
Pandu kc008 gdg
171
“Evaluation of the effect of Gudanagaradi Vati in Pandu”. Thesis submitted to the Rajiv Gandhi University of Health Sciences, Karnataka, Bangalore. In partial fulfillment of regulations for the Award of the degree of DOCTOR OF MEDICINE (AYURVEDA VACHASPATHI) By Iranna B. Kotturshetti Guide Dr. Ch. Ranga Rao. M.D. (Ayu) Professor and Head of the Department Post Graduate and Research Center D. G. M. Ayurvedic Medical College, Gadag. Co-Guide Dr. Siva Rama Prasad Ketamakka. M.D. (Ayu) Reader in Kayachikitsa Post Graduate and Research Center D.G.M. Ayurvedic Medical College, Gadag. POST GRADUATE AND RESEARCH CENTRE (KAYACHIKITSA) D.G.M.AYURVEDIC MEDICAL COLLEGE, GADAG. 2001
-
date post
19-Oct-2014 -
Category
Documents
-
view
1.826 -
download
1
description
Evaluation of the effect ofGudanagaradi Vati in Pandu , Iranna B. Kotturshetti Post Graduate Studies & Research Center, D.G. MELMALAGI AYURVEDIC MEDICAL COLLEGE, GADAG
Transcript of Pandu kc008 gdg

“Evaluation of the effect of
Gudanagaradi Vati in Pandu”.
Thesis submitted to the Rajiv Gandhi University of Health Sciences, Karnataka, Bangalore.
In partial fulfillment of regulations for the Award of the degree of
DOCTOR OF MEDICINE
(AYURVEDA VACHASPATHI)
By
Iranna B. Kotturshetti
Guide Dr. Ch. Ranga Rao.
M.D. (Ayu) Professor and Head of the Department
Post Graduate and Research Center D. G. M. Ayurvedic Medical College, Gadag.
Co-Guide
Dr. Siva Rama Prasad Ketamakka. M.D. (Ayu)
Reader in Kayachikitsa Post Graduate and Research Center
D.G.M. Ayurvedic Medical College, Gadag.
POST GRADUATE AND RESEARCH CENTRE (KAYACHIKITSA)
D.G.M.AYURVEDIC MEDICAL COLLEGE, GADAG.
2001
Ayurmitra
TAyComprehended

This is to certify that Iranna B. Kotturshetti (M.D. (Ayurveda)
Kayachikitsa) has worked for his thesis on the topic entitled “Evaluation of the effect of Gudanagaradi Vati in Pandu”.
Cl inical tr ials are done under my supervision and
guidance. This thesis makes a dist inct advance on scienti f ic l ines
in the above subject and the f indings are highly signif icant at the
stat ist ical evaluation and have considerably contributed to the
present knowledge of the subject.
I am ful ly satisf ied with his or iginal work and hereby forward
the thesis for the evaluation of adjudicators.
Co-Guide
Dr. Siva Rama Prasad Kethamakka M.D. (Ayu) (Osm)
Reader in Kayachikitsa
Postgraduate and Research Center (Kayachikitsa)
D.G.M. Ayurvedic Medical College, Gadag.

This is to certify that the contents of this thesis entitled “Evaluation of the effect of Gudanagaradi Vati in Pandu”, has been worked out by
Iranna B. Kotturshetti under my supervision and close guidance and co
guidance of Dr. Siva Rama Prasad Kethamakka, M.D. (Ayu) (Osm).
This disease, Pandu was brought to light in Ayurvedic texts, the
etiology, pathogenesis etc., as advanced and explained by Iranna B.
Kotturshetti is solitary, scientific, and methodical and will definitely help in
explaining the disease in Ayurvedic parlance and further planning the
management.
This work is applied, scientific and an original contribution in the field of
research in Ayurveda.
I am fully satisfied with the work and recommend the thesis to be put
before the adjudication.
Guide
Dr.Ch.Ranga Rao M.D. (Ayu) (Osm)
Professor and head of the department Post graduation and research center
Kayachikitsa D.G.M. Ayurvedic Medical College, Gadag.

Index
Section I Introduction 1 -2
Section II Literary review 3 - 70
Historical
Shareera
Nidana
Contemporary Science
Chikitsa
Section III Material and methods 71 - 110
Drug review
Methods
Observations
Section IV Discussion and conclusion 111 - 122
Future Prospective 123
Summary 124
References
Bibliography

List of Charts
Chart number 1- Demographic Data of
“Evaluation of the effect of Gudanagaradi Vati in Pandu”.
Chart number 2A-1- Chief Complaints of
“Evaluation of the effect of Gudanagaradi Vati in Pandu”.
Chart number 2A-2 – Chief Complaints of
“Evaluation of the effect of Gudanagaradi Vati in Pandu”.
Chart number 2B – Chief Complaints of
“Evaluation of the effect of Gudanagaradi Vati in Pandu”.
Chart number 3 – Associated Complaints of
“Evaluation of the effect of Gudanagaradi Vati in Pandu”.
Chart number 4 – Nidana (etiology) of
“Evaluation of the effect of Gudanagaradi Vati in Pandu”.
Chart number 5a – Vatajadi lakshana of
“Evaluation of the effect of Gudanagaradi Vati in Pandu”
Chart number 5b – Vatajadi lakshana of
“Evaluation of the effect of Gudanagaradi Vati in Pandu”
Chart number 6 – Assessment of
“Evaluation of the effect of Gudanagaradi Vati in Pandu”
Chart number 7 Statistical assessment for the

“Evaluation of the effect of Gudanagaradi Vati in Pandu”
List of Graphs Graph number - 1
Age incidence in “Evaluation of the effect of Gudanagaradi Vati in Pandu"
Graph number - 2
Sex incidence in “Evaluation of the effect of Gudanagaradi Vati in Pandu"
Graph number - 3
Occupational incidence in “Evaluation of the effect of Gudanagaradi Vati in Pandu"
Graph number - 4
Economical status incidence in “Evaluation of the effect of Gudanagaradi Vati in Pandu
Graph number – 5
Diet incidence in “Evaluation of the effect of Gudanagaradi Vati in Pandu"
Graph number – 6
Objective parameters at mean values in regular intervals Heamoglobin and RBC count
Graph number – 7 Objective parameters at mean values in regular intervals PCV and Serum Iron
Graph number 8 Result of the “Evaluation of the effect of Gudanagaradi Vati in Pandu"

List of Photographs
Photograph - 1
Guda
Photograph - 2
Nagara
Photograph - 3
Mandura
Photograph - 4
Tila
Photograph - 5
Pippali

ACKNOWLEDEMENT
I express my deep sense of gratitude to my respected guide Prof. Dr. Ch.
Ranga Rao M.D (Ayu) Head of department of Kayachikitsa, D.G.M Ayurvedic
medical college and post graduate and research center, Gadag. He has been very
kind to guide me in the preparation of thesis and for whose extraordinary efforts,
tremendous encouragement and most valuable thoughts provoking advice made me
to complete this work.
I am also grateful to my respected co-guide Dr. Siva Rama Prasad
Kethamakka, M.D (Ayu) (Osm), Reader in Kayachikitsa, PGARC, D.G.M Ayurvedic
medical college, Gadag, for patiently going through the draft of thesis and correcting
with precious remarks which have been very useful.
I am extremely thankful to Dr. G.B. Patil principal D.G.M Ayurvedic medical
college and post graduate and research center Gadag, for providing all necessary
facilities for this research work.
It gives me pleasure to expresses my gratitude to Dr. A.K. Panda, M.D (Ayu)
Lecturer, P.G. Department, D.G.M. Ayurvedic Medical College, Gadag. For being
kind and affectionate through his valuable suggestions and advisees as and when
approach.

I am very much grateful to Dr. M.C Patil, M.D. (Ayu), P.G. Lecturer, for his
valuable suggestions on the important subjects.
I wish to convey thanks to my respected lecturers, Dr. G.S. Hiremath, Dr. U.V.
Purad, Dr. C.M. Sarangamath, Dr. S.A. Patil, Dr. R.K. Gachchinamath, Dr. G.S.
Jukthihiremath, Dr. B.S. Patil, Dr. C.S. Hiremath, Dr. K.S. Paraddi, and other
lecturers of D.G.M Ayurvedic Medical College, for their help and suggestions during
my post graduation studies.
I sincerely thank my beloved classmates Dr. S.S. Hiremath, Dr. A.S Patil,
Dr.(Smt) Yashoda Mudigoudar, Dr. S.T Hombal, for their deep co operation and
involvement in the P.G study.
I am also thankful to all my post graduate colleagues Dr. B.M Mulkipatil, Dr.
R.Y.Shettar, Dr. J.I Hiremath, Dr. Suresh R.D, Dr. S.K Tiwari, Dr. C.V. Rajashekar,
Dr.Shyal kumar, Dr. Jayaprakash, Dr. Anil Kumar Bacha, Dr. V.N. Kulkarni and Dr. D.
Sitarama prasad, for their constant cooperation and help.
I am ever thankful to Prof. S.V. Sankanur for his constant moral support,
encouragement and help throughout my carrier.
I wise to convey my thanks to beloved Dr. Shashidhar Doddamani, M.D (Ayu)
and Dr. S.R. Hiremath, for their constant help and rational suggestions at this
research work.
I wish to convey my thanks to beloved Dr. Mallikarjuna A.S, Dr. M.S.
Hiremath, Dr. A.M Adi, Dr. D.G. Kolume for their cooperation.
I am ever grateful to respected Dr. S.B. Lakkol, Sri R.P Huilgol, Dr. R.N Patil,
Sri S.V. Kori and Prof. Siddu yapalparavi, for their encouragement and help
throughout my carrier.

I wish to convey my thanks to beloved shri V.M Mundinamani and Mr.S.B.
Sureban for supplying me essential references in the study. I m thankful to Mr. B.S.
Tippanagoudar, Lab technician, who extended his co-operation in investigations.
I thanks to Mr. P.M. Nanda kumar for his help in the statistical evaluate.
I am highly indebted to my beloved parents Smt. & Sri Basavanneppa
Kotturshetti, Sisters Lalitha, Akamahadevi, Sumangala, Ratna, and beloved brother
Shiva for their love and affection rendered throughout my carrier.
Thanks to all lecturers, physicians, house-surgeons, hospital staff, nurses and
non teaching staff for their timely assistance in completion of this work.
Let me express my thanks to all patients, those are on the trial for their
consent for enrolling in this clinical study and obedience to advises.
This list is incomplete with out remembering my beloved wife, Dr. Veena, who
helped in all respects to complete this valuable dissertation work.
Lastly I pay my deep homage and tribute to my former teacher late Prof. Dr.
V.V.S. Sastri for his selection of this valuable project.
Iranna B. Kotturshetti

Ayurveda is an ancient Indian medical science reminded by lord Brahma1.
The main aim of this Ayurvedic medical science is to protect the human beings from
various diseases following by rules and regulations of Swasthavritta and to have
disease free human beings to have healthy society2.
Disease is nothing but, life under altered conditions. These altered conditions
in fact manifest themselves through the agency of doshas, Dhatus and mala in the
body.
The present day unwholesome food habits are influencing deficiencies of vital
nutrients and leads to nutritional disorders. The disease Panduroga that is dealt in all
Ayurvedic texts with its treatment which is very much similar to Anaemia in later
Introduction 1

period. The Panduroga has very much similarity with Anaemia in later period. The
word Anaemia first appeared for medical use in 1824 and in 1849 it began to have a
specific medical meaning. It is one of the common clinical conditions both in the
developed and developing countries like India. The W.H.O has recognized as a world
health problem, which is much common in our country.
The disease Panduroga is explained in all most all Ayurvedic classics with its
etiopathogenesis and treatment elaborately. Ayurveda advocate the treatment of
Pandu with many herbal and herbo-mineral combinations. Charaka (C.Chi 16/72)
and Vagbhata ( A.H.Chi 16/25) have highlighted the combination of Guda, Nagara,
Mandura, Tila and Pippali, as an effective recipe in Panduroga that is named as "
Gudanagaradivati " in the present study.
The ingredients of Gudanagaradivati are easily available and chief from their
qualities and this prospective the study is being conducted to evaluate the effect of it
as a combination in Panduroga.
In this clinical study 25 patients were incidentally selected and subjected in
one group. The duration of treatment was 21 days.
The clinical and hematological assessment was made before and after the
study. In this study it was observed and analyzed the effect of Gudanagaradivati was
statistically significant. The hemoglobin concentration raised significantly and
response of clinical features of Pandu to the drug was good.
Introduction 2

1 Astanga Hridaya Sutra 1/3 2 Susruta Sutra 1/6
Introduction 3

Unlike the history of any other subjects the "History of medicine" is medicine it
self such a history at hand will serve as a golden key to the understanding of many
aspects of medicine in both academic and practical ways. The history of Ayurvedic
literature reveals more information regarding Panduroga.
In a systemic enquire into the state of medical science in India, it may be
pointed out that the Brihatrayi, were the earliest of the medical literatures. Which
furnish us with detail description of the disease Pandu, for the sake of convenience
the history of Ayurveda can be divided as follows.
1. Vedic period
2. Pauranika (Purana) period
3. Samhita period
4. Sangraha period
5. Modern period
1. Vedic period:
In Vedic literature especially in Rigveda3 and Atharvaveda4, we found the
terms "Halima" and "Harita" which are observed to be correlative with Panduroga.
The treatment of the said disease also mentioned in both the Vedas.
Review of literature 3

2. Purana kala:
The word "Pandu" is available in Mahabharata when sage "Vyasa"
intercourse with "Ambilika" the widow of Vichitravirya; she became quite pale (Pandu
Varna) with fear. That's why her son who born became pales (Pandu) coloured and
named as "Pandu".
In Garuda purana there is a reference that takra mixed with lauha churna was
advocated in the treatment of Pandu patient. Besides the above the description of
Pandu is also available in Agnipurana, Valmiki Ramayana, and Yogavasistha.
3. Samhita period:
The main Samhita like Charaka and Susruta have clearly described about
Panduroga. In Charaka Samhita Chikitsa sthana 16th chapter and in Susruta Samhita
Uttaratantra 44th chapter we can find about the description of Panduroga.
4. Sangraha period:
In this period - Astanga Sangraha, Astanga Hridaya, Madhava Nidana was
written and elaborated about Panduroga.
5. Modern period:
In modern period so many commentators discussed about Panduroga and
they co-relate it with Anaemia. The word Anaemia first appeared for medical use in
1824 and in 1849 it began to have specific medical meaning (which is much more
similarity with Panduroga).
Review of literature 4

Naming of the disease - " PANDU ROGA"
According to Ayurveda diseases are innumerable (aparisankhyeya) as
described by Charaka5. But they may be classified on the basis of rupa (main
complaints), Varna (alteration in colors), samuthana (according to etiology) sthana
(according to seat or location) and samsthana (according to clinical features of the
disease) and so on. There fore the Panduroga is such a disease rather clinical
condition characterized by alteration in colour of skin and mucous membrane.
Panduroga its definition and literature meaning:
When there is decreasing of Rakta (blood), Meda (fat), Ojas (body immunity),
diminished of body activities and discoloration of body occurs, at that time it is known
as Panduroga6.
When Ranjakapitta mixed with the first Dhatu i.e., Rasadhatu, it produces
Rakta Dhatu (blood), but when this process vitiated the vikara takes place and
ultimately Panduroga occurs7.
The word Pandu is a relative term to indicate some colour. With this purpose
Charaka had quoted in 24 places, Susruta in 29 places and Vagbhata in 14 places
have used the words like Pandu, Pandutwa, Panduta, Pandubhava, Panduvarna,
Review of literature 5

Pandura, Pandugatra, Panduvadan etc. in their classical text. Chakrapani, Dalhana
and Arunadutta, commentator of above Brihatrayee of Ayurveda had explained its
meaning as sweta, dhushara swetavabhasa and peetavabhasa.
Acharya Gangadhara has defined a Pandu Varna as 'Mlana' Varna to explain
the colour. Different colorful objectives like Shankha, Madanphala (ripe), Katakidhuli,
Parushakphala (unripe) etc. have been quoted. Monier William in his Sanskrit -
English dictionary has defined Pandu as pallor.
In Ayurvedic classic Pandu has been taken in three forms i.e.,
Pandu as a disease
Pandu as a sings symptoms (clinical features)
Pandu as a complication
But maximum part it considers as a disease due to change of the natural body colour
into abnormal colour and "Raktalpata" occurs.
The word Pandu is derived 'padi nashane dhatu' by adding 'ku' pratyaya in it.
The meaning of which is always taken in the sense of "nasham" and as Pandu has
been kept under the group which is classified and named according to the change in
colour. Therefore the nashana will be in the Varna or colour, which is further,
approved by Charaka with the word " vaivarna". Thus Pandu is a disease in which
there is mainly vaivarna or change in colour of the body takes place.
Review of literature 6

From various dictionaries, the term "Pandu" is defined as -
Pandu pittasamvalitah suklah - (Amarakosh)
Pandustu pitabhagardhah ketakidhuli sannibha -
(Vachaspatyam)
Panduh sretavarna, ketakidhuli sannibha, pitabhagardha varna
vedascha - (sabdastommahanidhi)
Pandu - pale white, whitish, pale, yellowish.
The pale white or yellowish white colour (the students sanskrit
English dictionary by Vaman Shivram Apte.)
From the above derivatives it could be concluded that Pandu denotes some specific
colour. "Roga " derived from (ruja + ghang) or "ruja karoti roga" - it means which
gives some pain is known as Roga.
As per students Sanskrit English dictionary;
Roga means - a disease, malady, sickness etc. So from above discussion we
could say that
Panduroga = the disease with pallor of the body.
Review of literature 7

3 Rigveda 10-50-11 4 Atharvaveda 4-9-3 & 1-22-2 5 Charaka Samhita Sutra 18/43 6 Charaka Samhita Chikitsa 16/6 7 Susruta Samhita Sutra 14/
Review of literature 8

In the process of genesis of Pandu pathology it is necessary to consider the
organs in concern. Specifically skin and blood, an admixture of plasma and blood
corpuscles has to be studied in detail. Lung, Liver, Spleen, and bone marrow also
have its impact on the genesis of pathology in Pandu. Here a stretch has been given
towards blood, as it is the specific cause of showing decreased haem and also total
blood cell (RBC) count along with Skin a covering and protective agent of the entire
body as it reflects the deficiency of blood in the body.
I. Twak
Vasa and shattwacha are the upadhatu of Mamsa Dhatu8, which are going to
develop in the process of dhatwagni paka of sequential progression of Dhatus the
Mamsa is said to be making the covering of the body9 and responsible for gati. The
skin (Upadhatu of Mamsa) is developed from Mamsa, show the characteristic
features in Panduroga as the twacha is being affected or showing the disease
significance in the skin, its importance is to be elucidated.
According to the opinion of Vagbhata embryological development of the skin
is from the blood i.e., Rakta as if from the boiling milk cream develops10. The skin is
having seven layers. At the present disease concern the first layer Avabhasini or
otherwise Udakadhara referred by Shalya and Kayachikitsa faculties respectively.
The shat twacha are as follows 11-
Literary review - Shareera 8

1. Avabhasini or Udakadhara
2. Lohita or Asrigdhara
3. Swetha or Sidhmakilasa sambhava
4. Tamra or Dadru Kusta sambhava
5. Vedini or Alaji vidradhi sambhavadhistana
6. Rohini
7. Mamsadhara
Avabhacini
This is the outer most and first layer of the skin. It reflects or shows the
colour of the second layer Lohita. As it reflects the colour it is presumed that the
colour change in Lohita is witnessed in Avabhasini. It is being said at the size of
1/18th of vrhee.
Lohita
Lohita looks in arunavarna i.e., red in colour and 1/16th of vrhee. It prevents
the blood flow to outside from the body. The colour of the blood in the lohita is
reflected through Avabhasini.
II. Rakta
Rakta i.e. blood is a liquid connective tissue, which is made of cells and
plasma and in further it is described as liquid intercellular substance. When freshly
shed, blood is a red, thick, opaque and slightly alkaline fluid. Out of its normal
Literary review - Shareera 9

functions as regular transportation, maintenance of Iron balance and acid base
balance are said to be specific.
Formation of Rakta
The essence of Ahara after being subjected to paka by Ranjakapitta attains
red colour and becomes Rakta Dhatu12. Susruta further says that the rasa is formed
from the Ahara rasa after reaching Yakrit and Pleha from the Kosta.
Now, coming to the point as to what the Rakta Dhatu may be in terms of
modern physiology, it can be said that the cellular portion of the blood is as Rakta
Dhatu and liquid part of blood is considered as Rasa Dhatu. Therefore, blood
includes both Rasa and Rakta Dhatu and for the convenience of description blood
can be referred to as 'Rasa Rakta'.
Blood cells
The cellular portion of rasa Rakta comprises 45%. The blood cells are of 3 types.
1. Erythrocytes or R.B.C.s
2. Leukocytes or W.B.C.s and
3. Thrombocytes or platelets.
R.B.C.s number about 5-6 millions/cu.mm diameter 7.7 microns and
Thickness of 2.2 microns. R.B.Cs do not contain nuclei while they are in circulation.
These cells enter the blood at bone marrow as and how they are produced and
Literary review - Shareera 10

matured in the red bone marrow. The rate of production of R.B.Cs by the bone
morrow is about 7 millions/second and the R.E. cells of the circulation will destroy
approximately the same number of cells. The red bone morrow gets stimulation for
the synthesis of materials required for the R.B.C production from the haemopoitic
factors present in the stomach, Brunner's glands of duodenum, liver, spleen and
R.E.F (Renal erythropoitic factor) of juxta glomerular apparatus. Apart from these
internal factors iron (Fe) copper (Cu), B12, folic acid and proteins of food serve as
extrinsic factors. By the influence of the above said factors hemoglobin is
synthesized in the body, and gets fixed to the R.B.C s. if the hemoglobin is not
synthesized well, the red bone marrow sends only premature R.B.Cs devoid of
hemoglobin.
Hemoglobin
The red colour of R.B.C s is due to the hemoglobin. This pigment is
composed of 2 substances viz. Heam and globulin heam contains prophyrin and Fe
(iron). Therefore the main component of hemoglobin is iron. This compound (Hb) can
combine with oxygen 60 times more than what the water can i.e., we are able to get
on with 6 liters of blood only due to the presence of this hemoglobin. If there had
been water instead of blood we would require 360 liters. Another advantages with Hb
are it can readily combine with O2 in the lungs and CO2 in the tissues and form the
unstable compounds, carboxy and oxy hemoglobin, and thus serving the oxygen
needs of the body with maximum quickness.
Quantity = 16 grams/100c.c. of blood in adults.
Literary review - Shareera 11

The life of R.B.C s is about 120 days. After this period since the R.B.C becomes
old and incapable to carry its functions, the R.E. cells of liver and spleen will destroy
such cells. The iron content of hemoglobin of these destroyed cells is mostly used
again for the synthesis of hemoglobin and part of it is spent for the production of bile
juice. If the destruction of R.B.Cs is increased more than normal, more of bilirubin will
be produced. And accumulates in the circulation resulting in jaundice (Kamala) the
hemolytic jaundice) the jaundice may also be caused by the damage of liver
(infective or hepatic jaundice) or by the obstruction of bile ducts (obstructive jaundice
- Avaruddha kamala). Thus the main functions of hemoglobin are.
1. To impart O2 carrying capacity to blood.
2. To impart colour to the body through blood.
3. To help again for the manufacture of Hb, and
4. To contribute some constituents required for the production of bile juice.
Functions of Rakta13
1 Varna prasada Colour of the skin
2 Mamsapusti Nourishment to other Dhatus like Mamsa
3 Jeevana vyapara O2 supply
4 Bala Strength
5 Sukha Health and happiness
6 Prasannata Tranquility
7 Ayuh Life
Literary review - Shareera 12

Suddha rakta purusha lakshanas14
(Characteristics of the person endowed with pure blood)
As long as a person is having pure blood in him -
His colour and complexion are very attractive.
His Indriyas and Indriyardhas are perfectly normal
His digestive power is perfect.
Will be quite healthy and happy.
His Dhatupusti and Bala are perfectly normal.
Suddha Rakta lakshanas15
The following colors indicate of pure blood.
Pure blood looks like a bright indra gopa
Like pure gold
Looks like Padma (lotus flower) and Alaktaka (lacca) and
Gunjaphala savarnam i.e. brightly red like Gunja seed
PANCHABOUTIKATA OF BLOOD16
The following qualities of blood represent the presence of their respective
Mahabhutas and thus establish the fact that the blood is Panchaboutika its.
1. Visrata = Fleshy odour indicates pruthvi bhuta
2. Dravata = Fluidity of out indicates jala bhuta.
3. Raga = Redness odour indicates agni bhuta
4. Spandana = Movement odour indicates vayu bhuta, and
5. Laghuta = Lightness odour indicates akasha bhuta.
Literary review - Shareera 13

Role of Phupphusa, Yakrit and Pleeha in Rakta Shodhana:
(Role of lungs, liver and spleen in the purification of blood)
Blood reaches the lungs through pulmonary artery from the right ventricle and
is distributed all around the pulmonary alveoli in lungs through the single cell walled
capillary net work. The alveolar wall also is extremely thin to facilitate the free
exchange of gases between the blood and air. Blood thus oxygenated in the lungs
passes on to the left atrium through pulmonary veins. Thus, the lungs are responsible
for the oxygenation of blood. Here, the CO2 of blood brought from the right side of the
heart gets eliminated through lungs during expiration and the O2 is taken in side by
the blood after inspiration.
SPLEEN:
The reticulo endothelial cells of the spleen destroy the old RBCs of the blood.
Bilirubin is formed out of the hemoglobin of the destroyed RBCs, spleen also helps in
the storage of blood.
LIVER:
Conjugation of bile pigments to form bile juice takes place in the liver.
Destruction of old RBCs takes place to some extent in the liver also by the Kupffer's
cells of liver. Moreover, as already described, the harmful substances like toxins,
bacteria, absorbed drugs etc., circulating in the blood are destroyed by the liver cells
and excreted through bile juice. The liver maintains the composition of blood.
Literary review - Shareera 14

COMPOSTION OF BLOOD
Cellular portion 45%
1 RBC"s 5 to 6 millions per c.mm.
2 WBC"s 6000 to 8000 per c.mm. and
3 Platelets 2 to 3 lakhs per c.mm
RBC, WBCm ratio: 1000: 1
RBC, platelets ratio: 20:1
Platelets WBC ratio: 50:1
Plasma 55%
Water = 92% proteins = 7%
Na, K, Ca, Mg, P, Fe, C etc. 0.9%
Non-protein nitrogenous substances -
Such as uric acid, Creatine, NH3 amino acid, neutral fat, = traces
The plasma proteins are
Serum albumin = 4.7%
Serum globulin = 0.4%
Fibrinogen = 2.2%
RAKTA KSHAYA LAKSHANAS17
1. Amla sishira preeti = desire for acrid and cold substances
2. Sirashaithilyata = collapse of blood vessels, and
3. Rookshata = dryness of skin
Literary review - Shareera 15

RASA VAHA AND RAKTA VAHA SROTASES18
The origin of Rakta vaha srotases is Yakrit (liver) and Pleha (spleen). The
above descriptions state that, the nutrients required for plasma and the storage of
blood take place in Raktavaha srotomoolas i.e., liver and spleen whereas the
pumping station for blood which as a basic nutrient supplier for all the Dhatus is
Hridaya along with its 10 dhamanis. These ten dhamanis cannot correctly be
described according to modern physiology. To correlate the number (10) we have to
take the important arteries like
1. Right and
2. Left coronary arteries
3. Inanimate artery
4. Subclavian artery and so on.
RAKTA SARA PURUSHA LAKSHANAS19
A person having fully developed Rakta Dhatu from the birth onwards is known
as Raktasarapurusha. His/her Karna (ears), Netra (eyes), Mukha (face), Jihva
(tongue), Nasa (nose), Oshtha (lips), Panitala (palms), Padatala (soles of the foot),
Nakha (nails), Lalata (fore head), Medhra (penis) etc., look brightly red glistening and
attractive.
Literary review - Shareera 16

8 Charaka Samhita Chikitsa 15/17 9 Astanga Hridaya Sutra 11/4 10 Astanga Hridaya Shareera 3/8 11 Susruta Samhita Shareera 4/3; Charaka SamhitaShareera 7/5 12 Charaka Samhita Chikitsa 15/27 13 Charaka Samhita Sutra 24/3 Susruta Samhita Sutra 5/6 14 Charaka Samhita Sutra 24/23 15 Charaka Samhita Sutra 24/21 16 Susruta Samhita Sutra 14/9 17 Astanga Hridaya Sutra 11/17 18 Charaka Samhita Vimana 5/9 19 Charaka Samhita Vimana 8/114
Literary review - Shareera 17

Literary review - Nidana 17
Factors, which are responsible for production of Pandu Roga, are clearly
mentioned by our Ayurvedic classics.
According to Charaka20
Intake of Kshara (alkali), Amla (acid) Lavana (salt), Ati Ushnata, virudha
Ahara, asatmya Ahara, Nishpava, Masha, Pinyaka, Tilataila, day sleep, excessive
exercise, Atimaithuna (excessive indulgence in the sexual acts), immediate alteration
of daily routine life, suppression of the natural urges (vegadadharan).
Human having excessive sexual willing, thought, fear, anxieties, anger,
person after taking the above etiological factors; his/her Pitta (Sadhakapitta which is
at heart) got aggravated and it mixed with vayu (Vyanavata) (which is more powerful
among the Tridosha). Than it makes "sthana sanshraya" within skin and muscle and
polluted Kapha, Vata, Rakta, Twacha (skin) Mamsa and create Pandu Roga.
According to Susruta21
Excess exercise, acidic and salty diet, madya (alcohol), mrit (soil), day sleep,
etc. - All these factors create Panduroga. Certain disease which act as causative
factor in the production of Panduroga (Nidanarthakar Roga) are -
1. Bleeding tendency diseases like - vividha abhighata, krimi roga (helminthic
manifestation), Arsha (piles), Rakta pitta, Rakta pradara etc.

Literary review - Nidana 18
2. Diseases of liver and spleen - Yakritdalyodar, Pleehodara,
(hepatospleenomegaly) Jalodar (ascities), Grahani (sprue).
3. Metabolic and other diseases like - Prameha, Raj-yakshma, Atimaithuna janya
Vyadhi (diseases because of excessive indulgence in sexual act), Visama jwara
(malarial fever), etc.
4. Pyogenic diseases like - Vrana, Arbuda (malignancy tumor).
5. Panduroga is also due to nidanarthakar roga - when some disease produce
another diseases are known as nidanarthakar roga. With this understanding
many diseases are found in Ayurvedic literatures, that precipitated Pandu,
possibly due to loss of blood from the human system. Examples are -
Raktarbuda22
Raktapradara23
Raktapitta24
Katika-taruna marmavedha 25
Raktakshaya26
Yakrit Pleha vedha27 etc,.
Various Ayurvedic Samhita describes the causative factors of Panduroga as
follows -
1. Ahara Hetu (Dietary factors)
2. Vihara Hetu (physical factors)
3. Manasika Hetu (factors affecting mind)

Literary review - Nidana 19
Samhita Ahara Vihara Manasika
Charaka28 Rasa Kshara Diwaswpna
Vyayama
Ativyavaya
Kama
Amla
Lavana
Guna Atiushna Prati Karma Chinta
Dravya Nishpav Ritu vaishamya
Vegadharana
Bhaya
Masha Krodha
Tila taila Shoka
Prinyaka
Susruta29
Madhava Nidana
Yogaratnakara
Rasa: Amla Diwaswpna
Lavana Ativyayama
Guna Atiteekshna
Dravya Madhya
Mrit

Literary review - Nidana 20
Purvarupa of panduroga
The sign and symptoms, which give the earlier idea about disease, which are
to be developed further, are called Poorvarupa that is prodromal symptoms of the
disease30. Acharya Susruta has described six stages of Kriyakala out of which the
forth stage of Kriyakala is sthanasamshraya represents the prodromal phase or
Poorvarupa of the disease.
In this stage the virgin doshas or dushyas are vitiated to the place in the body
where they suited place in khavaigunya and development of disease takes place at
that site.

Literary review - Nidana 21
Poorvarupa described by Brihatrai31
S.No Signs/Symptoms Charaka Susruta Vagbhata
1 Hrit Spandhana (palpitation) + - +
2 Rooksha (dryness) + - +
3 Swedabhava (No sweating) + - +
4 Shrama (Fatigue) + - +
5 Twak Sputana (cracking of skin) - + +
6 Hrillasa (Nausea) - + +
7 Pada gourava (Heaviness in lower limbs) - + +
8 Mridbhakshaneccha - + +
9 Akshi Koota shota (puffiness around eyes) - + +
10 Avipaka (Indigestion) - + +
11 Peeta mutrata (yellow urine) - + +
12 Peeta Purisha (yellow stool) - + +
13 Aruchi (loss of appetite) - - +
Purva rupa described by laghrutrayi Harita Samihita Vangasena32
Twak spotona
Sthevana
Gatrashoola
Mridbhaksanechcha
Prekshan kuta shoota
Purisha petata
Mutra petata
Avipaka
Akshikuta shotha
Shwayathu
Shareera panduta
Peta mutrata
Twak pradeeryata
Pipasa
Aruchi
Hrillasa
Urodaha
Anga gourava
Raktalochanata

Literary review - Nidana 22
Lakshana (Roopa) of Pandu
The term roopa implies both the signs and symptoms through which a disease is
identified. In addition to the cardinal signs and symptoms, a number of constitutional
symptoms will also manifest in Pandu. Few of the symptoms aid in distinguishing the
types on the basis of doshanubandha. In the advanced stage with deterioration of the
general condition, a number of other symptoms will develop. Accordingly the signs
and symptoms can be classified as follows.
1) Pratyatma lakshanas (cardinal signs and symptoms)
2) Samanye lakshanas (general signs and symptoms)
3) Vishishta lakshanas (distinguishing features of doshanubanda)
1. Pratyatma Niyata lakshanas
It is the invariable feature present in a disease Pandu Varna of the twacha is
considered as the pratyatma Niyata lakshanas of Panduroga. This is an abnormal
colour imparted to the skin due to rasa and Rakta kshaya in the body. This is almost
like colour of pollens of kethaki flower.
In addition to the above in vathaja Pandu krishna or arunavarna is associated
with Panduroga. In pittaja pandu peetha, haritha, haridra, likewise in kaphaja pandu
shwetha varna is associated with pandu varma and changes the normal colour of the
skin like krishna, shyama, avadatha, shymavedata to krishna pandutha, haridra
pandutha, shwetha pandutha etc.

Literary review - Nidana 23
2. Samanya lakshanas
A number of constitutional symptoms will manifest in varying degrees, which
are considered as general symptoms.
• Alparaktha
• Dourbalya
• Hridrava
• Shwasa
• Bhrama
• Kati uru and parshwaruk
• Karna kshewada
• Mandagni
• Sadana
• Gourava
• Shoonkshi koota
• Shotha
This is an important lakshana that can be observed in Panduroga. The
quantity of Rakta in whole body is stated to be about ashtanjali (eight anjali) and
Rakta Varna in its colour. Here guru and ushna gunas are on account of prithvi
dravatha due to Ap mahabutha. Rakthata is an account of tejo mahabhuta. Hence
this Rakta is attributed as Jeeva Rakta. Rakta imparts colour and complexion to the
skin and hence causes Pandu Varna.
Literary review - Nidana 24
Alpa Raktata
Alap raktata or Raktalpatha can also occur due to the kshaya of Rasadhatu
and Panduroga is grouped under rasapradoshaja vikaras. The kshaya of Rasadhatu
can be mainly due to two reasons, first being scarce availability of Ahara dravyas,
which are considered as basic requirements for the rasa prapthi. Any scarcity either
quantitative or qualitative results in rasaabhava owing to under nutrition and
malnutrition respectively.
The second reason, which can result in rasaabhava, is the vikruti of
Pachakapitta. Any vikruti in Pachakapitta results in the improper production of
Rasadhatu and in turn in the production of Rakta Dhatu depends on its previous
Dhatu the rasa.
Sometimes even though the production of Rasadhatu is proper any vikruti of
Ranjakapitta can also result in rakthalpatha as the process of rasaranjana is
impaired.
Along with Pachakapitta and Ranjakapitta the aganthu reasons like abhighata
can also result in rakthalpatha and in turn it may leads to Panduroga.
The conditions like Arshas, Pleehodara, Jeernavishama - Jwara, Raktharbudha,
Yakshma, Rakthapitta which result in Rakta nasha is also responsible for the
occurrence of Pandu. The disease Pandu that is resulted out of rasa and
raktakshaya can exhibit the following lakshanas.

Literary review - Nidana 25
1) Hridrava
2) Trishna
3) Roukshya
4) Shrama
5) Shosha
6) Glani
7) Daha
8) Sheeta pradhana
9) Krusha
10) Shwasa
11) Mandanala
12) Pandutha
13) Twak spotana
14) Dhatukshaya
15) Dourbalya
16) Gatrasada
17) Gurugatrata
18) Varnabeda
19) Nidralutva
20) Tandra
21) Shopha
Dourbalya
The extent of dourbalya in Pandu can be measured in relation to his normal
bala. The degree of rakthalpatha can also help in estimating whether dourbalya is
mrudu, madya or dharuna.
Karshya
Karshya in Pandu is related to the body of the individual in his healthy state.
Anyway the kshaya of poshaka dhatu such as Rasa, Rakta, Mamsa etc., can cause
the shushkta of the spik, greeva and udara. Dhamanijala will be prominent and
sthoolaparva may be present. The lakshanas appear as the vitiated Vata finds its
place in Raktadhatu.

Literary review - Nidana 26
Hridrava
Rasa kshaya and rakthakshaya result in Vata vriddhi cause Hridaya
spandana there will be an extra load on Hridaya as the hridayagati increases in order
to reach Raktadhatu to all parts of the body. This may ultimately result in Hridaya
visthara.
Shwasa
Shwasa in Pandu referred to the increases in the number of shwasa gathi this
is a common manifestation of dourbalya and many times indicated as Hridaya
dourbalya resulted out of extra load on Hridaya. This shramaja shwasa suggests the
prakopa of vayu and Kapha in general and prakopa of Pranavata in particular.
Bhrama
Any increase in rajoguna along with the prakopa of Vata and Pitta is
responsible for Bhrama. The vitiated Vata influencing Rakta, Mamsa and Medas
causes Bhrama. Pittavrutavata, ksheena kapha, ksheena majja, can also cause
Bhrama. Bhrama occurs due to the involvement of all these factors in Panduroga.
Kati, uru and pada ruk
The vrudha Vata of Panduroga is responsible for the pain in the above
regions.

Literary review - Nidana 27
Karnakshweda
It is a nanatmaja vikara of Vata. Due to Rakta Pitta the shravanendriya is not
nourished properly and due to alpamedaskatha, the snehanakriya does not takes
place, resulting in sthanika rooksha guna vriddi and vitiated vayu takes shelter in
karna to lead to karnakashweda.
Mandagni
Mandagni is due to rakthalpata. This is due to the vitiated Pitta, Kapha and
also due to the influence of vayu over koshtagni.
Sadana
Avayavasadana is a nanatmaja vikara of Pitta dosha, Mamsa Dhatu
ksheenatha and ojoksheenatha are mainly responsible for causing sadana in the
body so we can say sadana in Pandu is due to Dhatu kshaya and ojokshaya.
Gourava
It is due to the increased Kapha dosha and Ama dosha in the body. In
Panduroga this occurs due to Agnimandya which results in the formation of Ama that
causes the Dhatu shaithilyatha in the body.
Shoonakshikoota
Occurrence of shotha in akshikoota is due to rakthalpata in Panduroga. This
is again due to the increase in Amadosha.

Literary review - Nidana 28
Sheernalomatha
This is due to increase of Vata and Pitta in the body. Due to rakthalpata other
Dhatus will be undernourished due to which sheernalomatha occurs.
Hathaprabha
This is due to the causes like raktalpatha and Pitta prakopa. Rakta Dhatu and
Pitta prakopa are responsible for imparting colour and complexion to the body. The
person of Panduroga suffers from the loss of complexion due to ojokshaya in the
body.
Shwetaakshitwa
This is explained by kashyapa under the heading of samanya lakshanas of
Panduroga. This is due to increased vayu and majjagatha Kapha vikruthi.
Shwethanakhatwa
This is due to the rakthalpata and vitiated Kapha in the body.
Satwahani
The word satwa denotes 'bala' so satwahani means balahani. Dhatu shaitilya
and agnimandya leads to mal nourishment and satwahani. Satwa also signifies
Manas, so the involvement of Manas in Pandu is also significant. The satwa amsha
of Manas is deteriorated due to Ojokshaya in the body.

Literary review - Nidana 29
Tabular form of Pandu Lakshana
S.No Lakshana Charaka Susruta Vagbhata 1 Karnakseweda + - + 2 Hatanala + - + 3 Dourbalya + - + 4 Sadana + - - 5 Annadwesha + - + 6 Shrama + - + 7 Bhrama + - + 8 Gatrashoola + - - 9 Jwara + - + 10 Swasha + - - 11 Gourava + - + 12 Aruchi + - + 13 Gatramardata + - + 14 Gatrapeeda + - - 15 Gatronmatana + - - 16 Soonakshikoota + - + 17 Harita varna + - Panduvarna 18 Sheerna lomata + - + 19 Hata prabha + - - 20 Kopanata + - + 21 Shishira dweshi + - + 22 Nidraluta + - - 23 Pindikodweshtana + - - 24 Katiruk + - - 25 Pada ruk + - - 26 Pada sada + - - 27 Ururuk + - - 28 Kati sada + - - 29 Uru sada + - - 30 Dhatu saithilya + - + 31 Ojo guna kshaya + - + 32 Alpa raktata + Raktadusti + 33 Alpamedaskata + - + 34 Nissarata + - + 35 Hridrava + - + 36 Sithilendriyata + - + 37 Twacha panduta + + + 38 Swetakshitwa - - - 39 Sweta nakhatwa - - - 40 Swetha vakrata - - -

Literary review - Nidana 30
3. Vishista roopas
The lakshanas specified to doshic virulence is also an important part of their
study, for the early diagnosis and for the purpose of prognosis. The different
classification of Panduroga is mentioned with reference to samanya Samprapti.
Classification of Panduroga
According to sankya Samprapti the classification of Panduroga described in
different Samhita granthas in different views. Charaka, Vagbhata, Madhava,
Sharangandhara, Yogaratnakara and Kashyapa all mentioned 5 types of Panduroga.
They are as follows33.
1.Vataja
2.pittaja
3.kaphaja
4.sannipataja
5.mritbhakshanajanya
Susruta has claimed that there are only 4 types of Panduroga34
1.vataja
2.pittaja
3.kaphaja
4.sannipataja
According to Susruta different types of mrit produces particular
doshavaishamya or doshaprakopa and afterwards gets converted into doshaja
Pandu. Hence he has not included the mritbhakshanajanya Pandu as 5th type of
Panduroga.

Literary review - Nidana 31
Taking in to consideration all these opinions we can say that there are 5 types
of Panduroga as described by Acharya Charaka and Vagbhata.
Vathaja Panduroga
As said earlier the prevalence of vathaja Panduroga is in those who are of
vathaja tendency. Hence in this the colours like krishna and aruna are associated
with Panduroga.
Due to the vitiation of Vata the person suffers from kampa, parshwashoola,
shirogourava etc., apart from the above features we can also note some other
features in vathaja Panduroga like nakhachippitathe, nakhabhangrurathe etc.,
Pittaja Pandu:
Pittaja Panduroga occurs to those who are usually of pittaja tendency where
severe aggravation of Pitta is present.
Kaphaja Pandu lakshana
Kaphaja Panduroga usually occurs in those persons who are usually of
kaphaja tendency. Here Kapha will be severely associated with Pitta dosha resulting
in the causation of Panduroga Kapha will be aggravated in Dhatus and vitiates
mainly rasa and Rakta resulting in Dhatu shaitilyatha. This further leads to conditions
like balakshaya, sneha kshaya, Varna kshaya and ojokshaya.

Literary review - Nidana 32
Showing the lakshana of vataja Pandu35
S.No Lakshana Charaka Susruta Vagbhata
1 Krishna panduta + - -
2 Krishna nakatwa - + -
3 Aruna nakatwa - + -
4 Krishana Akshitwa - + -
5 Krishna siratwa - + -
6 Shrama + - +
7 Rookshangata + - -
8 Arunangata + - -
9 Rukshanetrata - + -
10 Angatoda + - +
11 Angamarda + - -
12 Kampa + - +
13 Parshwaruk + - +
14 Shiroruk + - +
15 Asyavairasya + - +
16 Shofa + - +
17 Balakshaya + - +

Literary review - Nidana 33
Showing the lakshana of Pittaja Pandu36
S.No Lakshana Charaka Susruta Vagbhata
1 Gatrapeetata + - +
2 Harita + - +
3 Peeta sira - + +
4 Jwara + + +
5 Daha + - +
6 Trishna + - +
7 Chardi + - -
8 Sweda + - +
9 Amlodgara + -
10 Dourabalya + -
11 Peetomutrata + +
12 Shosha + -
13 Peeta vitkata + +
14 Binna varchastva + -
15 Shopa - -

Literary review - Nidana 34
Showing the lakshana of Kaphaja Pandu37
S.No Lakshana Charaka Susruta Vagbhata
1 Shwethavabasatha + -
2 Shuklakshita - + +
3 Shuklanakataha - + +
4 Shuklananathva - + +
5 Gourava + + +
6 Moorcha + - -
7 Bramaha + - -
8 Shwasa + - -
9 Alasya + - -
10 Shwayathu + - -
11 Shuklamootratva + + -
12 Shuklavarchaskatha + + -

Literary review - Nidana 35
Sannipathaja lakshana
If the vitiation of all the dosha is equally severe then it may be resulting in
tridoshajnya Panduroga. This causes severe degree of Dhatu shaitilyatha and
dhatugourava from which deterioration of Dhatu and Ojas occurs very rapidly. We
can find the features of sannipataja Panduroga in Harita Samhita only. Others have
sated the manifestation due to the degree of variations In the doshic imbalance, this
Panduroga considered as Asadhaya.
Tridoshajanya Panduroga lakshanas as stated by Harita38 -
1) Tandra
2) Alasya
3) Shotha
4) Vamana
5) Kasa
6) Hrullasa
7) Shosha
8) Vitbadha
9) Parusha
10) Jwara
11) Kshudarta
12) Moha
13) Trushna
14) Klama
Mritbhakshanajanya pandu lakshana39
A separate or a unique explanation of this condition is seen in Charaka
Samhita. Susruta has included this condition is sannipathaja Panduroga only.
Mritbhakshana or consumption of mud or soil is a peculiar condition in which it
causes Panduroga only. That is why Vijayarakshitha has quoted this instance of
occurrence of Panduroga due to mud eating and here soil eating is to be considered
as Vyadhi karana. Consumption of soil vitiates all the three doshas in the body. If the
soil is kashayarasa, then the increase of Vata can be observed. Like wise if it is
katurasa then of Pitta or if it in madura rasa then the increase of Kapha can be
observed in the Panduroga.

Literary review - Nidana 36
1) swatantra Panduroga. Where the condition has appeared as a specific
disease entity, and
2) paratantra Panduroga where the Pandu appears as a clinical feature or
complication of other disease like pittija pratisyaya, pittija kosha, pittarsha,
pittija promeha, grahani krimi roga, sosha, etc.
Table for classification of Pandu in different Samhita
S.no Name of the Pandu CS SS AH AS BP VS MN HS
1 Vataja + + + + + + + +
2 Pittaja + + + + + + + +
3 Slesmika + + + + + + + +
4 Sannipataja + + + + + + + +
5 Mridvakshanaja + - + + + + + -
(CS = Charaka Samhita, SS = Susruta Samhita, AH = Astanga Hridaya,
AS = Astanga Sangraha, BP = Bhava Prakasha, VS = Vanga sena
MN = Madhava Nidana, HS = Harita Samhita)

Literary review - Nidana 37
Samprapti of Pandu and its co-relations
Ayurveda believes in the doshika theory for creation of any type of disease
according to our classics there is three dhosas namely Vata, Pitta and Kapha in our
body. As long as these doshas (humors) are in complete harmony, body is in normal
condition and as soon as they imbalance, any kind of disease is produced40. This
imbalance state is usually because of the vitiation of a particular dosha or in
combination of other, leads to the production of disease, is known as Samprapti.
According to Vagbhata Samprapti is the process of the disease, which deals
with the process of vitiation of doshas, which spread all over the body and with the
manifestation of the sign and symptoms of a disease. Thus the study of the entire
changes taking place in the body under the influence of the etiological factors leading
to production of disease is known as "Samprapti"41. It deals with the body changes
both in the clinical as well as sub clinical stages of the disease.
According to Charaka, due to intake of Pitta prdhana tridosha prakopak Ahara
and Vihara, the Pitta (Sadhakapitta) which is situated in the heart is excited and this
excited Pitta throws away from the heart via ten dhamanis with the help of vitiated
vayu. Then it wanders through out the whole body and finally takes
(sthanasamsraya) in the space between skin and muscle and they're by vitiating
Kapha, Vata, Rakta, Twak and Mamsa and producing Pandu varna (pale coloration),
haridra varna (deep yellow colour), Harita varna (greenish colour), etc. the skin42.

Literary review - Nidana 38
Samprapti according to Charaka in summarized form43
Pitta pradhan tridosha prakopak nidan sevan
Agni vikar and rasa dusti
Dosha prakopa (mainly Sadhakapitta inside heart)
Prasara via srotas by vayu
Dhatu dusti (vikriti)
Dhatu kshaya (raktalpata)
Panduta (discoloration of skin)
Susruta has distinctly subdivided the entire process of the production of disease
in to six stages and has termed as " shat Kriyakala". These stages have importance
from both diagnostic and treatment point of view. These six stages of progression of
pathology are44 -
sanchaya (accumulation)
prakopa (excitation)
prasara (spread)
sthana samsraya (localization)
vyakti (manifestation)
veda (complication)

Literary review - Nidana 39
Sanchaya:
In Panduroga due to excessive intake of paittika Ahara - Vihara, the Pitta
dosha will be vitiated which accumulates in its chief site i.e., Amashaya. Here this
person may develop mild symptoms in the form of ichha and dwesha, which means,
he may like the sheeta and madhura dravyas and dislikes ushna and tikshna
dravyas. If person recognizes these instincts (likes and dislikes) and acts accordingly
the dosha will come back to their normal condition, on the other hand if they are not
recognized and the patient continue to indulge in Pitta vardhak Nidana; the doshas
increase again.
Prakopa:
In Panduroga due to continuous indulgence of paittika Ahara - Vihara, the
Pitta dosha increase further and spread to many of their own sites like Yakrit, Pleha,
twaka, drika etc. and produce its own specific symptoms in all places. These are
moderate in nature, the person feels that he is not well but goes about his daily
routine. He can easily get over this abnormality by suitable adjustment in foods,
activities and simple drugs and remedial measures by consulting physicians.
Negligence in appropriate action leads to the next stage of abnormality.
Prasara:
In Panduroga excited Pitta dosha enter in to the Hridaya (Hridaya
samvasthitam) by leaving its original sites i.e. Yakrit, Pleha, twak etc. after reaching
Hridaya, this excited Pitta dosha spread to all over the body through dhamanies with
the help of vayu. Here the person develops some powerful symptoms. If effective

Literary review - Nidana 40
treatment become available the doshas will come back to normal. If the person
continues to indulge the same etiology, or if treatment is ineffective, the abnormality
continues further to the inset of the fourth stage.
Sthanasamshraya
The fourth stage of Kriyakala is also as Sthanasamshraya. At this stage
dosha - doosya samorchhana occurs. The increase doshas, which were higher to
travelling all over, the body mixed with the circulating rasa Dhatu. Now tend to
localize in the particular tissue, organ or system because of early symptoms of the
specific disease start manifesting
Vyakti:
This is the stage of full manifestation of specific disease with all its
characteristic of specific disease with its entire characteristic sign and symptoms. In
case of Panduroga, after the localization of vitiated Pitta dosha in between twak and
Mamsa, the specific sign and symptoms of Pandu like pale yellow and greenish and
different types of discoloration of skin develops.
Bheda:
In this stage the body forces may arrest the pathological process and disease
may subside or it may be passed to sub acute or chronic stage or stage of
complication may begin.

Literary review - Nidana 41
Co-relation:
Vatika Pandu:
Although Pitta plays main role in the development of Pandu but Vata dosha is
also vitiated in the process of pathogenesis. It acts along with Pitta on the Rakta
Dhatu, so that they absorb fluid portion of the cell and as a result cell assumes
smaller size. Thus the vatika Pandu may be correlated with the microcytic anemia
and other anemia's having disorders in the shape of RBC like sickle cell anemia.
Paittika Pandu:
In this type of Pandu, there is a disturbed metabolic activity of the
erythrocytes due to increased metabolic activity. So there is no proper formation of
blood and on the other hand there is accumulation of waste products (mala
Sanchaya). Thus in patient of paittika Pandu, there is increased haemolysis due to
break down of R.B.C. as Pitta is predominantly acting on the Rakta so there is more
and more haemolysis. Hence the size of red cell and hemoglobin concentration is
same but the number of red blood corpuscles remains low. So the paittika Pandu
may be correlated with normocytic anemia.
Kaphaja Pandu:
Kapha and Pitta are antagonistic to each other, one being of sheeta guna
other of ushna guna. Thus the sheeta quality of Kapha is neutrialized by ushna guna
of Pitta. In Kapha fluid portion is more, hence more and more fluid is absorbed by the
cell and assumes large size. Therefore kaphaja Pandu may be correlated with
macrocytic anemia.

Literary review - Nidana 42
Sannipataja Pandu:
When all doshas are involved and act together, naturally it will produce
different types of cells. When there will be more activity of Kapha, the cells assume
large size and when Pitta activity is more, the cells remain normal and when Vata
activity is more, it assumes smaller size. So there will be anisocytosis and
polikilocytosis. This type of pandu may be correlated with mixed type of anemia
having dimorphic picture.
Mrid bhakshana janya pandu :
In this condition any of the three doshas may be vitiated according to nature
of the clay and doshas when vitiated will produce corresponding types of Pandu.
Ayurveda Nidana Chikitsa ka sidhanta by prof. R.H. Singh, it is clearly
mentioned that after eating of Mrit (soil) the worms are created in side abdomen and
hamper the absorption of the nutrition's and ultimately iron deficiency anemia.
Modern medical science also believe that pica (i.e. eating of clay) is the one of the
major factor for iron deficiency anemia45.

Literary review - Nidana 43
Factors of Samprapti
I. Dosha
a. Pitta dosha -
Pitta is the chief factor responsible for Panduroga. Before explaining the
pathological process of the doshas it is ideal to briefly know its physiological function
in the body.
Generally Pitta dosha is responsible for various functions like vision
(darshana), digestion and metabolism (pakti rushma), appetite (kshut), thirst
(thrishna), unctuousness (deha mardava), complexion (prabha), intellectuality (meda)
etc.,
Pitta dosha, which is situated in the Amashaya, is responsible for nourishing
and regulating the subsidiaries like Sadhakapitta, Ranjakapitta, and Alochakapitta
and Bhrajakapitta. These varieties have their definite and specific actions in the body.
In Panduroga Pitta dosha attain morbidity due to Nidana sevana. There at
first the Pachakapitta is the target of morbidity and this morbid and increased Pitta
transforms the poshaka rasa into the state of amavastha and circulates all over the
body along with it, in this process it vitiates other Pitta and other doshas etc.
The Pachakapitta which itself is excited and morbid fails in its own functions
and also in the nourishment of other Pitta in the body. The process of digestion is

Literary review - Nidana 44
suffered and metabolism is impaired. The desire for the food is lost, the thirst
increased, the complexion is changed and the intelligence interfered.
It may not be out of place here to mention that the modern medicine
postulates the importance of castle intrinsic factor in the absorption of vitamin B12 (an
extrinsic factor). Which is essential for the synthesis of erythrocytes that is from the
proerythroblastic phase. This intrinsic factor is present in the gastric mucosa and in
the normal gastric juice. This is an enzyme like unidentified substance secreted by
stomach.
The factors responsible for the erosion of gastric mucosa and for the altered
pH of gastric juice may lead to the absence of intrinsic factor leading to pernicious
anemia.
In Ayurveda the highest importance is given for the maintenance of
Jatharagni which in other words can also be called as Pachakapitta. If this Pitta is
normal then the digestion and metabolism of the food material is proper. If this
paktirushma is disturbed due to various extrinsic factors like consumption of madya,
katu, rooksha, teekshana aharas leads to the khavaigunya in the Amashaya. Due to
the above cause the walls of Amashaya (gastric, mucosa) is impaired due to
khavaigunya in the Amashaya, the Ahara rasa will not be digested and absorbed
because it attains Ama roopa. In this context we can quote the reference of
chakrapani who mentions "raktaposhaka sarabhaga anutpadana" or the non-

Literary review - Nidana 45
production of Rakta poshaka rasabhaga in the Amashaya is one of the chief cause of
Panduroga.
As explained earlier the remaining Pitta like Sadhaka, Ranjaka, Brajaka get
involved in the causation of Panduroga. The Ranjakapitta, which is situated in Yakrit
and Pleha, is responsible for the coloration of Rasadhatu. The Yakrit and Pleha are
the seats of Raktavaha Srotas vitiation of Ranjakapitta leads to the impaired
coloration of Rakta Dhatu.
The modern physiology says that the bile pigments and the chlorophyll are
necessary for the hemoglobin formation. The two chief constituents of bile pigments
are billirubin and biliverdin, which is present in bile. The old and worn out RBCs
disintegrated and they are removed from the circulation through the cells of reticule
endothelial system. The bone marrow appears to be the most active site.
Hemoglobin is released by the degradation and is broken into amino acid, which
enters the general amino acid pool In the formation of new hemoglobin. The rest of
the haem is converted into yellow pigment.
The deficiency of bile pigment and chlorophyll leads to the loss of hemoglobin
formation and therefore leads to hypo chromic anemia.
As said earlier the mala of Rakta is known to be Pitta. Though it is very
difficult to establish this malaroopa Pitta as bile itself, yet basing on the available
references we can say that bile is one of the chief constituents of Rakta Dhatu

Literary review - Nidana 46
(RBC's) which are old and damaged. These are disintegrated in Yakrit and Pleha and
are broken down. If the Pitta is provoked in Yakrit and Pleha then again the
malaroopa Pitta is increased and these may ultimately interfere in the formation of
Rakta through rasa ranjana, where bile pigments are affected and ultimately cause
Pandu or hypo chromic anemia.
After the vitiation of Pachakapitta and Ranjakapitta the next target is the
hridistita Sadhakapitta. Due to alpa raktata the Hridaya which is responsible for the
circulation is strained and the cardiac effort will be increased. Due to this the
Sadhakapitta is influenced by the vitiated Rakta and is circulated all over the body
and locates in vitiated twacha and Mamsa, when Sadhakapitta is vitiated and located
between twak and Mamsa is further influenced on Bhrajakapitta of twacha. The
Bhrajakapitta, which is already, affected from the lack of nourishment (due to
Pachakapitta vitiation) its functions like prabha and Varna are interfered leading to
Pandutha of the skin.
b. Vata dosha
The vayu is the chief factor in the body for initiation of all the activities.
Vitiated vayu is responsible of the expulsion of Sadhakapitta from Hridaya to dasha
dhamanies. Here vayu is responsible for manifestation of various signs and
symptoms due to Dhatu kshaya and margavarodha. In the pathogenic process
Samanavata may play an important role in the vitiation of Pachakapitta likewise due
to rakthalpata Vyanavata may be increased in the body and this further increases the

Literary review - Nidana 47
cardiac effect and the function of Hridaya impaired. On the causation of vathaja
Pandu Charaka mentions the person who consumes the food materials which
provoke Vata may suffer from vataja Pandu by manifesting the signs and symptoms
like rookshatha, angamarda, kampa, parshwaruk, shotha, balakshaya and krishna
pandutwa. The prevalence of vathaja Pandu is seen in those who are known to be of
vathaja tendency.
c. Kapha dosha
The role of Kapha in Panduroga is again to be discussed on the basis of the
association in this disease, Kledakakapha and Avalambakakapha are the chief
factors for the causation of Panduroga.
Incase of kaphaja Panduroga Charaka mentions some of the important
features like shwasa, kasa, aruchi, vakgraha, brama, klama, moorcha. The
prevalence of kaphaja Pandu is more in those persons of kaphaja tendency.
II. DOOSHYAS
a. Rasa
It is interesting to know the involvement of Rasadhatu in the occurrence of
Panduroga. Physiologically the function of Rasadhatu is attributed to nourishment
(preenanam) and also helps nourishment. If this Dhatu is efficient then it is not only
nourishes itself, but also helps to nourish the other Dhatus of the body. And its
upadhatus like twacha and Lasika. In case of Panduroga rasa Dhatu is basically

Literary review - Nidana 48
influenced by the vitiated Pitta dosha and attains the amaroopa due to coming in
contact with the amaroopa poshaka rasa. In this stage instead of its normal functions
of Rasadhatu results in the form of Dhatu shaitilya, from which the integrity in the
functions of rasa Dhatu and other Dhatus will be lost and later results in Shareera
gourava. This ultimately fails in the nourishment of twacha and may result in
rookshatha and vaivarnya.
b. Rakta Dhatu
In fact the Dhatu that has direct bearing with Panduroga though in the earlier
reference it is mentioned that Rasadhatu is involved. The function of rasa ranjana is
interfered in the raktavaha srothamoola i.e., Yakrit and Pleha. The result of the
interference is alparakata, nissarata, vaivarnyata, indriya shaitilyatha in the body. The
Rakta alpata either may be directly due to the involvement of Yakrit and Pleha or
indirectly it is affected due to the failure mechanism of Jatharagni. At this juncture the
importance of Pleha in its subtle control over the bone marrow in the RBC formation
is to be noted.
III. The role of Agni
The independent study of Agni is equally essential for the study of Panduroga. It
is of 4 types -
1. Doshagni
2. Jatharagni
3. Dhatwagni
4. Panchabhootagni

Literary review - Nidana 49
1. Dhoshagni
The Pitta doshagni is responsible for complexion digestion and metabolism in
the body at different levels. The Agni constituent of Pitta dosha is severely impaired
due to which the doshas is impaired in the body leading to increased amaroopi dosha
in the body.
2. Jatharagni
This is basically, impaired in the body resulting in the formation of Ama. This
is directly responsible for Pandu due to khavaigunya in Amashaya and has indirect
influence on other Agnis to cause Pandu due to Ranjakapitta dushti.
3. Dhatwagni
The dhatwagni especially rasa dhatwagni and Rakta dhatwagni are impaired
due to amaroopi poshakarasa. Hence the twacha loses its integral functions. Rakta is
deteriorated in its functions in the body.
4. Panchabhootagni
The tejamsha of the tejo mahabhoota is interfered in Pandu and the ap-
bhutagni is associated with it. As the tejoagni is impaired the digestion and
metabolism, the complexion of the body is impaired. In the due course the ap-
bhootagni is associated due to which the person may suffer from shotha.

Literary review - Nidana 50
IV. Ama
The non-homologous undigested substance can be called as Ama. In
Panduroga, the Ama may be formed due to the impairment of Jatharagni, doshagni
and dhatwagni etc.
V. Srotas
The important srotas, which are involved in panduroga, are -
1) Rasavaha srothas
2) Rakthavaha srothas
1. Rasavaha srotas
Here the Hridaya is involved along with dasha damanies and the functions of
this is impaired leading to various signs and symptoms.
2. Raktavaha srotas
The Yakrit and Pleha are the chief organs involved in Panduroga where
Ranjakapitta is vitiated.
VI. Pandu as Rasa pradoshaja vikara
Both Charaka and Susruta considered pandutwa and Panduroga in
rasapradoshajavikara. Before explaining the rasapradoshaja vikaras, Charaka has
told that the vikaras are caused by the vitiated doshas, which affects the rasadi
dhatus. Apart from this in the context of graham while explaining amothpatti he has
told that when rasadhi dhatus are affected by Ama dosha it leads to rasaprdoshaja

Literary review - Nidana 51
Vyadhi while commentating on the word 'rasadoshaja' told by Susruta, Dalhana says
that -
"rasadoshaja iti doshadushitha rasajathna"
It means the disease produced by the vitiated doshas that affects rasa.
So the disease Pandu is included in rasa pradoshaja Vyadhi because it is
manifested due to the vitiation of rasa Dhatu by vitiated vatadi doshas and Ama
dosha.
The Panduroga lakshanas explained in the classics are almost similar with
that of dhatukshaya lakshanas. By this it is evident dhatukshaya leads to Panduroga,
because through rasa dhatu other dhatus are nourished. Here in Panduroga
dhatukshaya may occur after the manifestation of the disease not only directly Rakta
and its srotases involves in this diseases but also other srotases such as rasa,
medhas, etc., when they are under diminished condition gives rise twak roushyata,
etc.,

Literary review - Nidana 52
Upadravas of Panduroga46
Roga arambhaka dosha prokopajanya vikara is known as Upadrava of that
particular disease. Any factor which is early part causes development of disease, if
the same factor is later part produces any other severe manifestation then it is called
as Upadravas (complications), in Ayurvedic classics the various complications are
available. These are aruchi (anorexia), jwara (pyrexia), pipasa (thirst), agnisada
(maldigestion), moordha jura, chhardi (vomiting), murchha (fainting), abalatwa
(weakness), shotha (oedema) klama (nuresthenia), hridayawapidanam (pre-cardial
pain), kasa (cough), shoola (pain), avipaka (improper digestion), atisara (diarrohea),
daha (burning sensation) swarabheda (obstruction of speech), shwas (dyspnoea).
The symptoms are described above when aggravated require special
management but few of them usually may be more important and require more
attention.
Moordha ruja - It is due to increased Kapha and Vata. When there is lack of blood
formation due to dysaemopoiesis. It is like sub acute combined degeneration as
obtained in pernicious Anaemia.
Murchha - It is due to increased activity of Pitta. There is more and more blood
destruction and in turn fainting (murcha) may develop.
Hridayawapidanam - It is due to excessive loss of rasa and Rakta. Heart has to
perform more activity for the compensation of the blood supply of the whole body. If

Literary review - Nidana 53
this condition is continued for long time, the heart may be dilated and this may
develop the symptoms of precordial pain.
Shotha - Due to loss of blood, there is hypoproteinaemia which in turn may produce
shotha (oedema).
Kasa - It is due to the loss of blood and increased activity of Kapha, because of it
kasa may develop.
Atisara - It is due to aruchi (anorexia) and avipaka (improper digestion) atisara may
develop.
Swasa - Due to severe loss of blood, there is anoxia, which simulates the respiratory
center, and breathing is increased.
Daha (burning sensation) - It is due to diminution of rasa and Rakta and increased
activity of Pitta, symptoms of daha may develop.
Prognosis of Pandu (sadhyasadhyata)
The disease Pandu leads to balakshaya and person becomes nihsar. So the
body immunity of the person is reduced. If the disease is severe and untreated it may
be fatal.

Literary review - Nidana 54
Sadhya - Asadhyata of Panduroga47
Sadhya lakshana
1. Diseases which are caused with less causative factors
2. Which are created with unequaled in nature in dosha and dushya, dosha and
prakruthi, dosha and kala, dosha and dushya.
3. Which is situated in any one out of shaakha, marma asthi sandi and koshta.
4. Which is new and without any complication
5. Which arises from one dosha
6. The patients body which is capable of taking all kinds of medicine.
The above features are considered to be sadhya for the management of Panduroga.
Asadya lakshanas
1. A chronic Shotha in a due course in whom the eyes are looking peethabha.
2. A chronic and deteriorated person
3. The person who is suffering from Atisara or who is passing stools with Kapha and
is haritha in its colour.
4. The person who is suffering from severe degree of pallor due to Rakta kshaya.
5. The person who is suffering from Chardi, Moorcha
6. Occurrence of Shotha in the dependent parts
7. Occurrence of Shotha in the abdomen

Literary review - Nidana 55
20 Charaka Samhita Chikitsa 16/7-8 21 Susruta Samhita Uttara 44/3 22 Susruta Samhita Nidana 11/17 23 Susruta Samhita Shareera 2/21 24 Charaka Samhita Chikitsa 2/27 25 Susruta Samhita Shareera 6/27 26 Harita Samhita 3-9-39 27 Susruta Samhita Shareera 9/12 28 Charaka Samhita Chikitsa 16/7-11 29 Susruta Samhita Uttara 44/3 30 Astanga Hridaya Nidana 1/3-4 31 Charaka Samhita Chikitsa 16/12 Susruta Samhita Uttara 44/5 Astanga Hridaya Nidana 13/8 Astanga Sangraha Nidana 13/9 Madhava Nidana 8/3 32 HaritaSamhita 3/8 Vangasena Panduroga /2 33 Charaka Samhita Chikitsa 16/17-30 Astanga Hridayam Nidana 13/7 Madhava Nidana 8/1 Yogaratnakara Panduroga Nidana /1 34 Susruta Samhita Uttara 44/4 35 Charaka Samhita Chikitsa 16/17-18 Astanga Hridayam Nidana 13/8-10 Susruta Samhita Uttara 44/7 36 Charaka Samhita Chikitsa 16/19-22 Astanga Hridayam Nidana 13/10-11 Susruta Samhita Uttara 44/8 37 Charaka Samhita Chikitsa 16/23-25 Astanga Hridayam Nidana 13/11-12 Susruta Samhita Uttara 44/9 38 Harita Samhita Panduroga Chikitsa 8/10 39 Charaka Samhita Chikitsa 16/27-30 Astanga Hridayam Nidana 13/13-14 40 Charaka Samhita sutra 3/3 41 Astanga Hridaya Nidana 1/8 42 Charaka Samhita Chikitsa 16/9-11 43 Ibid 16/4, 9-11 44 Susruta Samhita Sutra 21/36 45 Auartely medical review. Vol. 47 no-2 april, 1996 46 Susruta Samhita Uttara 44/13 47 Charaka Samhita Chikitsa 16/31-33 Susruta Samhita Sutra 33/23 Madhava Nidana 8/12-15

Literary review - Contemporary science 55
The most important function of the red cell is the transport of hemoglobin,
again important function of hemoglobin is to supply of essential oxygen to all cells
tissues of the body and to maintain normal colour of skin and mucous membrane.
The most common and important disorder associated with the disease of the red cell
is Anaemia, which defined as qualitative and quantitative deficiency of R.B.C count
and or hemoglobin percentage in relation of standard age and sex.
There are endless causes of Anaemia. But iron deficiency is the commonest
cause of Anaemia. It is also the commonest nutritional disorder in humans and widely
prevalent almost all over the world although more common in the developing
countries like ours.
Classification of Anaemia
Anaemia can be classified in different way but the etiological and
morphological classification is most important.
Etiological classification of Anaemia
From etiological point of view Anaemia can be classified into three sub groups
1. Anaemia due to deficient supply of nutrients or pre modular causes - these
includes deficiency of high protein diet, iron, Vitamin B12, folic acid, vit. C etc.
2. Decreased production of red cell or medullar cause - it includes leukemia,
Aplasia, chronic infection, rheumatoid arthritis etc.
Literary review - Contemporary science 56
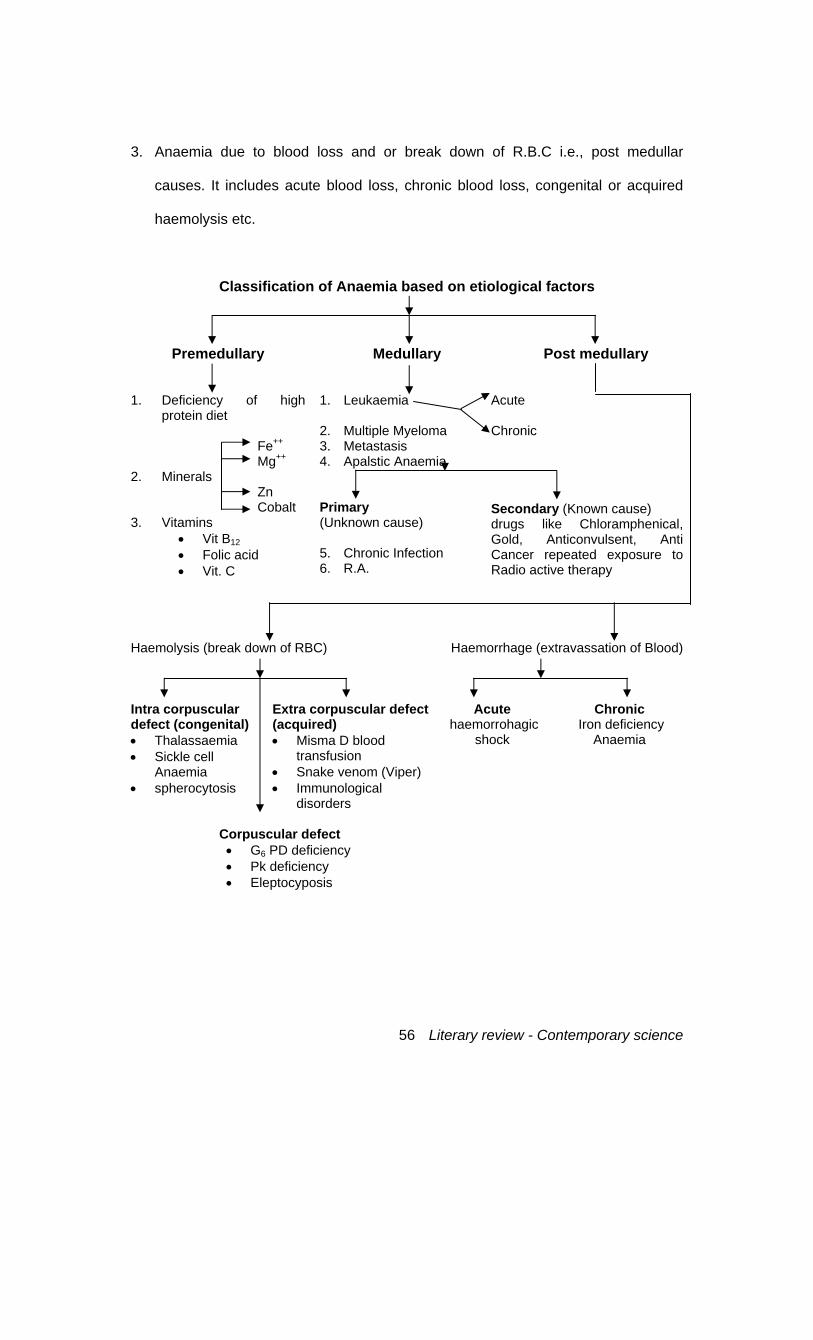
3. Anaemia due to blood loss and or break down of R.B.C i.e., post medullar
causes. It includes acute blood loss, chronic blood loss, congenital or acquired
haemolysis etc.
Classification of Anaemia based on etiological factors
Premedullary Medullary Post medullary
1. Deficiency of high protein diet
Fe++ Mg++
2. Minerals Zn Cobalt
3. Vitamins • Vit B12 • Folic acid • Vit. C
1. Leukaemia 2. Multiple Myeloma 3. Metastasis 4. Apalstic Anaemia Primary (Unknown cause) 5. Chronic Infection 6. R.A.
Acute Chronic
Secondary (Known cause) drugs like Chloramphenical, Gold, Anticonvulsent, Anti Cancer repeated exposure to Radio active therapy
Haemolysis (break down of RBC) Haemorrhage (extravassation of Blood)
Intra corpuscular defect (congenital) • Thalassaemia • Sickle cell
Anaemia • spherocytosis
Extra corpuscular defect (acquired) • Misma D blood
transfusion • Snake venom (Viper) • Immunological
disorders
Acute haemorrohagic
shock
Chronic Iron deficiency
Anaemia
Corpuscular defect • G6 PD deficiency • Pk deficiency • Eleptocyposis

Literary review - Contemporary science 57
Morphological classification
Anaemia can be classified in terms of the appearance of the red cells. There are
three major types of Anaemia:
1. Hypochromic microcytic with a low mean corpuscular volume ( M.C.V.).
2. Normochromic normocytic with a normal ( M.C.V.).
3. Macrocytic with a high ( M.C.V.).
Summary of iron balance (in our body)
The iron balance may be summarized (In adult) as follows:
Input Body Iron Output
Male Average : 1mg/day derived from foods a) animal muscle b) Vegetables - the
average diet contains 10 to 20 mg Iron of which about 10% is absorbed.
N.B. for Female it is about 2mg.
Total 3 to 6 gms. a) functional Iron in haemoglobin myoglobin 80% at least enzyme systems transferrin b) storage Iron in Liver, Spleen, Bone marrow 20% as Ferrritin and or less Hemosedarin
Average 1mg/day Skin desquamation and miscellaneous secretion Menstruation This extra loss of about 0.5 to 1 mg requires extra input in the females
Iron deficiency Anaemia results when this delicate balance is upset in one of three
main ways, described below:
1. In creased output: this almost always occurred by blood loss - often small in
amount and chronic (1 ml blood loss = .5mg iron). In the female uterine bleeding
is a common cause and in both sexes bleeding from the alimentary tract is
important.

Literary review - Contemporary science 58
2. Decreased input:
A) Poor diet (including diets containing substances antagonistic to iron
absorption e.g., phytates pbhosphates).
B) malabsorcption - due to bowel disease or post surgical.
3. Increased body requirement:
a) During rapid growth in childhood.
b) In pregnancy
Usually Anaemia develops slowly (except in case of serious hemorrhage)
Iron of deficiency
Metabolisation of reserves (First hemosedarin then feratin)
Exhaustion of reserves Increased absorption of available in diet may postpone
Deficient synthesis of hemoglobin
Anaemia
Iron deficiency Anaemia
Anaemia due to deficient of iron in the body is known as iron deficiency
Anaemia. The exact prevalence of iron deficiency Anaemia is difficult to define.
Morphologically it belongs to hypochromic microcytic group.

Literary review - Contemporary science 59
Hypochronic microcytic Anaemia
Due to Iron deficiency Other than Iron deficiency
Sideroblastic Anaemia Thalassaemia Anaemia of chronic disorders
Causes of iron deficiency:
Iron deficiency Anaemia develops when there is an inadequate amount of iron for
hemoglobin synthesis. A normal level of hemoglobin is maintained for as long as
possible until all the iron stores are depleted; during this time latent iron deficiency is
said to be present -
Poor intake
Decreased absorption
Increased demands
Blood loss
Most iron deficiency occurs from blood loss. Pre menopausal women are
always in a state of precious iron balance owing to menstruation. Nutritional iron
deficiency is rare in developed countries. In UK, it is sometimes see in vegetarian.
Asian women eating chapatis containing phytate. The commonest cause of iron
deficiency worldwide is blood loss from gastrointestinal tract due to hook work
infestation.

Literary review - Contemporary science 60
The causes vary with the age and sex of the patients. Careful consideration of
the clinical features, especially of the history, will establish the causes in many cases,
but further investigation is often necessary.
Major etiological factors in iron deficiency:
1) Females in the reproductive period of life
• Menstruation
• Pregnancy
• Lactation
• Pathological blood loss
• Deficient diet
2) Adult males and post menopausal females
• Pathological blood loss
• Deficient diet
3) Infant and children
• Deficient diet
• Diminished iron stores at birth.
4) chronic gastrointestinal blood loss due to
• peptic ulcer
• haemorrhoids
• hiatus hernia
• carcinoma of the stomach
• carcinoma of the colon
• chronic aspirin ingestion
• oesophageal varics
• ulcerative colitis
• hook worm infestation

Literary review - Contemporary science 61
Clinico pathological changes
Changes in Anaemia
Haematological Non haematological (epithelial tissue changes)
a) blood picture -
i) R.B.C. ii) W.B.C. iii) Platelet
b) Bone marrow - c) Biochemical findings
a) Angular cheilosis and atrophic glossitis b) Dysphagia c) Gastric mucosa d) Koilonychia e) Minimal changes in peripheral nerve
A. Hematological
a. Blood picture
1. R.B.C
Changes in the blood are mainly in the red cells which become microcytic (cells
smaller-mean diameter <6.7) and hypochromic (contain less hemoglobin i.e., less
well stain).
The M.C.V. (f1) (mean cell column) is low <80
The M.C.H. (Pg) (mean cell hemoglobin) is low<25
The M.C.H.C. (mean corpuscular hemoglobin concentration is low<30%
(Normal = 34%)
The serum iron (normal 13-32 u mol/ 1) is raised>70 (2.5-4.0mg.1)
The bone marrow is hyper cellular and contains many small poorly haemoglobinised
normoblast. No stainable iron is present.

Literary review - Contemporary science 62
2) W.B.C
The white cell count and differential are usually normal. Macropolycytes are
often found.
3) Platelet
The platelet count is usually normal but may be slightly to moderately increase
especially in-patients with hemorrhageic or hemolytic manifestation.
b. Bone marrow
The bone marrow is hyper cellular and contains many small poorly
haemoglobinised normoblast. No stainable Iron is present. Haemosiderin store is
depleted. Macropogcytes are found a few.
c. Bio - chemical findings
the level of serum iron is decreased due to deficiency in total amount of iron present
in the body. The level of serum iron is reduced to values usually ranging from 2.5 to
10u mol/1 and the total iron binding capacity (TIBC) of the serum is increased
sometimes upto 100u mol/1
normal values ;
serum iron ; 60 - 150ug/100ml.
Serum TIBC ; 270 - 380ug/100ml
B) angular cheilosis and atrophic glossitis ;
Fissures at angles of mouth is occure and atrophy of the papillae of tongue resulting
in pale, smooth, shiny and glazed tongue.

Literary review - Contemporary science 63
c) dysphagia ; difficulty in swallowing due to constriction at the entrance of
oesophagus and incordinate movements in pharynx. Desquamating epithelial
cells forms.
d) Gastric mucosa ; here the gastric mucosa become thin. Gradually
hypochlorhydria and achlorthydria occurs. This aggravates any malabsorption
of iron.
e) Koilomychia ; dystrophy of the finger nails in which they are thinned and
concve, with raised edges occurs. This also known as brittle spoon-shaped
nails.
f) Minimal changes in periferal nerves ; causing paraesthesia. Here thing ling in
hands feet occur.
PATHOGENESIS
Anaemia develops usually when the supply of iron is insufficient for the
requirements of haemoglobin synthesis when iron balance becomes nagative,
the deficit is made good by iron mobilized from tissue stores and an adequate
supply of iron for haemoglobin formation is maintained. It is only when the tissue
stores are exhausted that the supply of iron to the marrow for haemoglobin
synthesis becomes inadequate and hypochronic anaemia develops
Thus iron deficiency may be regarded as developing as two stages ;
a) the progressive depletion and ultimate exhaustion of available tissue iron
stores and
b) the development of anaemia.

Literary review - Contemporary science 64
This increased demand occurs in children during the peiod of growth and in
women during their reproductive period of life.
During the period of growth, there is a progressive increase in the number of red
cells in the body and consequently in the total amount of haemoglobin. This
results in an increased demand for iron by the marrow for haemoglobin synthesis.
There is an additional, but much smaller demand for the synthesis of mioglobin in
the progressively increasing mass of other tissues. Growth is most rapid from the
age of 6-24 months, the time of the greatest incidence of iron deficiency Anaemia
in young children.
During the reproductive life of the memale, menstruation, pregnancy, parturition,
and lactation significantly increased the physiological requirements for iron. The
average monthly loss from menstruation is 15-28mg. Each pregnancy requires
about 500-600mg. For the fetus and to cover food loss parturition, although this is
partly compensated for by the absence of menstrual loss. Lactation causes
further demands even though the iron content of breast milk is relatively low.
Pathological blood loss.
Since 60-70% of the total iron content of the body is contained in the
haemoglobin of red cells, it is obvious that the loss of blood to any extent uses
lowering of the total body iron. The normal adult has tissue ironreserves sufficient
to replace between one-third and one-half of the circulating haemoglobin (see
table 3.1). once this reserve is exhausted, continued bleeding causes a state of
iron deficiency . blood loss from pathological lesions may cause iron deficiency
anaemia at all ages and in both sexes, but the development of iron deficiency

Literary review - Contemporary science 65
must be viewed specially seriously in adult males and in females after the
menpause in whom there is no physiological cause for the deficiency.
Inadequate intake.
Inadequate intake may result from either nutritional deficiency or impaired
absorption. In western countries inadequate intake is generally a contributing
rather than a sole causative factor, except in the presence of increased
physiological demand or haemorrhage.
Nutritional deficiency as a result of an inadequate diet is of major importance in
infants and young children. It may also occur in adults due to poor economic
circumstances, dietary fads or dislikes, and anorexia, specially in pregnancy.
Poor bioavailabilty of dietary non-haem iron is an important factor is an imprtant
factor in the third world.

Literary review - Chikitsa 66
When we examine the patient suffering from Panduroga it is to be analyzed that
the Pandu rogi will be curable or not? Because Acharya Charaka and Susruta has
described the treatment of sadhya Panduroga only48. The line of treatment in sadhya
Panduroga is as follows.
Chikitsa sutra
Initially Panduroga has to be unctuated with ghrita and when samyaksnigdhata is
attained the dosha have to be evacuated either with vamana or virechana according to
the necessity. When patient attains suddhakostata selected shamana aushadhi has to
be administered.
In general Pandu patient after having the unctuouation virechana is administered
as the Pandu is a pittaja vyadhi. For the virechana triphala ghrita with lodhra kalka or
any other virechana aushadhi with ghrita can be given49.
Acharyas has prescribed very specifically sneha prayoga in vataja Pandu to take
out roushyata of Vata, tiktarasa in pittaja Pandu as it creates saitya in the body and katu
rooksha ushna dravyas in kaphaja Pandu to rule out the effect of Kapha. Dwandwaja
and sannipataja pandu are treated with combinations and permutations according to the
necessity50.
Literary review - Chikitsa 67
Snehana
In Panduroga there is natural reduction in snehabhava of the body along with
raktalpata, alpamedaskata, nissara, ojaksheya etc., roukshatwa is appeared on whole
body therefore there is great necessity of snehana. Acharyas has prescribed the
snehana as abhyantara snehana as well as bahya snehana In Panduroga. The snehas
used for the treatment of Panduroga are given below51.
Panchagovya gritha
Mahatikta gritha
Kalyanaka gritha
Panchatikta gritha
Triphala gritha
Due to samyak snehana vatanulomana takes place Agni comes to its normal stage
snigdha varchaskata snigdhata and mardhavata is also found out52.
SHODHANA
Acharya Charaka has described the urdhwa as well as adhoshodhana in the
treatment of Panduroga. The shodhana to be assessed in those patients of Panduroga
in which vyadhibala, rogibala, degree of srotorodha in mridhbakshnajanya Panduroga
are in much severe form.
VAMANA
According to Dalhana mridu vamana can be given in the Panduroga with respect
to ritu, desha, kala, rogibala etc., where as charaka advised teekshna vamana.
Vamanartha dravya :
Kathakaphala or dhamargava,
ikishwaku kalpa,
kritevadana kalpa.

Literary review - Chikitsa 68
VEERACHANA
Virechana is the best shodhana karma of Pitta dosha. In Panduroga Pitta dosha
place a great role in Samprapti. Hence Virechana is the best and most acceptable
shodhanakarma in Panduroga.
Virechana prayoga :
Mridukosto rogi -
1. Godugdha or gomutrayukta dugdha up to 15 days. (Vagbhata)
2. Dantikwatha + gambari phala or draksha phala
3. Pittaja pandu - nishothara churna + dwiguna sharkara
4. Kaphaja pandu - aragwadha majja + trikatu churna
5. Vataja pandu - gomootra + haritaki churna
Panduhara grithas :
Charaka Samhita
• Dadimadi gritha,
• Katukadi gritha,
• Pathy gritha,
• Dantigritha,
• Drakshadi gritha
Susruta Samhita
• Haridra gritha,
• Darvyadi gritha,
• Bruhatyadi gritha
Vagbhata:
• Durlabhadi gritha

Literary review - Chikitsa 69
Dosha vishesha Chikitsa in tabular form53
1. Vataja pandu - snehabhuvistha
2. Kaphaja pandu - katu, tikta and ushna dravya
3. Pittaja pandu - tikta and sheetal proyoga
4. Sannipatika pandu - vimishrayoga proyoga
5. Mridbhakshanajanya pandu - mrittika bhakshana niverana , doshaja chikitsa
Other formulas:
• Novoyasa loha,
• Poonarnava mondura,
• Pandu panchanana,
• Mondura vataka,
• Monduradyaristha,
• Dhatrayarista,
• Lohasava,
• Tapyadi loha,
• Dhatrayavaleha
Bhasma :
• Loha bhasma,
• Swarnamakshika,
• Mondura, tamra
Importance of (Loha) iron in the treatment of Pandu:
Astanga Sangraha and Astanga Hridaya mentions importance of iron. Vagbhata
said that iron is superior drug for treatment of Pandu. Charaka, Susruta, Vagbhata,
Sarangadhara, Bhavamishra etc., all ancient authors mentioned many drug formulae
which contains iron or iron compounds for the cure of Pandu54.


Literary review - Chikitsa
Pathyapathya55 Pathya Ahara
Sukadhanya varga - purana shali, purana yava, godhuma
Shamidhanya varga - mudga mashara
Mamsa varga - jangala mamsa -matsya
Saka varga - patola vruddha, kushmanda, jivantika, vartaka,
Lashunadwayam, bimbi, punarnava and nagakesara
Phala varga - toruna, kadaliphala, abhaya, dhatri
Ikshu varga - ikshu rasa
Gorasa varga - takra, ghritha, navaneetha
Mutra varga - surabhi jala
Madhya varga - souviraka, tushodaka
anya dravya - guduchi, dronapuspi, haridra, chandana,
yavakshara and lohabasma
Apathya Ahara Rasa - kshara, amla, katu, lavana
Anna - virudha bhojana, asatmya bhojana
Jala - adhikambupana, dushitajala
Krtanna varga - pinyaka
Shamidhanya varga - masha, tila, kulatha, nishpava
Sneha varga - tila taila
Gorasa varga - dahi masthu
Madhya varga - sukto souviraka
Ahara dravyas - hingu, tambula, teekshnapadartha like,
krishna Maricha, vidhahipadratha, atiushnapadratha,
mrittbhakshana.

Literary review - Chikitsa
48 Susruta Samhita Uttara 44/14 Charaka Samhita Chikitsa 16/39 49 Yogaratnakara Panduroga Nidana 27 50 Ibid 26 - 28 Charaka Samhita Chikitsa 16/116 51 Charaka Samhita Chikitsa 16/43 Astanga Sangraha Chikitsa 12/ Astanga Hridaya Chikitsa 16/ 52 53 Charaka Samhita Chikitsa 16/116 54 Astanga Hridaya Uttara 4/41 55 Charaka Samhita Chikitsa 16/41-42 Susruta Samhita Uttara 44/ Harita Samhita Panduroga Chikitsa 8/34-36

Materials and Methods - Drug review 71
1. Guda
Sanskrit Guda
Hindi Gud
English Tracle, Jaggary
Kannada Bella
Synonyms Guda, Ikshusara, Madhura, Rasapakaja, Sishupriya,
Sitadi56,
Utpatti well-cooked sugarcane juice when solidifies and
becomes hard like stone is known as guda57.
Properties
Rasa madhura
Guna Laghu (purana Guda)
Doshaghnata Tridosha shamaka

Materials and Methods - Drug review 72
Uses58
Purana guda is said to be best because of its action over all dhatu vaha
samstana. It is agni vardhaka and ruchya, there by easily digests it self and
nourishes and kindles the Jatharagni. It is vrishya and also claimed as sadya
shukrala, in association with shukravardhaka dravya forms of sugarcane or
especially purana guda is prescribed. Its role on rakta and rakta vaha srotas
is remarkable. It enriches the production and shows the qualitative and
quantitative increase of the Rakta dhatu. It is also Hridya as its action
conferred on Rasa and Rakta reflects as such rasarakta complex is flown in
the hridaya and dashadhamani. It is said as mala mootra vikara shodhaka
and acts on prameha (Kaphaja) as it is mootrala. Very specifically it cures a
condition of rakta kshaya lakshana and Vyadhi such as Pandu. It is
shramaharam also. Dark brown Jaggary (purana Guda) has far more Iron59.
Amaika prayoga
Guda as anupana together with Nagara, Haritakai and Ardhraka taken, it
mitigates Vata, Pitta and Kapha respectively.

Materials and Methods - Drug review 73
2. Nagara
Zingiber officinale60, roscoe.
Sanskrit : Shunti
Hindi : Sonth
Kannada : Shunti
English : Dry zinger
Family : Scitaminaceae
Synonyms :Sunti, Nagara, Mahowshadha, Viswabheshaja,
Sringavera,
Distribution:
Ginger is cultivated in many parts of India; on a large scale in the warm, moist
regions, in Madras, Cochin and Travanacore, and to a somewhat less extent in
Bengal and the Punjab.
Description:
Rhizome, stout, tuberous with erects leafy stems 0.6 to 1.2-meter height.
Leaves narrow, flowers greenish. It is a well-known plant.

Materials and Methods - Drug review 74
Parts used:
Scraped and dried rhizomes
Preparation of Shunti (dried ginger):
The green is first sun- dried, cleaned and soaked in water. The outer skin is
scraped off and the scraped ginger washed and again sun-dried. Both ginger and
shunti are used as condiment and also medicinally.
Pharmacological properties:
Rasa katu
Guna laghu
Veerya ushna
Vipaka madhura
Prabhava Kaphavata shamaka
Constituents:
“Indian ginger contains an aromatic volatile oil,1 to 5 p.c. of light yellow colour
having a characteristic odour and containing camphene, phellandrene, zingiberine,
cineol and borneol; gingerol a yellow pungent body an oleo-resin-“gingerin” the active
principle, other resin and starch; K-oxalate. The essential oil and resin, to which
ginger owes its pungent flavor, occur just beneath the skin or epidermis. The pungent
principles of ginger are not found in the volatile oil. It has how ever, been isolated and
been named gingerol, but its true chemical nature has not yet been finally settled.”

Materials and Methods - Drug review 75
Action:
It is aromatic, carminative, stimulant to the gastrointestinal tract, and
stomachic, also sialogogue and digestive. Externally, a local stimulant and
rubrifacient.
Action and uses in Ayurveda - katu rasam, ushna veerya, vata-kapha-hara,
katu vipaka, lagu, snigda, pancha, ruchya, vrishya, swarya, vibhandha hara. In
grahani, agnimanthya, amavatha, chardhi, swasa, shoola, arsas, anaha, hrith-roga,
udhara roga, externally in Kapha, swellings, head ache.
Uses in general:
Ginger is prepared from the dried rhizomes. Ginger being aromatic and
pleasantly pungent, is commonly used as a spice and in the preparation of
condiments, curries, ginger bread, and a conserve and syrup and made from the
fresh younger rhizomes. Rhizomes are also pickled.

Materials and Methods - Drug review 76
3. Mandura
Sanskrit - manduram, rakta bhasma
English - iron rust, inpure oxide of iron, magnatite ironoxide, magnatite
Hindi - lohaka zung
Kannada - kabbinada kilubu or kitta
Chemical name - Ferroso - Ferric oxide
Synonyms61 - lohakitta, lohabhava, lohamala, lohetchista, loha singhanika,
kitti, sinhanam,
Panduroga is well known disease since vedic period. In Rigveda and
Atharveda Panduroga is mentioned by word viloha. The meaning of this word is loss
or deficiency of loha. There are mainly two types of treatment while treating the
Panduroga.
Lohayukta yoga
Lohaitara vanaspathika yoga
Mandoora is a upadahtu of lohadhatu of course all Ayurvedic grantha karas have
advise the use of mandura that is lohakitta in the treatment of Pandu.
Utpatti62
When loha is heated for long time its malabhaga get separated from it. Which
is known as lohakitta or mandura. On biting the hot loha it losses its mala which is
known as mandura.

Materials and Methods - Drug review 77
Sources
Mandura is occurred free in soil. The red colour soil is due to that upadhatu of
loha that is mondura in India southindia main sources of mondura.
Properties63
Rasa - kashaya, tikta, madhura
Veerya - sheeta
Other gunas - guru, ruksha,sara, sheeta
Karmukata - action on doshas, vatanashaka, kapha pittanasaka
that is tridoshagna
Action on dhatus raktavridhikara, vrishya
Action on organs chakstushya pleehagna
Others lekhan vayastapana, deepana, rucheekara
Rogaghnata -Pandu, arsha, shotha, pleeharoga, kamala, kumba
kamala, halimaka, shosha, medoroga, prameha, krimi,
kustha.
Amenorrhoea, dysmenorhoea, menorrhagia, chlorosis also diarrhoea, chronic
bowel complaints, dyspepsia, and nervous disease,(neuralgia) kidney disease,
(albuminuria) guda mandura is a favorite medicine for dyspepsia with pain after
taking food.

Materials and Methods - Drug review 78
4. Tila
Sesamum indicum linn
All Ayurvedic authorities advocated the use of sneha dravyas (fats or lipids)
both for dietary purposes64 and for the purpose of treatment as medicated oil and or
the pure fats both internally or externally in sneha kriyas65. Of these sneha drayas
four are important one of vegetable origin viz tila (seeds of Sesamum indicum linn)
and the other three being of animal origin viz. Ghrita, vasa and majja. The
understanding that in Ayurveda, Tila is the most efficacious for the purpose of
strength and oleation may recognize the importance of the tila66.
Nomenclature
Sanskrit -tila,
English - gingelly, sesamum
Kannada - yellu
Hindi - til
Family - pedaliaceae
Synonyms - phala, snehaphala, hemadhanya,
pavitra, pitrutarpana, papaghani, jatila

Materials and Methods - Drug review 79
Description
This plant is cultivated extensively throughout India. Erect herbs, about 70 cm
high; branching often from base, puberculous, leaves up to 10 x6 cm lanceoate,
lower pedatisect, glabrous above, puberulous beneath. Flowers pinkish purple about
2.5 cm long, axilliary, solitary or in recemes about 4 cm long pedicles glandular at
base, calyx 0.3 long 5 partite, puberulous, corolla 2.5 cm long ventrioles faintly
gibbous at base 2-lipped, stames4, didagnamous, include ovary glabous style
filiform, stigma 2 lobed, disk annular, capsules 1.5 cm long quadrangular, shortly
beaked pubscent dehiscing about half way down, seeds black compressed glabrous
oily. Flowering and fruit in April - July.
The seeds and oil are used in Ayurvedic medicines. Bhavamishra states that
according to the color, the tila seeds are of three-varieties - out of the black variety
are used and considered the best.
(1) black
(2) white and
(3) Red.
Properties of sesame seeds67
Rasa - katu, slight kashaya, more of madhura and tikta
Virya - ushna
Vipaka - katu, according to sushruta - madhura68
Gunas - snigdha, guru, swada, (tasty) cold to touch

Materials and Methods - Drug review 80
Composition of Tila
Saturated fatty acids -
Palmitic acid - 9.1%
Stearic acid - 4.3 %
Arachidic acid - 0.8 %
Unsaturated fatty acids
Oleic acid 45.4 %
Linoleic acid - 40.4%
Karma69
- vataghna, grahi, balya, good for hair, skin, teeth and ulcers, improves
Agni and intellect, increases semen, reduces the urinary out-put. It does
not aggravate Kapha, Susruta states that it alleviates Kapha, deepana,
pachana, brimhanam, balyam, preenanam, vrishyam lekhanam, promotes
skin health, intellect digestive fire, health of eyes,complexion, strength and
stability of mamsadhatu, krimighna, causes constipation and reduces the
quantity of urine, good for the hair, cleanses the garbhashya and yoni
helps in overcoming aging process and fatigue, causes Rakta Pitta.
- In combination with different drugs, it is said to be cured all diseases, and
when it is used as roborant to emaciate and reduces the obese. It is used
for alleviation of Vata, in vasti, nasya for internal administration, to be
used in ears and eyes and in dietary articles.

Materials and Methods - Drug review 81
5. Pippali
Piper longum. linn.
Sanskrit Pippali
Hindi Peepal
Kannada Hippali
Family Piperaceae.
Synonyms Magadhi, Kana, Krishna,Chapal, Ushana, Kola70.
Distribution
Hotter provinces of India, Ceylon, Malasia etc it is cultivated.
Parts used
Dry fruits.
Short description- Fruits are very small, ovoid in shape and completely sunk in solid
fleshy spike which is 2.5 to 3.8 cm. It is ovoid– oblong, erect, blunt and blackish
green in colour.
Pharmacological properties71 –
Guna -Laghu, snigdha, Teekshna.
Rasa - Katu
Vipaka - Madhura.
Veerya - Anushna Sheeta.
Doshaghnata - Kapha vata hara.

Materials and Methods - Drug review 82
Chemical composition –
Resin, volatile oil, Starch, gum, fatty oil, inorganic matter and an alkaloid,
piperine.
Actions72 –
It subsides Kapha and Vata because of its katu rasa and snigdha guna
respectively. It acts as yogavahi. According to Rajanighantu it is Jwara nashaka,
veerya vardhaka and jatharagni deepaka. Bhavaprakasha clearly states that, if
Pippali added to Guda it subside Ajeerna, aruchi, kasa, swasa, kusta, Pandu and
krimiroga.

Materials and Methods - Drug review 83
Preparation of the drug " Gudanagaradivati 73"
Ingredients of Gudanagaradivati is as beneath -
Guda - 1 part
Nagara - 1 part
Mandura - 1 part
Tila - 1 part
Pippali - 2 parts
Collection of drugs
Medically useful parts or the ingredients of Gudanagaradivati were collected
from the local market of the Gadag and the Mandura bhasma of reputed company
was purchased from the Ayurvedic medical shop.
Method of preparation
The collected drugs Nagara, tila, and Pippali were powdered with help of
Powder making mechine. Then Mandura Bhasma was added to the prepared Churna
and mixed thoroughly. Then 1 part of Guda and 4 parts of water boiled together
made it into semisolid paste then pre prepared Churna added to this preparation and
made into 500 mg. Vati and dried and collected.
Storage
The dried and collected vati are stored in glass jar. Its shelf life period is
enhanced for 1 year as it is made in the form of vati with Guda as binding agent.

Materials and Methods - Drug review 84
56 Rajanighantu Paniyadi varga 100 57 Bhavaprakasha poorvakhanda Ikshuvarga 23 58 Ibid 24-25 Rajanighantu Paniyadi varga 100 Yogaratnakara poorvardha 59 API text Book of Medicine pp859 60 Indian materia medica pp 1308 - 1315 Indian medicinal plants Vol IV pp 2435 -2438 Bhvaprakasha Haritakyadi varga Dravyaguna Vijnana pp263 Susruta Samhita Sutra 46/ 61 Rasatarangini 20/124 62 Bhavarakasha poorvakhanda Dhatwadi varga 52 Rasatarangini 20/123 63 Ibid 132 Bhavarakasha poorvakhanda Dhatwadi varga 49 Indian materia medica Vol II pp62-63 64 Charaka Samhita Vimana 1/13 Ibid Sutra 27/286 65 Ibid 13/9 66 Ibid 13/12 Susruta Samhita Sutra 45/130 67 Charaka Samhita Sutra 27/30 Astanga Hridaya Sutra 6/21 Bhavaprakasha poorvakhanda Dhanyavarga 63-65 68 Susruta Samhita Sutra 46/39 69 Bhavaprakasha poorvakhanda Dhanyavarga 63-65 70 Bhavaprakasha poorvakhanda Haritakyadivarga 54 71 Ibid 55 72 Ibid 57-58 Rajanighantu Pippalyadi varga 13 Charaka Samhita Vimana 1/16 73 Ibid Chikitsa 16/72 Astanga Hridaya Chikitsa 16/25

Material and Methods - Examination 84
Present day unwholesome food habits are influencing deficiencies of vital
nutrients (iron, Vitamin B12 etc.) as the main cause of Pandu. The Bhootabhishanga
(parasitic infection) also has a prime role in developing Pandu. Even after so many
treatments are available from alternative systems. The incidence of Pandu is high in
the developing countries due to malnutrition and poor hygienic status.
Ayurveda advocated treatment of Pandu with many herbal and herbomineral
combinations. Out of such one claimed by Charaka Samhita, as an effective recipe
for Pandu is "Gudanagaradi Vati".
The Pandu Roga is dealt in Brihatrayee with its treatment elaborately. The
whitish discoloration of skin is said as Pandu Varna the disease named as
Panduroga, which shows its lakshanas in between twak (skin) and Mamsa (muscle).
The compound of present study (Gudanagaradi Vati) is mentioned in Charaka
Samhita said to be effective in Pandu Roga. The composition of Gudanagaradi Vati
(guda, sunthi, mandoora, tila and pippali) also individually has considerable effect
over Raktadhatu and Raktavaha Srotas.
Objectives of study
To study the efficacy of Gudanagaradi Vati in Pandu

Material and Methods - Examination 85
Methods of study
Source of data
1. Patients
Patients suffering from Pandu are selected from post graduation and research
center O.P.D of D.G.M Ayurvedic Medical College Hospital by preset inclusion and
exclusion criteria.
2. Drug
Trial drug (Gudanagaradi Vati) is prepared in college pharmacy after proper
identification of the raw drugs.
3. Literature
Literary aspect of study is done from classical Ayurvedic texts, modern texts
and updated through journals, which is already explained from Drug review.
Method of collection of data
Exclusive criteria
• The patients below mentioned are excluded
• Age group of below 5 years and above 55 years
• Associated with vital organic disease
• Sever blood loss
• Parasitic infection
• Discontinuation of treatment schedule
Inclusive criteria
The patients of both sexes between the age of 5 to 55 years with mild to
moderate Anaemia, other than that of exclusive criteria are included in the present
study.

Material and Methods - Examination 86
Study design
Prospective clinical trail
Sample size
Minimum of 25 patients are subjected for the study
Treatment schedule of Gudanagaradi Vati
Posology
• 40mg/kg, body weight /24 hours or
• At the maximum of 2gm./24hrs. in divided doses.
Study duration
• 21 days
Assessment of results
• The results will be assessed by clinical, as well as
hematological study.
• Hb% is assessed for all at the interval of 7 days.
Hematological Investigations
• Hemoglobin percentage
• Total count of R.B.C
• Packed cell volume
• Mean corpuscular volume
• Mean corpuscular hemoglobin concentration
• Peripheral smear
• Serum iron

Material and Methods - Examination 87
Examination of a patient with Pandu (Iron deficiency Anaemia)
I. History
i) Female in reproductive period of life
Menstrual history - especially menorrhagia
Pregnancy - number of frequency
Miscarriage
Diet
Alimentary blood loss
Haematuria, epistaxis, haemorrhoids
Gastro intestinal surgery
Chronic Asprin ingestion
ii) Male and post menopausal females
Alimentary blood loss
Hemorrhoids
Haematemesis or melaena, epistaxis, haematuric haemoptysis
Gastro-intestinal surgery
Diet
Chronic aspirin ingestion
iii) infant and children
Detail dietary history, especially and supplemental feeding
Premature, multiple births or iron deficiency mother
Gastrointestinal disturbance
Blood loss

Material and Methods - Examination 88
II) physical examination
Abdomen-abdominal mass, tenderness, feature of liver disease
Rectal examination
Pelvic examination
Telangiectasia of face and mouth - tongue, mucous membrane, palpable
conjunctiva, palm etc.
Nails
III) laboratory investigation
Urine - routine and microscopic examination
Stool - occult blood and any parasites (especially hook worm and
roundworm).
Blood - R.B.C. morphology
Routine test of blood i.e., T.C.,D.C., Hb%. E.S.R.
Total R.B.C. count P.C.V., M.C.V., M.C.H.,M.C.H.C.
Serum iron
Serum transferrin (total iron binding capacity)
Serum ferritin
Bone marrow - iron staining
After confirm action the iron deficiency Anaemia investigate to know -
Inadequate intake
Malnutrition
Mal absorption

Material and Methods - Examination 89
The sample case sheet for the evaluation of Pandu patient is as under. In this
demographic data is thoroughly dealt as par the guidelines of research. Then chief
complaints with duration are dealt with specific focus on the Vaivarnya, Shrama,
Bhrama, Gatra shoola, Pindikodwestana, Sadana, Alpameda, and Shotha.
Associated complaints with the duration are also classified.
A general examination is undertaken as a routine for the evaluation of fitness
of patient. Specific Ahara and Vihara Nidana according to the classical texts
summarized. The lakshana were drawn special importance with reference to the
Pandu in general and in specific with that of classification of Pandu, such as Vataja
Pittaja, Kaphaja and Mritbhashana janya pandu. Dwandwaja and sannipataja are
specified as the combination and permutations of doshic involvement.
Asadhya lakshana are noted to rule out the problematic area of research.
Parameters of objective determined are monitored at regular intervals and entered in
to the special case sheet for "Evaluation of the effect of Gudanagaradi Vati in
Pandu".
Method of Estimation of Objective parameters,
1. Hb% 2. RBC counts 3. PCV 4. MCH 5. MCHC 6. Serum Iron
Is as follows.

Material and Methods - Examination 90
1. Hemoglobin estimation
Sahli's method (sahli's haemoglobinometer ; superior - germany)
This is based on conversion of hemoglobin to acid haematin, which has a
brown colour. Fill hemoglobin tube till 20 mark with N/10 HCL. To this add blood
sucked till the specific mark (20µl) on the hemoglobin pippette and wait for 5-45
minutes. During this time keep stirring the mixture of acid-blood in the tube. Add
distilled water until a match is obtained with the brown glass standard (comparator)
provided. Read the lower level of fluid mensicus on gm/% side of the tube. Report
hemoglobin in gm/100 ml of blood. If hemoglobin is less than 2 gm%, take double the
quantity of blood and divide the result by 2. If haemoglobin concentration is extremely
high dilute blood with equal amount of normal saline, take the reading and multiply by
2. This mehod, however, does not estimate carboxyhaemoglobin, methaemoglobin
and sulphaemoglobin. Non-hemoglobin substances (protein, lipids) in plasma and
cell stroma may influence the colour of blood diluted with acid. It therefore is not a
very satisfactory method.
Gradations of Heamoglobin percentage:
Mild Hb% above 9.0 gm/100 ml
Moderate Hb% between 9.0 to 6.0 gm/ 100 ml
Severe Hb% below 6.0 gm

Material and Methods - Examination 91
2. RBC' count
Diluting fluid:
This should be isotonic so that RBC's are not haemolysed. Normal saline can
be used but it may cause crenation of the RBC's and allow rouleaux formation.
One can use
1. Sodium citrate 3 gm.
Formalin 1 ml
Distilled water to 100 ml (Cheap and good)
Or
2. Hayem's fluid
Mercuric chloride 0.5 gm
Sodium chloride 1.0 gm
Sodium sulphate 5.0gm
Distilled water to 200ml.
(Needs to be made frequently and in hyperglobulinaemia one may set precipitation of
protein so RBC clumping may occur. Mercuric chloride acts as an antiseptic).
Method
Draw blood to the 0.5 mark in the RBC pipette. Wipe tip clean and draw
diluting fluid to the 101 mark. Shake for 3 minutes. Charge the chamber. Count the
RBC's using 40 X objective in the 80 smallest squares as indicated in the diagram of
the chamber.

Material and Methods - Examination 92
RBC count =
No of cells counted x dilution factor x depth factor
Area counted
Where dilution id 1 in 200, depth is 1/10 mm
80 = 1 Area counted is sq mm
400 = 5
Number Counted x 200 x10 =
1/5
= number counted x 10000
Interpretation
RBC counts are low in Anaemia (Pandu) and high in polycythemia causes of
Anaemia has already been discussed.
3. Haematocrit /packed cell volume (PCV)
Definition
Haematocrit is the volume of red cells expressed as a percentage of the
volume of whole blood in the sample. The venous Haematocrit is almost same as
that obtained from a skin puncture. Dried heparin, EDTA or double oxalates are
satisfactory anticoagulants.

Material and Methods - Examination 93
Methods
Wintrobe's tube
Fill the wintrobe's tube till the 100 mark on top with a pasteur pipette ensuring
that there are no air-bubbles in the flood column. Centrifuge this tube for 15 minutes
at 3500 rpm (or longer at lower speeds) until packing is complete. After centrifuging,
the blood is separated into 3 layers, a column of red blood cells at the bottom, a
narrow middle layer - buffy coat of white blood cells, and platelets and the topmost
fluid column of plasma. The percentage of the height of the column of blood occupied
by packed red cells constitutes the Haematocrit. Roughly the Haematocrit value is
three times the hemoglobin concentration.
Sources of error
1. Inadequate mixing of blood
2. Irregularity of the bore of the tube
3. Incomplete packing
Normal range
Men - range 42-52% average =47%
Women - range 37-47% average = 42%
4. MCH (The mean cell hemoglobin)
Hemoglobin in grams / liter = Pg.
Red cell count / ml Normal MCH in adults is from 27 to 32 pg.

Material and Methods - Examination 94
5. MCHC (The mean cell hemoglobin concentration )
Hb in grams X 100 = 31 to 35 gm%
PCV 6. Serum Iron (Nitro -PAPS method)
Principle
Iron ions are dissociated from is carrier protein, transferring in an acid
medium and simultaneously reduced to the ferrous form. The ferrous ions react with
the chromogen Nitro-PAPS to a colour-complex highly specific. The resulting
absorbance is directly proportional to the iron contents.
Transferrin-bound iron is released at an acid pH and reduced from ferric to
ferrous ions. These ions react with ferrozine to form a violet colored complex, which
is measured spectrophotometrically at 560 nm. The absorbance measured at this
wavelength is proportional to serum iron concentration.
Total Iron-binding capacity (TIBC)
A known amount of ferrous ions are added to serum at an alkaline pH. The
ferrous ions bind with transferrin at unsaturated Iron-binding sites. The additional
unbound ferrous ions are measured using the ferrozine reaction. The difference
between the amount of ferrous ions added and the unbound ion measured is the
unsaturated iron-binding capacity (UIBC). The TIBC is equal to the serum iron
concentration plus the UIBC.
Clinical significance
In most cases, both serum iron and TIBC values are necessary for greatest
diagnostic significance. Low serum iron values are seen in chronic blood loss,

Material and Methods - Examination 95
insufficient intake or absorption of iron, and increased demand on the body stores
(e.g. pregnancy). Elevated serum iron values are seen in increased red cell
destruction, decreased red cell synthesis, increased iron intake, or increased iron
stores release.
Increase in the TIBC may be due to increased production of apotransferrin
(e.g. chronic iron deficiency) or an increased release of ferritin, as in hepatocellular
necrosis.
Decreases in the TIBC can occur with cirrhosis and hemachromatosis due to
a deficiency in ferritin, or in nephrosis due to a loss of apotransferrin.
Kit contents
Iron reagent - ready-to-use
Iron standard 30µmol/1 - ready-to-use
Avoid contamination of ready-to-use reagents. Always use fresh pipette tips.
Keep always the caps tightly closed. Reagents are stable until expiry date mentioned
on the label. Store all the reagents at 2-8°C.
Warning and precautions
1. For in vitro diagnostic use
2. Avoid ingestion of reagent, as toxicity has not yet been determined.
3. Specimens should be considered infectious and handled appropriately.
4. Do not interchange the caps of reagent bottles.

Material and Methods - Examination 96
Specimen collection and storage
1. Fresh, unhemolyzed serum is the specimen of choice.
2. Serum should be separated as soon as clot has formed.
3. Heparinized plasma may be used but other anticoagulants should not
be used to avoid possible iron contamination.
4. Serum iron is reported to be stable for four days at room temperature
(15-30°c) and seven days at 2-8°C.
Determination of iron
Wavelength : 578 nm Pipette into test tubes Blank Standard Test Iron reagent 500µl 500µl 500µl Distilled water 25µl - - Standard - 25µl - Sample - - 25µl Mix and incubate at 37°C for 3 min. and measure the absorbance of sample A(s) and
standard A (STD) against the blank A (BL), at 578nm.
Calculation of Serum iron (µmol/1) =
A(s) - A (BL) X 30
A (STD) - A (BL) Expected values
Men 9.5 - 30µmol/1(53-167µg/dl)
Women 8.8-27 µmol/1(49-151µg/dl)
Linearity 180µmol/1
Special case sheet follows in the next page.

observations 101
Chart number 1- Demographic Data of “Evaluation of the effect of Gudanagaradi Vati in Pandu”.
S .no OPD Age Sex Occupation Economical Status Food Result
M F S A L 1 2 3 4 5 V Mx C P R NR D 1 417 16 + + + + + 2 248 55 + + + + + 3 397 50 + + + + + 4 499 15 + + + + + 5 624 35 + + + + + 6 707 29 + + + + + 7 729 22 + + + + + 8 730 26 + + + + + 9 747 42 + + + + + 10 683 55 + + + + + 11 750 25 + + + + + 12 710 25 + + + + + 13 872 40 + + + + + 14 751 45 + + + + + 15 875 45 + + + + + 16 963 55 + + + + + 17 998 35 + + + + + 18 921 38 + + + + + 19 1045 25 + + + + + 20 340 21 + + + + + 21 995 30 + + + + + 22 903 40 + + + + + 23 906 32 + + + + + 24 1062 40 + + + + + 25 831 40 + + + + + Total 10 15 0 18 7 9 8 6 2 0 13 12 07 13 05 00 00
M= male, F= female, S= Sedentary, A= Active, L= Labor, 1= Poor, 2= Lower Middle class, 3= Middle class, 4= higher middle class, 5 = Aristocrat, V= Vegetarian, Mx = Mixed diet.
C = Cured (well responded), P = Palliative, R = Responded, NR =Not Responded, D = Discontinued

observations 102
Chart number 2A-1- Chief Complaints of " “Evaluation of the effect of Gudanagaradi Vati in Pandu”.
S.no
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 B A B A B A B A B A B A B A B A B A B A B A B A B A B A B A
1 + - + - - - - - - - - - - - - - + + - - - - - - - - - - - - 2 + - + - - - - - - - - - - - - - - - - - - - - - - - - - + - 3 + - + - + - - - - - + - - - - - - - - - - - - - - - - - - - 4 + - + - + - - - - - - - - - - - - - - - - - - - - - - - - - 5 + - + - + - - - - - - - - - - - - - - - - - - - - - - - - - 6 + - + - + - - - - - - - - - - - - - - - - - - - - - - - - - 7 + - + - + - + - - - - - - - - - - - - - - - - - - - - - - - 8 + - + - + - + - - - - - - - - - - - - - - - - - - - - - - - 9 + - + - + - - - - - - - - - - - - - - - - - - - - - - - - - 10 + - + - + - - - - - - - - - - - - - - - - - - - - - - - - - 11 + - + - + - - - - - - - - - - - - - - - - - - - - - - - - - 12 + - + - - - - - - - - - - - - - + + - - - - - - - - - - - - 13 + - + - + - - - - - - - - - - - - - - - - - - - - - - - - - 14 + - + - + - - - - - - - - - - - - - - - - - - - - - - - - - 15 + - + - + - - - - - - - - - - - - - - - - - - - - - - - - - 16 + - + - + - - - - - - - - - - - - - - - - - - - - - - - - - 17 + - + - + - - - - - - - - - - - - - - - - - - - - - - - - - 18 + - + - + - - - - - - - - - - - - - - - - - - - - - - - - - 19 + - + - + - - - - - - - - - - - - - - - - - - - - - - - - - 20 + - + - + - - - - - - - - - - - - - - - - - - - - - - - - - 21 + - + - + - - - - - - - - - - - - - - - - - - - - - - - - - 22 + - + - + - - - - - - - - - - - - - - - - - - - - - - - - - 23 + - + - + - - - - - - - - - - - - - - - - - - - - - - - - - 24 - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - 25 + - + - + - - - - - - - - - - - - - - - - - - - - - - - - -
1= Pandu nakha, 2= Pandu netra 3= Pandu twacha 4= Pandu vit 5 = Pandu mootra, 6 = Pandu sira 7= Krishna nakha, 8= Krishna netra 9= Krishna twacha 10= Krishna vit 11 = Krishna mootra, 12 = Krishna sira
13= Aruna nakha, 14= Aruna netra 15= Aruna twacha

observations 103
Chart number 2A-2 - Chief Complaints of " “Evaluation of the effect of Gudanagaradi Vati in Pandu”.
S.no
16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 B A B A B A B A B A B A B A B A B A B A B A B A B A B A B A
1 - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - 2 - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - 3 - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - 4 - - - - - - - - - - - - + - - - - - - - - - - - - - - - - - 5 - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - 6 - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - 7 - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - 8 - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - 9 - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - 10 - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - 11 - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - 12 - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - 13 - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - 14 - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - 15 - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - 16 - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - 17 - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - 18 - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - 19 - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - 20 - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - 21 - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - 22 - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - 23 - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - 24 - - - - - - + - + - + - - - - - - - - - - - - - - - - - - - 25 - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -
16= Aruna vit 17 = Aruna mootra, 18 = Aruna sira 19= Peeta nakha, 20= Peeta netra 21= Peeta twacha 22= Peeta vit 23 = Peeta mootra, 24 = Peeta sira 25= Shukla nakha, 26= Shukla netra 27= Shukla twacha
28= Shukla vit 29 = Shukla mootra, 30 = Shukla sira

observations 104
Chart number 2B - Chief Complaints of " “Evaluation of the effect of Gudanagaradi Vati in Pandu”.
S.no 1 2 3 4 5 6 7 8 9 10 11 12 13
1 - - - - - - - + + + - + + 2 - - - - - - - + + + - - + 3 - - - - - - - + + + - + + 4 - - - - - - - + + + - + - 5 - - - - - - - + + + + + + 6 - - - - - - - + + + - + + 7 - - - - - - - + + + + + + 8 - - - - - - - + + + - + + 9 - - - - - - - + - + - - - 10 + - - - - - + + + + - + - 11 - - - - - - - + + - - - + 12 - - - - - - - + - + - - + 13 - - - - - - - + + + + + + 14 - - - - - - - + - + - - - 15 - - - - - - + + + + - + - 16 - - - - - - - + + + - + + 17 - - - - - - - + + + - - + 18 - - - - - - - + + + - + - 19 - - - - - - - + + + + - + 20 - - - - - - - + + + - + + 21 - - - - - - - + + + - - + 22 - - - - - - - + + + - - + 23 + + + - - - + + + + - - + 24 - - - - - - - + + + - + + 25 - - - - - - - + + + - + +
1 = akshikoota shotha, 2= gandapradesha shotha, 3= kapola shotha, 4= bhru shotha, 5= lingashotha, 6= nabhi shotha,
7=pada shotha, 8= shrama, 9= bhrama, 10= gatra shoola, 11= pindikodwestana, 12= sadana, 13= alpameda

observations 105
Chart number 3 - Associated Complaints of " “Evaluation of the effect of Gudanagaradi Vati in Pandu”.
S.no
1 2 3 4 5 6 7 8 9 10
11
12
13
14
15
16
17
18
19
20
21
22
23
1 + + + + + + + + + + + + + + 2 + + + + + + + + + + + 3 + + + + + + + + 4 + + + + + + 5 + + + + + + + + + + + + 6 + + + + 7 + + + + + + + + + + + + + 8 + + + + + 9 + + + + + + + + 10 + + + + + + + 11 + + + + + + + + + + + 12 + + + + + + + + + 13 + + + + + + + + + + + 14 + + + + + 15 - + + + + + + + 16 + + + + + + + 17 + + + + + + + + 18 + + + + + + + 19 + + + + + + + 20 + + + + + + 21 + + + + + + + + 22 + + + + + + + + 23 + + + + + + + + 24 + + + + + + + 25 + + + + + + + + +
1= Aruchi, 2= Agnimandya, 3= Toda, 4= Praseka, 5=Alasya, 6= Tandra, 7= Karna kshweda, 8= Sishira dweshi,
9=Swedavabhava, 10= Mritbhashanapekshana, 11= Jwara, 12=Swasa, 13= Kasa, 14= Trishna,15= Swarakshaya,
16= Sheerna Loma, 17= Hritdrava, 18= Anaha, 19=Chardi, 20=Klama, 21= Kampana, 22= Prabhanasha, 23= Nissara

observations 106
Chart number 4 - Nidana (etiology) of " “Evaluation of the effect of Gudanagaradi Vati in Pandu”.
S.no
Ahara Vihara A1
A2
A3
A4
A5
A6
A7 V1
V2
V3 V4 V5 V6 V7 V8
A B C a b c d e f g h i j k l m
1 + + + + + + + 2 + + + + + + + 3 + + + + + + + + 4 + + + + + + + + 5 + + + + + + + + + + 6 + + + + + + + + 7 + + + + + + + 8 + + + + + + + + + + 9 + + + + + + + + + + + 10 + + + + + + + 11 + + + + + + + + + + 12 + + + + + + + 13 + + + + + + + + + + 14 + + + + + + + + 15 + + + + + + 16 + + + + + + + 17 + + + + + + + + + + + 18 + + + + + + + + + + 19 + + + + + + + + + + 20 + + + + + 21 + + + + + + + + + 22 + + + + + + + + 23 + + + + + + + + + + + 24 + + + + + + + + + + + + 25 + + + + + + + +
A1=Amla, A2=Lavana, A3=Teekshna, A4=Kshara, A5=Viruddha, A6=Asatmya, A7=Mrit, A=Kashaya, B=Kshara, C=Madhura, V1=Ativyayama,
V2=Ativyavaya, V3=Manasika, a=Chinta, b=Shoka, c =Bhaya, V4= Vyasana, d= Madyapana, e=Dhoomapana, V5=Nidra, f= Sound, g= Disturbed, V6=
Malapravritti, h=Regular, i= irregular, V7= Mootra Pravritti, j=Prakrita, k= Vaikrita, V8= Rajah Pravritti, l=Prakrita, m=Raktapradara or Atyartava

observations 107
Chart number 5a - Vatajadi lakshana of " “Evaluation of the effect of Gudanagaradi Vati in Pandu”
s.no Vataja Pandu Pittaja Pandu 1 2 3 4 5 6 7 8 9 10 A B C D E F G H
1 + + + + + + + + + 2 + + + + + 3 + + + + 4 + + + + 5 + + + + + + + + + 6 + + + + + 7 + + + + + + 8 + + + + + 9 + + + + + + 10 + + + + + + 11 + + + + + + + 12 + + + + + 13 + + + + + + 14 + + 15 + + 16 + + + + + + 17 + + + + + + + + 18 + + + + + 19 + + + 20 + + + + 21 + + + + 22 + + + + + + 23 + + + + 24 + + + + + + + + + + 25 + + + + + +
1= krishna or aruna varna or rookshata of nakha, netra, twacha, vit mootra, sira,2= soochivat vedana. 3= bhrama, 4= kampana,
5= parswashoola, 6= shirashoola, 7= shopha, 8= asya vairasya, 9= anaha, 10= bala kshaya, A= peetata of twacha, nakha vit, netra mootra, B= daha, C= trisna, D= sheeta kamitwa,
E= sweda pravritti, F= jwara, G= atisara, H= dourbalya,

observations 108
Chart number 5b - Vatajadi lakshana of " “Evaluation of the effect of Gudanagaradi Vati in Pandu”
s.no
Kaphaja Pandu Mitbhashanajanya Pandu
1 2 3 4 5 6 7 8 9 10 11 12 13 14 A B C 1 + + + + + 2 + + + + + + + 3 + + + + + + 4 + + + + + + 5 + + + + + 6 + + + + 7 + + + + 8 + 9 + + + + + +
10 + + + + + + + 11 + + + + + + 12 + + + + + 13 + + + + + + 14 + + + + + 15 + + + + 16 + + + + + 17 + + 18 + + + + + 19 + + + + + 20 + + + + 21 + + + + + 22 + + + + + + 23 + + + + + + + 24 + 25 + + + + +
1= shwetha vrna of twacha, mootra, mala netra mukh, 2= shota, 3=tandra, 4=aslasya, 5= shareera gurutva,
6= kapha praseka, 7= chardi, 8= bharama, 9= klama, 10= swasa, 11= kasa, 12= aruchi, 13= vak graha, 14= swara graha, A= shotha of akshikoota, bhroo, gandapradesha, nabhi, linga pada, B= krimikosta, C= rakta kapha mala pravratti,

observations 109
Chart number 6 - Assessment of " “Evaluation of the effect of Gudanagaradi Vati in Pandu”
S.No Hemoglobin Percentage (gm%) Total RBC count(millions/cu.mm) Packed cell volume
Serum Iron (mmol)
B 7 14 21 D B 7 14 21 D B A D B A D 1 8.8 9.2 10.2 10.6 1.8 4.6 5.0 5.1 5.2 0.6 43 45 2 6.5 12.5 6.0 2 8.8 9.2 9.4 9.6 0.8 4.8 5.6 5.8 5.8 1.0 44 46 2 6.4 13.0 6.6 3 8.4 8.8 8.8 8.6 0.2 4.4 4.4 4.6 4.6 0.2 35 37 2 6.8 11.0 4.2 4 6.8 7.0 7.6 8.2 1.4 4.6 4.7 4.8 5.0 0.4 43 45 2 7.0 10.6 3.6 5 9.0 9.2 9.4 10.0 1.0 5.2 5.2 5.3 5.4 0.2 40 44 4 8.1 24.8 16.7 6 10.0 10.2 10.6 11.0 1.0 4.8 5.0 5.1 5.3 0.5 35 37 2 13.5 20.8 7.3 7 9.4 9.8 10.2 10.8 1.4 4.8 5.0 5.1 5.4 0.6 38 42 4 8.0 16.0 8.0 8 7.6 8.4 9.8 10.8 3.2 4.9 5.2 5.4 5.8 0.9 40 42 2 17.6 26.0 8.4 9 9.0 10.0 10.6 11.2 2.2 5.0 5.1 5.2 5.6 0.6 44 46 2 26.2 32.0 5.8
10 6.2 7.4 7.6 8.2 2.0 4.6 4.8 4.8 5.0 0.4 44 48 4 9.86 14.0 4.14 11 6.8 7.2 8.4 9.4 2.6 4.7 5.0 5.2 5.4 0.7 40 44 4 7.4 14.6 7.2 12 9.8 10.2 10.6 11.0 1.2 4.9 5.0 5.2 5.4 0.5 49 50 1 6.1 11.0 4.9 13 9.4 10.2 10.6 11.0 1.6 5.2 5.4 5.6 5.8 0.6 42 45 3 7.2 14.0 6.8 14 7.0 7.6 7.8 10.0 3.0 5.0 5.1 5.4 5.8 0.8 40 42 2 5.8 31.0 25.2 15 6.8 7.2 8.2 9.0 2.2 4.8 5.0 5.1 5.4 0.6 40 44 4 28.5 32.0 3.5 16 8.0 8.4 9.0 9.8 1.8 4.7 4.8 5.0 5.2 0.5 41 43 2 26.0 34.0 8.0 17 8.0 8.6 8.8 9.4 1.4 4.9 5.0 5.2 5.4 0.5 40 42 2 16.0 22.0 6.0 18 9.2 9.8 10.2 10.8 1.6 5.0 5.3 5.6 5.8 0.8 40 42 2 7.4 16.0 8.6 19 8.0 8.4 9.0 9.8 1.8 4.8 5.0 5.2 5.4 0.6 39 42 3 8.0 14.0 6.0 20 8.6 9.4 10.2 11.0 2.4 5.0 5.2 5.4 5.8 0.8 42 45 3 5.0 10.0 5.0 21 7.6 8.2 9.0 9.4 1.8 4.4 4.5 4.6 5.0 0.6 40 44 4 5.4 11.0 5.6 22 9.8 9.8 9.9 10.0 0.2 5.1 5.4 5.6 5.8 0.7 39 42 3 5.8 12.6 6.8 23 6.2 7.0 7.8 9.0 2.8 4.6 4.8 5.1 5.4 0.8 40 44 4 6.0 14.0 8.0 24 9.8 10.5 10.8 11.6 1.8 4.8 5.0 5.2 5.6 0.8 42 44 2 7.2 12.0 4.8 25 9.2 9.8 10.0 10.8 1.6 4.8 4.8 5.0 5.2 0.4 42 45 3 7.0 14.6 7.6
B= Before A= After D= Difference 7+ 7days interval, 14= 14 days interval 21 = 21 days interval
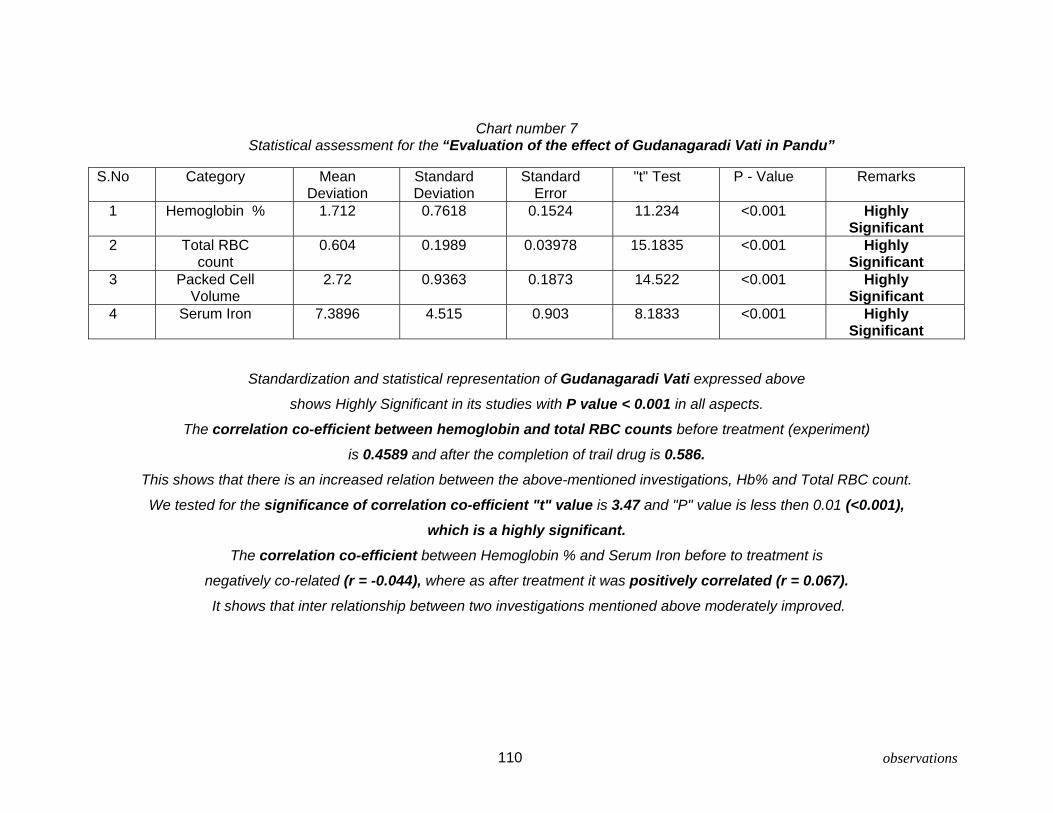
observations 110
Chart number 7 Statistical assessment for the “Evaluation of the effect of Gudanagaradi Vati in Pandu”
S.No Category Mean
Deviation Standard Deviation
Standard Error
"t" Test P - Value Remarks
1 Hemoglobin %
1.712 0.7618 0.1524 11.234 <0.001 Highly Significant
2 Total RBC count
0.604 0.1989 0.03978 15.1835 <0.001 Highly Significant
3 Packed Cell Volume
2.72 0.9363 0.1873 14.522 <0.001 Highly Significant
4 Serum Iron
7.3896 4.515 0.903 8.1833 <0.001 Highly Significant
Standardization and statistical representation of Gudanagaradi Vati expressed above
shows Highly Significant in its studies with P value < 0.001 in all aspects.
The correlation co-efficient between hemoglobin and total RBC counts before treatment (experiment)
is 0.4589 and after the completion of trail drug is 0.586. This shows that there is an increased relation between the above-mentioned investigations, Hb% and Total RBC count.
We tested for the significance of correlation co-efficient "t" value is 3.47 and "P" value is less then 0.01 (<0.001), which is a highly significant.
The correlation co-efficient between Hemoglobin % and Serum Iron before to treatment is
negatively co-related (r = -0.044), where as after treatment it was positively correlated (r = 0.067). It shows that inter relationship between two investigations mentioned above moderately improved.

Discussion and Conclusion 111
The study of 25 cases of Panduroga was treated with gudanagaradivati in
post graduation and research center (Kayachikitsa) of Sri DGM Ayurvedic medical
college Gadag.
Nidana described in the classics taken into account by the detailed
questioning patient’s pin pointedly to understand specific Nidana of Panduroga.
Among the 25 patients reserved for the trail most of the patients having the habit of
eating Amla, Lavana, rasapradana Ahara dravyas. Some patients were fond of taking
atiushna Ahara as their food. Some patients were fond of taking tikshnaaharas like
chilies etc., in their food. Many patients are of labor group and they are with
ativyayama and chinta, bhaya, etc., in the trial group.
Majority of the signs and symptoms explained in our classics regarding
Panduroga were observed in this clinical study. The patients who were selected for
clinical trail had panduta (discoloration) of twacha, nakha, netra, In all most all the
cases with maximum of chief complaints and associated complaints.
In relation to Agni patients having mandagni are largely prone for the
development of disease Panduroga.
The Anaemia, which results from the deficiency of iron and characterized by
reduction of Heamoglobin concentration, red cell count and packed cell volume to
below normal level is called as iron deficiency Anaemia (I.D.A). In this study, all these
signs and symptoms and lab investigations shows that all most all the patients
suffering from the Pandu can be considered as iron deficiency Anaemia (I.D.A) in

Discussion and Conclusion 112
contemporary medicine. The importance to the Loha i.e. Iron (IDA) is even given by
Acharyas of Ayurveda and also at present study. The role of Iron in the formation of
Rakta is not elaborated in Ayurveda, through suggesting it as main line of treatment
to Pandu, Vagbhata and Charaka justified its importance in respect with rectification
of pathogeneses. Therefore in this study very precisely concentrated on iron
deficiency Anaemia in contemporary review of literature.
In the Ayurvedic view of classification, present study Panduroga has
Sannipathaja Panduroga more. In those vatakaphaja Panduroga’s are more. Even
though Pandu is said as Pittapradanavyadhi, here in the study 6 patients did not
shows any Pittaja lakshnas and more over they show purely vatakaphaja lakshanas.
Other 19 patients fall under sannipatajapandu i.e., Tridosha (dementedly kaphaja)
lakshanas.
In this study the treatment of Panduroga by Gudanagaradi vati was selected
from Charaka Samhita Pandu Chikitsa and also Vagbhata referred in his work
Astanga Hridaya. The ingredients are Guda, Nagara, Mandura, Tila, and Pippali.
In the drug review the actions of Guda is being dealt that Guda is
Agnivardhaka, Raktavruddhikara, Vrishya, Hridya, and Tridoshagna are to be
considered here. In this preparation Guda acts as binding agent and also definitely
notified that it is chiefly Pandurogahara i.e. reduces Pandu.
The ingredient Nagara as the synonym indicates it is Viswabheshajam i.e.
medicine for all ailments. Here the action of Nagara Vatakaphahara vrisha, Swarya,
Ruchya are to consider. It also acts in Hridroga, Agnimandya, Swasa, and Shoola.
Mandura is updhatu of lohadhatu and also having the same qualities as
lohadhatu has. Iron is present in Heamoglobin, Myoglobin, Cytocroms and many

Discussion and Conclusion 113
Oxidetive enzymes. Heamoglobin percentage contains ferrous iron it is essential for
carrying to different tissues. Mandura otherwise said as Iron in the form of Ferric
Oxide. All Ayurvedic classics dealt the use of Mandura in the treatment of
Panduroga. Its action raktavridhikara helps in Panduroga which is the one of the
main compliant i.e., raktalpata. Also its actions are informed that panduhara,
shotahara, pleeharogahara, shoshahara, and krimihara, which are the upadravas or
nidanardakara vyadhies of Panduroga.
Even though it is said that the Tilasevana is leads to Panduroga, It is one of
the ingredients at present treatment schedule. It is supposed that the Pandu, which is
a chronic disease developed because of Loha content decrease in the body by
means of disturbing the assimilation or absorption of Loha is because of the excess
intake of tila or its byproducts. At this background using Tila in the combination
suggests that the leena dosha by using a material causing the disease in stipulated
doses along with the ingredients, those rectifies the disease will improve the
deficiencies of Loha in the body. It constructs Normal Rakta to perform its normal
function “Jeevana” by getting more Heam to exchange O2 and CO2 in the body. It
helps in promoting skin health and acts as deepana, pachana, brimhana, preenana,
balya and Krimighna.
Pippali is one of the ingredient i.e., 2 parts. Pippali which is yogavahi it
enhances the action of other ingredients. It subsides Kapha because of Katu Rasa it
subsides Vata because of Snigdha guna. Pippali added with Guda subsides Ajeerna,
Aruchi, Kasa, Swasha which Panduroga having the lakshanas. It’s effect over
Panduroga and Krimiroga are to be considered here.

Discussion and Conclusion 114
36 to 4532%
26 to 3524%
16 to 2524%
6 to 154%
46 to 5516%
Age incidence
Present study of “Evaluation of the effect of Gudanagaradi Vati in
Pandu" has the following age incidences. It suggests that much of the patient's
fall under the age groups in between 16 to 45 i.e. 80%, rest of 20% is from other
groups. The data as follows. As 80% of people incidence shows between the age
groups it suggests that nutritional deficiencies are more along with essential
elements for the synthesis of Rakta in these group. In further care taken towards
filling the gap of deficiencies and rectification of Rakta formation can correct the
Pandu.
S.No Age group Number of patients percentage 1 6 to 15 1 4 2 16 to 25 6 24 3 26 to 35 6 24 4 36 to 45 8 32 5 46 to 55 4 16
Total 25 100
Graph number - 1
Age incidence in “Evaluation of the effect of Gudanagaradi Vati in Pandu"

Discussion and Conclusion 115
Sex incidence
“Evaluation of the effect of Gudanagaradi Vati in Pandu" has the
following data in sex incidence. From the data available we can draw a conclusion,
that the incidence of Pandu is more in female's i.e. 60% (15 Patients), as such nature
is allowing more loss of blood in the form of menstruation and where as male's are of
only 40% (10 Patients). The ratio reveals in the study is as 2:3 for male and female
respectively.
S.No Sex Number of patients Percentage
1 Male 10 40 2 Female 15 60 Total 25 100
Female60%
Male40%
Graph number - 2 Sex incidence in “Evaluation of the effect of Gudanagaradi Vati in Pandu"

Discussion and Conclusion 116
0
18
7
0 5 10 15 20
Labor 7
Active 18
Sedentary 0
Occupation incidence
Study suggests that the patients out of active occupational group are more
prone to get the Pandu. Out of 25 cases studied 18 are in active and 7 are in labor
group of occupational categories. The percentages of active and labor are 72 and 28
respectively. It clearly suggests that the patients those who are active in their nature
of work needs more calories of energy which can not supplement the needs of
sequential progression of Rakta formation, in further the active occupational require
more O2 exchange, which is based on the Haem in the blood. Study clearly
evidential that Gudanagaradi vati is more helpful in these catagories.
S.No Category Number of patients Percentage
1 Sedentary 00 00 2 Active 18 72 3 Labor 07 28 Total 25 100
Graph number - 3
Occupational incidence in “Evaluation of the effect of Gudanagaradi Vati in Pandu"

Discussion and Conclusion 117
98
6
2
00
2
4
6
8
10
Economical Status 9 8 6 2 0
Poor Lower middle class Middle class Higher middle
class Aristocrat
Economical status
Data collected in the study shows that, more values of percentage i.e. 68%
(17 patients) of the patient's fall under economically lower group or other wise at the
poverty line. Few of the middle and above class patients are also reported that is 8
patients out of 25 refers to 32%, suggests that there is remarkable malnutrition,
deficiency of Iron and Pandu even in this group, where essential commodities are
plenty available in day to day life. For the rectification of the above said the
"Gudanagaradi Vati" is a medicine fits to the all groups of patients with exceptionally
at low price.
S.No Category Number of patients Percentage 1 Poor 9 36 2 Lower middle class 8 32 3 Middle class 6 24 4 Higher middle class 2 8 5 Aristocrat 0 0 Total 25 100
Graph number - 4
Economical status incidence in “Evaluation of the effect of Gudanagaradi Vati in Pandu"

Discussion and Conclusion 118
Vegetarian52%
Mixed diet48%
Diet (Food Habits) The food habit distribution in the locality of research has more percentage of
vegetarians in comparison even though the are said as mixed diet dependents. The
ratio of percentage between vegetarian and mixed diet is 13:12 i.e. 52% and 48%
respectively. In Pandu there is no specific vegetables mentioned in Ayurveda to
supplement the deficiency of Iron, which gives rise the disease. The data values are
given in data table along with graphical representation.
S.No Category Number of patients Percentage 1 Vegetarian 13 52 2 Mixed diet 12 48 Total 25 100
Graph number - 5 Diet incidence in “Evaluation of the effect of Gudanagaradi Vati in Pandu"

Discussion and Conclusion 119
0
2
4
6
8
10
12
Before treatment 8.328 4.816After 7 days 8.86 5.012After 14 days 9.38 5.184After treatment 10.044 5.42Difference of Beforeand After
1.712 0.604
Heamoglobin % (gm/L) Total RBC count in million/ Cumm
Objective parameters at mean values in regular intervals
Objective parameters are said to be foremost for assessing any research
works. Present study Pandu applies Heamoglobin %, Total RBC count, PCV and
Serum Iron as prescribed parameters. The study reveals that the effect of
Gudanagaradi Vati has consistent convinced results over Pandu. The data referred
to the statistics explained in detail at the master charts. Here the mean values are
taken for the evaluation and presentation. The data follows in the tabular form.
Before treatment
After 7 days
After 14 days
After treatment
Difference of Before and After
Heamoglobin % (gm/L)
8.328 8.86 9.38 10.044 1.712
Total RBC count in million/ Cu mm
4.816 5.012 5.184 5.42 0.604
Graph number – 6 Objective parameters at mean values in regular intervals
Heamoglobin and RBC count

Discussion and Conclusion 120
05
1015202530354045
Before 40.88 10.3504After 43.6 17.74Difference 2.72 7.3896
PCV % Serum Iron
The PCV % and Serum Iron values before and after the treatment is as
follows in tabular form and graphical.
Before treatment After treatment Difference of Before and After
PCV % 40.88 43.6 2.72 Serum Iron (mmol) 10.3504 17.74 7.3896
Graph number – 7 Objective parameters at mean values in regular intervals
PCV and Serum Iron

Discussion and Conclusion 121
Palliative52%
Cured28%
Responded20%
Not Responded
0%
Discontinued0%
Result
The present study “The evaluation of effect of Gudanagaradi Vati in
Pandu” is based on assessment criteria’s as clinical symptomatology and
Heamoglobin percentage. Clinically all the patients are observed to attain
normalcy and free from Panduroga. Hematologically even though they did
not reach the normal stipulated values of Heamoglobin they show remarkable
increase of serum Iron along with risen values of Heamoglobin percentage,
up to 3.2 % as highest difference in the study. The mean value difference oif
base line data is 1.712. The result declared is as under.
Category Number of patients Percentage
Cured 07 28
Palliative 13 52
Responded 05 20
Not Responded 00 00
Discontinued 00 00
Graph number 8 Result of the “Evaluation of the effect of Gudanagaradi Vati in Pandu"

Discussion and Conclusion 122
The result declared above is based on the Heamoglobin percentage along
with clinical assessments. Clinical assessment of all patients falls under cured, as
they show symptomatically well being. The Heamoglobin as objective parameter
considered in the present study was categorized in to three for the convenience of
study. Usually 10% of the normal value deviation is considered to state either
pathological state or recovery. All most all the patients have got rise of 10% of
Heamoglobin to their baseline data. The categories of assessment of Heamoglobin
are as under.
2 to 4 % rise in Heamoglobin % fall under Cured (well responded)
1 to 2 % rise in Heamoglobin % fall under Palliative (better responded)
0 to 1 % rise in Heamoglobin % fall under Responded
Other wise Not Responded and
Discontinued.
With the above criteria result is cured or well responded is 7 patients i.e. 28%,
palliative or better responded is 13 patients i.e. 52% and
Responded is of 5 patients’ i.e. 20%.
No discontinued or not responded cases recorded.

Future prospective
Though in this work maximum efforts put to fulfil the subject and to achieve
the aims and objectives of the present project work. There is still a wide scope to a
greater distance of studies as following.
Grouping could be made and in one group the efficacy of the drug on the other
hand studied after subjecting the individual for Samshodhana karma.
As the disease has wide range of etiology one can assess the role of
Gudanagaradivati in each of the etiological factors with its individual components
and also as a whole.
123

Summary
This study was formulated to evaluate the effect of Gudanagaradivati in
Panduroga.
The definition, history, etiology, Nidana panchaka, classification of Pandu,
upadrava, sadhya asadhyata and the treatment of Pandu according to the
classics and also the definition and etiological classification of anemia and iron
deficiency anemia were reviewed in the study.
The drug Gudanagaradivati and its composition was reviewed and discussed and
importance of Gudanagaradivati in the treatment of Pandu with respect to its
etiology is highlighted.
The study was conducted in a prospective clinical trial design on 25 patients.
Gudanagaradivati was administered in a dosage of 500 mg. 4 times a day or 2
gms/ 24 Hrs which ever is higher after the food for 21 days.
In this study the incidences of age, sex, occupation, economical status and diet
incidents were highlighted in the observation.
Each and every symptom of Pandu reported in this study showed response to the
drug.
No side effect of Mandura (iron) was reported during the treatment period.
The drug significantly elevated the Heamoglobin concentration in blood. It is
proved through statistical statements as p value <0.001, which is highly
significant.
Over all response to the drug was exceptionally best.
124

References for
“Evaluation of the effect of Gudanagaradi Vati in Pandu”.
1 Astanga Hridaya Sutra 1/3 2 Susruta Sutra 1/6 3 Rigveda 10-50-11 4 Atharvaveda 4-9-3 & 1-22-2 5 Charaka Samhita Sutra 18/43 6 Charaka Samhita Chikitsa 16/6 7 Susruta Samhita Sutra 14/ 8 Charaka Samhita Chikitsa 15/17 9 Astanga Hridaya Sutra 11/4 10 Astanga Hridaya Shareera 3/8 11 Susruta Samhita Shareera 4/3;
Charaka SamhitaShareera 7/5 12 Charaka Samhita Chikitsa 15/27 13 Charaka Samhita Sutra 24/3
Susruta Samhita Sutra 5/6 14 Charaka Samhita Sutra 24/23 15 Charaka Samhita Sutra 24/21 16 Susruta Samhita Sutra 14/9 17 Astanga Hridaya Sutra 11/17 18 Charaka Samhita Vimana 5/9 19 Charaka Samhita Vimana 8/114 20 Charaka Samhita Chikitsa 16/7-8 21 Susruta Samhita Uttara 44/3 22 Susruta Samhita Nidana 11/17 23 Susruta Samhita Shareera 2/21 24 Charaka Samhita Chikitsa 2/27

25 Susruta Samhita Shareera 6/27 26 Harita Samhita 3-9-39 27 Susruta Samhita Shareera 9/12 28 Charaka Samhita Chikitsa 16/7-11 29 Susruta Samhita Uttara 44/3 30 Astanga Hridaya Nidana 1/3-4 31 Charaka Samhita Chikitsa 16/12
Susruta Samhita Uttara 44/5
Astanga Hridaya Nidana 13/8
Astanga Sangraha Nidana 13/9
Madhava Nidana 8/3 32 HaritaSamhita 3/8
Vangasena Panduroga /2 33 Charaka Samhita Chikitsa 16/17-30
Astanga Hridayam Nidana 13/7
Madhava Nidana 8/1
Yogaratnakara Panduroga Nidana /1 34 Susruta Samhita Uttara 44/4 35 Charaka Samhita Chikitsa 16/17-18
Astanga Hridayam Nidana 13/8-10
Susruta Samhita Uttara 44/7 36 Charaka Samhita Chikitsa 16/19-22
Astanga Hridayam Nidana 13/10-11
Susruta Samhita Uttara 44/8 37 Charaka Samhita Chikitsa 16/23-25
Astanga Hridayam Nidana 13/11-12
Susruta Samhita Uttara 44/9 38 Harita Samhita Panduroga Chikitsa 8/10 39 Charaka Samhita Chikitsa 16/27-30
Astanga Hridayam Nidana 13/13-14 40 Charaka Samhita sutra 3/3 41 Astanga Hridaya Nidana 1/8

42 Charaka Samhita Chikitsa 16/9-11 43 Ibid 16/4, 9-11 44 Susruta Samhita Sutra 21/36 45 Auartely medical review. Vol. 47 no-2 april, 1996 46 Susruta Samhita Uttara 44/13 47 Charaka Samhita Chikitsa 16/31-33
Susruta Samhita Sutra 33/23
Madhava Nidana 8/12-15 48 Susruta Samhita Uttara 44/14
Charaka Samhita Chikitsa 16/39 49 Yogaratnakara Panduroga Nidana 27 50 Ibid 26 - 28
Charaka Samhita Chikitsa 16/116 51 Charaka Samhita Chikitsa 16/43
Astanga Sangraha Chikitsa 12/
Astanga Hridaya Chikitsa 16/ 52 Charaka Samhita Sutra 22/8 53 Charaka Samhita Chikitsa 16/116 54 Astanga Hridaya Uttara 4/41 55 Charaka Samhita Chikitsa 16/41-42
Susruta Samhita Uttara 44/
Harita Samhita Panduroga Chikitsa 8/34-36 56 Rajanighantu Paniyadi varga 100 57 Bhavaprakasha poorvakhanda Ikshuvarga 23 58 Ibid 24-25
Rajanighantu Paniyadi varga 100
Yogaratnakara poorvardha 59 API text Book of Medicine pp859

60 Indian materia medica pp 1308 - 1315
Indian medicinal plants Vol IV pp 2435 -2438
Bhvaprakasha Haritakyadi varga
Dravyaguna Vijnana pp263
Susruta Samhita Sutra 46/ 61 Rasatarangini 20/124 62 Bhavarakasha poorvakhanda Dhatwadi varga 52
Rasatarangini 20/123 63 Ibid 132
Bhavarakasha poorvakhanda Dhatwadi varga 49
Indian materia medica Vol II pp62-63 64 Charaka Samhita Vimana 1/13
Ibid Sutra 27/286 65 Ibid 13/9 66 Ibid 13/12
Susruta Samhita Sutra 45/130 67 Charaka Samhita Sutra 27/30
Astanga Hridaya Sutra 6/21
Bhavaprakasha poorvakhanda Dhanyavarga 63-65 68 Susruta Samhita Sutra 46/39 69 Bhavaprakasha poorvakhanda Dhanyavarga 63-65 70 Bhavaprakasha poorvakhanda Haritakyadivarga 54 71 Ibid 55 72 Ibid 57-58
Rajanighantu Pippalyadi varga 13
Charaka Samhita Vimana 1/16 73 Ibid Chikitsa 16/72
Astanga Hridaya Chikitsa 16/25

BIBLIOGRAPHY
API Text book of Medicine.By G.S.Sainani 5th edition 1992
Published by Association of Physicians of India, Bombay.
Astanga Hridaya with commentaries of Arunadatta and Hemadri By Harisastry paradakar Vaidya1939 Published by Nirnaya sagar press Bombay.
Astanga Samgraha of Vagbhata 1st edition 1996 By Prof K.R.Srikantha Murthy. Published by Chowkhamba Orientalia, Varanasi.
Basavaraajeeyam By Vaidya Basavaraju, 1959 Published by Konda Shankaraiah, vani press, Secundrabad.
Bhavaprakasa By Sri Brahmasankara Misra. 4th edition 1984 Published by Chowkhamba Sanskrit Sansthan, Varanasi.
Bhela Samhita by Girija Dayal Shukla, 1959 Published by Chowkhamba publication, Varnasi
Blood disorder in pregnancy Chatterjee, JB, Ray RN Dawn Books 25-B, C.I.T. Road, Sch. 52, Cakcytta-700014, Seventh Ed.1978: P-227.
Chakradatta By Priyavrat Sharma. 2nd edition 1998 Published by Chowkhamba Orientalia, Varanasi.
Charaka Samhita Poorvardha 1st edition 1962, by Vaidya Satyanaryana Shastri. Published by Chowkhamba Vidya Bhavan. Varanasi.
Charaka Samhita Uttarardha, 1st edition 1962 By Vaidya Satyanaryana Shastri.
Published by Chowkhamba Vidya Bhavan. Varanasi.
Cunninghama Manual of Pratactical Anatomy Vol 1 to 3 Published at Great Britain, Oxford University Press.
Control of nutritional Anaemia with special reference to Iron deficiency World Health Organization Technical Report Series No. 580 Report of an IAEA, USAID, WHO joint meeting, 1975.
Bibliography

Davidson’s Principles and Practice of medicine, By John Maclod 1992, Published by Pitman press, Great Britain.
Digestion and Metabolism in Ayurveda, By C.Dwarkanath, Published by Baidyanath Publications, Calcutta.
Dorland’s Pocket Medical Dictionary.
By Douglas M. Anderson. 24th edition 1989 Published by Oxford & IBH publishing Co. Pvt. Ltd. Bombay.
Diseases of the blood, “Clinical Medicine”, Kumar PJ, Clark M.L ELBS, 2nd edition, 1992, P-300, P-96
De Gruchy’s Clinical Haemtaology in Medical Practice,
Delhi, Oxford University Press, Bombay, calcutta, Madras, 5th edition, 1993, P-44,49.
Essentials of Basic Ayurveda Concepts.
By Prof Dr. V.V.S.Sastri. 1999 Published by Publication Division, PGARC, DGM Ayurvedic Medical College, Gadag
General Examination, Essentials of Clinical diagnosis Sen S. K. The Standard Book House, 1/1/1B, Bankim Chatterjee Street, Calcutta 73, Seventh edition – 1994, P – 14.
Gray’s Anatomy
by Henry Gray, 1973 Published by Longman group Ltd.
Human Physiology By Dr C.C.Chatterjee, 11th edition 1992 Published by Medical Allide Agency, Calcutta.
Hypochronic Anaemia : Iron Deficiency and Sideroblastic Anaemia
Ftrkin, F.et al, Delhi, Oxford University Press, Bombay, Calcutta, Madras, 5th edition, 1993, P-44,49.
Indian Materia Medica by K.M.Nadkarni. Vol 1 - 2 2nd edition 1982Published by Popular Prakashan Bombay
Indian Medicinal Plants by Kirtikar & Basu, Vol 1 - 3 2nd edition 1975
Bibliography

Introduction to Kayachiktsa, By C. Dwarkanath, Published by Chowkamba offest press, Varanasi.
Iron deficiency anaemia. Pathology illustarted Govan. AT. Macferlane, PS; Callamder, R Churchill Livingstone, Edinburgh London Melbourne and New York, 2nd Ed. 1986, P – 532.
Iron deficiency and Iron overload syndrome Agrawal, MB Quarterly Medical Review. Raptakos, Brett & Co. Ltd., Worli, Mumbai-400025, 1996.
Kashyapa Samhita, by Vridha Jeevaka,
1953 Published by Chowkhamba Vidya Bhavan. Varanasi
Madhava Nidana with Madhukosha sanskrit vyakarna. By Acharya Sri Narindranath shastri. 1st edition 1989Published by Motilal Banarasidas, Varnasi.
Principles of Internal Medicine By T.R. Harrison and Co. 1962
Rajanighantu By Pandit Narahari. 2nd edition 1998Published by Krishnadas Academy, Varansai. Researches in Ayurveda
By Dr. M.S.Baghel. 1st edition 1997 Published by Mridu Ayruvedic Publication and Sales. Jamnagar.
Review of medical Physiology By Willam. F. Ganong, 11th edition 1983 Published by Lange Medical publications, Maruzen.
Sushruta Samhita Poorvardha 8th edition By Kaviraja Ambikadutta shastri. Published by Chowkhamba Sanskrit Sansthan, Varanasi.
Bibliography

Sushruta Samhita Uttarardha 8th edition By Kaviraja Ambikadutta shastri. Published by Chowkhamba Sanskrit Sansthan, Varanasi
Shareera kriya vijnanam By M. Ramasundar Rao, 2nd edition 1994 Published by M. Madhava, Metro Printers, Vijayawada.
Symptoms and signs in clinical medicine – An introduction to Medical diagnosis Chamberlain, EN ; Oglive, C : The English Language Book Society and Bristol, John Wright & sons Ltd Ninth Edition1974, p-293.
Text book of pathology
by william Boyd, 1974
The Ayurveda Encyclopedia By Swami Sada shiva Tirtha. 1st edition 1998 Published by Indian books centre, Delhi.
Yogaratnakaram Shastry . L.P. Vidyotini Hindi commentary Published by Chowkhamba Sanskrit Sansthan, Varanasi
Bibliography


Co-Guidance : Dr. K. Siva Rama PrasadGuidance : Dr.Ch.Ranga Rao

“ The evaluation of the effect of
Gudanagaradi Vatiin Pandu
By
I.B.Kotturshetti

Introduction • In clinical practice first observation falls on
patients skin.
• The “Panduvarna” i.e Anemic Skin colour is easily noted by the physician.
• Thus the cause of the Pandu is noted as deficiency of vital nutrients and minerals.
• The incidence is so high in developing countries even though multi discipline regimens are available.

In Ayurvedic classics the term "Pandu" (Anaemia) familiar as a-
DiseaseSign or symptomComplication

Definition:• The word derives from
to it
•The pale white or yellowish white colour -Students Sanskrit English dictionaryby Vaman Sivaram Apte

Nidana:Samhita Ahara Vihara Manasika
KsharaAmla
Rasa
Lavana
DiwaswpnaVyayamaAtivyavaya
Kama
Guna Atiushna Prati Karma ChintaNishpav BhayaMasha Krodha
Tila taila
Charaka
Dravya
Prinyaka
Ritu vaishamyaVegadharana
Shoka
Amla DiwaswpnaRasa:
Lavana Ativyayama
Guna AtiteekshnaMadhya
SusrutaMadhava NidanaYogaratnakara
DravyaMrit

Pandu Poorvarupa Hrit Spandhana (palpitation) Rooksha (dryness) Swedabhava (No sweating) Shrama (Fatigue) Twak Sputana (cracking of skin) Hrillasa (Nausea) Pada gourava (Heaviness in lower limbs) Mridbhakshaneccha Akshi Koota shota (puffiness around eyes) Avipaka (Indigestion) Peeta mutrata (yellow urine) Peeta Purisha (yellow stool) Aruchi (loss of appetite)

SampraptiPitta pradhan tridosha prakopak nidan sevan
Agni vikar and rasa dusti
Dosha prakopa (mainly Sadhakapitta inside heart)
Prasara via srotas by vayu
Dhatu dusti (vikriti)
Dhatu kshaya (raktalpata)
Panduta (discoloration of skin)

Tabular form of Pandu Lakshana
S.No Lakshana Charaka Susruta Vagbhata1 Karnakseweda + - +2 Hatanala + - +3 Dourbalya + - +4 Sadana + - -5 Annadwesha + - +6 Shrama + - +7 Bhrama + - +8 Gatrashoola + - -9 Jwara + - +10 Swasha + - -

Tabular form of Pandu Lakshana-2
S.No Lakshana Charaka Susruta Vagbhata11 Gourava + - +12 Aruchi + - +13 Gatramardata + - +14 Gatrapeeda + - -15 Gatronmatana + - -16 Soonakshikoota + - +17 Harita varna + - Panduvarna18 Sheerna lomata + - +19 Hata prabha + - -20 Kopanata + - +

Tabular form of Pandu Lakshana - 3
S.No Lakshana Charaka Susruta Vagbhata21 Shishira dweshi + - +22 Nidraluta + - -23 Pindikodweshtana + - -24 Katiruk + - -25 Pada ruk + - -26 Pada sada + - -27 Ururuk + - -28 Kati sada + - -29 Uru sada + - -30 Dhatu saithilya + - +

Tabular form of Pandu Lakshana - 4
S.No Lakshana Charaka Susruta Vagbhata31 Ojo guna kshaya + - +32 Alpa raktata + Raktadusti +33 Alpamedaskata + - +34 Nissarata + - +35 Hridrava + - +36 Sithilendriyata + - +37 Twacha panduta + + +38 Swetakshitwa - - -39 Sweta nakhatwa - - -40 Swetha vakrata - - -

Method of collection of dataExclusive criteria• Age group of below 5 and above 55 years• Associated with vital organic disease• Sever blood loss• Parasitic infection• Discontinuation of treatment scheduleInclusive criteria
The patients of both sexesBetween the age of 5 to 55 years With mild to moderate Anaemia, Other than that of exclusive criteria

Study designProspective clinical trail
Sample size25 patients
Study duration 21 days
Posology40mg/kg, body weight /24 hours or maximum of 2gm./24hrs.
Assessment of results• The results will be assessed by clinical, as well
as haematological study.• Hb% is assessed for all at the interval of 7 days.

Hematological Investigations
Hemoglobin percentageTotal count of R.B.CPacked cell volumeMean corpuscular volumeMean corpuscular haemoglobin concentration Peripheral smearSerum iron

Preparation of Gudanagaradi Vati
IngredientsGuda - 1 partNagara - 1 partMandura - 1 partTila - 1 partPippali - 2 parts

Dravya Rasa Guna Veerya Vipaka OnDosha
Karma
Guda Madhura Laghu Seeta Madhura VPKAgni Vriddhi
RuchyaPanduhara
Shramahara
Nagara Katu Laghu Ushna Madhura KV
VatanulomanaAgni Deepana
PachanaSwarya
SwasaharaShoolahara
ManduraTikta
KashayaMadhura
GuruRooksha Seeta - VPK
Pandu, Arsha,Shootha,
Pleeharoga,Kamala, Sosha,
Krimihara
TilaKatu
KashayaMadhura
Tikta
SnigdhaGuru Ushna
Katu(Madhura
-Su)V
BalyaDeepanaPachanaBrimhanaPreenana
Twakprasadana
Pippali KatuLaghu
SnigdhaTeekshna
Anushnashee
taMadhura KV
YogavahiJatharagnideepana
KasaswasaharaPanduharaKrimiharaRasayana

Observations in StudyTotal Patients 25
• Aruchi 24
• Agnimandya 24
• Toda 20
• Alasya 24
• Tandra 20
• Kampana 18
• Prabhanasha 16
• Nissara 14
• Pandu Twacha 21
• Pandu Netra 24
• Pandu Nakha 24
• Shrama 25
• Bhrama 23
• Gatra Shoola 24
• Sadana 15
• Alpameda 19

Ahara• Amla 20
• Lavana 18
• Teekshna 17
Vihara• Ativyayama 16
• Ativyavaya 10
Manasika Karana• Chinta 23
• Shoka 14
NidanaTotal Patients = 25

Observations at the IntervalsBefore
treatmentAfter 7days
After 14days
Aftertreatment
Differenceof Beforeand After
Heamoglobin %(gm/L)
8.328 8.86 9.38 10.044 1.712
Total RBC count inmillion/ Cu mm
4.816 5.012 5.184 5.42 0.604
Statistical assessmentCategory Hb % Total RBC
countPCV % Serum
IronMean Deviation 1.712 0.604 2.72 7.3896
Standard Deviation 0.7618 0.1989 0.9363 4.515S.E 0.1524 0.0397 0.1873 0.903
"t" Test 11.234 15.1835 14.522 8.1833P - Value <0.001 <0.001 <0.001 <0.001Remarks H.S H.S H.S H.S
H.S = Highly Significant

Statistical representation of Gudanagaradi Vatishows Highly Significance with P value < 0.001.
The Correlation co-efficient between hemoglobin and total RBC counts before treatment (experiment) is 0.4589 and after the completion of drug is 0.586.
This shows that there is an increased relation between the above-mentioned investigations, Hb% and Total RBC count.
It is tested for the significance of correlationco-efficient "t" value is 3.47 & "P" value is <0.001,(less then 0.01) which is highly significant.
The correlation co-efficient between Hemoglobin % and Serum Iron before to treatment is negatively co-related (r = - 0.044), where as after treatment it was positively correlated (r = 0.067).
It shows that inter relationship between two investigations mentioned above are moderately improved.

ResultNot
Responded0%
Responded20%
Cured28%
Palliative52%
13 Patients
7 Patients5 Patients

ConclusionThis study was formulated to evaluate the effect of Gudanagaradi Vati in Pandu.In this study most of the symptoms explained in the text are reported.All symptoms reported responded well.The drug significantly evaluated the Haemoglobin concentrations in the blood.It is proved through statistical evaluation and also significance of correlation co-efficient "t" value.
Over all response to the drug was exceptionally best.

Thank You


















