Paradoxes of Health Transition Albania 1950-90
26
Paradoxes of Health Transition in Europe's Poorest Country: Albania 1950-90 Author(s): Arjan Gjonca, Chris Wilson and Jane Falkingham Source: Population and Development Review, Vol. 23, No. 3 (Sep., 1997), pp. 585-609 Published by: Population Council Stable URL: http://www.jstor.org/stable/2137576 . Accessed: 23/07/2014 14:13 Your use of the JSTOR archive indicates your acceptance of the Terms & Conditions of Use, available at . http://www.jstor.org/page/info/about/policies/terms.jsp . JSTOR is a not-for-profit service that helps scholars, researchers, and students discover, use, and build upon a wide range of content in a trusted digital archive. We use information technology and tools to increase productivity and facilitate new forms of scholarship. For more information about JSTOR, please contact [email protected]. . Population Council is collaborating with JSTOR to digitize, preserve and extend access to Population and Development Review. http://www.jstor.org This content downloaded from 151.100.102.94 on Wed, 23 Jul 2014 14:13:45 PM All use subject to JSTOR Terms and Conditions
-
Upload
dritan-mico -
Category
Documents
-
view
14 -
download
1
description
Arjan Gjonca, Chris Wilson and Jane Falkingham
Transcript of Paradoxes of Health Transition Albania 1950-90

Paradoxes of Health Transition in Europe's Poorest Country: Albania 1950-90Author(s): Arjan Gjonca, Chris Wilson and Jane FalkinghamSource: Population and Development Review, Vol. 23, No. 3 (Sep., 1997), pp. 585-609Published by: Population CouncilStable URL: http://www.jstor.org/stable/2137576 .
Accessed: 23/07/2014 14:13
Your use of the JSTOR archive indicates your acceptance of the Terms & Conditions of Use, available at .http://www.jstor.org/page/info/about/policies/terms.jsp
.JSTOR is a not-for-profit service that helps scholars, researchers, and students discover, use, and build upon a wide range ofcontent in a trusted digital archive. We use information technology and tools to increase productivity and facilitate new formsof scholarship. For more information about JSTOR, please contact [email protected].
.
Population Council is collaborating with JSTOR to digitize, preserve and extend access to Population andDevelopment Review.
http://www.jstor.org
This content downloaded from 151.100.102.94 on Wed, 23 Jul 2014 14:13:45 PMAll use subject to JSTOR Terms and Conditions

DATA AND PERSPECTIVES
Paradoxes of Health Transition in Europe's Poorest Country: Albania 1950-90
ARJAN GJONrA CHRIS WILSON JANE FALKINGHA-M
IN RECENT YEARS scholars interested in the ways in which good health, as indicated by low mortality, can be provided at low cost have paid consid- erable attention to countries and regions in Asia and Latin America where this has been achieved. China, Cuba, Sri Lanka, and the Indian state of Kerala have often been cited in this regard (Caldwell 1986; Halstead, Walsh, and Warren 1985). Until recently the similar experience of a poor devel- oping country in Southeast Europe, Albania, has been impossible to study. For decades the country was virtually cut off from the outside world, hav- ing only limited links with some other communist countries. Thus com- prehensive reviews of European health and mortality trends, such as those by Okolski (1994) and Caselli (1996), present almost no results for Albania in their otherwise exhaustive tabulations. Following the collapse of the commu- nist dictatorship in 1990, however, detailed information on the trends and determinants of Albania's mortality transition have become available. These data provide insights into both the extent of Albania's achievements in reduc- ing mortality since 1950 and the limits to that reduction. The present study considers the socioeconomic and political background to health transition in Albania, charts the main trends in mortality, examines the proximate causes of the mortality decline, and considers the wider significance of the results.
POPULATION AND DEVELOPMENT REVIEW 23(3):585-609 (SEPTEMBER 1997) 585
This content downloaded from 151.100.102.94 on Wed, 23 Jul 2014 14:13:45 PMAll use subject to JSTOR Terms and Conditions

586 HEALTH TRANSITION IN ALBANIA
Political and economic background
Albania has long remained a closed book, even to most other Europeans. From the fifteenth century until independence in 1912, Albania's isolation from Western Europe persisted because the country was under the control of the Ottoman Empire. After little more than three decades of increased contact with Western Europe (including several years under military oc- cupation by the Axis powers during World War II), Albania again found itself outside the West's sphere of influence. In October 1944 the Commu- nist Party of Albania under Enver Hoxha seized power and imposed re- pressive political control and a set of isolationist policies that became in- creasingly severe over time. All political dissent was ruthlessly suppressed and an autarkic policy of "self-reliance' was adopted. As Logoreci (1977: 201) put it, Albanians came to feel as if "they lived on an island off Europe which for centuries had been surrounded by a world that was either hos- tile or merely indifferent to their interests and general welfare." To out- siders, Albania's isolation meant that it remained for decades both a for- gotten and a forbidden place. For a small country (about the size of Wales or the state of Maryland) with an estimated 1.23 million people in 1950, and 3.38 million in 1995, the costs of this politically imposed self-reli- ance were great.
The history of communist Albania was punctuated by successive and disruptive rifts with the country's main political allies and economic sup- porters. Immediately following World War II Albania had strong links with Yugoslavia, but these were severed when the latter asserted its indepen- dence from Moscow in 1948. During the 1950s Albania had close ties to the Soviet Union and some of its European allies, and benefited substan- tially from Soviet economic aid, especially in the form of expert advice and technical assistance. Following the split between the Soviet Union and China in the late 1950s, Albania cut off all dealings with Moscow in 1961 and came to be dependent on China for similar assistance. This link, too, was ultimately broken in the late 1970s, so that by the time the dictatorship collapsed in 1990 the country's isolation was effectively complete. The iso- lation did not arise by chance, as self-sufficiency was the primary policy goal throughout the communist period, culminating in the 1976 Constitu- tion that enshrined the virtually total isolation of the country (Logoreci 1977: 166-167). Moreover, although ostensibly committed to Marxism, the Albanian regime pursued policies that Hall (1994: xx) has characterized as "essentially a nationalism infused with regionalism and the strong self -in- terest of a small ruling group employing Marxist ideology ... as a buttress to power and a justificatory veneer."
Since 1990 the country, in common with other former communist states of Eastern Europe, has undergone massive economic and political
This content downloaded from 151.100.102.94 on Wed, 23 Jul 2014 14:13:45 PMAll use subject to JSTOR Terms and Conditions

ARJAN GJONQA / CHRIS WILSON / JANE FALKINGHAM 587
changes. After a period of economic collapse, Albania experienced rapid economic growth and increased integration into the wider European economy in the period 1993-95. This progress was once again reversed when the country was swept by a wave of financial and political crises in 1996-97. In order to place the mortality trends since 1950 in their proper context, we need to consider the effect of some of these long-term factors in more detail.
In many ways Albania from 1950 to 1990 represents an extreme ver- sion of the communist mode of development. Economic growth was lim- ited, compared with the market economies of Europe, but significant ad- vances were made on the social agenda of health care, education, and social security. Even compared with the rest of communist Eastern Europe, how- ever, Albania stands out as having a unique developmental history. For example, economic policy was more thoroughly Stalinist in its orientation than that of the Soviet Union itself. Schnytzer (1982: 2) suggests that Al- banian economic policy under communism closely followed the guidelines of Stalin's last book, Economic Problems of Socialism in the USSR, which were, in fact, never implemented in the Soviet Union. In particular, the collec- tivization of the economy was pursued more completely in Albania than elsewhere. In effect, private property was virtually abolished. One of the first laws passed by the communists after taking power, the Agrarian Land Reform, nationalized all land (Sjoberg 1991). The collectivization of agri- cultural production was also pursued with rigor, though over a longer pe- riod, so that it was not considered complete until 1967. By that time, only garden-sized plots remained available to farmers to help meet personal do- mestic requirements; over 95 percent of land was either in cooperative farms or directly under state control (Hall 1994: 121).
Moreover, collectivization was just one part of a wider process whereby the state took control of all aspects of life: education, health, and social security, as well as food supply became prerogatives of the state. Albania also manifested a particularly thorough version of Marxism in its policy on income distribution. For most of the communist period the highest income level allowed was only 2.5 times the lowest, and in the 1970s this differen- tial was reduced to less than two (Bollano 1984). A small party elite ben- efited from payments in kind and a variety of perquisites, including access to foreign-made goods and much better housing in an exclusive section of the capital, Tirana. However, they represented a tiny fraction of the popu- lation and were thus of no demographic significance. The economic power of the state was matched by its total control of political life. Dissent of any kind was forbidden, and all competing sources of legitimacy, such as orga- nized religion, were suppressed. Even compared with other European com- munist regimes, the oppression endured by the Albanian people under Hoxha was remarkable for its severity (Frey et al. 1990: iii-vi).
This content downloaded from 151.100.102.94 on Wed, 23 Jul 2014 14:13:45 PMAll use subject to JSTOR Terms and Conditions

588 HEALTH TRANSITION IN ALBANIA
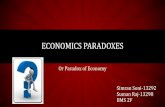
Albania remained predominantly rural and agricultural throughout the communist era. In the 1989 census, for example, 64 percent of the population was still classified as rural, with agriculture the dominant eco- nomic activity. Some measure of the slowness of urbanization in Albania can be seen from Figure 1, which compares the proportion rural with the same information for other former communist countries in Eastern Europe.
As might be expected with such a pace of urbanization, industry and trade grew slowly under communism. As late as 1989 over half the labor force was still in agriculture, in spite of an investment allocation that greatly favored heavy industry throughout the communist period (Hall 1994: 69). By the 1970s over 40 percent of the industrial output came from heavy industry (Schnytzer 1982: 65). Interpreting economic statistics for com- mand economies is problematic, as much incentive existed to manipulate information to fit with the demands of successive economic plans. More- over, Marxist economic concepts do not always translate readily into more conventional measures such as gross national product per head. Neverthe- less, it is clear from a careful reading of the relevant statistics that industri- alization was slow, limited, and excessively focused on producing low-qual- ity import-substituting items. Only the hydroelectric, petroleum, and
FIGURE 1 Percent of the population that is rural: Albania and other Eastem European countries, 1950-90
100
80-
lan .~~~~ni
60 Yugoslavia oai
Bulgaria 40 -
20 - Czechoslovakia
20
1950 1960 1970 1980 1990
SOURCES: United Nations, Demographic Yearbooks, 1950-92, and the Statistical Yearbooks of each country.
This content downloaded from 151.100.102.94 on Wed, 23 Jul 2014 14:13:45 PMAll use subject to JSTOR Terms and Conditions

ARJAN GJONQA / CHRIS WILSON / JANE FALKINGHAM 589
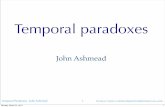
mineral extraction industries were strongly developed, and the latter two led to extensive, if localized, pollution, especially of rivers. Most of the facto- ries built in the 1950s were supported by the substantial aid Albania received from the Soviet Union during that decade. After the split with Moscow, China provided considerable economic assistance until 1978. Taken together, aid from the Soviet Union and China is estimated to have amounted to 12 percent of the 'net material product' between 1950 and 1978 (Hall 1994: 111). The economic viability of the country's industrial development is doubtful, how- ever, since after the Chinese withdrawal the lack of technical assistance resulted in a substantial decline in the industrial economy. It appears that virtually no significant investment in industry was made between 1978 and 1990, and that during these years little or no economic growth oc- curred. Figure 2 confirms this general conclusion, suggesting that between 1950 and 1976 the economy grew at an average of about 3 percent a year, with the most rapid period of expansion during the postwar reconstruc- tion. Between the mid-1970s and 1990 growth was almost nil, even be- fore the collapse of the economy that precipitated the fall of the commu- nist regime. The inherent contradictions of trying to impose a Stalinist economic system on a predominantly agrarian society are well laid out by Schnytzer (1982: 88-89).
FIGURE 2 Index of real income per capita in Albaiia, 1950-90 250
200
150
100 1950 1955 1960 1965 1970 1975 1980 1985 1990
SOURCES: General State Archive of Albania; Statistical Yearbooks of Albania.
This content downloaded from 151.100.102.94 on Wed, 23 Jul 2014 14:13:45 PMAll use subject to JSTOR Terms and Conditions

590 HEALTH TRANSITION IN ALBANIA
Conventional measures of GNP or GDP tend to understate income substantially in a subsistence economy, while purchasing-power-parity estimates (PPP) contain an element of conjecture in the absence of de- tailed price statistics. Thus estimates of Albania's GNP per head made since 1990 have varied greatly, with conventional GNP sometimes put as low as $380 per head (World Bank 1996: 172), and PPP estimates as high as $3,500 (United Nations 1995: 156). The most authoritative source on internationally comparable long-run estimates (Maddison 1995: 217) puts Albania's GDP per head in 1950, measured in 1990 dollars, at $1,007, while the 1990 figure is $2,500. While these must be viewed as approximate, some idea of the low level of development they imply is indicated by the fact that the 1950 figure is lower than most Western European countries had attained in 1820, when Maddison's survey be- gins, while the 1990 figure is comparable to values for other Southern European countries in the 1910s and 1920s.
Given the inevitable imprecision of such estimates, perhaps a more instructive assessment is one based on the extent and quality of physical infrastructure. In this respect, Albania is poor indeed compared with the rest of Europe. For example, in 1990 the country possessed only 2,850 kms (1,770 miles) of surfaced roads, a particular irony for a country that has considerable deposits of bitumen (Hall 1994: 126). Moreover, even these roads are poorly maintained. Other roads are mostly rough tracks that are frequently impassable in winter. This is especially significant given the mountainous nature of the country and the widely dispersed rural settle- ment. Thus, even today, many of the country's 3,000 villages are, in effect, cut off from other areas of the country for part of the year. Most other aspects of infrastructure were in similarly parlous condition by 1990. In spite of possessing considerable potential for hydroelectric power, electric- ity supply is irregular in most parts of the country, and water is often in short supply, especially in summer. Although such problems were exacer- bated by the collapse of effective state control in 1990 and 1991, they also reflect a poor long-run record of development. As a further indication of this, modern domestic appliances were rare and private cars unknown be- fore 1990. In sum, while it is impossible to specify the level of economic development achieved under communism, it is certain that Albania remained the poorest and least-developed economy in Europe throughout the 40 years following 1950. Its level of development, at least in terms of infrastructure and urbanization, might best be characterized as comparable to parts of North Africa or West Asia, such as Morocco or Yemen, or with the less-advanced parts of Latin America, such as Bolivia or Honduras. Most pertinently of all, perhaps, the level and nature of development in Albania is similar to that of the Central Asian republics of the former Soviet Union, whose course of development has many parallels with Albania's (World Bank 1996).
This content downloaded from 151.100.102.94 on Wed, 23 Jul 2014 14:13:45 PMAll use subject to JSTOR Terms and Conditions

ARJAN GJONQA / CHRIS WILSON / JANE FALKINGHAM 591
While the economic record of Albania's communist government was unquestionably poor, and the political repression ruthless, the irnprovements brought about in the areas of health and education were considerable.
The health care system
In common with other communist countries, the Albanian government gave high priority to improving health. In doing so they started from an extremely low base of development, as health and other social conditions, both before and after World War II, were dire. Infectious diseases, especially tuberculosis, and gastrointestinal conditions were widespread and malaria was endemic. In the 1930s up to 58 percent of children in Albanian cities were diagnosed as being infected with the malaria parasite (Hackett 1944).
In 1938, the last precommunist year for which relevant statistics ex- ist, only 102 Albanians were qualified as medical doctors and the number of physicians (including dentists) stood at 1.1 per 10,000 population. At the same time there was only one hospital bed per 1,000 people, and health expenditure amounted to one percent of the government budget. Table 1 suggests the improvements made in some of these areas. A wide-ranging social insurance and medical scheme was introduced in 1947 under which most medical treatment was free, although some medicines were still charged for. Legislation was also introduced in the late 1940s to improve maternal and child health and to improve sanitary conditions and the treat- ment of infectious diseases. By 1950, although the number of physicians had not risen, there were four times as many hospital beds per head, and health expenditures had risen to almost 5 percent of the budget.
The Albanian health care system shared several features common to most communist countries. Entitlement to care was universal, the public sector operated a monopoly of service provision and drug supply, the cen- trally planned resource allocation was largely based on inputs such as beds
TABLE 1 Basic indicators of medical and health provision in Albania, 1938-90
1938 1950 1960 1970 1980 1990
Physicians per 10,000 population 1.1 1.1 3.0 7.4 16.8 17.1
Beds per 1,000 population 1.0 4.4 5.4 4.1 6.5 5.9 Health expenditure as a percent of total public expenditure 1.0 4.9 5.9 5.3 5.3 6.6
Consultations with general practitioners per 1,000 population - 614 1,220 2,223 2,970 3,399
SOURCES: General State Archive of Albania; Statistical Yearbooks of Albania.
This content downloaded from 151.100.102.94 on Wed, 23 Jul 2014 14:13:45 PMAll use subject to JSTOR Terms and Conditions

592 HEALTH TRANSITION IN ALBANIA
or staff numbers rather than on services provided, and the centralized man- agement structure offered little incentive to improve the quality of care, increase efficiency, or control costs. In spite of these weaknesses, the ini- tial success of the system was dramatic, with a marked reduction in mor- tality during the 1950s and 1960s. By 1980, the number of physicians had grown to 16.8 per 10,000, with 6.5 hospital beds per 1,000. According to information relating to the 1980s, half of the country's physicians were nonspecialists, indicating an emphasis on primary care, and some 800 medi- cal institutions were spread around the country, with most urban centers having more than one hospital. A policy of directing resources to many of the more remote areas of the country was also followed, so that by 1971 every village was said to have a health center and more than 80 percent of medical institutions were located in villages (Hall 1994: 71). This was es- sential in order for the health care system to have a marked impact on a population that was still overwhelmingly rural.
Among the efforts to improve health care, special importance was given to maternal and infant and child health. Since the infant mortality rate in 1950 was 134 per 1,000 live births, such a focus was clearly required. Ma- ternal and child health centers were established in both urban and rural areas, and antenatal care was made widely available for the first time. Rela- tively generous maternity leave arrangements along with subsidized child- care and kindergarten facilities completed the picture. Perhaps most im- portant of all, the proportion of deliveries in hospital rose from 0.4 percent of births in 1938 (when there was only one maternity hospital in the coun- try) to 36 percent in 1960, 76 percent in 1976, and over 99 percent in 1982. Vaccination rates also reached high levels. In 1990 the proportion of children immunized with the polio, measles, and DPT vaccines exceeded 90 percent (UNICEF 1994: 104).
While the health services clearly expanded substantially, the quality of service is another matter. We have limited evidence on this point, so our conclusions are tentative. It will become clear below, however, that Albania's record on maternal and infant mortality in many respects lagged behind success at other ages, so that the quality of service in these specifi- cally targeted groups cannot have reached expectations. In many cases, hospital beds must simply have been beds in a building called a hospital, but lacking even basic equipment and drugs (Hamilton 1992). After the break with the Soviet Union and later with China, there were increasing shortages of equipment and other technical requirements. As Albania grew ever more isolated, medical personnel were cut off from global advances in technology and pharmaceuticals, while the local drug industry remained locked into outmoded lines and processes. The limited range of locally pro- duced drugs and the lack of hard currency made available for imports left medical practitioners with no option but to prescribe substandard treat-
This content downloaded from 151.100.102.94 on Wed, 23 Jul 2014 14:13:45 PMAll use subject to JSTOR Terms and Conditions

ARJAN GJONXA / CHRIS WILSON / JANE FALKINGHAM 593
ments. The dogma of self-reliance was especially dysfunctional in this re- gard. Moreover, the regime took pride in the provision of new physical infrastructure at the expense of maintenance and training. By 1989 Albania's limited and diminishing economic resources could no longer sup- port the health system, and, in the turbulent events surrounding the fall of the communist regime, much of the basic physical infrastructure was dam- aged or destroyed.
The educational system
Given the significance attached to education in most studies of the de- terminants of health transition, it is clearly important to examine Al- bania's record in this respect. Immediately upon seizing power in 1944, the communist regime gave high priority to opening schools and reor- ganizing the educational system along ideologically determined lines. As with health, the prevailing educational situation was antiquated. In 1938 there were only 20 secondary schools in the country, with a total enrollment of 5,700 students. At the end of World War II, it is estimated that more than 80 percent of adults were illiterate, 95 percent in some rural areas. Female illiteracy was nearly universal in rural areas and the norm even in the cities. The first priority of the new educational system, therefore, was to seek to eliminate illiteracy. The "struggle" against illit- eracy was based on the Educational Reform Law of 1946. This introduced the first national system of education, based on the Soviet model, with preschool up to age five, a seven-year primary school curriculum, and four years of secondary schooling. Primary school attendance was made compulsory. In 1949 the drive against illiteracy was intensified with a further law requiring illiterates between ages 12 and 40 to learn to read and write (Keefe et al. 1971: 86).
Further expansion of the school system began in 1950 with an in- crease in secondary schooling, again along Soviet lines. Various techni- cal and professional secondary schools were established, including in- stitutions aimed at preparatory studies for medicine, finance, commerce, agriculture, and the petroleum industry. By 1956 illiteracy was deemed to have been eliminated, and a steady expansion of secondary and higher-level educational facilities took place through the 1960s and 1970s. Logoreci (1977: 69), in most respects a severe critic of the com- munist regime, acknowledged that "Albania's single most impressive post-war achievement was the expansion of its educational facilities." Moreover, in a traditionally patriarchal and strongly male-dominated society, the provision of equal educational access to boys and girls must have been a revolutionary change. Even so, the country's success in increasing enrollments was not matched by the quality of its educational
This content downloaded from 151.100.102.94 on Wed, 23 Jul 2014 14:13:45 PMAll use subject to JSTOR Terms and Conditions

594 HEALTH TRANSITION IN ALBANIA
provision. As was the case with the health care system, the quality of service provision left much to be desired. In addition to the large ele- ment of compulsory ideological study, often little more than brainwash- ing, schools suffered from overcrowding and a dearth of materials and books. Here, too, self-reliance proved to be an unfortunate strategy, cut- ting Albania off from the rest of the world. Specialist and up-to-date literature was lacking in most fields of education, while strict censor- ship and the lack of personal freedom exacerbated the situation.
Demographic data
Until 1990 almost all statistical information on Albania was deemed to be a state secret, and any attempt to acquire it was tantamount to espionage. As Sjoberg (1991: 9) writes, 'it is difficult to conceive of a European nation where conditions are as unfavourable with respect to access to data. This does not necessarily mean, however, that Albanian statistics are useless.' In fact, surprising amounts of demographic, economic, and social statistics were provided to the central government, but were not published. The first comprehensive Statistical Yearbook of Albania, published in 1991, included a variety of historical time-series (Institute of Statistics 1991). What is more, scholars are now able to examine data from a number of previously secret archives. This study, for example, is based on data provided from the archive of the Statistical Institute and the General State Archive, especially the de- pository of the State Planning Commission. With these sources it has be- come feasible to reconstruct Albania's demographic history since 1950 with some certainty. The data have certain weaknesses and at times need care- ful interpretation, but, taken together, they provide a consistent and sur- prisingly comprehensive basis for study.
Censuses were carried out in 1950, 1955, 1960, 1969, 1979, and 1989. Although the earliest data show some age heaping, it is not severe and is restricted mostly to males over age 50 and females over 30. Interestingly, because the 1950 census was also used as a means to specify ages on iden- tity cards, the dates of birth specified in that year became fixed. Thus, any heaping present in these older cohorts in 1950 follows them through suc- cessive censuses. The existence of this date-of-birth heaping becomes ap- parent when considering the 1969 census. The gap between the census dates of 1960 and 1969 was eight and a half years, and heaping in the latter census moved from ages ending in 0 and 5 to those ending in 3 and 8. Such problems, however, are minor and easily dealt with. Overall, the census provides a good basis for demographic analysis.
The vital registration system also mostly functioned well. Coverage of births and deaths was incomplete in the 1950S, but improved to nearly full coverage by the 1970s. Estimates of completeness based on the Brass growth
This content downloaded from 151.100.102.94 on Wed, 23 Jul 2014 14:13:45 PMAll use subject to JSTOR Terms and Conditions

ARJAN GJONQA I CHRIS WILSON I JANE FALKINGHAM 595
balance method and the Bennett-Horiuchi method indicate figures of 78 to 85 percent coverage in the 1950s, rising to 98 percent by the 1980s (Gjonca 1996a). Again, compared with the problems encountered in using vital registration data in many developing countries, such underregistration is slight and easily taken into account when calculating life tables. Age data on death records also appear to be generally reliable. On the other hand, information on cause of death is more problematic. In the first years of the communist era, only a minority of deaths were certified by medically trained personnel, though this rose substantially over time. In 1950 only about 20 percent of causes of death were reported in this way, while by 1980 the fraction had risen to over 90 percent. Clearly caution is needed in inter- preting cause-of-death data.
In addition to basic demographic and medical statistics, the archives also hold a wealth of information on the nature and budgets of the health system and background information that can deepen our understand- ing of policy decisions. Nevertheless, the isolationist policies of the com- munist regime extended to its statistical system. Unlike the rest of East- ern Europe, Albania did not adopt the full Soviet data-gathering system. Thus, even today, many social and medical statistics that are routinely available for all other former Eastern bloc states are not found for Alba- nia. In recent reports on health and mortality changes during the tran- sition to market economies, for example, many tables of social indica- tors have a blank cell for Albania (UNICEF 1994). Thus, the scope for detailed comparative analysis of the socioeconomic determinants of mor- tality change is constrained.
Mortality decline in international perspective
To assess the scale of Albania's improvement in mortality since 1950, we should view the gains in the context of experiences in other countries in Eastern and Southern Europe. Albania's former communist allies in the Balkans-Bulgaria, Romania, and Yugoslavia-had much in common in terms of their health and education provision and the form of economic organization. In contrast, the market-oriented states of Southern Europe- Greece, Italy, Portugal, and Spain-provide examples of health transition in very different social and economic conditions, but share many of the cultural features typical of the Mediterranean, such as diet. Moreover, in spite of the government's policies of isolation, Albania's health transition was clearly part of the global process of medical and public health improve- ment and must be viewed in the appropriate international context.
As a first point of departure, Figure 3 presents the values for life ex- pectancy at birth for both sexes combined over the period 1950-90 for Al- bania and the countries used for comparative purposes. Table 2 gives the
This content downloaded from 151.100.102.94 on Wed, 23 Jul 2014 14:13:45 PMAll use subject to JSTOR Terms and Conditions

596 HEALTH TRANSITION IN ALBANIA
FIGURE 3 Life expectancy (in years) at birth: Albania and other countries of Eastern and Southern Europe, 1950-90
80
70
Italy ,'"Romani
i~~~~~ai
60 Portua/
Yugoslavia lbania
50 II
1950 1960 1970 1980 1990
SOURCES: See Table 2.
sex-disaggregated values. The Albanian statistics are based on our own life table calculations, while the values for other countries are drawn from vari- ous UN Demographic Yearbooks and the publications of the national statisti- cal services. The Albanian results differ in some ways from those published by other scholars, though the differences are minor (Meksi and Iaquinta 1991; Meksi and Dalla Zuanna 1994).
Figure 3 and Table 2 make several points quite clear. First, life ex- pectancy at birth in Albania in 1950, a little over 51 years for each sex, was substantially lower than in any of the other countries shown. By 1960 there had been a marked improvement, so that eo had reached 62 for women and 61 for men, an increase of more than 10 years over the decade. However, Albania still remained at the bottom of the European ladder, though its level of eo was only slightly lower than that of Yugo- slavia or Portugal. By 1970 Albania's relative position had improved fur- ther, with male life expectancy surpassing the value for Portugal. Through the 1970s and 1980s, despite the lack of economic growth, life expectancy continued to improve in Albania, though not as rapidly as in noncommunist Southern Europe. Interestingly, the country did not experience any marked slowdown in mortality improvement as occurred in many Eastern European countries under the last decades of commu-
This content downloaded from 151.100.102.94 on Wed, 23 Jul 2014 14:13:45 PMAll use subject to JSTOR Terms and Conditions

ARJAN GJONFA / CHRIS WILSON / JANE FALKINGHAM 597
TABLE 2 Life expectancy (in years) at birth, by sex, for Albania and selected other countries, 1950-90
Country 1950 1960 1970 1980 1990
Males Albania 51.1 61.2 64.1 (1969) 65.4 (1979) 67.8 (1989)
Selected countries of Central and Eastern Europe
Bulgaria 64.3 (1953) 67.5 69.1 68.5 68.2 Romania 58.0 64.6 (1962) 65.8 66.6 66.8 Yugoslavia 54.8 61.8 65.0 67.8 69.6
Selected countries of Southern Europe
Greece 63.4 67.3 70.1 72.1 74.6 Portugal 55.4 61.5 62.6 68.0 69.8 (1991) Italy 63.4 (1951) 66.9 68.7 (1971) 71.0 73.6 Spain 59.8 67.4 69.6 72.5 73.4
Females Albania 51.4 62.2 68.4 (1969) 72.0 (1979) 74.2 (1989)
Selected countries of Central and Eastern Europe
Bulgaria 70.2 (1953) 71.1 73.5 73.9 74.9 Romania 62.0 68.5 (1962) 70.4 71.8 73.3 Yugoslavia 58.5 65.2 69.8 73.3 75.6
Selected countries of Southern Europe
Greece 66.7 70.4 73.5 76.6 79.7 Portugal 60.6 66.8 68.9 75.5 77.3 (1991) Italy 67.0 (1951) 71.8 74.8 (1971) 77.6 80.3 Spain 64.3 72.2 75.1 78.6 80.5
SOURCES: Authors' calculations for Albania; others based on data from UN Demographic Yearbooks, 1950-92, and the Statistical Yearbooks of each country.
nist rule. The data give evidence of such a feature for Romania and Bul- garia, where life expectancy in 1990 was about the same as in 1970. Data for other parts of Eastern Europe and the Soviet Union show marked worsening. For example, levels of eo in Hungary and Russia were lower in 1990 than they had been 25 years before (UNICEF 1994: 24). This worsening or slowdown in improvement of mortality was particu- larly noticeable for males in most communist countries.
Another noteworthy feature of the data on life expectancy in Al- bania is the very small female advantage in early years. In 1950 the female eo was 51.4 compared with 51.1 for males, while in 1960 the female value of 62.2 was exactly one year more than the analogous fig-
This content downloaded from 151.100.102.94 on Wed, 23 Jul 2014 14:13:45 PMAll use subject to JSTOR Terms and Conditions

598 HEALTH TRANSITION IN ALBANIA
ure for males. In most other parts of Europe by that time, female eo was at least four years higher than the value for males, even in countries where overall life expectancy was little longer. Interestingly, however, the Yugoslav region of Kosovo, which is almost entirely populated by ethnic Albanians, showed similarly little female advantage. In 1950 life expectancy for females there was 51.9 against 51.8 for males, and in 1960 the male eo was actually higher than the female: 56.8 versus 55.5. By 1970 in both Albania and Kosovo, the female advantage had be- come more evident, and by 1990 the female advantage in eo in Albania exceeded six years. The similarity of the sex-specific patterns in Albania and Kosovo, and their difference from other countries at similar levels of mortality, suggest the existence of traditional cultural traits that were relatively disadvantageous for females.
Although life expectancy at birth is a convenient indicator of over- all mortality conditions, it can mask significant differences in the rela- tive improvement at different ages. This is certainly true for Albania. The most significant improvement in mortality over this period occurred at the youngest ages, as must be the case in any transition from an eo of around 50 to one above 70. Early-age mortality is, therefore, clearly worth considering first. Figures 4 and 5 show infant and child mortality
FIGURE 4 Infant mortality rate: Albania and other countries of Eastern and Southern Europe, 1950-90
150
\Yugoslavia
125-
Romana ioo 1 Albania
> 0 ~~Portugal
25 -..
0 I 1 I
1950 1960 1970 1980 1990
SOURCES: See Table 2.
This content downloaded from 151.100.102.94 on Wed, 23 Jul 2014 14:13:45 PMAll use subject to JSTOR Terms and Conditions

ARJAN GJON;A / CHRIS WILSON / JANE FALKINGHAM 599
FIGURE 5 Child mortality rate: Albania and other countries of Eastern and Southern Europe, 1950-90
0.12
- 0.10 \
-X \Albania
u 0.08
3 0.06
DPortugal
-0.04 _. Yugoslavia Greece Romania
0.02 X=Span
1950 1960 1970 1980 1990
SOURCES: See Table 2.
rates for the sexes combined in the same years and countries examined above. Tables 3 and 4 give the sex-specific values. All of the countries shown have registered gains in mortality under age 5, but Albania has consistently had the lowest values of infant and child survival. More- over, females were at a disadvantage in both measures until 1970 and even in 1990 between their first and fifth birthdays still had worse mor- tality than males. The reduction of the infant mortality rate from 134 to 42 per 1,000 live births, and of the child mortality rate (ages 1-4) from 108 to 16, over the course of the four decades was clearly a major achievement for the Albanian health care system. However, this still left it consistently underachieving when compared with neighboring countries. By 1990 the relatively high rate of childhood mortality was es- pecially noticeable, being about double the rate for Romania.
In contrast with the mixed record in infant and child health, Alba- nian adults experienced relatively low mortality throughout the postwar decades. Figure 6 and Table 5 present the relevant information on life ex- pectancy at age 15. Albania's more favorable relative position is clear; even in 1950 e15 for males exceeded the values for Portugal and Yugoslavia, and after a rapid improvement during the 1950s the value was better than that
This content downloaded from 151.100.102.94 on Wed, 23 Jul 2014 14:13:45 PMAll use subject to JSTOR Terms and Conditions

600 HEALTH TRANSITION IN ALBANIA
TABLE 3 Infant mortality rate (deaths per 1,000 live births) for Albania and selected other countries, by sex, 1950-90
Country 1950 1960 1970 1980 1990
Males Albania 133.2 95.1 87.9 (1969) 66.1 45.4
Selected countries of Central and Eastern Europe
Bulgaria 102.5 48.4 31.2 23.0 16.8 Romania 84.0 (1955) 81.6 54.2 32.8 29.8 Yugoslavia 125.5 91.7 57.1 32.9 20.5
Selected countries of Southern Europe
Greece 41.0 32.4 19.9 9.9 Portugal 100.2 83.4 62.5 27.2 12.3 Italy 68.3 47.6 32.6 16.4 8.9 Spain 74.6 39.2 23.4 13.9 8.3
Females Albania 134.9 106.9 91.1 (1969) 65.6 38.0
Selected countries of Central and Eastern Europe
Bulgaria 86.0 41.5 23.1 17.2 12.6 Romania 72.2 (1955) 69.5 44.4 25.8 23.9 Yugoslavia 111.1 83.5 53.7 29.8 17.9
Selected countries of Southern Europe
Greece 39.1 26.5 15.9 9.6 Portugal 87.5 71.2 53.2 21.2 9.6 Italy 59.2 39.9 26.4 12.5 7.8 Spain 64.8 31.6 18.0 10.7 6.9
SOURCES: See Table 2.
for Italy, a far richer country. Adult female mortality was also comparable with the levels seen in richer parts of Southern Europe, which are among the best in the world. Relatively little improvement occurred after 1960, but in 1990 Albania's e15 values of 58 for men and 64 for women were several years longer than for any other former communist country. A re- cent study of age-specific mortality throughout Eastern Europe came to the same conclusion (UNICEF 1994). The latter study showed that in 1990 mortality in Albania was the highest among the former communist states of Eastern Europe at ages under 5, was average for 5-19-year-olds, yet was by far the lowest above age 20 (UNICEF 1994: 38). The reasons for this apparent paradox are considered in the next section.
This content downloaded from 151.100.102.94 on Wed, 23 Jul 2014 14:13:45 PMAll use subject to JSTOR Terms and Conditions

ARJAN GJONFA / CHRIS WILSON / JANE FALKINGHAM 601
TABLE 4 Child mortality rate (proportion dying between exact age 1 and 5 multiplied by 1,000) for Albania and selected other countries, by sex, 1950-90 Country 1950 1960 1970 1980 1990
Males Albania 94.8 51.4 20.7 17.0 15.5
Selected countries of Central and Eastern Europe
Bulgaria 21.4 (1953) 11.2 5.2 4.8 4.0 Romania 10.4 (1962) 10.0 7.3 8.4 Yugoslavia 43.1 17.9 9.6 4.4 2.8
Selected countries of Southern Europe
Greece 12.4 6.9 2.8 1.4 Portugal 53.0 27.6 14.7 5.6 3.6 (1991) Italy 17.9 (1951) 8.1 4.0 (1971) 2.0 1.6 Spain 28.6 8.4 4.3 2.9 2.0
Females Albania 121.7 68.4 24.4 23.5 15.6
Selected countries of Central and Eastern Europe
Bulgaria 22.2 (1953) 11.2 4.4 4.4 3.2 Romania 10.4 (1962) 9.2 5.9 6.8 Yugoslavia 43.1 18.2 10.4 4.0 2.4
Selected countries of Southern Europe
Greece 11.2 5.7 2.3 1.1 Portugal 51.1 25.3 13.1 4.3 2.8 (1991) Italy 17.5 (1951) 8.1 3.2 (1971) 2.0 1.6 Spain 27.6 7.3 3.5 2.4 1.6
SOURCES: See Table 2.
The determinants of mortality transition
The story of the health transition in Albania is in many ways the story of its political and social history over the last half-century. At the outset health conditions were very poor, and the health care and social policies intro- duced by the communist regime produced rapid and substantial improve- ment. The more or less equal access to basic educational and health ser- vices and the national coverage of the primary health care system formed the basis for this improvement. On the other hand, the communist policy of relentless self-sufficiency stalled advances in medical information and technology. Moreover, the poor state of infrastructure and the inadequate
This content downloaded from 151.100.102.94 on Wed, 23 Jul 2014 14:13:45 PMAll use subject to JSTOR Terms and Conditions

602 HEALTH TRANSITION IN ALBANIA
FIGURE 6 Life expectancy (in years) at age 15: Albania and other countries of Eastern and Southern Europe, 1950-90
64
7,
62
L iAlbania
60
Romania 56
54
Yugoslavia 52
1950 1960 1970 1980 1990
SOURCE: See Table 2.
quality of medical services ultimately imposed limits to the speed and scale of improvement. To achieve the very lowest levels of mortality, not only is high technology increasingly needed, but so is speedy access to emergency services. Neither of these is generally present in Albania. In many parts of the world an infant mortality rate of 42 per 1,000 in 1990 would have been seen as a great triumph. Indeed, compared with the situation in Al- bania in 1950, it was. In the context of other European countries, how- ever, it can only be judged a limited success.
While infant and child mortality in Albania remained the worst in Europe, adult mortality was another matter. Here two points emerge as significant. The first is the sharp decline in malaria, tuberculosis, and other infectious diseases in the 1950s and early 1960s. These had been major adult killers in earlier decades, and their near-elimination is evident in the proportionate contribution of the major cause-of-death categories to all deaths. As mentioned above, the proportion of deaths certified by a medi- cal practitioner was only 20 percent in 1950, and thus the cause-of-death data early in the study period must be viewed with caution. However, this fraction rose to 60 percent within a decade, so that the results presented in Figure 7 should be fairly representative. Certain irregularities, such as the fluctuations in the proportion of deaths attributed to "old age" or to respi- ratory causes, probably reflect changes in classification procedures. Viewed
This content downloaded from 151.100.102.94 on Wed, 23 Jul 2014 14:13:45 PMAll use subject to JSTOR Terms and Conditions

ARJAN GJON;A / CHRIS WILSON / JANE FALKINGHAM 603
TABLE 5 Life expectancy (in years) at age 15, for Albania and selected other countries, by sex, 1950-90
Country 1950 1960 1970 1980 1990
Males Albania 52.5 56.9 57.7 (1969) 57.4 (1979) 57.8 (1989)
Selected countries of Central and Eastern Europe
Bulgaria 57.3 57.0 55.7 54.9 Romania 55.1 (1962) 55.6 54.7 54.5 Yugoslavia 51.2 55.1 55.0 55.7 56.4
Selected countries of Southern Europe
Greece 57.5 58.7 59.2 60.6 Portugal 51.6 54.6 54.9 55.6 56.2 (1991) Italy 55.0 (1951) 56.0 56.5 (1971) 57.5 59.6 Spain 54.1 56.4 56.8 59.0 59.4
Females Albania 55.5 60.3 62.7 (1969) 66.8 (1979) 63.8 (1989)
Selected countries of Central and Eastern Europe
Bulgaria 60.4 60.8 60.6 61.3 Romania 58.5 (1962) 59.5 59.4 60.5 Yugoslavia 54.3 58.1 59.8 61.1 62.4
Selected countries of Southern Europe
Greece - 60.3 61.8 63.4 65.7 Portugal 56.4 59.2 60.6 62.6 63.5 (1991) Italy 58.1 (1951) 60.5 62.2 (1971) 63.9 66.2 Spain 56.1 60.6 61.9 64.8 66.4
NOTE: Female value for Albania in 1980 is evidently distorted by data problems. SOURCES: See Table 2.
overall, Figure 7 shows the patterns that one would expect. Infectious dis- eases, especially tuberculosis and gastrointestinal disorders, dropped sharply, from over 40 percent of all deaths in 1950 to very small values by the 1980s. Their place in the cause-of-death hierarchy was taken by cardiovascular and respiratory diseases and cancers.
With the reduction or elimination of the main infectious diseases af- fecting adults, life expectancy after childhood improved substantially. This enabled the effect of the second crucial factor to emerge: the Albanian diet and lifestyle. Albanians benefit from eating a rather extreme version of the classic Mediterranean diet now widely recommended by nutritionists. Table 6 presents estimates on caloric intake and the contribution of animal prod- ucts in the diet in Albania, along with the same information for the com- parison group of four noncommunist Southern European countries. Over-
This content downloaded from 151.100.102.94 on Wed, 23 Jul 2014 14:13:45 PMAll use subject to JSTOR Terms and Conditions

02 o ao~~~~~~~~~~~~ 4-
00 0% OR0'00
' 0 _
t
,
0 . Q
VI S 0 us - , _V
~~s S S 2
0~~~~~~~~~~~~~~~~~~~~~
oo
_. A
- _ 'a .o
Lo%~~~~~~~~~~~~~~~~~0
d UU
H ,"~~~~~~~~~~~~~~~~~~~~~~~E
- he ( R- _ _,1 t Ys - 0 ~~~~ - O0?
~~~~~~~~~~~~~o * _4,
'0 u' 0 0 g - VI * ~~~~~~~~~~o
This content downloaded from 151.100.102.94 on Wed, 23 Jul 2014 14:13:45 PMAll use subject to JSTOR Terms and Conditions

ARJAN GJONSA / CHRIS WILSON / JANE FALKINGHAM 605
all caloric intake in Albania is noticeably below the other group, but with over 3,000 calories per day this is still likely to be sufficient in most cases. The contribution of foods of animal origin, at 12 percent of the overall caloric intake, is far lower in Albania than elsewhere in Europe. Detailed statistics collected by the World Health Organization confirm that the con- sumption of meat and other animal products is very low indeed in Alba- nia. According to their figures, Albanians eat only 75 grams per day of meat (Gjonsa 1996b: 13). This is less than half the next lowest figure in Europe (WHO 1993: 19). The country also occupies the lowest position in terms of the consumption of all fats and oils. Moreover, olive oil, now well known for its beneficial qualities, is widely used. While a number of micro-nutri- ent deficiencies exist in the Albanian diet, overall it must be judged emi- nently healthy by current nutritional standards (UNICEF 1994: 84).
In addition to the advantages of diet, the lifestyle experienced by most Albanians under communism also conferred benefits. Alcohol consump- tion was low, again by far the lowest in Europe; smoking was rare among women, although common for men; and the lack of private vehicles ne- cessitated everyone taking regular exercise simply to carry out daily activi- ties (UNICEF 1994: 67; WHO 1993: 24). In short, the very poverty of their circumstances was, paradoxically, a significant factor in keeping Albanians healthy. This is clearly an ironic situation. Given a choice, there is little doubt that most Albanians would have preferred to eat more meat and other animal products. Similarly, many would have liked to have drunk more alcoholic beverages. It seems certain that they would also have wel- comed the chance to substitute car journeys for the lengthy walks and bi- cycle rides they had to undertake as part of their daily routine. If nothing else, this paradoxical situation should cause us to reflect further on the meaning of the term "quality of life" and to realize that life expectancy only tells us the average length of the human lifecourse.
TABLE 6 Consumption, per person per day, of major food products and of total calories: Albania and average of four other Southern European countries in the 1990s
Greece, Italy, Spain, Food Portugal (average)a Albaniab
Meat and meat products 251 grams 75 grams Milk and milk products 578 grams 400 grams Total fats and oils 85 grams 50 grams Vegetables, beans, and fruits 857 grams 610 grams Grains, rice, potatoes, and other cereals 572 grams 622 grams
Total calories 3,624a 3,115c From vegetable products 2,648 2,741 From animal products 976 (26.9 percent) 374 (12 percent)
SOURCES: a FAO 1996 (data refer to 1992-94). b Living Standard Survey, Institute of Statistics, Tirana, 1993. c Statistical Yearbook of Albania, 1991.
This content downloaded from 151.100.102.94 on Wed, 23 Jul 2014 14:13:45 PMAll use subject to JSTOR Terms and Conditions

606 HEALTH TRANSITION IN ALBANIA
Conclusions
We may summarize our main findings in the following three points. 1. Albania experienced considerable gains in life expectancy during
the communist period, with life expectancy at birth for the sexes combined increasing from 51.3 years in 1950 to 70.9 years in 1989, in spite of re- maining by far the poorest country in Europe. The gains reflected the glo- bal process of public health improvement, as well as the high priority given to health care and other aspects of the social agenda under conumunism, against the background of certain favorable aspects of lifestyle, especially diet.
2. The increase in life expectancy still left levels of infant and child mortality as the worst in Europe by some margin. As Table 7 shows, in the late 1980s the under-5 death rate in Albania was much higher than in
TABLE 7 Estimates of child and adult mortality rates in Albania and selected other countries
Between age 0 and 5 a Between age 15 and 60 b
Country Year Male Female Male Female
Albania 1984-85 50 45 134 73 Countries of Central and Eastern Europe
Bulgaria 1987 20 16 206 95 Czechoslovakia 1986 17 13 228 100 East Germany 1985-90 11 07 179 92 Hungary 1987 22 17 277 127 Poland 1987 21 16 248 103 Romania 1984 33 27 224 115 Soviet Union 1985-90 35 26 268 110 Yugoslavia 1987 30 27 198 98
Selected Southern European countries
Greece 1986 14 12 120 60
Italy 1985 13 10 144 67
Portugal 1987 18 15 175 81
Spain 1985 11 9 141 61
Selected developing countries
China 1986 44 33 166 149
North Korea 1985-90 46 35 214 123
Sri Lanka 1983 43 39 225 127
Cuba 1986 19 15 150 112
a Values of 5qo (proportion dying between exact age 0 and 5) multiplied by 1,000. b Values of 45q15 (proportion dying between exact age 15 and 60) multiplied by 1,000. SOURCES: Authors' calculations for Albania; Murray, Yang, and Qiao (1992) for others.
This content downloaded from 151.100.102.94 on Wed, 23 Jul 2014 14:13:45 PMAll use subject to JSTOR Terms and Conditions

ARJAN GJONCA / CHRIS WILSON / JANE FALKINGHAM 607
other European countries, but was similar to the values seen in such coun- tries as China and Sri Lanka. The relatively high rate of infant and child mortality is believed to reflect the continued inadequacy of medical care, especially emergency care, in Albania, exacerbated by poor infrastructure that prevented much of the rural population (almost two-thirds of the to- tal) from having effective access to emergency medical assistance.
3. Adult mortality in contrast is among the lowest in Europe. The death rates between ages 15 and 60 shown in Table 7 are comparable to those of Italy or Spain, much richer and more developed countries. This success has been achieved by the elimination of the main infectious diseases, com- bined with a particularly healthy diet and aspects of lifestyle, many of which, paradoxically, reflect the continuing poverty of the country.
Epilogue: Albania in political transition
Albania, whose political and economic regime had been the most extreme of all European communist countries, was the last to fall in the great po- litical changes that swept through Europe in 1989 and 1990. As elsewhere, the last years of communism and the first years of the new order saw per- vasive economic dislocations. Estimated GNP per head fell over 40 percent during 1990 and 1991. The collapse led Albania to ask for and receive un- precedented supplies of emergency aid, especially food. In 1992 and 1993 the country received more food aid per head than any other in the world, amounting to 4.7 percent of the global food aid provision in 1992 and 3.8 percent in 1993 (UNICEF 1994: 77). Yet, following so deep a crisis, which left virtually the entire nonagricultural sector in chaos, the Albanian economy then experienced a period of remarkable growth. From 1993 to 1996 GNP per head is estimated to have grown over 10 percent a year. However, the financial and political crisis that overwhelmed the country in early 1997 clearly poses significant problems for continued growth.
At present a detailed demographic picture of postcommunist Albania is lacking. The Institute of Statistics, in Tirana, has estimated that life ex- pectancy in 1993 was 73 years for both sexes combined, an appreciable improvement over the 1989 level, achieved despite the economic slow- down that precipitated the fall of the old regime and the economic crisis of the early 1 990s. In some other formerly communist countries, notably Rus- sia, the 1990s have been, in contrast, disastrous; by 1993 life expectancy at birth for males in Russia had fallen to 58.6 years, a value more commonly seen in the poorest developing countries (Shkolnikov, Mesle, and Vallin 1995: 916). With much statistical information still to be quarried from the archives, the full story of Albania's relative success cannot yet be told, but we can make a number of speculations. The first is to recall the extent to which Albania remained basically an agricultural and rural population
This content downloaded from 151.100.102.94 on Wed, 23 Jul 2014 14:13:45 PMAll use subject to JSTOR Terms and Conditions

608 HEALTH TRANSITION IN ALBANIA
throughout the communist era. This helped it to avoid many of the prob- lems associated with pollution that were prevalent in much of Eastern Eu- rope and to limit the social consequences of the industrial decline. More- over, since Albania's success in health care lay in the provision of relatively unsophisticated primary care and the maintenance of a healthy lifestyle, there was less scope for problems to arise when the health care system began to fail. The lifestyle issues are again likely to be of crucial importance. In par- ticular, alcoholism, a serious problem among men in Russia and a number of other Eastern European countries, is far less significant in Albania.
When assessing changes after the fall of the communist regime, men- tion must also be made of the provision of international aid after 1991. As a small country, with only 3 million people, Albania posed humanitarian problems of a manageable scale, unlike those that beset the much larger populations of many other former communist states, especially Russia. Moreover, a substantial, but still undocumented, fraction of the Albanian population has migrated, mostly temporarily and often illegally, to nearby states. An estimated 10 percent of the entire population left between 1991 and 1994, though net flows to and from the country are now believed to be roughly balanced. The migrants provided substantial remittances, smoothing the economic problems faced in the transition to a market economy. Again, this is an adjustment mechanism that is scarcely open on such a scale to countries with larger populations.
Note The authors acknowledge the financial support of the Wellcome Trust for the History of Medicine.
References
Bollano, P. 1984. 'The limitation of wage differentials,' Albanian Life, No. 29: 21. Caldwell, John C. 1986. "Routes to low mortality in poor countries," Population and Devel-
opment Review 12, no. 2: 171-220. Caselli, Graziella. 1996. "National differences in the health transition in Europe," Historical
Methods 29, no. 3: 107-125. FAO. 1996. Food Balance Sheets. Rome: Food and Agriculture Organization. Frey, B. et al. 1990. Human Rights in the People's Socialist Republic of Albania. Minneapolis:
Minnesota Lawyers' International Human Rights Committee. Gjonqa, Arjan. 1996a. "The demographic regime in Albania, 1950-1990," paper presented
at the International Conference on Demography in the Balkans, Thessaloniki, Greece, June. . 1996b. "Mortality and health transition in Albania, 1950-1990," paper presented
at the Annual Conference of the British Society for Population Studies, St. Andrews, Scotland, September.
Hackett, L. W. 1944. "Spleen measurement in malaria," Journal of the National Malaria Soci- ety 3, no. 2: 121-133.
This content downloaded from 151.100.102.94 on Wed, 23 Jul 2014 14:13:45 PMAll use subject to JSTOR Terms and Conditions

ARJAN GJONCA / CHRIS WILSON / JANE FALKINGHAM 609
Hall, Derek. 1994. Albania and the Albanians. London and New York: Pinter. Halstead, Scott B., Julia A. Walsh, and Kenneth S. Warren (eds.). 1985. Good Health at Low
Cost: Proceedings of a Conference Held at the Bellagio Conference Center, Bellagio, Italy, April 29-May 2 1985. New York: Rockefeller Foundation.
Hamilton, Bill. 1992. Albania: Who Cares? Grantham, England: Autumn House. Institute of Statistics. 1991. Vjetari statistikor i Shqiperse (Statistical Yearbook of Albania).
Tirana, Albania. Keefe, E. K. et al. 1971. Area Handbook for Albania. Washington, D.C.: US Government Print-
ing Office. Logoreci, Anton. 1977. The Albanians: Europe's Forgotten Survivors. London: Victor Gollancz;
Boulder, CO: Westview Press. Maddison, Angus. 1995. Monitoring the World Economy, 1820-1992. Paris: Organisation for
Economic Cooperation and Development. Meksi, Ermelinda and Pietro Iaquinta. 1991. "Aspects de l'evolution demographique en
Albanie, Population 46, no. 3: 679-692. Meksi, Ermelinda and Gianpiero Dalla Zuanna. 1994. "La mortalite generale en Albanie
(1950-1990)," Population 49, no. 3: 607-636. Murray, Christopher, J. L., Gonghuan Yang, and Xinjian Qiao. 1992. "Adult mortality: Lev-
els, patterns and causes,' in Richard G. A. Feachem et al. (eds.), The Health of Adults in the Developing World. Oxford and New York: Oxford University Press.
Okolski, Marek. 1994. "Health and mortality," in United Nations Economic Commission for Europe and United Nations Population Fund, European Population Conference, Vol. 1,pp. 119-205.
Shkolnikov, Vladimir, France Mesle, and Jacques Vallin. 1995. "La crise sanitaire en Russie," Population 50, no. 4-5: 907-982.
Schnytzer, Adi. 1982. Stalinist Economic Strategy in Practice: The Case of Albania. Oxford and New York: Oxford University Press.
Sjoberg, Orjan. 1991. Rural Change and Development in Albania. Boulder, CO and Oxford: Westview Press.
UNICEF. 1994. Crisis in Mortality, Health and Nutrition. Florence, Italy: UNICEF International Child Development Centre.
United Nations Development Programme. 1995. Human Development Report. Oxford and New York: Oxford University Press.
World Bank. 1996. World Development Report 1996. Oxford and New York: Oxford University Press.
World Health Organization. 1993. STOA Report on Nutrition in Europe. Geneva: WHO Re- gional Office for Europe.
This content downloaded from 151.100.102.94 on Wed, 23 Jul 2014 14:13:45 PMAll use subject to JSTOR Terms and Conditions