
Parenteral Nutrition in the NICU
13
DOI: 10.1542/neo.12-3-e130 2011;12;e130-e140 NeoReviews Nahed O. ElHassan and Jeffrey R. Kaiser Parenteral Nutrition in the Neonatal Intensive Care Unit http://neoreviews.aappublications.org/cgi/content/full/neoreviews;12/3/e130 located on the World Wide Web at: The online version of this article, along with updated information and services, is Online ISSN: 1526-9906. Illinois, 60007. Copyright © 2011 by the American Academy of Pediatrics. All rights reserved. by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, it has been published continuously since 2000. NeoReviews is owned, published, and trademarked NeoReviews is the official journal of the American Academy of Pediatrics. A monthly publication,
-
Upload
suparno-adi-santika -
Category
Documents
-
view
18 -
download
1
description
nutrisi parenteral yang digunakan di NICU
Transcript of Parenteral Nutrition in the NICU

DOI: 10.1542/neo.12-3-e130 2011;12;e130-e140 NeoReviews
Nahed O. ElHassan and Jeffrey R. Kaiser Parenteral Nutrition in the Neonatal Intensive Care Unit
http://neoreviews.aappublications.org/cgi/content/full/neoreviews;12/3/e130located on the World Wide Web at:
The online version of this article, along with updated information and services, is
Online ISSN: 1526-9906. Illinois, 60007. Copyright © 2011 by the American Academy of Pediatrics. All rights reserved. by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village,it has been published continuously since 2000. NeoReviews is owned, published, and trademarked NeoReviews is the official journal of the American Academy of Pediatrics. A monthly publication,

Parenteral Nutrition in theNeonatal Intensive Care UnitNahed O. ElHassan, MD,
MPH,* Jeffrey R. Kaiser,
MD, MA†
Author Disclosure
Drs ElHassan and
Kaiser have disclosed
no financial
relationships relevant
to this article. This
commentary does
contain a discussion
of an unapproved/
investigative use of a
commercial
product/device.
AbstractNeonatal parenteral nutrition (PN) is readily available in many hospitals and plays anessential role in the management of sick and growing preterm and term infants. PNcan be used as the sole source of nutrition support for infants who cannot be fed or asan adjunct to enteral feeding. Preterm infants are a particularly vulnerable populationbecause they are born at a time, if they had remained in utero, of rapid intrauterinebrain and body growth. The impact of early malnutrition can have long-lastingnegative effects on central nervous system development and growth. Despite this, PNis often provided to preterm infants based on local traditions rather than experimentalevidence. The quality of PN and its early initiation are critical in providing the mostadequate substrates for appropriate development. This article reviews the energy andfluid requirements of infants and presents by component (protein, carbohydrates,lipids, minerals such as calcium and phosphorus, trace elements, and multivitamins)the available literature on neonatal PN and its complications. In addition, suggestedguidelines for PN administration for preterm and term neonates are presented.
Objectives After completing this article, readers should be able to:
1. Describe the different components of PN for neonates.2. Review the suggested recommendations for macro/micronutrients in PN for neonates.3. Understand the function and benefits of macro/micronutrients in PN for neonates.4. Discuss the neonatal morbidities and possible complications associated with each of
the PN components.
IntroductionNeonatal PN was first used in 1967 for an infant who had intestinal atresia and postoper-ative weight loss. (1) The goal of PN in preterm neonates has been to approximate the
nutrition they would have received if they have remained inutero for appropriate extrauterine growth and development.(2) PN can be used as the sole source of nutrition support forneonates who cannot be fed or as an adjunct to enteralfeeding. Since its implementation, many lessons have beenlearned about the benefits and complications of PN. Animportant milestone in neonatal nutrition research was therealization of the valuable impact of early initiation onneurocognitive development. Despite this fact, the clinicalpractice of providing PN is often based on local tradition anddogma rather than experimental evidence. (2)(3) Althoughfetuses receive continuous nutrition from the placentathrough the umbilical vein, many preterm newborns haveessential nutrients limited or entirely withheld due totheoretical concerns and previous experiences with olderPN preparations. The quality of PN and its early initiationare critical in providing the most appropriate substrates for
*Assistant Professor of Pediatrics, Department of Pediatrics, Neonatology, University of Arkansas for Medical Sciences, Collegeof Medicine, Arkansas Children’s Hospital, Little Rock, AR.†Associate Professor, Departments of Pediatrics and Obstetrics and Gynecology, Neonatology, University of Arkansas forMedical Sciences, College of Medicine, Arkansas Children’s Hospital, Little Rock, AR.
Abbreviations
AA: amino acidALA: alpha-linolenic acidBUN: blood urea nitrogenCa: calciumEFAD: essential fatty acid deficiencyELBW: extremely low birthweightFDA: United States Food and Drug AdministrationFFA: free fatty acidLA: linoleic acidP: phosphorusPN: parenteral nutritionVLBW: very low birthweight
Article parenteral nutrition
e130 NeoReviews Vol.12 No.3 March 2011

appropriate growth and development. (2)(3) This articleaims to discuss the “art and science” of PN in neonatesand reviews the benefits and potential complications ofthe multiple components provided in PN for pretermand term neonates. When there is limited evidence, andrecommendations are made, this is stated. Definitions ofpreterm infants for this article are stated in Table 1.
Energy RequirementsKnowing the appropriate energy requirements for neo-nates is fundamental in prescribing PN. Energy is essen-tial for body maintenance and growth. The basal restingmetabolic rate reflects the energy expenditure requiredfor maintenance of vital processes. The resting metabolicrate has been estimated to be 40 to 60 kcal/kg per day inparenterally fed neonates maintained in a thermoneutralenvironment. (4) Each gram of weight gain for growth,including the stored energy and the energy costs ofcomponent synthesis, requires between 3 and 4.5 kcal.(4) Thus, an ideal daily weight gain of 15 g/kg (whichestimates daily fetal growth) requires an additional ca-loric requirement of 45 to 67 kcal/kg above the esti-mated resting metabolic rate. (4) A summary of theenergy requirements during the neonatal period is pre-sented in Table 2. These estimated energy requirementshave been calculated in healthy growing preterm in-fants at 3 to 4 weeks of age. There is relatively minimalinformation, however, on the energy requirements forsick infants and especially extremely low-birthweight(ELBW) infants during early postnatal life. ELBW in-fants are believed to have increased metabolic demandsdue to their large body proportion of metabolically activeorgans, including the heart, liver, kidney, and brain. (4)
Fluid RequirementsThe percentage of total body water in fetuses decreasesfrom approximately 95% early in development to 80%by 8 months’ gestation and to 75% at term. (5) Duringthe first day after birth, term infants require a minimum
of 60 mL/kg per day to meet maintenance fluid needs(replacing net losses). As infants mature, fluid needsgradually increase to a total of 120 to 150 mL/kg per dayto allow for increased renal solute load, stool wateroutput, and growth. (5) Preterm infants have more in-sensible water losses than term infants due to their largesurface area, skin immaturity, and ensuing increasedevaporation. Thus, fluid needs are higher on the firstpostnatal day at 80 to 100 mL/kg per day and increaseby 10 to 20 mL/kg per day to a total of 130 to 180 mL/kgper day as preterm infants mature (Table 2). (5)
Infusion RoutesPN may be infused via peripheral and central catheters.Peripheral infusion typically is used for short-term nutri-tion support. Peripheral vein osmolarity tolerance rangesfrom 700 to 1,000 mOsm/L. Osmolarity is calculatedusing the equation: (6)
osmolarity (mOsm/L)�([amino acids (g/L) � 8]� [glucose (g/L) � 7] � [sodium (mEq/L) � 2]� [phosphorus (mg/L) � 0.2] � 50)
The osmolarity of glucose solutions rises from 255 to1,020 mOsm/L with increasing concentration from 5%to 20%, respectively. Generally, glucose concentrationsof 12.5% or less are well tolerated by peripheral veins aslong as no other osmolarity-increasing agents are added.Central infusion of PN is delivered via central venouscatheters and is the preferred route for long-term PN.
Components of Parenteral Nutrition (Table 2)Protein
Previously used intravenous amino acid (AA) prepara-tions were based on casein hydrolysates. Current crystal-line AA solutions have elevated ratios of essential tononessential AAs, leading to the endogenous produc-tion of higher concentrations of the branch amino acids:leucine, isoleucine, and valine. (7) Despite extensiveendeavors to create optimized AA preparations, how-ever, plasma AA concentrations in infants receiving cur-rent intravenous solutions are still reduced comparedwith breastfed infants. (8) This is partly due to the poorsolubility or stability of various intravenous AAs (eg,glutamine, tyrosine, and cysteine). (8) Cysteine is oftenconsidered a semi-essential AA in the newborn periodand is, therefore, routinely added to AA preparationsto circumvent low cysteine synthesis, low plasma concen-trations, and impaired protein synthesis. (9) Cysteine isa major substrate for glutathione, a tripeptide (glutamicacid/cysteine/glycine) antioxidant, and is important inmaintaining redox potential and calcium homeostasis.
Table 1. Classification of PretermInfants• Preterm infants are born <37 weeks’ gestation.• Low-birthweight infants weigh <2,500 g at birth.• Very low-birthweight infants weigh <1,500 g at
birth.• Extremely low-birthweight infants weigh <1,000 g
at birth.
parenteral nutrition
NeoReviews Vol.12 No.3 March 2011 e131

Tab
le2.
Sugg
este
dRe
com
men
dati
ons
for
Pare
nter
alN
utrit
ion
Mac
ronu
trie
nts
for
Neo
nate
s
Sour
ceIn
itial
Adm
inis
trat
ion
Adva
ncem
ent
Goal
Neo
nate
Bloo
dCo
ncen
trat
ion
Pote
ntia
lCom
plic
atio
ns
Flui
d60
to70
mL/
kgpe
rda
y80
to10
0m
L/kg
per
day
10to
20m
L/kg
per
day
10to
20m
L/kg
per
day
130
to15
0m
L/kg
per
day
130
to18
0m
L/kg
per
day
Term
Pret
erm
——
Tota
lEne
rgy
Inta
ke—
—90
kcal
/kg
per
day
Term
——
120
kcal
/kg
per
day
Pret
erm
Ener
gyEx
pend
ed40
to60
kcal
/kg
per
day
Rest
ing
met
abol
icra
te40
to50
kcal
/kg
per
day
Activ
ity0
to5
kcal
/kg
per
day
Ther
mor
egul
atio
n0
to5
kcal
/kg
per
day
Synt
hesi
s15
kcal
/kg
per
day
Ener
gyEx
cret
ed15
kcal
/kg
per
day
Ener
gySt
ored
20to
30kc
al/k
gpe
rda
yAm
ino
Acid
s12
to3
g/kg
per
day
1g/
kgpe
rda
y3
g/kg
per
day
Term
—Ch
oles
tasi
s2
to3
g/kg
per
day
0.5
to1
g/kg
per
day
3.5
to4
g/kg
per
day
Pret
erm
Dext
rose
8m
g/kg
per
min
ute
4to
6m
g/kg
per
min
ute2
1to
3m
g/kg
per
min
ute
1to
3m
g/kg
per
min
ute
12m
g/kg
per
min
ute
12m
g/kg
per
min
ute
Term
Pret
erm
>45
to<
150
to22
0m
g/dL
>45
to<
150
to22
0m
g/dL
Hyp
ergl
ycem
iais
asso
ciat
edw
ith:
1.De
ath
2.Pr
olon
ged
hosp
itals
tay
3.In
trav
entr
icul
arhe
mor
rhag
eGr
ade
3&
44.
Nec
rotiz
ing
ente
rcol
itis
5.Se
psis
Fat3
2to
3g/
kgpe
rda
y0.
5to
1g/
kgpe
rda
y3
to3.
5g/
kgpe
rda
yTe
rm<
150
to25
0m
g/dL
4Ch
oles
tasi
s2
to3
g/kg
per
day
0.5
to1
g/kg
per
day
3to
3.5
g/kg
per
day
Pret
erm
<15
0to
250
mg/
dL4
1E
arly
and
aggr
essi
vede
liver
yof
amin
oac
ids
does
not
lead
toth
ede
velo
pmen
tof
azot
emia
,hyp
eram
mon
emia
,or
met
abol
icac
idos
is.
2G
luco
sein
fusi
onra
teis
som
etim
eslim
ited
to4
mg/
kgpe
rm
inut
ein
extr
emel
ylo
w-b
irth
wei
ght
infa
nts
who
have
hype
rgly
cem
ia.
320
%in
trav
enou
sfa
tem
ulsi
ons
are
typi
cally
used
and
infu
sed
over
24ho
urs
tom
axim
ize
clea
ranc
e.4So
me
drug
s(e
g,am
phot
eric
inB
and
ster
oids
)le
adto
elev
ated
trig
lyce
ride
conc
entr
atio
ns.
parenteral nutrition
e132 NeoReviews Vol.12 No.3 March 2011

(9) Because the inclusion of cysteine in AA solutions istechnically difficult due to its low solubility, it is typicallyadded last to the solution at a dose of 30 to 40 mg/g AA.Cysteine also decreases the pH of AA solutions andreduces calcium and phosphorus precipitation. (10)
Protein accretion rates by fetuses at 24 to 25 weeks’,27 to 28 weeks’, and 30 to 32 weeks’ gestation have beenestimated to be 4.0, 3.6, and 3.3 g/kg per day, respec-tively. (11)(12) Infusion of AA with glucose as early asthe first postnatal day decreases protein catabolism andenhances net protein accretion. (13)(14) Thus, reducingthe number of hours that infants receive suboptimalnutrition (without AAs) has been emphasized recently asan important goal of neonatal intensive care. (13)(14)(15) The purpose of early AA supplementation is toprovide preterm infants with substrate that promotesprotein deposition that closely approximates fetal energyproduction and growth. (13) For most preterm infants,1.0 to 1.5 g/kg per day of intravenous AA along withglucose prevents protein catabolism. (15) When nonpro-tein energy intake is 80 to 85 kcal/kg per day and AAintake is 2.7 to 3.5 g/kg per day, nitrogen retention andgrowth might actually approach the intrauterine rate.(16) Recent studies have challenged the older practice ofstarting at 0.5 to 1 g/kg per day of AA and graduallyadvancing the AA infusion rate. (13)(14)(15)(16)(17)(18) In a retrospective study, Valentine and associates(13) suggested that providing 3 g/kg per day ofAA within 24 hours of birth to very low-birthweight(VLBW) infants was safe and associated with betterweight gain and shorter duration of PN administration.ELBW infants may require up to 4 g/kg per day ofintravenous AA to maintain stores and promote growth.(15) More research is needed to establish the optimal AArequirements in critically ill infants and in those who havesepsis and renal and hepatic dysfunction.
The major concerns about early and aggressive deliv-ery of AA, especially to ELBW infants, are the develop-ment of azotemia, hyperammonemia, and metabolic ac-idosis. These complications of PN were reported usingearlier AA preparations and rarely occur with currentcrystalline solutions. Blood urea nitrogen (BUN) repre-sents the complex interaction of hydration status, renalfunction, energy quality and quantity, and degree ofillness. (19)(20)(21) Rising BUN values are, therefore,not just a reflection of the ELBW infant’s intolerance toAA infusion. (19)(20)(21) In fact, studies of fetal AAoxidation suggest that higher BUN reflects appropriateAA utilization for both energy and lean mass production.In addition, metabolic acidosis during the first postnatalweek occurs independently of the duration and amount
of AA delivery. (20) Metabolic acidosis in VLBW infantscan be caused by multiple factors (eg, defects of urinaryacidification, acute illness, hypotension, poor perfusion)and cannot be solely attributed to AA administration.(21) Prolonged exposure to intravenous AA solutionsdoes contribute to the development of PN-associatedcholestasis. (22)
CarbohydrateGlucose is transported across the placenta via facilitateddiffusion and is the principal energy substrate for thefetus. The primary storage form of glucose is glycogen,which is only produced during the third trimester. Glu-cose is the chief energy source for the neonatal brain andis of paramount importance for preterm infants who, inaddition to having limited glycogen stores, also haveespecially metabolically active organs. (7) Endogenousglucose production varies with age and was estimated tobe 8 mg/kg per minute in term newborns and 6 mg/kgper minute in preterm infants. (23)(24) These produc-tion rates provide an appropriate starting point for glu-cose infusion rates in PN for term and preterm infants.The upper rate of glucose administration is dictated bythe maximal glucose oxidative capacity for energy pro-duction and glycogen deposition. When glucose is givenin excess, it is converted into lipid via lipogenesis. Thisconversion is inefficient, increases energy expenditure,and may have additional clinical consequences via in-creased carbon dioxide production and exacerbation oflung disease. (23)(25)(26) The maximum glucose oxi-dation capacity is 12 mg/kg per minute in term new-borns and preterm infants receiving long-term PN (27)and generally should not exceed this concentration. Ges-tational age and clinical status modify glucose oxidativecapacity. For example, it has been estimated to be7 mg/kg per minute in preterm infants during the first2 postnatal weeks and 5 mg/kg per minute in critically illchildren who have burns. (28)
The minimum recommended blood glucose concen-tration is 45 mg/dL (2.5 mmol/L). (8) Despite limitedglycogen storage capacity, ELBW infants often experi-ence episodes of hyperglycemia during the first few post-natal days. This may be due to surges in glucose produc-tion caused by birth-related increases in catecholamines,possibly compounded by an exogenous supply of cat-echolamines and inotropic drugs, a decrease in endoge-nous production of insulin, and an increase in peripheraland hepatic insulin resistance. (7) In addition, ELBWinfants often fail to suppress endogenous glucose pro-duction completely in response to an exogenous supplyof PN glucose. (29) Although there is no consensus
parenteral nutrition
NeoReviews Vol.12 No.3 March 2011 e133

definition of hyperglycemia, especially in ELBW infants,a suggested range may be 150 to 220 mg/dL (8.3 to12.2 mmol/L). (29) The primary concern for hyper-glycemia in infants is its association with death, pro-longed hospitalization, intraventricular hemorrhagegrades 3 and 4, necrotizing enterocolitis, and late-onsetbacterial and fungal sepsis. (29) Early AA supplementa-tion on the first day after birth seems to stabilize highblood glucose concentrations by stimulating endoge-nous insulin secretion. (7) Other interventions for hyper-glycemia include reducing the glucose infusion rate ortreating with intravenous insulin. (29) Of note, a Coch-rane review evaluating these two strategies for treatmentof hyperglycemia found no difference in death or seriousmorbidities. (29) A randomized trial in preterm infantswho have hyperglycemia needs to be conducted to ad-dress this question.
There is also a concern about the potential risk oflactic acidemia in infants receiving high insulin and glu-cose administration. (7) Because the safety of insulintherapy and its impact on hyperglycemia-related morbid-ities have not been established, the consensus in theliterature points toward incrementally decreasing theglucose infusion rate to approximately 4 mg/kg perminute and reserving insulin use for infants whose bloodglucose concentrations are greater than 250 mg/dL(13.9 mmol/L) while receiving this infusion rate.
LipidsLipid emulsions are especially important components ofneonatal PN because they supply an energy source thathas low osmolarity and high energy content per unitvolume. (30) Intravenous fat emulsions currently avail-able in the United States are 10% (1.1 kcal/mL) or20% (2 kcal/mL) soy or soy/safflower oil-based emul-sions. (30) The 10% emulsion is typically not used be-cause it contains high amounts of phospholipids that cancontribute to hyperphospholipidemia and subsequenthypercholesterolemia. (8)
It is crucial to provide a minimum of 0.5 to 1.0 g/kgper day of lipids to prevent essential fatty acid deficiency(EFAD), which can develop in preterm infants duringthe first postnatal week and as early as the second dayafter birth. (8)(18)(30)(31) Essential fatty acids havedouble bonds in the �-6 and �-3 positions and cannot besynthesized endogenously by humans. (31) Therefore,specific �-6 and �-3 fatty acids or their precursors withdouble bonds at these positions (ie, linoleic acid [LA,18:2 �-6] and alpha-linolenic acid [ALA, 18:3 �-3])must be provided in PN. (12) LA and ALA have criticalroles in postnatal brain development. EFAD is associated
with poor growth, scaly skin lesions, and visual andneurologic abnormalities and has been observed in in-fants who have been maintained for several weeks on PNwithout essential fatty acids.
Because lipids are the primary source of energy supplyin PN, inadequate lipid intake can lead to caloric under-nutrition and proteolysis. (32)(33) Although it has beencommon practice to increase lipid intake incrementallyover several days in preterm infants requiring PN, thereis no scientifically valid argument why these newbornsshould not be offered 2 to 3 g/kg per day of AA and 2 to3 g/kg per day of lipids immediately after birth. In fact,it has been shown that provision of 3.5 g/kg per day ofAA and 3 g/kg per day of lipids within the first 24 hoursof birth to VLBW infants was well tolerated and withoutadverse effects. (34) In addition, despite phobias aboutbeginning lipids early, a Cochrane meta-analysis reportedno increased risk of necrotizing enterocolitis, sepsis,thrombocytopenia, or significant jaundice or increasedduration of ventilation when lipids were introduced early(�12 hours) versus later (�6 days). (35)
Moreover, several investigators have shown that in-fants treated with the “traditional” practices of restrictedprotein supplementation and limited energy supply dur-ing the immediate postnatal period had significant post-natal growth restriction and poor neurodevelopmentaloutcomes. (36)(37)(38) Ehrenkranz and associates (37)showed that increased growth velocity in ELBW new-borns (presumably due to better nutrient intake) exerts asignificant positive influence on neurodevelopment andgrowth outcomes at 18 to 22 months corrected age. Inaddition, preterm infants who had increased energy sup-ply during the first postnatal week have been shown tohave a 4.6-point increase in Bailey Mental DevelopmentIndex for each additional 10 kcal/kg per day they re-ceived. (36) Although data showing the specific benefitsof early initiation of lipids are limited, early and aggres-sive supplementation has not been associated with in-creased adverse effects. Lipids may be initiated earlyduring the first day after birth at doses of more than 1 to2 g/kg per day to increase energy supply and improvelong-term growth and neurodevelopment.
The maximum lipid dose is determined by an infant’sability to metabolize fat emulsions. (30) Lipoproteinlipase in the capillary endothelium of extrahepatic tissues,hepatic lipase in the endothelium of hepatic capillaries,and lecithin cholesterol acyltransferase are the three en-zymes that determine the rate of PN lipid clearance. (39)Although high doses of heparin can stimulate lipoproteinlipase activity, heparin infusion does not improve theutilization of intravenous lipids because it also causes an
parenteral nutrition
e134 NeoReviews Vol.12 No.3 March 2011

increase in free fatty acids (FFAs) beyond the infant’sclearance ability. (40) Intravenous lipids should be in-fused over 24 hours to maximize clearance. (13) Whenthe lipid infusion rate exceeds hydrolysis rates, concen-trations of plasma triglycerides and FFAs increase. Al-though there is no clear consensus in the literature,current recommendations for maximal plasma triglycer-ide concentrations range between 150 mg/dL and250 mg/dL. (7)(13)(18)(30)
Some drugs and medical conditions lead to elevatedserum triglyceride concentrations. (30) Liposomal am-photericin B contains fat emulsion (30) and steroids,such as hydrocortisone, that can lead to transient in-creases in triglyceride concentrations. (30)
Carnitine facilitates the transport of long-chain fattyacids across the mitochondrial membrane, making themavailable for beta-oxidation. (40) Studies evaluating car-nitine supplementation in infants and children, however,have yielded controversial results. Carnitine concentra-tions decrease during prolonged carnitine-free PN, espe-cially in immature preterm infants, (40) but a meta-analysis showed no benefit of carnitine supplementationon lipid tolerance, ketogenesis, or weight gain in infantsrequiring PN. (41) Nonetheless, carnitine supplementa-tion at 2 to 10 mg/kg is recommended in infants exclu-sively receiving PN for more than 4 weeks. (18)
Intravenous fat emulsions used in the United Statesare comprised of either soybean oil or a combination ofsafflower and soybean oil and are rich in proinflammatory�-6 fatty acids. (42) Many clinicians believe that the high�-6 content of these fat emulsions contribute to PN-associated cholestasis. (43)
Another fat emulsion prepared from fish oils that isnot yet approved for use in the United States has beenshown to reverse cholestasis in infants six times fasterthan in those receiving soybean oil-based fat emulsions,probably because this emulsion has �-3 fatty acids thathave anti-inflammatory properties. (43)(44) In addition,use of the fish oils emulsion is not associated with hyper-triglyceridemia, coagulopathy, or EFAD. (43)(44) Cur-rently, this emulsion can only be prescribed in the UnitedStates via United States Food and Drug Administration(FDA) compassionate approval.
Calcium (Ca) and Phosphorus (P)Although there is no consensus on optimal parenteralrequirements for Ca and P, the third-trimester fetal ac-cretion rates of 3.5 mmol/kg per day (140 mg/kg perday) for Ca and 2.4 mmol/kg per day (75 mg/kg perday) for P are often used. (11) Fetal accretion rates peakduring the third trimester, with upwards of 80% of fetal
skeletal mineralization taking place during this period.(11) Thus, the goal of PN in preterm infants is to achieveintrauterine rates of bone mineralization, and preterminfants who lack part or all of the fetal third trimester areat increased risk of osteopenia. (8)(11)(18) Unfortu-nately, due to delayed establishment of full enteral feed-ings, prolonged PN, and chronic use of certain medica-tions (diuretics and corticosteroids) that increase mineralexcretion, attaining this goal is often very difficult. (11)
Further, the ability to provide neonates with the rec-ommended amounts of Ca and P has been limited in theUnited States by their precipitation in PN solution. (45)(46) The solubility of Ca and P are affected by pH,temperature, Ca and P concentrations, AA product andconcentration, lipid emulsions, dextrose, and magne-sium concentration. Another very critical component ofCa-P compatibility has been the type of phosphate saltsused. Organic phosphate, used in Europe and Canada,has far superior compatibility with Ca salts than inorganicphosphate, approved for use in the United States. (45)(46) Organic phosphates consist of a phosphate groupcovalently bonded to an organic molecule such as glyc-erol, glucose, or fructose. The phosphate group, there-fore, cannot be fully ionized and is much less available tointeract with Ca. (46) As natural substrates for extra-cellular phosphatases, nutritional bioavailability of or-ganic phosphates is assured. In addition, organic phos-phates are well tolerated without significant toxicity. (46)
In the United States, P is typically supplemented assodium phosphate, a constituent contaminated by alumi-num. The FDA guidelines for aluminum content recom-mend PN components to have less than 4 to 5 �g/kg perday. (47) Aluminum overexposure may cause hypochro-mic microcytic anemia, neurotoxicity, and metabolicbone disease in which infants chronically exposed toparenteral aluminum have reduced lumbar spine and hipbone mass during adolescence. (47)(48) Although it isdifficult to adhere to the current FDA recommendationsbecause of the high aluminum content in PN compo-nents, one method to reduce aluminum intake is to usesodium phosphate (9.5 mg of aluminum/mmol) ratherthan potassium phosphate (24 mg of aluminum/mmol).
Ca in PN is typically provided as Ca gluconate, a saferchoice than calcium chloride. (45) The 12-carbon or-ganic gluconate salt of Ca is only partially ionized inaqueous solutions, and the degree of its dissociationdecreases as the concentration increases. (45) This de-crease in the availability of freely dissociated Ca ions issufficient to reduce the potential for precipitation withphosphate ions. In contrast, the dissociation of Ca ions
parenteral nutrition
NeoReviews Vol.12 No.3 March 2011 e135

from the inorganic chloride salt is constant, irrespectiveof its final concentration.
Trace ElementsTrace mineral preparations are commercially availableas single agents or as combination products. Thetrace elements currently recommended for neonatal PNare zinc, copper, manganese, chromium, selenium, andmolybdenum. Although the optimum time to start traceelements supplementation has not undergone extensive
testing, most neonatologists begin supplementationwithin the first few days after birth (11) and provide itdaily in PN. A summary of trace element doses, func-tions, deficiencies, and toxicities is shown in Tables 3and 4.
None of the combination preparations of neonataltrace elements meet the needs of every gestational orpostnatal age or clinical condition, and manganese con-tent may be up to five times the recommended dose inthe currently available combination preparations. (11)
Table 3. Trace Elements in Neonatal Parenteral Nutrition (PN)1
Dosing Category(weight)
Zinc2
(�g/kg per day)Copper3(�g/kg per day)
Manganese3
(�g/kg per day)Chromium4,5
(�g/kg per day)Selenium2,5
(�g/kg per day)
<3 kg 400 20 1.0 0.05 to 0.2 2>3 to 10 kg 200 20 1.0 0.2 2>10 to 15 kg 100 20 1.0 0.14 to 0.2 21Molybdenum at 1 �g/kg per day is recommended for low-birthweight infants receiving PN for more than 4 weeks. (11)(18)2Infants who have short bowel syndrome lose significant amounts of zinc and selenium in diarrhea and small bowel effluent, necessitating close monitoringof serum zinc and selenium. (11)(18)3Copper supplementation is limited to 10 �g/kg per day, and no manganese is given to infants who have cholestasis. (11)(18)4Chromium is a contaminant of PN solutions that results in a 10% to 100% increase in amount of chromium delivered, necessitating serum chromiummonitoring for infants receiving long-term PN. (11)(18)5No chromium or selenium supplementation is recommended for infants who have chronic renal failure. (11)(18)
Table 4. Function, Deficiencies, and Toxicities of Trace Elements (11)(18)
Trace Elements Function Reported Deficiencies Reported Toxicities
Zinc Important component of severalenzymes (eg, carbonic anhydraseand carboxypeptidase), importantfor growth
Failure to thrive, alopecia, diarrhea,dermatitis (commonly perianal),ocular changes, rash (crusted,erythematous, involving face,extremities, and anogenitalareas), nail hypoplasia ordysplasia
Depresses phagocytic andbacterial leukocyticactivity, pancreatitis
Copper Component of several enzymes suchas cytochrome oxidase,superoxidase dismutase,monoamine oxidase, andlysyl oxidase
Anemia, osteoporosis,depigmentation of hair andskin, neutropenia, poor weightgain, hypotonia, and ataxialater in life
Hepatic cirrhosis
Manganese Role in enzyme activation (eg,superoxide dismutase), importantfor normal bone structure, rolein carbohydrate metabolism
Nausea, vomiting, dermatitis, hairdepigmentation, growthretardation
Basal ganglia damage,neurotoxicity, cholestasis
Chromium Role in carbohydrate and lipidmetabolism, regulator of insulinaction
None Chronic renal failure
Selenium Component of glutathioneperoxidase, important in thyroidmetabolism
Implicated in oxidative diseasessuch as bronchopulmonarydysplasia and retinopathy ofprematurity, hypothyroidism,myopathy
None
Molybdenum Essential for several enzymesinvolved in DNA metabolism
None Interferes with coppermetabolism
parenteral nutrition
e136 NeoReviews Vol.12 No.3 March 2011
Manganese neurotoxicity is a special concern for infants(18) because the element may be deposited in the basalganglia. (49) Excessive intakes of parenteral manganesemay also induce PN-associated liver disease. (49) There-fore, individual trace elements should be used in neonatalPN instead of combination products at this time.
MultivitaminsAlthough the optimal time to begin vitamin supplemen-tation in PN is unknown, most practitioners administerthem within the first few days of birth and provide themon a daily basis. Preterm infants are especially at risk forvitamin deficiency due to their poor vitamin stores andincreased requirement for rapid growth. (11) A summaryof multivitamin doses and composition is presented inTable 5.
The clinical impact of free radicals, which can developin intravenous multivitamin preparations, has been eval-uated. (50) Hydrogen peroxide and other peroxides aregenerated in light-exposed PN. Light-sensitized ribofla-vin available in parenteral multivitamin preparations cat-alyzes electron transfer between electron donors, such asvitamin C, AA, or lipids and oxygen dissolved in PNsolution. (50) Shielding PN from light has been associ-ated with a decreased risk of death or bronchopulmonarydysplasia and with lower triglyceride concentrations.(50) The amount of hydrogen peroxide infused with PNcan be reduced by half when the entire PN solution anddelivery system (ie, PN constituents, dextrose bag, lipidsyringe, and tubing) is light-protected. As an alternative,studies in animals have shown that the mixture of multi-vitamins with lipid emulsion can dramatically decreasethe generation of lipid peroxides and protect against theloss of antioxidant vitamins. (50) Light protection of PN,however, is not currently widely used in neonatal inten-sive care units.
ConclusionThe nutritional management of term and preterm neo-nates presents a constant challenge in adapting an ap-proach that maximizes both short- and long-term out-comes while reducing morbidities. In addition, manyclinicians still prescribe PN based on local dogma andoutdated concerns. Although substantial experimentalevidence has been acquired in recent years, there are stillmany gaps of knowledge in the provision of the mostoptimal neonatal intravenous nutrition, especially forextremely preterm infants. As is evident in this review,further research and evaluation are needed in many areasof neonatal PN, such as the most appropriate approach totreat hyperglycemia in the first few postnatal days inELBW infants, the safety of providing early aggressiveintravenous lipids, the optimal time to add multivitaminsor trace elements to intravenous PN, and the impact ofprotecting PN from light exposure. In addition, otherproblems must be dealt with by the manufacturers, in-cluding producing combination trace elements packagesthat meet the needs of all neonates and reducing alumi-num content of PN components. Hopefully, over time,the previously noted suggested PN guidelines will bechallenged by new and emerging knowledge and re-search, and clinicians will initiate and advance PN ac-cording to this evidence rather than local lore.
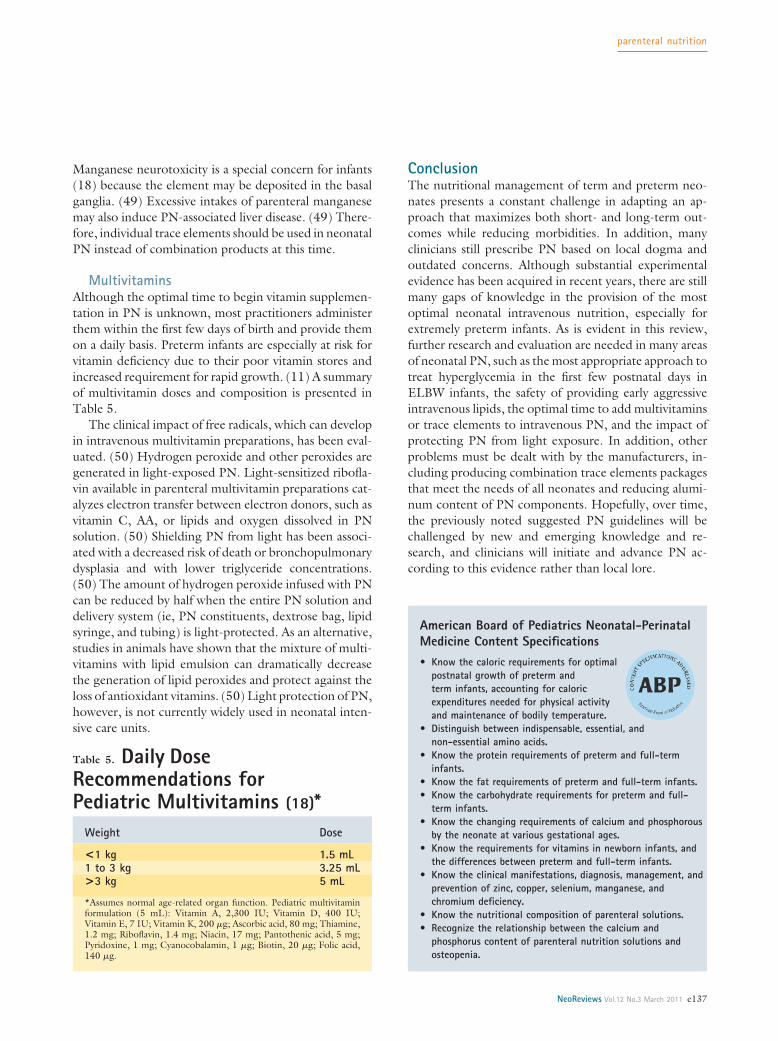
Table 5. Daily DoseRecommendations forPediatric Multivitamins (18)*
Weight Dose
<1 kg 1.5 mL1 to 3 kg 3.25 mL>3 kg 5 mL
*Assumes normal age-related organ function. Pediatric multivitaminformulation (5 mL): Vitamin A, 2,300 IU; Vitamin D, 400 IU;Vitamin E, 7 IU; Vitamin K, 200 �g; Ascorbic acid, 80 mg; Thiamine,1.2 mg; Riboflavin, 1.4 mg; Niacin, 17 mg; Pantothenic acid, 5 mg;Pyridoxine, 1 mg; Cyanocobalamin, 1 �g; Biotin, 20 �g; Folic acid,140 �g.
American Board of Pediatrics Neonatal-PerinatalMedicine Content Specifications• Know the caloric requirements for optimal
postnatal growth of preterm andterm infants, accounting for caloricexpenditures needed for physical activityand maintenance of bodily temperature.
• Distinguish between indispensable, essential, andnon-essential amino acids.
• Know the protein requirements of preterm and full-terminfants.
• Know the fat requirements of preterm and full-term infants.• Know the carbohydrate requirements for preterm and full-
term infants.• Know the changing requirements of calcium and phosphorous
by the neonate at various gestational ages.• Know the requirements for vitamins in newborn infants, and
the differences between preterm and full-term infants.• Know the clinical manifestations, diagnosis, management, and
prevention of zinc, copper, selenium, manganese, andchromium deficiency.
• Know the nutritional composition of parenteral solutions.• Recognize the relationship between the calcium and
phosphorus content of parenteral nutrition solutions andosteopenia.
parenteral nutrition
NeoReviews Vol.12 No.3 March 2011 e137

References1. Wilmore DW, Dudrick SJ. Growth and development of aninfant receiving all nutrients exclusively by vein. JAMA. 1968;203:860–8642. Ziegler EE, Thureen PJ, Carlson SJ. Aggressive nutrition of thevery low birthweight infant. Clin Perinatol. 2002;29:225–2443. Neu J. Is it time to stop starving premature infants? J Perinatol.2009;29:399–4004. Committee on Nutrition. Nutritional needs of the preterminfant. In: Kleinman RE, ed. Pediatric Nutrition Handbook. 6th ed.Elk Grove Village, IL: American Academy of Pediatrics; 2009:79–1045. Bhatia J. Fluid and electrolyte management in the very low birthweight neonate. J Perinatol. 2006;26(suppl 1):S19–S216. Pereira-da-Silva L, Virella D, Henriques G, Rebelo M, SerelhaM, Videira-Amaral JM. A simple equation to estimate the osmolar-ity of neonatal parenteral nutrition solutions. JPEN J ParenterEnteral Nutr. 2004;28:34–377. Hay WW Jr. Intravenous nutrition of the very preterm infant.Acta Paediatr Suppl. 2005;94:47–568. Valentine C, Puthoff T. Enhancing parenteral nutrition therapyfor the neonate. Nutr Clin Pract. 2007;22:183–939. Van Goudoever JB, Sulkers EJ, Timmerman N, et al. Aminoacid solutions for premature neonates during the first week of life:the role of N-acetyl-L-cysteine and N-acetyl-L-tyrosine. JPEN JParenter Enteral Nutr. 1994;18:404–40810. Fitzgerald KA, Mackay MW. Calcium and phosphate solubilityin neonatal parenteral nutrient solutions containing TrophAmine.Am J Hosp Pharm. 1986;43:88–9311. Pediatric Nutrition Practice Guide. Parenteral nutrition. In:Groh-Wargo S, Thompson M, Cox JH, eds. ADA Pocket Guide toNeonatal Nutrition. Chicago, IL: Precept Press, Inc; 2009:29–6312. Anderson D, Pittard WB. Parenteral nutrition for neonates. In:Baker R, Baker S, Cavis A, eds. Pediatric Parenteral Nutrition. NewYork, NY: International Thompson Publishing; 1997:301–31413. Valentine CJ, Fernandez S, Rogers LK, et al. Early amino acidadministration improves preterm infant weight. J Perinatol. 2009;29:428–43214. Thureen PJ, Hay WW Jr. Early aggressive nutrition in preterminfants. Semin Neonatol. 2001;6:403–41515. Ziegler EE, Carlson SJ. Early nutrition of very low birth weightinfants. J Matern Fetal Neonatal Med. 2009;22:191–19716. te Braake FW, van den Akker CH, Wattimena DJ, HuijmansJG, van Goudoever JB. Amino acid administration to prematureinfants directly after birth. J Pediatr. 2005;147:457–46117. Saini J, MacMahon P, Morgan JB, Kovar IZ. Early parenteralfeeding of amino acids. Arch Dis Child. 1989;64:1362–136618. Koletzko B, Goulet O, Hunt J, Krohn K, Shamir R. ParenteralNutrition Guidelines Working Group; European Society for Clini-cal Nutrition and Metabolism; European Society of PaediatricGastroenterology, Hepatology and Nutrition (ESPGHAN); Euro-pean Society of Paediatric Research (ESPR). Guidelines on Paedi-atric Parenteral Nutrition of the European Society of PaediatricGastroenterology, Hepatology and Nutrition (ESPGHAN) and theEuropean Society for Clinical Nutrition and Metabolism (ESPEN),Supported by the European Society of Paediatric Research (ESPR).J Pediatr Gastroenterol Nutr. 2005;41:S1–S8719. Ridout E, Melara D, Rottinghaus S, Thureen PJ. Blood ureanitrogen concentration as a marker of amino-acid intolerance in
neonates with birthweight less than 1250 g. J Perinatol. 2005;25:130–13320. Radmacher PG, Lewis SL, Adamkin DH. Early amino acidsand the metabolic response of ELBW infants (� 1000 g) in threetime periods. J Perinatol. 2009:29:433–43721. Roggero P, Gianni ML, Morlacchi L, et al. Blood urea nitro-gen concentrations in low-birth-weight preterm infants duringparenteral and enteral nutrition. J Pediatr Gastroenterol Nutr.2010;51:213–21522. Brown MR, Thunberg BJ, Golub L, Maniscalco WM, Cox C,Shapiro DL. Decreased cholestasis with enteral instead of intrave-nous protein in the very low birth weight infant. J Pediatr Gastro-enterol Nutr. 1989;9:21–2723. Kalhan SC, Kilic I. Carbohydrate as nutrient in the infant andchild: range of acceptable intake. Eur J Clin Nutr. 1999;53:S94–S10024. Sunehag A, Ewald U, Larsson A, Gustafsson J. Glucose pro-duction rate in extremely immature neonates (� 28 weeks) studiedby use of deuterated glucose. Pediatr Res. 1993;33:97–10025. Nose O, Tipton JR, Ament ME. Effect of the energy source onchanges in energy expenditure, respiratory quotient, and nitrogenbalance during total parenteral nutrition in children. Pediatr Res.1987;21:538–54126. Forsyth JS, Murdock N, Crighton A. Low birthweight infantsand total parenteral nutrition immediately after birth. III. Random-ized study of energy substrate utilisation, nitrogen balance, andcarbon dioxide production. Arch Dis Child Fetal Neonatal Ed.1995;73:F13–F1627. Jones MO, Pierro A, Hammond P, Nunn A, Lloyd DA.Glucose utilization in the surgical newborn infant receiving totalparenteral nutrition. J Pediatr Surg. 1993;28:1121–112528. Lafeber HN, Sulkers EJ, Chapman TE, Sauer PJ. Glucoseproduction and oxidation in preterm infants during total parenteralnutrition. Pediatr Res. 1990;28:153–15729. Bottino M, Cowett RM, Sinclair JC. Interventions for treat-ment of neonatal hyperglycemia in very low birth weight infants.Cochrane Database Syst Rev. 2009;21:CD00745330. Shulman RJ, Philips S. Parenteral nutrition in infants andchildren. J Pediatr Gastroenterol Nutr. 2003;36:587–60731. Innis SM. Essential fatty acids in growth and development.Prog Lipid Res. 1991;30:39–10332. Auestad N, Halter R, Hall RT, et al. Growth and develop-ment in term infants fed long-chain polyunsaturated fatty acids: adouble-masked, randomized, parallel, prospective, multivariatestudy. Pediatrics. 2001;108:372–38133. Auestad N, Scott DT, Janowsky JS, et al. Visual, cognitive, andlanguage assessments at 39 months: a follow-up study of childrenfed formulas containing long-chain polyunsaturated fatty acids to1 year of age. Pediatrics. 2003;112:e177–e18334. Ibrahim HM, Jeroudi MA, Baier RJ, Dhanireddy R, KrouskopRW. Aggressive early total parenteral nutrition in low-birth-weightinfants. J Perinatol. 2004;24:482–48635. Simmer K, Rao SC. Early introduction of lipids to parenterally-fed preterm infants. Cochrane Database Syst Rev. 2005;18:CD00525636. Stephens BE, Walden RV, Gargus RA, et al. First-week proteinand energy intakes are associated with 18–month developmentaloutcomes in extremely low birth weight infants. Pediatrics. 2009;123:1337–134337. Ehrenkranz RA, Dusick AM, Vohr BR, Wright LL, Wrage LA,Poole K and the National Institutes of Child Health and HumanDevelopment Neonatal Research Network. Growth in the neonatal
parenteral nutrition
e138 NeoReviews Vol.12 No.3 March 2011

intensive care unit influences neurodevelopmental and growth out-comes of extremely low birth weight infants. Pediatrics. 2006;117:1253–126138. Martin CR, Brown YF, Ehrenkranz T, et al and the ExtremelyLow Gestational Age Newborns Study Investigators. Nutritionalpractices and growth velocity in the first month of life in extremelypremature infants. Pediatrics. 2009;124:649–65739. Brans YW, Andrew DS, Carrillo DW, Dutton EP, MenchacaEM, Puleo-Scheppke BA. Tolerance of fat emulsions in very lowbirth weight neonates. Am J Dis Child. 1988;142:145–15240. Peterson J, Bihain BE, Bengtsson-Olivecrona G, DeckelbaumRJ, Carpentier YA, Olivecrona T. Fatty acid control of lipoproteinlipase: a link between energy metabolism and lipid transport. ProcNatl Acad Sci USA. 1990;87:909–91341. Cairns PA, Stalker DJ. Carnitine supplementation of parenter-ally fed neonates. Cochrane Database Syst Rev. 2000;4:CD00095042. Mirtallo JM, Dasta JF, Kleinschmidt KC, Varon J. State of the artreview: intravenous fat emulsions: current applications, safety profile,and clinical implications. Ann Pharmacother. 2010;44:688–70043. de Meijer VE, Gura KM, Meisel JA, Puder M. Parenteral fishoil monotherapy in the management of patients with parenteralnutrition associated liver disease. Arch Surg. 2010;145:547–551
44. Puder M, Valim C, Meisel JA, et al. Parenteral fish oil improvesoutcomes in patients with parenteral nutrition-associated liver in-jury. Ann Surg. 2009;250:395–49245. Parikh MJ, Dumas G, Silvestri A, Bistrian BR, Driscoll DF.Physical compatibility of neonatal total parenteral nutrient admix-tures containing calcium and inorganic phosphate salts. Am JHealth Syst Pharm. 2005;62:1177–118346. Hicks W, Hardy G. Phosphate supplementation for hypophos-phatemia and parenteral nutrition. Curr Opin Clin Nutr MetabolCare. 2001;4:227–23347. Driscoll M, Driscoll DF. Calculating aluminum content intotal parenteral nutrition admixtures. Am J Health Syst Pharm.2005;62:312–31548. Fewtrell MS, Bishop NJ, Edmonds CJ, Isaacs EB, Lucas A.Aluminum exposure from parenteral nutrition in preterm infants:bone health at 15-year follow-up. Pediatrics. 2009;124:1372–137949. Erikson KM, Thompson K, Aschner J, Aschner M. Manganeseneurotoxicity: a focus on the neonate. Pharmacol Ther. 2007;113:369–37750. Sherlock R, Chessex P. Shielding parenteral nutrition fromlight: does the available evidence support a randomized, controlledtrial? Pediatrics. 2009;123:1529–1533
NeoReviews Quiz
1. Energy is essential for body maintenance and growth. Knowing the energy balance and its components isimportant for prescribing parenteral nutrition (PN) in neonates. Of the following, the estimated energy costin preterm infants is highest for:A. Basal metabolism.B. Body growth.C. Excretory loss.D. Physical activity.E. Temperature regulation.
2. PN solutions may be infused via peripheral or central catheters. Peripheral infusion is usually reserved forshort-term nutrition support. The osmolarity of the infusate that can be safely administered via theperipheral route is less than that of the infusate administered via the central route. Of the following, theupper threshold of osmolarity tolerance range for peripherally infused PN solutions is closest to:A. 500 mOsm/L.B. 750 mOsm/L.C. 1,000 mOsm/L.D. 1,250 mOsm/L.E. 1,500 mOsm/L.
3. Previously used intravenous amino acid preparations were based on casein hydrolysates. Current crystallineamino acid preparations have elevated ratios of essential-to-nonessential amino acids. Of the following, theamino acid considered semi-essential in the newborn period and required for the synthesis of glutathioneantioxidant is:A. Arginine.B. Cysteine.C. Leucine.D. Tyrosine.E. Valine.
parenteral nutrition
NeoReviews Vol.12 No.3 March 2011 e139

4. Endogenous glucose production varies with gestational age, and its estimate provides an appropriatestarting point for glucose infusion rate in neonatal PN. The upper rate of glucose administration withadvancing PN is influenced by the maximal glucose oxidation capacity of the infant. Of the following, themost appropriate initial rate, daily rate of increase, and maximal rate of glucose infusion in extremelypreterm infants receiving PN is:
Initial infusion(mg/kg per minute)
Daily increment(mg/kg per minute)
Maximal rate(mg/kg per minute)
A. 1 to 2 4 to 6 8B. 1 to 2 4 to 6 9C. 2 to 4 2 to 4 10D. 4 to 6 1 to 2 12E. 4 to 6 1 to 2 16
5. Lipid emulsions are important components of neonatal PN because they provide an energy source with lowosmolarity and high energy content per unit volume. Withholding lipid can lead to essential fatty aciddeficiency, which can develop in preterm infants within the first postnatal week and as early as the secondday after birth. Of the following, the minimal amount of lipid required to prevent essential fatty aciddeficiency in preterm infants is:
A. 0.1 to 0.4 g/kg per day.B. 0.5 to 1.0 g/kg per day.C. 1.1 to 1.4 g/kg per day.D. 1.5 to 2.0 g/kg per day.E. 2.1 to 2.4 g/kg per day.
6. The trace elements currently recommended for neonatal PN are zinc, copper, manganese, chromium,selenium, and molybdenum. Although the optimal dose of each trace element remains unconfirmed, thegoal in nutrition is to prevent deficiency of the trace element and avoid its toxicity. Of the following, themost typical manifestation of zinc deficiency in neonates is:
A. Acquired hypothyroidism.B. Diffuse osteopenia.C. Hair depigmentation.D. Hepatic cholestasis.E. Perianal dermatitis.
7. The trace element preparations for neonatal PN are commercially available as single agents or ascombination products. None of the combination products meets the needs of neonates of every gestationalor postnatal age or clinical condition, and each may inadvertently provide a specific trace element inamounts in excess of the recommended dose, leading to potential toxicity. Of the following, theneurotoxicity from trace element deposition in the basal ganglia as a special concern for infants receivingparenteral nutrition is most attributed to:
A. Chromium.B. Copper.C. Manganese.D. Molybdenum.E. Selenium.
parenteral nutrition
e140 NeoReviews Vol.12 No.3 March 2011

DOI: 10.1542/neo.12-3-e130 2011;12;e130-e140 NeoReviews
Nahed O. ElHassan and Jeffrey R. Kaiser Parenteral Nutrition in the Neonatal Intensive Care Unit
& ServicesUpdated Information
s;12/3/e130http://neoreviews.aappublications.org/cgi/content/full/neoreviewincluding high-resolution figures, can be found at:
Permissions & Licensing
http://neoreviews.aappublications.org/misc/Permissions.shtmltables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints http://neoreviews.aappublications.org/misc/reprints.shtml
Information about ordering reprints can be found online:


















