Paradigm Shifts in Chaplaincy & The Implementation of Spiritual
86
SHIFTS IN CHAPLAINCY 1 Paradigm Shifts in Chaplaincy & The Implementation of Spiritual Assessment Tools Corinna H. Chung Buddhist Chaplaincy Training Program, Upaya Zen Center, Santa Fe, NM Spiritual Care, Christus St. Vincent Regional Medical Center, Santa Fe, NM Email: [email protected]
Transcript of Paradigm Shifts in Chaplaincy & The Implementation of Spiritual

SHIFTS IN CHAPLAINCY 1
Paradigm Shifts in Chaplaincy &
The Implementation of Spiritual Assessment Tools
Corinna H. Chung
Buddhist Chaplaincy Training Program, Upaya Zen Center, Santa Fe, NM
Spiritual Care, Christus St. Vincent Regional Medical Center, Santa Fe, NM
Email: [email protected]

SHIFTS IN CHAPLAINCY 2
TABLE OF CONTENTS PAGE
Abstract 5
I. Introduction 6
II. Christian Chaplaincy Model 8
A. Historical and Traditional Chaplains 8
B. Theology Science Dichotomy 9
C. Rome Gaia Dichotomy 10
III. Integrated Chaplaincy Model 11
A. Professional Chaplains 11
B. Secular Chaplaincy 13
C. Defining Patients’ Needs 14
i. Secular 15
ii. Existential 15
iii. Humanist 15
iv. Spiritual versus Religious 16
D. Dangers of Interpretation 18
E. Expanding Chaplaincy Services 19

SHIFTS IN CHAPLAINCY 3
IV. Science Friendly Chaplaincy: Implementing Spiritual Assessment Tools 19
A. Holistic Medicine 19
B. Reasons for Using Assessment Tools 21
C. Types of Tools 24
i. Self-Assessment Tools 24
ii. Quantitative Assessment Tools 25
iii. Qualitative Assessment Tools 25
iv. Outcome Measure Tools 27
D. Bias and Limitation 31
E. Levels of Assessment 32
i. Screening 32
ii. Structured Quantitative Assessment 34
iii. Structured Qualitative Assessment 34
(The Integrative Assessment Tool)
iv. Unstructured Qualitative Assessment 43
V. Palliative Care Chaplaincy 44
VI. Chaplaincy Skills and Challenges 49
SHIFTS IN CHAPLAINCY 4
A. Listening and Communication Skills 49
B. Silence 50
C. Power Imbalance 51
D. Authority 51
E. Intimacy 52
F. The Midwife 52
G. Wounded Healer in the Valley of Shadows 53
H. The Human Condition 54
I. Knowing One’s Mind 54
VII. One Objection to “The Consensus Conference Report” 55
VIII. Interventions 58
IX. Conclusion 59
A. End of Life Care Chaplaincy 59
B. Environmental Chaplaincy 60
Acknowledgements 62
References 63
Appendices 1 - 7 70 - 86
SHIFTS IN CHAPLAINCY 5
Abstract
Reflecting on the changing role of chaplains interrelated with Church history, the theology
science dichotomy and cultural paradigm shifts in society at large, the author outlines how in the
current model of chaplaincy, science has become an ally by endorsing the effectiveness of
spiritual care. This paper explores the use of spiritual assessment tools to enhance hospital
chaplaincy by monitoring quality through outcome measures, and fostering skills other than
intuition in chaplains. The new “Integrative Assessment Tool” created by the author includes a
section to address end-of-life planning and is followed by a discussion on palliative care
chaplaincy. Chaplains’ skills needed to properly implement spiritual assessment tools
emphasizes the importance of self-knowledge. The chaplains’ role has widened in response to
the reshaping of their profession, which is now rooted in both spiritual and fundamental human
values and, as another paradigm shift emerges, also encompasses environmental chaplaincy.
SHIFTS IN CHAPLAINCY 6
I. Introduction
The changing role of chaplains mirrors broad shifts in the social and cultural arenas that
took place in the Western world. As values and thought systems evolve, so do understanding and
expectations of chaplaincy. When chaplaincy was still nested within the Christian Church, other
faiths, atheism and science were seen as antagonists. The interfaith model of contemporary
chaplaincy is inclusive of, but distinct from its Christian interpretation, and therefore more
attuned to the pluralistic religious landscapes of the ‘global village’.
Particularly since the turn of the 20th century, conceptual frameworks changed within
institutions and in society at large. Theosophy popularized the perspective that each religion
presents only one of different roads to the truth. Rudolf Steiner infused Waldorf pedagogy with
implicit spirituality. Vatican II greatly impacted the Roman Catholic Church by opening up
dialogue with other faiths, empowering congregations to participate in mass in their own
languages opposed to Latin, and making it legitimate for people born into Catholic culture to find
personal interpretations of what it means to be Catholic ‘in spirit’. The modern world has
become more secularized and atheist, agnostic, existentialist and humanist movements are
reflected today in the change in patients’ needs. The shifts in chaplaincy might have been more
gradual than the dramatic paradigm shift in physics initiated by Einstein’s special relativity;
some nonetheless consider it revolutionary. The indignant refusal of a New York Times reader1
to embrace the idea that ministry to the sick and dying could not only be nonsectarian, but
secular, exemplifies the barriers to see beyond a model of chaplaincy which has integrated other
faiths, but not the lack thereof.

SHIFTS IN CHAPLAINCY 7
Today’s model of hospital chaplaincy must be attuned to the needs of patients who
consider themselves spiritual, but not religious. When the Western world achieved materialistic
success and saturation, the thirst for satisfaction, inner peace and meaning failed to be quenched.
In terms of Maslow’s hierarchy of needs, it was maybe because the basic needs of satisfying
physical survival and safety was met, that a large population was free to pursue Eastern
philosophies, which lead to meditation and yoga no longer remaining ‘avant garde’ and
accessible to few but becoming mainstream, as did therapy and other self-esteem and self-
actualization techniques, the two highest needs in the Maslow hierarchy. Many titles in the top-
selling book lists over the past decades reflect interest in self-transformation and finding purpose
and peace. The 1960’s movement opened different ways to perceive reality and consciousness2
(Huxley, 1954), and not all were brought about by the use of psychedelics; the neurosciences
continue to puzzle over the nature of consciousness till today. Key elements of the 60’s became
integrated by society at large and are expressed in more women becoming chaplains, the critical
questioning of standard values and the continued search for alternatives to a purely materialistic
worldview. This could at least partly explain why chaplaincy services are growing in response to
an increasing number of people accepting chaplains’ visits1.
A new paradigm of chaplaincy has emerged which embraces scientific research. In spite
of its historical role as antagonist, science surprisingly has become an ally providing empirical
evidence for the efficiency and value of spiritual care. On one hand, scientific studies were
precipitated by an increasing interest to overcome the split between science-based and holistic
medicine and to prove the positive correlation between spiritual care and physical health. On the
other hand, pastoral research was necessitated by health care facilities demanding accountability
and hard facts, not anecdotal data, to justify the cost of spiritual care departments by showing

SHIFTS IN CHAPLAINCY 8
measurable outcomes, for example, shorter hospital stays or less use of pain medication. Critics
argue against chaplains becoming full-fledged members of heath care teams or having full access
to medical files and contend that spiritual care is but the emperor’s new clothes.3 Overcoming
historical confrontations, science and spirituality can converge in a chaplaincy model that is a
higher synthesis with patients being the beneficiaries.
II. Christian Chaplaincy Model
A. Historical and Traditional Chaplains
Saint Martin of Tours (319-397 AD) aspired to serve God when in his childhood.
However, it was required of him to join the army at age 15 and he remained a soldier until he
was 20. In the winter of 337 AD, riding near the city gates of Amiens, Gaul, he noticed a beggar
destitute of clothing. He cut his military cloak into two equal halves and gave one to the
shivering beggar. As Severus (360-425 AD), his friend and biographer, writes further, “Martin,
that man full of God, had nothing except his arms and his simple military dress. Some by-
standers laughed at him because the cloak was now an unsightly object. Those of sounder
understanding groaned because they had done nothing similar.” The following night Martin was
rewarded with a vision of Christ wearing his half cloak and making known to the angels his act
of mercy. St. Martin was acclaimed Bishop of Tours in 371 AD.
Cappellanus (Latin) denoted a cleric who was the custodian of the sacred cloak of St.
Martin under the Frankish kings. The first chapel4 was a sanctuary to preserve St. Martin’s cloak.
Later, clerics officiating in the chapel of a sovereign or in settings where the people did not have
free, frequent access to a regular cleric, such as in a hospital, were called chaplains. Prior to the
appointment as chaplain, a cleric first has to thoroughly train and serve in his own faith
SHIFTS IN CHAPLAINCY 9
community. The use of the word ‘chaplaincy’ probably only began when General Orders issued
in 1776 provided a chaplain for each US regiment. The traditional chaplain ministered and
sought to guide others to his own faith group5.
B. Theology Science Dichotomy
One cannot ignore that the 18th century is also the time of the Roman, and fourth
manifestation of the Inquisition since 1184, leaving a long legacy of forced conversions, witch-
hunts, torture and execution of purported heretics. As it happens, St. Martin, who gave chaplains
their name, intervened – albeit unsuccessfully – when the Priscillianists became the first
Christians executed for heresy in 385 AD. For centuries the relationship between theology and
science was characterized by struggle more than by dialogue. St. Augustine, the contemporary
church father of St. Martin, regarded scientia, scientific knowledge, as spiritually barren and
misleading. Because it was inferior to sapientia, theological wisdom, the Church considered
theology ‘the queen of sciences’ for centuries. Thomas Aquinas, the 13th century Roman
Catholic philosopher, also saw theology as a science. He stated that it is a confluence of faith and
reason that allows knowledge of God. During the Reformation Martin Luther and John Calvin
opposed the view of theology being a science and defined it as the practical study of the
relationship between God and human beings6 (VandeCreek, 2008). Although science and
theology in many ways seek answers to the same fundamental questions, the fact remains that the
Church frowned on scientific experiments and observation, repressed new ways of thinking and
persecuted scientists. The famous trial against Galileo Galilei took place in 1633 because of his
publication ‘Dialogue of the Two Chief World Systems’. In the year 2000 Pope John Paul II
reopened Galileo’s case and issued an apology titled ‘Memory & Reconciliation’ for the sins
committed over the ages in the name of the Church.
SHIFTS IN CHAPLAINCY 10
C. Rome Gaia Dichotomy
Other ancient controversies than theology and science continue into the present. Reigning
Pope Benedict XVI recently warned about ‘the danger of worshiping nature as the new divinity’;
the Vatican criticized the film ‘Avatar’ as godless, ‘it cleverly winks at all those pseudo doctrines
that turn ecology into the religion of the 21st century’. Reactions7, especially from young people
reflect views of the Roman Catholic Church seen as an irrelevant anachronism, as being
‘repressive, rigidly dogmatic’ and having ‘archaic viewpoints’. It is possible, commentators
write, ‘to honor nature and feel in an interdependent relationship with all life while still
respecting and honoring God; the worship of nature does not seem stranger than the worship of a
virgin mother; God is creation and creation is God’. Many voices reiterate that this film has
struck a deep cord not because it is about the worship of nature as a God per se, but that the
message could be interpreted in the words of Aldo Leopold8 as: “We abuse land because we
regard it as a commodity belonging to us. When we see land as a community to which we
belong, we may begin to use it with love and respect” (A Sand County Almanac, 1949). Even in
earth’s recent history there are countless incidences that mirror the imaginary struggle of the
Na’vi on Pandora, be it the people of Austin, Texas, in 1992 coming together to protect Barton
Springs against unchecked development, or the alliances formed to stop the destruction of the
rainforest. According to an offshoot of general systems theory, which was intended to formalize
the concept of ‘life’, the earth qualifies as much as a living system as does a human being: “a
nonrandom accumulation of matter-energy in physical time-space organized into interacting,
interrelated subsystems”9. Humans could be regarded as little subsystems nested within the
higher-level system of Mother Earth.
SHIFTS IN CHAPLAINCY 11
III. Integrated Chaplaincy Model
A. Professional Chaplains
Whether or not millions of movie-goers think of this film as a parable of how
corporations/countries/Church have accumulated wealth and power by exploiting earth’s
resources/foreign countries/indigenous people through capitalism/colonization/conquistadors, the
fact remains that there are populations in the modern world offended by either words ‘religious’
or ‘spiritual’, even if latter carries less negative connotations: atheist, materialist, agnostic,
humanist, existentialist, secular ‘free-thinkers’; indigenous, ethnic, shamanistic and other
traditions that survived into the present; followers of contemporary paganism, (pagan from the
Latin paganus, means ‘rustic, from the country’, because conversions often did not reach people
living in the countryside, and later developed into a pejorative term, like heathen, referring to an
uneducated godless person), a post-modern development in industrialized countries reviving pre-
Christian cults, such as Druids, worshipers of Nordic or Germanic god, Occultists, Wicca, those
who honor the Great Goddess in its various manifestations and feel patriarchic Christianity
suppressed matriarchic traditions, and many others.
Independent of their faith or lack of faith, most people do not want to be alone, unseen,
unheard in a hospital or at the end of their life, and would derive much benefit from being tended
to by spiritual care practitioners capable of providing the most essential of services: the genuine
warmth and presence of a fellow human being, attentive listening without judgment or need to
manipulate. In Albert Camus’ novel ‘The Plague’ he defines the good man as ‘the man who has
the fewest lapses of attention’ while in ‘The Stranger’ the chaplain gets very upset when he
cannot ‘save’ Meursault, the protagonist. Often the refusal of pastoral visits stems from the

SHIFTS IN CHAPLAINCY 12
lingering image of the traditional chaplain trying to convince a person that the only salvation is
to turn to the Christian God. This is actually a misconception of the role of a professional
chaplain of the 21st century; proselytizing is considered unethical practice and a violation of
trust. As a result of the spread of democratic values and religious tolerance, the professional
chaplain is expected not only to have an ecumenical attitude concerning the Christian unity, but
tolerance and full respect toward all faiths, or lack of faith, ethnicity and gender. “The chief
modus operandi is that of a deep-seated respect for religious freedom, freedom of conscience and
an attempt to serve all people within an inclusive and holistic framework without negating one’s
own faith’10.
In an attempt to use terminology that is inclusive of all spiritualities and to standardize
names, especially in hospital settings, it has been recommended to substitute predominantly
Christian terms such a chaplain, chapel and pastoral care with spiritual care practitioner, sacred
space and spiritual care department11, 17. In this document ‘chaplain’ appears because it has two
syllables rather than eight, and the history of St. Martin splitting his cloak serves as reminder to
caregivers to be loving, yet wise enough not to freeze in the cold (or to burn out).
Although the author does not draw inspiration from St. Martins later enthusiasm for
destroying ancient pagan places of worship, his act of generously sharing his cloak does call to
mind words very inspirational for chaplaincy: “Come, ye blessed of my Father, inherit the
kingdom…For when I was naked, ye clothed me: I was sick, and ye visited me: I was in prison,
and ye came unto me…Inasmuch as ye have done it unto one of the least of these my brethren,
ye have done it unto me.” (Matthew 22:34-40).
SHIFTS IN CHAPLAINCY 13
“Unto me?” I do not know you
“Unto me?” I do not know you --
Where may be your House?
“I am Jesus – Late of Judea --
Now – of Paradise” --
Wagons – have you –to convey me?
This is far from Thence –
“Arms of Mine – sufficient Phaeton –
Trust Omnipotence” --
I am spotted – “I am Pardon” --
I am small – “The Least
is esteemed in Heaven the Chiefest --
Occupy my House” --
Emily Dickinson
B. Secular Chaplaincy
Regardless of the name, the role of the chaplain certainly is changing. “They are in some
ways a different breed”, says Josephine Schrader of the Association of Professional Chaplains
(APC), the largest certification body for chaplains. “The new chaplaincy culture is more
professional and secular, more adaptable in approach.” When the New York Times issued a
SHIFTS IN CHAPLAINCY 14
front-page article entitled “Hospice Chaplains Take up Bedside Counseling” by Paul Vitello in
October 2009, it caused heated online discussions whether it was appropriate to use the word
‘secular’ in connection with ‘chaplaincy’. “Listening to final inquiries has long been the domain
of a Priest or Rabbi”, the article stated, “but it is increasingly likely to belong to an emerging
professional class known as chaplain, who may or may not be a clergy member. More and more
ministering to the terminally ill is likely to be nonsectarian or even secular.”
In one study palliative care patients identified their top 6 spiritual needs as follows: to
have time to think, to retain hope, to deal with unresolved issues, to prepare for death, to express
true feelings without being judged, to speak of important relationships12 (Kernonhan, 2007).
Another study developed from open-ended questions13 (Strang, 2003) lists the questions most
frequently posed to hospital chaplains by palliative care patients as fitting into four main
categories. They were of a general existential nature concerned with meaning (34%), death and
dying (21%), pain and illness (13%) and relationships (15%). Only 8% were religious. “The ones
with family priests are not calling on us” (Vincent Corso, Pastoral Care Director for Visiting
Nurse Service of New York). “There is a shift in the way people are meeting their spiritual
needs. Chaplains give spiritual council to that growing segment of the population that describes
itself in polls as feeling connected to a higher power but not to an organized faith” (Rev. G.
Handzo, vice president of Health Care Chaplaincy).
C. Defining Patient’s Needs
In current discussions various adjectives are used to name and categorize patients’ needs.
Defining and clarifying these concepts helps the chaplain and other team members to understand
them.
SHIFTS IN CHAPLAINCY 15
i. The definition of secularism as “that which seeks the development of the physical,
moral and intellectual nature of man to the highest possible point as the immediate duty of life”
(English Principles of Secularism, 17) does not make the notion of a secular chaplain sound
paradoxical. However, the American Secular Union has for its object the separation of Church
and State and for its platform the Nine Demands of Liberalism. The second one states: “the
employment of chaplains in Congress (the first chaplain in the United States House of
Representatives was elected in 1789) and all institutions supported by public money shall be
discontinued”.
ii. Existential might be a less ambiguous choice, because it simply relates or deals with
human existence. Existentialism can be defined as a philosophical movement emphasizing the
uniqueness of each human being, freedom of choice and personal responsibility. Christian
existentialism describes a group of writings that take a philosophically existential approach to
Christian theology, relying on Kierkegaard’s understanding that God, for the most part, can be
equated with love. “Early Christianity” that existed during the first three decades of the
Resurrection of Christ, is held to be more pure than its present form.14
iii. From a humanist perspective God might represent a set of values, which is one’s
focus and purpose in life (Oddnall,1996)15, 66. Humanism affirms the dignity and worth of all
people, based on the ability to determine right and wrong by appeal to universal human qualities,
particularly rationalism. It entails a commitment to the search for truth and morality. In focusing
on self-determination, Humanism rejects transcendental justifications, dependence on faith, the
supernatural or divinely revealed texts.16
SHIFTS IN CHAPLAINCY 16
iv. Spiritual comes from the Latin spiritualitas, breath. Spirituality is often considered an
elastic term not capable of universal definition. However, some attempts have been made. In the
report of the consensus conference the multidisciplinary team agreed on the following definition
of spirituality:
Spirituality is the aspect of humanity that refers to the way individuals seek and express
meaning and purpose and the way they experience their connectedness to the moment, to
self, to others, to nature, and to the significance of the sacred.17 (Consensus Conference
Report, 2009)
In a leaflet entitled “Spirituality and Mental Health”, Britain’s Royal College of
Psychiatrists (RCP) offers the following explanation:
In healthcare, spirituality is identified with experiencing a deep-seated sense of meaning
and purpose in life, together with a sense of belonging. It is about acceptance, integration
and wholeness.
Spirituality is whatever or whoever gives one a transcendent18 meaning in life. This may
be expressed as religion but may also refer to nature, energy, belief in the good of all, the
importance of family and community.19
There are many presuppositions about what comprises spiritual practices. Some people
regard the following as spiritual: cooking, gardening, being in nature, acts of compassion, team
sports, martial arts, artistic pursuits or appreciation of art.
Persons who consider themselves spiritual but not religious, may regard their body as the
place of worship accessible at any time, not only Sundays; they do not rely on clergy as an

SHIFTS IN CHAPLAINCY 17
intermediary to the divine; they do not believe only one religion has exclusive access to the truth
or Sacred Source. Various spiritual or esoteric Gnostic beliefs hold that creation including our
own being is essentially sacred; we carry a divine spark. Through both the gift of blessing and
personal effort in contemplation, meditation and prayer one may effect a spiritual transformation
and the spark, once enflamed, consumes the egoic self. The spiritual practitioner/petitioner may
experience “I and the Father are one”, or become a more fully realized human being, or one
could say, does justice to having been “created in the Image and Likeness of God”. The Sacred is
both transcendent and immanent, a deep kinship and respect is felt for ‘God’ and all beings. This
spiritual experience is unifying rather than divisive and an attitude of cooperation rather than
competition would be a natural consequence. Fighting ‘spiritual wars’ does not make sense.
A survey done on eleven different sample groups in the USA called “Unfuzzing the
Fuzzy”20, 66 (Zinnbauer, 1997) found that 74% of the participants considered themselves both
religious and spiritual; in a 2009 Newsweek survey it was 48%, while 30% said they were
spiritual but not religious. Religion and spirituality were most frequently considered overlapping
concepts yet different from one another. “It is important to use both religious and spiritual (when
implementing the FICA assessment tool, see appendix 2) because individuals may relate to one
and may even take offence at the other” (Hallenbeck, 2003).21
A national survey in Canada11 (Woodland, 2009) found that focus groups with patient
and faith community representations preferred ‘spiritual’ care to ‘pastoral’ care, because it
encompasses all faith/culture groups. Religion, from the Latin religare, to bind together, means
‘relating to or manifesting faith and devotion to an acknowledged God/deities/ ultimate reality’.
Religiosity can be intrinsic and extrinsic (McFadden, 1996),22, 66 traditional and non-traditional,
subjective and objective, but often religion is considered a less broad concept than spirituality. In
SHIFTS IN CHAPLAINCY 18
the assessment tool known under the mnemonic HOPE, for example, O stands for organized
religion while P stands for personal spirituality, reflecting the predominant association of
religion with a more structured belief system, institutionalized religiosity, including organized
worship and community (see appendix 2).
D. The Dangers of Interpretation
It cannot be assumed that religion always supports an integrative process of healing. Most
established religions expect adherence to a particular body of doctrines; a person’s belief system
or interpretation of the doctrine could also inflict spiritual pain: by fostering shame, guilt or a
sense of condemnation/rejection from God, Church and/or the faith community; by instilling fear
of eternal judgment/punishment; through actively or implicitly discouraging the expression of an
individualized search for meaning, including challenging questions; by judgmental attitudes
causing the suppression, but not resolution of painful and negative feelings, such as doubt, anger
at God/others/self; the experience/image of God/Church/community as distant, punishing, rigid,
hypocritical versus personal, forgiving, open, supportive.19
Without reiterating what was said earlier concerning the ancient struggle between
theology and science, ‘religion’ for some might still be associated with rigid dogma and the
persecution of anyone who dared to think outside of it, including Christian Gnostics and Mystics
burned at the stake. Fortunately, the Holy Office of the Inquisition, renamed in 1908 and since
1965 the Congregation for the Doctrine of Faith, honors the spiritual disciplines of the Desert
Fathers, John of the Cross, Thomas Kempis, Thomas Merton and Thomas Keating, all of whom
emphasize a contemplative tradition, which the author believes to be of particular import for
SHIFTS IN CHAPLAINCY 19
chaplains of all faiths. In the words of Mother Teresa: “We maybe doing social work in the eyes
of some people, but we must be contemplatives in the heart of the world.”23
E. Expanding Chaplaincy Services
Recently the proportion of patients choosing to receive spiritual counseling and the new
chaplains entering the field to meet the need have risen sharply. Chaplains’ services in New York
nearly doubled since 2004. 65% of New York’s 4000 hospice patients accept visits from
chaplains compared to 35% four years ago1 (Visiting Nurse Service of New York & Continuum
Hospice Care, 2009). A nationwide study by National Center for Health Statistics of the Centers
for Disease Control set the proportions of patients accepting a chaplain’s care at 72% in one
sampling compared to 59% in 2000. According to Josephine Schrader of the Association of
Professional Chaplains, an estimated 3,000 chaplain representing a 50% increase, have been
working in hospice care in the last ten years1. There is a shortage of clergy and a decline in
traditional worship, but the need for most people near the end of life to make sense of existence
remains unchanged. Chaplains now need the ability to be a partner in existential discussions,
address psychosocial issues, and all the while not neglect their training to respond to spiritual and
religious matters.
IV. A Science Friendly Chaplaincy: Implementing Spiritual Assessment Tools
A. Holistic Medicine
There are two main reasons why there has been a dramatic growth in the number of
empirical studies to clarify the relationship between spirituality / religion and medicine over the
last few decades24. First, the renewed interest in holistic medicine, and second, the fact that
health care facilities have to justify the expenses for spiritual care practitioners. The research
SHIFTS IN CHAPLAINCY 20
provided consistent proof that spiritual well-being is an essential aspect of wellness and a
determinant of health. The Royal College of Psychiatrists in Britain state, “Evidence for the
benefits for mental health of belonging to a faith community, holding religious or spiritual
beliefs, and engaging in associated practices, is now substantial.” “It is safe to say that over one
thousand research studies have quantitatively examined relationships between
spirituality/religion and health, many reporting positive findings… It is time to move forward in
addressing the split between science-based medicine and the more holistic understanding of the
person in the body.”25, 66
The holistic (etymologically the same root as whole, health, heal, holy) perspective, akin
to systems theory, emphasizes the interrelationship between parts and the whole. Holistic
medicine sees the physical body (Greek: soma) as one integral system within the higher-level
system, the wholeness of a human being. As in psychosomatic medicine body and mind are
recognized as affecting each other, corresponding to the common element of all systems, which
is: knowing one part of a system tells us about another part. Treatment cannot only be aimed at a
set of symptoms, psychosocial, spiritual as well as behavioral and environmental factors impact
dis-ease and well-being of a ‘patient’ (etymologically ‘the bearer of suffering’). The National
Health Service (NHS) in Britain recognizes in its guidelines for staff that “a person’s spiritual
dimension is one of the most vital aspects of care and recovery in mental health”.
It is regrettable, but understandable that the chaplain’s vocation suffered devaluation
during the age of Enlightenment. Descartes presented his dualistic metaphysical belief in res
cognitas (mind) and res extensa (matter/body) in 1641, but separating body and mind has long
had other philosophical and religious roots as well. In any case, reductionism, reasoning and
scientific method have certainly led to many vital discoveries and science-based medicine will

SHIFTS IN CHAPLAINCY 21
continue to make valuable contributions, such as finding new cures. Although there are parallels
in holistic medicine to ancient healing traditions, which sometimes only offered very inadequate
care, this is not a rediscovery so much as going up along the spiral to a higher level, where the
correlation of body-mind is recognized but the know-how of science-based medicine is put into
use at the same time.
B. Reasons for Using Assessment Tools
An assessment is a statement of perception and a process of information gathering and
interpretation.26 Spiritual assessment is considered a prerequisite for effective spiritual care. The
chaplain needs to understand the needs, strengths and particular issues relevant to the individual
patient, so that care can be provided where it is most needed. Both subjective statements and
objective observations indicate spiritual distress or health.
The Joint Commission on Accreditation of Healthcare Organizations (JCAHO) mandates
a spiritual assessment for clients who enter an approved facility, but does not stipulate
specifications as to how the documentation must be done;27the World Health Organization
(WHO) recognized spirituality as an important dimension in quality of life; the North American
Nursing Diagnosis Association (NANDA) lists ‘distress of the human spirit’ as a valid diagnosis,
and its negative impact on health risks has been researched.28, 29
In spite of this growing acknowledgement in the medical world of a correlation between
spirituality and health, there still is an urgent demand for research, especially with prospective,
experimental design. There are several problems to consider:
1. Even in the few chaplaincy studies undertaken, pastoral care researchers so far have
predominantly been Judeo-Christian Euro-American white males.

SHIFTS IN CHAPLAINCY 22
2. As already alluded to in the section about the theology science dichotomy, hesitations
to engage in scientific research possess deep historical roots.
3. Spiritual care practioners of any faith tend to feel that numbers, data and statistic are
alien to their way of functioning and have little to do with their ministry.
When the author’s own Clinical Pastoral Education (CPE) group at Christus St. Vincent
completed the Myers-Briggs Type Indicator test, most members including the author had the
typical characterizations of parish clergy and pastoral counselors: caring, intuitive, supportive.
Critical thinking and skeptical faculties are usually not their strength31 (Southard, 1976). We
cannot, however, keep putting other disciplines in the position of convincing critics of the
effectiveness and value of spiritual care. Empirical evidence has bearing on discussions, such as
the present health coverage debate, and could ensure that Medicare reimburses not only
consultations about end of life treatment, but also pastoral care and counseling. Hospices and
hospitals are increasingly under pressure to justify the expenses of spiritual care by
demonstrating its efficiency. It is not yet universally accepted that spirituality is a component of
a comprehensive evaluation and treatment plan. To summarize, spiritual assessment is:
• Improves the quality of spiritual care and is a means to achieve best practice
• Raises the standard of care by efficiently identifying patient’s issues so that the
chaplain can provide care where it is needed
• Means to collect outcome measures as basis for future research to advocate for
hospital chaplaincy and justify its cost
• Assessment tools fosters chaplains’ skills other than their intuition
SHIFTS IN CHAPLAINCY 23
• Assessment questions are a guide to explore essential areas and reminder of what
topics were either forgotten/avoided by the chaplain or the patient/their loved
ones
• Previous assessments serve as support for memory, acting as a reminder of the
history of a particular patient/their loved one before the follow up visit, or if a
different chaplain undertook the last visit
• Standardized way to contribute to the pool of information, facilitating and
improving communication between chaplain and interdisciplinary team
• Clarifies the role of chaplaincy in a multidisciplinary team by enhancing
understanding of the nature and function of spiritual care
• Helps in discharge planning and ensures continuity of care by transmitting
information about the patient’s history, preferences and problems when the
patient is discharged to other settings, such as a hospice. Even if new chaplains
make their own assessment, the information provided is valuable and serves at
least as a briefing and gives a sense of history.
• Assures timely gathering of information to avoid “last minute rush” in terminal
event planning
• Evidence-based spiritual care delivery plan is proposed as future model11, 17
Assessment leads to ‘mapping’. Although spiritual assessment is bound to seem like a
linear process, putting the pieces of information together is an integrative task. Slowly, the blank
spaces on a map representing the whole person are filled in. Although “the body is a sacred
SHIFTS IN CHAPLAINCY 24
garment”, as Martha Graham said, in a patient-centered holistic approach, the belief systems and
attitudes, resources and relationships, and other aspects of the person in the body are
acknowledged to significantly impact healing and recovery. “It is more important to know who
has the disease than to know the disease the person has” (Sir William Osler, MD).
C. Types of Tools
Three main types of tools are currently in use for spiritual assessment: self-assessment,
quantitative and qualitative assessment.
i. Self-Assessment
A spiritual self-assessment form (see appendix 1) could be handed out as part of the
standard procedure for newly admitted patients once they are settled in their rooms. The form
could be collected and deposited in a designated folder at the nurse station, regularly emptied by
the chaplaincy service. The self-assessment sheets can never replace human contact, but it can
serve to glean substantial information that helps to determine priorities in the chaplains’ visiting
schedule. In view of the fact that spiritual assessment is often overlooked during the current
screening protocols administered in hospital settings, self-assessment forms represent another
opportunity to identify patients who suffer from spiritual distress.
However, self-assessment is unsuitable for palliative care patients, because often they
already suffer from exhaustion and confusion. Ideally, all patient in palliative care service should
receive a personal visit by a spiritual care practitioner, even if no specific demand for chaplaincy
services has been made.

SHIFTS IN CHAPLAINCY 25
ii. Quantitative Assessment
Quantitative assessment mostly takes the form of a checklist. After visiting with a
patient/their loved ones, chaplains put their check marks on an assessment form (often already
part of the electronic files) based on the information and impressions gathered during the
interaction. Quantitative data is important for a scientific study because it is easy to measure in
contrast to information gathered during a qualitative assessment. Although this assessment is
convenient and quick it remains superficial being limited by its mechanistic rigid nature; it
cannot be individualized. The chaplain cannot go into detail; little space is available to comment
on observations of non-verbal communication, such as tone of voice, timing, mimic and other
body language. As psychologists know, gathering this information is as relevant as the spoken
word in order to arrive at a valid diagnosis, especially when dealing with such subtle phenomena
as in spiritual assessment.
iii. Qualitative Assessment:
(a) The Back-up Narrative
A descriptive narrative should back up all ‘checklist’ assessments, unless there are severe
time restraints or one collects exclusively quantitative data for a research project. This qualitative
assessment sums up the chaplain’s visit, highlights information and explicitly communicates
latent messages, patterns and non-verbal language that cannot be conveyed by the checkmarks of
a quantitative assessment. The narrative validates the chaplain’s judgment and allows others to
follow and understand how specific conclusions were reached. The descriptive narrative the
author submits to Mrs. San Luis to report on palliative care patient visits include headings such
as family and spiritual history, issues, intervention, analysis and recommendations.
SHIFTS IN CHAPLAINCY 26
(b) Structured Qualitative Assessment
A structured qualitative assessment uses a specific set of questions, sometimes known
under mnemonics like HOPE32, FICA33ab or SPIRIT34 (see appendix 2). They give a structure to
the interaction between the chaplain and the patient/their loved ones, which facilitates the
documentation of preferences and needs, for example, the patient’s faith denomination and
personal practices, their impact on health care decisions and terminal events planning. Optimal
practice would be to keep note taking to a minimum while with the patient. After the visit,
however, a descriptive narrative needs to be written to sum up the interaction and communicate
relevant information.
(c) Unstructured Qualitative Assessment
This interaction is not structured by a set of preconceived questions and therefore is
unpredictable. The chaplain accompanies the patient, but does not take the lead. Open-ended
questions are only asked if deemed necessary to support the patient in the telling of his/her story.
A comprehensive spiritual assessment will always require either a structured or
unstructured qualitative assessment, because the phenomena dealt with are abstract and subtle in
nature. As will be discussed in the following ‘outcome measure’ section, the Support Team
Assessment Schedule (STAS) is an attempt to measure the increase of acceptance and decrease
of distress by using a 5-point Likert scale. But to quantify the amount of opening to a higher
perspective, finding meaning etc. will always remain a somewhat elusive goal.
Lynda Mainwaring35 lists different assumptions of the two paradigms underlying
quantitative and qualitative research:

SHIFTS IN CHAPLAINCY 27
Principles of logical positivism underlying quantitative research:
• Reality can be objectively determined by empirical observations
• Causality is linearly determined
• The hypothethico-deductive system of theory testing can lead to theory verification or
disconfirmation.
• Generalization can be established through induction.
Qualitative research:
• Individuals describe reality by reference to their conclusions based on the structure and
function of mentation.
• The observer and observed impact one another.
• Investigations, including scientific investigations, are value-laden.
• Meaning is a social, linguistic, historical, cultural, and contextual product.
• Chaplain and patients are both active agents.
iv. Outcome Measure Tools
Chaplains are part of multidisciplinary care teams and, like the rest of the hospital staff,
are not exempt from accountability. Feedback from patients/their loved ones, including the
subjective assessment of their own satisfaction (‘I felt the chaplain cared about me’) and the
objective characteristics of care (‘I received the follow up visit I had requested’) are valuable in
as much as they accurately (Bell & Davis, 2000) point to areas in which the quality of care can
SHIFTS IN CHAPLAINCY 28
be improved. Just as the consumer movement of the 1970’s demanded accountability of service
providers, measuring outcomes will contribute not only to acknowledging the significance of
spiritual care, it is also a learning tool for chaplains on how to increase their effectiveness.
Implementing outcome measure tools at a hospital, for example Christus St. Vincent,
would require approval from the administration, the spiritual care department and the ethics
committee. Samples would need to be diverse in terms of religious affiliation, ethnicity, gender,
age and if possible even in social standing and profession.
Here are three ways to obtain outcome measures:
1. The spiritual assessment tool itself automatically becomes an outcome measure tool
when it is implemented over a certain period of time. Compared to the data collected (from
patients’ answers) at the intake assessment, how do the results differ three days later, one week
later, or on the day of discharge? In simple terms, if fewer areas of spiritual distress and more
sources of strength are marked on the quantitative assessment form, or the end of life reaction is
identified as acceptance rather than anger, this indicates a subjective increase in the quality of
life.
2. After each assessment the chaplain evaluates the result by using a outcome measure
tool to arrive at a quantitative measurement. The Support Team Assessment Schedule36ab, 66
(STAS), for example, implements a 5-point Likert scale. The STAS was developed to audit care
given by palliative care teams by assessing 17 core items. The 5-point Likert scale to assess
spirituality is one of these core items:

SHIFTS IN CHAPLAINCY 29
Spiritual: Degree to which the patient is content with their own spiritual beliefs or philosophy.
0 = content in self and worldview, without feelings of guilt or punishment over illness.
Any denomination or agnostic.
1 = Occasional doubts or unrealistic expectations. Patient able to resolve feelings /
problems themselves.
2 = Uncertain, sometimes troubled. Doubts. Patient unable to resolve their feelings /
problems themselves.
3 = Uncertainty and guilt. For example troubled, conflicts, worry.
4 = Distraught with uncertainty or guilt over beliefs. In chaos as to how to remedy
situation. Crisis, unable to resolve things, inability to cope, symptomatic
(physical/emotional).
Other core items chaplains could assess include: patient anxiety, family anxiety,
professional (of the multidisciplinary team) anxiety; patient-family communication,
communication from professionals to patient and family, communication between professionals;
patient insight (awareness of prognosis), family insight; planning (of patient’s affairs), practical
aid (after discharge).
(c) To collect more data about the effectiveness of spiritual care, an evaluation form
could be handed out before discharge. Patients/their loved ones may be asked to put a checkmark
next to the response that most describes their experience. After each statement 5 options are
offered: strongly agree, agree, disagree, strongly disagree; the 5th option is ‘non applicable’.
SHIFTS IN CHAPLAINCY 30
The chaplain introduced him/herself.
I felt the chaplain cared about me.
I felt the chaplain was trustworthy.
I felt heard and attentively listened to.
I was comfortable to talk freely because I did not feel judged.
I had moral support / was supported in my spiritual/religious practice.
I felt empowered to explore my inner strengths.
The chaplain respected my wishes/opinions/beliefs.
The chaplain provided care in a thoughtful and sensitive manner.
The chaplain did not turn away when I expressed my fears/doubts/concerns/anger.
Receiving spiritual care made hospitalization easier.
I felt I had enough time with the chaplain.
I received the follow up visits I had requested.
The chaplain left a calling card.
The evaluation form could end by: Was there something the chaplain did you particularly
liked or disliked? How can chaplains better serve future patients?
A more detailed methodology can be found in ‘The Correlates of Chaplain’s
Effectiveness in Meeting Spiritual/Religious and Emotional Needs of Patients’, Flannelly et al.,
SHIFTS IN CHAPLAINCY 31
200937. The referral rate to chaplains and rate of completion of spiritual assessments lend
themselves to quantitative measurement and indicate increase or decrease of the use of spiritual
care resources.
Other facts indicative of the patient’s comfort and worth monitoring include: fewer calls
to nurse, less pain medication, increased healing rate as measured by length of stay, fewer
lawsuits filed against hospital.
D. Bias and Limitations
Chaplains themselves function as much as a research instrument as the questionnaires,
but they are not objective. The cognitive mechanism by which the chaplain tries to makes sense
of the patient’s affect, behavior and conduct is biased. A chaplain tries to communicate his/her
understanding to another reader through placing a checkmark or attributing numbers
(quantitative assessment) or through a narrative (qualitative assessment). But either assessment
can only approximate the human experience, it is never truly empirical, only a relative analogy
of what a human experience meant to the chaplain.38 Even a questionnaire does not provide pure
quantitative data. It can be quantified by counting the check marks, but in pure quantitative
research the researcher always remains outside and separate from the object under research. Even
when using a validated outcome measure tool, the chaplain’s evaluation may consciously or
unconsciously have a self-serving bias. Therefore critics will always demand studies with a true
experimental design demonstrating empirical outcomes.
The statements made by patients might be considered to be subjective in contrast to the
objective observations of the chaplain, but of course any observation is tainted by the chaplains’
own filters of perception. As in other fields of scientific enquiry, which have had to contend with

SHIFTS IN CHAPLAINCY 32
the observer effect, the chaplain as participant in the interaction with a patient is also a
contaminating factor in objective research. The chaplain is not only an observer but an active
agent in the exchange. The chaplain’s presence, words and behavior all convey messages and
impact the interaction. It is only an assumption that patients will freely provide an objective
evaluation. In fact, they have little energy, are in a dependant situation and most likely will give
what they believe are the expected, socially acceptable, polite answers. This tendency even gets
aggravated in a relationship that in any case is marked by a power imbalance, when the chaplain
is idealized and perceived as an authority figure. This is the reason why it is so essential that
chaplains earn trust and make patient feel comfortable enough to speak openly and honestly.
Even with the greatest care, each patient’s criteria will vary as to how they evaluate care.
Their positive or negative impressions may not be based on objective characteristics of care, but
be influenced by the chaplain’s personal faith, gender, age, appearance or any number of other
variables. Quantification of outcomes will always be a challenge in spiritual care, because the
nature of the phenomena dealt with are of a subtle existential or spiritual nature. How can one
precisely quantify the reconciliation with God, the relief of suffering, the degree of forgiveness
or how much one has found meaning in life or the illness?
E. Processes of Assessment (Using the example of Christus St. Vincent)
i. Screening
At a desk in the main entrance for Christus St. Vincent patients are listed according to
spiritual preference. Both the Catholic Father and the Rabbi use this as prime resource in
planning their daily visiting schedules. However, the three folders labeled “non-preferential”,
“non-denominational” and “other” are consistently the most voluminous. The author was told
SHIFTS IN CHAPLAINCY 33
this actually indicates that the basic spiritual care question - to determine a person’s religious
affiliation - is overlooked in the screening / triage process, maybe because medical staff already
carried a heavy workload. For the same reason chaplains often are unable to greet all newly
admitted patients, which is regarded as optimal practice, even if a patient has not made the
formal request for a visit. This is in accord with the Association of Professional Chaplains’
recent encouragement to chaplains to assume a more proactive stance toward patients and initiate
conversation. It follows that although new admissions is an opportunity to identify patients
suffering from spiritual struggle or otherwise in need of a chaplain’s visit, a person could easily
be overlooked and might be difficult to identify later.
Undervaluing spiritual care is one of the barriers for implementing a screening protocol.
Medical staff can be sensitized to the importance of including spirituality/religion in screening,
in order to identify patients who need support at this vulnerable time. One possibility is to offer
education about the great body of research documenting that spiritual/religious struggle is a
significant predictor of harmful effects, including increased mortality and disability, greater
depression, poorer quality of life, physical health and recovery.39 Hospital administrations might
also be interested in research demonstrating that chaplains help to reduce medical costs while
improving patient satisfaction, which results in giving higher ratings to the hospital.40
Screening does not leave time to ask open-ended questions. The goal is to quickly
identify patients who might benefit from a chaplain’s visit. Determining the person’s religious
affiliation may be necessary, but it is not enough. Suggestions:
1) “Do you have a faith or philosophy of choice that gives your life meaning?”
Formulating the question in a more inclusive way might result in also recording people
SHIFTS IN CHAPLAINCY 34
who do not feel affiliated with institutionalized religion. If self-administered, options
beside major world religions should be included.
2)“Has there ever been a time when spirituality or religion were important to you?” A
“yes” to this second question would signal that a chaplain’s visit is appropriate. If a
person feels that his or her faith is not working for them as a resource at present, but
spirituality or religion played a role at some point in their life, spiritual distress may be
indicated and referral to a chaplain appropriate.
When these two spiritual screening question are consistently administered (and the
folders labeled ‘no preference’, ‘no denomination’ and ‘other’ have hopefully become less
voluminous) Christus St. Vincent could then consider the regular use of the spiritual screening
tool recently published by Fitchett and Risk41 (see appendix 4). Once the patient is settled in
his/her room, medical staff can easily administer this protocol to identify patients, who may be
experiencing spiritual struggle or would welcome a chaplain’s visit for other reasons.
ii. Structured Quantitative Assessment
Health care facilities often issue their own quantitative assessment form for internal use.
Chaplains are instructed to put their check mark next to the item that best describes their
judgment. An example can be found in appendix 5.
iii. Structured Qualitative Assessment:
Using as example the author’s “The Integrative Assessment Tool” (Appendix 6)
“Follow Me, and I will make you become fishers of men” (John 21:17). Assessment must
be done in a way that ‘casts the net’ as wide as possible. “The Integrative Assessment Tool” was
SHIFTS IN CHAPLAINCY 35
created by the author as a sensitive method aimed at identifying spiritual distress and coping
skills of as many patients as possible, independent of their faith or lack thereof. Although
patients in the United States will predominantly be Christian, the word “God” does not appear
explicitly. Instead, a more inclusive language is used in order to encompass both vertical
(concerned with relationship to God and concern in earthly activities affecting an afterlife) and
horizontal belief systems (concerned with social relationships and a concern with the effects of
activities in the community).42, 66 In this way the tool is not overtly religious but does not exclude
religion either.
The questions offer a framework eliciting thoughts, memories and experiences that give
coherence to a person’s life, and help locate their source of strength or distress (be it
intrapersonal, interpersonal or transpersonal). The hope is that patients will be encouraged to
name anything that lends support at this vulnerable time and to have their needs (identified in a
previously mentioned study) met: to feel free to express true feelings without being judged, to
speak about important relationships, to discuss unresolved issues, to have time to prepare for
death. The other research cited in the discussion under the heading ‘A Shift in Chaplaincy’
demonstrates that patients’ questions mainly pertained to general existential issues; only 8%
were overtly religious in nature. This is reflected in the author’s ‘The Integrative Assessment
Tool’. At the same time ‘The Integrative Assessment Tool’ covers what Stoll43 describes as the
four essential areas for spiritual assessment:
1. Concept of God/transcendence
2. Source of hope and strength
3. Religious practices
SHIFTS IN CHAPLAINCY 36
4. Relationship between spirituality and health
On one hand, the set of questions in ‘The Integrative Assessment Tool’ help the chaplain
to effectively collect objective data, such as faith denomination and the impact of the patient’s
faith on medical care. On the other hand, and in contrast to most existing tools known to the
author, ‘The Integrated Assessment Tool’ focuses on deeper more subjective data. The set of
questions provide a framework for the chaplain and the patient to explore the two basic
categories of spiritual assessment:
1. Functional information, the ‘How’ of spiritual life, because most people can relate
to these common human quests, even if the patient has found no answers:
(cognitive) search for meaning/ purpose; (experiential) feeling
hope/joy/peace/comfort; (relational) relationship between health and
beliefs/practices; relationship to family/ friends/ community; coping skills.
2. Substantive information, the ‘What’ of spiritual life: past spiritual/religious
background and present spiritual/religious affiliation; beliefs about self/others/
transcendence; present personal practices, rituals, faith community; the level of
involvement/support they provide.44
The ‘Integrative Assessment Tool‘ also contains a section for palliative care patients to
address end of life planning. These questions aid the chaplain and patient to explore subjects
such as end of life reaction, terminal event arrangements, afterlife beliefs and reconciliation with
self/others/Spiritual Source.
SHIFTS IN CHAPLAINCY 37
Instruction to the Chaplain on how to use ‘The Integrative Assessment Tool’:
• Chaplains can use ‘The Integrative Assessment Tool‘ as a guide to support them
in conducting semi-structured interviews. Not all questions have to be asked; they
represent available options for the chaplain to invite reflections, memories and
stories, slowly mapping this individual’s resources and the barriers to using them.
• The author assumes the religious denomination has already been determined
during the screening protocol. This information, together with answers about faith
community and who the patient would like to contact to talk with about religious
or other matters, will come up naturally as the chaplain poses the questions that
explore resources and how the patient finds meaning.
• Besides establishing rapport and trust in whatever way is appropriate, chaplains
need to determine how best to preface the questions themselves. For example, by
beginning with “If you are comfortable talking about this topic, would you please
share some of your beliefs about…”.
• With minor modifications (not include here) ‘The Integrative Assessment Tool‘
can be used for assessing family, friends or medical staff. It is of course crucial to
follow up, explain, reassure and counsel the patient’s loved ones.
• While with the patient, it is recommended to keep note-writing to a minimum in
order to give as much undivided attention as possible to the patient. Even if notes
have to be made, the chaplain should provide an atmosphere of communion rather
than that of an interview.

SHIFTS IN CHAPLAINCY 38
Listen to where resources stem from / who or what gives meaning; listen to what might be
source of distress; listen to clues for effective interventions:
1. intrapersonal / self: recognition of positive traits, healthy self-esteem in spite of physical
disabilities, being in touch with oneself, quiet time, ability to relax, ability to tolerate stress,
ability to endure loss/vulnerability/uncertainty/ambiguity, accepts and embraces the impossibility
to find meaning, completion of tasks, finished business, feels involved in decision-making, has
some degree of control, positive outlook, gratitude, forgiveness.
2. interpersonal / relational: love, sense of belonging, closeness, closure with others,
significant other, family, friends, pets, social networks, fellowship – spiritual, cultural,
professional or other.
3. transpersonal / religious / contemplative: God, deities, ultimate reality, sense of the sacred,
set of values, connectedness with or feeling looked after by Higher Power, surrender into God’s
hands, sacred scriptures, sacraments, spiritual community, clergy, faith, worship, hymns, prayer,
guided imagery, meditation, spiritual/religious practices, rituals.
4. environmental / creative / therapeutic: experience nature, music, literature, poetry, beauty,
creating collage or other art projects, journal-keeping, life review.
THE QUESTIONS:
(a) Securing and Strengthening Resources45
(past – coping skills)
How has your attitude to life, spirituality or religion sustained you
during difficult times in the past?
SHIFTS IN CHAPLAINCY 39
What in your life has brought you joy or peace?
(present - resources)
What could nurture your inner strength or your spirit while you are here?
How does your faith, relationships or other resources you have, help you during this illness?
What can I do to make you feel more comfortable?
(future – retaining hope / goal setting)
What inspires you with hope?
What kind of goals do you look forward to? (consider short, medium and long-term goals)
(b) Finding meaning / Opening to a higher perspective
(past)
Looking back over your life, what moments, people or experiences stand out as important?
What did you consider the most meaningful things in life?
(present)
What really matters to you now?
What helps you make sense of being here?
How has your relationship changed to important things in your life?
Where does your sense of what to do, or how to look at things come from?
(future)
What is important for you to happen in the next few days or weeks?
SHIFTS IN CHAPLAINCY 40
What would help you find peace of mind?
What do you wish for?
(c) Impact on Medical Care and Decision Making46
How do your beliefs influence the way you think about your health?
How do your beliefs influence how you look at your disease?
How do your beliefs impact your decisions about your treatment and medical care?
What would you like your caregivers to know and pay special attention to?
(d) Special Considerations
TV on/off, curtains open/closed, lights bright/soft, temperature higher/lower, frequency of
visitors more/less, display of religious or cultural symbols, personal photo frames, flowers, wall
decoration, special blanket and other personal items, CD player, DVD player, writing or art
supply, room with a view of sky/mountains if desired and possible.
(e) Cultural / Interfaith Considerations
Interfaith and cultural considerations become particularly important toward end of life and
require awareness of the chaplain’s own ethnocentricity. Although it is unrealistic to expect a
chaplain to be fully competent at intercultural communication skills and to know the customs,
taboos, etc. of all cultures, an effort in behavioral flexibility and interfaith education has to be
made to avoid major missteps. It might be helpful to solicit the patient/their loved ones as
teachers regarding faith/cultural practices by saying, for example, “I am not very familiar with
your culture / faith, could you help me understand…”.

SHIFTS IN CHAPLAINCY 41
Christus St. Vincent and other hospitals have interpreter services available. The spiritual care
department is at present working on the compilation of an interfaith prayer book. To learn how to
navigate today’s pluralistic society and religious landscape see P. Fosarelli’s ‘Prayers & Rituals
At a Time of Illness and Dying’47 and other book recommendations.48, 49
(f) End of life Planning
As mentioned previously, with some modification – not included here - the same questions can be
used to assess the patient’s loved ones.
Care:
How do your beliefs impact your hospital care, treatment or medical procedures?
What aspects of your religion or spirituality might impact how you would like
– or would not like to be cared for?
Do you have an advanced directive to let caregivers know what treatments you wish them to
withhold?
What would you like your caregivers to know and pay special attention to?
Regrets / Forgiveness / Closure:
What do you feel you have lost in the course of this illness?
Is there any kind of “unfinished business” you would feel comfortable sharing with me?
If you had your life to live over – what would you like to be the same
and what would you like to have done differently?

SHIFTS IN CHAPLAINCY 42
In terms of your relationships (or whatever issue causes distress) – what would you like to be the
same and what would you like to have done differently?
Whose visit would mean a lot to you now?
Are there people you would like me to contact for you now, even if you have not seen them in a
long time? (For example, to say that you forgive them, or to ask for their forgiveness)
Are there people who you would like to call and come visit
(so that you can say ‘good-bye’ and ‘I love you’)?
How can I support you in finding a sense of closure as you approach the end of your life?
Even if your body should not get cured, what would help you now to find peace of mind?
Life review
What would you say were ‘the milestones’ in your life?
Would you be interested in drawing or writing a timeline of your life (or spiritual history)
including remarkable encounters and important events?
Some say “wisdom is what floats to the top like cream after a rich life” – What kind of wisdom
or legacy would you like to share or leave behind for others?
Would you like to tell me about X as a person?
Preparation:
Where would you like to die?
What does death mean to you?
SHIFTS IN CHAPLAINCY 43
What does it mean to you that this is happening?
Actual death:
What is important about how others will care for your body before and after you die?
What is important about how others conduct themselves at time of your death?
What specific instructions do you have about the care of your body after you die?
Funeral arrangements:
Where and how would you like to be buried or cremated?
What kind of ritual or funeral service would you choose?
Is there someone special you would like to officiate?
Is there something special you would like to be said at your funeral?
After death / Afterlife:
How do you want to be remembered?
What do you believe happens after death?
If your health should decline, how does your faith - or other resources -
prepare you for what is ahead?
‘The Integrative Assessment Tool‘ can be found in appendix 6.
iv. Unstructured Spiritual Assessment
This in-depth assessment does not use a specific set of questions to structure the
interaction between chaplain and patient. Mastering ‘the art of non-interference’ and the

SHIFTS IN CHAPLAINCY 44
chaplain’s ability to let go of control are prerequisites. The unstructured interaction consists of
active listening to the patient’s story and - without manipulation - following his/her lead as it
unfolds. By conveying attentiveness, genuine empathy and a non-judgmental attitude, the
chaplain him/herself becomes the instrument to facilitate the expression of thoughts and feelings
in verbal and non-verbal ways; they are allowed to surface, are validated and may or may not
need to be named.
V. Palliative Care Chaplaincy
The historical relationship between spiritual and palliative care goes back to the Middle
Ages when monasteries offered hospitium, a safe resting place for weary, and sometimes dying,
travelers. The ancient monks’ mission was to save souls. Although today’s standards of spiritual
care reflect the change the role of chaplain has undergone over the centuries, the mission of both
spiritual and palliative care remain the same: to make dying easier.
The medical profession still treats its role as an art as much as a science, relying on
philosophical principles like the rule of double effect, attributed to the 13th century
Roman Catholic philosopher Thomas Aquinas. Even if there is a foreseeable bad
outcome, like death, it is acceptable if it is unintended and outweighed by an intentional
good outcome – the relief of unyielding suffering before death.50
One provision of the House health care bill passed in November 2009 recognizes that
palliative care may include treatment “furnished for the purpose of alleviating pain or
discomfort, even if the use may increase the risk of death.” Constant vigilance concerning abuse
is appropriate, for example to monitor whether terminal sedation is administered because of
pressure from family, economic reasons or out of convenience. The Institute for Healthcare
SHIFTS IN CHAPLAINCY 45
Improvements (IHI) lists “learn how to provide care that is death accepting” as optimum practice
in their recommendations.51 Ars moriendi, ‘the art of dying’ (a term originating in the Middle
Ages) in modern times could refer to palliative care efforts to restore death to its sacred or
significant place, in contrast to it being a technological or management issue. Florence
Nightingale reintroduced the notion of holistic care in the 19th century. The Sisters of Charity,
the same Order that established St. Vincent in New Mexico in 1865, opened the first hospices in
Ireland and France. Dame Cicely Saunders was a key figure from the 1940’s onward and
pioneered the hospice movement in England. In the USA Elizabeth Kubler-Ross captured the
interest of a large lay audience with her research on the stages of dying. Between 1986 and 1996
the Elizabeth Kubler-Ross Institute in El Rito was part of the Northern New Mexico College. For
linguistic reasons, the French Canadians chose to name their hospice service in Montreal
‘palliative’ care when it was established in 1974 (palliative from Latin palliare, to cloak or
cover; care that palliates, i.e. alleviates or relieves suffering).
The author’s ‘Integrative Assessment Tool’ contains an ‘end-of-life planning’ section. It
takes into consideration the particular concerns of palliative care patients and helps the chaplain
to address them in a sensitive manner. Palliative care chaplains explore the patient’s/their loved
one’s beliefs about death and afterlife, how these affect medical decisions, such as organ
donation and blood transfusion. They may have to lend their support to discuss an advanced
medical directive, including DNR (Do Not Resuscitate order), and the patient’s preferred site of
death.
But besides assuring the collection of essential information, the ‘Integrative Assessment
Tool’ could also point out areas a chaplain avoids consciously or unconsciously, because of
his/her own unease with the subject. This can occur due of a lack of self-knowledge, for

SHIFTS IN CHAPLAINCY 46
example, if chaplains have not explored their own hopes and fears about what a ‘good death’ or
‘bad death’ might mean for them; attitude and issues concerning mortality, loss of control, etc.
Self-knowledge is an essential prerequisite for a chaplain to use assessment tools in general and
in palliative care in particular.
Many examples of empirical research studies have already been cited in this document
showing that patients, especially those in palliative care, feel spirituality is one of the most
important contributors to their quality of life and strongly desire it to be included in their care.
Further research affirms that questions of a spiritual nature - Who am I? Is there a meaning to
life? - arise around the teenage years and stay prevalent into the early 20s. They are mostly put
aside when time and energy is dedicated to building a career and founding a family. However,
these concerns resurface and become a vital focus again when a life threatening illness is
diagnosed or a person approaches the end of their life. This renewed urge to reconnect to one’s
spiritual ‘roots’ and to explore these profound questions has to be satisfied by chaplains being
integral part of all interdisciplinary palliative care teams.
The chaplain’s presence could be of pivotal importance for people who experience the
crisis as an opportunity for spiritual healing, growth or transformation. Both the spiritual and
psychosocial dimensions of dying are within the scope of a chaplain. Most patient benefit from
support in dealing with end of life reactions, including: anger, feeling like a burden, the change
and loss of virtually everything familiar and dear, self-image, social station etc., issues of
forgiveness and reconciliation with oneself, an estranged friend / family member / Spiritual
Source. All these are prominent needs and exploring them might well be a prerequisite for being
at peace and dying in peace.
SHIFTS IN CHAPLAINCY 47
Spiritual well-being stands in inverse relationship with desire for hastened death, suicidal
ideation and hopelessness. Research has already cited demonstrated religion and spirituality to be
a crucial coping skill protecting the patient against end of life despair and that spiritual care
greatly comforts terminal patients. Early referral is a major factor in successful intervention. It
takes time to establishing rapport and trust. One of the most important things a chaplain can
convey is that he/she is not in a hurry, that this meeting is the most important and precious thing
to do at this moment. Exploring spiritual pain is not done quickly. Dame Cicely Saunders
concept of ‘total pain’ emphasizes that the patient’s mood, morale and the meaning pain has for
the patient all modulate the experience of pain. Spiritual interventions such as gathering of loved
ones the patient wishes to take leave of; finding closure through reconciliation; a life review,
spiritual genogram and other creative tools for the reframing or renovation of experience all take
time and must not be rushed. Yet, decline is often rapid, as in advanced cancer, and energy and
clarity of mind are quickly lost; functioning becomes slower and spiritual work might become
difficult to master. Especially for palliative patients and their loved ones time is of the essence
and early referral to spiritual care is vital.
Most Americans would prefer to die at home,52 but an analysis of Medicare recipients
shows that up to 85% die in hospitals or nursing homes.53, 54 In hospital settings medical staff is
often pressured by understaffing, limited budget and management demands. If not trained in end-
of-life care, a professional attitude to medical care could mean one that is based on facts, but
does not necessarily consider the emotional impact of giving bad news for example. The
conventional curative model places emphasis on technology, quantity of life, curing at any cost.
Patients, even when close to death, might still be intubated, ventilated and monitored by
machines. The palliative model and holistic medicine integrate spiritual care and promote a

SHIFTS IN CHAPLAINCY 48
person-centered approach. This means services are people oriented, centering the patients’
experience more in terms of human relationships and quality of life, rather than only medical and
physiological issues. With holistic care it is possible for a dying patient to feel comfortable and
experience healing, even if the illness cannot be cured.
As previously mentioned studies have demonstrated, prevalent needs of palliative care
patients include: to have time to think, to resolve ‘unfinished business’ and to prepare for death.
There does not seem any reason to delay referrals other than misconceptions about the role and
function of palliative of which spiritual care is a very important component. In recent public
debates over the House health care bill, which allows doctors to be reimbursed for discussions
with patients about what treatments they would want or decline, some Republicans charged that
‘death panels would decide who deserves to live or die’.50 Another misunderstanding is that not
prolonging life artificially equals euthanasia. In fact, providing high quality palliative care,
including pain management and spiritual care, results in patients feeling more comfort and the
wish for a hastened death diminishes.
Considering that the average stay of people in hospice unfortunately still only averages
one week,55, 66 it is imperative to continue educating medical staff about why early referrals to
both palliative care and spiritual practitioners make a big difference for the patient’s well-being.
No harm can be done: A chaplain recognizes when the moment it is not right and will not impose
his/her visit; and it is always hoped that patients will graduate from hospice. Early referral also
impacts the patient’s family and friends because bereavement support needs to start prior to the
death of the patient. Family can also benefit by trained chaplain assisting them to make difficult
decisions by being coached in the 4 bases of ethical decision-making: autonomy, non-
maleficence, beneficence and justice. An optimal practice for all hospitals, including Christus St.

SHIFTS IN CHAPLAINCY 49
Vincent would be a as a matter of course to include a chaplain’s visit to all palliative care
patients on a daily basis, and to continue offering education on the benefits of both palliative and
spiritual care.
VI. Chaplaincy Skills and Challenges
Even when adequate assessment tools are available and consistently implemented, the
main tasks for chaplains remain: to learn how to use these tools properly. This is actually not a
question of acquiring a new technique. The chaplain him/herself serves as an instrument and is
an active agent impacting the exchange. It is therefore essential to cultivate this awareness of the
observer effect and to employ subtle skills that keep the chaplain’s personal agenda to the
minimum, while he/she seeks to see through the patient’s eyes and invites the patient’s
participation to its fullest extent. Each individual chaplain has to find ways to elevate ethical
awareness, deepen self-knowledge and increase the capacity for empathy and compassion.
A. Listening and Communication Skills
Both structured and unstructured spiritual assessments require subtle listening and
communication skills to be of real value. Most communications occur nonverbally. Studies show
that mindfulness, developed through contemplative practice for example, enhances a person’s
ability to pick up subtle changes in body language and mimic, and will therefore help a chaplain
to notice indirect non-verbal clues and latent messages. The chaplain must observe the ABC of
affect, behavior, communication, and consider whether all three elements are coherent. When a
patient says, “ I am fine” in an angry or depressed tone, this is incoherent56 and if the chaplain
places a checkmark based on this “I am fine”, it will be a false assessment.
SHIFTS IN CHAPLAINCY 50
‘Why’ questions - why me? why now? - do not require the chaplain to voice an opinion,
which in fact might block the patient from a painful but necessary exploration. Not to turn away
from suffering when there is no right answer, and to stay with the patient in this time of deep
inquiry and doubt is an essential skill a chaplain has to offer.
B. Silence
The chaplain him/herself embodies the spiritual assessment tool as much as the set of
questions themselves. Sometimes not questions, but a pause or period of silence is the best way
to communicate - or even better - to be in communion with the patient, for example when the
patient finds it difficult to express spiritual or existential experiences in words. Empathetic
silence can also function as an acknowledgment and convey permission to stay with a feeling or
experience. This offers far superior support than shallow council. In this case ‘being’ is more
than ‘doing’. For both patient and chaplain a pause in their interaction can serve as moment to
reflect, become aware of one’s inner state and motivation, or simply to take a deep breath.
Confused mind is sometimes like muddy water - by letting it settle it retrieves its inherent clarity.
Contemplative practice fosters the ability to abide in serenity no matter how chaotic the situation.
The Christian Desert Fathers said that ‘one who lives rightly does good even by his silence’. The
quality of silence embodied by a chaplain trained in contemplation can manifest like an island of
sanity and functions as grounding anchor for persons in distress. It might be silence, not words
that shifts energy or opens a new perspective.
Artificial silence is a different matter, especially if it is used as a barrier or is due to
lacking skill in communication. If chaplains feel anxious or are unfamiliar with silence, they
might not feel comfortable with naturally occurring pauses, and then the patient, too, will feel

SHIFTS IN CHAPLAINCY 51
awkward. Silence might be broken prematurely because of a chaplain’s own insecurity, which
then drives him/her to fill up the space of silence with words.
C. Power Imbalance
The chaplain must remain mindful of how vulnerable a hospitalized patient is. There is
no balance of power. The supine patient dressed in an open-back bed gown has to look up to us
even when we are seated. The shock of hospitalization, prolonged illness or treatment may have
drained the patient of energy. He/she might suffer from nausea or confusion or any number of
other symptoms that hamper the patient’s ability to assert his/her needs, or to enforce boundaries.
Therefore the relationship lacks equality and reciprocity, even if both chaplain and patient are
active agents and both have the potential to be transformed by the shared experience. It might
help the chaplain to remember well that one may quickly find oneself in the patient’s situation.
The ethics of reciprocity and foundation of human rights, a golden rule found in many cultures
throughout the ages, applies here, too: “Do unto others as you would have them do unto you”
(Matthew 22:39).
D. Authority
Although many people still expect and wish a chaplain to be a patriarchic authority figure
providing safety and certainty, the previously discussed shift in patients’ needs also indicate that
a growing number of patients seek chaplains as companion on their inner journeys of
exploration; someone who supports a positive outlook, but also listens and reflects without
judgment when doubt and the dark side of human nature is expressed. A chaplain could use the
authority invested in him/her to empower the patient, to make him/her feel involved and in
control as much as possible; these are researched patient priorities.

SHIFTS IN CHAPLAINCY 52
E. Intimacy
Talking about one’s spirituality can be as intimate as revealing matters pertaining to
sexuality. Even if the chaplain is willing to acknowledge and respect an individual’s sexuality
and faith, the depth and value of an assessment depends on the degree of rapport he/she is able to
invite. The chaplain’s inner fortitude and non-judgmental openness creates a safe space and
consequently the patient might feel comfortable enough to reveal such intimate information, and
maybe talk about the causes of his/her suffering. However, the chaplain must also be sensitive
enough to recognize if the time is not ripe and when trust has to be earned. The chaplain’s care
might be rejected and he/she must have matured inner confidence enough not perceive this as a
personal failure, especially if another caregiver receives the gift of intimacy right away. Who a
patient chooses as collaborator in this journey of discovery is not necessarily a reflection on the
competence of the chaplain, and it may change from day to day.
F. The Midwife
The patient him/herself might find it difficult to articulate his/her needs or recognize the
potentially transformative relationship to loss or any form of change. Sometimes, the chaplain
acts like a midwife57 attending to, but not initiating the process when a patient’s new insight into
the spiritual dimension of disease is born. Unlike a midwife, the chaplain does not know for
certain what the outcome will be, and needs to guard against expectations. Like a midwife,
journeying with the patient is easier if one already has some personal experience of the territory;
the chaplain benefits from his/her own lived experience of personal growth through crisis, when
for example an illness acted as a wake up call and became a turning point in life. Change occurs
SHIFTS IN CHAPLAINCY 53
despite our resistance, and to discover an ending transform into new beginning, can be like a
rebirth after emerging from the dark night of the soul.
G. Wounded Healer in a Valley of Shadows
The chaplain’s task is to follow the patient as his/her complex world unfolds, even if the
journey leads into a ‘valley of shadows’. Without extensive self-knowledge the chaplain will not
be able to resist the urge ‘to quickly fix the problem’ or ‘make light of it’, both a manipulation to
reach higher ground and escape the unease. The Christian Desert Father’s advice was not only
“stay silent and don’t judge others’, but also ‘meet your own thoughts and feelings in your heart
and to look the vices in the face’.58 Spiritual care often is an opportunity ‘to be with’ not ‘to do
for’. It also demands resilience ‘to sit in the fire of the charnel ground’ until the patient
him/herself does - or does not - move on. Victor Frankl59 was a living example how it is possible
to find meaning in all circumstances, even as a Jewish detainee in a Nazi concentration camp.
Nonetheless, the chaplain must be honest and perceptive enough to notice whether the patient
finds meaning or closure authentically, or whether he/she is hastened toward ‘a solution that is
spoon fed’ by a chaplain driven by his/her own need to succeed in fixing problems. It is one of
the worst practices in spiritual care to unconsciously manipulate and impose one’s own need on
the patient. Besides profound self-awareness, the integration of one’s own difficult life
experiences, those that have broken one’s heart open, become a chaplain’s precious resources.
For both patient and chaplain genuine compassion can be the phoenix rising from the ashes of
suffering.
SHIFTS IN CHAPLAINCY 54
H. The Human Condition
The shared human condition, suffering and mortality forges a fundamental bond between
patient and chaplain. Commonly experienced trials and tribulations of human existence and the
awareness of death might cause a person to break out of a trance-like habitual routine, and
become a springboard to launch a patient’s quest for meaning. Again, it is not up to chaplains to
take a leading role; their service consists of making the patient feel free to explore at will and to
arrive at their own conclusions. This could be the realization that all the person has is the here-
and-now; the discovery of a transcendent realm of being; to make a leap of faith and put
him/herself in the hands of God; or to revisit the valley of despair. Without some form of
thorough pastoral or contemplative education, chaplains will not easily respect the other person’s
unique journey.
I. Knowing One’s Mind
In qualitative research there is one dialogue with the patient, but on another level there is
also the internal dialogue of the chaplain going on at the same time. Firstly, this can keep the
chaplain from being fully attentive to what the patient is saying. Secondly, humans simply are
meaning making creatures and we will immediately try to make sense of what is said. However,
the subtle skill required of chaplains is to remain conscious of how their own mind works, not to
jump to conclusions, but keep the ‘field of infinite possibilities’ wide open without narrowing
down options of interpretation too soon. This calls for patience, confidence and the ability to
tolerate ‘not knowing’, uncertainty and ambiguity. Training one’s mind not to grasp at the first
available clue helps to keep a fresh state of mind and allows the chaplain to discern the
emergence of patterns more easily. This mental discipline is well described by VandeCreek60
SHIFTS IN CHAPLAINCY 55
under the heading ‘how the researcher thinks’: “…one can abandon oneself totally into the
present experience rather than holding onto the security of previous definitions. The researcher
can also learn to endure the ambiguity of the undefined experience longer, more confidently
without premature rushing to the surface for the security of a defining name.”
VII. One Objection to the “Consensus Conference Report”
“All trained health care professionals should do spiritual screening and history taking.
These caregivers should also identify any spiritual diagnoses and develop a plan of care.
Detailed assessment and complex diagnosis and treatment are the purview of the board-
certified chaplains working with the interprofessional team as the spiritual care experts.”
This is one recommendation listed in the Report of the Consensus Conference to improve
the quality of spiritual care.61 The consensus report panel outlined a three-tiered model for
spiritual assessment. As for the first tier, screening, which is a short routine triage administered
by medical staff, the consensus report and this document agree. Screening protocol options and
improvements have been suggested earlier in this document. Also, the ‘unstructured spiritual
assessment’ is the same as the third tier in the consensus report called ‘in-depth spiritual
assessment’. Both describe interactions that are not structured by a fixed set of questions. The
second tier is called ‘spiritual history taking’ in the consensus report and ‘structured spiritual
assessment’ in this document. Both refer to an interaction with the patient structured by a set of
questions, e.g. the already known assessment tools like FICA, or the new ‘Integrative
Assessment Tool’ presented earlier in this document.
In the Consensus Conference Report referral to spiritual care is only deemed necessary
for the so-called third tier, the ‘in-depth’ or ‘detailed’ assessment. The author’s objection is to
SHIFTS IN CHAPLAINCY 56
the recommendation that any member of the medical staff - not a qualified chaplain - should do
the so-called second tier, the spiritual history taking, plus the spiritual diagnosis and care plan
development. The author argues that these tasks fall into the domain of a spiritual care
practitioner. Talking about a person’s spiritual history often leads into a detailed spiritual
assessment. The division into second and third tier is only a teaching concept that does not
correspond to the reality in the patient encounter. This discussion is not about competing for
territory, but it is an objection made for the benefit of the patients and their loved ones.
• “Life reviews can become, in essence, spiritual assessment”.62 Each patient is unique and
the course an interaction will take is unpredictable. For educational purposes the
consensus report and this document present three levels of assessment, but in the reality
of the work situation, spiritual history taking very easily evolves into a life review or in-
depth spiritual assessment for which medical staff generally are underequipped. Only in
theory is there a fixed barrier or distinction between ‘spiritual history taking’ and
‘detailed assessment’. In practice these levels of assessment are fluid. How can one
expect to know in advance how simple or complex an encounter will be?
• It is just as artificial to say that ‘identifying spiritual diagnosis and to develop a spiritual
plan of care’ (tier 2) can be done by any ‘trained’ health care professional, because it is
entirely different from a ‘complex diagnosis and treatment’ only board-certified chaplains
are qualified for (tier 3).
• It has to be specified what training is meant in “all trained health professionals should do
history taking … identify any spiritual diagnosis and develop a plan of care”. What
‘training’ exactly have general health care professionals undergone? Medical staff might
SHIFTS IN CHAPLAINCY 57
have attended lectures or received some information on spiritual care, but their primary
training, concern and competence is taking care of the physical diagnosis, treatment and
care of the patient. A chaplain’s primary training and focus is to take care of needs of the
patient other than physical. For the same reason that it is difficult to quantify spiritual
care outcomes - dealing with subtle phenomena - it is not easy to do a valuable spiritual
assessment. A chaplain is a person who intensively trained and then served in their faith
community even prior to qualifying as spiritual care practitioners. The chaplain’s
qualification attest to awareness and prolonged training in the spiritual dimension of
his/her own life, which in turn serves as the foundation to provide spiritual care for
patients. Although many members of the medical staff may well be spiritual people
personally, do they possess what was described in this document as ‘chaplain’s skills’?
• In surveys nurses themselves admit to not having adequate training in spiritual
assessment and care, and cite heavy workload, lack of time, role confusion and unease
with the topics as their barriers.63, 64, 65 Surely it is desirable that all health care
professionals, especially in palliative care, support the patient’s spiritual needs in their
daily care for the patient. But when medical staff members are the ones responsible for
completing a spiritual assessment, diagnosis and spiritual care plan development, this is
indicative of understaffing and underfunding. A recommendation for improving the
quality of spiritual care would entail that the professional chaplains administer both
structured (spiritual history taking) and unstructured (detailed) assessments.
• Medical staff often is under pressure from management to complete their workload
within limited time in spite of understaffing. Spiritual assessment, diagnosis and care plan
cannot be hurried and represent yet another burden for the medical staff. It is an essential
SHIFTS IN CHAPLAINCY 58
characteristic of a chaplain to have time for the patient. Suffering from lack of sleep,
personal worry, etc. could lead to attitudes that negatively impact the patient’s responses.
Chaplains are specifically trained how not to bring their personal problems into the
patient’s room.
• Spiritual history is one of the best doors for a chaplain to enter into the patient’s world.
To talk about intimate spiritual matters the chaplain needs to first establish rapport, trust
and familiarity with the patient; this is often accomplished speaking about a person’s
history.
• However, it can be a great emotional strain for a patient to go through what might be a
challenging experience twice.
• Even if medical staff pass on a patient’s spiritual information to the chaplain, the vital
opportunity to observe affect, behavior and communication, all the nonverbal signals and
clues that make up most communication, is missed.
• Patients’ stay in hospital tends to be short. There might not be another opportunity to
receive a chaplain’s visit, let alone a follow-up visit or an intervention like the facilitation
of a life review. This is especially true in view of the fact that spirituality is often
overlooked in the screening protocol. As discussed in the section on palliative care, even
once the patient is settled in his room, early referrals to spiritual care remain rare,
although it takes much less time to do a referral than to take the patient’s history.
VIII. Interventions
The interventions are for the most part contained in:

SHIFTS IN CHAPLAINCY 59
1) The chaplain’s skills listed in this document
2) The process of dialoguing with the patient in itself addresses the issues
3) The patient’s answers lead to further exploration and may be transformative
4) The human contact, authentic presence, genuine warmth and empathy
5) Attentiveness and active listening
6) The chaplain offering prayer, practices and all rituals that mark stages and give
comfort, solace and reassurance.
IX. Conclusion
A. End-Of-Life Care Chaplaincy
Every human being has needs which reflect a depth of being beyond mere physical
concerns. To love, be loved, be connected and respected; to speak thoughts and feeling that are
one’s truth; to explore the meaning of one’s life and disease and be supported in transformative
healing, or simply to not be alone – these all are fundamental human quests to be honored,
especially at such a vulnerable and vital time as hospitalization or dying.
Any human being will benefit from a non-judgmental attitude, human contact, caring and
kindness. Mother Teresa tells of a day in Calcutta, India: There was a man we picked up from the
drain, half eaten by worms and, after we had brought him to the home, he only said,” I have lived
like an animal in the street, but I am going to die as an angel, loved and cared for.” 23

SHIFTS IN CHAPLAINCY 60
B. Environmental Chaplaincy
It took a new model of chaplaincy to elevate the standards in professional pastoral care to
embrace an ecumenical attitude not only toward other Christian denominations, but also toward
all other faiths, and to open the profession of chaplain to women. Another shift in chaplaincy
brought about a holistic framework that integrates science as well as a humanist, existentialist or
even a secular way of ministering to the sick and dying in response to their changing needs.
What are the barriers that keep the majority of people from accepting the new way of
thinking already established in science, according to which our planet earth has all the
characteristics of a living system? Will people embrace the model of an environmental
chaplaincy that advocates for earth’s other species’ needs, using moral authority to take a stand
against pollution, and a stand for the conservation of undeveloped, pristine places? Some
ecologists see parallels between cancer, characterized by unchecked growth that harms its host,
and the effects of some human behavior driven by ignorance, aggression and greed, e.g.
overpopulation and profit-making overriding all other values. All that raises awareness and
inspires a more holistic understanding of man and nature is welcome at this crucial time. It may
well take a collaboration of art, science and religion to heal our environment with spiritual care
which, unlike a misconceived idea of religion, encourages genuine efforts to understand and
overcome the real causes of suffering.
Synthesizing timeless wisdom and scientific knowledge, we may succeed in turning away
from the insatiable accumulation of ‘more’ and the perpetual chase after a better tomorrow as
necessitated by a purely materialistic worldview. The role of environmental chaplains could be to
help usher in a new conscience and consciousness to find contentment, the appreciation of inner

SHIFTS IN CHAPLAINCY 61
riches over outer wealth, quality over quantity. The universal religious and human values of
honesty, far-sightedness, mutual kindness and understanding are not only the key for a brighter
future, but also for a happier, more fully and consciously lived present.
In closing, as we enter the third millennium, we are urgently called to action in two
distinct capacities: to serve as hospice workers to a dying culture, and to serve as
midwives to an emerging culture. These two tasks are required simultaneously; they call
upon us to move through the world with an open heart - meaning we are present for the
grief and the pain - as we experiment with new visions and forms for the future. Both are
needed. (W. Keepin, Principles of Spiritual Leadership)67

SHIFTS IN CHAPLAINCY 62
Acknowledgements
I would like to express my profound gratitude for the unrepayable kindness of all my Tibetan
Buddhist teachers. Chaplaincy is my small effort to pass on a little of the caring I received.
However, every person I tended to gave me an individual gift, so I am grateful to each of them.
My deep bow and warmest gratitude to Roshi Joan Halifax, PhD, who conceived of a whole new
approach to chaplaincy in response to the changing needs of the world; to Jean Wilkins, BSc,
MA, who is more than I could ever wish for as a mentor and became my dearly treasured
Vajrasister; to all the other teachers and Upaya residents who made the chaplaincy program
possible; to Janet Schreiber, PhD, for directing the profound Grief, Loss & Trauma program at
South Western College and her invaluable help to make this project work; to Cynthia San Luis,
MSc Palliative Care (UK), MD (Phil), palliative care consultant, who inspired my SAT study
and provided me with resources,66 for giving personal encouragement, friendship and precious
opportunities to learn; to Susan Rush, MA, spiritual care coordinator, who opened St. Vincent’s
doors and made my work possible, for granting me her trust, advice and becoming a spiritual
sister; to my supervisors and peers in my CPE group, and last but not least to my husband, Eric,
for his love and patience.

SHIFTS IN CHAPLAINCY 63
References
1. Vitello, Hospice Chaplains Take Up Bedside Counseling, New York Times, 2008/10/28.
Article and readers’ commentaries retrieved from http://nyt.com
2. Huxley, The Doors of Perception, 1954
3. Basch, Spirituality: the emperor’s new clothes? Journal of Clinical Nursing, 2004, U.S.
National Library of Medicine
4. Oxford English Dictionary, Oxford University Press, 1971 and www.askoxford.com. Chapel
from Old French chapele, from Latin capella, ‘little cape’, the first chapel being a sanctuary in
which St. Martin’s cloak was preserved.
5. Adapted from http://sacredheart.net, http://newadvent.org, http://wikipedia.org
6. VandeCreek et al., Research in Pastoral Care and Counseling, Wipf & Stock Publishers, 2008
7. Vatican Slams Avatar, 2009. Article and readers’ commentaries retrieved from http://cnn.com
8. Leopold, A Sand County Almanac, 1949
9. Miller, Living Systems, 1978
10. Adapted from Maness, http://sacredheart.net
11. Woodland and Taylor, Implications for the Delivery of Spiritual Care in Canadian
Healthcare: A Perspective from a Canadian Health Authority, 2009
12. Kernonhan et al., An evidenced based palliative care chaplaincy service in Northern Ireland,
J of Pastoral Care and Counseling, 2007
SHIFTS IN CHAPLAINCY 64
13. Strang, Questions Posed to by Palliative Care Patients in Irish Hospices, J of Pastoral Care
and Counseling, 2003
14. Adopted from Stanford Encyclopedia of Philosophy, revised 2007, http://plato.stanford.edu,
http://newadvent.org, http://wikipedia.org
15. Oddnall, A Critical Analysis of Nursing: Meeting the Spiritual Needs of Patients, Journal of
Advanced Nursing, 1996
16. Adopted from Stanford Encyclopedia of Philosophy, revised 2007, http://plato.stanford.edu,
http://wikipedia.org
17. Puchalski et al., Improving the Quality of Spiritual Care as a Dimension of Palliative Care:
The Report of the Consensus Conference. Journal of Palliative Medicine, 2009
18. Transcendent: ‘above and independent of the material experience of the universe’, American
Heritage Dictionary, 1982
19. University of Maryland, School of Medicine, Spirituality and Palliative Care, Spiritual
Assessment, updated 2009
20. Zinnbauer et al., Religion and Spirituality: Unfuzzing the Fuzzy, Journal for the Scientific
Study of Religion, 1997
21. Hallenbeck, Palliative care perspectives: chapter 7: psychosocial and spiritual aspects of care,
Oxford University Press, 2003
22. McFadden, Religion and Spirituality, Encyclopedia of Gerontology, 1996
23. From a talk given at the National Prayer Breakfast in Washington DC, 1994
SHIFTS IN CHAPLAINCY 65
24. Stiles, 1990; Burkhardt 1994; Kurtz & Kurtz, 1995; Fredette, 1995; Smucker 1996;
Farrell et al., 1996; Wyatt & Friedman, 1996; Fehrink et al., 1997; Baillard et al., 1997;
Feher & Maly, 1999; Klemm & Miller, 1999; Watson, 1999; Fryback & Reinert 1999,
Fernsier et al., 1999; Chiu, 2000
25. Koenig, Medicine, Religion & Health, Templeton Foundation Press, 2009
26. Pierce, The introduction and evaluation of a spiritual assessment tool in a palliative care unit.
Scottish J of Healthcare Chaplaincy, 2004
27. http://jointcommission.org/accreditation/programs/homecare/standards
28. Fitchett et al., Religious Struggle: Prevalence, correlates and mental health risks in diabetic,
congestive heart failure, and oncology patients, International J Psychiatric Medicine, 2004
29. Pargament et al., Religious coping methods as predictors of psychological, physical and
spiritual outcomes among medially ill elderly patients” A two-year longitudinal study. Journal of
Health and Psychology, 2004
30. Kytle and Handzo, Current Research in Chaplaincy Care, Health Care Chaplaincy, Christus
St. Vincent Webinar, 2009. Contact www.healthcarechaplaincy.org
31. Southard, Religious Inquiry, Nashville, Abingdon Press, 1976
32. Anandarajah and Height, Spirituality and medical practice: Using the HOPE questions as a
practical tool for spiritual assessment, American Fam Physician, 2001
33 a. Puchalski, Spiritual assessment in clinical practice, Psychiatr Ann, 2006
SHIFTS IN CHAPLAINCY 66
33 b. Pulchalski and Romer, Taking a spiritual history allows clinicians to understand patients
more fully, Journal of Palliative Medicine, 2000
34. Maugans, The SPIRITual history, Fam Med, 1996
35. Mainwaring,1991. Cited in VandeCreek et al., Research in Pastoral Care and Counseling,
page 74, Wipf & Stock Publishers, 2008
36 a. Higginson, The Support Team Assessment Schedule, a thesis submitted in the Faculty of
Medicine, University of London, 1992
36 b. Higginson (ed), Clinical Audit in Palliative Care, Radcliffe Medical Press, 1993
37. Flannelly et al., The Correlates of Chaplain’s Effectiveness in Meeting Spiritual/Religious
and Emotional Needs of Patients, J of Pastoral Care & Counseling, 2009
38. Adapted from VandeCreek et al., Research in Pastoral Care and Counseling, Wipf & Stock
Publ., 2008
39. Koenig et al., 1998; Fitchett et al., 1999;Pargament et al., 2004; Ano and Vascolcelles, 2005;
McConnell et al., 2006
40. Kytle and Handzo, Current Research in Chaplaincy Care, Health Care Chaplaincy, Christus
St. Vincent Webinar, 2009. Contact www.healthcarechaplaincy.org
41. Fitchett and Risk, Screening for Spiritual Struggle, Journal of Pastoral Care and Counseling,
2009. Contact: [email protected]
42. Woods and Ironson (citing Davidson), Religion and spirituality in the face of illness, Journal
of Health Psychology.
SHIFTS IN CHAPLAINCY 67
43. Stoll as cited in Kendrick and Robinson: Spirituality: its relevance and purpose for clinical
nursing in the new millennium, Journal of Clinical Nursing, 2000
44. Glass et al., Principles of Patient and Family Assessment, Textbook of Palliative
Nursing, Oxford University Press, 2006
45. Phelps et al., Religious coping and use of intensive life-‐prolonging care near death in
patients with advanced cancer, JAMA 2009
46. Silvestri et al., Importance of faith on medical decisions regarding cancer care, J of
Clinical Oncology, 2003
47. Fosarelli, Prayers and Rituals At a Time of Illness and Dying, Templeton Foundation Press,
2008
48. Lipson et al. (eds.), Culture and Nursing Care: A Pocket Guide, San Francisco: University of
California Nursing Press, 1996
49. Andrews and Boyle, Competence in transcultural nursing care, Am J Nurs, 1997
50. Hartocollis, Hard Choices for a Comfortable Death: Drug Induced Sleep, New York Times,
12/27/2009
51. Lynn et al., Recommendation for Areas of Focus and Targets for Improvement in Heath Care
Agencies Involved in IHI Collaborative, 2007
52. Adamson, RAND Health White Paper, 2003
53. Dartmouth Atlas Map of Incidence of Death in Hospitals, AHA Press, 1999

SHIFTS IN CHAPLAINCY 68
54. Brock & Foley, Hospice Journal, 1998
55. ELNEC, 2007
56. Pumphries, Personal Communication, 1989
57. Hanson, The Midwife, 1996 in Dykstra (ed), Images of Pastoral Care, 2005
58. Grun, quoting Evagrius Ponticus, in his study of the Desert Fathers, 1994
59. Frankl, Man’s Search for Meaning, Washington Square Press, 1984
60. VandeCreek et al., Research in Pastoral Care and Counseling, p. 83, Wipf & Stock
Publishers, 2008
61. Puchalski et al., Improving the Quality of Spiritual Care as a Dimension of Palliative Care:
The Report of the Consensus Conference, p. 895, Journal of Palliative Medicine, 2009
62. LeFavie and Wessels, Life review in pastoral care counseling: background and efficacy for
the terminally ill, J Pastoral Care and Counseling, 2003
63. Taylor et al., Predictors of oncology and hospice nurses’ spiritual care and practices; Appl
Nurs Res 1999
64. Highfield et al., Preparation to care: the spiritual care education of oncology and hospice
nurses; J Hosp Palliat Nurs, 2000
65. Kuuppelomaki, Spiritual support for families of patients with cancer: a pilot study of nursing
staff assessments, Cancer Nurs, 2002

SHIFTS IN CHAPLAINCY 69
66. Several quotes in this document have been taken from: San Luis, Assessing spirituality at the
end of life, dissertation submitted to King’s College, University of London, 2002, and San Luis,
Palliative Care Seminars, 2009
67. Keepin, Principles of Spiritual Leadership, adapted from a presentation given at Schumacher
College, Totnes, England, 1997
68. Ambuel and Weissman, Fast Fact and Concept, Taking a Spiritual History, 1999.
End of Life Education Project: http://eperc.mcw.edu
SHIFTS IN CHAPLAINCY 70
Appendices
Appendix 1: Self-Assessment Form 71 - 73
Appendix 2: HOPE, FICA, SPIRIT 73
Appendix 3: STAS 74
Appendix 4: Screening for Spiritual Struggle 75
Appendix 5: Quantitative Spiritual Assessment Form 76 - 78
Appendix 6: The Integrative Assessment Tool 79 - 85
Appendix 7: Suggestions for a Spiritual Care Evaluation Form 86

SHIFTS IN CHAPLAINCY 71
Appendix 1: Self-Assessment Form
Taylor & Johnston, Spiritual Care: Nursing Theory, Research and Practice; Upper Saddle River,
NJ; Pearson Education, Inc., 2002. Copyright 2002 by Pearson Education, Inc.
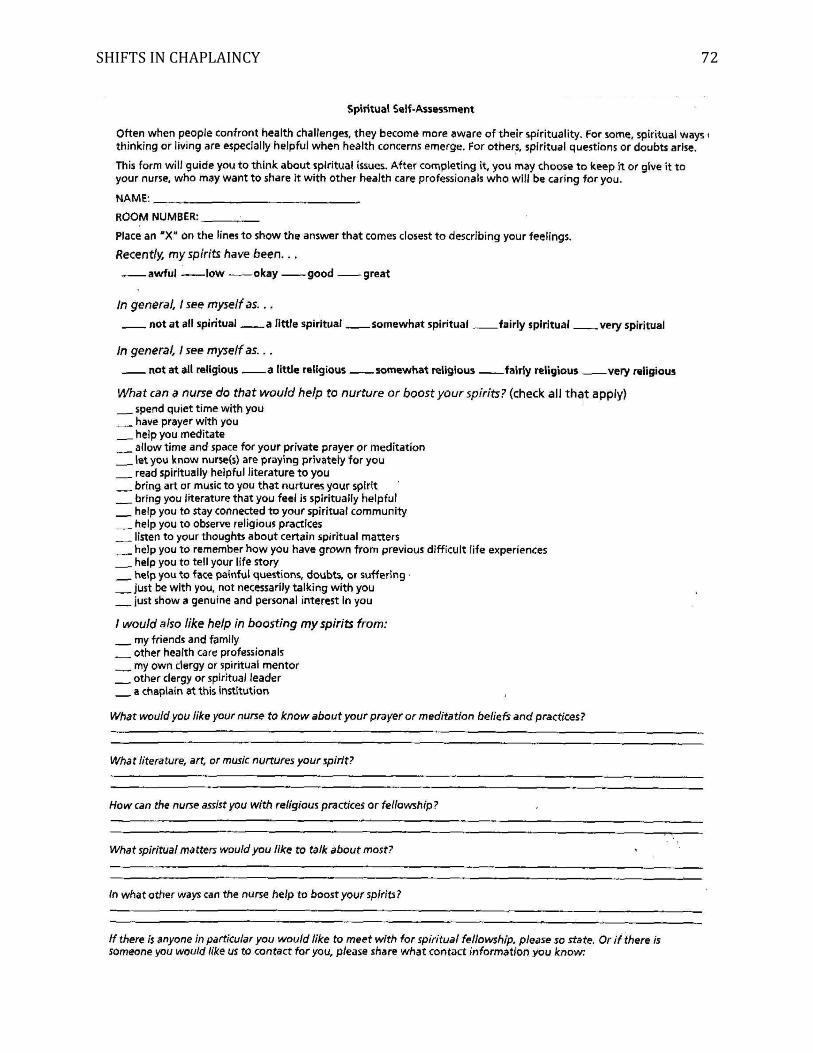
SHIFTS IN CHAPLAINCY 72
SHIFTS IN CHAPLAINCY 73
Appendix 2: HOPE, FICA, SPIRIT
(see also INSPIRIT, Kass, 1991 and Spiritual Well-Being Scale, Paloutzian, 1982)
HOPE32 (Can be downloaded from http://aafp.org)
H – Sources of Hope
O – Organized Religion
P – Personal Spirituality and Practices
E – Effects on Medical Care and End of Life Issues
FICA34 (Copyright 1996 by Christina Puchalski)
F – Faith, Belief, Meaning
I – Importance and Influence
C – Community
A – Address / Action in Care
SPIRIT35, 68 (see also: End of Life Education Project: http://eperc.mcw.edu)
S – Spiritual belief system
P – Personal spirituality
I – Integration with spiritual community
R – Ritualized practice and restrictions
I – Implications for medical care
T – Terminal event planning

SHIFTS IN CHAPLAINCY 74
Appendix 3: The Support Team Assessment Schedule (STAS)
Copyright 1992 by Irene J. Higginson
The STAS was developed to audit care given by palliative care teams by assessing
seventeen core items. The 5-point Likert scale to assess spirituality is one of these core items.
Spiritual
Degree to which the patient is content with their own spiritual beliefs or philosophy.
0 = content in self and worldview, without feelings of guilt or punishment over illness.
Any denomination or agnostic.
1 = Occasional doubts or unrealistic expectations. Patient able to resolve their feelings /
problems themselves.
2 = Uncertain, sometimes troubled. Doubts. Patient unable to resolve their feelings /
problems themselves.
3 = Uncertainty and guilt. For example troubled, conflicts, worry.
4 = Distraught with uncertainty or guilt over beliefs. In chaos as to how to remedy
situation. Crisis, unable to resolve things, inability to cope, symptomatic
(physical/emotional).
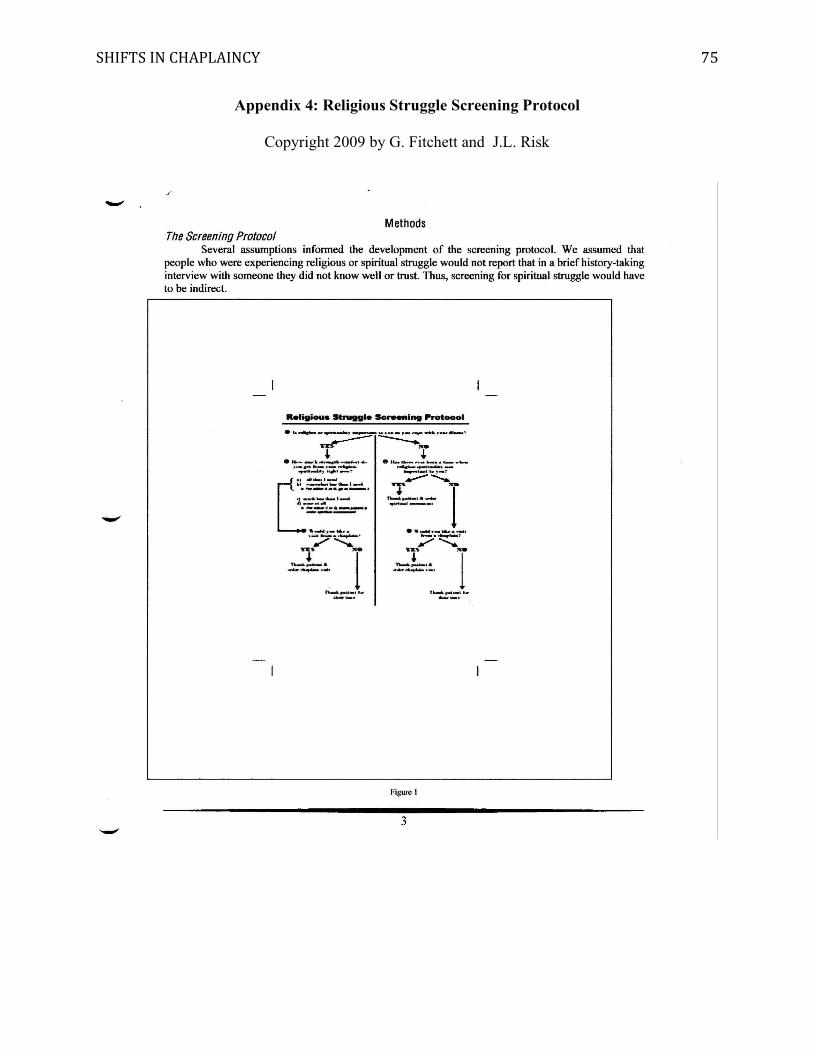
SHIFTS IN CHAPLAINCY 75
Appendix 4: Religious Struggle Screening Protocol
Copyright 2009 by G. Fitchett and J.L. Risk

SHIFTS IN CHAPLAINCY 76
Appendix 5: Example for a Quantitative Spiritual Assessment Form
DO NOT REPRODUCE

SHIFTS IN CHAPLAINCY 77
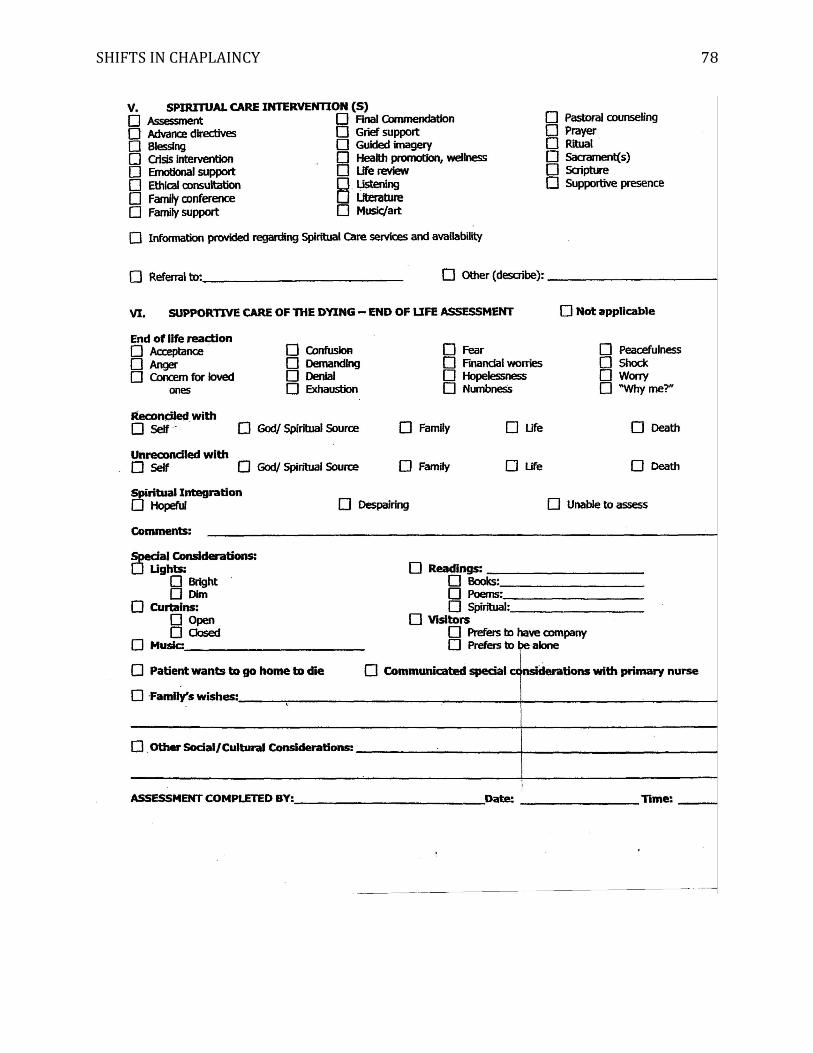
SHIFTS IN CHAPLAINCY 78
SHIFTS IN CHAPLAINCY 79
Appendix 6: The Integrative Assessment Tool
Instruction to the Chaplain on how to use ‘The Integrative Assessment Tool’:
• Chaplains can use ‘The Integrative Assessment Tool‘ as a guide to support them in
conducting semi-structured interviews. Not all questions have to be asked; they represent
available options for the chaplain to invite reflections, memories and stories, slowly
mapping this individual’s resources and the barriers to using them.
• The author assumes the religious denomination has already been determined during the
screening protocol. This information, together with answers about faith community and
who the patient would like to contact to talk with about religious or other matters, will
come up naturally as the chaplain poses the questions that explore resources and how the
patient finds meaning.
• Besides establishing rapport and trust in whatever way is appropriate, chaplains need to
determine how best to preface the questions themselves. For example, by beginning with
“If you are comfortable talking about this topic, would you please share some of your
beliefs about…”.
• With minor modifications – that the author did not include here – ‘The Integrative
Assessment Tool‘ can be used for assessing family, friends or medical staff. It is of
course crucial to follow up, explain, reassure and counsel the patient’s loved ones.
• While with the patient, it is recommendable to keep writing notes to a minimum in order
to give as much undivided attention to the patient as possible. Even if notes have to be
made, the chaplain may aspire to create an atmosphere of communion rather than that of
an interview.
SHIFTS IN CHAPLAINCY 80
Listen to where resources stem from / who or what gives meaning; listen to what might be source of
distress; listen to clues for effective interventions:
1. intrapersonal / self: recognition of positive traits, healthy self-esteem in spite of physical disabilities,
being in touch with oneself, quiet time, ability to relax, ability to tolerate stress, ability to endure
loss/vulnerability/uncertainty/ambiguity, accepts and embraces the impossibility to find meaning,
completion of tasks, finished business, feels involved in decision-making, has some degree of control,
positive outlook, gratitude, forgiveness.
2. interpersonal / relational: love, sense of belonging, closeness, closure with others, significant other,
family, friends, pets, social networks, fellowship – spiritual, cultural, professional or other.
3. transpersonal / religious / contemplative: God, deities, ultimate reality, sense of the sacred, set of
values, connectedness with or feeling looked after by Higher Power, surrender into God’s hands, sacred
scriptures, sacraments, spiritual community, clergy, faith, worship, hymns, prayer, guided imagery,
meditation, spiritual/religious practices, rituals.
4. environmental / creative / therapeutic: experience nature, music, literature, poetry, beauty, creating
collage or other art projects, journaling, life review.

SHIFTS IN CHAPLAINCY 81
THE QUESTIONS:
(a) Securing and Strengthening Resources45
(past – coping skills)
How has your attitude to life, spirituality or religion sustained you
during difficult times in the past?
What in your life has brought you joy or peace?
(present - resources)
What could nurture your inner strength or your spirit while you are here?
How does your faith, relationships or other resources you have, help you during this illness?
What can I do to make you feel more comfortable?
(future – retaining hope / goal setting)
What inspires you with hope?
What kind of goals do you look forward to? (consider short-, medium- and long-term goals)
(b) Finding meaning / Opening to a higher perspective
(past)
Looking back over your life, what moments, people or experiences stand out as important?
What did you consider the most meaningful things in life?
(present)
What really matters to you now?
What helps you make sense of being here?
SHIFTS IN CHAPLAINCY 82
How has your relationship changed to important things in your life?
Where does your sense of what to do, or how to look at things come from?
(future)
What is important for you to happen in the next few days or weeks?
What would help you find peace of mind?
What do you wish for?
(c) Impact on Medical Care and Decision Making46
How do your beliefs influence the way you think about your health?
How do your beliefs influence how you look at your disease?
How do your beliefs impact your decisions about your treatment and medical care?
What would you like your caregivers to know and pay special attention to?
(d) Special Considerations
TV on/off, curtains open/closed, lights bright/soft, temperature higher/lower, frequency of visitors
more/less, display of religious or cultural symbols, personal photo frames, flowers, wall decoration,
special blanket and other personal items, CD player, DVD player, writing or art supply, room with a view
of sky/mountains if desired and possible.
(e) Cultural / Interfaith Considerations
Interfaith and cultural considerations become particularly important toward end of life and require
awareness of the chaplain’s own ethnocentricity. Although it is unrealistic to expect a chaplain to be fully
competent at intercultural communication skills and to know the customs, taboos, etc. of all cultures, an
SHIFTS IN CHAPLAINCY 83
effort in behavioral flexibility and interfaith education has to be made to avoid major missteps. It might
be helpful to solicit the patient/their loved ones as teachers regarding faith/cultural practices by saying, for
example, “I am not very familiar with your culture / faith, could you help me understand…”.
Christus St. Vincent and other hospitals have interpreter services available. The spiritual care department
is at present working on the compilation of interfaith prayer book. To learn how to navigate today’s
pluralistic society and religious landscape see P. Fosarelli’s ‘Prayers & Rituals At a Time of Illness and
Dying’47 and other book recommendations.48, 49
(f) End of life Planning
Care (in addition to previous section ‘impact on medical care and decision making’:
How do your beliefs impact your hospital care, treatment or medical procedures?
What aspects of your religion or spirituality might impact how you would like
– or would not like to be cared for?
Do you have an advanced directive to let caregivers know what treatments you wish them to withhold?
What would you like your caregivers to know and pay special attention to?
Regrets / Forgiveness / Closure:
What do you feel you have lost in the course of this illness?
Is there any kind of “unfinished business” you would feel comfortable sharing with me?
If you had your life to live over – what would you like to be the same
and what would you like to have done differently?
In terms of your relationships (or whatever issue causes distress) – what would you like to be the same
and what would you like to have done differently?

SHIFTS IN CHAPLAINCY 84
Whose visit would mean a lot to you now?
Are there people you would like me to contact for you now, even if you have not seen them in a long
time? (For example, to say that you forgive them, or to ask for their forgiveness)
Are there people who you would like to call and come visit
(so that you can say ‘good-bye’ and ‘I love you’)?
How can I support you in finding a sense of closure as you approach the end of your life?
Even if your body should not get cured, what would help you now to find peace of mind?
Life review
What would you say were ‘the milestones’ in your life?
Would you be interested in drawing or writing a timeline of your life (or spiritual history) including
remarkable encounters and important events?
Some say “wisdom is what floats to the top like cream after a rich life” – What kind of wisdom or legacy
would you like to share or leave behind for others?
Would you like to tell me about X as a person?
Preparation:
Where would you like to die?
What does death mean to you?
What does it mean to you that this is happening?
Actual death:
What is important about how others will care for your body before and after you die?

SHIFTS IN CHAPLAINCY 85
What is important about how others conduct themselves at time of your death?
What specific instructions do you have about the care of your body after you die?
Funeral arrangements:
Where and how would you like to be buried or cremated?
What kind of ritual or funeral service would you choose?
Is there someone special you would like to officiate or
Is there something special you would like to be said at your funeral?
After death / Afterlife:
How do you want to be remembered?
What do you believe happens after death?
If your health should decline, how does your faith - or other resources -
prepare you for what is ahead?
SHIFTS IN CHAPLAINCY 86
Appendix 7: Suggestions for a Spiritual Care Evaluation Form
After each statement 5 options would be offered: strongly agree, agree, disagree, strongly disagree and
‘non applicable’. Patients/their loved ones would to put a checkmark next to the response that most
describes their experience. The form could be handed out before discharge.
The chaplain introduced him/herself.
I felt the chaplain cared about me.
I felt the chaplain was trustworthy.
I felt heard and attentively listened to.
I was comfortable to talk freely because I did not feel judged.
I had moral support / was supported in my spiritual/religious practice.
I felt empowered to explore my inner strengths.
The chaplain respected my wishes/opinions/beliefs.
The chaplain provided care in a thoughtful and sensitive manner.
The chaplain did not turn away when I expressed my fears/doubts/concerns/anger.
Receiving spiritual care made hospitalization easier.
I felt I had enough time with the chaplain.
I received the follow up visits I had requested.
The chaplain left a calling card.
How can chaplains serve patients better?