
Paraneoplastic cerebellar degeneration. -...
8
Paraneoplastic cerebellar degeneration. I. A clinical analysis of 55 anti-Yo antibody-positivepatients K. Peterson, MD; M.K. Rosenblum, MD; H. Kotanides, MS; and J.B. Posner, MD Article abstract-We reviewed the clinical findings in 55 patients with cerebellar degeneration associated with the anti-Yo antibody (an anti-Purkinje cell antibody identified in this study by histochemistry and Western blot). The patients were all women, 26 to 85 years old. Fifty-two of them proved to have malignancies, almost exclusively breast or gynecologic cancers and usually confined to the involved organs and local lymph nodes. One woman had adenocarci- noma of the lung, and in three no malignancy has yet been identified. In 34 of 52 patients with cancer, the neurologic syndrome preceded the diagnosis of cancer and in many led to that diagnosis. Patients subacutely developed a pancere- bellar disorder that was substantially disabling in most, with 37 of 48 assessable patients being unable to walk or sit unassisted. Laboratory evaluation revealed lymphocytic pleocytosis in 35 patients, with eventual cerebellar atrophy on imaging studies in seventeen. The disabling neurologic syndrome generally did not respond to treatment, but the can- cer was often successfully treated. The presence of the anti-Yo antibody in patients with cerebellar symptoms warrants an aggressive approach to diagnosis and treatment of the underlying cancer, as many are curable at the time neurolog- ic symptoms develop. NEUROLOGY 1992; 42:1931-1937 Paraneoplastic cerebellar degeneration (PCD) is a clinical syndrome in which cerebellar dysfunction is associated with identifiable or occult cancer but without direct involvement of the nervous system by the cancer. Typically, the disorder evolves sub- acutely, causes severe pancerebellar dysfunction, and is associated with extensive Purkinje cell loss, sometimes accompanied by meningeal and deep cerebellar nuclear inflammatory infiltrates.1-3 Up until 1982, Henson and Urich3 were able to identify only 50 pathologically proven cases. Even with recent renewed interest in the disorder, the num- ber of patients reported in the literature is about two h ~ n d r e d . ~ Although the disorder is rare, Henson and Urich3 estimate that at least 50% of middle-aged patients who present with a subacute- ly developing pancerebellar disorder prove within a few years to have cancer. It is increasingly apparent that PCD, despite its rarity, subdivides into several disorders that can be distinguished clinically and immunologically, and that differ in their prognoses and in the types of associated malignancies. The clinical findings in 55 patients with one of these disorders, PCD associat- ed with a particular autoantibody designated “anti- YO,” are described in this paper. The two papers that.follow (pages 1938 and 1944) describe PCD associated with Hodgkin’s disease, and an unusual variant of PCD associated with small-cell lung can- cer (SCLC) in which the majority of patients also have the Lambert-Eaton myasthenic syndrome. A fourth disorder, in which PCD may be the present- ing symptom of a more widespread encephalomyeli- tis associated with SCLC and an antinuclear anti- body called “anti-Hu,’?is detailed e l ~ e w h e r e . ~ , ~ Recognizing the specific variant of PCD on clinical grounds and with immunologic testing often allows the physician to better predict the clinical course and direct the search for an underlying occult malignancy. Methods. Patients. The medical records of all anti- Yo-positive patients (defined by immunohistochemistry and immunoblotting) identified in our laboratory were reviewed. Eighteen of these patients had been reported previ~usly.~ Since only 10 of the 55 patients were exam- From the Departments of Neurology {Drs. Peterson and Posner) and Pathology (Dr. Rosenblum) and the George C. Cotzias Laboratory of Neuro- Oncology (H. Kotanides and Dr. Posner), Memorial Sloan-Kettering Cancer Center, and the Department of Neurology and Neuroscience (Drs. Peterson and Posner), Cornell University Medical College, New York, NY. Supported in part by NIH Grant #NS26064. Presented in part at the 43rd annual meeting of the American Academy of Neurology, Boston, MA, April 1991 Received January 17, 1992. Accepted for publication in final form March 24, 1992. Address correspondence and reprint requests to Dr. Jerome B. Posner, Department of Neurology, Memorial Sloan-Kettering Cancer Center, 1275 York Avenue, New York, NY 10021. Dr. Peterson’s current address is Department of Neurology, University of Minnesota Medical School, Minneapolis, MN. October 1992 NEUROLOGY 42 1931
Transcript of Paraneoplastic cerebellar degeneration. -...

Paraneoplastic cerebellar degeneration
I A clinical analysis of 55 anti-Yo antibody-positive patients
K Peterson MD MK Rosenblum MD H Kotanides MS and JB Posner MD
Article abstract-We reviewed the clinical findings in 55 patients with cerebellar degeneration associated with the anti-Yo antibody (an anti-Purkinje cell antibody identified in this study by histochemistry and Western blot) The patients were all women 26 to 85 years old Fifty-two of them proved to have malignancies almost exclusively breast or gynecologic cancers and usually confined to the involved organs and local lymph nodes One woman had adenocarci- noma of the lung and in three no malignancy has yet been identified In 34 of 52 patients with cancer the neurologic syndrome preceded the diagnosis of cancer and in many led to that diagnosis Patients subacutely developed a pancere- bellar disorder that was substantially disabling in most with 37 of 48 assessable patients being unable to walk or sit unassisted Laboratory evaluation revealed lymphocytic pleocytosis in 35 patients with eventual cerebellar atrophy on imaging studies in seventeen The disabling neurologic syndrome generally did not respond to treatment but the can- cer was often successfully treated The presence of the anti-Yo antibody in patients with cerebellar symptoms warrants an aggressive approach to diagnosis and treatment of the underlying cancer as many are curable at the time neurolog- ic symptoms develop
NEUROLOGY 1992 421931-1937
Paraneoplastic cerebellar degeneration (PCD) is a clinical syndrome in which cerebellar dysfunction is associated with identifiable or occult cancer but without direct involvement of the nervous system by the cancer Typically the disorder evolves sub- acutely causes severe pancerebellar dysfunction and is associated with extensive Purkinje cell loss sometimes accompanied by meningeal and deep cerebellar nuclear inflammatory infiltrates1-3 Up until 1982 Henson and Urich3 were able to identify only 50 pathologically proven cases Even with recent renewed interest in the disorder the num- ber of patients reported in the literature is about two h ~ n d r e d ~ Although the disorder is rare Henson and Urich3 estimate that at least 50 of middle-aged patients who present with a subacute- ly developing pancerebellar disorder prove within a few years to have cancer
It is increasingly apparent that PCD despite its rarity subdivides into several disorders that can be distinguished clinically and immunologically and that differ in their prognoses and in the types of associated malignancies The clinical findings in 55
patients with one of these disorders PCD associat- ed with a particular autoantibody designated ldquoanti- YOrdquo are described in this paper The two papers thatfollow (pages 1938 and 1944) describe PCD associated with Hodgkinrsquos disease and an unusual variant of PCD associated with small-cell lung can- cer (SCLC) in which the majority of patients also have the Lambert-Eaton myasthenic syndrome A fourth disorder in which PCD may be the present- ing symptom of a more widespread encephalomyeli- tis associated with SCLC and an antinuclear anti- body called ldquoanti-Hursquo is detailed e l ~ e w h e r e ~ ~ Recognizing the specific variant of PCD on clinical grounds and with immunologic testing often allows the physician to better predict the clinical course and direct the search for an underlying occult malignancy
Methods Patients The medical records of all anti- Yo-positive patients (defined by immunohistochemistry and immunoblotting) identified in our laboratory were reviewed Eighteen of these patients had been reported previ~usly~ Since only 10 of the 55 patients were exam-
From the Departments of Neurology Drs Peterson and Posner) and Pathology (Dr Rosenblum) and the George C Cotzias Laboratory of Neuro- Oncology (H Kotanides and Dr Posner) Memorial Sloan-Kettering Cancer Center and the Department of Neurology and Neuroscience (Drs Peterson and Posner) Cornell University Medical College New York NY Supported in part by NIH Grant NS26064
Presented in part at the 43rd annual meeting of the American Academy of Neurology Boston MA April 1991
Received January 17 1992 Accepted for publication in final form March 24 1992
Address correspondence and reprint requests to Dr Jerome B Posner Department of Neurology Memorial Sloan-Kettering Cancer Center 1275 York Avenue New York NY 10021 Dr Petersonrsquos current address is Department of Neurology University of Minnesota Medical School Minneapolis MN
October 1992 NEUROLOGY 42 1931
ined by one or more of the authors referring physicians sending sera andlor CSF for antibody testing provided the neurologic and oncologic profiles Telephone calls to the physicians most recently caring for the patients pro- vided follow-up as of December 1991 Microscopic slides and blocks of the cerebellum obtained at autopsy in three patients and tumor tissue in seven patients were studied directly by us
Serum and CSF database Approximately 2000 sera andor CSF samples have been examined in our laborato- ry for the presence of anticerebellar antibodies These samples were sent from throughout the United States and many other countries by physicians suspecting the diagnosis of a neurologic paraneoplastic syndrome Some patients had known cancers whereas others did not All samples were s tudied by immunofluorescence or immunoperoxidase histochemistry and by Western blot- ting against Purkinje cell extracts A search of the data- bank also identified all patients in 1989 and 1990 with cerebellar syndromes with or without cancer and all patients with ovarian or breast cancer with or without cerebellar syndromes
Immunologic techniques Immunohistochemistry and Western blott ing techniques against Purkinje cell extracts as well as the CDR 62 fusion protein that corre- sponds to the 62 kd antigen to which the anti-Yo anti- body binds have been described extensively in previous publications from this l a b ~ r a t o r y ~ - ~
Results Immunologic findings Serum or CSF from 55 patients was positive for the anti-Yo anti- body as determined by immunohistochemistry and Western blotting In 41 of 41 patients tested sera also reacted positively against the Yo fusion pro- tein14
Several patients who had atypical histochemical staining andor atypical immunoblotting were excluded Excluded patients included one whose serum was positive by histochemistry but reacted on Western blotting against Purkinje cell extracts with a band of 68 kd (but not 34 kd ) and was neg- ative against the Yo fusion protein Three patients had atypical Purkinje cell cytoplasmic staining and were negative on immunoblotting Two patients with PCD showed neuronal nuclear staining and a band at 35 to 40 kd on Western blot (typical of the anti-Hu antibody) but were negative when tested against the Yo fusion protein and one other with atypical nuclear staining was negative with both immunoblotting techniques
Thirteen patients with Hodgkins disease and PCD 45 patients with breast cancer and 24 with ovarian cancer with or without cerebellar syn- dromes 325 patients with cerebellar syndromes with or without cancer and 50 normal controls (blood bank donors) were also negative by both his- tochemistry and immunoblotting
Clinical results The 55 patients with the typical anti-Yo antibody presented a stereotypic clinical syndrome All patients were women 26 to 85 years old
Tumors Fifty-two of the patients currently have histologically proven malignancies The most com- mon tumor ovarian was found in 26 of 55 patients
1932 NEUROLOGY 42 October 1992
13 had breast cancer and seven had other gyneco- logic malignancies (four endometrial two fallopian tube and one mesovarium) One patient had both breast and fallopian tube cancers One patient had an adenocarcinoma of the lung and is without known gynecologic malignancy
There were six patients with adenocarcinoma of unknown primary Three of these presented with axillary nodes likely representing breast cancer although no primary was found in the breast One patient with adenocarcinoma of unknown primary had had resection 2 years previously of an ovarian mass that had shown benign pathology at autopsy this patient was found to have had a periaortic node pathologically suggestive of ovarian cancer and had staining for CA 125 antigen which is asso- ciated with ovarian cancers One patient presented with carcinoma in an inguinal lymph node One other patient had a poorly differentiated adenocar- cinoma in an abdominal lymph node compatible with ovarian cancer but no ovarian tumor was found At autopsy 3 years later she was found to have a hepatoma but no adenocarcinoma the origi- nal primary was not found
Three patients had no tumor identified One of these patients had resection of an ovarian mass with benign histology (ovarian cystadenoma) she died 24 months after the onset of her neurologic syndrome and no cancer was found at autopsy Two patients are still living up to 24 months after the onset of their neurologic disorder and have so far shown no evidence of malignancy despite serial physical and radiologic examinations
In 34 of 52 patients with known cancer the neu- rologic syndrome preceded the diagnosis of malig- nancy by up to 15 months and in many of the cases prompted a search for the underlying cancer Of these 34 patients 16 had ovarian cancer notably four had microscopic disease not found by routine diagnostic testing and detected only at laparotomy However one patient with a negative mammogram and normal pelvic examination underwent laparoscopy with ovarian biopsy and then hys- terectomy and bilateral salpingo-oophorectomy without a malignancy being found Four months after the initial normal mammogram a breast abnormality was detected and biopsy revealed an intraductal carcinoma
Most patients with known cancer had limited oncologic disease at the time of onset of neurologic symptoms with only 7 of 52 having evidence of widely metastatic cancer Ten patients had local disease 26 had regional metastases and six patients were in remission Three patients present- ed with neurologic symptoms coincident with recur- rence of a malignancy that had previously been in remission
Neurologic findings Patients presented with a characteristic pancerebellar disorder with truncal and limb ataxia dysarthria and nystagmus of subacute onset (1 day to 16 weeks) and subsequent stabilization Complete details of the neurologic
examination were available to us in 48 patients The ataxia was init ially asymmetric in 20 although in most ataxia became symmetric as the disease progressed Most patients were severely disabled by the neurologic syndrome with 37 of 48 patients being unable to walk or sit unassisted due to severe ataxia 9 of 48 could walk with some assistance and 2 of 48 could walk unassisted but were unsteady
All patients had some degree of horizontal nys- tagmus with a rotatory or vertical component in twenty-seven Seventeen patients were specifically reported to have downbeating nystagmus All of the 10 patients we examined had downbeating nys- tagmus we suspect that this finding was underre- ported in records we reviewed Five patients reported oscillopsia and 19 patients experienced diplopia However limitation of extraocular move- ments with unilateral or bilateral abducens palsies was detected in only six In 20 patients there was other bulbar involvement including dysphagia in 16 and facial weakness in seven Opsoclonus was reported in two patients and sleep myoclonus in one other
Signs or symptoms of involvement at other lev- els of the neuraxis were common but usually mild Although accurate mental status testing was diffi- cult t o confirm because of dysarthria and motor dysfunction 10 patients were believed clinically to have some cognitive impairment usually emotional lability and memory deficit Twenty-eight had extensor plantar responses or other long-tract signs Two patients had extrapyramidal rigidity and tremor or dyskinesias Twenty-six had hypore- flexia or mild distal sensory complaints suggesting peripheral neuropathy Two patients had progres- sive visual loss This finding was believed clinically to be a result of either optic neuropathy or retinal degeneration although this was unconfirmed by electrographic studies
Headache was an uncommon complaint promi- nent in only six patients Twenty patients com- plained of vertigo Nausea and vomiting were debil- itating symptoms in two
None of the patients was known t o have other immunologic rheumatic or collagen vascular dis- eases save for hypothyroidism in two patients and adult-onset diabetes mellitus in one
Laboratory eualuation CSF examination was performed in all patients Of the 42 patients in whom detailed CSF results were available only seven had normal CSF Thirty-five patients had inflammatory changes that included a predomi- nantly lymphocytic pleocytosis (between 6 and 93 WBCmm3) in 26 of 42 and elevated protein (between 48 and 106 mgdl) in 22 of 42 patients The ratio of CSF to serum IgG was increased in 12 of 14 patients for whom this information was avail- able oligoclonal bands were present in 6 of 7 patients tested and elevated myelin basic protein reported in one
CT andor MRI was performed in all patients
Table 1 Clinical findings in 55 anti-Yo-positive PCD patients
Sex Women Men
26 to 85 years
Before diagnosis of cancer After diagnosis of cancer No cancer known
Severe (unable to walk) Moderate (walks with assist) Mild (walks but unsteady) Severity not known
Rotatory or vertical
EOM abnormality detected
Age
Time of neurologic presentation
Ataxia
Nystagmus
Dip 1 o p i a
Opsoclonus Myoclonus Dysphagia Facial weakness Cognitive impairment Long-tract signs Extrapyramidal signs Peripheral neuropathy Progressive visual loss Headache Vertigo Severe nausea and vomiting CSF
Negative cytology Normal Inflammatory Details not known
Negative for metastasis Cerebellar atrophy
Immunosuppressive therapy Plasmapheresis Steroids Cyclophosphamide Azathioprine ACTH
No response Mild transient improvement Mild sustained improvement
CT or MRI
Response to therapy
Living (291) Died
55 0
61 (median)
34 18 3
55 37 9 2 7
55 27 19 6 2 1
16 7
10 28 2
26 2 6
20 2
55 7
35 13
55 17 29 22 17 4 2 1
23 5 1
36 19
EOM Extraocular movement
Most of these studies were init ially normal although 17 patients had evidence of cerebellar atrophy on CT or MRI particularly later in the dis- ease process In seven patients studied with 18F-flu- orodeoxyglucose positron emission tomography the mean regional metabolic rate for glucose was sig-
October 1992 NEUROLOGY 42 1933
~~~~~~ ~ ~~ ~
Figure (A) Photomicrograph of normal cerebellar cortex from a 55-year-old man who died of disseminated carcinoma without neurologic involvement Purkinje cells are prominent at the junction of the molecular and granular layers (hematoxylin-eosin XlOO before 29 reduction) (B) View of the cerebellar cortex from a patient who died with anti- Yo-positive PCD demonstrating total Purkinje cell loss Note the absence of inflammatory infiltrates (hematoxylin-eosin XlOO before 29 reduction)
nificantly reduced in the cerebellum and several cortical regions as well when compared with that of normal indi~idua1sl~
Treatment On the rationale that this neurologic syndrome was autoimmune several immuno- suppressive therapies were tried in various combi- nations in a total of 29 patients These included plasmapheresis i n 22 pat ients (a t least five exchanges) There was mild but transient improve- ment in the symptoms of ataxia and dysarthria in four patients Another patient had a moderate sus- tained benefit regaining her ability to walk with assistance This correlated with a decrease in her serum antibody titers from 14000 pre-treatment t o 1200 post-treatment However five other patients with documented decline in serum anti- body titers after treatment showed no clinical response possibly related to the finding that there was no corresponding decline in CSF antibody titers16 High-dose steroids (40 to 100 mgd for at least 2 weeks) gave mild but transient improve- ment in one of 17 patients treated There was no beneficial effect of cyclophosphamide in four patients azathioprine in two o r ACTH in one patient One patient was reported t o have had moderate improvement with treatment of the underlying tumor
At the time of most recent follow-up 36 patients are still living up to 77 months after the onset of neurologic symptoms Most of these are in remis- sion from their malignancies but remain severely disabled neurologically Nineteen patients have died between 2 and 36 months after the onset of their neurologic symptoms due to progression of their oncologic disease and inanition (table 1)
Pathology The neuropathologic findings at
1934 NEUROLOGY 42 October 1992
autopsy were available for review in three cases and conformed to previous descriptions of PCD in patients with breast and gynecologic ~ a n c e r ~ All were characterized chiefly by cerebellar cortical atrophy with near-total depletion of Purkinje cells and proliferation of Bergmann astrocytes (figure) Thinning of the granule cell population was an additional feature of two cases Scattered small lymphocytes mainly T-cells by immunotyping were noted in the cerebellar leptomeninges but in no case were inflammatory infiltrates identified in the cerebellar cortex proper Small numbers of mature lymphocytes again mainly T-cells also cuffed blood vessels in the dentate nucleus but were not associated with appreciable neuronal loss As expected the dentate amiculum (composed nor- mally of Purkinje cell axons) exhibited axonal depopulation and secondary demyelination in all cases
Microscopic sections of the PCD-associated neo- plasm at its primary site were available for review in seven cases (one fallopian tube one endometrial two mammary and three ovarian) Both breast pri- maries were high-grade poorly differentiated infil- t r a t ing adenocarcinomas of the duct type Similarly the endometrial ovarian and tuba1 neo- plasms were found to be high-grade mullerian ade- nocarcinomas composed of solid and papillary ele- ments An unusual and striking feature common to the stroma of all seven neoplasms was a conspicu- ous lymphoid infiltrate dominated by mature plas- ma cells As previously described12 expression of the Yo antigen by PCD-associated neoplasms was demonstrable in immunohistochemical and Western blot assay in all 10 instances in which fresh tumor tissue was available for analysis
Table 2 Autoantibodies in paraneoplastic cerebellar degeneration
Antigen distribution titer (immunohistochemistry)
Immunoblots (antigen Mr) Author Tumor (no)
Hodgkinrsquos ( 1 ) Trotter et a120 1976
Stefansson et ally 1981
Brown et alZ2 1985
Purkinje cell cytoplasm 120
Axons dendrites in cerebral cerebellar cortex
Purkinje cell cytoplasm neurons in deep cerebellar nuclei brainstem forebrain
Purkinje cell cytoplasm
Hodgkinrsquos (1)
Lung (small cell) (1) 85 Mouse cerebellum brain spinal cord
210 Kornguth et aP3 1985
Rodriguez et aP4 1986
Tanaka et aP6 1986
Ovary (1)
ldquoGynecologic cancerrdquo (4) Purkinje cell cytoplasm
Non-Hodgkinrsquos (1) Purkinje cell cytoplasm 250 125 (cerebrum) 125 (cerebellum) Rat cytoplasmic proteins
- Greenlee and BrasheaP 1983
Greenlee et aP1986 Greenlee and Liptonz8 1986
Jaeckle e t a18 1985
Purkinje cell cytoplasm 1640
Purkinje and granule cell cytoplasm Purkinje and granule cell nuclei CNS neurons 1320
Purkinje cell cytoplasm 11000
Ovary breast (9)
Lung (small cell) (3) Breast (1)
34-38 62-64 Human Purkinje cell
Ovary breast (7)
Cunningham et alg 1986
Bourdette and N i I a ~ e r ~ ~ 1987
Royal et a130 1987
Anderson et al3I 1988
Lung (small cell) (5) Hodgkinrsquos (5)
Benign monoclonal gammopathy
Breast (1)
Absent Absent
Purkinje cell cytoplasm
Purkinje cell cytoplasm 34-38 62-64
5664 68 80 Purkinje cell cytoplasm fine granular pattern human rat rabbit bovine 13000
Weak staining cortical hippocampal brainstem neurons 1 5 0
Purkinje cell cytoplasm
Lung (adeno) (1)
Ovary (9) breast (61 adenocarcinoma
unknown 1rdquo (3) Lung (adeno) (l) colon (1) Lung (small cell) (1) Breast (1)
34-38 62-64
-
35-40 (anti-Hu) 53-61 79-84
5258
3046 3840
Anderson et a17 1988
Purkinje cell cytoplasm
All neuronal nuclei All neuronal nuclei
Ovary (21 uterus (2)
Purkinje stellate basket cells deep cerebellar nuclei cortical hippocampal neurons 110000 All neuronal cells 1100000
Tsukamoto et a P 1989
Breast ( l ) lung (1)
October 1992 NEUROLOGY 42 1935
Discussion This report confirms and extends findings previously reported on 18 patients from this laboratory7 and in a similar survey of 32 PCD patients published recently from the Mayo Clinic In the Mayo series 16 antibody-positive patients were identified17 From these reports emerges a rather stereotypic picture of the anti-Yo antibody- positive PCD patient Always female and usually not previously known to have cancer she develops over a matter of weeks a severe pancerebellar dis- order with t runcal and appendicular a taxia dysarthria and nystagmus often with a downbeat- ing component The clinical findings stabilize with- in a couple of months leaving most patients unable to walk without the assistance of one or two people unable to write legibly frequently unable to read or watch television because of oscillopsia or diplopia and having difficulty in being understood when speaking The behavioral and long-tract signs when present are usually mild and opsoclonus and myoclonus are not characteristic features Interestingly two of our patients had progressive prechiasmal visual loss possibly due to optic neu- ropathy or retinal degeneration Most patients remain stable but severely disabled and except in a few isolated cases18 do not improve with plasma- pheresis or immunosuppression With few excep- tions the anti-Yo antibody-positive PCD patient is eventually found to have an associated gynecologic cancer
Several different autoantibodies have been iden- tified in patients with PCD (table 2) In comparison with anti-Yo-positive PCD patients those without the anti-Yo antibody though pathologically simi- lar are frequently clinically distinct and make up a heterogeneous group Taken together patients without the anti-Yo antibody have an approximate- ly equal sex distribution a variety of associated malignancies (most commonly bronchial carcinoma and Hodgkinrsquos lymphoma) and more frequently present with their neurologic syndrome after the malignancy has been diagnosed Particular subsets of patients with PCD are discussed in the following two papers and e l s e ~ h e r e ~ - ~ J ~ J ~ ~ ~ ~
With the data reported here and with other recently reported cases or series of PCD it seems likely that PCD is a group of disorders each related to a particular cancer or cancers The utility of dif- ferentiating between the different anti-Purkinje cell antibodies is that when a particular antibody is present such as anti-Yo it strongly suggests the presence of an underlying neoplasm and directs the search for the occult malignancy to one or a few organs We believe that the presence of the anti-Yo antibody warran ts a n aggressive diagnostic approach that begins with careful breast and pelvic examination mammography pelvic CT and mea- surement of ovarian tumor antigen CA 125 If no malignancy is revealed with this initial workup repeat mammography pelvic examination under anesthesia and uterine D amp C should be per- formed If there is still no cancer evident surgical
1936 NEUROLOGY 42 October 1992
exploration and removal of pelvic organs may be warranted particularly in the postmenopausal woman
Unfortunately early detection and even cure of the underlying cancer does not usually affect the neurologic symptoms Although there are occasion- al reports of patients with paraneoplastic syn- dromes responding to treatment of the underlying tumor21 none of the patients in this series substan- tially improved after successful treatment of the cancer and follow-up of more than 4 years In none of the patients has there been progression of the cerebellar dysfunction after treatment of the can- cer however in most of the patients the cerebellar dysfunction had stabilized by the time the cancer diagnosis was made and treatment instituted Interestingly the anti-Yo antibody has persisted in all the patients we have followed after what is assumed to be successful treatment of the cancer In two patients in remission for more than 4 years the antibody persists in the serum although there has been no progression of their cerebellar dysfunc- tion or evidence of recurrent tumor Thus the major importance of identification of the anti-Yo antibody is that early diagnosis leads to treatment and at times cure of the cancer Identification of the antibody does not appear to be helpful in ame- liorating the neurologic disease
The pathogenesis of anti-Yo-positive PCD is unknown The high titer of antibody suggests an autoimmune mechanism but there are no reports of successful attempts to reproduce the disease in experimental animals A recent report of intrathe- cal injection of anti-Yo antibodies into experimen- tal animals was apparently successful in getting the antibody to the Purkinje cells but not in caus- ing neurologic dy~funct ion~~ Furthermore autopsy studies indicate that in most patients there is no inflammation around the degenerated Purkinje cells Thus there is no direct evidence for either a humoral- o r cell-mediated immune reaction in patients with anti-Yo-positive PCD Further work will be necessary to establish the pathogenesis of the disorder
References 1
2
3
4
5
6
Brain WR Daniel PM Greenfield JG Subacute cortical cerebellar degeneration and its relation t o carcinoma J Neurol Neurosurg Psychiatry 19511459-75 Brain WR Wilkinson M Subacute cerebellar degeneration associated with neoplasms Brain 196588465-478 Henson RA Urich H eds Cancer and the nervous system the neurological manifestations of systemic disease Oxford UK Blackwell Scientific 1982346-367 Hammack JE Posner JB Paraneoplastic cerebellar degen- eration In Plaitakis A ed Cerebellar degenerations clini- cal neurobiology Boston Kluwer Academic 1992 Anderson NE Rosenblum MK Graus F Wiley RG Posner JB Autoantibodies in paraneoplastic syndromes associated with small-cell lung cancer Neurology 1988381391-1398 Dalmau J Graus F Rosenblum MK Posner JB Anti-Hu associated paraneoplastic encephalomyelitissensory neu- ronopathy a clinical s tudy of 7 1 pa t ien ts Medicine 19927159-72
7 Anderson NE Rosenblum MK Posner JB Paraneoplastic cerebellar degeneration clinical-immunological correlations Ann Neurol 198824559-567
8 Jaeckle KA Graus F Houghton A Cardon-Cardo C Nielsen SL Posner JB Autoimmune response of patients with para- neoplastic cerebellar degeneration t o a Purkinje cell cyto- plasmic protein antigen Ann Neurol 198518592-600
9 Cunningham J Graus F Anderson N Posner JB Partial characterization of the Purkinje cell antigens in paraneo- plastic cerebellar degeneration Neurology 1986361163- 1168
10 Dropcho EJ Chen Y Posner JB Old LJ Cloning of a brain protein identified by autoantibodies from a patient with paraneoplastic cerebellar degeneration Proc Natl Acad Sci
11 Furneaux HM Dropcho E J Barbut D e t al Characterization of a cDNA encoding a 34-kDa Purkinje neuron protein recognized by sera from patients with para- neoplastic cerebellar degeneration Proc Natl Acad Sci USA
12 Furneaux HM Rosenblum MK Dalmau J Wong E Woodruff P Posner JB Selective expression of Purkinje cell antigens in tumor tissue derived from patients with parane- oplastic cerebellar degenerat ion N Engl J Med
13 Chen Y Rettig WJ Yenamandra AK e t a] Cerebellar degeneration-related (CDR) antigen a highly conserved neu- roectodermal marker mapped to chromosome X in human and mouse Proc Natl Acad Sci USA 1990873077-3081
14 Fathallah-Shaykh H Wolf S Wong E Posner JB Furneaux HM Cloning of a leucine zipper protein recognized by the sera of patients with antibody-associated paraneoplastic cerebellar degenerat ion Proc N a t l Acad Sci USA
15 Anderson NE Posner JB Sidtis J J e t al The metabolic anatomy of paraneoplastic cerebellar degeneration Ann Neurol 198823533-540
16 Gram F Abos J Roquer J Mazzara R Pereira A Effect of plasmapheresis on serum and CSF autoantibody levels in CNS paraneoplastic syndromes Neurology 1990401621- 1623
17 Hammack J E Kimmel DW OrsquoNeill BP Lennon VA Paraneoplastic cerebellar degeneration a clinical compari- son of patients with and without Purkinje cell cytoplasmic antibodies Mayo Clin Proc 1990651423-1431
18 Cocconi G Ceci G Jinvarra G et al Successful treatment of subacute cerebellar degeneration in ovarian carcinoma with plasmapheresis a case report Cancer 1985562318-2320
19 Stefansson K Ante1 JP Wollman RL Levin KH Larson R Arnason BGW Anti-neuronal antibodies in serum of a pat ient with Hodgkinrsquos disease and cerebellar a taxia [abstract] Neurology 198131(No 4 Pt 2)126
USA 1987844552-4556
1989862873-2877
19903221844-1851
1991883451-3454
20 Trotter JL Hendin BA Osterland CK Cerebellar degenera- tion with Hodgkinrsquos disease an immunological study Arch Neurol 197633660-661
21 Kearsley JH Johnson P Halmagyi GM Paraneoplastic cerebellar disease remission with excision of the primary tumor Arch Neurol 1985421208-1210
22 Brown RH J r Ronthal M Come S et al Antibodies t o 85000 dalton protein in paracarcinomatous cerebellar degeneration [abstract] Neurology 198535(suppl 1)288
23 Kornguth S Kalinke T Grunwald G Brooks B Zimmerman E Anti-neurofilament antibodies associated with paraneo- plastic syndromes [abstract] Fed Proc 198544966
24 Rodriguez M Truh LI OrsquoNeill BP Lennon VA Autoimmune paraneoplastic cerebellar degeneration ultrastructural localization of antibody-binding sites in Purkinje cells Neurology 1988381380-1386
25 Tanaka K Yamazaki M Sat0 S Toyoshima I Yamamoto A Miyatake T Antibodies to brain proteins in paraneoplastic cerebellar degeneration Neurology 1986361169-1172
26 Greenlee J E Brashear HR Antibodies to cerebellar Purkinje cells in patients with paraneoplastic cerebellar degenerat ion a n d ovarian carcinoma Ann Neurol
27 Greenlee J E Brashear HR Jaeckle KA Stroop WG Anticerebellar antibodies in sera of patients with paraneo- plastic cerebellar degeneration studies of antibody specifici- ty and response to plasmapheresis [abstract] Ann Neurol 198620 139
28 Greenlee JE Lipton HL Anticerebellar antibodies in serum and cerebrospinal fluid of a patient with oat cell carcinoma of the lung and paraneoplastic cerebellar degeneration Ann Neurol 19861982-85
29 Bourdette DN Nilaver G Cerebellar degeneration associat- ed with anti-Purkinje cell antibodies and benign IgG mono- clonal gammopathies [abstract] Neurology 198737(suppl 1)291
30 Royal W 111 Galasko DR McKhann GM Cunningham JM Dropcho EJ Clinical course immunologic and biochemical features of a patient with paraneoplastic cerebellar dysfunc- tion [abstract] Neurology 198737(suppl 1)305-306
31 Anderson NE Budde-Steffen C Wiley RG et al A variant of the anti-Purkinje cell antibody in a patient with paraneo- plastic cerebellar degeneration Neurology 1988381018- 1026
32 Tsukamoto T Yamamoto H Iwasaki Y Yoshie 0 Terunuma H Suzuki H Antineural autoantibodies in patients with paraneoplastic cerebellar degeneration Arch Neurol
33 Gram F Illa I Agusti M Ribalta T Cruz-Sanchez F Juarez C Effect of intraventricular injection of an anti-Purkinje cell antibody (anti-Yo) in a guinea pig model J Neurol Sci
198314609-613
1989461225-1229
199110682-87
October 1992 NEUROLOGY 42 1937
DOI 101212WNL421019311992421931 Neurology
K Peterson MD M K Rosenblum H Kotanides MS et al positive patientsminus
Yo antibodyminusParaneoplastic cerebellar degeneration IA clinical analysis of 55 anti
This information is current as of October 1 1992
ServicesUpdated Information amp
httpnneurologyorgcontent42101931fullhtmlincluding high resolution figures can be found at
Citations httpnneurologyorgcontent42101931fullhtmlotherarticles
This article has been cited by 20 HighWire-hosted articles
Permissions amp Licensing
httpnneurologyorgmiscaboutxhtmlpermissionsor in its entirety can be found online atInformation about reproducing this article in parts (figurestables)
Reprints
httpnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Inc All rights reserved Print ISSN 0028-3878 Online ISSN 1526-632Xsince 1951 it is now a weekly with 48 issues per year Copyright copy 1992 by Edgell Communications
reg is the official journal of the American Academy of Neurology Published continuouslyNeurology

ined by one or more of the authors referring physicians sending sera andlor CSF for antibody testing provided the neurologic and oncologic profiles Telephone calls to the physicians most recently caring for the patients pro- vided follow-up as of December 1991 Microscopic slides and blocks of the cerebellum obtained at autopsy in three patients and tumor tissue in seven patients were studied directly by us
Serum and CSF database Approximately 2000 sera andor CSF samples have been examined in our laborato- ry for the presence of anticerebellar antibodies These samples were sent from throughout the United States and many other countries by physicians suspecting the diagnosis of a neurologic paraneoplastic syndrome Some patients had known cancers whereas others did not All samples were s tudied by immunofluorescence or immunoperoxidase histochemistry and by Western blot- ting against Purkinje cell extracts A search of the data- bank also identified all patients in 1989 and 1990 with cerebellar syndromes with or without cancer and all patients with ovarian or breast cancer with or without cerebellar syndromes
Immunologic techniques Immunohistochemistry and Western blott ing techniques against Purkinje cell extracts as well as the CDR 62 fusion protein that corre- sponds to the 62 kd antigen to which the anti-Yo anti- body binds have been described extensively in previous publications from this l a b ~ r a t o r y ~ - ~
Results Immunologic findings Serum or CSF from 55 patients was positive for the anti-Yo anti- body as determined by immunohistochemistry and Western blotting In 41 of 41 patients tested sera also reacted positively against the Yo fusion pro- tein14
Several patients who had atypical histochemical staining andor atypical immunoblotting were excluded Excluded patients included one whose serum was positive by histochemistry but reacted on Western blotting against Purkinje cell extracts with a band of 68 kd (but not 34 kd ) and was neg- ative against the Yo fusion protein Three patients had atypical Purkinje cell cytoplasmic staining and were negative on immunoblotting Two patients with PCD showed neuronal nuclear staining and a band at 35 to 40 kd on Western blot (typical of the anti-Hu antibody) but were negative when tested against the Yo fusion protein and one other with atypical nuclear staining was negative with both immunoblotting techniques
Thirteen patients with Hodgkins disease and PCD 45 patients with breast cancer and 24 with ovarian cancer with or without cerebellar syn- dromes 325 patients with cerebellar syndromes with or without cancer and 50 normal controls (blood bank donors) were also negative by both his- tochemistry and immunoblotting
Clinical results The 55 patients with the typical anti-Yo antibody presented a stereotypic clinical syndrome All patients were women 26 to 85 years old
Tumors Fifty-two of the patients currently have histologically proven malignancies The most com- mon tumor ovarian was found in 26 of 55 patients
1932 NEUROLOGY 42 October 1992
13 had breast cancer and seven had other gyneco- logic malignancies (four endometrial two fallopian tube and one mesovarium) One patient had both breast and fallopian tube cancers One patient had an adenocarcinoma of the lung and is without known gynecologic malignancy
There were six patients with adenocarcinoma of unknown primary Three of these presented with axillary nodes likely representing breast cancer although no primary was found in the breast One patient with adenocarcinoma of unknown primary had had resection 2 years previously of an ovarian mass that had shown benign pathology at autopsy this patient was found to have had a periaortic node pathologically suggestive of ovarian cancer and had staining for CA 125 antigen which is asso- ciated with ovarian cancers One patient presented with carcinoma in an inguinal lymph node One other patient had a poorly differentiated adenocar- cinoma in an abdominal lymph node compatible with ovarian cancer but no ovarian tumor was found At autopsy 3 years later she was found to have a hepatoma but no adenocarcinoma the origi- nal primary was not found
Three patients had no tumor identified One of these patients had resection of an ovarian mass with benign histology (ovarian cystadenoma) she died 24 months after the onset of her neurologic syndrome and no cancer was found at autopsy Two patients are still living up to 24 months after the onset of their neurologic disorder and have so far shown no evidence of malignancy despite serial physical and radiologic examinations
In 34 of 52 patients with known cancer the neu- rologic syndrome preceded the diagnosis of malig- nancy by up to 15 months and in many of the cases prompted a search for the underlying cancer Of these 34 patients 16 had ovarian cancer notably four had microscopic disease not found by routine diagnostic testing and detected only at laparotomy However one patient with a negative mammogram and normal pelvic examination underwent laparoscopy with ovarian biopsy and then hys- terectomy and bilateral salpingo-oophorectomy without a malignancy being found Four months after the initial normal mammogram a breast abnormality was detected and biopsy revealed an intraductal carcinoma
Most patients with known cancer had limited oncologic disease at the time of onset of neurologic symptoms with only 7 of 52 having evidence of widely metastatic cancer Ten patients had local disease 26 had regional metastases and six patients were in remission Three patients present- ed with neurologic symptoms coincident with recur- rence of a malignancy that had previously been in remission
Neurologic findings Patients presented with a characteristic pancerebellar disorder with truncal and limb ataxia dysarthria and nystagmus of subacute onset (1 day to 16 weeks) and subsequent stabilization Complete details of the neurologic
examination were available to us in 48 patients The ataxia was init ially asymmetric in 20 although in most ataxia became symmetric as the disease progressed Most patients were severely disabled by the neurologic syndrome with 37 of 48 patients being unable to walk or sit unassisted due to severe ataxia 9 of 48 could walk with some assistance and 2 of 48 could walk unassisted but were unsteady
All patients had some degree of horizontal nys- tagmus with a rotatory or vertical component in twenty-seven Seventeen patients were specifically reported to have downbeating nystagmus All of the 10 patients we examined had downbeating nys- tagmus we suspect that this finding was underre- ported in records we reviewed Five patients reported oscillopsia and 19 patients experienced diplopia However limitation of extraocular move- ments with unilateral or bilateral abducens palsies was detected in only six In 20 patients there was other bulbar involvement including dysphagia in 16 and facial weakness in seven Opsoclonus was reported in two patients and sleep myoclonus in one other
Signs or symptoms of involvement at other lev- els of the neuraxis were common but usually mild Although accurate mental status testing was diffi- cult t o confirm because of dysarthria and motor dysfunction 10 patients were believed clinically to have some cognitive impairment usually emotional lability and memory deficit Twenty-eight had extensor plantar responses or other long-tract signs Two patients had extrapyramidal rigidity and tremor or dyskinesias Twenty-six had hypore- flexia or mild distal sensory complaints suggesting peripheral neuropathy Two patients had progres- sive visual loss This finding was believed clinically to be a result of either optic neuropathy or retinal degeneration although this was unconfirmed by electrographic studies
Headache was an uncommon complaint promi- nent in only six patients Twenty patients com- plained of vertigo Nausea and vomiting were debil- itating symptoms in two
None of the patients was known t o have other immunologic rheumatic or collagen vascular dis- eases save for hypothyroidism in two patients and adult-onset diabetes mellitus in one
Laboratory eualuation CSF examination was performed in all patients Of the 42 patients in whom detailed CSF results were available only seven had normal CSF Thirty-five patients had inflammatory changes that included a predomi- nantly lymphocytic pleocytosis (between 6 and 93 WBCmm3) in 26 of 42 and elevated protein (between 48 and 106 mgdl) in 22 of 42 patients The ratio of CSF to serum IgG was increased in 12 of 14 patients for whom this information was avail- able oligoclonal bands were present in 6 of 7 patients tested and elevated myelin basic protein reported in one
CT andor MRI was performed in all patients
Table 1 Clinical findings in 55 anti-Yo-positive PCD patients
Sex Women Men
26 to 85 years
Before diagnosis of cancer After diagnosis of cancer No cancer known
Severe (unable to walk) Moderate (walks with assist) Mild (walks but unsteady) Severity not known
Rotatory or vertical
EOM abnormality detected
Age
Time of neurologic presentation
Ataxia
Nystagmus
Dip 1 o p i a
Opsoclonus Myoclonus Dysphagia Facial weakness Cognitive impairment Long-tract signs Extrapyramidal signs Peripheral neuropathy Progressive visual loss Headache Vertigo Severe nausea and vomiting CSF
Negative cytology Normal Inflammatory Details not known
Negative for metastasis Cerebellar atrophy
Immunosuppressive therapy Plasmapheresis Steroids Cyclophosphamide Azathioprine ACTH
No response Mild transient improvement Mild sustained improvement
CT or MRI
Response to therapy
Living (291) Died
55 0
61 (median)
34 18 3
55 37 9 2 7
55 27 19 6 2 1
16 7
10 28 2
26 2 6
20 2
55 7
35 13
55 17 29 22 17 4 2 1
23 5 1
36 19
EOM Extraocular movement
Most of these studies were init ially normal although 17 patients had evidence of cerebellar atrophy on CT or MRI particularly later in the dis- ease process In seven patients studied with 18F-flu- orodeoxyglucose positron emission tomography the mean regional metabolic rate for glucose was sig-
October 1992 NEUROLOGY 42 1933
~~~~~~ ~ ~~ ~
Figure (A) Photomicrograph of normal cerebellar cortex from a 55-year-old man who died of disseminated carcinoma without neurologic involvement Purkinje cells are prominent at the junction of the molecular and granular layers (hematoxylin-eosin XlOO before 29 reduction) (B) View of the cerebellar cortex from a patient who died with anti- Yo-positive PCD demonstrating total Purkinje cell loss Note the absence of inflammatory infiltrates (hematoxylin-eosin XlOO before 29 reduction)
nificantly reduced in the cerebellum and several cortical regions as well when compared with that of normal indi~idua1sl~
Treatment On the rationale that this neurologic syndrome was autoimmune several immuno- suppressive therapies were tried in various combi- nations in a total of 29 patients These included plasmapheresis i n 22 pat ients (a t least five exchanges) There was mild but transient improve- ment in the symptoms of ataxia and dysarthria in four patients Another patient had a moderate sus- tained benefit regaining her ability to walk with assistance This correlated with a decrease in her serum antibody titers from 14000 pre-treatment t o 1200 post-treatment However five other patients with documented decline in serum anti- body titers after treatment showed no clinical response possibly related to the finding that there was no corresponding decline in CSF antibody titers16 High-dose steroids (40 to 100 mgd for at least 2 weeks) gave mild but transient improve- ment in one of 17 patients treated There was no beneficial effect of cyclophosphamide in four patients azathioprine in two o r ACTH in one patient One patient was reported t o have had moderate improvement with treatment of the underlying tumor
At the time of most recent follow-up 36 patients are still living up to 77 months after the onset of neurologic symptoms Most of these are in remis- sion from their malignancies but remain severely disabled neurologically Nineteen patients have died between 2 and 36 months after the onset of their neurologic symptoms due to progression of their oncologic disease and inanition (table 1)
Pathology The neuropathologic findings at
1934 NEUROLOGY 42 October 1992
autopsy were available for review in three cases and conformed to previous descriptions of PCD in patients with breast and gynecologic ~ a n c e r ~ All were characterized chiefly by cerebellar cortical atrophy with near-total depletion of Purkinje cells and proliferation of Bergmann astrocytes (figure) Thinning of the granule cell population was an additional feature of two cases Scattered small lymphocytes mainly T-cells by immunotyping were noted in the cerebellar leptomeninges but in no case were inflammatory infiltrates identified in the cerebellar cortex proper Small numbers of mature lymphocytes again mainly T-cells also cuffed blood vessels in the dentate nucleus but were not associated with appreciable neuronal loss As expected the dentate amiculum (composed nor- mally of Purkinje cell axons) exhibited axonal depopulation and secondary demyelination in all cases
Microscopic sections of the PCD-associated neo- plasm at its primary site were available for review in seven cases (one fallopian tube one endometrial two mammary and three ovarian) Both breast pri- maries were high-grade poorly differentiated infil- t r a t ing adenocarcinomas of the duct type Similarly the endometrial ovarian and tuba1 neo- plasms were found to be high-grade mullerian ade- nocarcinomas composed of solid and papillary ele- ments An unusual and striking feature common to the stroma of all seven neoplasms was a conspicu- ous lymphoid infiltrate dominated by mature plas- ma cells As previously described12 expression of the Yo antigen by PCD-associated neoplasms was demonstrable in immunohistochemical and Western blot assay in all 10 instances in which fresh tumor tissue was available for analysis
Table 2 Autoantibodies in paraneoplastic cerebellar degeneration
Antigen distribution titer (immunohistochemistry)
Immunoblots (antigen Mr) Author Tumor (no)
Hodgkinrsquos ( 1 ) Trotter et a120 1976
Stefansson et ally 1981
Brown et alZ2 1985
Purkinje cell cytoplasm 120
Axons dendrites in cerebral cerebellar cortex
Purkinje cell cytoplasm neurons in deep cerebellar nuclei brainstem forebrain
Purkinje cell cytoplasm
Hodgkinrsquos (1)
Lung (small cell) (1) 85 Mouse cerebellum brain spinal cord
210 Kornguth et aP3 1985
Rodriguez et aP4 1986
Tanaka et aP6 1986
Ovary (1)
ldquoGynecologic cancerrdquo (4) Purkinje cell cytoplasm
Non-Hodgkinrsquos (1) Purkinje cell cytoplasm 250 125 (cerebrum) 125 (cerebellum) Rat cytoplasmic proteins
- Greenlee and BrasheaP 1983
Greenlee et aP1986 Greenlee and Liptonz8 1986
Jaeckle e t a18 1985
Purkinje cell cytoplasm 1640
Purkinje and granule cell cytoplasm Purkinje and granule cell nuclei CNS neurons 1320
Purkinje cell cytoplasm 11000
Ovary breast (9)
Lung (small cell) (3) Breast (1)
34-38 62-64 Human Purkinje cell
Ovary breast (7)
Cunningham et alg 1986
Bourdette and N i I a ~ e r ~ ~ 1987
Royal et a130 1987
Anderson et al3I 1988
Lung (small cell) (5) Hodgkinrsquos (5)
Benign monoclonal gammopathy
Breast (1)
Absent Absent
Purkinje cell cytoplasm
Purkinje cell cytoplasm 34-38 62-64
5664 68 80 Purkinje cell cytoplasm fine granular pattern human rat rabbit bovine 13000
Weak staining cortical hippocampal brainstem neurons 1 5 0
Purkinje cell cytoplasm
Lung (adeno) (1)
Ovary (9) breast (61 adenocarcinoma
unknown 1rdquo (3) Lung (adeno) (l) colon (1) Lung (small cell) (1) Breast (1)
34-38 62-64
-
35-40 (anti-Hu) 53-61 79-84
5258
3046 3840
Anderson et a17 1988
Purkinje cell cytoplasm
All neuronal nuclei All neuronal nuclei
Ovary (21 uterus (2)
Purkinje stellate basket cells deep cerebellar nuclei cortical hippocampal neurons 110000 All neuronal cells 1100000
Tsukamoto et a P 1989
Breast ( l ) lung (1)
October 1992 NEUROLOGY 42 1935
Discussion This report confirms and extends findings previously reported on 18 patients from this laboratory7 and in a similar survey of 32 PCD patients published recently from the Mayo Clinic In the Mayo series 16 antibody-positive patients were identified17 From these reports emerges a rather stereotypic picture of the anti-Yo antibody- positive PCD patient Always female and usually not previously known to have cancer she develops over a matter of weeks a severe pancerebellar dis- order with t runcal and appendicular a taxia dysarthria and nystagmus often with a downbeat- ing component The clinical findings stabilize with- in a couple of months leaving most patients unable to walk without the assistance of one or two people unable to write legibly frequently unable to read or watch television because of oscillopsia or diplopia and having difficulty in being understood when speaking The behavioral and long-tract signs when present are usually mild and opsoclonus and myoclonus are not characteristic features Interestingly two of our patients had progressive prechiasmal visual loss possibly due to optic neu- ropathy or retinal degeneration Most patients remain stable but severely disabled and except in a few isolated cases18 do not improve with plasma- pheresis or immunosuppression With few excep- tions the anti-Yo antibody-positive PCD patient is eventually found to have an associated gynecologic cancer
Several different autoantibodies have been iden- tified in patients with PCD (table 2) In comparison with anti-Yo-positive PCD patients those without the anti-Yo antibody though pathologically simi- lar are frequently clinically distinct and make up a heterogeneous group Taken together patients without the anti-Yo antibody have an approximate- ly equal sex distribution a variety of associated malignancies (most commonly bronchial carcinoma and Hodgkinrsquos lymphoma) and more frequently present with their neurologic syndrome after the malignancy has been diagnosed Particular subsets of patients with PCD are discussed in the following two papers and e l s e ~ h e r e ~ - ~ J ~ J ~ ~ ~ ~
With the data reported here and with other recently reported cases or series of PCD it seems likely that PCD is a group of disorders each related to a particular cancer or cancers The utility of dif- ferentiating between the different anti-Purkinje cell antibodies is that when a particular antibody is present such as anti-Yo it strongly suggests the presence of an underlying neoplasm and directs the search for the occult malignancy to one or a few organs We believe that the presence of the anti-Yo antibody warran ts a n aggressive diagnostic approach that begins with careful breast and pelvic examination mammography pelvic CT and mea- surement of ovarian tumor antigen CA 125 If no malignancy is revealed with this initial workup repeat mammography pelvic examination under anesthesia and uterine D amp C should be per- formed If there is still no cancer evident surgical
1936 NEUROLOGY 42 October 1992
exploration and removal of pelvic organs may be warranted particularly in the postmenopausal woman
Unfortunately early detection and even cure of the underlying cancer does not usually affect the neurologic symptoms Although there are occasion- al reports of patients with paraneoplastic syn- dromes responding to treatment of the underlying tumor21 none of the patients in this series substan- tially improved after successful treatment of the cancer and follow-up of more than 4 years In none of the patients has there been progression of the cerebellar dysfunction after treatment of the can- cer however in most of the patients the cerebellar dysfunction had stabilized by the time the cancer diagnosis was made and treatment instituted Interestingly the anti-Yo antibody has persisted in all the patients we have followed after what is assumed to be successful treatment of the cancer In two patients in remission for more than 4 years the antibody persists in the serum although there has been no progression of their cerebellar dysfunc- tion or evidence of recurrent tumor Thus the major importance of identification of the anti-Yo antibody is that early diagnosis leads to treatment and at times cure of the cancer Identification of the antibody does not appear to be helpful in ame- liorating the neurologic disease
The pathogenesis of anti-Yo-positive PCD is unknown The high titer of antibody suggests an autoimmune mechanism but there are no reports of successful attempts to reproduce the disease in experimental animals A recent report of intrathe- cal injection of anti-Yo antibodies into experimen- tal animals was apparently successful in getting the antibody to the Purkinje cells but not in caus- ing neurologic dy~funct ion~~ Furthermore autopsy studies indicate that in most patients there is no inflammation around the degenerated Purkinje cells Thus there is no direct evidence for either a humoral- o r cell-mediated immune reaction in patients with anti-Yo-positive PCD Further work will be necessary to establish the pathogenesis of the disorder
References 1
2
3
4
5
6
Brain WR Daniel PM Greenfield JG Subacute cortical cerebellar degeneration and its relation t o carcinoma J Neurol Neurosurg Psychiatry 19511459-75 Brain WR Wilkinson M Subacute cerebellar degeneration associated with neoplasms Brain 196588465-478 Henson RA Urich H eds Cancer and the nervous system the neurological manifestations of systemic disease Oxford UK Blackwell Scientific 1982346-367 Hammack JE Posner JB Paraneoplastic cerebellar degen- eration In Plaitakis A ed Cerebellar degenerations clini- cal neurobiology Boston Kluwer Academic 1992 Anderson NE Rosenblum MK Graus F Wiley RG Posner JB Autoantibodies in paraneoplastic syndromes associated with small-cell lung cancer Neurology 1988381391-1398 Dalmau J Graus F Rosenblum MK Posner JB Anti-Hu associated paraneoplastic encephalomyelitissensory neu- ronopathy a clinical s tudy of 7 1 pa t ien ts Medicine 19927159-72
7 Anderson NE Rosenblum MK Posner JB Paraneoplastic cerebellar degeneration clinical-immunological correlations Ann Neurol 198824559-567
8 Jaeckle KA Graus F Houghton A Cardon-Cardo C Nielsen SL Posner JB Autoimmune response of patients with para- neoplastic cerebellar degeneration t o a Purkinje cell cyto- plasmic protein antigen Ann Neurol 198518592-600
9 Cunningham J Graus F Anderson N Posner JB Partial characterization of the Purkinje cell antigens in paraneo- plastic cerebellar degeneration Neurology 1986361163- 1168
10 Dropcho EJ Chen Y Posner JB Old LJ Cloning of a brain protein identified by autoantibodies from a patient with paraneoplastic cerebellar degeneration Proc Natl Acad Sci
11 Furneaux HM Dropcho E J Barbut D e t al Characterization of a cDNA encoding a 34-kDa Purkinje neuron protein recognized by sera from patients with para- neoplastic cerebellar degeneration Proc Natl Acad Sci USA
12 Furneaux HM Rosenblum MK Dalmau J Wong E Woodruff P Posner JB Selective expression of Purkinje cell antigens in tumor tissue derived from patients with parane- oplastic cerebellar degenerat ion N Engl J Med
13 Chen Y Rettig WJ Yenamandra AK e t a] Cerebellar degeneration-related (CDR) antigen a highly conserved neu- roectodermal marker mapped to chromosome X in human and mouse Proc Natl Acad Sci USA 1990873077-3081
14 Fathallah-Shaykh H Wolf S Wong E Posner JB Furneaux HM Cloning of a leucine zipper protein recognized by the sera of patients with antibody-associated paraneoplastic cerebellar degenerat ion Proc N a t l Acad Sci USA
15 Anderson NE Posner JB Sidtis J J e t al The metabolic anatomy of paraneoplastic cerebellar degeneration Ann Neurol 198823533-540
16 Gram F Abos J Roquer J Mazzara R Pereira A Effect of plasmapheresis on serum and CSF autoantibody levels in CNS paraneoplastic syndromes Neurology 1990401621- 1623
17 Hammack J E Kimmel DW OrsquoNeill BP Lennon VA Paraneoplastic cerebellar degeneration a clinical compari- son of patients with and without Purkinje cell cytoplasmic antibodies Mayo Clin Proc 1990651423-1431
18 Cocconi G Ceci G Jinvarra G et al Successful treatment of subacute cerebellar degeneration in ovarian carcinoma with plasmapheresis a case report Cancer 1985562318-2320
19 Stefansson K Ante1 JP Wollman RL Levin KH Larson R Arnason BGW Anti-neuronal antibodies in serum of a pat ient with Hodgkinrsquos disease and cerebellar a taxia [abstract] Neurology 198131(No 4 Pt 2)126
USA 1987844552-4556
1989862873-2877
19903221844-1851
1991883451-3454
20 Trotter JL Hendin BA Osterland CK Cerebellar degenera- tion with Hodgkinrsquos disease an immunological study Arch Neurol 197633660-661
21 Kearsley JH Johnson P Halmagyi GM Paraneoplastic cerebellar disease remission with excision of the primary tumor Arch Neurol 1985421208-1210
22 Brown RH J r Ronthal M Come S et al Antibodies t o 85000 dalton protein in paracarcinomatous cerebellar degeneration [abstract] Neurology 198535(suppl 1)288
23 Kornguth S Kalinke T Grunwald G Brooks B Zimmerman E Anti-neurofilament antibodies associated with paraneo- plastic syndromes [abstract] Fed Proc 198544966
24 Rodriguez M Truh LI OrsquoNeill BP Lennon VA Autoimmune paraneoplastic cerebellar degeneration ultrastructural localization of antibody-binding sites in Purkinje cells Neurology 1988381380-1386
25 Tanaka K Yamazaki M Sat0 S Toyoshima I Yamamoto A Miyatake T Antibodies to brain proteins in paraneoplastic cerebellar degeneration Neurology 1986361169-1172
26 Greenlee J E Brashear HR Antibodies to cerebellar Purkinje cells in patients with paraneoplastic cerebellar degenerat ion a n d ovarian carcinoma Ann Neurol
27 Greenlee J E Brashear HR Jaeckle KA Stroop WG Anticerebellar antibodies in sera of patients with paraneo- plastic cerebellar degeneration studies of antibody specifici- ty and response to plasmapheresis [abstract] Ann Neurol 198620 139
28 Greenlee JE Lipton HL Anticerebellar antibodies in serum and cerebrospinal fluid of a patient with oat cell carcinoma of the lung and paraneoplastic cerebellar degeneration Ann Neurol 19861982-85
29 Bourdette DN Nilaver G Cerebellar degeneration associat- ed with anti-Purkinje cell antibodies and benign IgG mono- clonal gammopathies [abstract] Neurology 198737(suppl 1)291
30 Royal W 111 Galasko DR McKhann GM Cunningham JM Dropcho EJ Clinical course immunologic and biochemical features of a patient with paraneoplastic cerebellar dysfunc- tion [abstract] Neurology 198737(suppl 1)305-306
31 Anderson NE Budde-Steffen C Wiley RG et al A variant of the anti-Purkinje cell antibody in a patient with paraneo- plastic cerebellar degeneration Neurology 1988381018- 1026
32 Tsukamoto T Yamamoto H Iwasaki Y Yoshie 0 Terunuma H Suzuki H Antineural autoantibodies in patients with paraneoplastic cerebellar degeneration Arch Neurol
33 Gram F Illa I Agusti M Ribalta T Cruz-Sanchez F Juarez C Effect of intraventricular injection of an anti-Purkinje cell antibody (anti-Yo) in a guinea pig model J Neurol Sci
198314609-613
1989461225-1229
199110682-87
October 1992 NEUROLOGY 42 1937
DOI 101212WNL421019311992421931 Neurology
K Peterson MD M K Rosenblum H Kotanides MS et al positive patientsminus
Yo antibodyminusParaneoplastic cerebellar degeneration IA clinical analysis of 55 anti
This information is current as of October 1 1992
ServicesUpdated Information amp
httpnneurologyorgcontent42101931fullhtmlincluding high resolution figures can be found at
Citations httpnneurologyorgcontent42101931fullhtmlotherarticles
This article has been cited by 20 HighWire-hosted articles
Permissions amp Licensing
httpnneurologyorgmiscaboutxhtmlpermissionsor in its entirety can be found online atInformation about reproducing this article in parts (figurestables)
Reprints
httpnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Inc All rights reserved Print ISSN 0028-3878 Online ISSN 1526-632Xsince 1951 it is now a weekly with 48 issues per year Copyright copy 1992 by Edgell Communications
reg is the official journal of the American Academy of Neurology Published continuouslyNeurology

examination were available to us in 48 patients The ataxia was init ially asymmetric in 20 although in most ataxia became symmetric as the disease progressed Most patients were severely disabled by the neurologic syndrome with 37 of 48 patients being unable to walk or sit unassisted due to severe ataxia 9 of 48 could walk with some assistance and 2 of 48 could walk unassisted but were unsteady
All patients had some degree of horizontal nys- tagmus with a rotatory or vertical component in twenty-seven Seventeen patients were specifically reported to have downbeating nystagmus All of the 10 patients we examined had downbeating nys- tagmus we suspect that this finding was underre- ported in records we reviewed Five patients reported oscillopsia and 19 patients experienced diplopia However limitation of extraocular move- ments with unilateral or bilateral abducens palsies was detected in only six In 20 patients there was other bulbar involvement including dysphagia in 16 and facial weakness in seven Opsoclonus was reported in two patients and sleep myoclonus in one other
Signs or symptoms of involvement at other lev- els of the neuraxis were common but usually mild Although accurate mental status testing was diffi- cult t o confirm because of dysarthria and motor dysfunction 10 patients were believed clinically to have some cognitive impairment usually emotional lability and memory deficit Twenty-eight had extensor plantar responses or other long-tract signs Two patients had extrapyramidal rigidity and tremor or dyskinesias Twenty-six had hypore- flexia or mild distal sensory complaints suggesting peripheral neuropathy Two patients had progres- sive visual loss This finding was believed clinically to be a result of either optic neuropathy or retinal degeneration although this was unconfirmed by electrographic studies
Headache was an uncommon complaint promi- nent in only six patients Twenty patients com- plained of vertigo Nausea and vomiting were debil- itating symptoms in two
None of the patients was known t o have other immunologic rheumatic or collagen vascular dis- eases save for hypothyroidism in two patients and adult-onset diabetes mellitus in one
Laboratory eualuation CSF examination was performed in all patients Of the 42 patients in whom detailed CSF results were available only seven had normal CSF Thirty-five patients had inflammatory changes that included a predomi- nantly lymphocytic pleocytosis (between 6 and 93 WBCmm3) in 26 of 42 and elevated protein (between 48 and 106 mgdl) in 22 of 42 patients The ratio of CSF to serum IgG was increased in 12 of 14 patients for whom this information was avail- able oligoclonal bands were present in 6 of 7 patients tested and elevated myelin basic protein reported in one
CT andor MRI was performed in all patients
Table 1 Clinical findings in 55 anti-Yo-positive PCD patients
Sex Women Men
26 to 85 years
Before diagnosis of cancer After diagnosis of cancer No cancer known
Severe (unable to walk) Moderate (walks with assist) Mild (walks but unsteady) Severity not known
Rotatory or vertical
EOM abnormality detected
Age
Time of neurologic presentation
Ataxia
Nystagmus
Dip 1 o p i a
Opsoclonus Myoclonus Dysphagia Facial weakness Cognitive impairment Long-tract signs Extrapyramidal signs Peripheral neuropathy Progressive visual loss Headache Vertigo Severe nausea and vomiting CSF
Negative cytology Normal Inflammatory Details not known
Negative for metastasis Cerebellar atrophy
Immunosuppressive therapy Plasmapheresis Steroids Cyclophosphamide Azathioprine ACTH
No response Mild transient improvement Mild sustained improvement
CT or MRI
Response to therapy
Living (291) Died
55 0
61 (median)
34 18 3
55 37 9 2 7
55 27 19 6 2 1
16 7
10 28 2
26 2 6
20 2
55 7
35 13
55 17 29 22 17 4 2 1
23 5 1
36 19
EOM Extraocular movement
Most of these studies were init ially normal although 17 patients had evidence of cerebellar atrophy on CT or MRI particularly later in the dis- ease process In seven patients studied with 18F-flu- orodeoxyglucose positron emission tomography the mean regional metabolic rate for glucose was sig-
October 1992 NEUROLOGY 42 1933
~~~~~~ ~ ~~ ~
Figure (A) Photomicrograph of normal cerebellar cortex from a 55-year-old man who died of disseminated carcinoma without neurologic involvement Purkinje cells are prominent at the junction of the molecular and granular layers (hematoxylin-eosin XlOO before 29 reduction) (B) View of the cerebellar cortex from a patient who died with anti- Yo-positive PCD demonstrating total Purkinje cell loss Note the absence of inflammatory infiltrates (hematoxylin-eosin XlOO before 29 reduction)
nificantly reduced in the cerebellum and several cortical regions as well when compared with that of normal indi~idua1sl~
Treatment On the rationale that this neurologic syndrome was autoimmune several immuno- suppressive therapies were tried in various combi- nations in a total of 29 patients These included plasmapheresis i n 22 pat ients (a t least five exchanges) There was mild but transient improve- ment in the symptoms of ataxia and dysarthria in four patients Another patient had a moderate sus- tained benefit regaining her ability to walk with assistance This correlated with a decrease in her serum antibody titers from 14000 pre-treatment t o 1200 post-treatment However five other patients with documented decline in serum anti- body titers after treatment showed no clinical response possibly related to the finding that there was no corresponding decline in CSF antibody titers16 High-dose steroids (40 to 100 mgd for at least 2 weeks) gave mild but transient improve- ment in one of 17 patients treated There was no beneficial effect of cyclophosphamide in four patients azathioprine in two o r ACTH in one patient One patient was reported t o have had moderate improvement with treatment of the underlying tumor
At the time of most recent follow-up 36 patients are still living up to 77 months after the onset of neurologic symptoms Most of these are in remis- sion from their malignancies but remain severely disabled neurologically Nineteen patients have died between 2 and 36 months after the onset of their neurologic symptoms due to progression of their oncologic disease and inanition (table 1)
Pathology The neuropathologic findings at
1934 NEUROLOGY 42 October 1992
autopsy were available for review in three cases and conformed to previous descriptions of PCD in patients with breast and gynecologic ~ a n c e r ~ All were characterized chiefly by cerebellar cortical atrophy with near-total depletion of Purkinje cells and proliferation of Bergmann astrocytes (figure) Thinning of the granule cell population was an additional feature of two cases Scattered small lymphocytes mainly T-cells by immunotyping were noted in the cerebellar leptomeninges but in no case were inflammatory infiltrates identified in the cerebellar cortex proper Small numbers of mature lymphocytes again mainly T-cells also cuffed blood vessels in the dentate nucleus but were not associated with appreciable neuronal loss As expected the dentate amiculum (composed nor- mally of Purkinje cell axons) exhibited axonal depopulation and secondary demyelination in all cases
Microscopic sections of the PCD-associated neo- plasm at its primary site were available for review in seven cases (one fallopian tube one endometrial two mammary and three ovarian) Both breast pri- maries were high-grade poorly differentiated infil- t r a t ing adenocarcinomas of the duct type Similarly the endometrial ovarian and tuba1 neo- plasms were found to be high-grade mullerian ade- nocarcinomas composed of solid and papillary ele- ments An unusual and striking feature common to the stroma of all seven neoplasms was a conspicu- ous lymphoid infiltrate dominated by mature plas- ma cells As previously described12 expression of the Yo antigen by PCD-associated neoplasms was demonstrable in immunohistochemical and Western blot assay in all 10 instances in which fresh tumor tissue was available for analysis
Table 2 Autoantibodies in paraneoplastic cerebellar degeneration
Antigen distribution titer (immunohistochemistry)
Immunoblots (antigen Mr) Author Tumor (no)
Hodgkinrsquos ( 1 ) Trotter et a120 1976
Stefansson et ally 1981
Brown et alZ2 1985
Purkinje cell cytoplasm 120
Axons dendrites in cerebral cerebellar cortex
Purkinje cell cytoplasm neurons in deep cerebellar nuclei brainstem forebrain
Purkinje cell cytoplasm
Hodgkinrsquos (1)
Lung (small cell) (1) 85 Mouse cerebellum brain spinal cord
210 Kornguth et aP3 1985
Rodriguez et aP4 1986
Tanaka et aP6 1986
Ovary (1)
ldquoGynecologic cancerrdquo (4) Purkinje cell cytoplasm
Non-Hodgkinrsquos (1) Purkinje cell cytoplasm 250 125 (cerebrum) 125 (cerebellum) Rat cytoplasmic proteins
- Greenlee and BrasheaP 1983
Greenlee et aP1986 Greenlee and Liptonz8 1986
Jaeckle e t a18 1985
Purkinje cell cytoplasm 1640
Purkinje and granule cell cytoplasm Purkinje and granule cell nuclei CNS neurons 1320
Purkinje cell cytoplasm 11000
Ovary breast (9)
Lung (small cell) (3) Breast (1)
34-38 62-64 Human Purkinje cell
Ovary breast (7)
Cunningham et alg 1986
Bourdette and N i I a ~ e r ~ ~ 1987
Royal et a130 1987
Anderson et al3I 1988
Lung (small cell) (5) Hodgkinrsquos (5)
Benign monoclonal gammopathy
Breast (1)
Absent Absent
Purkinje cell cytoplasm
Purkinje cell cytoplasm 34-38 62-64
5664 68 80 Purkinje cell cytoplasm fine granular pattern human rat rabbit bovine 13000
Weak staining cortical hippocampal brainstem neurons 1 5 0
Purkinje cell cytoplasm
Lung (adeno) (1)
Ovary (9) breast (61 adenocarcinoma
unknown 1rdquo (3) Lung (adeno) (l) colon (1) Lung (small cell) (1) Breast (1)
34-38 62-64
-
35-40 (anti-Hu) 53-61 79-84
5258
3046 3840
Anderson et a17 1988
Purkinje cell cytoplasm
All neuronal nuclei All neuronal nuclei
Ovary (21 uterus (2)
Purkinje stellate basket cells deep cerebellar nuclei cortical hippocampal neurons 110000 All neuronal cells 1100000
Tsukamoto et a P 1989
Breast ( l ) lung (1)
October 1992 NEUROLOGY 42 1935
Discussion This report confirms and extends findings previously reported on 18 patients from this laboratory7 and in a similar survey of 32 PCD patients published recently from the Mayo Clinic In the Mayo series 16 antibody-positive patients were identified17 From these reports emerges a rather stereotypic picture of the anti-Yo antibody- positive PCD patient Always female and usually not previously known to have cancer she develops over a matter of weeks a severe pancerebellar dis- order with t runcal and appendicular a taxia dysarthria and nystagmus often with a downbeat- ing component The clinical findings stabilize with- in a couple of months leaving most patients unable to walk without the assistance of one or two people unable to write legibly frequently unable to read or watch television because of oscillopsia or diplopia and having difficulty in being understood when speaking The behavioral and long-tract signs when present are usually mild and opsoclonus and myoclonus are not characteristic features Interestingly two of our patients had progressive prechiasmal visual loss possibly due to optic neu- ropathy or retinal degeneration Most patients remain stable but severely disabled and except in a few isolated cases18 do not improve with plasma- pheresis or immunosuppression With few excep- tions the anti-Yo antibody-positive PCD patient is eventually found to have an associated gynecologic cancer
Several different autoantibodies have been iden- tified in patients with PCD (table 2) In comparison with anti-Yo-positive PCD patients those without the anti-Yo antibody though pathologically simi- lar are frequently clinically distinct and make up a heterogeneous group Taken together patients without the anti-Yo antibody have an approximate- ly equal sex distribution a variety of associated malignancies (most commonly bronchial carcinoma and Hodgkinrsquos lymphoma) and more frequently present with their neurologic syndrome after the malignancy has been diagnosed Particular subsets of patients with PCD are discussed in the following two papers and e l s e ~ h e r e ~ - ~ J ~ J ~ ~ ~ ~
With the data reported here and with other recently reported cases or series of PCD it seems likely that PCD is a group of disorders each related to a particular cancer or cancers The utility of dif- ferentiating between the different anti-Purkinje cell antibodies is that when a particular antibody is present such as anti-Yo it strongly suggests the presence of an underlying neoplasm and directs the search for the occult malignancy to one or a few organs We believe that the presence of the anti-Yo antibody warran ts a n aggressive diagnostic approach that begins with careful breast and pelvic examination mammography pelvic CT and mea- surement of ovarian tumor antigen CA 125 If no malignancy is revealed with this initial workup repeat mammography pelvic examination under anesthesia and uterine D amp C should be per- formed If there is still no cancer evident surgical
1936 NEUROLOGY 42 October 1992
exploration and removal of pelvic organs may be warranted particularly in the postmenopausal woman
Unfortunately early detection and even cure of the underlying cancer does not usually affect the neurologic symptoms Although there are occasion- al reports of patients with paraneoplastic syn- dromes responding to treatment of the underlying tumor21 none of the patients in this series substan- tially improved after successful treatment of the cancer and follow-up of more than 4 years In none of the patients has there been progression of the cerebellar dysfunction after treatment of the can- cer however in most of the patients the cerebellar dysfunction had stabilized by the time the cancer diagnosis was made and treatment instituted Interestingly the anti-Yo antibody has persisted in all the patients we have followed after what is assumed to be successful treatment of the cancer In two patients in remission for more than 4 years the antibody persists in the serum although there has been no progression of their cerebellar dysfunc- tion or evidence of recurrent tumor Thus the major importance of identification of the anti-Yo antibody is that early diagnosis leads to treatment and at times cure of the cancer Identification of the antibody does not appear to be helpful in ame- liorating the neurologic disease
The pathogenesis of anti-Yo-positive PCD is unknown The high titer of antibody suggests an autoimmune mechanism but there are no reports of successful attempts to reproduce the disease in experimental animals A recent report of intrathe- cal injection of anti-Yo antibodies into experimen- tal animals was apparently successful in getting the antibody to the Purkinje cells but not in caus- ing neurologic dy~funct ion~~ Furthermore autopsy studies indicate that in most patients there is no inflammation around the degenerated Purkinje cells Thus there is no direct evidence for either a humoral- o r cell-mediated immune reaction in patients with anti-Yo-positive PCD Further work will be necessary to establish the pathogenesis of the disorder
References 1
2
3
4
5
6
Brain WR Daniel PM Greenfield JG Subacute cortical cerebellar degeneration and its relation t o carcinoma J Neurol Neurosurg Psychiatry 19511459-75 Brain WR Wilkinson M Subacute cerebellar degeneration associated with neoplasms Brain 196588465-478 Henson RA Urich H eds Cancer and the nervous system the neurological manifestations of systemic disease Oxford UK Blackwell Scientific 1982346-367 Hammack JE Posner JB Paraneoplastic cerebellar degen- eration In Plaitakis A ed Cerebellar degenerations clini- cal neurobiology Boston Kluwer Academic 1992 Anderson NE Rosenblum MK Graus F Wiley RG Posner JB Autoantibodies in paraneoplastic syndromes associated with small-cell lung cancer Neurology 1988381391-1398 Dalmau J Graus F Rosenblum MK Posner JB Anti-Hu associated paraneoplastic encephalomyelitissensory neu- ronopathy a clinical s tudy of 7 1 pa t ien ts Medicine 19927159-72
7 Anderson NE Rosenblum MK Posner JB Paraneoplastic cerebellar degeneration clinical-immunological correlations Ann Neurol 198824559-567
8 Jaeckle KA Graus F Houghton A Cardon-Cardo C Nielsen SL Posner JB Autoimmune response of patients with para- neoplastic cerebellar degeneration t o a Purkinje cell cyto- plasmic protein antigen Ann Neurol 198518592-600
9 Cunningham J Graus F Anderson N Posner JB Partial characterization of the Purkinje cell antigens in paraneo- plastic cerebellar degeneration Neurology 1986361163- 1168
10 Dropcho EJ Chen Y Posner JB Old LJ Cloning of a brain protein identified by autoantibodies from a patient with paraneoplastic cerebellar degeneration Proc Natl Acad Sci
11 Furneaux HM Dropcho E J Barbut D e t al Characterization of a cDNA encoding a 34-kDa Purkinje neuron protein recognized by sera from patients with para- neoplastic cerebellar degeneration Proc Natl Acad Sci USA
12 Furneaux HM Rosenblum MK Dalmau J Wong E Woodruff P Posner JB Selective expression of Purkinje cell antigens in tumor tissue derived from patients with parane- oplastic cerebellar degenerat ion N Engl J Med
13 Chen Y Rettig WJ Yenamandra AK e t a] Cerebellar degeneration-related (CDR) antigen a highly conserved neu- roectodermal marker mapped to chromosome X in human and mouse Proc Natl Acad Sci USA 1990873077-3081
14 Fathallah-Shaykh H Wolf S Wong E Posner JB Furneaux HM Cloning of a leucine zipper protein recognized by the sera of patients with antibody-associated paraneoplastic cerebellar degenerat ion Proc N a t l Acad Sci USA
15 Anderson NE Posner JB Sidtis J J e t al The metabolic anatomy of paraneoplastic cerebellar degeneration Ann Neurol 198823533-540
16 Gram F Abos J Roquer J Mazzara R Pereira A Effect of plasmapheresis on serum and CSF autoantibody levels in CNS paraneoplastic syndromes Neurology 1990401621- 1623
17 Hammack J E Kimmel DW OrsquoNeill BP Lennon VA Paraneoplastic cerebellar degeneration a clinical compari- son of patients with and without Purkinje cell cytoplasmic antibodies Mayo Clin Proc 1990651423-1431
18 Cocconi G Ceci G Jinvarra G et al Successful treatment of subacute cerebellar degeneration in ovarian carcinoma with plasmapheresis a case report Cancer 1985562318-2320
19 Stefansson K Ante1 JP Wollman RL Levin KH Larson R Arnason BGW Anti-neuronal antibodies in serum of a pat ient with Hodgkinrsquos disease and cerebellar a taxia [abstract] Neurology 198131(No 4 Pt 2)126
USA 1987844552-4556
1989862873-2877
19903221844-1851
1991883451-3454
20 Trotter JL Hendin BA Osterland CK Cerebellar degenera- tion with Hodgkinrsquos disease an immunological study Arch Neurol 197633660-661
21 Kearsley JH Johnson P Halmagyi GM Paraneoplastic cerebellar disease remission with excision of the primary tumor Arch Neurol 1985421208-1210
22 Brown RH J r Ronthal M Come S et al Antibodies t o 85000 dalton protein in paracarcinomatous cerebellar degeneration [abstract] Neurology 198535(suppl 1)288
23 Kornguth S Kalinke T Grunwald G Brooks B Zimmerman E Anti-neurofilament antibodies associated with paraneo- plastic syndromes [abstract] Fed Proc 198544966
24 Rodriguez M Truh LI OrsquoNeill BP Lennon VA Autoimmune paraneoplastic cerebellar degeneration ultrastructural localization of antibody-binding sites in Purkinje cells Neurology 1988381380-1386
25 Tanaka K Yamazaki M Sat0 S Toyoshima I Yamamoto A Miyatake T Antibodies to brain proteins in paraneoplastic cerebellar degeneration Neurology 1986361169-1172
26 Greenlee J E Brashear HR Antibodies to cerebellar Purkinje cells in patients with paraneoplastic cerebellar degenerat ion a n d ovarian carcinoma Ann Neurol
27 Greenlee J E Brashear HR Jaeckle KA Stroop WG Anticerebellar antibodies in sera of patients with paraneo- plastic cerebellar degeneration studies of antibody specifici- ty and response to plasmapheresis [abstract] Ann Neurol 198620 139
28 Greenlee JE Lipton HL Anticerebellar antibodies in serum and cerebrospinal fluid of a patient with oat cell carcinoma of the lung and paraneoplastic cerebellar degeneration Ann Neurol 19861982-85
29 Bourdette DN Nilaver G Cerebellar degeneration associat- ed with anti-Purkinje cell antibodies and benign IgG mono- clonal gammopathies [abstract] Neurology 198737(suppl 1)291
30 Royal W 111 Galasko DR McKhann GM Cunningham JM Dropcho EJ Clinical course immunologic and biochemical features of a patient with paraneoplastic cerebellar dysfunc- tion [abstract] Neurology 198737(suppl 1)305-306
31 Anderson NE Budde-Steffen C Wiley RG et al A variant of the anti-Purkinje cell antibody in a patient with paraneo- plastic cerebellar degeneration Neurology 1988381018- 1026
32 Tsukamoto T Yamamoto H Iwasaki Y Yoshie 0 Terunuma H Suzuki H Antineural autoantibodies in patients with paraneoplastic cerebellar degeneration Arch Neurol
33 Gram F Illa I Agusti M Ribalta T Cruz-Sanchez F Juarez C Effect of intraventricular injection of an anti-Purkinje cell antibody (anti-Yo) in a guinea pig model J Neurol Sci
198314609-613
1989461225-1229
199110682-87
October 1992 NEUROLOGY 42 1937
DOI 101212WNL421019311992421931 Neurology
K Peterson MD M K Rosenblum H Kotanides MS et al positive patientsminus
Yo antibodyminusParaneoplastic cerebellar degeneration IA clinical analysis of 55 anti
This information is current as of October 1 1992
ServicesUpdated Information amp
httpnneurologyorgcontent42101931fullhtmlincluding high resolution figures can be found at
Citations httpnneurologyorgcontent42101931fullhtmlotherarticles
This article has been cited by 20 HighWire-hosted articles
Permissions amp Licensing
httpnneurologyorgmiscaboutxhtmlpermissionsor in its entirety can be found online atInformation about reproducing this article in parts (figurestables)
Reprints
httpnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Inc All rights reserved Print ISSN 0028-3878 Online ISSN 1526-632Xsince 1951 it is now a weekly with 48 issues per year Copyright copy 1992 by Edgell Communications
reg is the official journal of the American Academy of Neurology Published continuouslyNeurology

~~~~~~ ~ ~~ ~
Figure (A) Photomicrograph of normal cerebellar cortex from a 55-year-old man who died of disseminated carcinoma without neurologic involvement Purkinje cells are prominent at the junction of the molecular and granular layers (hematoxylin-eosin XlOO before 29 reduction) (B) View of the cerebellar cortex from a patient who died with anti- Yo-positive PCD demonstrating total Purkinje cell loss Note the absence of inflammatory infiltrates (hematoxylin-eosin XlOO before 29 reduction)
nificantly reduced in the cerebellum and several cortical regions as well when compared with that of normal indi~idua1sl~
Treatment On the rationale that this neurologic syndrome was autoimmune several immuno- suppressive therapies were tried in various combi- nations in a total of 29 patients These included plasmapheresis i n 22 pat ients (a t least five exchanges) There was mild but transient improve- ment in the symptoms of ataxia and dysarthria in four patients Another patient had a moderate sus- tained benefit regaining her ability to walk with assistance This correlated with a decrease in her serum antibody titers from 14000 pre-treatment t o 1200 post-treatment However five other patients with documented decline in serum anti- body titers after treatment showed no clinical response possibly related to the finding that there was no corresponding decline in CSF antibody titers16 High-dose steroids (40 to 100 mgd for at least 2 weeks) gave mild but transient improve- ment in one of 17 patients treated There was no beneficial effect of cyclophosphamide in four patients azathioprine in two o r ACTH in one patient One patient was reported t o have had moderate improvement with treatment of the underlying tumor
At the time of most recent follow-up 36 patients are still living up to 77 months after the onset of neurologic symptoms Most of these are in remis- sion from their malignancies but remain severely disabled neurologically Nineteen patients have died between 2 and 36 months after the onset of their neurologic symptoms due to progression of their oncologic disease and inanition (table 1)
Pathology The neuropathologic findings at
1934 NEUROLOGY 42 October 1992
autopsy were available for review in three cases and conformed to previous descriptions of PCD in patients with breast and gynecologic ~ a n c e r ~ All were characterized chiefly by cerebellar cortical atrophy with near-total depletion of Purkinje cells and proliferation of Bergmann astrocytes (figure) Thinning of the granule cell population was an additional feature of two cases Scattered small lymphocytes mainly T-cells by immunotyping were noted in the cerebellar leptomeninges but in no case were inflammatory infiltrates identified in the cerebellar cortex proper Small numbers of mature lymphocytes again mainly T-cells also cuffed blood vessels in the dentate nucleus but were not associated with appreciable neuronal loss As expected the dentate amiculum (composed nor- mally of Purkinje cell axons) exhibited axonal depopulation and secondary demyelination in all cases
Microscopic sections of the PCD-associated neo- plasm at its primary site were available for review in seven cases (one fallopian tube one endometrial two mammary and three ovarian) Both breast pri- maries were high-grade poorly differentiated infil- t r a t ing adenocarcinomas of the duct type Similarly the endometrial ovarian and tuba1 neo- plasms were found to be high-grade mullerian ade- nocarcinomas composed of solid and papillary ele- ments An unusual and striking feature common to the stroma of all seven neoplasms was a conspicu- ous lymphoid infiltrate dominated by mature plas- ma cells As previously described12 expression of the Yo antigen by PCD-associated neoplasms was demonstrable in immunohistochemical and Western blot assay in all 10 instances in which fresh tumor tissue was available for analysis
Table 2 Autoantibodies in paraneoplastic cerebellar degeneration
Antigen distribution titer (immunohistochemistry)
Immunoblots (antigen Mr) Author Tumor (no)
Hodgkinrsquos ( 1 ) Trotter et a120 1976
Stefansson et ally 1981
Brown et alZ2 1985
Purkinje cell cytoplasm 120
Axons dendrites in cerebral cerebellar cortex
Purkinje cell cytoplasm neurons in deep cerebellar nuclei brainstem forebrain
Purkinje cell cytoplasm
Hodgkinrsquos (1)
Lung (small cell) (1) 85 Mouse cerebellum brain spinal cord
210 Kornguth et aP3 1985
Rodriguez et aP4 1986
Tanaka et aP6 1986
Ovary (1)
ldquoGynecologic cancerrdquo (4) Purkinje cell cytoplasm
Non-Hodgkinrsquos (1) Purkinje cell cytoplasm 250 125 (cerebrum) 125 (cerebellum) Rat cytoplasmic proteins
- Greenlee and BrasheaP 1983
Greenlee et aP1986 Greenlee and Liptonz8 1986
Jaeckle e t a18 1985
Purkinje cell cytoplasm 1640
Purkinje and granule cell cytoplasm Purkinje and granule cell nuclei CNS neurons 1320
Purkinje cell cytoplasm 11000
Ovary breast (9)
Lung (small cell) (3) Breast (1)
34-38 62-64 Human Purkinje cell
Ovary breast (7)
Cunningham et alg 1986
Bourdette and N i I a ~ e r ~ ~ 1987
Royal et a130 1987
Anderson et al3I 1988
Lung (small cell) (5) Hodgkinrsquos (5)
Benign monoclonal gammopathy
Breast (1)
Absent Absent
Purkinje cell cytoplasm
Purkinje cell cytoplasm 34-38 62-64
5664 68 80 Purkinje cell cytoplasm fine granular pattern human rat rabbit bovine 13000
Weak staining cortical hippocampal brainstem neurons 1 5 0
Purkinje cell cytoplasm
Lung (adeno) (1)
Ovary (9) breast (61 adenocarcinoma
unknown 1rdquo (3) Lung (adeno) (l) colon (1) Lung (small cell) (1) Breast (1)
34-38 62-64
-
35-40 (anti-Hu) 53-61 79-84
5258
3046 3840
Anderson et a17 1988
Purkinje cell cytoplasm
All neuronal nuclei All neuronal nuclei
Ovary (21 uterus (2)
Purkinje stellate basket cells deep cerebellar nuclei cortical hippocampal neurons 110000 All neuronal cells 1100000
Tsukamoto et a P 1989
Breast ( l ) lung (1)
October 1992 NEUROLOGY 42 1935
Discussion This report confirms and extends findings previously reported on 18 patients from this laboratory7 and in a similar survey of 32 PCD patients published recently from the Mayo Clinic In the Mayo series 16 antibody-positive patients were identified17 From these reports emerges a rather stereotypic picture of the anti-Yo antibody- positive PCD patient Always female and usually not previously known to have cancer she develops over a matter of weeks a severe pancerebellar dis- order with t runcal and appendicular a taxia dysarthria and nystagmus often with a downbeat- ing component The clinical findings stabilize with- in a couple of months leaving most patients unable to walk without the assistance of one or two people unable to write legibly frequently unable to read or watch television because of oscillopsia or diplopia and having difficulty in being understood when speaking The behavioral and long-tract signs when present are usually mild and opsoclonus and myoclonus are not characteristic features Interestingly two of our patients had progressive prechiasmal visual loss possibly due to optic neu- ropathy or retinal degeneration Most patients remain stable but severely disabled and except in a few isolated cases18 do not improve with plasma- pheresis or immunosuppression With few excep- tions the anti-Yo antibody-positive PCD patient is eventually found to have an associated gynecologic cancer
Several different autoantibodies have been iden- tified in patients with PCD (table 2) In comparison with anti-Yo-positive PCD patients those without the anti-Yo antibody though pathologically simi- lar are frequently clinically distinct and make up a heterogeneous group Taken together patients without the anti-Yo antibody have an approximate- ly equal sex distribution a variety of associated malignancies (most commonly bronchial carcinoma and Hodgkinrsquos lymphoma) and more frequently present with their neurologic syndrome after the malignancy has been diagnosed Particular subsets of patients with PCD are discussed in the following two papers and e l s e ~ h e r e ~ - ~ J ~ J ~ ~ ~ ~
With the data reported here and with other recently reported cases or series of PCD it seems likely that PCD is a group of disorders each related to a particular cancer or cancers The utility of dif- ferentiating between the different anti-Purkinje cell antibodies is that when a particular antibody is present such as anti-Yo it strongly suggests the presence of an underlying neoplasm and directs the search for the occult malignancy to one or a few organs We believe that the presence of the anti-Yo antibody warran ts a n aggressive diagnostic approach that begins with careful breast and pelvic examination mammography pelvic CT and mea- surement of ovarian tumor antigen CA 125 If no malignancy is revealed with this initial workup repeat mammography pelvic examination under anesthesia and uterine D amp C should be per- formed If there is still no cancer evident surgical
1936 NEUROLOGY 42 October 1992
exploration and removal of pelvic organs may be warranted particularly in the postmenopausal woman
Unfortunately early detection and even cure of the underlying cancer does not usually affect the neurologic symptoms Although there are occasion- al reports of patients with paraneoplastic syn- dromes responding to treatment of the underlying tumor21 none of the patients in this series substan- tially improved after successful treatment of the cancer and follow-up of more than 4 years In none of the patients has there been progression of the cerebellar dysfunction after treatment of the can- cer however in most of the patients the cerebellar dysfunction had stabilized by the time the cancer diagnosis was made and treatment instituted Interestingly the anti-Yo antibody has persisted in all the patients we have followed after what is assumed to be successful treatment of the cancer In two patients in remission for more than 4 years the antibody persists in the serum although there has been no progression of their cerebellar dysfunc- tion or evidence of recurrent tumor Thus the major importance of identification of the anti-Yo antibody is that early diagnosis leads to treatment and at times cure of the cancer Identification of the antibody does not appear to be helpful in ame- liorating the neurologic disease
The pathogenesis of anti-Yo-positive PCD is unknown The high titer of antibody suggests an autoimmune mechanism but there are no reports of successful attempts to reproduce the disease in experimental animals A recent report of intrathe- cal injection of anti-Yo antibodies into experimen- tal animals was apparently successful in getting the antibody to the Purkinje cells but not in caus- ing neurologic dy~funct ion~~ Furthermore autopsy studies indicate that in most patients there is no inflammation around the degenerated Purkinje cells Thus there is no direct evidence for either a humoral- o r cell-mediated immune reaction in patients with anti-Yo-positive PCD Further work will be necessary to establish the pathogenesis of the disorder
References 1
2
3
4
5
6
Brain WR Daniel PM Greenfield JG Subacute cortical cerebellar degeneration and its relation t o carcinoma J Neurol Neurosurg Psychiatry 19511459-75 Brain WR Wilkinson M Subacute cerebellar degeneration associated with neoplasms Brain 196588465-478 Henson RA Urich H eds Cancer and the nervous system the neurological manifestations of systemic disease Oxford UK Blackwell Scientific 1982346-367 Hammack JE Posner JB Paraneoplastic cerebellar degen- eration In Plaitakis A ed Cerebellar degenerations clini- cal neurobiology Boston Kluwer Academic 1992 Anderson NE Rosenblum MK Graus F Wiley RG Posner JB Autoantibodies in paraneoplastic syndromes associated with small-cell lung cancer Neurology 1988381391-1398 Dalmau J Graus F Rosenblum MK Posner JB Anti-Hu associated paraneoplastic encephalomyelitissensory neu- ronopathy a clinical s tudy of 7 1 pa t ien ts Medicine 19927159-72
7 Anderson NE Rosenblum MK Posner JB Paraneoplastic cerebellar degeneration clinical-immunological correlations Ann Neurol 198824559-567
8 Jaeckle KA Graus F Houghton A Cardon-Cardo C Nielsen SL Posner JB Autoimmune response of patients with para- neoplastic cerebellar degeneration t o a Purkinje cell cyto- plasmic protein antigen Ann Neurol 198518592-600
9 Cunningham J Graus F Anderson N Posner JB Partial characterization of the Purkinje cell antigens in paraneo- plastic cerebellar degeneration Neurology 1986361163- 1168
10 Dropcho EJ Chen Y Posner JB Old LJ Cloning of a brain protein identified by autoantibodies from a patient with paraneoplastic cerebellar degeneration Proc Natl Acad Sci
11 Furneaux HM Dropcho E J Barbut D e t al Characterization of a cDNA encoding a 34-kDa Purkinje neuron protein recognized by sera from patients with para- neoplastic cerebellar degeneration Proc Natl Acad Sci USA
12 Furneaux HM Rosenblum MK Dalmau J Wong E Woodruff P Posner JB Selective expression of Purkinje cell antigens in tumor tissue derived from patients with parane- oplastic cerebellar degenerat ion N Engl J Med
13 Chen Y Rettig WJ Yenamandra AK e t a] Cerebellar degeneration-related (CDR) antigen a highly conserved neu- roectodermal marker mapped to chromosome X in human and mouse Proc Natl Acad Sci USA 1990873077-3081
14 Fathallah-Shaykh H Wolf S Wong E Posner JB Furneaux HM Cloning of a leucine zipper protein recognized by the sera of patients with antibody-associated paraneoplastic cerebellar degenerat ion Proc N a t l Acad Sci USA
15 Anderson NE Posner JB Sidtis J J e t al The metabolic anatomy of paraneoplastic cerebellar degeneration Ann Neurol 198823533-540
16 Gram F Abos J Roquer J Mazzara R Pereira A Effect of plasmapheresis on serum and CSF autoantibody levels in CNS paraneoplastic syndromes Neurology 1990401621- 1623
17 Hammack J E Kimmel DW OrsquoNeill BP Lennon VA Paraneoplastic cerebellar degeneration a clinical compari- son of patients with and without Purkinje cell cytoplasmic antibodies Mayo Clin Proc 1990651423-1431
18 Cocconi G Ceci G Jinvarra G et al Successful treatment of subacute cerebellar degeneration in ovarian carcinoma with plasmapheresis a case report Cancer 1985562318-2320
19 Stefansson K Ante1 JP Wollman RL Levin KH Larson R Arnason BGW Anti-neuronal antibodies in serum of a pat ient with Hodgkinrsquos disease and cerebellar a taxia [abstract] Neurology 198131(No 4 Pt 2)126
USA 1987844552-4556
1989862873-2877
19903221844-1851
1991883451-3454
20 Trotter JL Hendin BA Osterland CK Cerebellar degenera- tion with Hodgkinrsquos disease an immunological study Arch Neurol 197633660-661
21 Kearsley JH Johnson P Halmagyi GM Paraneoplastic cerebellar disease remission with excision of the primary tumor Arch Neurol 1985421208-1210
22 Brown RH J r Ronthal M Come S et al Antibodies t o 85000 dalton protein in paracarcinomatous cerebellar degeneration [abstract] Neurology 198535(suppl 1)288
23 Kornguth S Kalinke T Grunwald G Brooks B Zimmerman E Anti-neurofilament antibodies associated with paraneo- plastic syndromes [abstract] Fed Proc 198544966
24 Rodriguez M Truh LI OrsquoNeill BP Lennon VA Autoimmune paraneoplastic cerebellar degeneration ultrastructural localization of antibody-binding sites in Purkinje cells Neurology 1988381380-1386
25 Tanaka K Yamazaki M Sat0 S Toyoshima I Yamamoto A Miyatake T Antibodies to brain proteins in paraneoplastic cerebellar degeneration Neurology 1986361169-1172
26 Greenlee J E Brashear HR Antibodies to cerebellar Purkinje cells in patients with paraneoplastic cerebellar degenerat ion a n d ovarian carcinoma Ann Neurol
27 Greenlee J E Brashear HR Jaeckle KA Stroop WG Anticerebellar antibodies in sera of patients with paraneo- plastic cerebellar degeneration studies of antibody specifici- ty and response to plasmapheresis [abstract] Ann Neurol 198620 139
28 Greenlee JE Lipton HL Anticerebellar antibodies in serum and cerebrospinal fluid of a patient with oat cell carcinoma of the lung and paraneoplastic cerebellar degeneration Ann Neurol 19861982-85
29 Bourdette DN Nilaver G Cerebellar degeneration associat- ed with anti-Purkinje cell antibodies and benign IgG mono- clonal gammopathies [abstract] Neurology 198737(suppl 1)291
30 Royal W 111 Galasko DR McKhann GM Cunningham JM Dropcho EJ Clinical course immunologic and biochemical features of a patient with paraneoplastic cerebellar dysfunc- tion [abstract] Neurology 198737(suppl 1)305-306
31 Anderson NE Budde-Steffen C Wiley RG et al A variant of the anti-Purkinje cell antibody in a patient with paraneo- plastic cerebellar degeneration Neurology 1988381018- 1026
32 Tsukamoto T Yamamoto H Iwasaki Y Yoshie 0 Terunuma H Suzuki H Antineural autoantibodies in patients with paraneoplastic cerebellar degeneration Arch Neurol
33 Gram F Illa I Agusti M Ribalta T Cruz-Sanchez F Juarez C Effect of intraventricular injection of an anti-Purkinje cell antibody (anti-Yo) in a guinea pig model J Neurol Sci
198314609-613
1989461225-1229
199110682-87
October 1992 NEUROLOGY 42 1937
DOI 101212WNL421019311992421931 Neurology
K Peterson MD M K Rosenblum H Kotanides MS et al positive patientsminus
Yo antibodyminusParaneoplastic cerebellar degeneration IA clinical analysis of 55 anti
This information is current as of October 1 1992
ServicesUpdated Information amp
httpnneurologyorgcontent42101931fullhtmlincluding high resolution figures can be found at
Citations httpnneurologyorgcontent42101931fullhtmlotherarticles
This article has been cited by 20 HighWire-hosted articles
Permissions amp Licensing
httpnneurologyorgmiscaboutxhtmlpermissionsor in its entirety can be found online atInformation about reproducing this article in parts (figurestables)
Reprints
httpnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Inc All rights reserved Print ISSN 0028-3878 Online ISSN 1526-632Xsince 1951 it is now a weekly with 48 issues per year Copyright copy 1992 by Edgell Communications
reg is the official journal of the American Academy of Neurology Published continuouslyNeurology

Table 2 Autoantibodies in paraneoplastic cerebellar degeneration
Antigen distribution titer (immunohistochemistry)
Immunoblots (antigen Mr) Author Tumor (no)
Hodgkinrsquos ( 1 ) Trotter et a120 1976
Stefansson et ally 1981
Brown et alZ2 1985
Purkinje cell cytoplasm 120
Axons dendrites in cerebral cerebellar cortex
Purkinje cell cytoplasm neurons in deep cerebellar nuclei brainstem forebrain
Purkinje cell cytoplasm
Hodgkinrsquos (1)
Lung (small cell) (1) 85 Mouse cerebellum brain spinal cord
210 Kornguth et aP3 1985
Rodriguez et aP4 1986
Tanaka et aP6 1986
Ovary (1)
ldquoGynecologic cancerrdquo (4) Purkinje cell cytoplasm
Non-Hodgkinrsquos (1) Purkinje cell cytoplasm 250 125 (cerebrum) 125 (cerebellum) Rat cytoplasmic proteins
- Greenlee and BrasheaP 1983
Greenlee et aP1986 Greenlee and Liptonz8 1986
Jaeckle e t a18 1985
Purkinje cell cytoplasm 1640
Purkinje and granule cell cytoplasm Purkinje and granule cell nuclei CNS neurons 1320
Purkinje cell cytoplasm 11000
Ovary breast (9)
Lung (small cell) (3) Breast (1)
34-38 62-64 Human Purkinje cell
Ovary breast (7)
Cunningham et alg 1986
Bourdette and N i I a ~ e r ~ ~ 1987
Royal et a130 1987
Anderson et al3I 1988
Lung (small cell) (5) Hodgkinrsquos (5)
Benign monoclonal gammopathy
Breast (1)
Absent Absent
Purkinje cell cytoplasm
Purkinje cell cytoplasm 34-38 62-64
5664 68 80 Purkinje cell cytoplasm fine granular pattern human rat rabbit bovine 13000
Weak staining cortical hippocampal brainstem neurons 1 5 0
Purkinje cell cytoplasm
Lung (adeno) (1)
Ovary (9) breast (61 adenocarcinoma
unknown 1rdquo (3) Lung (adeno) (l) colon (1) Lung (small cell) (1) Breast (1)
34-38 62-64
-
35-40 (anti-Hu) 53-61 79-84
5258
3046 3840
Anderson et a17 1988
Purkinje cell cytoplasm
All neuronal nuclei All neuronal nuclei
Ovary (21 uterus (2)
Purkinje stellate basket cells deep cerebellar nuclei cortical hippocampal neurons 110000 All neuronal cells 1100000
Tsukamoto et a P 1989
Breast ( l ) lung (1)
October 1992 NEUROLOGY 42 1935
Discussion This report confirms and extends findings previously reported on 18 patients from this laboratory7 and in a similar survey of 32 PCD patients published recently from the Mayo Clinic In the Mayo series 16 antibody-positive patients were identified17 From these reports emerges a rather stereotypic picture of the anti-Yo antibody- positive PCD patient Always female and usually not previously known to have cancer she develops over a matter of weeks a severe pancerebellar dis- order with t runcal and appendicular a taxia dysarthria and nystagmus often with a downbeat- ing component The clinical findings stabilize with- in a couple of months leaving most patients unable to walk without the assistance of one or two people unable to write legibly frequently unable to read or watch television because of oscillopsia or diplopia and having difficulty in being understood when speaking The behavioral and long-tract signs when present are usually mild and opsoclonus and myoclonus are not characteristic features Interestingly two of our patients had progressive prechiasmal visual loss possibly due to optic neu- ropathy or retinal degeneration Most patients remain stable but severely disabled and except in a few isolated cases18 do not improve with plasma- pheresis or immunosuppression With few excep- tions the anti-Yo antibody-positive PCD patient is eventually found to have an associated gynecologic cancer
Several different autoantibodies have been iden- tified in patients with PCD (table 2) In comparison with anti-Yo-positive PCD patients those without the anti-Yo antibody though pathologically simi- lar are frequently clinically distinct and make up a heterogeneous group Taken together patients without the anti-Yo antibody have an approximate- ly equal sex distribution a variety of associated malignancies (most commonly bronchial carcinoma and Hodgkinrsquos lymphoma) and more frequently present with their neurologic syndrome after the malignancy has been diagnosed Particular subsets of patients with PCD are discussed in the following two papers and e l s e ~ h e r e ~ - ~ J ~ J ~ ~ ~ ~
With the data reported here and with other recently reported cases or series of PCD it seems likely that PCD is a group of disorders each related to a particular cancer or cancers The utility of dif- ferentiating between the different anti-Purkinje cell antibodies is that when a particular antibody is present such as anti-Yo it strongly suggests the presence of an underlying neoplasm and directs the search for the occult malignancy to one or a few organs We believe that the presence of the anti-Yo antibody warran ts a n aggressive diagnostic approach that begins with careful breast and pelvic examination mammography pelvic CT and mea- surement of ovarian tumor antigen CA 125 If no malignancy is revealed with this initial workup repeat mammography pelvic examination under anesthesia and uterine D amp C should be per- formed If there is still no cancer evident surgical
1936 NEUROLOGY 42 October 1992
exploration and removal of pelvic organs may be warranted particularly in the postmenopausal woman
Unfortunately early detection and even cure of the underlying cancer does not usually affect the neurologic symptoms Although there are occasion- al reports of patients with paraneoplastic syn- dromes responding to treatment of the underlying tumor21 none of the patients in this series substan- tially improved after successful treatment of the cancer and follow-up of more than 4 years In none of the patients has there been progression of the cerebellar dysfunction after treatment of the can- cer however in most of the patients the cerebellar dysfunction had stabilized by the time the cancer diagnosis was made and treatment instituted Interestingly the anti-Yo antibody has persisted in all the patients we have followed after what is assumed to be successful treatment of the cancer In two patients in remission for more than 4 years the antibody persists in the serum although there has been no progression of their cerebellar dysfunc- tion or evidence of recurrent tumor Thus the major importance of identification of the anti-Yo antibody is that early diagnosis leads to treatment and at times cure of the cancer Identification of the antibody does not appear to be helpful in ame- liorating the neurologic disease
The pathogenesis of anti-Yo-positive PCD is unknown The high titer of antibody suggests an autoimmune mechanism but there are no reports of successful attempts to reproduce the disease in experimental animals A recent report of intrathe- cal injection of anti-Yo antibodies into experimen- tal animals was apparently successful in getting the antibody to the Purkinje cells but not in caus- ing neurologic dy~funct ion~~ Furthermore autopsy studies indicate that in most patients there is no inflammation around the degenerated Purkinje cells Thus there is no direct evidence for either a humoral- o r cell-mediated immune reaction in patients with anti-Yo-positive PCD Further work will be necessary to establish the pathogenesis of the disorder
References 1
2
3
4
5
6
Brain WR Daniel PM Greenfield JG Subacute cortical cerebellar degeneration and its relation t o carcinoma J Neurol Neurosurg Psychiatry 19511459-75 Brain WR Wilkinson M Subacute cerebellar degeneration associated with neoplasms Brain 196588465-478 Henson RA Urich H eds Cancer and the nervous system the neurological manifestations of systemic disease Oxford UK Blackwell Scientific 1982346-367 Hammack JE Posner JB Paraneoplastic cerebellar degen- eration In Plaitakis A ed Cerebellar degenerations clini- cal neurobiology Boston Kluwer Academic 1992 Anderson NE Rosenblum MK Graus F Wiley RG Posner JB Autoantibodies in paraneoplastic syndromes associated with small-cell lung cancer Neurology 1988381391-1398 Dalmau J Graus F Rosenblum MK Posner JB Anti-Hu associated paraneoplastic encephalomyelitissensory neu- ronopathy a clinical s tudy of 7 1 pa t ien ts Medicine 19927159-72
7 Anderson NE Rosenblum MK Posner JB Paraneoplastic cerebellar degeneration clinical-immunological correlations Ann Neurol 198824559-567
8 Jaeckle KA Graus F Houghton A Cardon-Cardo C Nielsen SL Posner JB Autoimmune response of patients with para- neoplastic cerebellar degeneration t o a Purkinje cell cyto- plasmic protein antigen Ann Neurol 198518592-600
9 Cunningham J Graus F Anderson N Posner JB Partial characterization of the Purkinje cell antigens in paraneo- plastic cerebellar degeneration Neurology 1986361163- 1168
10 Dropcho EJ Chen Y Posner JB Old LJ Cloning of a brain protein identified by autoantibodies from a patient with paraneoplastic cerebellar degeneration Proc Natl Acad Sci
11 Furneaux HM Dropcho E J Barbut D e t al Characterization of a cDNA encoding a 34-kDa Purkinje neuron protein recognized by sera from patients with para- neoplastic cerebellar degeneration Proc Natl Acad Sci USA
12 Furneaux HM Rosenblum MK Dalmau J Wong E Woodruff P Posner JB Selective expression of Purkinje cell antigens in tumor tissue derived from patients with parane- oplastic cerebellar degenerat ion N Engl J Med
13 Chen Y Rettig WJ Yenamandra AK e t a] Cerebellar degeneration-related (CDR) antigen a highly conserved neu- roectodermal marker mapped to chromosome X in human and mouse Proc Natl Acad Sci USA 1990873077-3081
14 Fathallah-Shaykh H Wolf S Wong E Posner JB Furneaux HM Cloning of a leucine zipper protein recognized by the sera of patients with antibody-associated paraneoplastic cerebellar degenerat ion Proc N a t l Acad Sci USA
15 Anderson NE Posner JB Sidtis J J e t al The metabolic anatomy of paraneoplastic cerebellar degeneration Ann Neurol 198823533-540
16 Gram F Abos J Roquer J Mazzara R Pereira A Effect of plasmapheresis on serum and CSF autoantibody levels in CNS paraneoplastic syndromes Neurology 1990401621- 1623
17 Hammack J E Kimmel DW OrsquoNeill BP Lennon VA Paraneoplastic cerebellar degeneration a clinical compari- son of patients with and without Purkinje cell cytoplasmic antibodies Mayo Clin Proc 1990651423-1431
18 Cocconi G Ceci G Jinvarra G et al Successful treatment of subacute cerebellar degeneration in ovarian carcinoma with plasmapheresis a case report Cancer 1985562318-2320
19 Stefansson K Ante1 JP Wollman RL Levin KH Larson R Arnason BGW Anti-neuronal antibodies in serum of a pat ient with Hodgkinrsquos disease and cerebellar a taxia [abstract] Neurology 198131(No 4 Pt 2)126
USA 1987844552-4556
1989862873-2877
19903221844-1851
1991883451-3454
20 Trotter JL Hendin BA Osterland CK Cerebellar degenera- tion with Hodgkinrsquos disease an immunological study Arch Neurol 197633660-661
21 Kearsley JH Johnson P Halmagyi GM Paraneoplastic cerebellar disease remission with excision of the primary tumor Arch Neurol 1985421208-1210
22 Brown RH J r Ronthal M Come S et al Antibodies t o 85000 dalton protein in paracarcinomatous cerebellar degeneration [abstract] Neurology 198535(suppl 1)288
23 Kornguth S Kalinke T Grunwald G Brooks B Zimmerman E Anti-neurofilament antibodies associated with paraneo- plastic syndromes [abstract] Fed Proc 198544966
24 Rodriguez M Truh LI OrsquoNeill BP Lennon VA Autoimmune paraneoplastic cerebellar degeneration ultrastructural localization of antibody-binding sites in Purkinje cells Neurology 1988381380-1386
25 Tanaka K Yamazaki M Sat0 S Toyoshima I Yamamoto A Miyatake T Antibodies to brain proteins in paraneoplastic cerebellar degeneration Neurology 1986361169-1172
26 Greenlee J E Brashear HR Antibodies to cerebellar Purkinje cells in patients with paraneoplastic cerebellar degenerat ion a n d ovarian carcinoma Ann Neurol
27 Greenlee J E Brashear HR Jaeckle KA Stroop WG Anticerebellar antibodies in sera of patients with paraneo- plastic cerebellar degeneration studies of antibody specifici- ty and response to plasmapheresis [abstract] Ann Neurol 198620 139
28 Greenlee JE Lipton HL Anticerebellar antibodies in serum and cerebrospinal fluid of a patient with oat cell carcinoma of the lung and paraneoplastic cerebellar degeneration Ann Neurol 19861982-85
29 Bourdette DN Nilaver G Cerebellar degeneration associat- ed with anti-Purkinje cell antibodies and benign IgG mono- clonal gammopathies [abstract] Neurology 198737(suppl 1)291
30 Royal W 111 Galasko DR McKhann GM Cunningham JM Dropcho EJ Clinical course immunologic and biochemical features of a patient with paraneoplastic cerebellar dysfunc- tion [abstract] Neurology 198737(suppl 1)305-306
31 Anderson NE Budde-Steffen C Wiley RG et al A variant of the anti-Purkinje cell antibody in a patient with paraneo- plastic cerebellar degeneration Neurology 1988381018- 1026
32 Tsukamoto T Yamamoto H Iwasaki Y Yoshie 0 Terunuma H Suzuki H Antineural autoantibodies in patients with paraneoplastic cerebellar degeneration Arch Neurol
33 Gram F Illa I Agusti M Ribalta T Cruz-Sanchez F Juarez C Effect of intraventricular injection of an anti-Purkinje cell antibody (anti-Yo) in a guinea pig model J Neurol Sci
198314609-613
1989461225-1229
199110682-87
October 1992 NEUROLOGY 42 1937
DOI 101212WNL421019311992421931 Neurology
K Peterson MD M K Rosenblum H Kotanides MS et al positive patientsminus
Yo antibodyminusParaneoplastic cerebellar degeneration IA clinical analysis of 55 anti
This information is current as of October 1 1992
ServicesUpdated Information amp
httpnneurologyorgcontent42101931fullhtmlincluding high resolution figures can be found at
Citations httpnneurologyorgcontent42101931fullhtmlotherarticles
This article has been cited by 20 HighWire-hosted articles
Permissions amp Licensing
httpnneurologyorgmiscaboutxhtmlpermissionsor in its entirety can be found online atInformation about reproducing this article in parts (figurestables)
Reprints
httpnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Inc All rights reserved Print ISSN 0028-3878 Online ISSN 1526-632Xsince 1951 it is now a weekly with 48 issues per year Copyright copy 1992 by Edgell Communications
reg is the official journal of the American Academy of Neurology Published continuouslyNeurology

Discussion This report confirms and extends findings previously reported on 18 patients from this laboratory7 and in a similar survey of 32 PCD patients published recently from the Mayo Clinic In the Mayo series 16 antibody-positive patients were identified17 From these reports emerges a rather stereotypic picture of the anti-Yo antibody- positive PCD patient Always female and usually not previously known to have cancer she develops over a matter of weeks a severe pancerebellar dis- order with t runcal and appendicular a taxia dysarthria and nystagmus often with a downbeat- ing component The clinical findings stabilize with- in a couple of months leaving most patients unable to walk without the assistance of one or two people unable to write legibly frequently unable to read or watch television because of oscillopsia or diplopia and having difficulty in being understood when speaking The behavioral and long-tract signs when present are usually mild and opsoclonus and myoclonus are not characteristic features Interestingly two of our patients had progressive prechiasmal visual loss possibly due to optic neu- ropathy or retinal degeneration Most patients remain stable but severely disabled and except in a few isolated cases18 do not improve with plasma- pheresis or immunosuppression With few excep- tions the anti-Yo antibody-positive PCD patient is eventually found to have an associated gynecologic cancer
Several different autoantibodies have been iden- tified in patients with PCD (table 2) In comparison with anti-Yo-positive PCD patients those without the anti-Yo antibody though pathologically simi- lar are frequently clinically distinct and make up a heterogeneous group Taken together patients without the anti-Yo antibody have an approximate- ly equal sex distribution a variety of associated malignancies (most commonly bronchial carcinoma and Hodgkinrsquos lymphoma) and more frequently present with their neurologic syndrome after the malignancy has been diagnosed Particular subsets of patients with PCD are discussed in the following two papers and e l s e ~ h e r e ~ - ~ J ~ J ~ ~ ~ ~
With the data reported here and with other recently reported cases or series of PCD it seems likely that PCD is a group of disorders each related to a particular cancer or cancers The utility of dif- ferentiating between the different anti-Purkinje cell antibodies is that when a particular antibody is present such as anti-Yo it strongly suggests the presence of an underlying neoplasm and directs the search for the occult malignancy to one or a few organs We believe that the presence of the anti-Yo antibody warran ts a n aggressive diagnostic approach that begins with careful breast and pelvic examination mammography pelvic CT and mea- surement of ovarian tumor antigen CA 125 If no malignancy is revealed with this initial workup repeat mammography pelvic examination under anesthesia and uterine D amp C should be per- formed If there is still no cancer evident surgical
1936 NEUROLOGY 42 October 1992
exploration and removal of pelvic organs may be warranted particularly in the postmenopausal woman
Unfortunately early detection and even cure of the underlying cancer does not usually affect the neurologic symptoms Although there are occasion- al reports of patients with paraneoplastic syn- dromes responding to treatment of the underlying tumor21 none of the patients in this series substan- tially improved after successful treatment of the cancer and follow-up of more than 4 years In none of the patients has there been progression of the cerebellar dysfunction after treatment of the can- cer however in most of the patients the cerebellar dysfunction had stabilized by the time the cancer diagnosis was made and treatment instituted Interestingly the anti-Yo antibody has persisted in all the patients we have followed after what is assumed to be successful treatment of the cancer In two patients in remission for more than 4 years the antibody persists in the serum although there has been no progression of their cerebellar dysfunc- tion or evidence of recurrent tumor Thus the major importance of identification of the anti-Yo antibody is that early diagnosis leads to treatment and at times cure of the cancer Identification of the antibody does not appear to be helpful in ame- liorating the neurologic disease
The pathogenesis of anti-Yo-positive PCD is unknown The high titer of antibody suggests an autoimmune mechanism but there are no reports of successful attempts to reproduce the disease in experimental animals A recent report of intrathe- cal injection of anti-Yo antibodies into experimen- tal animals was apparently successful in getting the antibody to the Purkinje cells but not in caus- ing neurologic dy~funct ion~~ Furthermore autopsy studies indicate that in most patients there is no inflammation around the degenerated Purkinje cells Thus there is no direct evidence for either a humoral- o r cell-mediated immune reaction in patients with anti-Yo-positive PCD Further work will be necessary to establish the pathogenesis of the disorder
References 1
2
3
4
5
6
Brain WR Daniel PM Greenfield JG Subacute cortical cerebellar degeneration and its relation t o carcinoma J Neurol Neurosurg Psychiatry 19511459-75 Brain WR Wilkinson M Subacute cerebellar degeneration associated with neoplasms Brain 196588465-478 Henson RA Urich H eds Cancer and the nervous system the neurological manifestations of systemic disease Oxford UK Blackwell Scientific 1982346-367 Hammack JE Posner JB Paraneoplastic cerebellar degen- eration In Plaitakis A ed Cerebellar degenerations clini- cal neurobiology Boston Kluwer Academic 1992 Anderson NE Rosenblum MK Graus F Wiley RG Posner JB Autoantibodies in paraneoplastic syndromes associated with small-cell lung cancer Neurology 1988381391-1398 Dalmau J Graus F Rosenblum MK Posner JB Anti-Hu associated paraneoplastic encephalomyelitissensory neu- ronopathy a clinical s tudy of 7 1 pa t ien ts Medicine 19927159-72
7 Anderson NE Rosenblum MK Posner JB Paraneoplastic cerebellar degeneration clinical-immunological correlations Ann Neurol 198824559-567
8 Jaeckle KA Graus F Houghton A Cardon-Cardo C Nielsen SL Posner JB Autoimmune response of patients with para- neoplastic cerebellar degeneration t o a Purkinje cell cyto- plasmic protein antigen Ann Neurol 198518592-600
9 Cunningham J Graus F Anderson N Posner JB Partial characterization of the Purkinje cell antigens in paraneo- plastic cerebellar degeneration Neurology 1986361163- 1168
10 Dropcho EJ Chen Y Posner JB Old LJ Cloning of a brain protein identified by autoantibodies from a patient with paraneoplastic cerebellar degeneration Proc Natl Acad Sci
11 Furneaux HM Dropcho E J Barbut D e t al Characterization of a cDNA encoding a 34-kDa Purkinje neuron protein recognized by sera from patients with para- neoplastic cerebellar degeneration Proc Natl Acad Sci USA
12 Furneaux HM Rosenblum MK Dalmau J Wong E Woodruff P Posner JB Selective expression of Purkinje cell antigens in tumor tissue derived from patients with parane- oplastic cerebellar degenerat ion N Engl J Med
13 Chen Y Rettig WJ Yenamandra AK e t a] Cerebellar degeneration-related (CDR) antigen a highly conserved neu- roectodermal marker mapped to chromosome X in human and mouse Proc Natl Acad Sci USA 1990873077-3081
14 Fathallah-Shaykh H Wolf S Wong E Posner JB Furneaux HM Cloning of a leucine zipper protein recognized by the sera of patients with antibody-associated paraneoplastic cerebellar degenerat ion Proc N a t l Acad Sci USA
15 Anderson NE Posner JB Sidtis J J e t al The metabolic anatomy of paraneoplastic cerebellar degeneration Ann Neurol 198823533-540
16 Gram F Abos J Roquer J Mazzara R Pereira A Effect of plasmapheresis on serum and CSF autoantibody levels in CNS paraneoplastic syndromes Neurology 1990401621- 1623
17 Hammack J E Kimmel DW OrsquoNeill BP Lennon VA Paraneoplastic cerebellar degeneration a clinical compari- son of patients with and without Purkinje cell cytoplasmic antibodies Mayo Clin Proc 1990651423-1431
18 Cocconi G Ceci G Jinvarra G et al Successful treatment of subacute cerebellar degeneration in ovarian carcinoma with plasmapheresis a case report Cancer 1985562318-2320
19 Stefansson K Ante1 JP Wollman RL Levin KH Larson R Arnason BGW Anti-neuronal antibodies in serum of a pat ient with Hodgkinrsquos disease and cerebellar a taxia [abstract] Neurology 198131(No 4 Pt 2)126
USA 1987844552-4556
1989862873-2877
19903221844-1851
1991883451-3454
20 Trotter JL Hendin BA Osterland CK Cerebellar degenera- tion with Hodgkinrsquos disease an immunological study Arch Neurol 197633660-661
21 Kearsley JH Johnson P Halmagyi GM Paraneoplastic cerebellar disease remission with excision of the primary tumor Arch Neurol 1985421208-1210
22 Brown RH J r Ronthal M Come S et al Antibodies t o 85000 dalton protein in paracarcinomatous cerebellar degeneration [abstract] Neurology 198535(suppl 1)288
23 Kornguth S Kalinke T Grunwald G Brooks B Zimmerman E Anti-neurofilament antibodies associated with paraneo- plastic syndromes [abstract] Fed Proc 198544966
24 Rodriguez M Truh LI OrsquoNeill BP Lennon VA Autoimmune paraneoplastic cerebellar degeneration ultrastructural localization of antibody-binding sites in Purkinje cells Neurology 1988381380-1386
25 Tanaka K Yamazaki M Sat0 S Toyoshima I Yamamoto A Miyatake T Antibodies to brain proteins in paraneoplastic cerebellar degeneration Neurology 1986361169-1172
26 Greenlee J E Brashear HR Antibodies to cerebellar Purkinje cells in patients with paraneoplastic cerebellar degenerat ion a n d ovarian carcinoma Ann Neurol
27 Greenlee J E Brashear HR Jaeckle KA Stroop WG Anticerebellar antibodies in sera of patients with paraneo- plastic cerebellar degeneration studies of antibody specifici- ty and response to plasmapheresis [abstract] Ann Neurol 198620 139
28 Greenlee JE Lipton HL Anticerebellar antibodies in serum and cerebrospinal fluid of a patient with oat cell carcinoma of the lung and paraneoplastic cerebellar degeneration Ann Neurol 19861982-85
29 Bourdette DN Nilaver G Cerebellar degeneration associat- ed with anti-Purkinje cell antibodies and benign IgG mono- clonal gammopathies [abstract] Neurology 198737(suppl 1)291
30 Royal W 111 Galasko DR McKhann GM Cunningham JM Dropcho EJ Clinical course immunologic and biochemical features of a patient with paraneoplastic cerebellar dysfunc- tion [abstract] Neurology 198737(suppl 1)305-306
31 Anderson NE Budde-Steffen C Wiley RG et al A variant of the anti-Purkinje cell antibody in a patient with paraneo- plastic cerebellar degeneration Neurology 1988381018- 1026
32 Tsukamoto T Yamamoto H Iwasaki Y Yoshie 0 Terunuma H Suzuki H Antineural autoantibodies in patients with paraneoplastic cerebellar degeneration Arch Neurol
33 Gram F Illa I Agusti M Ribalta T Cruz-Sanchez F Juarez C Effect of intraventricular injection of an anti-Purkinje cell antibody (anti-Yo) in a guinea pig model J Neurol Sci
198314609-613
1989461225-1229
199110682-87
October 1992 NEUROLOGY 42 1937
DOI 101212WNL421019311992421931 Neurology
K Peterson MD M K Rosenblum H Kotanides MS et al positive patientsminus
Yo antibodyminusParaneoplastic cerebellar degeneration IA clinical analysis of 55 anti
This information is current as of October 1 1992
ServicesUpdated Information amp
httpnneurologyorgcontent42101931fullhtmlincluding high resolution figures can be found at
Citations httpnneurologyorgcontent42101931fullhtmlotherarticles
This article has been cited by 20 HighWire-hosted articles
Permissions amp Licensing
httpnneurologyorgmiscaboutxhtmlpermissionsor in its entirety can be found online atInformation about reproducing this article in parts (figurestables)
Reprints
httpnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Inc All rights reserved Print ISSN 0028-3878 Online ISSN 1526-632Xsince 1951 it is now a weekly with 48 issues per year Copyright copy 1992 by Edgell Communications
reg is the official journal of the American Academy of Neurology Published continuouslyNeurology

7 Anderson NE Rosenblum MK Posner JB Paraneoplastic cerebellar degeneration clinical-immunological correlations Ann Neurol 198824559-567
8 Jaeckle KA Graus F Houghton A Cardon-Cardo C Nielsen SL Posner JB Autoimmune response of patients with para- neoplastic cerebellar degeneration t o a Purkinje cell cyto- plasmic protein antigen Ann Neurol 198518592-600
9 Cunningham J Graus F Anderson N Posner JB Partial characterization of the Purkinje cell antigens in paraneo- plastic cerebellar degeneration Neurology 1986361163- 1168
10 Dropcho EJ Chen Y Posner JB Old LJ Cloning of a brain protein identified by autoantibodies from a patient with paraneoplastic cerebellar degeneration Proc Natl Acad Sci
11 Furneaux HM Dropcho E J Barbut D e t al Characterization of a cDNA encoding a 34-kDa Purkinje neuron protein recognized by sera from patients with para- neoplastic cerebellar degeneration Proc Natl Acad Sci USA
12 Furneaux HM Rosenblum MK Dalmau J Wong E Woodruff P Posner JB Selective expression of Purkinje cell antigens in tumor tissue derived from patients with parane- oplastic cerebellar degenerat ion N Engl J Med
13 Chen Y Rettig WJ Yenamandra AK e t a] Cerebellar degeneration-related (CDR) antigen a highly conserved neu- roectodermal marker mapped to chromosome X in human and mouse Proc Natl Acad Sci USA 1990873077-3081
14 Fathallah-Shaykh H Wolf S Wong E Posner JB Furneaux HM Cloning of a leucine zipper protein recognized by the sera of patients with antibody-associated paraneoplastic cerebellar degenerat ion Proc N a t l Acad Sci USA
15 Anderson NE Posner JB Sidtis J J e t al The metabolic anatomy of paraneoplastic cerebellar degeneration Ann Neurol 198823533-540
16 Gram F Abos J Roquer J Mazzara R Pereira A Effect of plasmapheresis on serum and CSF autoantibody levels in CNS paraneoplastic syndromes Neurology 1990401621- 1623
17 Hammack J E Kimmel DW OrsquoNeill BP Lennon VA Paraneoplastic cerebellar degeneration a clinical compari- son of patients with and without Purkinje cell cytoplasmic antibodies Mayo Clin Proc 1990651423-1431
18 Cocconi G Ceci G Jinvarra G et al Successful treatment of subacute cerebellar degeneration in ovarian carcinoma with plasmapheresis a case report Cancer 1985562318-2320
19 Stefansson K Ante1 JP Wollman RL Levin KH Larson R Arnason BGW Anti-neuronal antibodies in serum of a pat ient with Hodgkinrsquos disease and cerebellar a taxia [abstract] Neurology 198131(No 4 Pt 2)126
USA 1987844552-4556
1989862873-2877
19903221844-1851
1991883451-3454
20 Trotter JL Hendin BA Osterland CK Cerebellar degenera- tion with Hodgkinrsquos disease an immunological study Arch Neurol 197633660-661
21 Kearsley JH Johnson P Halmagyi GM Paraneoplastic cerebellar disease remission with excision of the primary tumor Arch Neurol 1985421208-1210
22 Brown RH J r Ronthal M Come S et al Antibodies t o 85000 dalton protein in paracarcinomatous cerebellar degeneration [abstract] Neurology 198535(suppl 1)288
23 Kornguth S Kalinke T Grunwald G Brooks B Zimmerman E Anti-neurofilament antibodies associated with paraneo- plastic syndromes [abstract] Fed Proc 198544966
24 Rodriguez M Truh LI OrsquoNeill BP Lennon VA Autoimmune paraneoplastic cerebellar degeneration ultrastructural localization of antibody-binding sites in Purkinje cells Neurology 1988381380-1386
25 Tanaka K Yamazaki M Sat0 S Toyoshima I Yamamoto A Miyatake T Antibodies to brain proteins in paraneoplastic cerebellar degeneration Neurology 1986361169-1172
26 Greenlee J E Brashear HR Antibodies to cerebellar Purkinje cells in patients with paraneoplastic cerebellar degenerat ion a n d ovarian carcinoma Ann Neurol
27 Greenlee J E Brashear HR Jaeckle KA Stroop WG Anticerebellar antibodies in sera of patients with paraneo- plastic cerebellar degeneration studies of antibody specifici- ty and response to plasmapheresis [abstract] Ann Neurol 198620 139
28 Greenlee JE Lipton HL Anticerebellar antibodies in serum and cerebrospinal fluid of a patient with oat cell carcinoma of the lung and paraneoplastic cerebellar degeneration Ann Neurol 19861982-85
29 Bourdette DN Nilaver G Cerebellar degeneration associat- ed with anti-Purkinje cell antibodies and benign IgG mono- clonal gammopathies [abstract] Neurology 198737(suppl 1)291
30 Royal W 111 Galasko DR McKhann GM Cunningham JM Dropcho EJ Clinical course immunologic and biochemical features of a patient with paraneoplastic cerebellar dysfunc- tion [abstract] Neurology 198737(suppl 1)305-306
31 Anderson NE Budde-Steffen C Wiley RG et al A variant of the anti-Purkinje cell antibody in a patient with paraneo- plastic cerebellar degeneration Neurology 1988381018- 1026
32 Tsukamoto T Yamamoto H Iwasaki Y Yoshie 0 Terunuma H Suzuki H Antineural autoantibodies in patients with paraneoplastic cerebellar degeneration Arch Neurol
33 Gram F Illa I Agusti M Ribalta T Cruz-Sanchez F Juarez C Effect of intraventricular injection of an anti-Purkinje cell antibody (anti-Yo) in a guinea pig model J Neurol Sci
198314609-613
1989461225-1229
199110682-87
October 1992 NEUROLOGY 42 1937
DOI 101212WNL421019311992421931 Neurology
K Peterson MD M K Rosenblum H Kotanides MS et al positive patientsminus
Yo antibodyminusParaneoplastic cerebellar degeneration IA clinical analysis of 55 anti
This information is current as of October 1 1992
ServicesUpdated Information amp
httpnneurologyorgcontent42101931fullhtmlincluding high resolution figures can be found at
Citations httpnneurologyorgcontent42101931fullhtmlotherarticles
This article has been cited by 20 HighWire-hosted articles
Permissions amp Licensing
httpnneurologyorgmiscaboutxhtmlpermissionsor in its entirety can be found online atInformation about reproducing this article in parts (figurestables)
Reprints
httpnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Inc All rights reserved Print ISSN 0028-3878 Online ISSN 1526-632Xsince 1951 it is now a weekly with 48 issues per year Copyright copy 1992 by Edgell Communications
reg is the official journal of the American Academy of Neurology Published continuouslyNeurology

DOI 101212WNL421019311992421931 Neurology
K Peterson MD M K Rosenblum H Kotanides MS et al positive patientsminus
Yo antibodyminusParaneoplastic cerebellar degeneration IA clinical analysis of 55 anti
This information is current as of October 1 1992
ServicesUpdated Information amp
httpnneurologyorgcontent42101931fullhtmlincluding high resolution figures can be found at
Citations httpnneurologyorgcontent42101931fullhtmlotherarticles
This article has been cited by 20 HighWire-hosted articles
Permissions amp Licensing
httpnneurologyorgmiscaboutxhtmlpermissionsor in its entirety can be found online atInformation about reproducing this article in parts (figurestables)
Reprints
httpnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Inc All rights reserved Print ISSN 0028-3878 Online ISSN 1526-632Xsince 1951 it is now a weekly with 48 issues per year Copyright copy 1992 by Edgell Communications
reg is the official journal of the American Academy of Neurology Published continuouslyNeurology








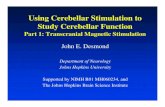



![[症例報告]A Case of Paraneoplastic Cerebellar Degeneration ...okinawa-repo.lib.u-ryukyu.ac.jp/bitstream/20.500.12001/...Ryukyu Med. J., 14(3)209-211, 1994 209 A Case of Paraneoplastic](https://static.fdocuments.net/doc/165x107/608abfa5228b9f68d263e46f/ca-case-of-paraneoplastic-cerebellar-degeneration-okinawa-repolibu-.jpg)





