Pancreatic Transplantation: What the Radiologist Needs to Know … · 15 Exocrine drainage The...
6
ACTA RADIOLÓGICA PORTUGUESA Janeiro-Abril 2017 Vol 29 nº1 13-18 Pancreatic Transplantation: What the Radiologist Needs to Know Transplante Pancreático: O que o Radiologista Deve Saber Natalie Antunes, Rosana Santos, Fernando G. Almeida, Nuno Carrilho 1Departamento de Radiologia, Hospital de Santa Marta, Centro Hospitalar Lisboa Central (CHLC), Lisboa, Portugal 2 Departamento de Radiologia, Hospital Curry Cabral, Centro Hospitalar Lisboa Central (CHLC), Lisboa, Portugal Correspondência Natalie Antunes Centro Hospitalar Lisboa Central (CHLC) Departamento de Radiologia Hospital de Santa Marta Rua de Santa Marta, nº 50 1169-024 Lisboa Portugal e-mail: [email protected] 13 Resumo O transplante pancreático representa uma alternativa cirúrgica para o tratamento de casos selecionados de doentes diabéticos, com o objetivo de evitar as complicações sistémicas da doença. A abordagem mais frequente é o transplante pancreático-renal simultâneo, em que o pâncreas é geralmente posicionado intra- peritonealmente na região pélvica direita. Vários métodos de imagem são usados para a avaliação do enxerto parenquimatoso, a anatomia vascular e a drenagem entérica. A compreensão do procedimento cirúrgico, das técnicas utilizadas e da anatomia pós-procedimento é fundamental à medida que o número destes casos aumenta. O radiologista deve também conhecer as possíveis complicações associadas e a sua aparência imagiológica, com a finalidade de preservar a máxima função do enxerto. Palavras-chave Pâncreas; Transplante; Diabetes; Imagiologia pancreática; Complicações pancreáticas Abstract Pancreatic transplantation represents a surgical alternative for the treatment of selected cases of diabetic patients, with the goal of avoiding the systemic complications associated with the disease. The most frequent approach is the simultaneous pancreas-kidney transplant, in which the pancreas is usually placed intraperitoneally in the right pelvis. Several imaging methods are used for the evaluation of the parenchymal graft, the vascular anatomy and the enteric drainage. An understanding of the transplantation procedure, the surgical techniques and the post-procedural anatomy is elemental as the number of these cases increases. The radiologist must also be aware of the possible associated complications and their imaging appearance, with the aim of preserving maximum graft function. Keywords Pancreas; Transplantation; Diabetes; Pancreatic imaging; Pancreatic complications Artigo de Revisão / Review Article Introduction Pancreatic transplantation represents a surgical alternative for the treatment of selected cases of insulin-dependent diabetes mellitus, mostly type 1 (93% of cases) and is indicated in patients with end-stage renal disease and/or failure to achieve glycemic control with a high risk for the development of secondary complications. 1 A relative contra-indication is the patient’s age (> 55 y.o.), due to the fact that the success rate is superior in younger individuals. 8 Its goals include the restoration of euglycemia, by providing a sufficient mass of ß-cells, and preventing or delaying systemic complications such as nephropathy or retinopathy. The procedure is associated with improved quality of life (partly because it reduces the need of insulin therapy and dialysis) and life expectancy. 2 Despite the recent advances of the surgical technique and immunosuppressive agents, which allowed higher graft survival rates (see Surgical Technique), the frequency of pancreatic transplantation procedures has been declining since 2014, 14 which is attributable to several factors: absence of appropriate primary referral, improvement in the medical care of diabetes, lack of acceptance in the diabetic community. 16 Although the global prevalence of type 1 diabetes mellitus is unknown, it is estimated that there are approximately 3 million patients in the USA 15 and until 2010 25.000 pancreatic transplantations were performed in this country, 14 which reflects that < 1% of cases are treated with this procedure. The most frequently used technique is whole-organ transplant from a cadaveric donor. The graft evaluation is generally multimodal, using ultrasound (US), computerized tomography (CT) or magnetic resonance (MR), depending on the clinical context. The imaging evaluation of the pancreatic transplant represents a challenge for the radiologist; here we review the most frequent transplantation techniques, the complex post-surgical anatomy and the possible spectrum of complications following the procedure. Surgical Technique & Post-operative Anatomy The most frequent surgical approach is the simultaneous pancreas-kidney transplant (SPK), in which the pancreatic and renal grafts of a single donor are inserted in one surgical act. This option represents approximately 80% of cases in USA; 2 the remainder being pancreas-after- kidney transplantation (PAK) and pancreas transplant alone (PTA), the latter usually indicated in diabetic patients with inadequate glycemic control but without nephropathy criteria. 2
Transcript of Pancreatic Transplantation: What the Radiologist Needs to Know … · 15 Exocrine drainage The...

ACTA RADIOLÓGICA PORTUGUESAJaneiro-Abril 2017 Vol 29 nº1 13-18
Pancreatic Transplantation: What the Radiologist Needs to Know
Transplante Pancreático: O que o Radiologista Deve Saber
Natalie Antunes, Rosana Santos, Fernando G. Almeida, Nuno Carrilho
1Departamento de Radiologia, Hospital de Santa Marta, Centro Hospitalar Lisboa Central (CHLC), Lisboa, Portugal2Departamento de Radiologia, Hospital Curry Cabral, Centro Hospitalar Lisboa Central (CHLC), Lisboa, Portugal
Correspondência
Natalie Antunes Centro Hospitalar Lisboa Central (CHLC)Departamento de RadiologiaHospital de Santa MartaRua de Santa Marta, nº 50 1169-024 LisboaPortugale-mail: [email protected]
13
Resumo
O transplante pancreático representa uma alternativa cirúrgica para o tratamento de casos selecionados de doentes diabéticos, com o objetivo de evitar as complicações sistémicas da doença. A abordagem mais frequente é o transplante pancreático-renal simultâneo, em que o pâncreas é geralmente posicionado intra-peritonealmente na região pélvica direita. Vários métodos de imagem são usados para a avaliação do enxerto parenquimatoso, a anatomia vascular e a drenagem entérica. A compreensão do procedimento cirúrgico, das técnicas utilizadas e da anatomia pós-procedimento é fundamental à medida que o número destes casos aumenta. O radiologista deve também conhecer as possíveis complicações associadas e a sua aparência imagiológica, com a finalidade de preservar a máxima função do enxerto. Palavras-chave
Pâncreas; Transplante; Diabetes; Imagiologia pancreática; Complicações pancreáticas
Abstract
Pancreatic transplantation represents a surgical alternative for the treatment of selected cases of diabetic patients, with the goal of avoiding the systemic complications associated with the disease. The most frequent approach is the simultaneous pancreas-kidney transplant, in which the pancreas is usually placed intraperitoneally in the right pelvis. Several imaging methods are used for the evaluation of the parenchymal graft, the vascular anatomy and the enteric drainage. An understanding of the transplantation procedure, the surgical techniques and the post-procedural anatomy is elemental as the number of these cases increases. The radiologist must also be aware of the possible associated complications and their imaging appearance, with the aim of preserving maximum graft function.
Keywords
Pancreas; Transplantation; Diabetes; Pancreatic imaging; Pancreatic complications
Artigo de Revisão / Review Article
Introduction
Pancreatic transplantation represents a surgical alternative for the treatment of selected cases of insulin-dependent diabetes mellitus, mostly type 1 (93% of cases) and is indicated in patients with end-stage renal disease and/or failure to achieve glycemic control with a high risk for the development of secondary complications.1 A relative contra-indication is the patient’s age (> 55 y.o.), due to the fact that the success rate is superior in younger individuals.8Its goals include the restoration of euglycemia, by providing a sufficient mass of ß-cells, and preventing or delaying systemic complications such as nephropathy or retinopathy. The procedure is associated with improved quality of life (partly because it reduces the need of insulin therapy and dialysis) and life expectancy.2Despite the recent advances of the surgical technique and immunosuppressive agents, which allowed higher graft survival rates (see Surgical Technique), the frequency of pancreatic transplantation procedures has been declining since 2014,14 which is attributable to several factors: absence of appropriate primary referral, improvement in the medical care of diabetes, lack of acceptance in the diabetic community.16 Although the global prevalence of type 1 diabetes mellitus is unknown, it is estimated that there are approximately 3 million patients in the USA15 and until 2010 25.000 pancreatic transplantations were
performed in this country,14 which reflects that < 1% of cases are treated with this procedure.The most frequently used technique is whole-organ transplant from a cadaveric donor.The graft evaluation is generally multimodal, using ultrasound (US), computerized tomography (CT) or magnetic resonance (MR), depending on the clinical context. The imaging evaluation of the pancreatic transplant represents a challenge for the radiologist; here we review the most frequent transplantation techniques, the complex post-surgical anatomy and the possible spectrum of complications following the procedure.
Surgical Technique & Post-operative Anatomy
The most frequent surgical approach is the simultaneous pancreas-kidney transplant (SPK), in which the pancreatic and renal grafts of a single donor are inserted in one surgical act. This option represents approximately 80% of cases in USA;2 the remainder being pancreas-after-kidney transplantation (PAK) and pancreas transplant alone (PTA), the latter usually indicated in diabetic patients with inadequate glycemic control but without nephropathy criteria.2

14
SPK demonstrated the best graft survival outcome of the three options; it also presented the best 10-year patient survival rates compared to diabetic patients who were submitted to only kidney transplantation.2The donor’s pancreas is harvested en bloc with its respective vascular support and a variable duodenal segment that contains the Ampulla of Vater.The most common technique consists in placing the pancreatic graft intraperitoneally in the right pelvic region and the renal graft in the left iliac fossa, extraperitoneally (Fig. 1).
The chosen surgical technique is usually dictated by the donor’s anatomy and the surgeon’s preference.2The portal drainage option represents a more physiologic mechanism for endocrine drainage and can avoid possible cases of hyperinsulinemia, but did not show better results in terms of cardiovascular mortality.
Figure 1 – Simultaneous pancreas-kidney transplant (SPK). Axial contrast-enhanced CT in a transplanted patient shows the usual positioning of the allografts. (pancreas - -> ; kidney g).
Arterial Supply
The pancreatic allograft receives its arterial inflow from the donor’s superior mesenteric artery – through the inferior pancreaticoduodenal artery (cephalic segment) – and from the splenic artery and its branches (body and tail segments).Additionally, the donor’s common iliac artery and its bifurcation are also retrieved, with the purpose of creating an inverted “Y” conduit, in which the internal and external iliac arteries are anastomosed end-to-end to the splenic and superior mesenteric artery, respectively (table 1).On the other hand, the common iliac artery of the donor is anastomosed end-to-side to the recipient’s common iliac artery (usually the right) (Fig. 2).
Table 1 – Arterial supply in pancreatic graft implantation. Illustrative dia-gram of the anastomoses created with the vascular supply of the donor and the recipient.
Venous/endocrine DrainageThe intrapancreatic venous tributaries drain in the superior mesenteric and splenic veins and, finally, in the donor’s portal vein, which is also harvested. The portal vein may, in turn, be anastomosed to the recipient’s common iliac vein or inferior vena cava – an option referred to as systemic drainage (Figs. 3 and 4) – or to the recipient’s superior mesenteric vein – portal drainage. Usually the cephalic pancreatic segment is displayed caudally in the case of systemic venous drainage and cranially in the portal drainage option.
Figure 2 – Arterial anastomoses in pancreatic transplantation. (a) (b) Contrast-enhanced CT in which (b) represents an inferior plane than (a), demonstrates (°) the anastomosis between the right common iliac artery and (->) the branching in superior mesenteric and splenic arteries. (c) VRT (Volume rendered CT) shows (g) the arterial anastomosis between the recipient’s right common iliac artery and the donor’s internal and external iliac arteries. Pancreatic graft (4 ).
Figure 3 – Systemic venous drainage in pancreas transplantation. The anastomosis between the inferior vena cava (recipient) and the portal vein (donor) is signalled (g).
Figure 4 – Venous drainage in SPK transplant. VRT (Volume rendered CT) reveals the venous anastomosis (arrow) between the portal vein (donor) and the inferior vena cava (recipient).

15
Exocrine drainage
The exocrine pancreatic secretions drain through the donor’s duodenum, that can be anastomosed to the small bowel (through a duodeno-jejunostomy with or without the creation of “Roux-en-Y”), approach designated as enteric, or to the recipient’s bladder (vesical drainage). The first option represents the majority of the procedures nowadays (approximately 80%) (Fig. 5). The duodeno-cystostomy presented several complications – chemical cystitis, hematuria, recurrent urinary tract infections, urethral stenosis – and has progressively been abandoned. In this case, the duodenal stump was anastomosed to the superior aspect of the bladder; this option had the advantage of monitoring the pancreas allograft’s function through urinary amylase.
patency – spectral Doppler mode (Fig. 7). Normal arterial waveform exhibits a sharp systolic upstroke and a continuous diastolic flow. In the immediate post-operative period the velocities of the arterial anastomosis may be very high due to possible post-operative edema and/or kinking of the anastomosis. Additionally, ultrasound may be fundamental in guiding the percutaneous biopsy.
Computed TomographyAllows assessment of the parenchyma, the vascular and enteric anastomoses and possible associated complications. The most frequent indications for CT are the suspicion of enteric complications, pancreatitis or abdominal infection. The protocol used should include (positive) enteric contrast that allows identification of intestinal loops adjacent to the graft and distinction from possible liquid collections. The donor’s duodenum is frequently collapsed, and may fill (or not) with the given oral contrast. The study should be multiphasic; however, the use of endovenous iodinated contrast should be weighed due to the risk of worsening the baseline renal function of these patients and their clinical context. Non-enhanced images should be acquired with the goal of locating the graft and possible early thrombus or hematoma. Late arterial phase can be obtained with the bolus-tracking technique located in the common iliac artery (attenuation value of 150 HU) and is very useful in the assessment of parenchymal enhancement and arterial anastomoses (Fig. 8a). 50 seconds after the administration of intravenous contrast material the portal venous phase evaluates the respective drainage and possible associated venous complications.8The graft’s parenchyma should demonstrate homogeneous enhancement, more intense in the arterial phase. The duodeno-jejunostomy is more easily identified in multiplanar reformations (coronal plane) (Fig. 8b).
Figure 5 – Exocrine drainage: enteric approach. Coronal CT reformat demonstrates the duodeno-jejunostomy (signalled by the metallic sutures – arrow).
Pancreatic Transplantation Imaging
UltrasoundUltrasound usually represents the first line imaging method in the assessment of the pancreatic graft, due to its portability and lack of ionizing radiation. Its evaluation may, however, be limited due to the intraperitoneal position of the allograft and intestinal gas overlap. B-mode US allows assessment of the parenchyma and possible complications, as intra- or peri-pancreatic fluid collections. Normal parenchyma should demonstrate a homogeneous echotexture, solid with low-level echoes, slightly hypoechoic relative to the native pancreas and adjacent mesenteric fat (Fig. 6).3Doppler US is essential in the evaluation of parenchymal perfusion – color Doppler mode – and vascular anastomosis
Figure 6 – US appearance of a normal pancreatic graft (g). Longitudinal image illustrates normal homogeneous echotexture and slight inferior echogenicity relative to the adjacent mesenteric fat.
Figure 7 – Doppler-mode US of pancreatic graft. Splenic artery (left image) and splenic vein (right image) examination are normal in this recently transplanted patient.

16
Figure 8 – Contrast-enhanced CT in late arterial phase of SPK transplant. (a) Axial image depicts the parenchyma of both grafts (g), the anastomoses and possible complications, such as a non-occlusive thrombus in the inferior vena cava (dotted arrow). Normal splenic vein is signaled (-->). (b) Coronal reformation in another patient who had a previous renal transplant (- ->), that failed. The pancreatic allograft parenchyma is unaltered (g). Note the metallic sutures adjacent to the duodeno-jejunostomy.
Magnetic ResonanceMR is usually indicated in young patients in which cumulative radiation is an essential consideration; it demonstrates, however, a lower spatial resolution compared with CT. An appropriate protocol includes axial T1-weighted (T1-WI) (pre-contrast; in-phase and out-of-phase), coronal T2-weighted (T2-WI) fast-spin-echo and axial T2-weight fat-suppressed sequences. Furthermore, images after intravenous contrast administration (gadolinium-based) should be acquired in arterial and venous phases.8In T1-WI the graft’s parenchyma should be homogeneous and hyperintense relative to the liver and usually demonstrates an intermediate signal between liquid and muscle in T2-WI.3MR cholangio-pancreatography (MRCP), on the other hand, presents the possibility of ductal system analysis.
AngiographyUsually reserved for patients who need endovascular intervention (venous trombectomy, stent placement, others).
ComplicationsThe most common complications include fluid collections, parenchymal, vascular and enteric complications (Table 2).
Early post-operative (until 4 weeks after transplantation)2
In the early post-operative period, the following complications are possible:
• Small peri-pancreatic fluid collections;• Duodenal wall thickening (donor);
Table 2 – Possible types of complications associated with pancreatic transplantation.
• Main pancreatic duct ectasia;• Peri-pancreatic fat stranding;
being that most are self-limited and do not determine functional repercussions.2
Fluid collectionsRepresent the most frequent complications associated to pancreatic transplantation, with an estimated incidence of 20%.9,13. Most arise in the first month following the procedure. They may reflect several entities: seroma (Fig. 9b), hematoma, abscess (Fig. 10), pseudo-cyst or lymphocele. They encompass, therefore, a broad severity spectrum: from clinically insignificant to potentially fatal. Multimodality imaging evaluation is frequently necessary. Percutaneous drainage, ultrasound- or CT-guided, may be vital for its definitive diagnosis and treatment, since imaging findings may be not specific.
Parenchymal complicationsMost pancreatitis cases occur in the early post-operative period (< 4 weeks) and are usually due to reperfusion injury.
Figure 9 – (a) Findings in the early post-operative period. Contrast-enhanced axial CT shows diffuse graft enlargement associated with free fluid and stranding of the adjacent mesenteric fat. These findings resolved spontaneously over the following weeks. (b) Peritransplant fluid collections. Coronal enhanced CT image demonstrates multiple fluid collections adjacent to the pancreatic graft that represented seromas.
(a) (b)

17
Figure 10 – Peritransplant collections: abscess. (a) Several peritransplant collections with a thick enhancing capsule (g) suspected to be abscesses. (b) In another patient with elevated inflammatory parameters, contrast-enhanced CT revealed (g) intra- and peri-graft collections, some containing gas bubbles. Percutaneous aspiration confirmed the presence of purulent content.
They are estimated to take place in up to 35% of cases,2 although the majority are sub-clinical and self-limited. In cases of severe pancreatitis US may show graft enlargement and heterogeneous structure and/or possible complications, such as fluid collections. Doppler mode US may evaluate the degree of parenchymal perfusion. Contrast-enhanced CT or MR are paramount in assessing regional or diffuse lack of parenchymal enhancement in cases of necrotizing pancreatitis as well as eventual complications (thrombosis, abscess, haemorrhage) (Fig. 11).
Rejection (acute, sub-acute or chronic) represents a pivotal cause of allograft loss and it is estimated that the chronic form occurs in 4-10% of the cases.2 Even though some imaging findings may be suggestive – glandular dimensional change, altered pattern of contrast enhancement, changes in T1 and T2 signal – these features are not specific, and graft’s biopsy with histological characterization remains the gold-standard.10
Vascular complicationsThese types of complications represent the most frequent cause of early transplantation failure.2Thrombosis (arterial or venous) usually happens in the first weeks after transplantation and may predispose to infarct, dehiscence of the anastomosis or infection. It affects approximately 5-14%2 of procedures and is usually multifactorial in origin. The chronic form (months – years after transplant) may represent the late stage of the rejection process. The US appearance of the graft in these cases is usually not specific: may be enlarged with loss of its echogenicity – due to associated edema – or with a heterogeneous structure. Doppler-mode evaluation is, therefore, paramount in revealing the absence of flow in the affected vessel and, occasionally, in the parenchymal enhancement of the graft (Fig. 12a).8 In contrast-enhanced
Figura 11 – Acute pancreatitis after SPK transplantation. In this patient with increasing inflammatory parameters (amylase and lipase) contrast-enhanced CT revealed an enlarged heterogeneous parenchymal graft, heterogeneous enhancement and adjacent fluid collections (g).
CT or MRI a thrombus may be demonstrated as a filling defect or an intra-luminal hypointensity, respectively, associated, or not, with diminished/absence of parenchymal enhancement (Fig. 12b). Stenosis of the anastomosis is uncommon and usually occurs in the early post-operative period. Pseudo-aneurysms are frequently associated to surgical or biopsy trauma, severe pancreatitis or infection. The arterial anastomoses are particularly prone to this type of complication. In US evaluation they are defined as anechoic structures, round or oval, immediately adjacent to the vessels, with internal “yin-yang” flow in Doppler-mode imaging. Contrast-enhanced CT or MR identify a saccular dilatation of the affected vessels that displays similar enhancement as the contiguous vascular territory. Arteriovenous fistula is an uncommon vascular compli-cation, usually as an iatrogenic effect (post-surgery or
Figure 12 – (a) Arterial thrombosis of the pancreatic allograft. Doppler-mode US evaluation demonstrates lack of appropriate flow in the superior mesenteric artery, suggestive of arterial thrombosis. Mode-B US was featureless (not shown). (b) Venous thrombosis in pancreatic transplant (enteric and intravenous contrast-enhanced axial CT). An intraluminal filling defect (g) is seen in the inferior aspect of the splenic vein, in keeping with partial venous thrombosis.
18
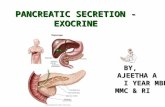
Figure 13 – Venous thrombosis associated with pancreas transplantation. (a) Sagittal and (b) axial contrast-enhanced CT illustrate non-occlusive thrombosis (arrows) of the inferior vena cava adjacent to the venous anastomosis of the pancreatic graft.
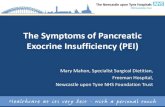
Figure 14 – Enteric complication in pancreatic graft implantation: small bowel obstruction. In a patient with symptoms of intestinal obstruction, CT highlighted significant small bowel dilatation that was attributable to adhesions.
biopsy). Doppler-mode evaluation reveals high velocity and low resistance turbulent flow in an arterial lumen that communicates with a vein, which, in turn, exhibits pulsatile flow. The arterial phase study may identify an early enhancement of the affected drainage vein (Fig. 13).
Enteric complicationsSmall bowel obstruction may be secondary to adhesions or internal hernia that arise from a mesenteric defect created during the surgical procedure (Fig. 14).
Recebido / Received 08/09/2016 Aceite / Acceptance 29/01/2017
Divulgações Éticas / Ethical disclosuresConflitos de interesse: Os autores declaram não possuir conflitos de interesse.Conflicts of interest: The authors have no conflicts of interest to declare.Suporte financeiro: O presente trabalho não foi suportado por nenhum subsídio ou bolsa. Financing Support: This work has not received any contribution, grant or scholarship.
Referências1. Hampson FA, Freeman SJ, Ertner J. Pancreatic transplantation: surgical technique, normal radiological appearances and complications. Insights Imaging. 2010;1:339-47. 2. O’Malley RB, Moshiri M, Osman S, Menias CO, Katz DS. Imaging of pancreas transplantation and its complications. Radiol Clin North Am. 2016;54(2):251-66.3. Vandermeer FQ, Manning MA, Frazier AA, Wong-You-Cheong JJ. Imaging of whole-organ pancreas transplants. Radiographics. 2012;32:411-35. 4. Oliver J, Beidas AK, Bongu A. A comparison of long-term outcomes of portal versus systemic venous drainage in pancreatic transplantation: systematic review and meta-analysis. Clin Transplant. 2015;29:882-92.5. Sandrasegaran K, Lall C, Berry WA, Hameed T, Maglinte DD. Enteric drainage pancreas transplantation. Abdom Imaging. 2006;31:588-95.6. Freund MC, Steurer W, Gassner EM. Spectrum of imaging findings after pancreas transplantation with enteric exocrine drainage: Part 1, posttransplantation anatomy. Am J Roentgenol. 2004;182:911-17.
7. Powell FE, Harper SJ. Postoperative CT in pancreas transplantation Clin Radiol. 2015;70:1220-8. 8. Tolat PP, Foley WD, Johnson C. Pancreas transplant imaging: how I do it. Radiology. 2015;275:14-27.9. Heller MT, Bhargava P. Imaging in pancreatic transplants. Indian J Radiol Imaging. 2014;24:339-49.10. Chen JL. Lee RC, Shyr YM. Imaging spectrum after pancreas transplantation with enteric drainage Korean J Radiol. 2014;15:45-53.11. Franca M, Certo M, Martins L. Imaging of pancreas transplantation and its complications Insights Imaging. 2010;1:329-38.12. Gimenez JM, Bluth EI, Simon A, Troxclair L. Evaluation of pancreatic allografts with sonography. J Ultrasound Med, 2012;31:1041-51. 13. Singh RP, Vrakas G, Hayek S. Clinically significant peripancreatic fluid collections after simultaneous pancreas-kidney transplantation. Transplantation. 2013;95:1263-69.14. Gruessner AC. Update on pancreas transplantation: comprehensive trend analysis of 25,000 cases followed up over the course of twenty-four years at the International Pancreas Transplant Registry (IPTR). Rev Diabet Stud. 2011;8:6-16.15. Chiang J, Kirkman S, Laffel L, Peters A. Type 1 diabetes through the life span: a position statement of the american diabetes association. Diabetes Care. 2014;37:2034-54.16. Stratta RJ, Fridell JA, Gruessner AC, Odorico JS, Gruessner RW. Pancreas transplantation: a decade of decline. Curr Opin Organ Transplant. 2016;21:386-92.
Enteric anastomosis leaks (duodeno-jejunostomy) may be early – attributable to ischemia – or late (4-weeks post-procedure) – secondary to infection or rejection. Free fluid, fluid collections and/or intra-peritoneal free air may be demonstrated in the imaging evaluation. In this context enteric contrast administration may be useful, revealing its intraperitoneal extravasation.
Conclusion
Pancreatic transplantation represents a therapeutic option in advanced cases of diabetes. The most frequent approach is simultaneous pancreatico-renal transplantation, which demonstrates the best graft survival rates. The surgical technique involves the creation of vascular and enteric anastomoses whose features the radiologist must be aware of. The imaging evaluation of the graft includes US, CT and MR depending on the indication and clinical context. The associated complications may be divided in parenchymal, vascular, enteric or fluid collections. Contrast-enhanced CT represents the best imaging method for the assessment of the vascular and enteric complications. Imaging techniques are also valuable in biopsy graft guidance (in case of suspected rejection) and to guide percutaneous drainage of collections.