PARAPNEUMONIC SYNDROME.pptx

of 29
-
Upload
saga-sabara -
Category
Documents
-
view
232 -
download
0
Transcript of PARAPNEUMONIC SYNDROME.pptx
-
7/28/2019 PARAPNEUMONIC SYNDROME.pptx
1/29
PARAPNEUMONIC
SYNDROME(Laporan Kasus)
Arismunandar H.P.U
0818011008
1
-
7/28/2019 PARAPNEUMONIC SYNDROME.pptx
2/29
1. ANAMNESIS
Identitas PasienNama : Tn. S
Umur : 60 tahun
Jenis Kelamin : Laki-laki Pekerjaan : Petani
Agama : Islam
Alamat : Punggur Tanggal Masuk : 19 Januari 2013,
pukul 18.00 WIB
2
-
7/28/2019 PARAPNEUMONIC SYNDROME.pptx
3/29
Keluhan Utama
Buang air besar cair sejak 1 hari SMRS
Keluhan Tambahan
Demam,batuk berdahak, pilek, sesak
3
-
7/28/2019 PARAPNEUMONIC SYNDROME.pptx
4/29
Riwayat Penyakit Sekarang Pasien datang ke IGD RSAY Metro dengan
keluhan buang air besar cair sejak 1 hariSMRS. Buang air besar sebanyak 5 kali
dengan konsistensi cair, ampas yang sedikitdan berlendir tanpa disertai darah. Pasien
juga mengeluh demam yang naik turun dandisertai dengan pilek, batuk berdahak dan
sesak serta dada terasa berat sejak 2 hariSMRS. Pasien juga mengaku tidak nafsumakan dan badan terasa lemas. Karenakhawatir akan kondisi dirinya, maka pasiendatang ke IGD RSAY Metro untuk berobat.
4
-
7/28/2019 PARAPNEUMONIC SYNDROME.pptx
5/29
Riwayat Penyakit Dahulu
Riwayat DM : disangkal
Riwayat hipertensi :
disangkal
Riwayat sakit jantung : disangkal
Riwayat minum OAT : disangkal
Pasien belum pernah mengalami sakit
seperti ini sebelumnya
5
-
7/28/2019 PARAPNEUMONIC SYNDROME.pptx
6/29
Riwayat Penyakit Keluarga
Riwayat penyakit serupa :
disangkal
Riwayat Hipertensi :disangkal
Riwayat DM : disangkal
Riwayat Jantung : disangkal
6
-
7/28/2019 PARAPNEUMONIC SYNDROME.pptx
7/29
PEMERIKSAAN FISIK Keadaan Umum : sakit berat,
compos mentis, gizi kurang
Tanda Vital Tekanan darah : 60/40 mmHg
Nadi : 124 x/menit
Pernapasan : 40 x/menit Suhu : 38,7 C
Saturasi O2 : 90 %
7
-
7/28/2019 PARAPNEUMONIC SYNDROME.pptx
8/29
Kepala : normochepal, simetris. Mata : Conjungtiva anemis (-/-),
sclera ikterik (-/-)
Pupil isokor (3 mm/3mm),Reflek cahaya (+/+).
Hidung : Nafas cuping hidung (+), darah (-),secret (-).
Telinga : darah (-), secret (-).
Mulut : mukosa basah (+), sianosis (-),
lidah kotor (-). Leher : Simetris, limfonodi coli tidak
membesar.
Thorax : retraksi (+).
8
-
7/28/2019 PARAPNEUMONIC SYNDROME.pptx
9/29
Jantung Inspeksi : ictus cordis tidak tampak
Palpasi : ictus cordis tidak teraba
Perkusi : batas jantung dalam batasnormal
Auskultasi : BJ I-II intensitas normal, reguler,murmur (-), gallop (-)
Paru
Inspeksi : Saat statis bagian dada kanan samadengan bagian kiri, saat dinamis, gerakan
dada kanan tertinggal dari kiri. Retraksiintercostal, dan subcostal ditemukan
Palpasi : Fremitus taktil kanan lebih lemah dari kiri
Perkusi : pekak/sonor
Auskultasi : ronki +/-, wheezing -/-
9
-
7/28/2019 PARAPNEUMONIC SYNDROME.pptx
10/29
Abdomen Inspeksi : tampak datar, dinding perut
sejajar dengan dinding dada
Auskultasi : bising usus (+)
Perkusi : Tympani
Palpasi : Supel, nyeri tekan (-),hepar/lien tidak teraba
Trunk
Inspeksi : Skoliosis (-), kifosis (-), lordosis (-)
Palpasi : Nyeri tekan (-), massa (-) Perkusi : Nyeri ketok (-)
Ekstremitas :Oedem -/- Akral dingin -/-
10
-
7/28/2019 PARAPNEUMONIC SYNDROME.pptx
11/29
PEMERIKSAAN PENUNJANG Laboratorium (19 Januari 2013) :
DL :
Hb : 9,5 g/dL
WBC : 34.600 /ul RBC : 4,46 juta /ul
PLT : 437.000 /ul
GDS : 94 mg/dL
Ureum : 66,2 mg/dL
Kreatinin : 2,02 mg/dL SGOT : 69,8 U/L
SGPT : 33,4 U/L
Albumin : 2,7 g/dL
Globulin : 1,74 g/dL
11
-
7/28/2019 PARAPNEUMONIC SYNDROME.pptx
12/29
UL : leukosit 10/ul, eritrosit 30/uL,epitel ++
Feses lengkap :
macros : konsistensi lembek,lendir, darah negatif
micros : leukosit, eritrosit
negatif BTA sputum S-P-S : negatif
Kultur darah (22-1-2013) : hasil
steril 12
-
7/28/2019 PARAPNEUMONIC SYNDROME.pptx
13/29
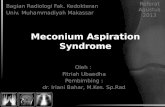
Foto Rontgen Thorax PA (23Januari 2013) :
13
Kesan:
Efusi pleura
dextra
bronkopneumonia
kardiomegalidengan elongatio
aorta
-
7/28/2019 PARAPNEUMONIC SYNDROME.pptx
14/29
USG Abdomen (21 Januari 2013) :
Complex pleural effusion supradiafragma dextra
Pielonefritis sinistra
Hepar,, lien, pancreas, vesica urinaria dalam batas normal
Dilakukan pungsi pleura pada tanggal 19 januari 2013, kemudian dilakukan
analisa dan sitologi cairan pleura, hasil :
Analisa cairan pleura (21-1-2013) :
Protein total serum : 5,76 g/dL, ratio 0,8 LDH serum : 291 U/L, ratio 3,2
Glukosa : 72 mg/dL
Pewarnaan BTA : negatif, pewarnaan gram : kokus gram positif
Sifat cairan pleura adalah eksudat dengan infeksi sekunder oleh kuman
kokus gram positif.
Patologi anatomi cairan pleura (24-1-2013) :
Sel malignancy negative
Peradangan kronis supuratif (abses)
14
-
7/28/2019 PARAPNEUMONIC SYNDROME.pptx
15/29
Diagnosa kerja:
1.Pneumonia dengan efusi pleura dextra
(parapneumonic syndrome)
2.Diarrhea
3. Malnutrisi underweight
5. PENATALAKSANAAN
O2 2L/mnt
IVFD RL guyur 1 liter maintenance 40 tetes/menit
Levofloxacin 1 x 750 mg i.v
Ceftriaxone 2 x gr i.v Metronidazol 3 x 500 mg i.v
Ranitidine 2 x 1 amp i.v
Metoclopramid 2 x 1 amp i.v
Diet : TKTP Nasi + ekstra telur
6. PROGNOSIS
Ad vitam : dubia
Ad sanam : dubia
Ad fungsionam : dubia
15
-
7/28/2019 PARAPNEUMONIC SYNDROME.pptx
16/29
PARAPNEUMONIC
SYNDROME
(Parapneumonic effusions and empyema)
16
-
7/28/2019 PARAPNEUMONIC SYNDROME.pptx
17/29
INTRODUCTION
Parapneumonic syndrome : Pneumonia symptoms with parapneumonic
effusion (exudative pleural effusion) that
results from pneumonia (CAP/NP) or lung
abses
Between 20% and 57% of the 1 million
patients hospitalized yearly in the U.S
with pneumonia, develop a PPE. Empyema is less common, occurring
in 5%10% of patients who experience
PPE 17
-
7/28/2019 PARAPNEUMONIC SYNDROME.pptx
18/29
Figure 1. Causes of empyema in 14 prior studies. Of the 1383
patients in the studies, 70% were parapneumonic. For the other
30% of patients, trauma was the cause of empyema in 7%,
empyema was postoperative in 6%, and prior tuberculosis was
the cause in 4%; 12% of cases were due to other causes.
18
-
7/28/2019 PARAPNEUMONIC SYNDROME.pptx
19/29
CLASSIFICATION
Clinical classificationof PPE : 1. uncomplicated parapneumonic
effusion (UPPE) 2. complicated parapneumonic effusion
(CPPE) 3. Empyema
Stages : 1. exudative 2. fibrinopurulent 3. final organizational
19
-
7/28/2019 PARAPNEUMONIC SYNDROME.pptx
20/29
CLINICAL PRESENTATION
Symptoms of pneumonia :
Fever, malaise, cough, dyspnea,
pleuritic chest pain
Eldery patients >> asymptomatic
20
-
7/28/2019 PARAPNEUMONIC SYNDROME.pptx
21/29
Pleural fluid analysis >>> to stage thePPE and guides initial management.
UPPEs : have a turbid appearance, witha pH >7.30, a glucose level >60 mg/dL,
an LDH level
-
7/28/2019 PARAPNEUMONIC SYNDROME.pptx
22/29
22
-
7/28/2019 PARAPNEUMONIC SYNDROME.pptx
23/29
recommended that all patients withpneumonia be evaluated for thepresence of pleural fluid.
With the possible or definite presenceof pleural fluid noted on a chestradiograph, an ultrasound-guidedthoracentesis should be performed.
Ultrasonography can detect strandingor septation in the fluid suggestive of aCPPE and can facilitate its drainage.
23
-
7/28/2019 PARAPNEUMONIC SYNDROME.pptx
24/29
Figure 3.A complex, septate pleural effusion
demonstrated by ultrasonography in a patient with
spontaneous hemorrhage into a pre-existing pleural
effusion. This precise pattern is typical of a complicatedparapneumoniceffusion as well. 24
-
7/28/2019 PARAPNEUMONIC SYNDROME.pptx
25/29
PATHOPHYSIOLOGY
Figure 2. The estimated time course ofuntreated or inappropriately treatedparapneumonic effusions. In general,an empyema will develop 46 weeks
after the onset of aspiration of bacteriainto the lung. 25
-
7/28/2019 PARAPNEUMONIC SYNDROME.pptx
26/29
MANAGEMENT
In general, early and appropriateantibiotic treatment will prevent the
development of a PPE and its
progression.
26
-
7/28/2019 PARAPNEUMONIC SYNDROME.pptx
27/29
MANAGEMENT Ant ib iot ic therapy: Early antibiotic therapy will prevent the development
of a PPE and its progression to a CPPE and empyema.
Pleural sp ace drainage :
Clinical factors that suggestpleural space drainage include :
prolonged pneumonia symptoms,
Comorbid disease,
failure to respond to antibiotic therapy, and presence of anaerobic organisms .
Chest radiograph findings that suggest the need for pleural space
drainage include an effusion involving >50% of the hemothorax
Stranding or septation noted on an ultrasound suggests the need for
pleural space drainage. Intrapleural f ibr inolyt ic s :fibrinolytic agents (urokinase and tissue
plasminogen activator) most effective in the early fibrinolytic stage in
avoiding the need for surgical drainage.
Surgery :pleural space drainage by tube thoracostomy has been
ineffective in controlling the pleural infection. (VATS).
27
-
7/28/2019 PARAPNEUMONIC SYNDROME.pptx
28/29
CONCLUSIONS1. Early antibiotic treatment usually prevents the development of a PPE and its
progression to a complicated PPE and empyema.
2. Pleural fluid analysis provides diagnostic information and guides therapy.
3. If the PPE is small to moderate in size, free-flowing, and nonpurulent (pH,
>7.30), it is highly likely that antibiotic treatment alone will be effective.
4. Prolonged pneumonia symptoms before evaluation, pleural fluid with a pH
-
7/28/2019 PARAPNEUMONIC SYNDROME.pptx
29/29
TERIMA KASIH
29


















