decreased knee flexion velocity at toe-off
rectus femorisvasti
early swing phase
opposite
heel striketoe-off
peak knee
flexion(Reinbolt J, et al., Journal of Biomechanics 2008)
Summary
• Computerized motion analysis techniques have increased our understanding of the pathomechanics of gait in a wide variety of pathologiespathologies
• Leads to more informed treatment decision-making and improved outcomes


















