Parotid Neoplasm
58
Parotid Neoplasms
-
Upload
kuothonyuwi -
Category
Health & Medicine
-
view
197 -
download
7
Transcript of Parotid Neoplasm
Parotid Neoplasms
Presenter : Dr. Kuotho T Nyuwi
Moderator: Dr. Ak Ibohal Singh
Salivary Glands
Three major
- Parotid
- Submandibular
- Sublingual
Many minor~450
Function – Mastication(lubrication)
Inhibits bacterial growth
Digestive enzymes
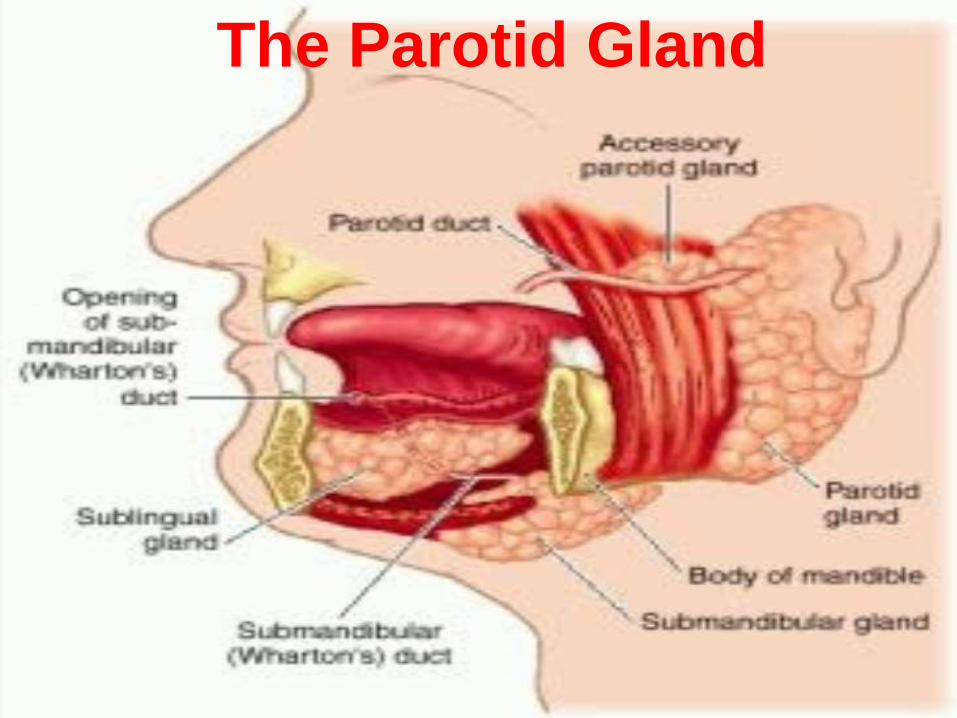
The Parotid Gland
ANATOMY
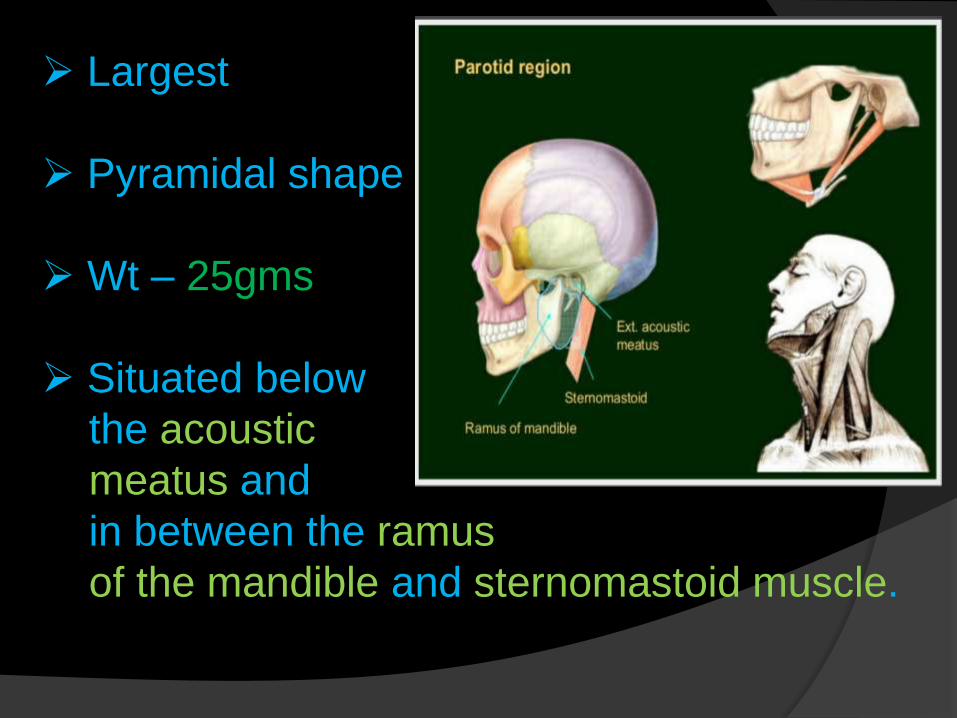
Largest
Pyramidal shape
Wt – 25gms
Situated below
the acoustic
meatus and
in between the ramus
of the mandible and sternomastoid muscle.
Resembles inverted 3 sided pyramid
Four surfaces
- Superior /base
- Superficial
- Anteromedial
- Posteromedial
Borders
- Anterior
- Posterior
- medial
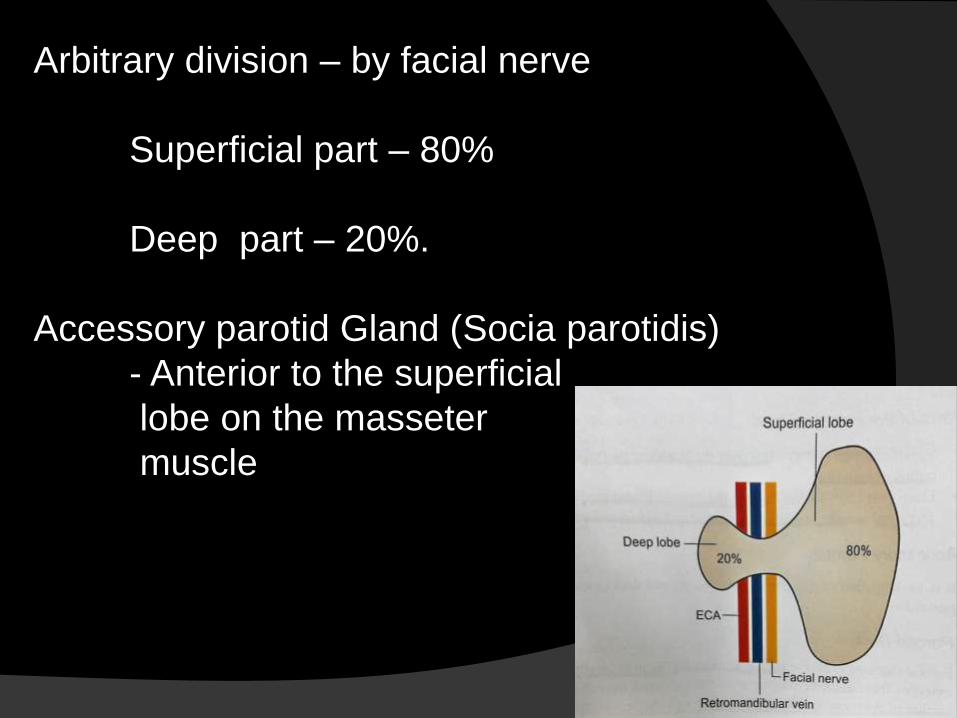
Arbitrary division – by facial nerve
Superficial part – 80%
Deep part – 20%.
Accessory parotid Gland (Socia parotidis)
- Anterior to the superficial
lobe on the masseter
muscle
Boundaries:
Ant – Masseter Muscle
Mandibular Ramus
Sup – Ext. Acoustic meatus
Condyle of the Mandible
Post - Mastoid process
Sternocleidomastoid muscle
Inf - Post. Belly of digastric
Med – Styloid process
Parotid capsule:
Derived from investing layer of deep cervical fascia
Superficial layer – Thick & closely adherent.
Sends fibrous septa into the gland
Deep Layer – Thin, Attached to styloid process,
mandible and tympanic plate.
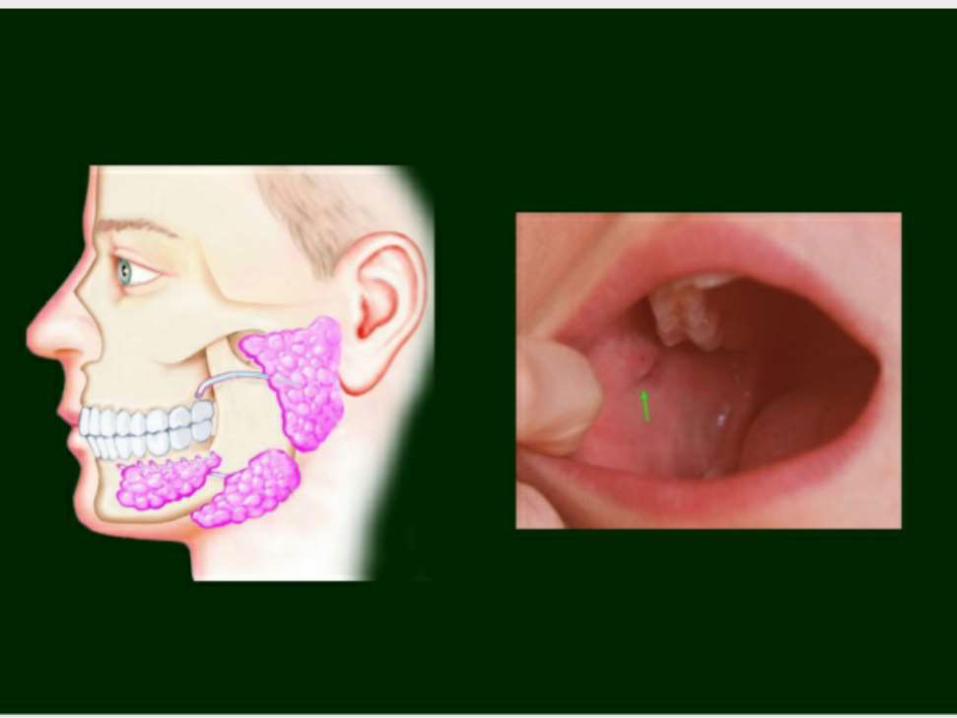
Parotid Duct (Ductus parotideus/ Stensen’s duct)
5cm in length
Appears at the ant. border of the gland
Runs ant. & downward on the masseter
At the ant. border of the masseter it pierces –
- Buccal pad of fat
- Buccopharyngeal fascia
- Buccinator Muscle
Opens opposite to the crown of 2nd upper molar tooth
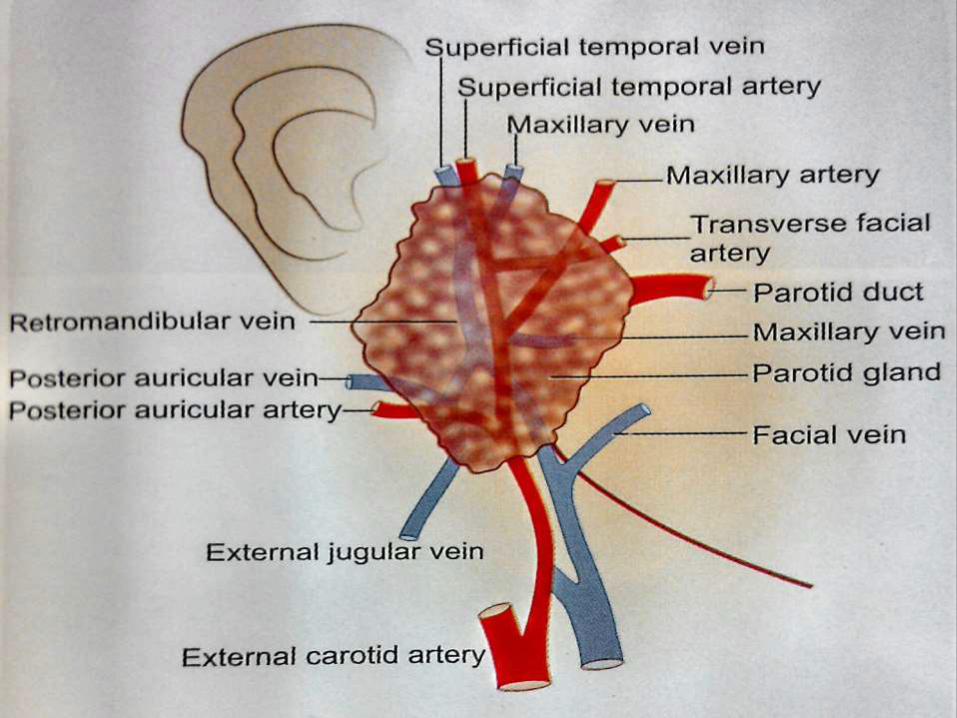
Structures within the parotid gland
- Facial Nerve
- Retromandibular vein
- External carotid artery
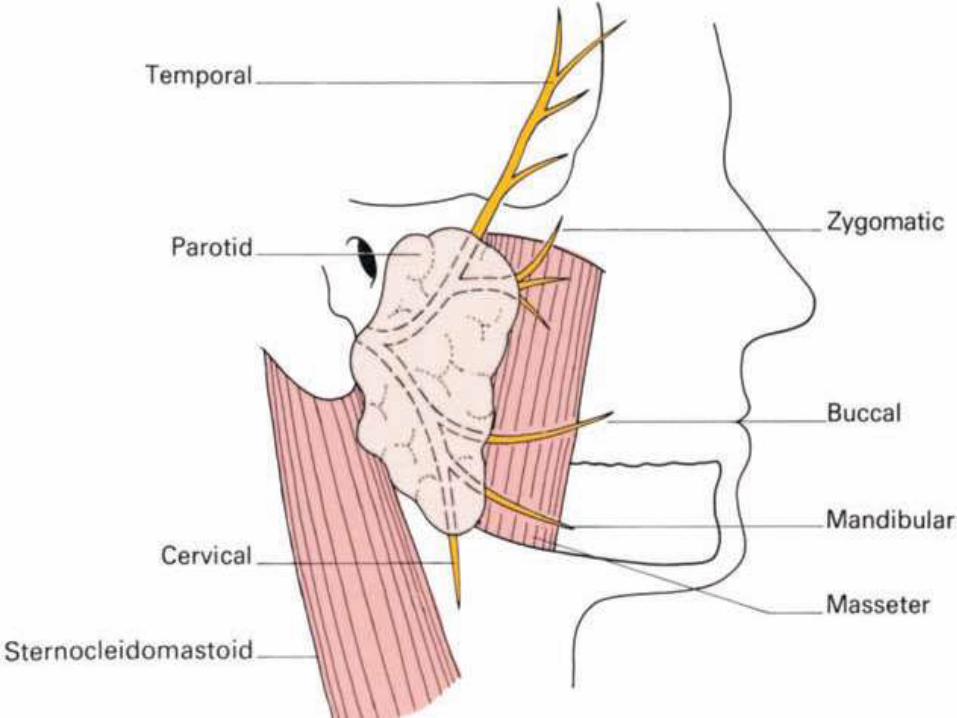
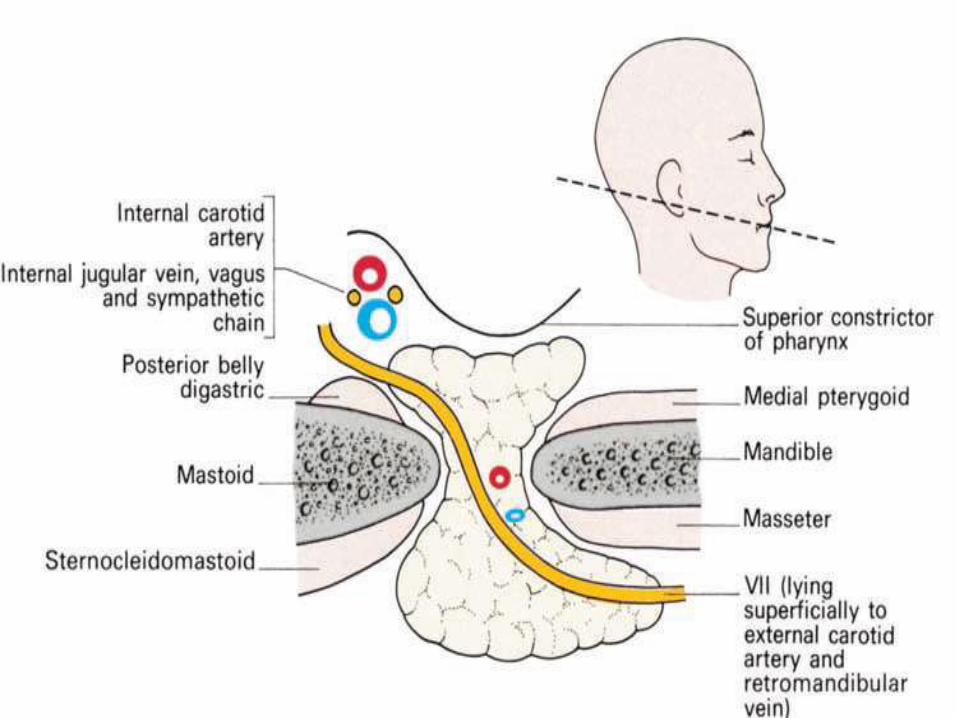
Facial nerve(Radiates like goose foot- pes anserinus)
Emerges from the stylomastoid foramen
Pierces the posteromedial surface
Lies superficial to the ext. carotid artery & retro
mandibular vein
Divides into:
1. Temporo-zygomatic trunk – Temporal
Zygomatic
2. Cervico facial trunk – Buccal
Marginal Mandibular
Cervical
Blood supply:
Arterial – Maxillary and Sup. temporal artery
(Branches of ext. carotid)
Veins – Retromandibular vein Ext.Juglar vein
Nerve supply :
Sensory – Auriculotemporal N.
Parasympathetic – Secretomotor
Via auriculotemporal N
sympathetic – Vasomotor
Ext. carotid plexus.
Lymphatic drainage
Intraglandular
Parotid lymph gland
Extraglandular (preauricular &
Infraauricular)
Deep cervical lymph glands
Parotid Neoplasm
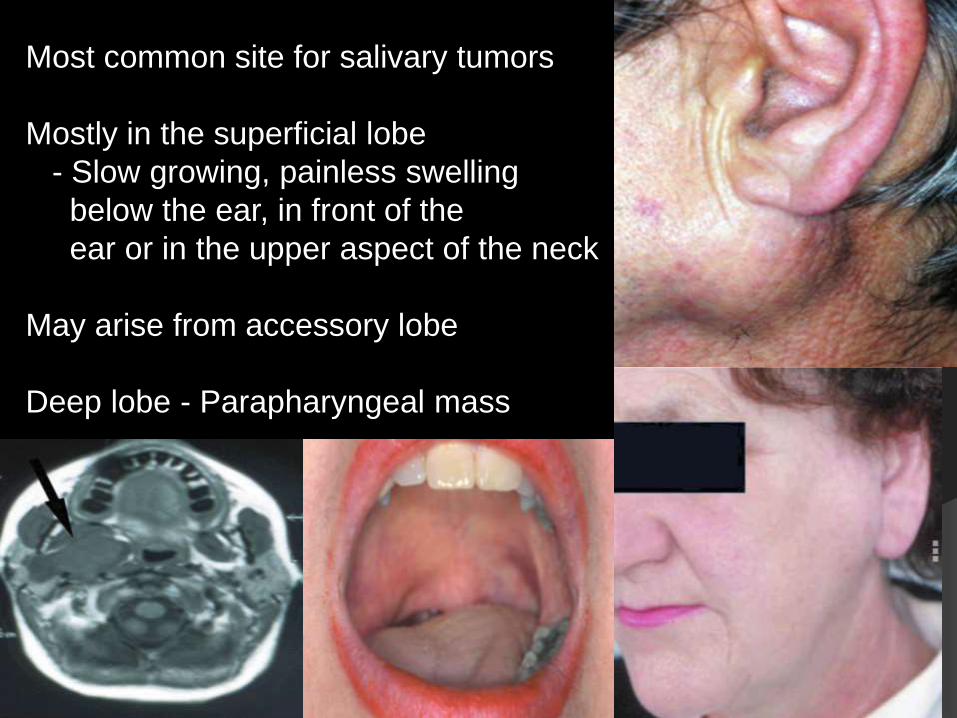
Most common site for salivary tumors
Mostly in the superficial lobe
- Slow growing, painless swelling
below the ear, in front of the
ear or in the upper aspect of the neck
May arise from accessory lobe
Deep lobe - Parapharyngeal mass
80% of salivary neoplasm occur in parotid gland
80-90% are benign (commonest – Pleomorphic Adenoma)
90% minor salivary gland tumor are malignant
Incidence of malignancy – inversely related to size of gland
Parotid ~ 20%
Submandibular ~ 40%
Sublingual ~ 60%
Minor glands ~ 80%
Aetiology
Radiation
Smoking (Warthin’s tumor)
Genetics – loss of alleles of chromosomes in
12q, 8q, 17q
Environment & diet – Def. of vit A, industrial agents like nickel,
cadmium, hair dyes, silica, preservatives
Infective – Mumps, EBV, chronic sailadenitis
Recurrent inflammation dysplasia carcinoma
ClassificationA) Epithelial (90%)
1) Adenomas
Pleomorphic adenoma
Monomorphic adenoma(Adenolymphoma)
2) Carcinomas
Mucoepidermoid carcinoma ( most common)
Acinic cell Ca.
Adenoid cystic Ca.
Adenocarcinoma
Sq. cell Ca.
Ca. in ex pleomorphic adenoma
B) Non epithelialHaemangioma
Lymphangioma
Neurofibromas
C) Malignant lymphomas
Primary – NHL
Secondary – Lymphoma in Sjogren’s syd
D) Secondary tumors
Local – Head and neck
Distant - Skin and bronchus
E) Unclassified tumors
F) Tumor like lesion
Solid lesion – Benign lymphoepithelial lesion
Adenomatoid hyperplasia
Cystic lesion – Salivary gland cyst.
Benign tumors
- Painless
- Slow growing
- No facial nerve involvement
Pleomorphic Adenoma
- Commonest (80%)
Parotid – 80%
Submandibular – 10%
Sublingual – 0.5%
- Histologically – Epithelial cells
Myoepithelial cells
Mucoid materials
Cartilages/pseudocartilages
- Grossly – Solid tissues
Cartilages
Cystic spaces
Diagnosis
- Usually unilateral
- Firm lobulated, mobile, painless swelling
- Not adherent to skin/ masseter muscle
- Positive curtain sign

Malignant transformation (3-5%)
- Recent increase in size
- Pain
- Involvement of skin, ulceration
- Involvement of masseter
- Involvement of the facial nerve
- Involvement of neck nodes
- Restriction of jaw movement
Pain is usually due to
Capsular distension by tumor
Obstruction to free flow of saliva
Nerve infiltration
Inflammation like in Warthin’s
Tumor necrosis

Investigations
FNAC – 95% accuracy
CT Scan – Status of deep lobe
Local extension
Spread
MRI
Open Biopsy – Contraindicated
- Chance of injury to facial nerve
- Chance of parotid fistula formation
- Seeding of tumor cells and high chance of recurrence
Treatment
Superficial parotidectomy
Total conservative parotidectomy
RT can be given
Recurrence(5%)
Spillage
Improper technique
Inadequate margin
Retained pseudopods
Multicentricity
Adenolymphoma
- Warthin’s Tumor/ Papillary Cystadenolymphomatosum
- Misnomer – Neither malignant nor Lymphoma
- 5-15% of Parotid tumor (2nd most common tumor)
- Smoking – 8 times more risk
- Mostly in the lower pole & overlies the angle of mandible
- Usually involve only the superficial lobe
- More common in male, elderly and in whites
- No malignant transformation
Microscopy –:
- Cystic/Glandular spaces
- Lined by columnar epithelium
- Abundant lymphoid tissue in the stoma
Investigations:
- FNAC
- Tc99 scan – Hot spot (due to high mitochondrial
content)
Treatment:
- Superficial parotidectomy
Oncocytoma
- < 1% of salivary gland tumor
- Mostly in parotid glands
- Gross: Small tan colored well circumscribed encapsulated
solid tumor
- Microscopy: Large oncocytes with swollen granular
cytoplasm
- Hot spot on Tc99
Malignant tumors
Mucoepidermoid Ca.
- Most common malignant tumor of the parotid
- Occurs both in minor & major glands
- Slow growing attaining large size
- High grade – Epidermoid cells mainly –regional & distant
spread
- Low grade – Mucous cells mainly – regional nodes spread.
Adenoid Cystic Carcinoma
- Rare in parotid gland
- Also called cylidromatous Ca.
- Slow growing but highly malignant
- High affinity for perineural spread(trigeminal ganglion)
- Blood spread – Lungs, Bones, Liver
- Treatment : Radical Parotidectomy
RT
- 5year survival – 70%
Acinic cell tumor
- Mainly in parotid gland
- Low grade malignant tumor
- 3% of salivary glad tumor, 90% in parotid
- Can involve facial nerve or neck nodes
- Mets to lungs and vertebra
- 5 year survival – 85%
Malignant Mixed tumor
- Worst prognosis
- Types:
- Ca. ex pleomorphic adenoma (commonest)
Most aggressive tumor
Radical Parotidectomy
- Primary Malignant mixed tumor
- Metastasizing mixed tumors
- 5years survival - <50%
Squamous cell Ca
- Rare
- High grade
- Common in 6th-7th decade
- Rapidly growing, pain, facial palsy, skin fixity, ulceration
- Poor prognosis
- Radical parotidectomy and RT
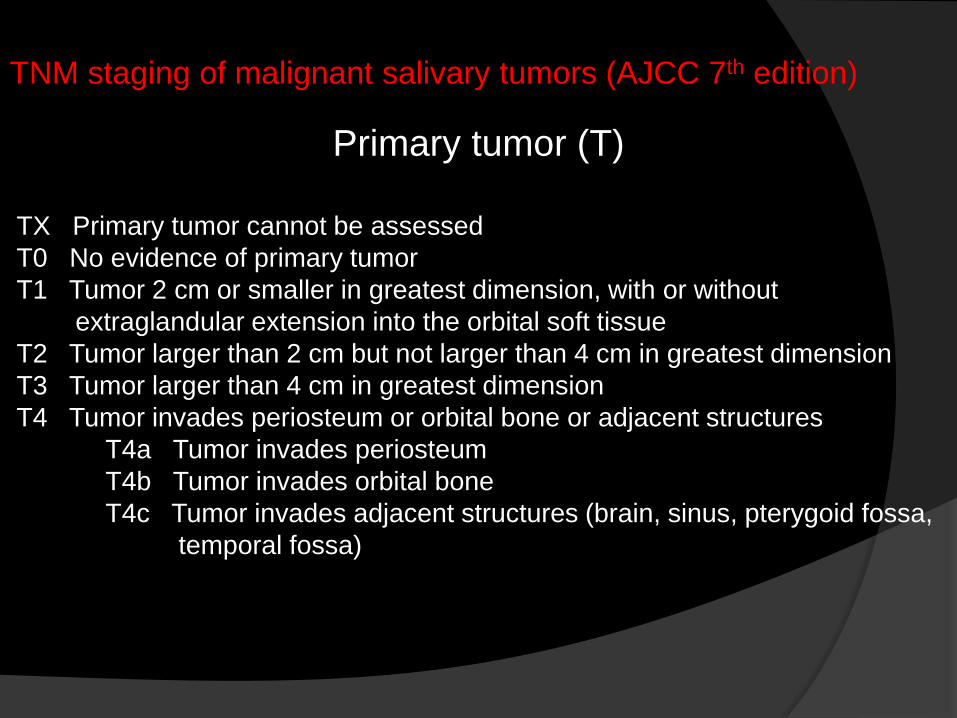
TNM staging of malignant salivary tumors (AJCC 7th edition)
Primary tumor (T)
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or smaller in greatest dimension, with or without
extraglandular extension into the orbital soft tissue
T2 Tumor larger than 2 cm but not larger than 4 cm in greatest dimension
T3 Tumor larger than 4 cm in greatest dimension
T4 Tumor invades periosteum or orbital bone or adjacent structures
T4a Tumor invades periosteum
T4b Tumor invades orbital bone
T4c Tumor invades adjacent structures (brain, sinus, pterygoid fossa,
temporal fossa)
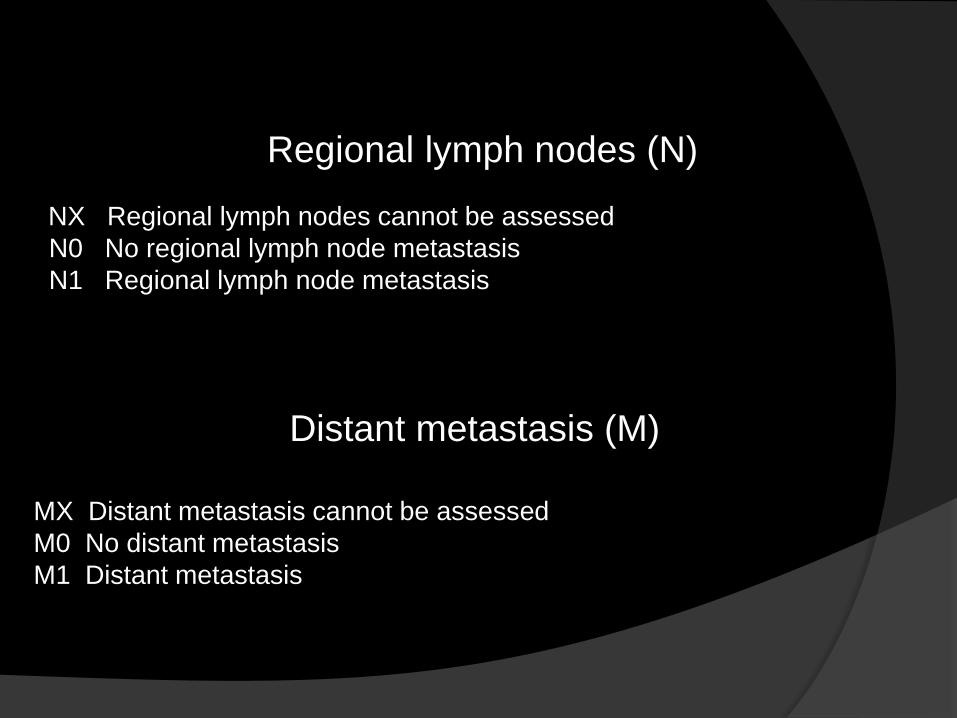
Regional lymph nodes (N)
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Regional lymph node metastasis
Distant metastasis (M)
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
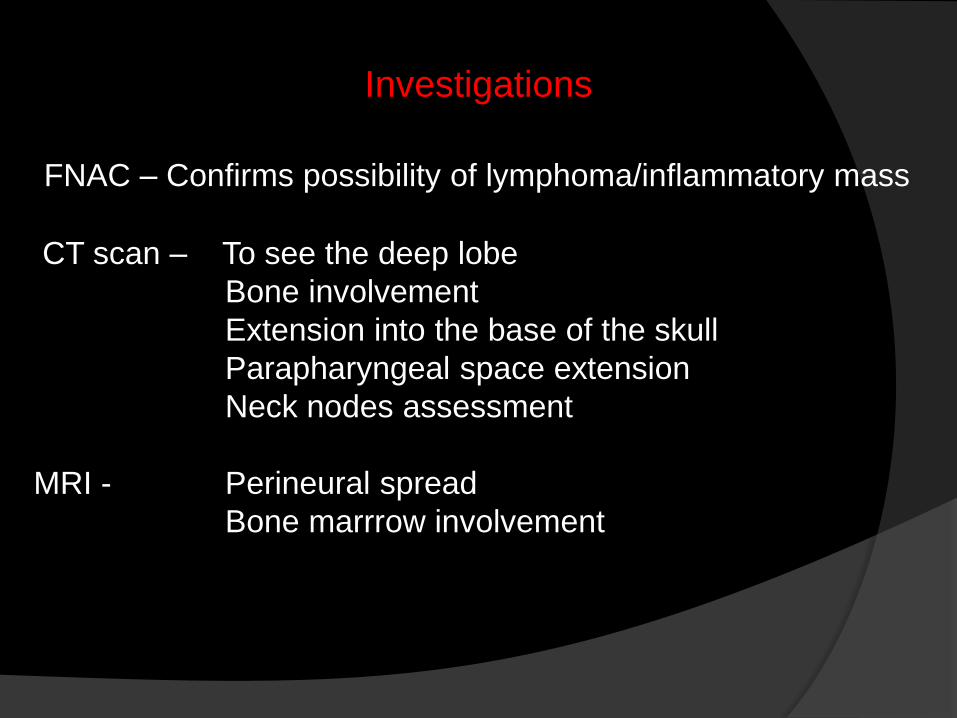
Investigations
FNAC – Confirms possibility of lymphoma/inflammatory mass
CT scan – To see the deep lobe
Bone involvement
Extension into the base of the skull
Parapharyngeal space extension
Neck nodes assessment
MRI - Perineural spread
Bone marrrow involvement
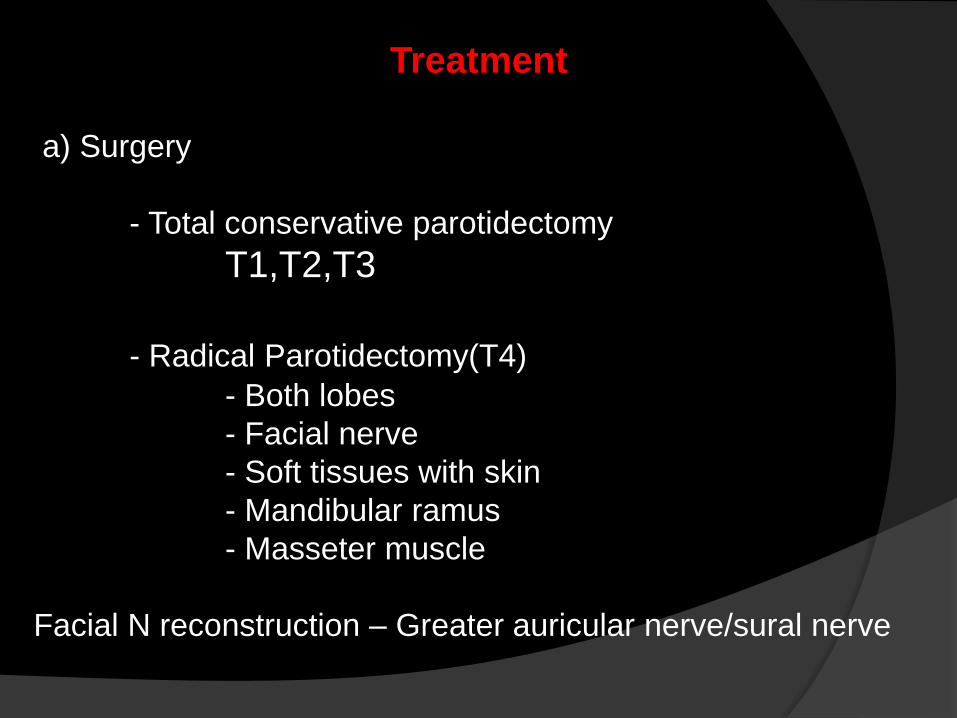
Treatment
a) Surgery
- Total conservative parotidectomy
T1,T2,T3
- Radical Parotidectomy(T4)
- Both lobes
- Facial nerve
- Soft tissues with skin
- Mandibular ramus
- Masseter muscle
Facial N reconstruction – Greater auricular nerve/sural nerve
b) Radiotherapy
3-6 weeks after surgery
Delayed for 6 weeks if nerve grafting is done
Dose – 50-70 Gy (1.5 - 2Gy in 5-8 weeks.
c) Chemotherapy
5FU
Cisplatin
Doxurubicin
Epirubicin
Parotidectomy
Superficial parotidectomy:
Most common procedure of parotid pathology
With/without hypotensive anesthesia
Reduce blood loss
Improve visual surgical field
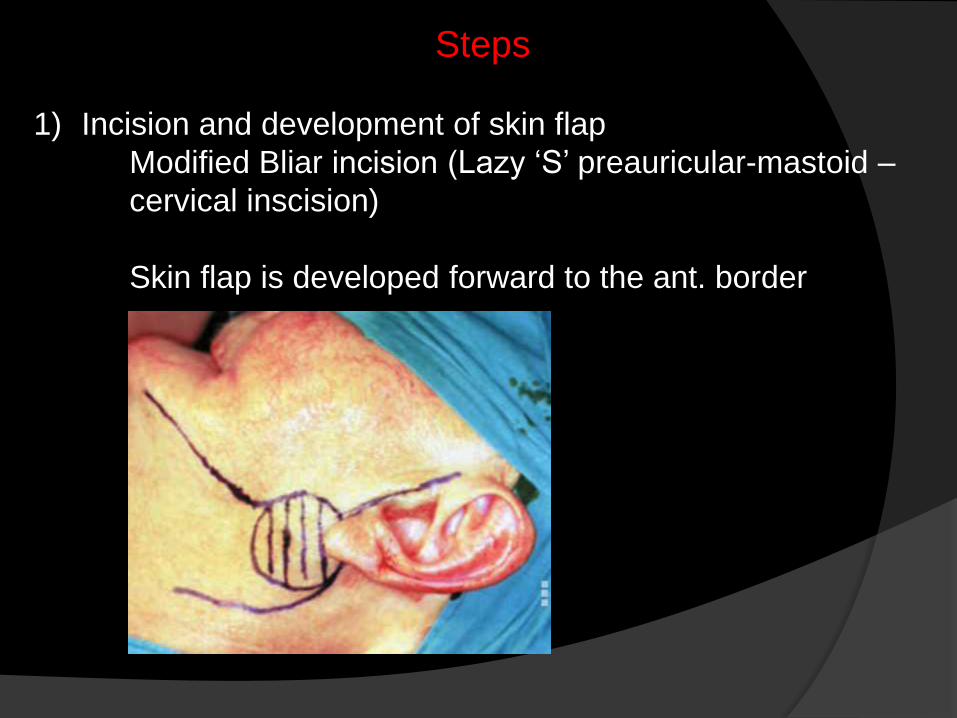
Steps
1) Incision and development of skin flap
Modified Bliar incision (Lazy ‘S’ preauricular-mastoid –
cervical inscision)
Skin flap is developed forward to the ant. border
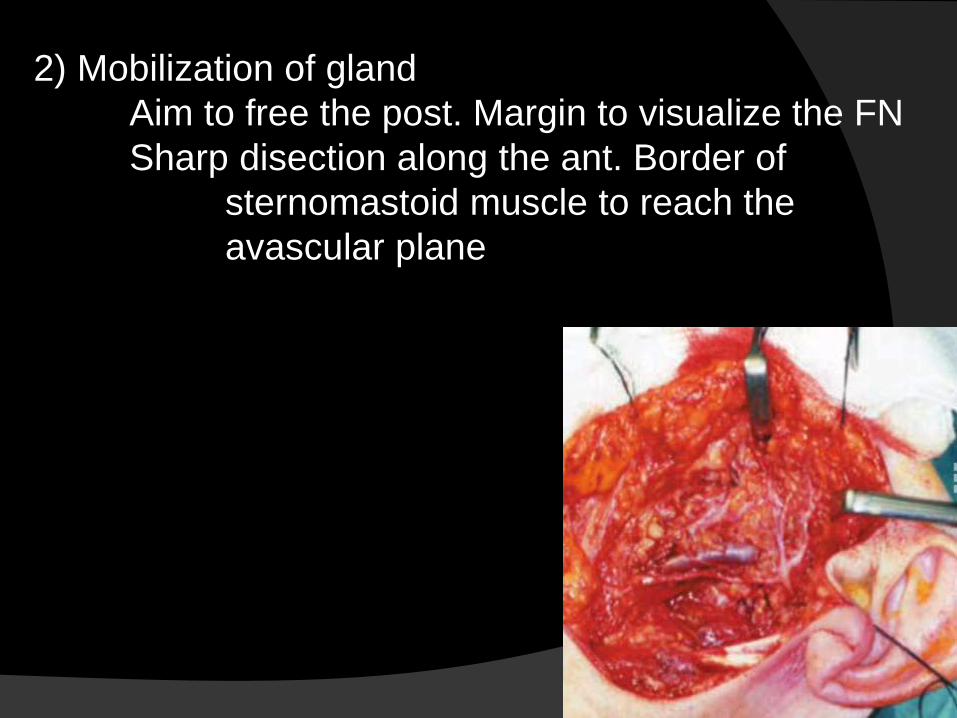
2) Mobilization of gland
Aim to free the post. Margin to visualize the FN
Sharp disection along the ant. Border of
sternomastoid muscle to reach the
avascular plane
3) Location of the FN trunk
Landmark to identify FN
Colney’s pointer
Upper border of post. belly of digastric M
Retrograde tracing
4) Dissection of the gland
From superior to inferior direction
Upper div. is usually tortuous & can be damaged
easily
5) Closure – Trendelenburg position to identify any
residual bleeding.
Complications of parotidectomy
- Haematoma
- Infection
- Temporary facial weakness
- Permanent facial weakness
- Permanent numbness of ear lobe
- Frey’s syndrome
Frey’s syndrome
(gustatory sweating)
- Considered an inevitable consequence of parotidectomy,
unless preventative measures are taken
- Sweating, redness and warmth in the preauricular region
while eating
- Damage of autonomic innervation – inappropriate
regeneration of parasympathetic postganglionic fibers into
the skin overlying the parotd- sweating.
Diagnosis
Minor’s test (iodine test)
Iodine applied over affected area
Dry starch applied over it
Turns blue in the presence of sweat.
Prevention:
Barrier between skin and parotid bed
Sternomastoid muscle flap
Temporalis fascia flap
Artificial membrane
Management of established Frey’s syndrome
- Antiperspirants
- Anticholinergic lotion
- Denervation by tympanic neurectomy
- Injection of botulinum toxin into the affected
skin.
THANK YOU