Pancreatic neoplasms
209
Pancreatic Neoplasms CHAIRPERSON DR. ARVIND K MS MCH ASSOCIATE PROFESSOR AND UNIT CHIEF DEPT. OF GENERAL SURGERY KIMS HUBLI PRESENTER Dr. Ajai Sasidhar PG Student
-
Upload
ajai-sasidhar -
Category
Health & Medicine
-
view
110 -
download
1
Transcript of Pancreatic neoplasms
Pancreatic Neoplasms
CHAIRPERSONDR. ARVIND K MS MCHASSOCIATE PROFESSOR AND UNIT CHIEFDEPT. OF GENERAL SURGERYKIMS HUBLI
PRESENTER
Dr. Ajai Sasidhar
PG Student
The most unforgiving organ in the human body.
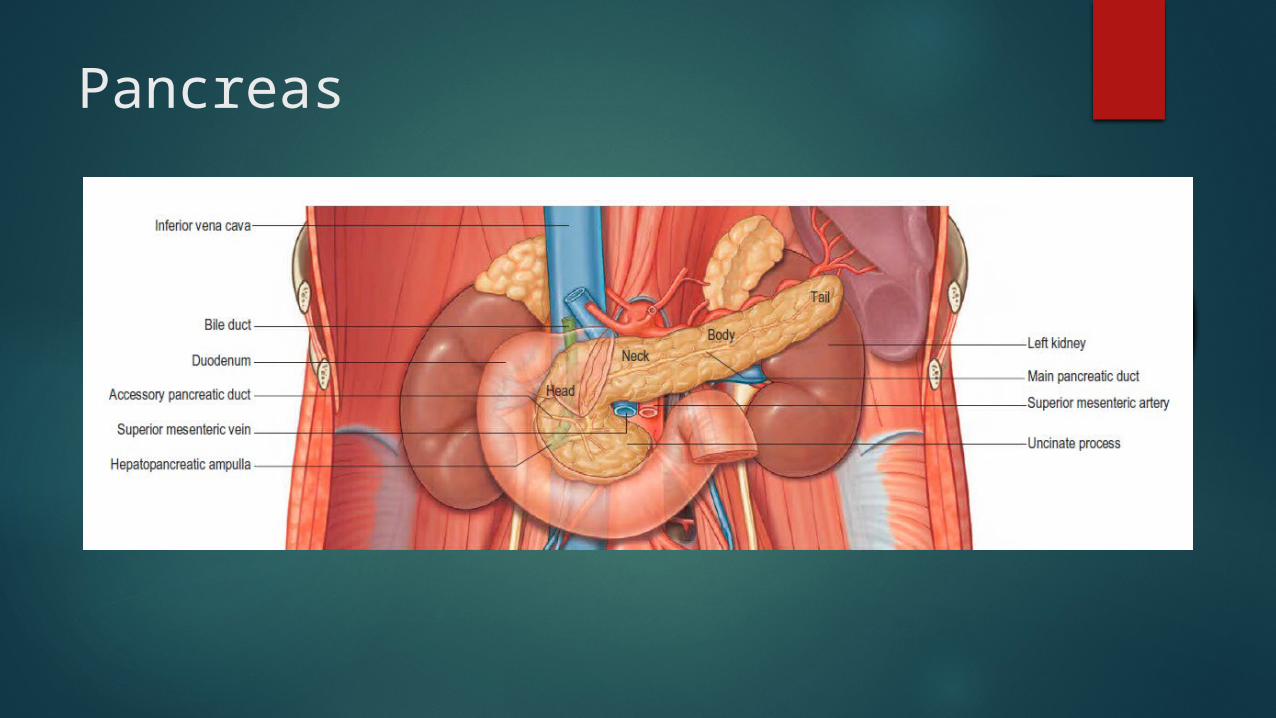
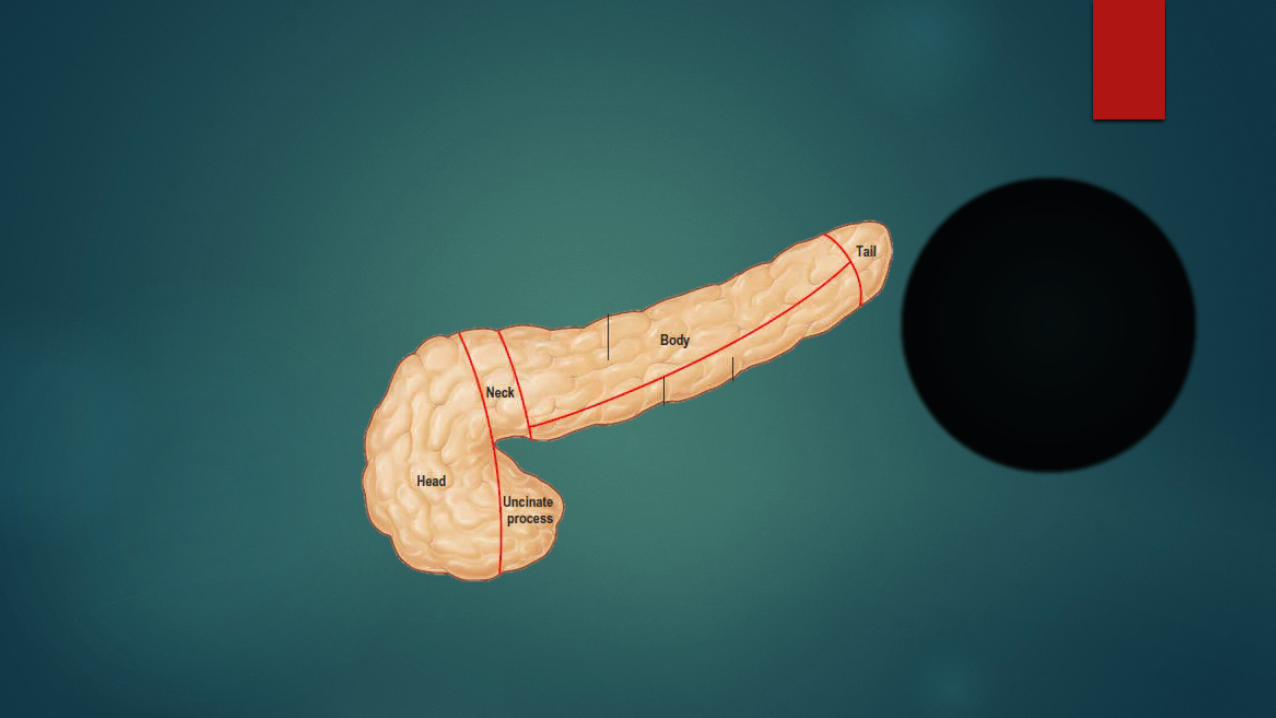
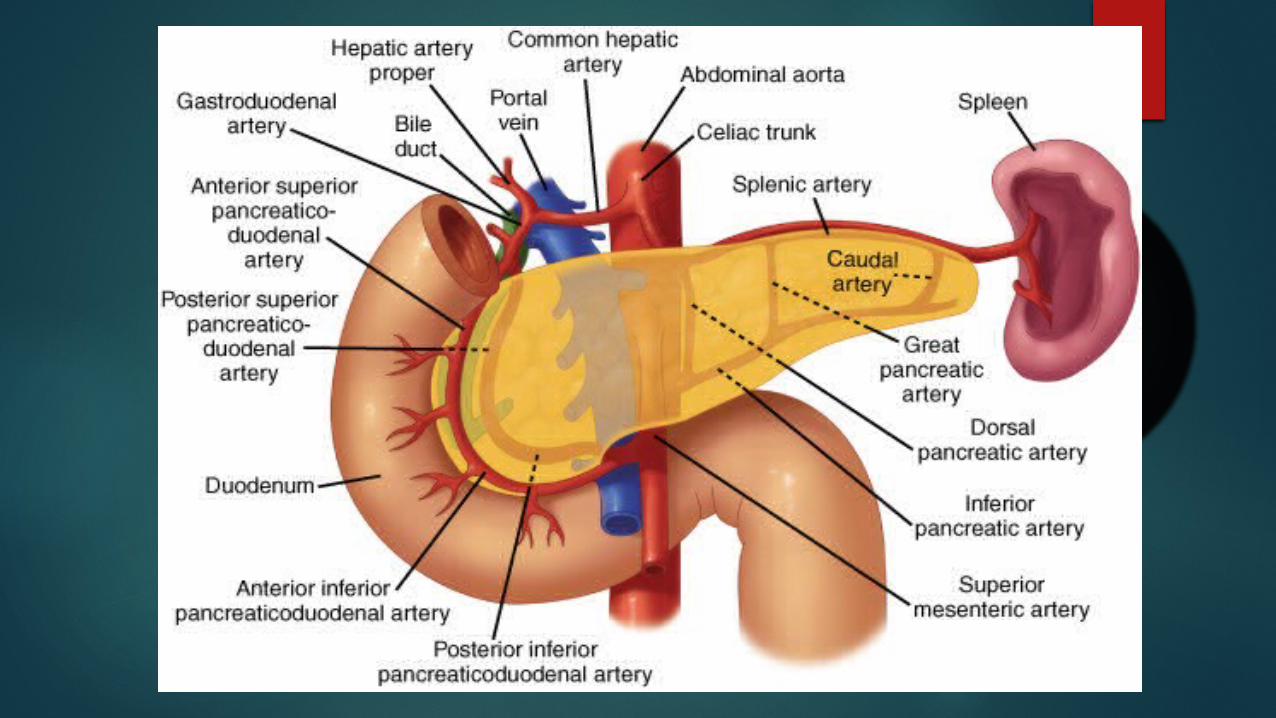
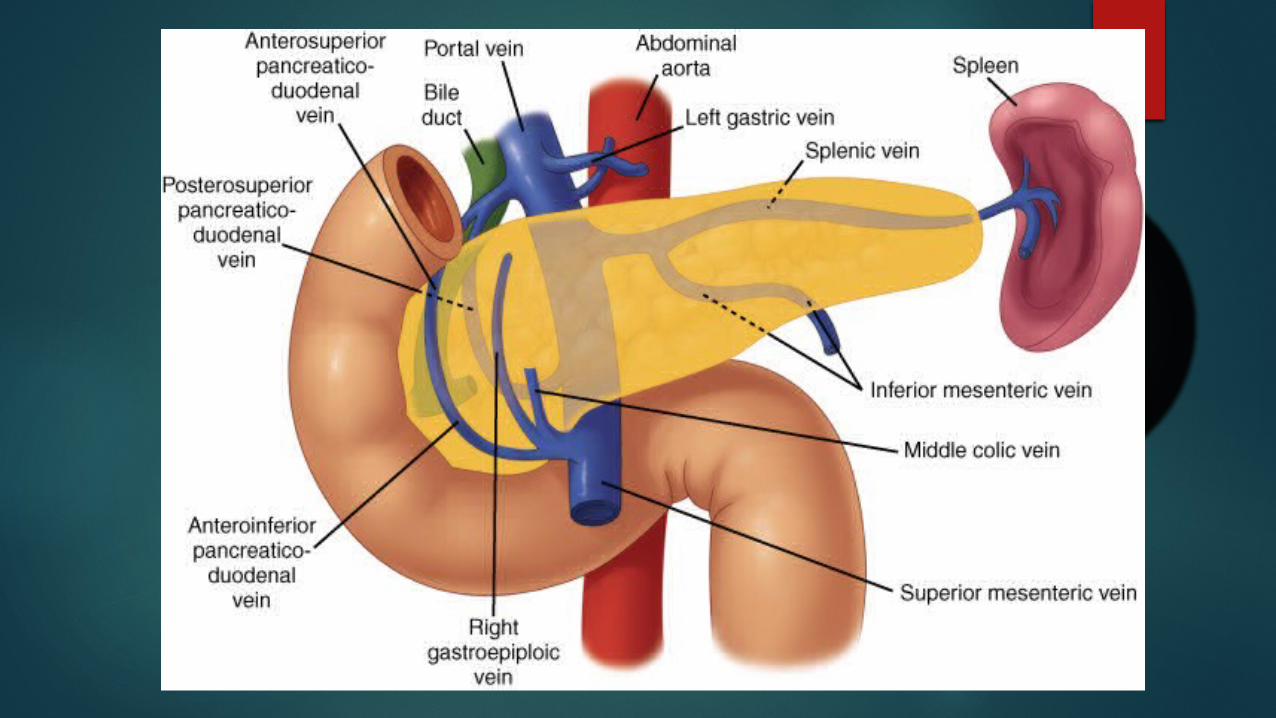
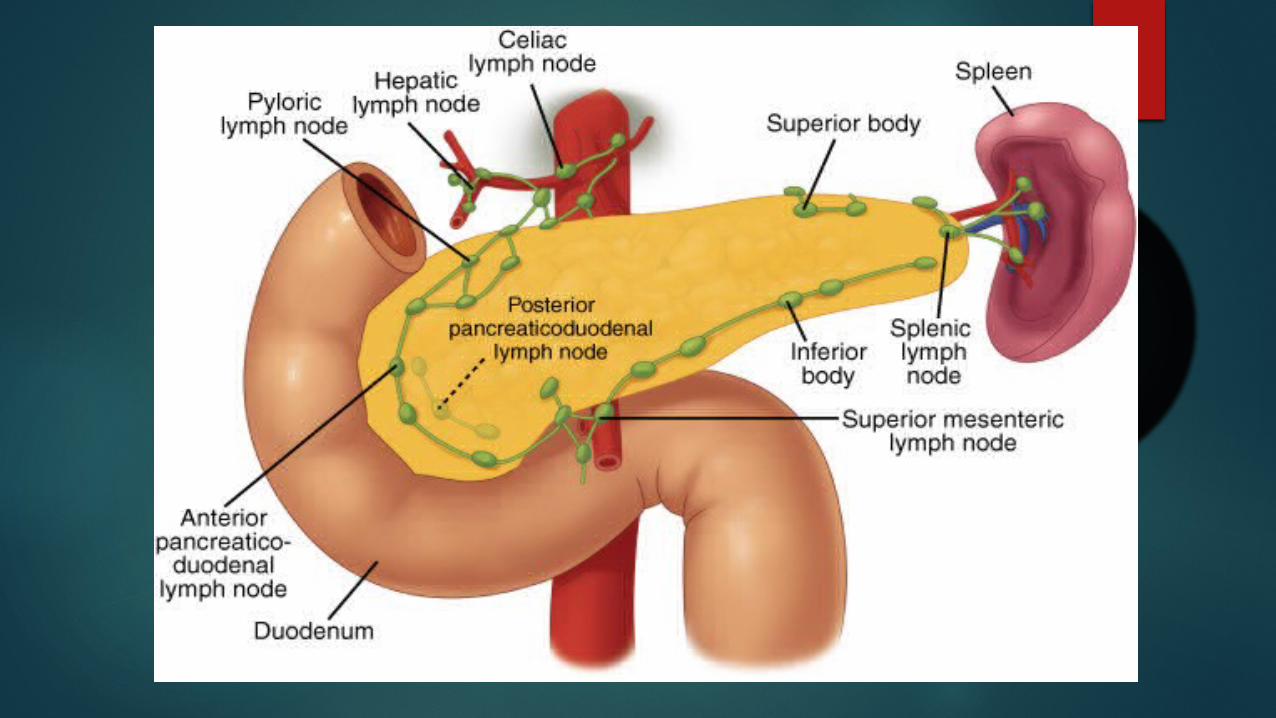
Pancreas
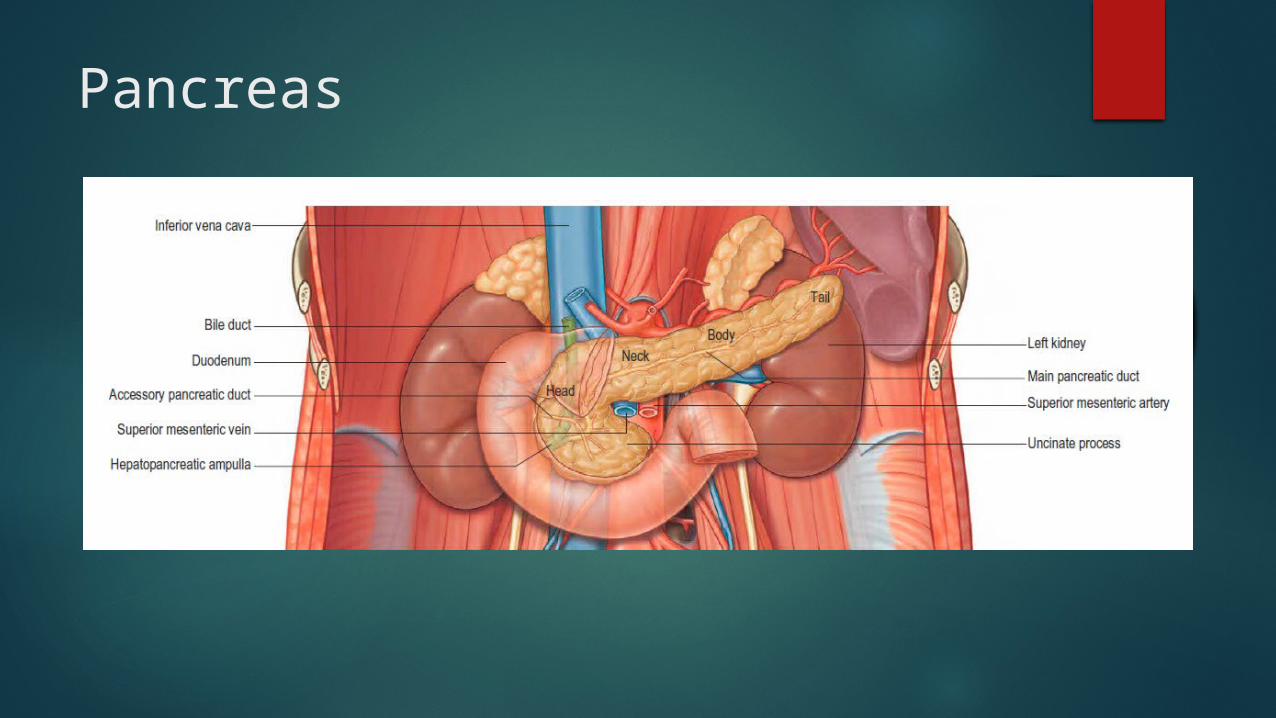
Pancreas

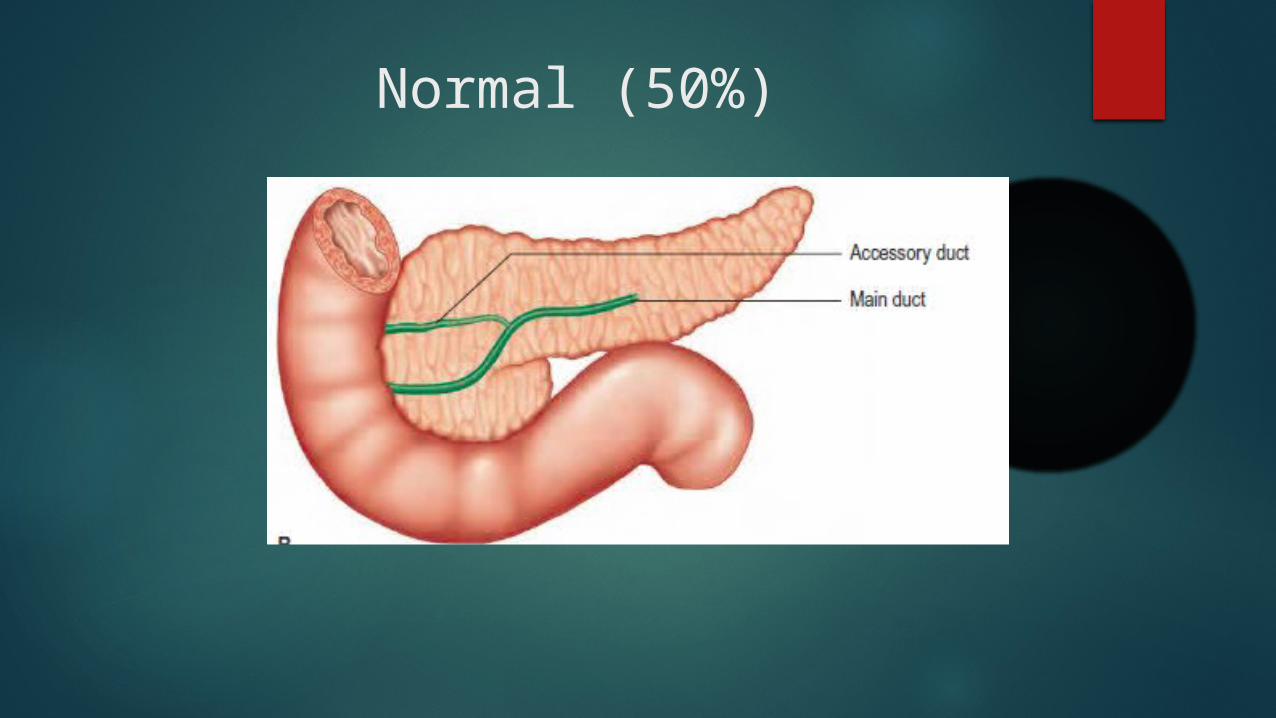
Normal (50%)

Pancreatic Neoplasms
Neoplasms of the pancreas
Solid tumors (Adeno Carcinomas) Cystic Neoplasms Endocrine tumors
Pancreatic adeno carcinoma5-year survival rate of only 6%.
9th most common cancer in the US , but 4th in terms of cancer deaths.
74% of patients die within the first year after diagnosis.
Common age >60 years, median age is 72 years.
Incidence is about 8 to 9 cases per 1,00,000 population.
Incidence is lowest in India and parts of middle east 8.1 and 7.0 per 1,00,000 in men and women respectively
Risk Factors
EnvironmentalGenetic
Risk Factors – Definitive Association
Smoking1 – 3 times riskDirectly proportional to the quantity
and duration of smoking (i.e. pack year)
Inherited susceptibility

Environmental risk Factors – Suggested Association
Diabetes Mellitus Chronic Pancreatitis Obesity Diet
Diabetes Mellitus
Glucose intolerance in 80% of patients , 50% overt diabetes.
Two fold increase in chance of Ca pancreas in patients with pre existing diabetes.
The new onset of diabetes - may be an early manifestation of occult pancreatic cancer.
Chronic Pancreatitis
Patients with chronic pancreatitis especially familial have up to a 20-fold increase in risk for pancreatic cancer.
Obesity
obese patients may be up to three times more likely to develop pancreatic cancer than non-obese individuals.
Diet Increased risk with increased total calorie intake, and
increased intake of carbohydrate, cholesterol, meat, salt, dehydrated food, fried food, refined sugar, and nitrosamines.
Fat, beta carotene, and coffee are of unproven risk.
Consumption of dietary fibre, vitamin C, fruits, vegetables, and unprepared food may have a protective effect, as may pressure and microwave cooking.

Environmental risk Factors – Unproven Association
Alcohol Coffee Radiation
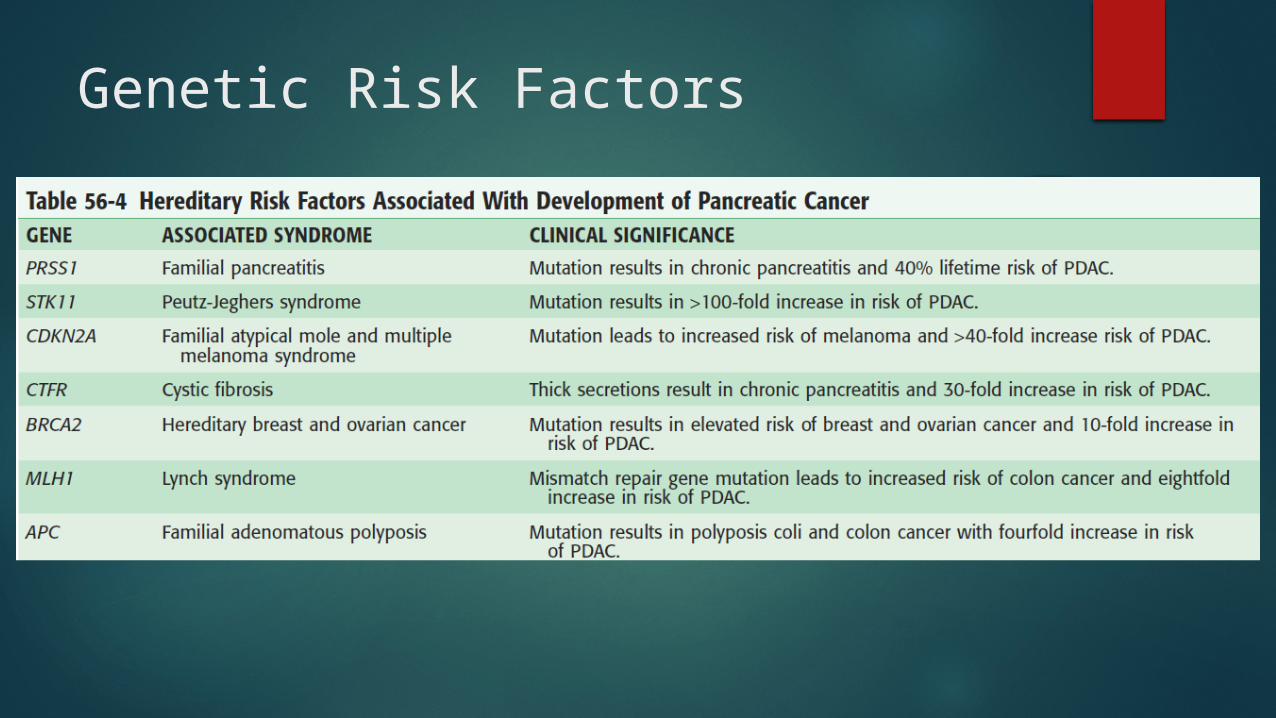
Genetic Risk Factors
Pathology
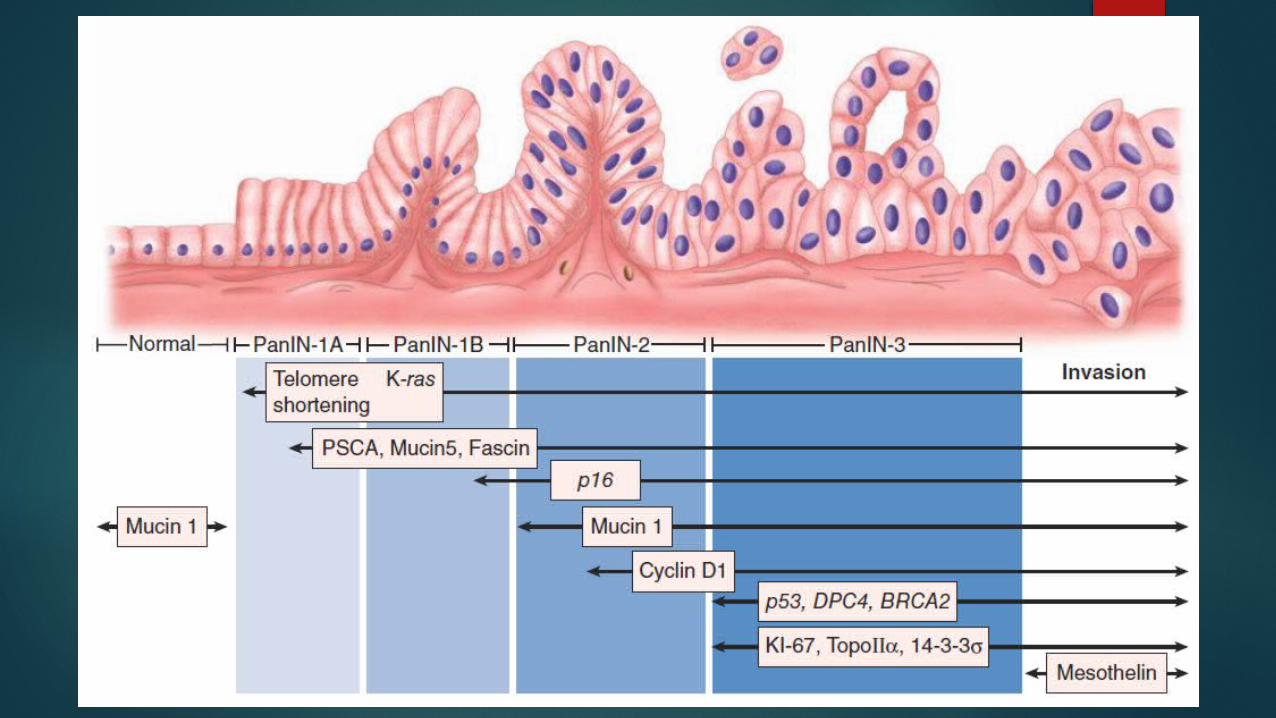
Pancreatic cancer probably arises through a stepwise progression of cellular changes.
From Pancreatic intra epithelial neoplasia to invasive adeno carcinoma.
75% are ductal adenocarcinoma Uncommon varieties include Adeno squamous and
Acinar cell carcinoma.
Adenosquamous carcinoma - has both glandular and squamous differentiation. The biologic behaviour similar to typical ductal adenocarcinoma.
Acinar cell carcinoma - presents as a large tumour, often 10 cm in diameter or more, the prognosis of patients with these tumours may be better than with ductal cancer.
Pancreatic Intraepithelial Neoplasia (PanIN)
Pre cursor lesions for invasive carcinoma Three stages of pancreatic intraepithelial neoplasia
have been defined. From PanIN 1 – PanIN 3 With progressive cellular atypia and architectural
disarray.
Location of the tumour
About two-thirds of pancreatic adenocarcinomas arise within the head or uncinate process of the pancreas
15% are in the body 10% in the tail, remaining tumours demonstrating diffuse
involvement of the gland.
Clinical features
The symptoms at presentation are related to the location of the tumour.
Lesions occurring in or near the bile duct presents with obstructive jaundice,
body or tail with pain. Weight loss, loss of appetite, generalised
weakness - non specific
Tumours in the pancreatic body and tail are generally larger at the time of diagnosis, and therefore, less commonly resectable.
Tumours in the head of the pancreas are typically diagnosed earlier because they cause obstructive jaundice.
Presentation - History
The classic constellation of symptoms in 66%-75% of cases. JaundicePruritusAcholic stoolsTea-coloured urine.
Pain, left sided tumour present with pain cachexia
Pancreatitis in the absence of cholelithiasis and ethanol abuse.
New onset diabetes mellitus and pancreatic exocrine insufficiency are rare as initial presentation.
Non specific symptoms include nausea anorexia, weight loss.
Symptoms of GOO – Indicate locally advanced disease.
Clinical signs
Anaemia scleral icterus, hepatomegaly, a palpable gallbladder (Courvoisier’s sign), and skin excoriation from pruritus and
scratching.
Signs of advanced disease
Cachexia palpable nodules in the liver palpable metastatic disease in the left supra-
clavicular fossa (Virchow’s node), palpable metastatic disease in the
periumbilical area (Sister Mary Joseph’s node) Pelvic metastatic disease palpable anteriorly
on rectal examination (Blumer’s shelf).
Biochemical investigations
LFTElevated bilirubin, alkaline phosphatase and
GGTOnly mild to moderate elevations in liver
transaminases
CA 19-9
Used in cases where diagnosis is in doubt. Elevated in 75% of patients with pancreas
cancer. also elevated in benign conditions of the
pancreas, liver, and bile ducts. To measure response to therapy or for
screening for recurrence Fallacy – can not be used in cases of jaundice.
Imaging
ultrasonography Computed tomography (CT), Endoscopic ultrasound (EUS) Magnetic resonance imaging (MRI) with or without
magnetic resonance cholangio-pancreatography (MRCP)
Endoscopic retrograde cholangio-pancreatography (ERCP)
Positron emission Tomography (PET)
Ultrasonography
Initial investigation The sensitivity is low, and the absence of a
pancreatic mass by RUQ ultrasonography does not rule out ca pancreas
sensitive for the detection of gallstones, the presence of a dilated biliary tree
Presence of acute cholecystitis
Dilation of the biliary tree, and pericholecystic fluid,
Also pick up hepatic metastases, pancreatic masses, peripancreatic and hilar lymphadenopathy, and ascites.

Longitudinal view reveals a mildly dilated common bile duct that terminates in a pancreatic head
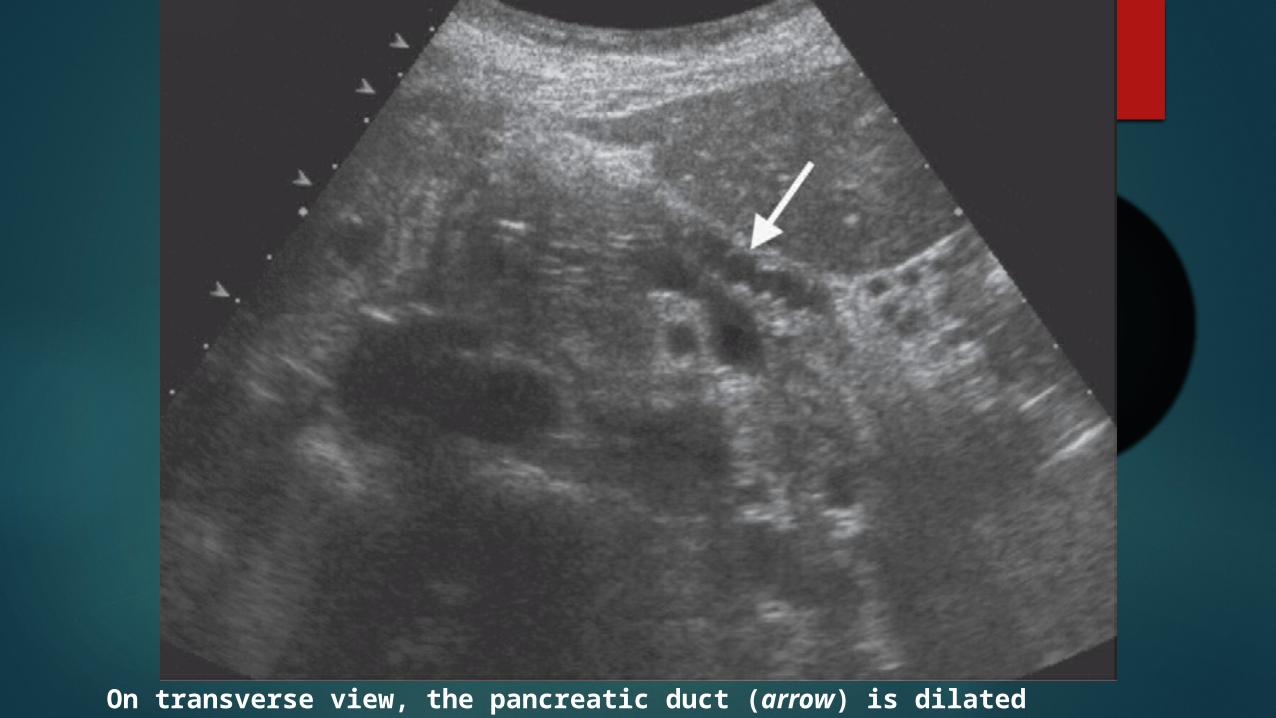
On transverse view, the pancreatic duct (arrow) is dilated
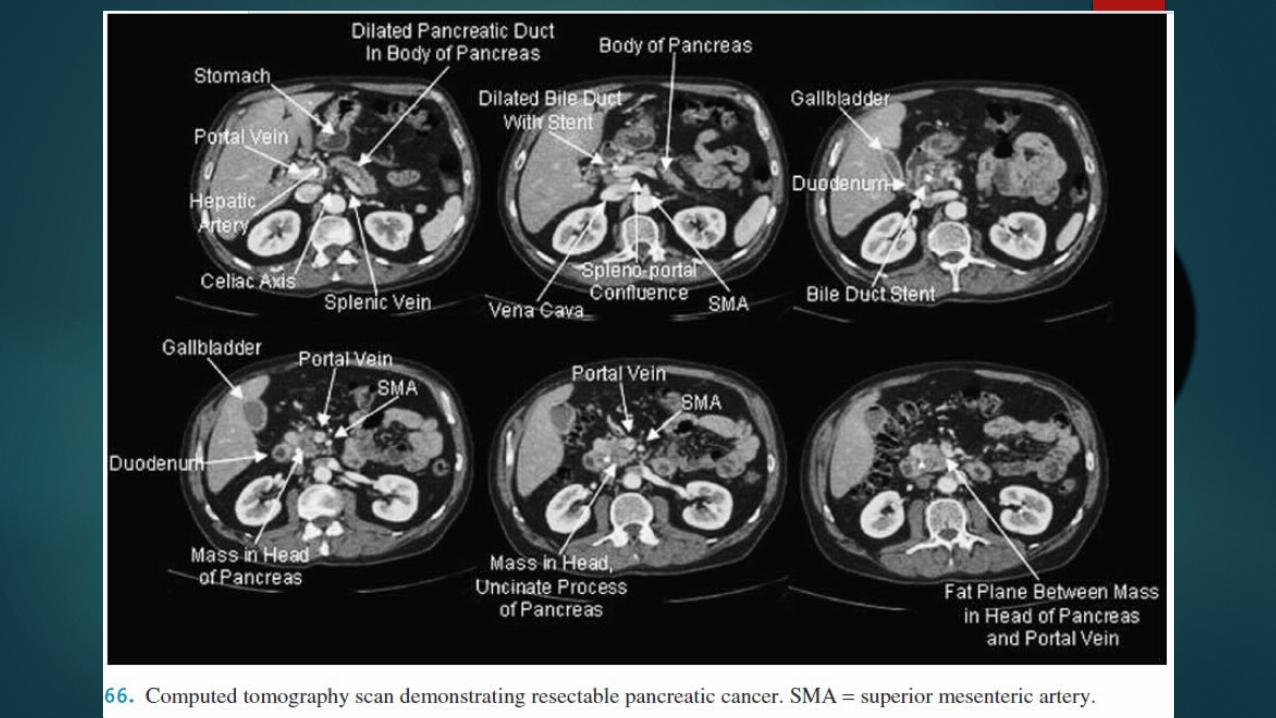
CT Scan for pancreas
Multi-detector spiral CT and is the single most useful diagnostic and staging modality.
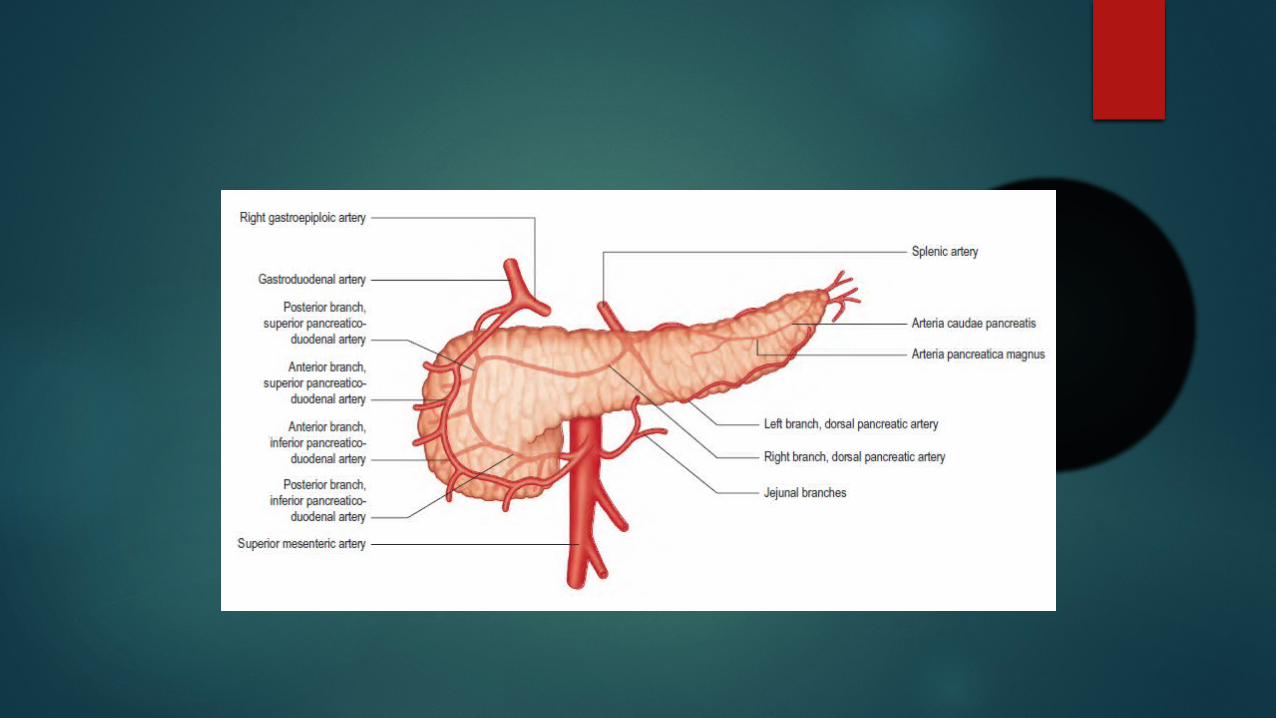
It gives information about adjacent vascular structures such as the portal, superior mesenteric, and splenic veins, as well as the superior mesenteric artery (SMA) and celiac axis.
Phases of an pancreatic protocol CT scan
Non Contrast CT Early arterial phase (15-20 s after injection of
contrast) Late arterial phase (35-40 s) Hepatic or portal venous phase (50-60s) Nephrogenic Phase (100 s) Delayed phase (6-10 minutes)
The non contrast phase - pancreatic calcifications, for localization of the precise levels the post contrast study.
The early arterial phase permits evaluation of pancreatic vasculature without interference from venous opacification.
The late arterial phase - distinguish pancreatic neoplasms from adjacent normal pancreatic tissue, to evaluate hyper-vascular liver metastases (neuroendocrine tumors of the pancreas).
The 4th phase portal venous phase - for hypo-vascular liver metastases
Unresectability in CT
Unresectability is defined on multiphase CT by involvement of
1. ≥ 180 degrees of the celiac axis2. hepatic or superior mesenteric artery, enlarged lymph
nodes outside the boundaries of resection3. ascites, and distant metastases. Invasion of the superior mesenteric vein or portal vein
is not in itself a contraindication to resection as long as the veins are patent. Resection of vein with reconstruction is possible.
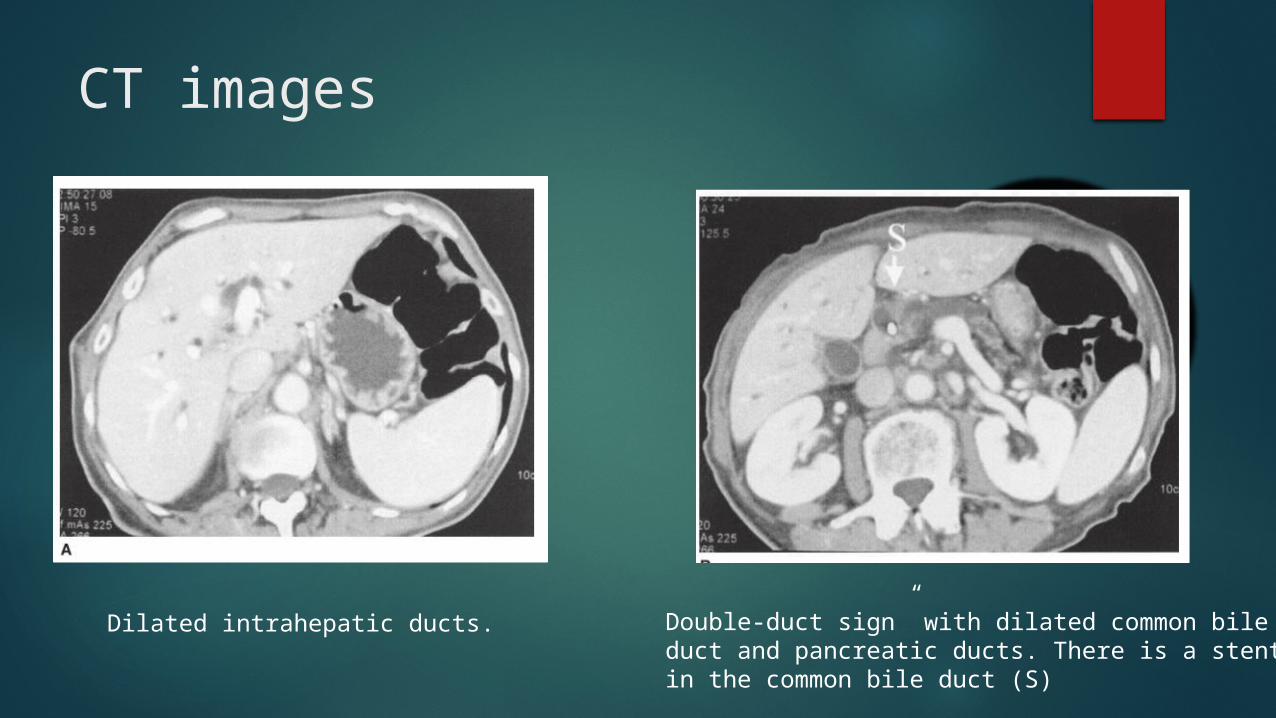
CT images
Dilated intrahepatic ducts. Double-duct sign” with dilated common bile duct and pancreatic ducts. There is a stent in the common bile duct (S)
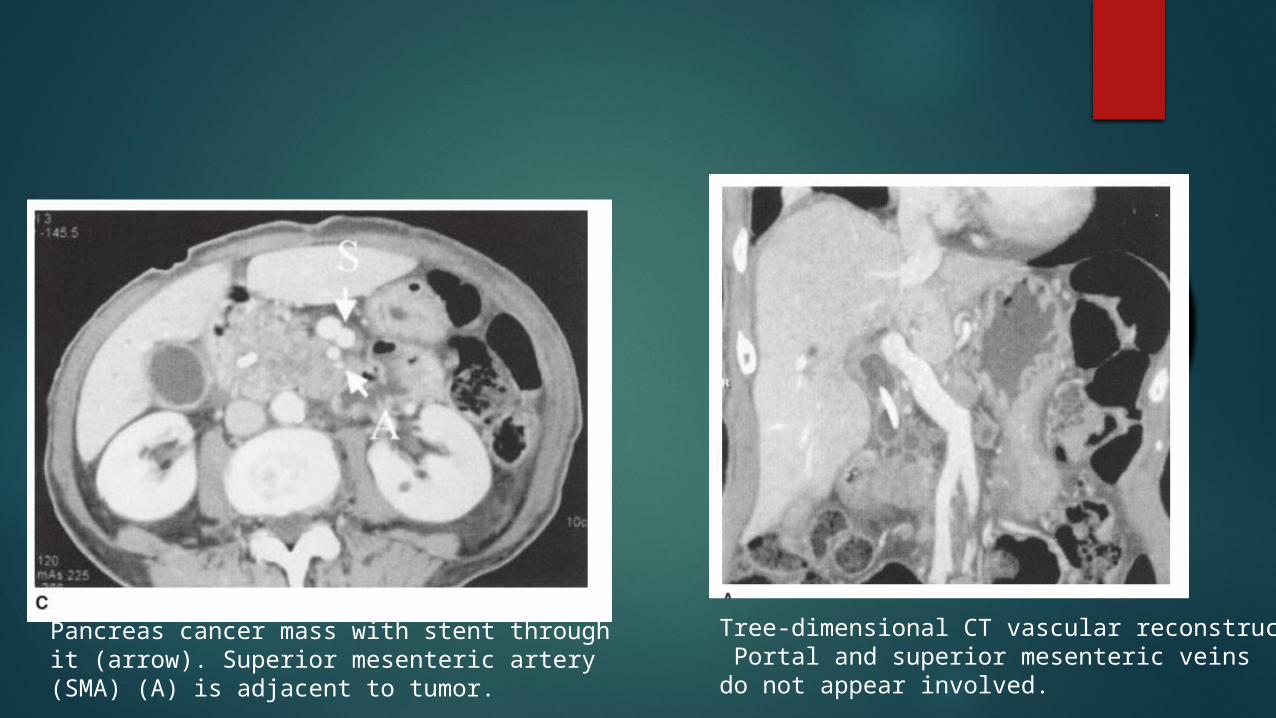
Pancreas cancer mass with stent through it (arrow). Superior mesenteric artery (SMA) (A) is adjacent to tumor.
Tree-dimensional CT vascular reconstruction Portal and superior mesenteric veinsdo not appear involved.
ENDOSCOPIC ULTRASOUND ( EUS )Sensitivity ranges from 69 to 94%.
Superior than CT for detecting the lesions smaller than 2cm
It is superior to CT for the venous invasion but it is less useful in determination of arterial involvement.
Another advantage of EUS is the ability to obtain tissue for biopsy via FNA.
With EUS, the issue of needle-tract tumour seeding is minimized, as the FNA is generally performed through a segment of duodenal or stomach wall that will be removed as part of a resection,
The duodenum, ampulla, head of the pancreas, and uncinated process of the pancreas are accessible with an ultrasound probe positioned in the duodenum.
The body and tail of the pancreas are accessible with an ultrasound probe positioned in the stomach.

Images eus
Endoscopic ultrasound (EUS) image with linear array echoendoscope demonstrating a mass in the head of the pancreas with no vascular invasion of the superior mesenteric artery (SMA), superior mesenteric vein (SMV), or portal vein (PORTAL).
MRI and MRCP
MRI, MRA, and MRCP can be performed in a single setting.
has the potential to provide information about tumour size and extent, biliary and pancreatic ductal anatomy, and vascular involvement through a single, non-invasive procedure.
Motion artefact, lack of bowel opacification, compromised resolution, and patient discomfort from the longer scanning times are disadvantages.
MRI Vs CT
There is no significant diagnostic advantage of MRI over contrast- enhanced CT
MRI is better at characterizing cystic lesions of the pancreas
has the capability to evaluate the bile ducts both above and below a stricture, and can also identify intrahepatic mass lesions
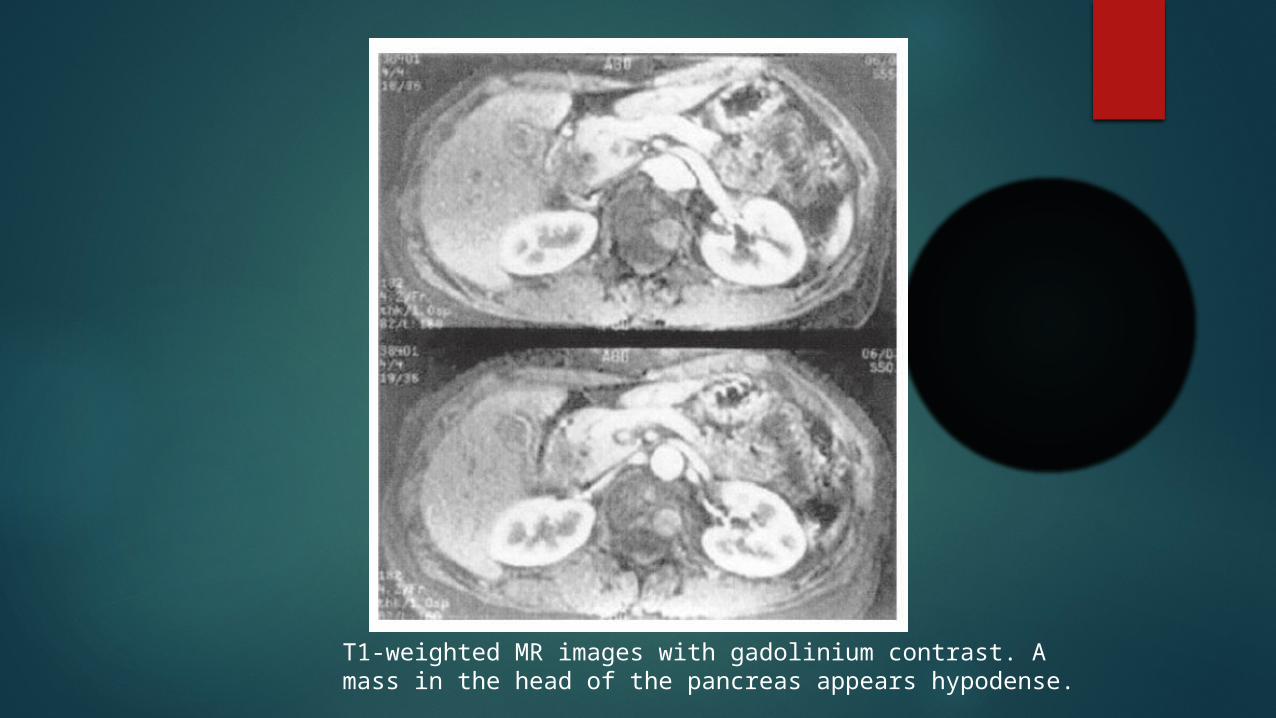
T1-weighted MR images with gadolinium contrast. A mass in the head of the pancreas appears hypodense.
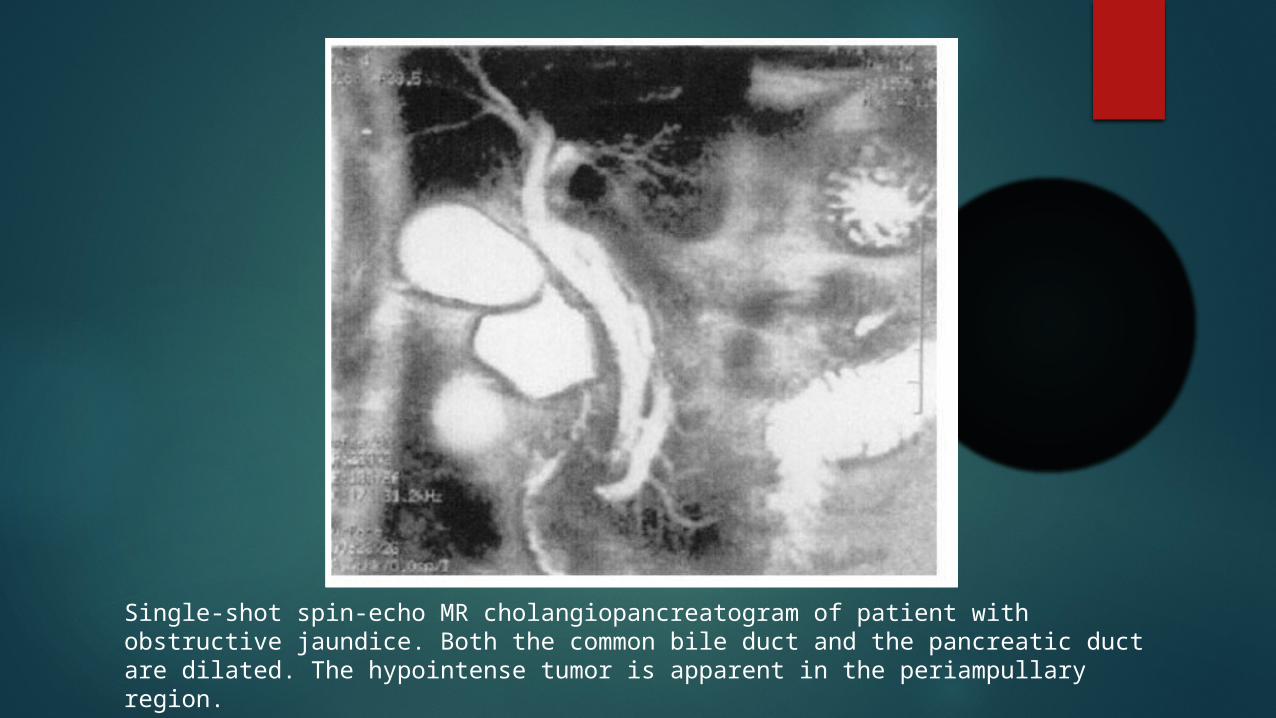
Single-shot spin-echo MR cholangiopancreatogram of patient with obstructive jaundice. Both the common bile duct and the pancreatic duct are dilated. The hypointense tumor is apparent in the periampullary region.
ERCP
ERCP may be of benefit in patients with biliary obstruction and cholangitis - endoscopic stent can be placed for decompression.
With current capabilities of CT and MRI, ERCP is rarely necessary.
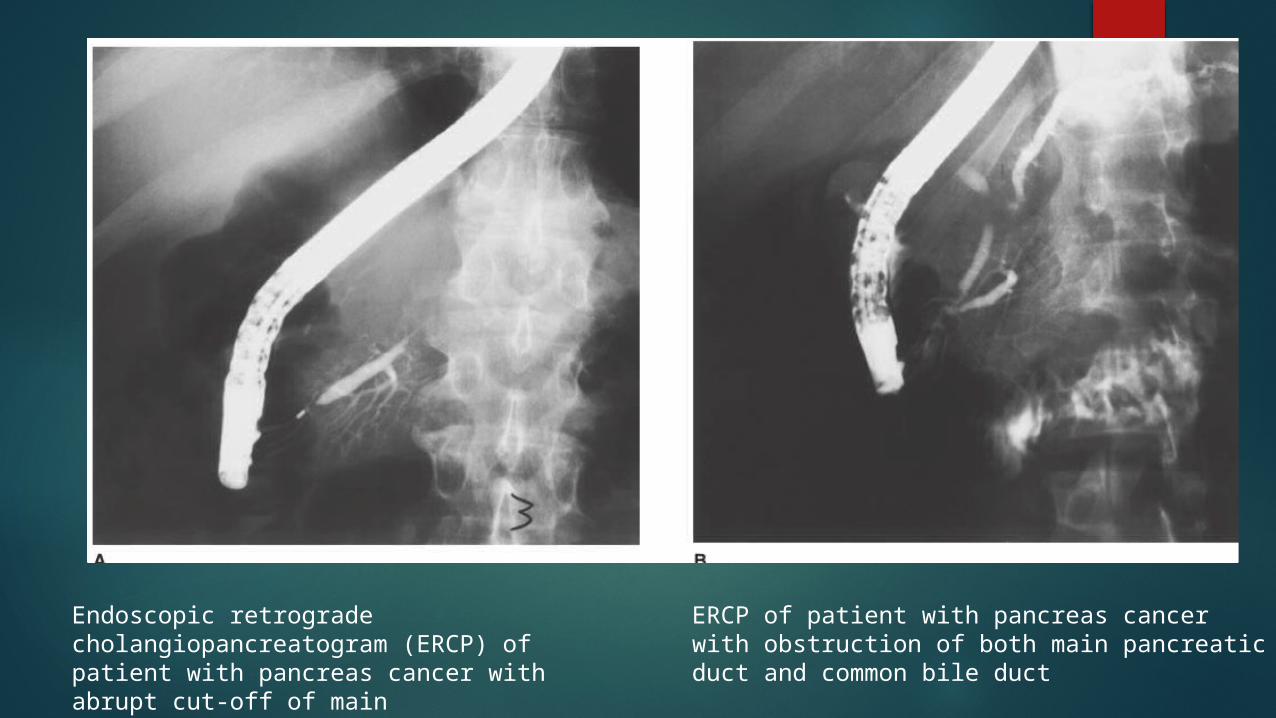
Endoscopic retrograde cholangiopancreatogram (ERCP) of patient with pancreas cancer with abrupt cut-off of mainpancreatic duct secondary to tumor.
ERCP of patient with pancreas cancer with obstruction of both main pancreatic duct and common bile duct
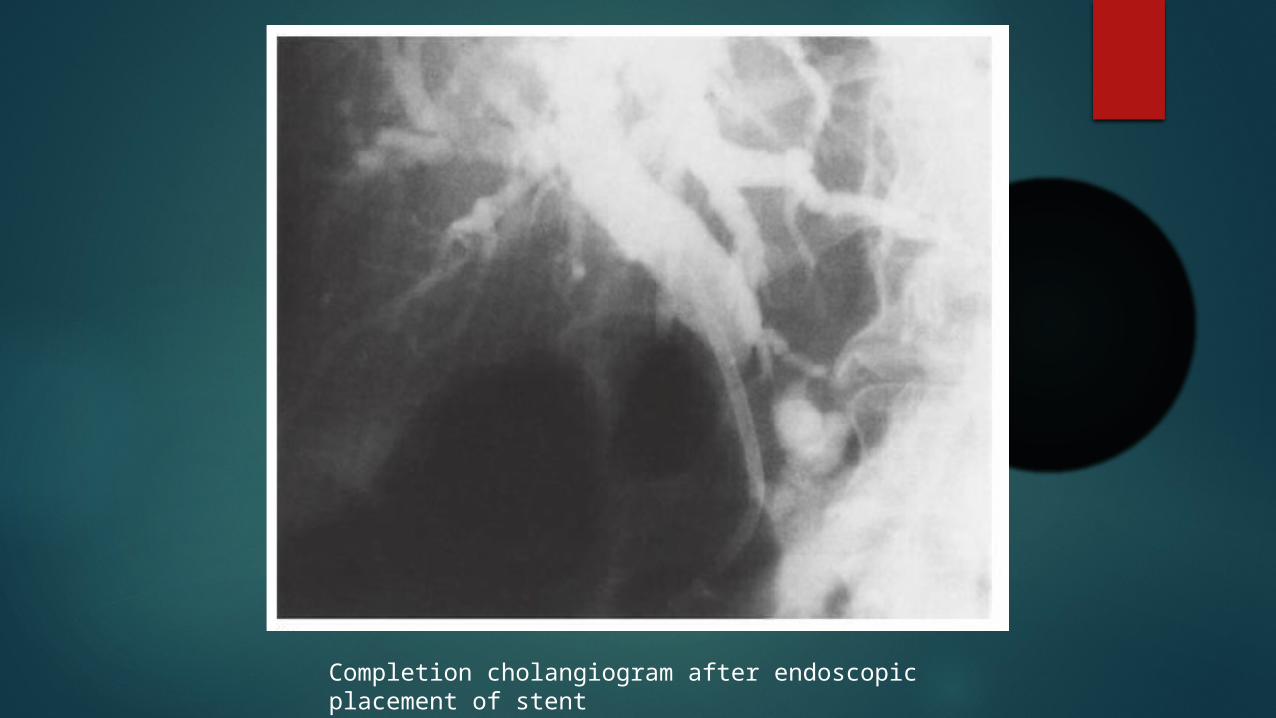
Completion cholangiogram after endoscopic placement of stent
Indications for pre operative decompression of biliary system.
Cachexic patient for nutritional improvement. In patients with cholangitis If your plan is non operative management.
Tissue diagnosis
A tissue diagnosis of adenocarcinoma is not required prior to an attempt at a curative resection.
Fibrosis in pancreatic cancer- may miss the malignant glands, so sensitivity is less.
Does not change treatment decision in a planned curative surgery.
FNA is required if
1. Patients undergoing neoadjuvant therapy.2. If the diagnosis of carcinoma is uncertain.3. In suspected neuroendocrine cancers, lymphomas, cystic lesions, FNA result may alter the treatment.
Staging
CT, EUS, MRI to detect local disease. Chest x-ray with SOS CT chest, Staging laparoscopy- varies between
institutions.

AJCC Staging
Staging of Pancreatic Cancer
TX: Primary tumor cannot be assessed T0: No evidence of primary tumor Tis: Carcinoma in situ T1: Limited to pancreas, ≤ 2 cm in greatest dimension T2: Limited to the pancreas, >2 cm in greatest dimension T3: Extends beyond the pancreas, without involving of
the celiac axis or the superior mesenteric artery T4: Involves the celiac axis or the superior mesenteric
artery (unresectable).
Regional lymph nodes - NX: Regional lymph nodes cannot be assessed - N0: No regional lymph node metastasis - N1: Regional lymph node metastasis present
Distant metastasis - MX: Distant metastasis cannot be assessed - M0: No distant metastasis - M1: Distant metastasis

Stage grouping
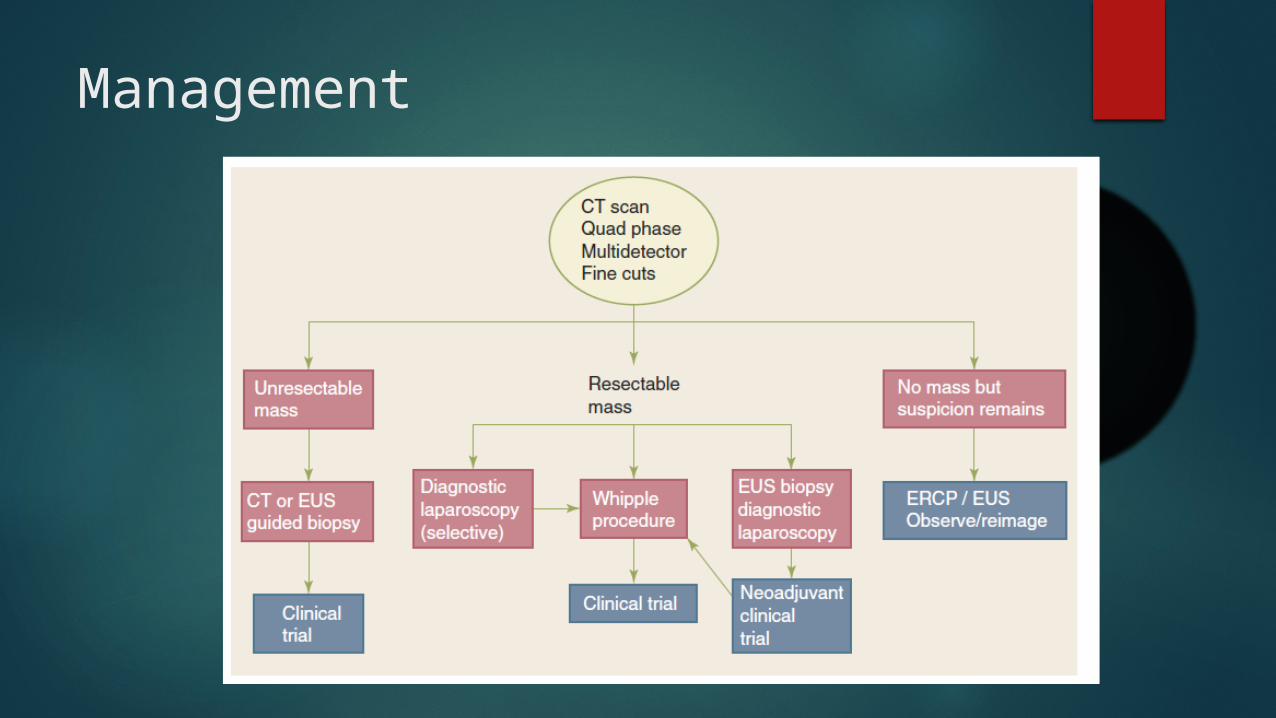
Management
Methods of surgical resection
For lesions involving HOP – Pancreatoduodenectomy
For body and tail tumors - Distal pancreatectomy with splenectomy
Pancreatoduodenectomy
midline incision from xiphoid to umbilicus or through a bilateral subcostal incision.
The initial portion of the procedure is an assessment of resectability
Assessment phase
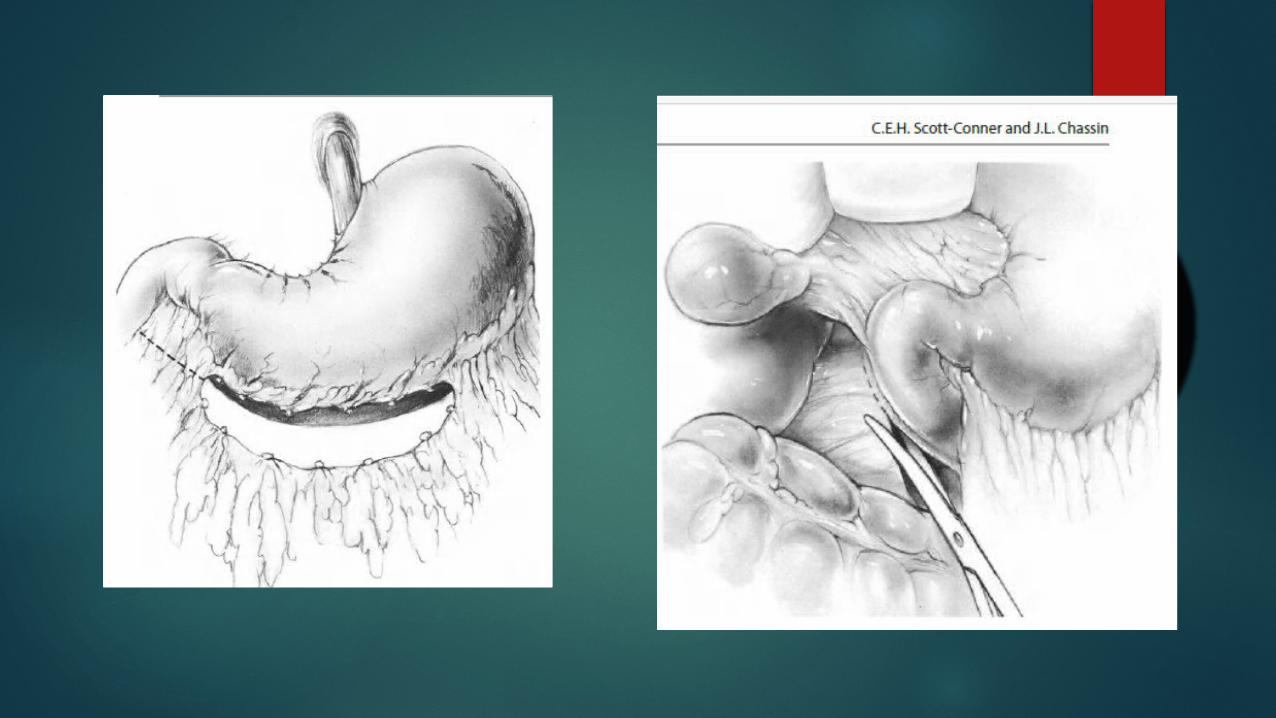
Assess The liver visceral and parietal peritoneal surfaces The gastrohepatic omentum is opened, The celiac axis area is examined for enlarged lymph
nodes. The base of the transverse mesocolon to the right
of the middle colic vessels is examined for tumor involvement.
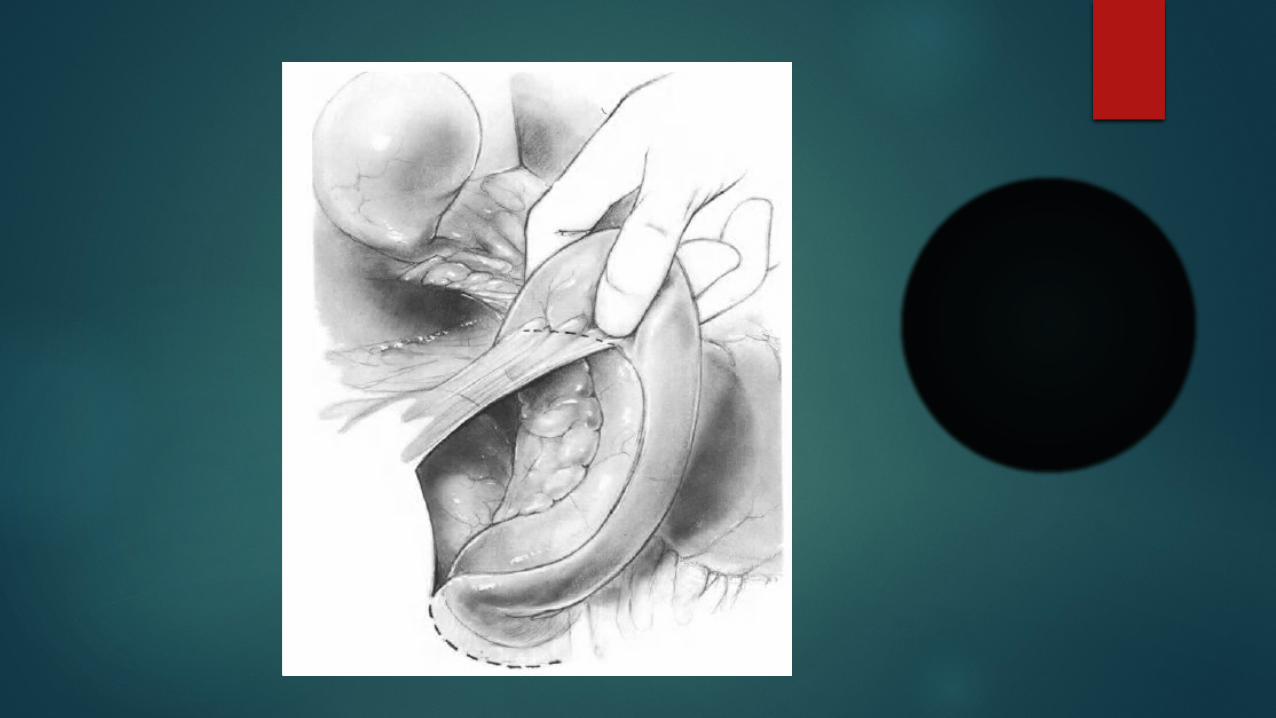
Extensive Kochers manoeuvre and head of pancreas reflected medially to examine SMA and SMV.
SMV is identified and traced up towards the inferior border of the neck of pancreas.
The gastroepiploic vein and artery are ligated to prevent any traction injury.
Assess for aberrant right hepatic artery origin from SMA. (20% of cases)
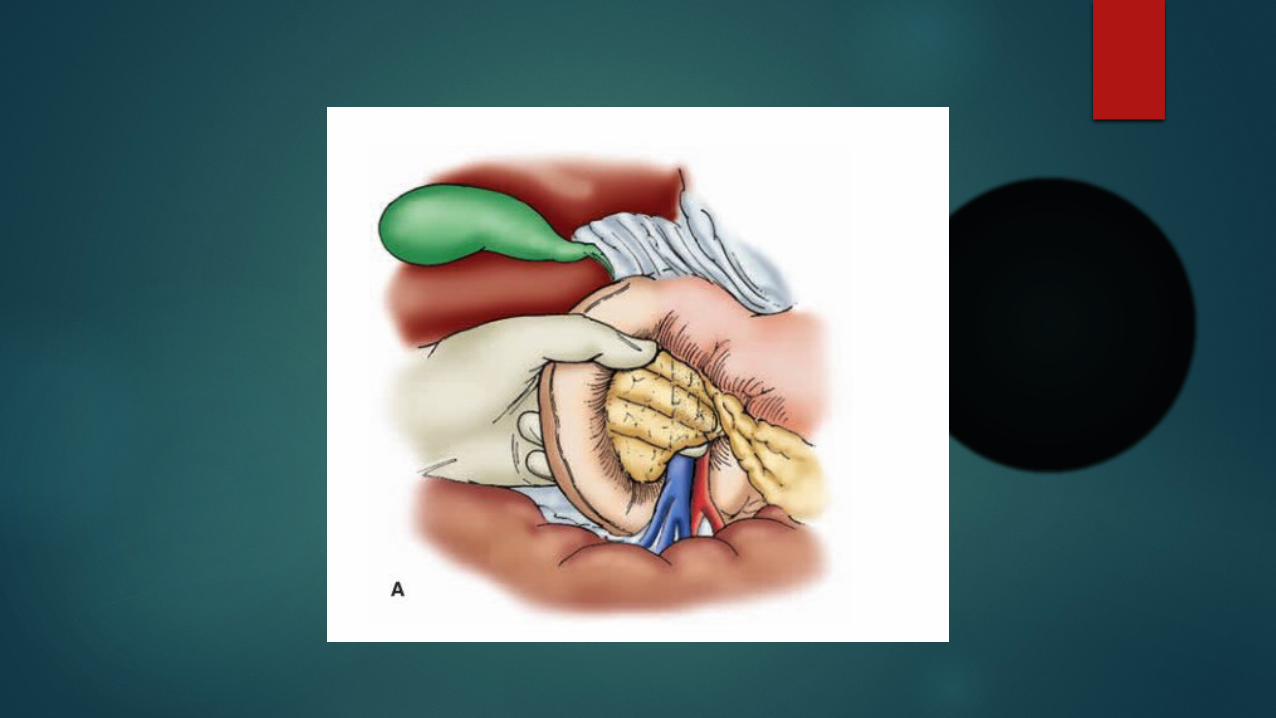
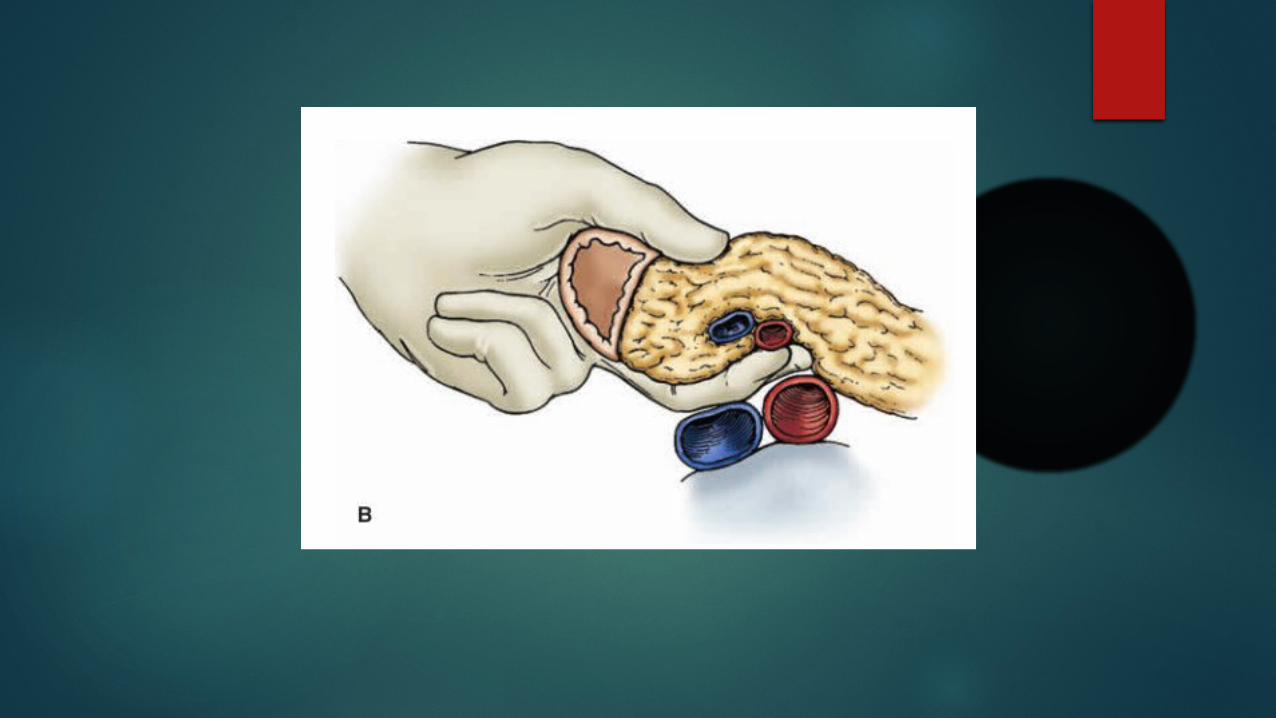
Aberrant SMA can be identified intraoperatively by palpation on the back side of the hepatoduodenal ligament.
Mobilise Gall bladder and the porta hepatis is examined.

Resection Phase
The easiest and safest portions of the resection should be performed first and the more difficult portions later.
The distal common hepatic duct is divided close to the level of the cystic duct entry site.
The bile duct is retracted caudally,
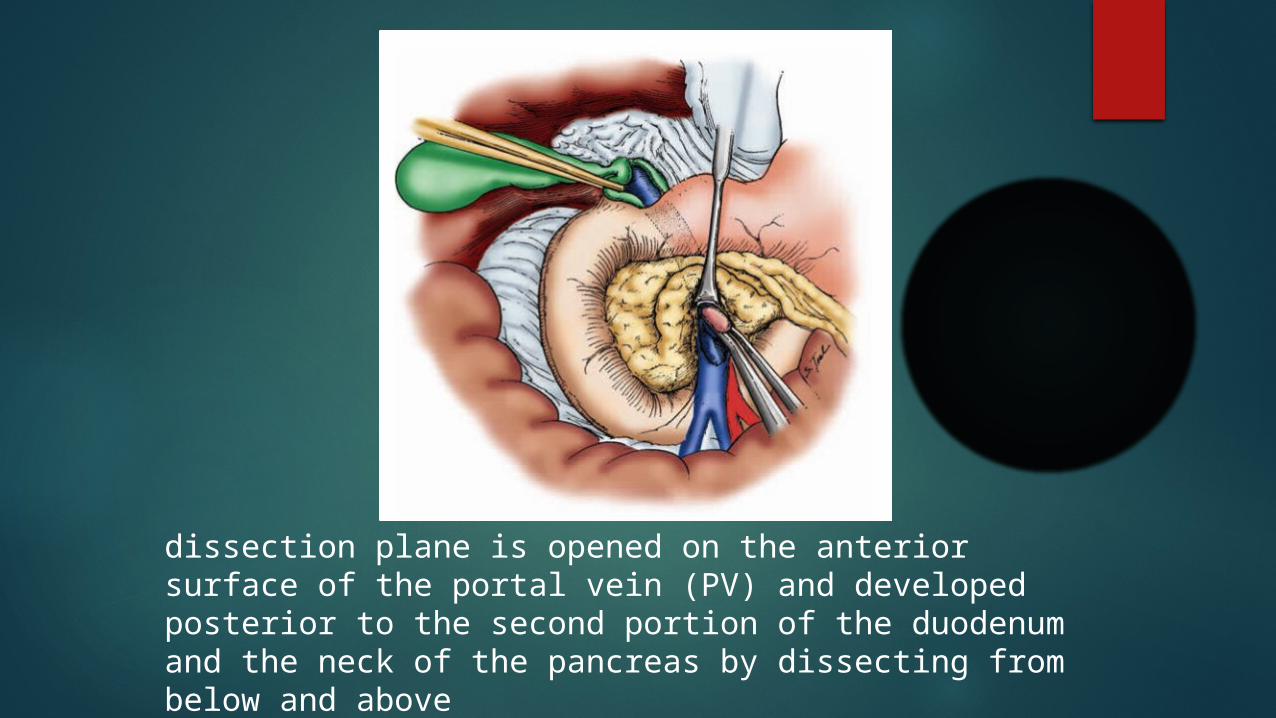
dissection plane is opened on the anterior surface of the portal vein (PV) and developed posterior to the second portion of the duodenum and the neck of the pancreas by dissecting from below and above
Check for origin of right hepatic artery from gastro duodenal artery, and preserve it.
The gastroduodenal artery is next identified and clamped atraumatically before ligation (Test clamping).
This manoeuvre confirms that the hepatic artery is not being supplied solely retrograde through the SMA collaterals (in the setting of celiac axis stenosis or occlusion)
Next is division of stomach
classic Whipple procedure, a 30–40% distal gastrectomy is performed by dividing the right gastric and right gastroepiploic arteries. The antrectomy is then completed using a linear stapling device.
pylorus-preserving pancreaticoduodenectomy, the proximal GI tract is divided 2–3 cm distal to the pylorus with a linear stapling device. The right gastric artery can often be spared.
Advantages of pyloric preservation
Prevention of reflux of pancreaticobiliary secretions into the stomach,
decreased incidence of marginal ulceration, normal gastric acid secretion and hormone release,
and improved gastric function. Patients with pylorus-preserving resections have
appeared to regain weight better than historic controls. it is controversial whether there is any significant
improvement in long-term quality of life with pyloric preservation.
Jejunum is divided distally at a point of mobile jejunum, typically 20 cm distal to the ligament of Treitz. The mesenteric vessels to this initial portion of the jejunum are carefully divided over clamps and tied to avoid bleeding.
Next is resection of pancreas
The SMV is identified running anterior to the third portion of the duodenum. In this location, the SMV is identified by dissecting the fatty areolar tissue surrounding the veins.
Division of the gastroepiploic vein emptying into the anterior surface of the SMV allows continued cephalad dissection.
The plane anterior to the SMV is developed under direct vision.
With the exception of the gastroepiploic vein, there are usually no veins entering the anterior surface of the SMV in this location.
Care should be taken to avoid inadvertent injury to the splenic vein as it joins the SMV posterior to the neck of the pancreas.
Penrose drain is looped under the neck of the pancreas.
Stay sutures are placed superiorly and inferiorly on the pancreatic remnant to reduce bleeding from the segmental pancreatic arteries running in those locations.
The pancreatic neck is then divided after confirming a free plane anterior to the portal and superior mesenteric veins.
The site of the main pancreatic duct should be noted so it can be incorporated into the subsequent reconstruction.
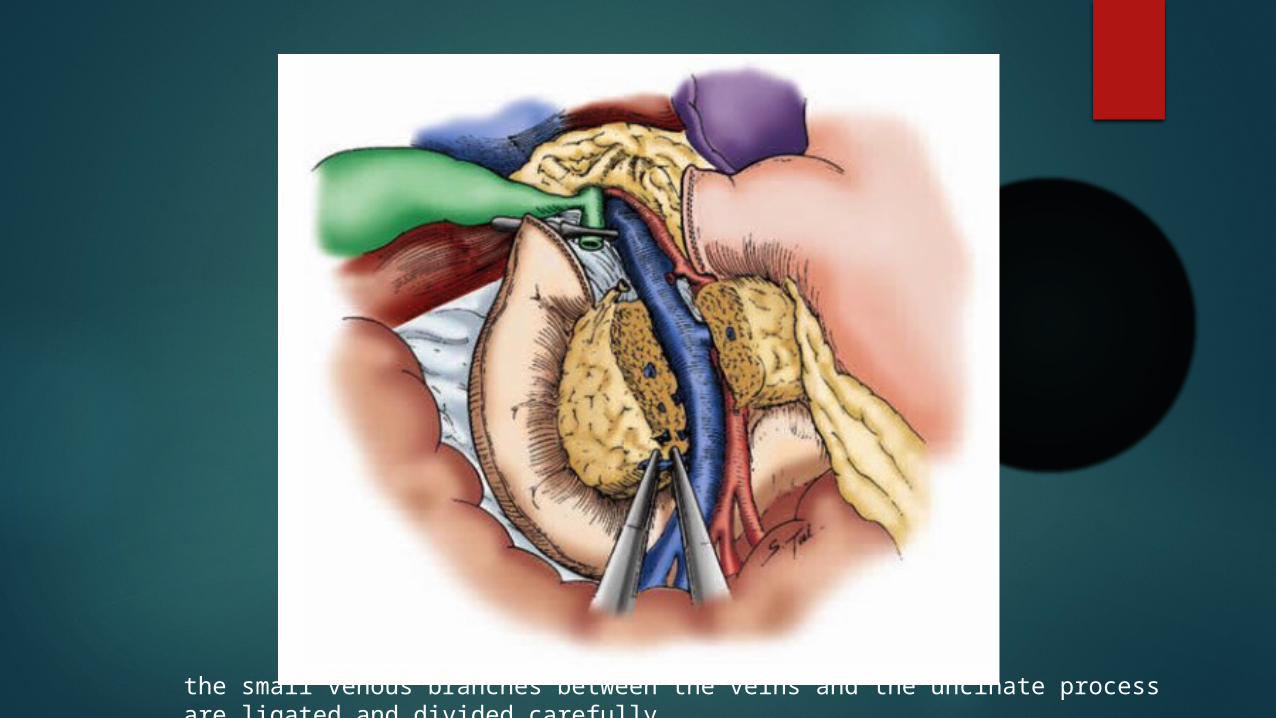
the small venous branches between the veins and the uncinate process are ligated and divided carefully.
With these areas dissected, the specimen is removed and the pancreatic neck margin, uncinate margin, and common hepatic duct margins are marked for the pathologists.
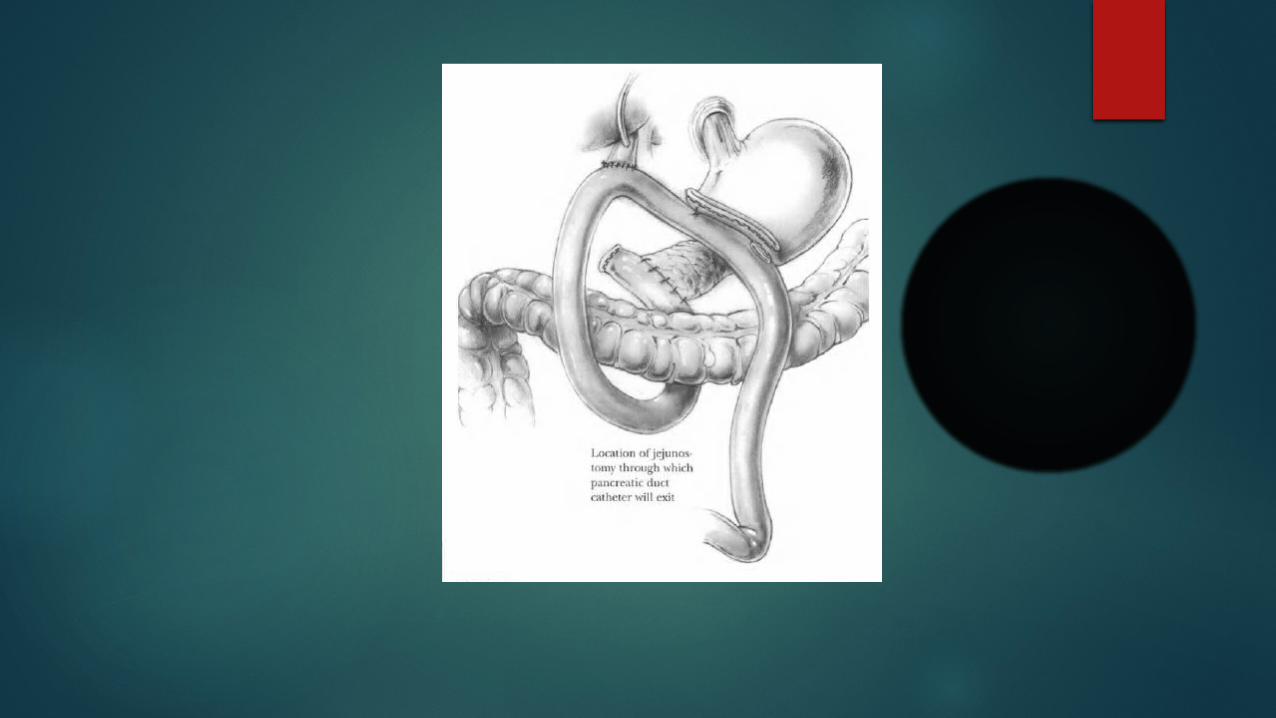
Reconstruction phase
The reconstruction involves anastomoses of the pancreas first, then the bile duct, and, finally, the duodenum or stomach.
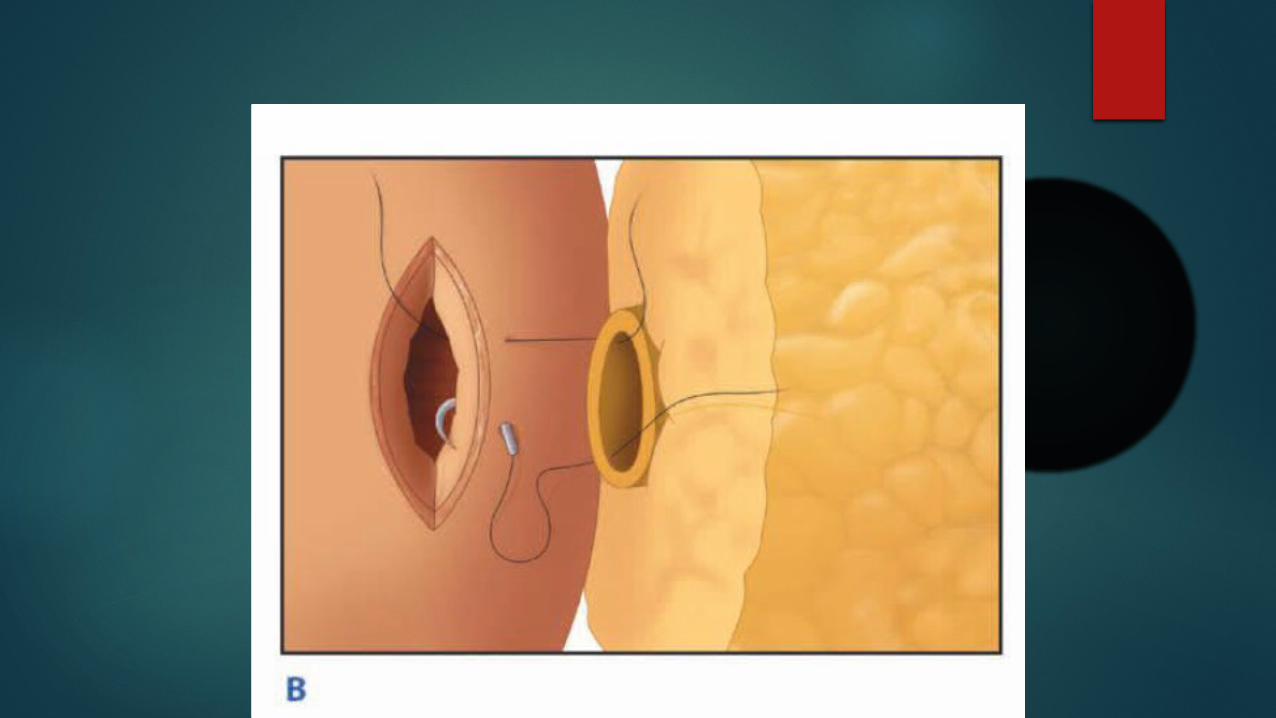
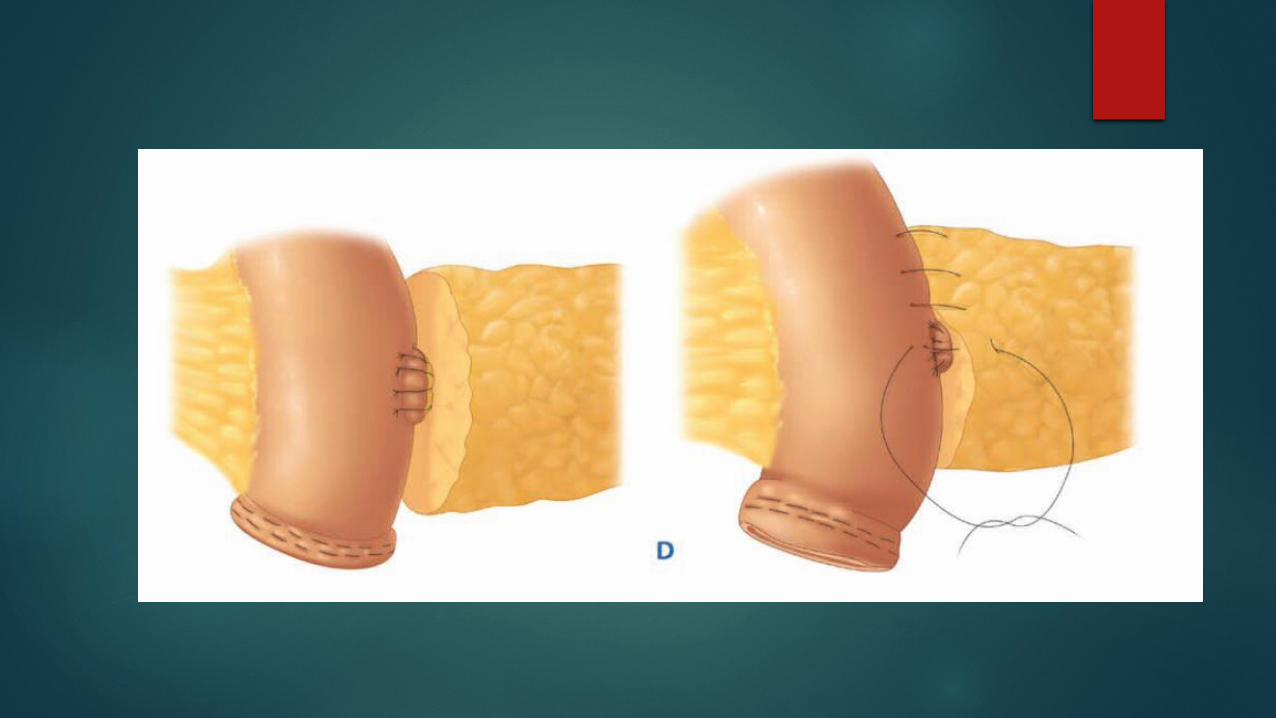
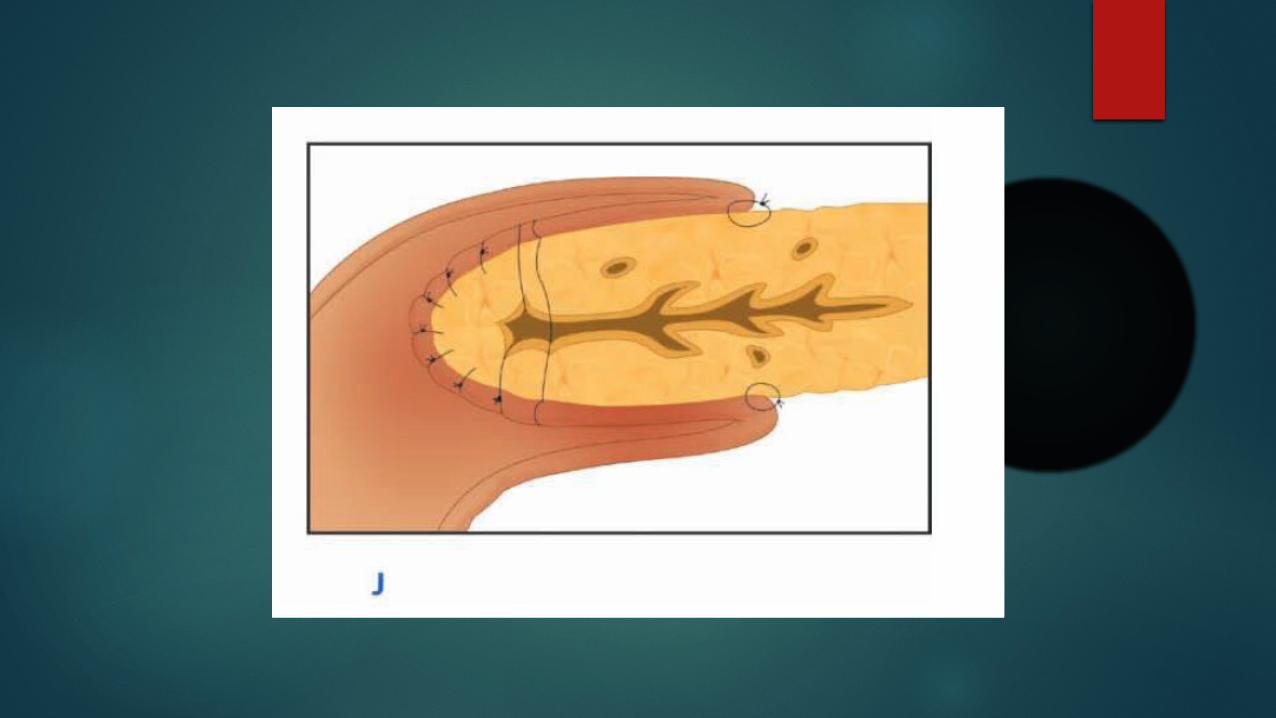
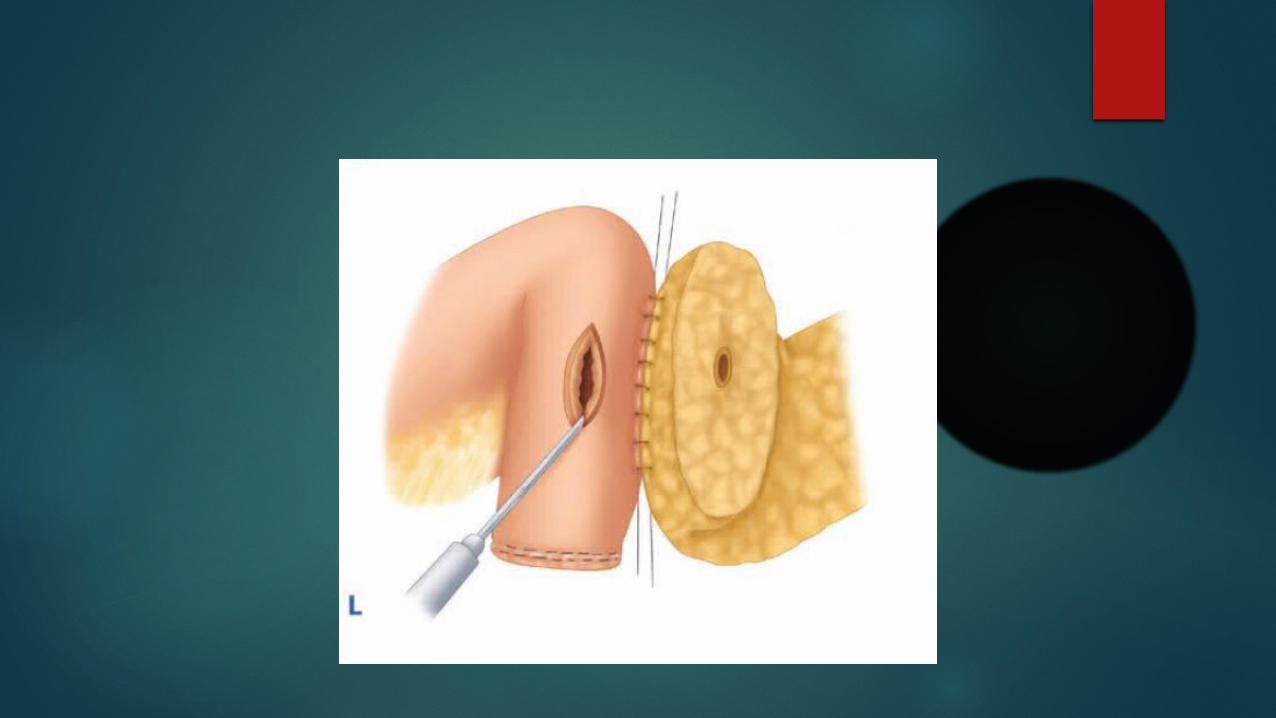
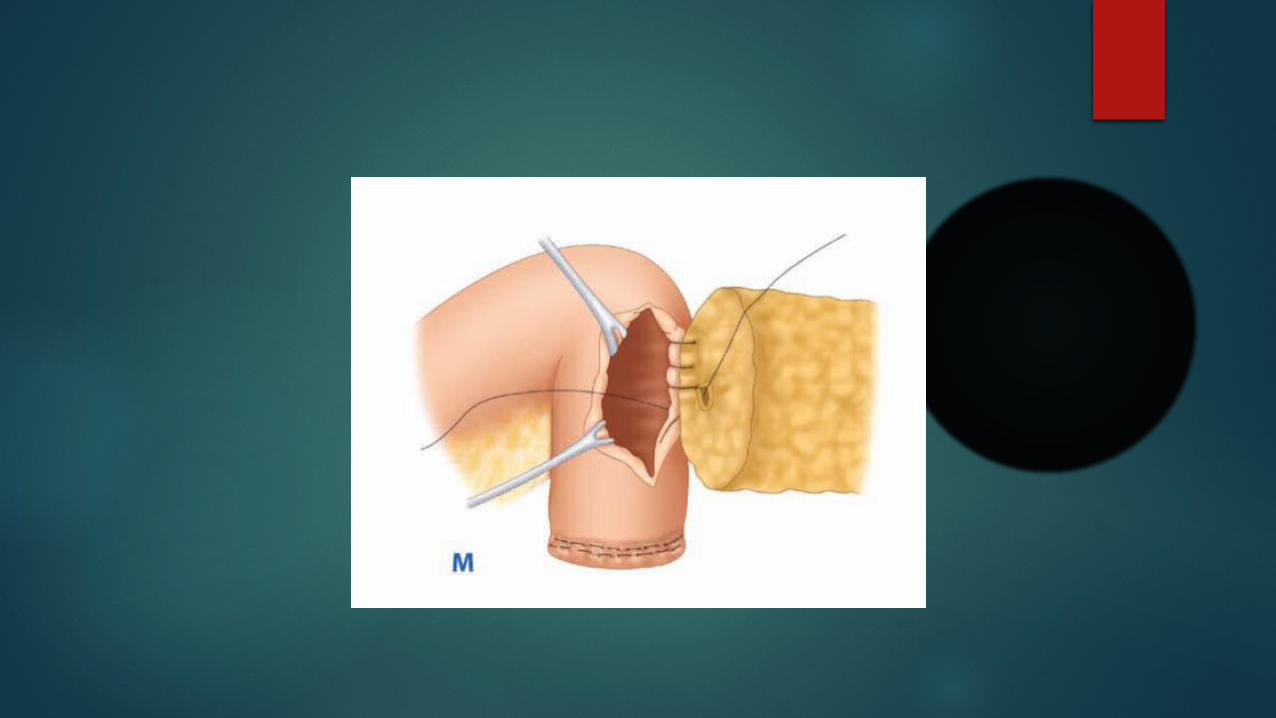
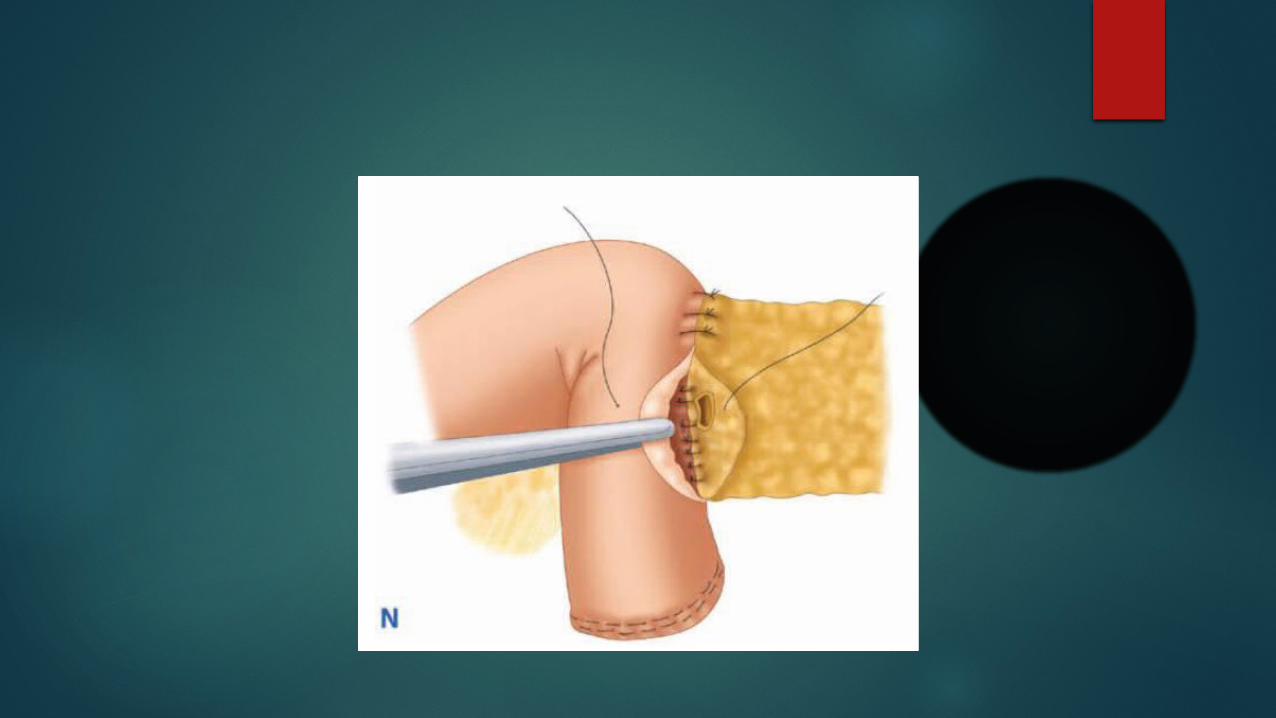
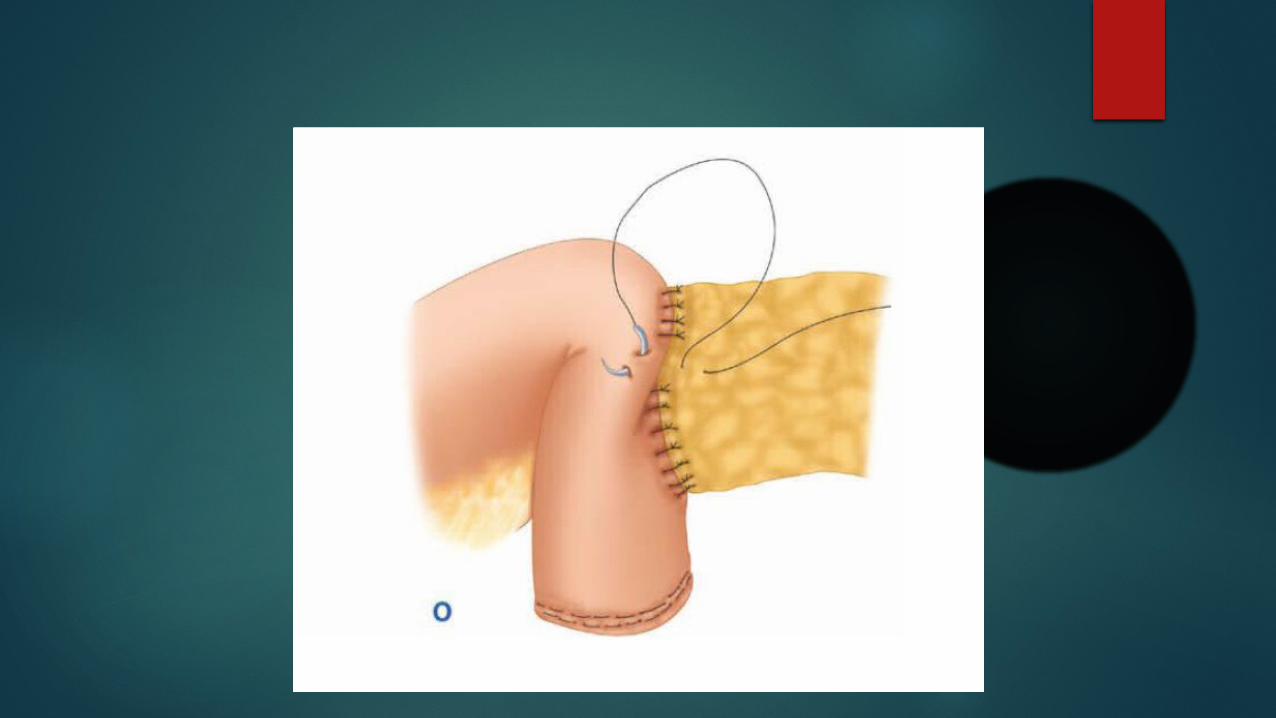
Pancreaticojejunostomy
Techniques for the pancreaticojejunostomy include end-to-side or end-to-end and duct-to-mucosa sutures or invagination.
proximal jejunal stump is brought through a defect in the mesocolon to the right of the middle colic artery.

End-to-side duct to mucosa

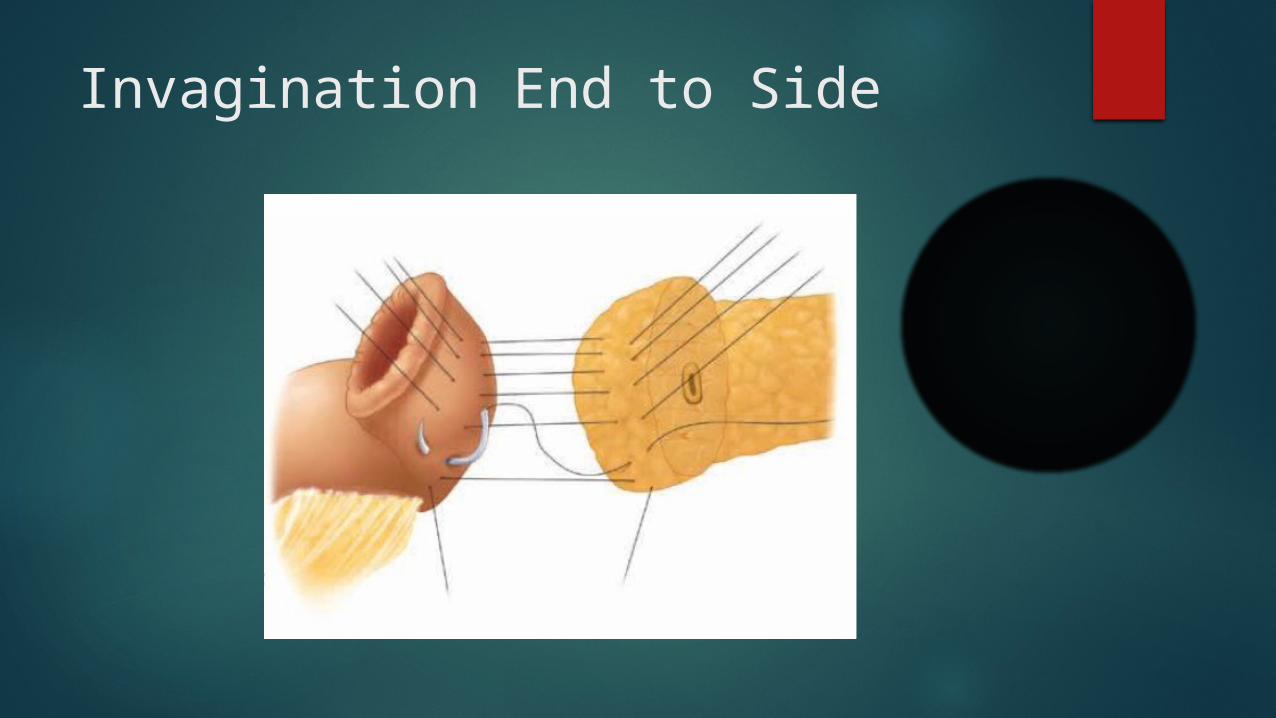
Invagination End to Side
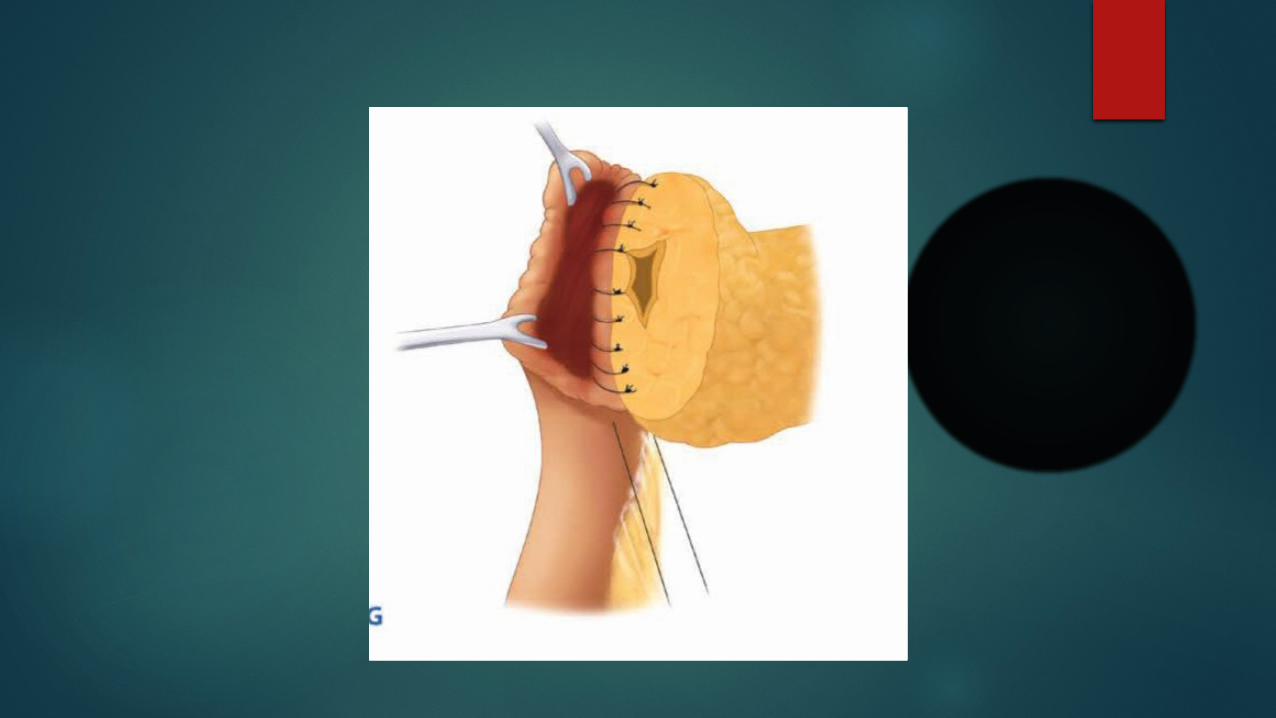
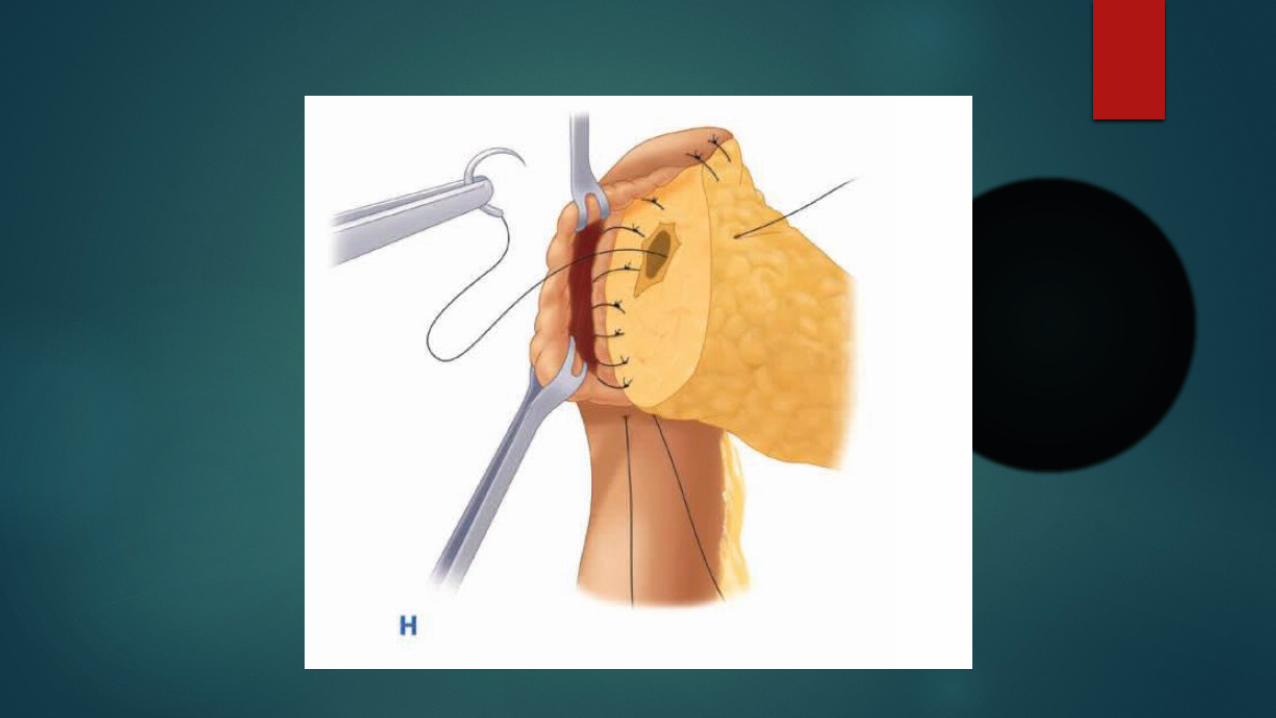
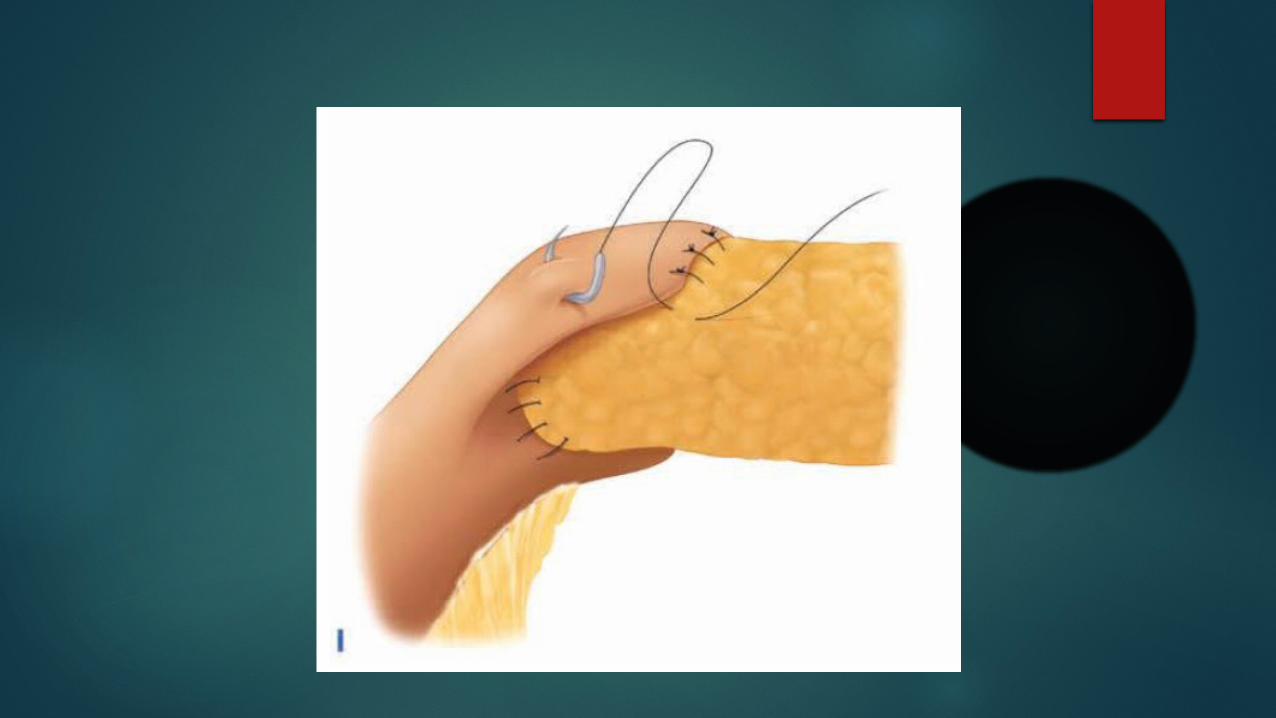

Invagination end to side
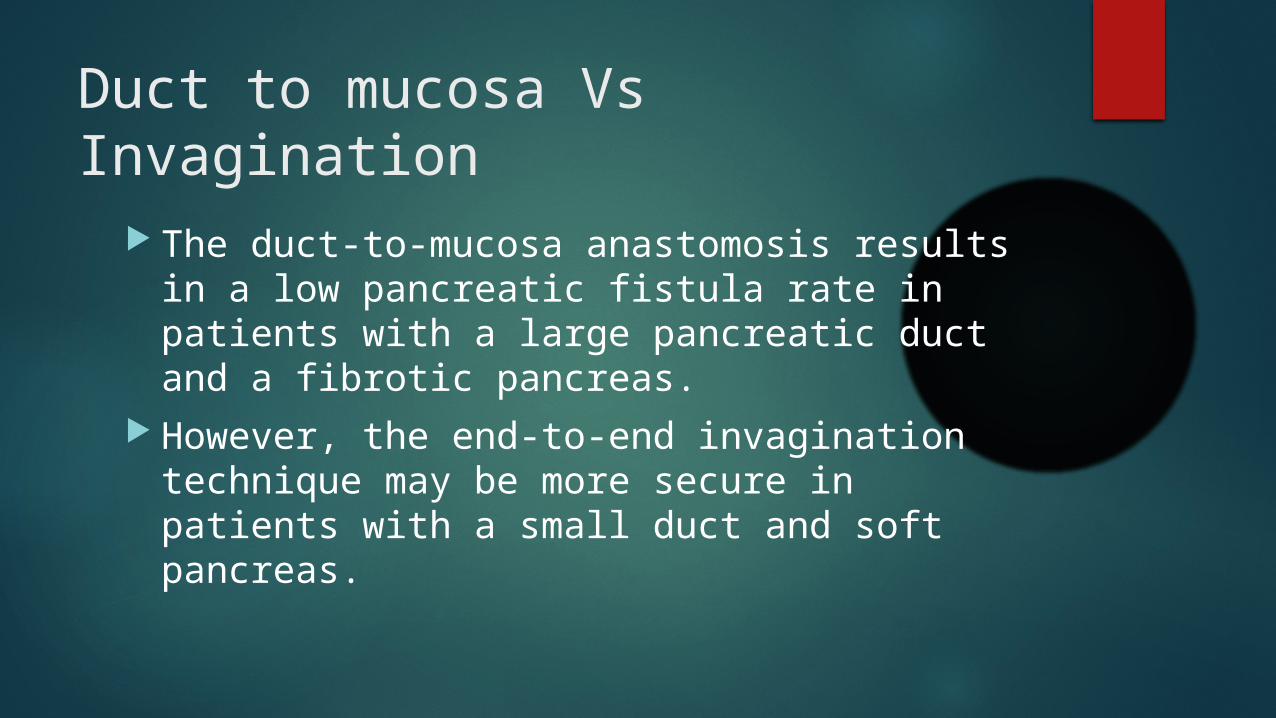
Duct to mucosa Vs Invagination
The duct-to-mucosa anastomosis results in a low pancreatic fistula rate in patients with a large pancreatic duct and a fibrotic pancreas.
However, the end-to-end invagination technique may be more secure in patients with a small duct and soft pancreas.
Pancreatic leak is 10% despite the used technique.
Usually, a pure pancreatic leak is controlled by the drains and will eventually seal spontaneously.
Combined pancreatic and biliary leaks - bile will activate the pancreatic enzymes.
Total pancreatectomy - pancreatic leaks are eliminated, but major morbidity from brittle diabetes and exocrine insufficiency outweigh any theoretical benefit.
In a prospective randomized trial comparing pancreaticogastrostomy to pancreaticojejunostomy, there was no difference in the leak or fistula rate between the two types of anastomoses.
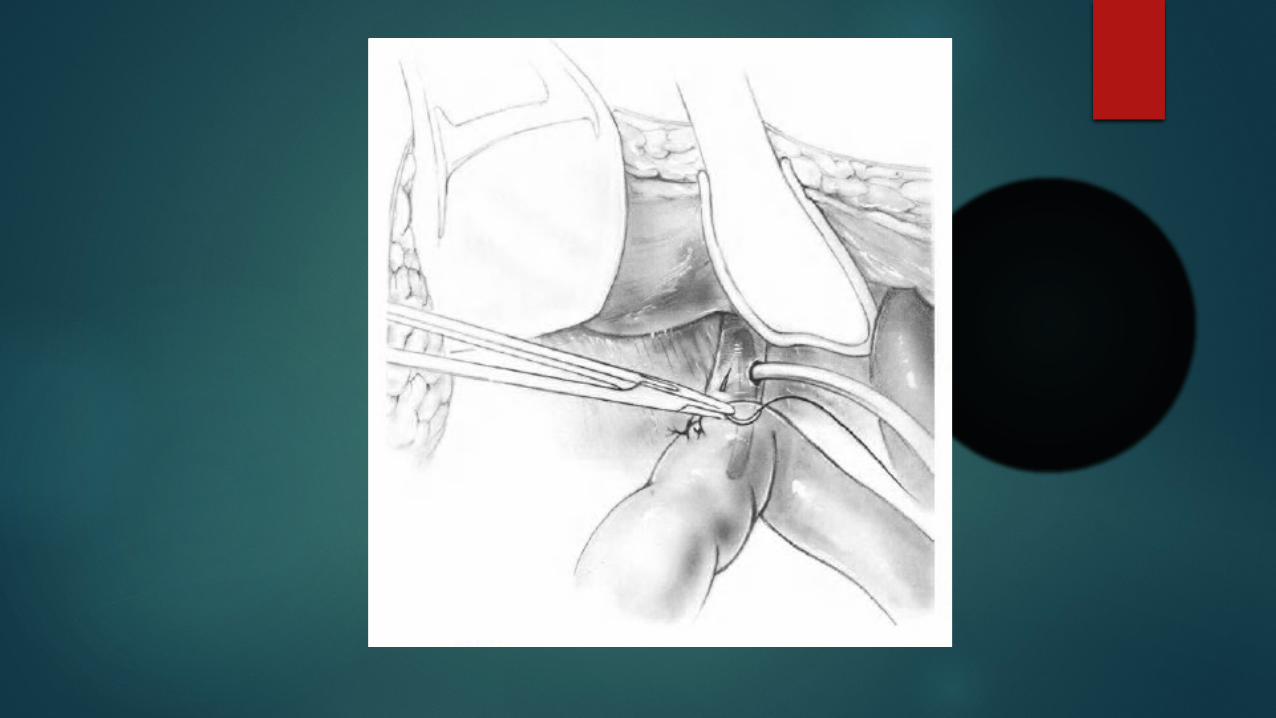
Biliary anastomosis
The biliary anastomosis is typically performed with an end-to-side hepaticojejunostomy distal to the pancreaticojejunostomy.
This anastomosis is performed with a single layer of interrupted absorbable sutures.
If the patient has a percutaneous biliary stent, this is left in place, traversing the anastomosis.

3rd anastomosis
Duodenojejunostomy in cases of pylorus preservation, or the Gastrojejunostomy.
This anastomosis is performed 10–15 cm downstream from the hepaticojejunostomy, proximal to the jejunum traversing the defect in the mesocolon.

Complications
Mortality of 5% in high volume centres. The most common causes of death are sepsis,
haemorrhage, and cardiovascular events. Postoperative complications - delayed gastric
emptying, pancreatic fistula, and haemorrhage.

PPPD - Video
Distal Pancreatectomy
Done for resectable body and tail tumors Combined with splenectomy
Why Splenectomy?
Ability to gain wider margins removal of lymph nodes and lymphatic tissues
at the tip of the pancreas and the hilum of the spleen,
avoidance of the tedious dissection of the splenic artery and vein away from the pancreatic parenchyma.
disadvantage is the increased incidence of post splenectomy sepsis
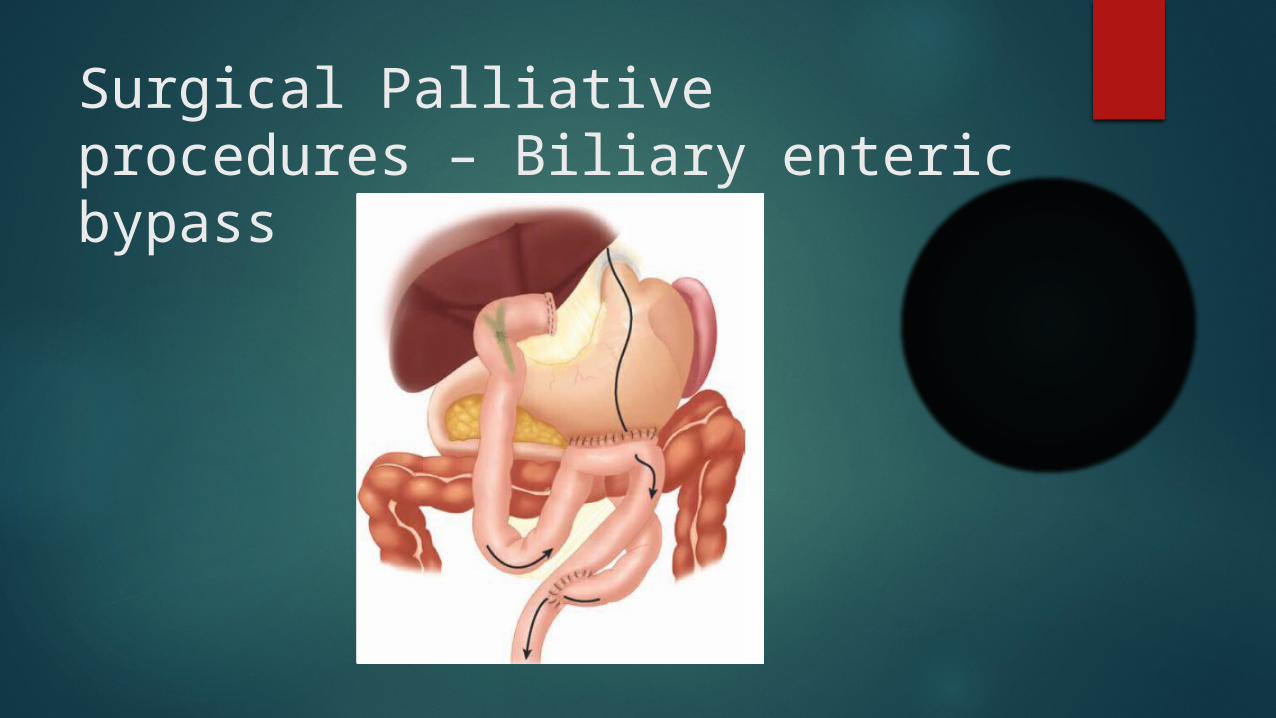
Surgical Palliative procedures – Biliary enteric bypass
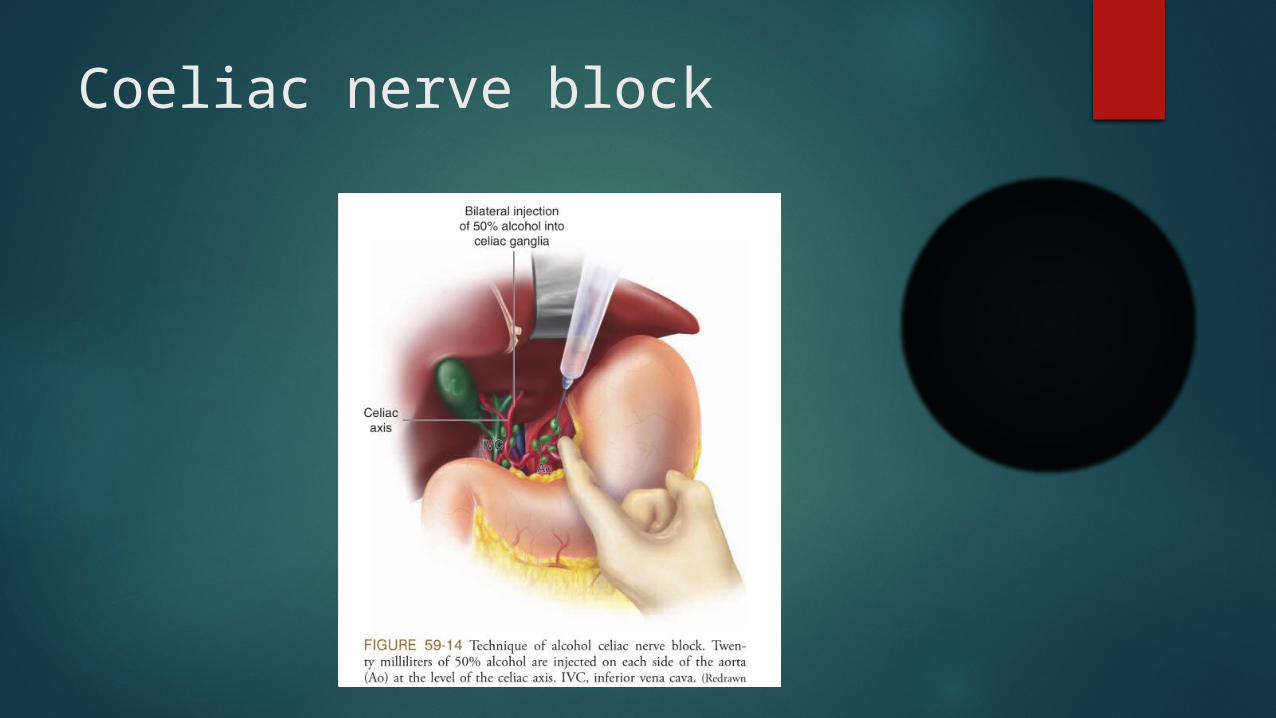
Coeliac nerve block
Non operative palliation
Nonoperative Palliation of Obstructive JaundicePer cutaneous drainage or endoscopic stenting
Nonoperative Palliation of Duodenal ObstructionSelf expanding gastro duodenal stenting
Chemotherapy
5 FU alone or combination with radiotherapy gemcitabine
ADJUVANT CHEMOTHERAPY
Current recommendation for adjuvant chemotherapy - gemcitabine
capecitabine, a prodrug for 5-FU. It is sequentially metabolized into active 5-FU by enzyme thymidine phosphorylase-highly expressed in the tumour.
This has four potential advantages: 1) systemic side effects are reduced,2) high concentrations are achieved in the
vicinity of the tumor,3) oral capecitabine has a pharmacokinetic
profile similar to that of a continuous systemic infusion 5-FU, and
4) Patients tolerate it better than 5-FU.
But clinical response in 24% and tumor response in 7% . Better responses when combined with gemcitabine.
INTRAOPERATIVE RADIOTHERAPY
EBRT on the pancreatic bed is limited – adjascent radiosensitive structures; so intraoperative radiotherapy (IORT) is useful.
Results unsatisfactory.
PALLIATIVE CHEMOTHERAPY
Gemcitabine is more beneficial than 5-FU when used as monotherapy in advanced pancreatic cancer.
Those receiving gemcitabine had a modest but significant increase in median survival (5.56 vs. 4.41 months; P = .0025) and improved clinical benefit (23.8% vs. 4.8%; P = .0022).
PALLIATIVE RADIOTHERAPY
Hyper fractionation and IMRT – Better tolerance
Cystic Neoplasms of Pancreas
Pathological classification of cystic neoplasms of the pancreas: The who international classification.
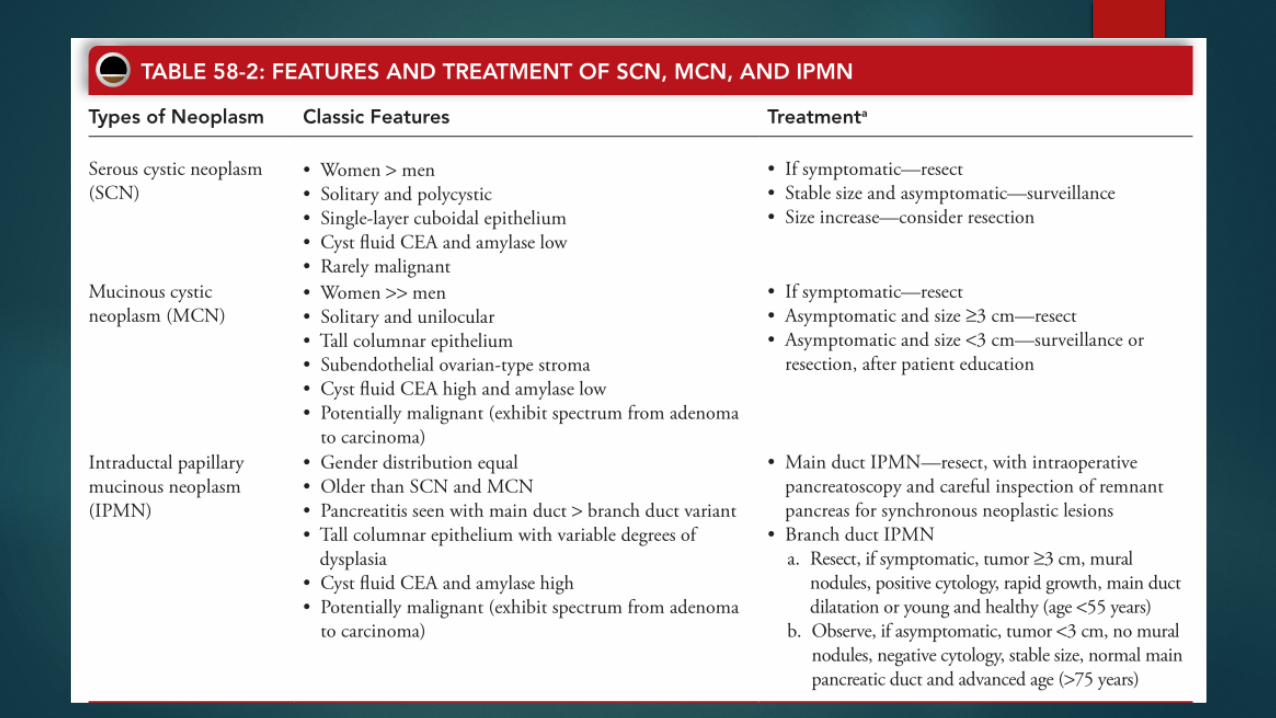
Serous cystic neoplasm (SCN)Mucinous cystic neoplasm (MCN) Intra-ductal papillary mucinous
neoplasm (IPMN)

Serous cystic neoplasm (SCN)
Microcystic adenomaOligocystic adenoma
Mucinous cystic neoplasm (MCN)
Mucinous cystadenomaMucinous cystic tumour–borderlineMucinous cystadenocarcinoma
Non-invasive (carcinoma in situ)Invasive
Intra-ductal papillary mucinous neoplasm (IPMN)
Adenoma/low-grade dysplasiaBorderline/moderate-grade dysplasiaCarcinoma in situ Invasive carcinoma
CYSTIC NEOPLASMS OF PANCREAS
They comprise approximately 10-15% of cystic lesions of pancreas and are heterogenous group of lesions that range from benign to malignant.
SEROUS CYSTIC NEOPLASM
First described by Comagno and Oertel in 1978 as microcystic and glycogen rich and they distinguished these lesions from mucinous cysts.
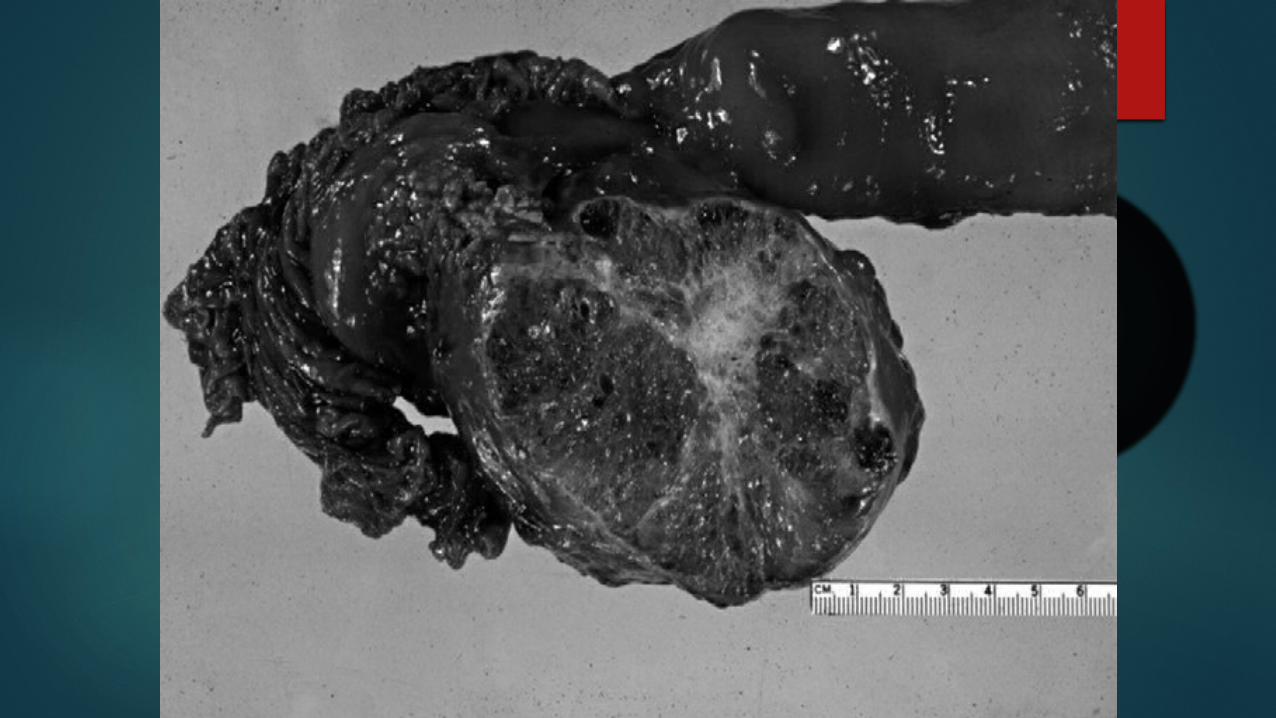
PATHOLOGY Cell of origin is centroacinar cell.
Soft mass which includes numerous small cysts filled with clear serous fluid arranged in a characteristic honeycomb-like pattern.
unique central calcification give rise to charecterstic central sunburst,radial or stellate scar pattern on CT.
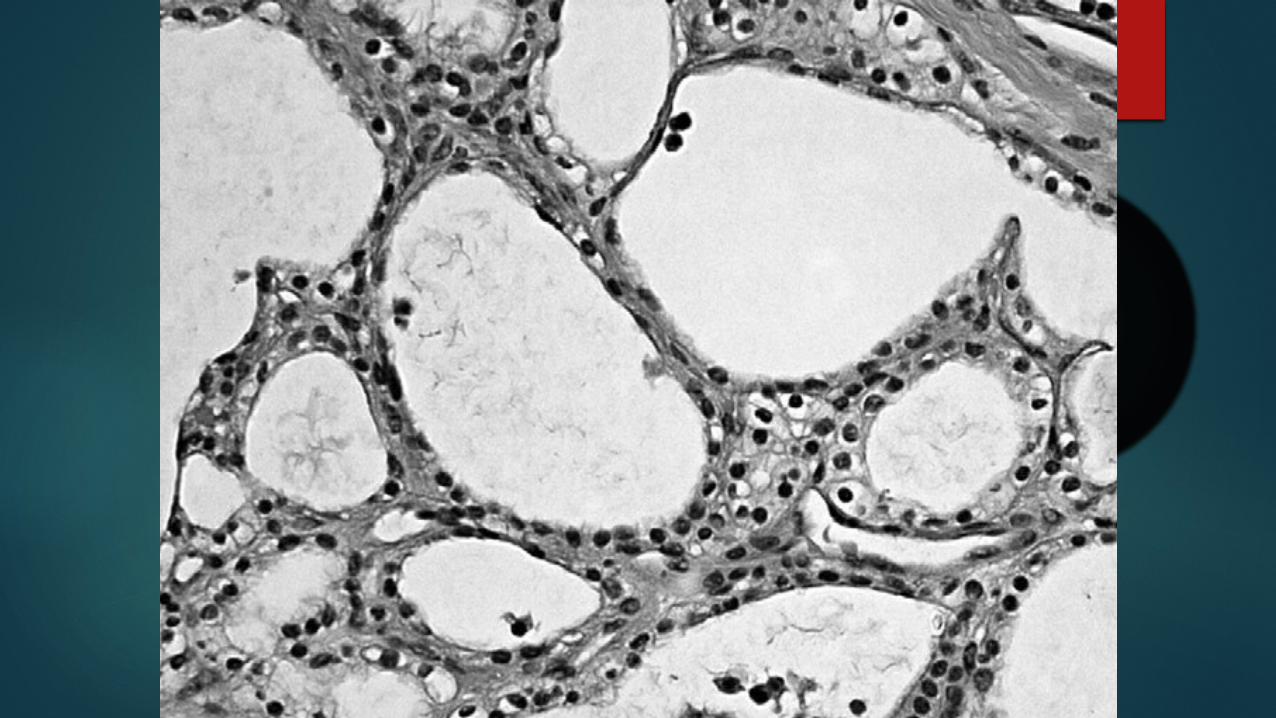
<10 % are serous oligocystic ( macrocystic )SCN have fewer cysts, usually >2cm but histopathologic appearance is similar to that of microcystic.
Histologically they are have bland cuboidal epithelial lining without nuclear pleomorphism or mitoses.
Syndromic association between VHL
SCAs are generally considered benign and only 25 cases of serous adenocarcinoma have been reported in world literature as of 2010.
True incidence of malignancy within SCA is less than 1%.
CLINICAL FEATURES
SCNs are typically asymptomatic and are observed more commonly in women ( 75 % )with a mean age at diagnosis of 62years.
Symptoms depends on cyst size; it includes - abdominal pain ( 25 % )
- fullness or mass ( 10% ) - jaundice ( 7% )
CT Findings
Most are well-demarcated solitary multicystic masses composed of innumerable small cysts. Up to one-third have a central, calcified starburst scar.
Predilection for body and tail.
EUS-FNA and analysis of fluid – SCN low amylase and viscosity.
CEA < 5ng/ml, CA 19-9 < 37U/L, excludes MCN and IPMN.
MUCINOUS CYSTIC NEOPLASMS
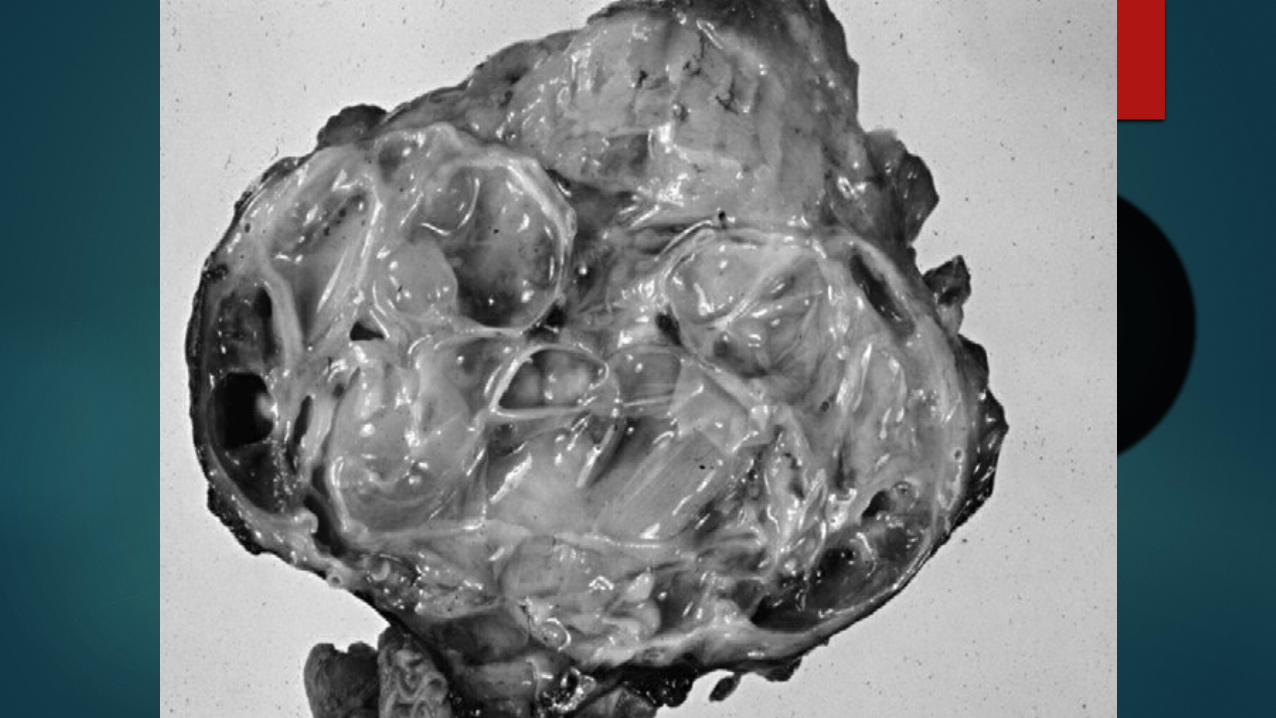
They are mucin secreating cystic tumours that lack communication with the pancreatic duct and contain mucin secreting columnar epithelium.
Grossly, individual cysts are typically greater than 2cm and the tumour mass can be as large as 25cm.these tumours are round with smooth surface and fibrous pseudocapsule.

MCNs are generally contain less than 6 cysts and are spherical in shape.
MCNs are typically located in body and tail ( 95 % ).peripheral eggshell like eccentric calcification occur in 15% of cases and are considered pathognomonic.
Ovarian like stroma surrounding the columnar epitheliumis also pathognomonic and it is the presumed reason that are almost exclusively seen in females( >95% ).

MCNs exhibit characteristics of an adenoma-carcinoma - sequence
RISK FACTORS
Large tumour size (4cm). Associated mass,mural nodules,asymmetrical
thickened wall. eggshell calcification. Age. Splenic vein obstruction.
IMAGING
CT - large cysts with thick irregular walls. Calcification of walls- High chance of malignancy.
MRI/MRCP – no communication with pancreatic duct.
EUS-FNA and analysis of fluid- CEA < 192ng/ml
INTRADUCTAL PAPILLARY MUCINOUS NEOPLASM
IPMNs constitute 15-30% of allcystic lesions. They are intraductal proliferation of neoplastic
mucinous cells leading to dilatation of main panreatic duct or branch ducts.
WHO classification1. Adenoma2. Borderline3. Ca in situ
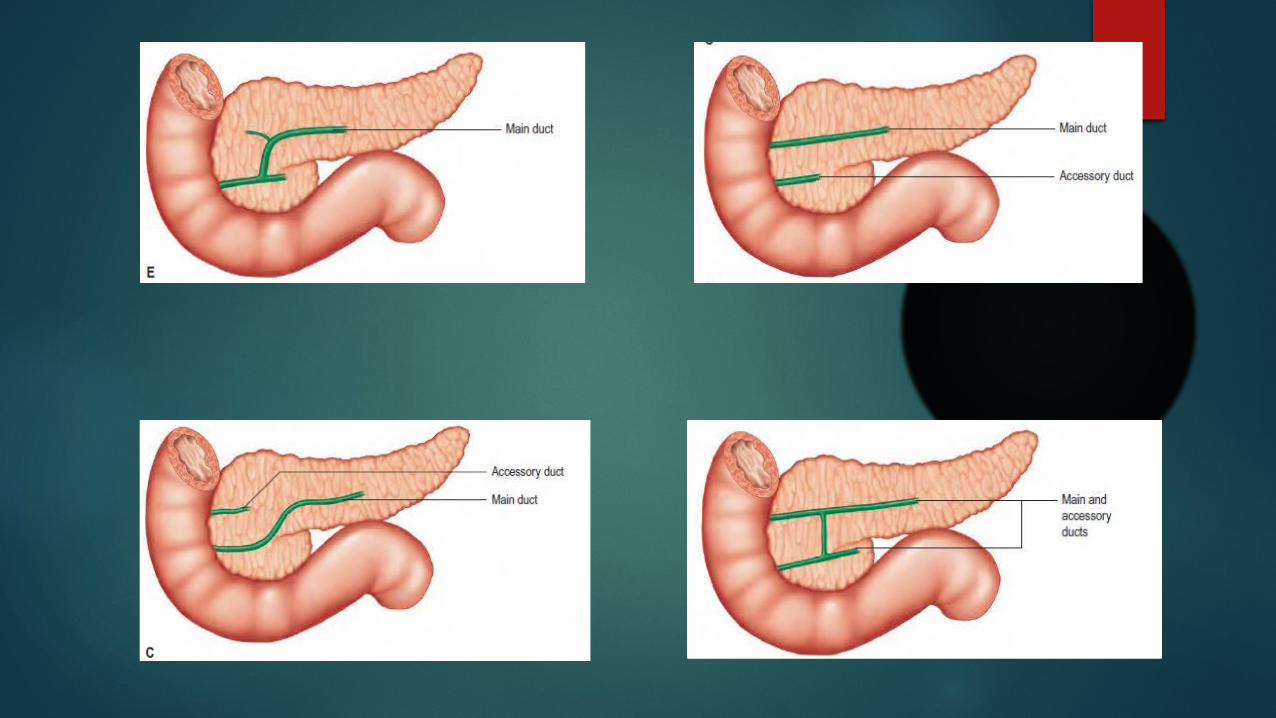
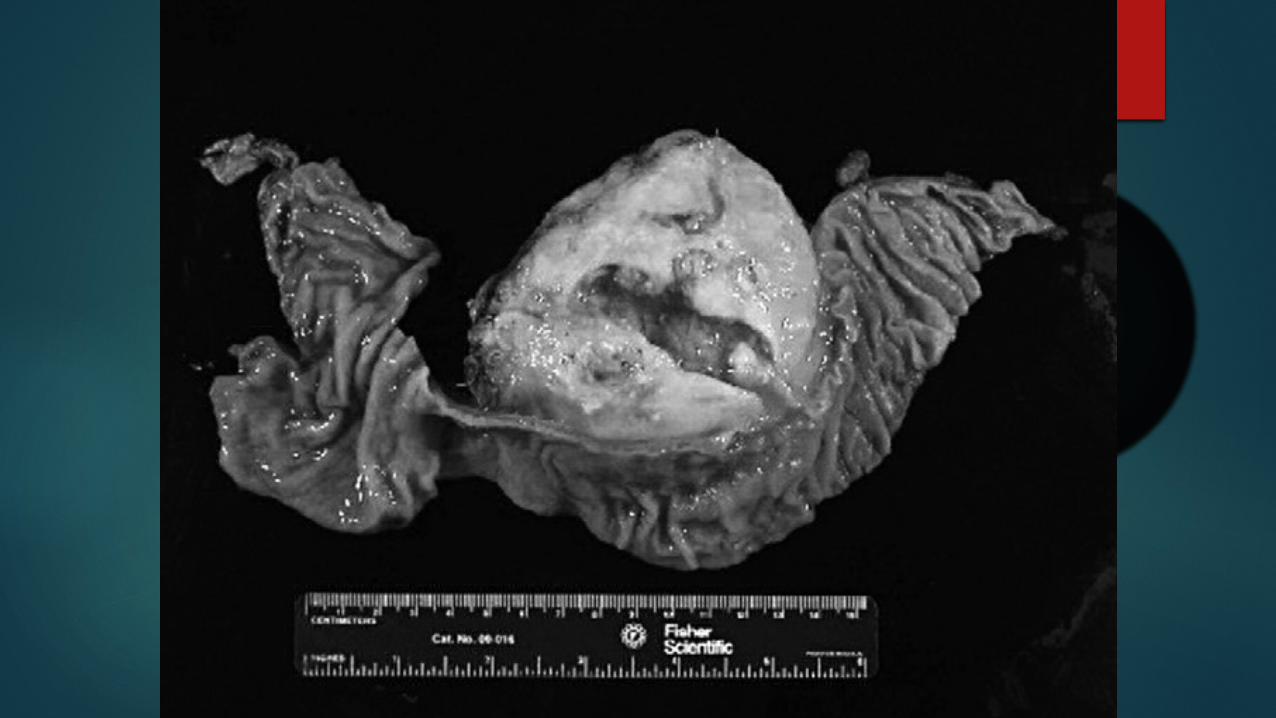
Morphology - IPMN
main duct type branch duct type combined type
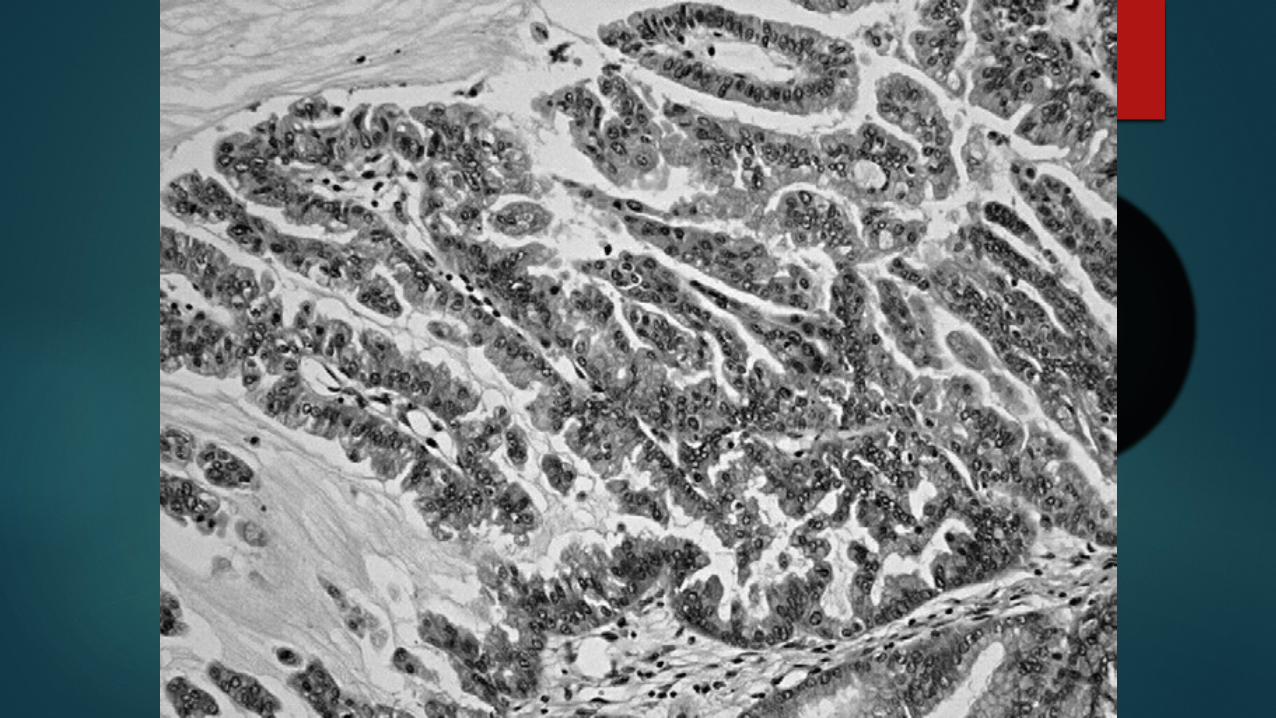
Histology
Gastric foveolar type – Tall columnar cells, mucin, scattered Goblet cells – Common in branch type.
Villous intestinal type- Resemble colonic villous adenoma- Common in Main duct type.
Pancreato biliary – lined by cuboidal cells
Clinical features
Main duct and combined are usually symptomatic early. Branch type present as asymptomatic cystic neoplasm.
Pancreatitis in main duct type, development of malignancy more in main duct type
RISK FACTORS FOR MALIGNANCY
Main duct disease – risk of malignancy 50 – 90%.invasion risk is 40 – 50%.
Branch duct – risk is 25% with invasion <15% Age >70yrS old Progressively worsening diabetes, abnormal
ca-19.9
Extra pancreatic malignancies in patients with IPMN
Colorectal adenomas and carcinopmas Barrets mucosa and gastric carcinoma
Imaging - CT
IPMNs- Cystic masses with dilatation of pancreatic duct, mural nodules projecting into the cystic spaces.
50% in pancreatic head.
IPMN, ERCP is the diagnostic procedure of choice - the communication between the cystic dilation (or branch-duct ectasia) and the main pancreatic duct,
Reveals the extend
Magnetic Resonance Cholangiopancreatography
more sensitive than ERCP in imaging pancreatic duct anatomy because plugging of side-branch ducts by mucin.
Non invasive, no risk of pancreatitis
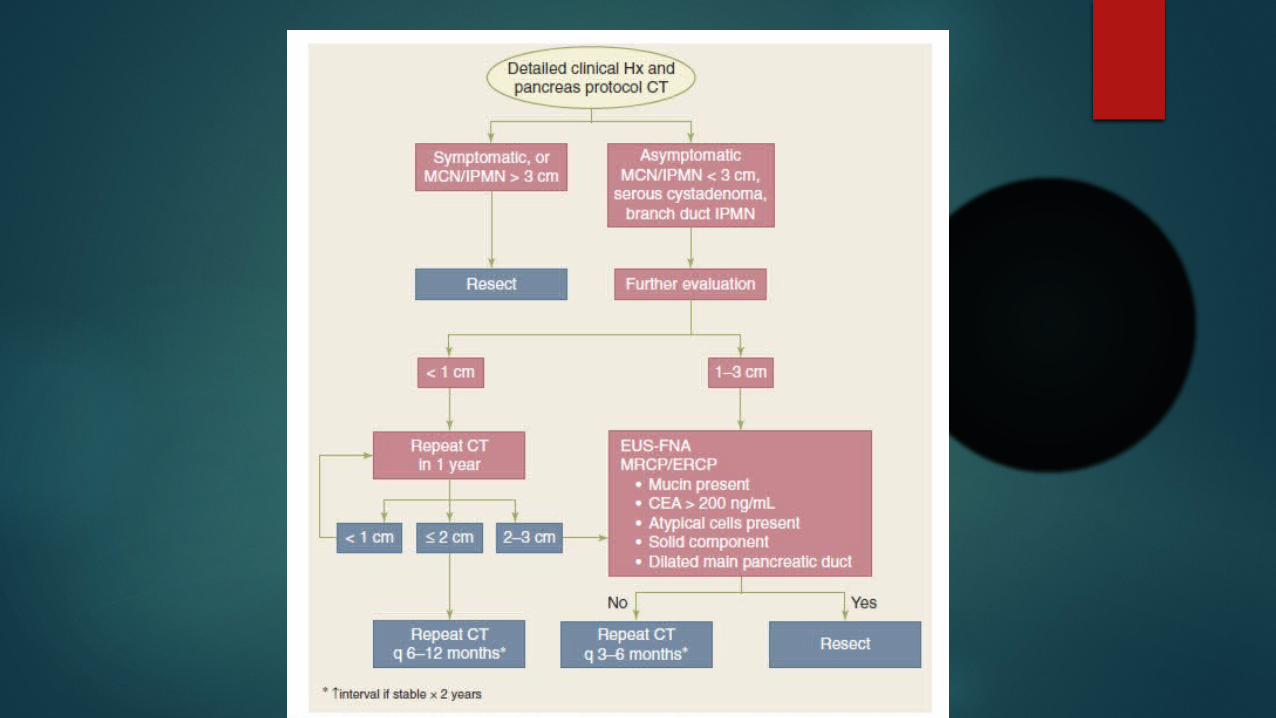
Imaging characteristics of development of invasive carcinoma
tumor size (cyst diameter ≥30 mm) main duct type IPMN main duct dilatation greater than or equal to 10 or 15
mm, patulous papilla, mural nodules presence of biliary ductal dilatation greater than or equal
to 15 mm, a solid mass, or occurrence of an area of abnormal attenuation in the
surrounding pancreas.
EUS
Endoscopic ultrasonography (EUS) can provide detailed images of the wall and the internal architecture of the cystic lesion (i.e., septations and mural nodules, observed in MCNs), - differentiating from SCN.
EUS guided FNA

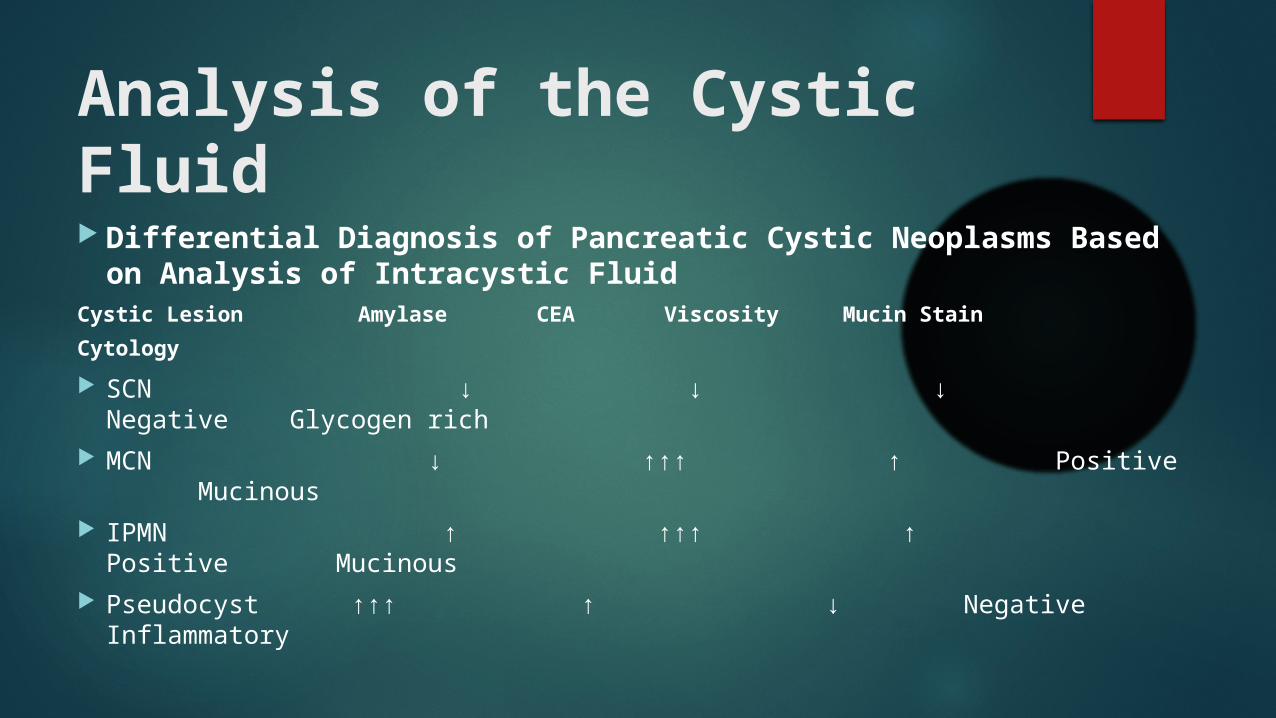
Analysis of the Cystic Fluid Differential Diagnosis of Pancreatic Cystic Neoplasms
Based on Analysis of Intracystic Fluid Cystic Lesion Amylase CEA Viscosity Mucin Stain Cytology SCN ↓ ↓ ↓ Negative Glycogen rich MCN ↓ ↑↑↑ ↑ Positive Mucinous IPMN ↑ ↑↑↑ ↑ Positive Mucinous Pseudocyst ↑↑↑ ↑ ↓ Negative Inflammatory
Likeintracystic CEA concentration greater than 250 ng/ml reliably differentiates a mucinous from a serous neoplasm,
a value of less than 5 ng/ml is quite sensitive for excluding a mucinous neoplasm.
high amylase activity (>×5 serum activity) strongly suggests that the cyst is a pancreatic pseudocyst

TREATMENT
SCN - Observation in asymptomatic patients. - Enucleation - Resection – PPPD / Central pancreatectomy /
distal pancreatectomy depending on location - if symptomatic or if the diagnosis is in doubt
MCN – All symptomatic MCNs and MCNs > 3 cm, or those containing nodules or papillae needs resection.
IPMN treatment
Formal oncologic resection of all IPMN of main duct type and mixed variants,
those showing main pancreatic duct dilatation greater than or equal to 10 mm
the presence of mural nodules, a positive cytology,
IPMN – observation if
Branch duct IPMNs less than 30 mm in diameter, without evidence of mural nodules or main duct dilatation.
Indications for resection in a case managed with observation
appearance of symptoms, cyst expansion to greater than 30 mm, detection of positive cytology on FNA,
development Identification of mural nodules or main
pancreatic duct dilatation (≥6 mm)
Pancreatic neuro endocrine tumours
PNET
Rare ,annual incidence of approximately 5 cases per 1,000,000 population.
Functioning and Non functioning Sporadically or as a part of syndromes.
Syndromic pNETS 10% are associated with an underlying genetic syndrome
(MEN1) and type IV (MEN4) –pNETS in 80-100% of patients Small, multifocal and microscopic Gastrinomas (>80% duodenal) develop in 54% of MEN-1 patients,
insulinomas in 18% and glucagonomas, VIPomas, somatostatinomas in <5%
Von Hippel-Lindau disease (VHL),-10% patients develop pNETS Neurofibromatosis type I (NF1), tuberous sclerosis complex (TSC)
2% of total pancreatic mass are islets APUD cells – 4 cell types, α, β, γ, δ

Insulinoma
Most common 60% Origin- β cells almost universally within the pancreas (1/3head – 1/3 body – 1/3 tail) F>M 90% benign, 10% malignant
Most solitary, 10% multiple(MEN 1) 21% MEN 1 – insulinomas The median age at diagnosis- 47yrs
Clinical Presentation Whipple’s triad -
(1) symptoms of hypoglycemia, (2) plasma glucose level ( <50
mg/dl), (3) relief of symptoms with administration of
glucose.
Over weight
Diagnosis: -monitored 72hrs fasting test
Neuroglycopenic symptoms Serum glucose<50mg/dl in men <40 in women Serum level of insulin >7μU/L Serum C-peptide(>0.7ng.ml),Proinsulin >6.5 pmol
Gastrinoma /Zollinger-Ellison Syndrome
Second most frequent 1 / 2.5 million 60% malignant (mets to liver) 75 % sporadic M>F Average age -50 years,5 to 10 years earlier in MEN-1 25 % MEN-1
How to suspect Gastrinoma
Refractory peptic ulcer disease. Ulcers at uncommon locations, ulcers in distal
duodenum and jejunum.
Symtoms
Symptoms of peptic ulcer disease with diarrhoea
• Clinical Features– Abdominal Pain 70%– Diarrhea 70%– Heartburn 50%– Nausea 25%– Vomiting 20%– Weight Loss 15%
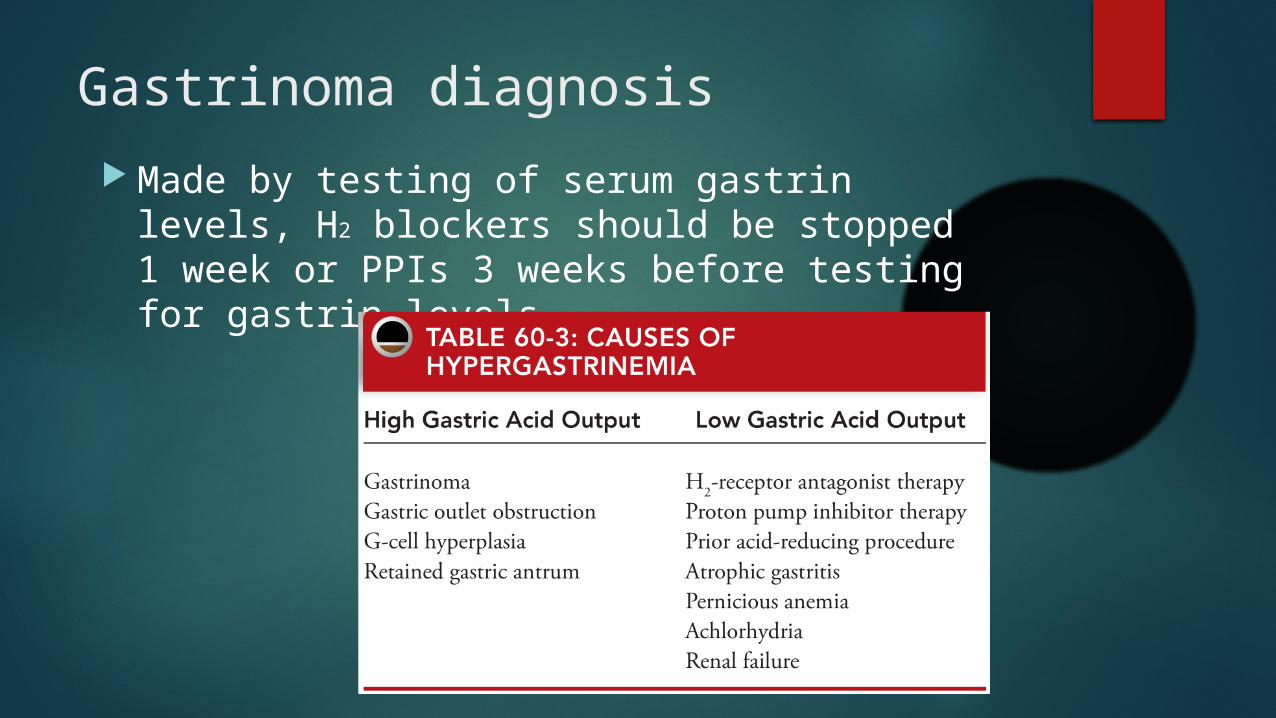
Gastrinoma diagnosis Made by testing of serum gastrin levels, H2
blockers should be stopped 1 week or PPIs 3 weeks before testing for gastrin levels.
Fasting Serum Gastrin (Cessation of PPI for 2 week) > 150pg/ml
Above 1000pg/ml is diagnostic
Provocative test(Secretin stimulation test) -Rise by 200 pg/mL or more
VIPOMA(Verner-Morrison Syndrome)
0.05-0.2 new cases per million adults Third most common neuroendocrine tumor of the pancreas Solitary, found in body or tail, usually detected at >3cm size 2/3 malignant Male-to-female ratio in children - 1:1,
in adults. - 1:3
Clinical features
Constant features Watery Diarrhea Hypovolemia Hypokalemia Acidosis
WDHA SYNDROME – Pancreatic cholera
Variable features Achlorhydria or
hypochlorhydria Hypercalcemia Hyperglycemia Flushing with rash.
VIPoma contd. Diagnostic triad
Secretory diarrhea
High levels of circulating VIP > 150pg/ml
A pancreatic tumor
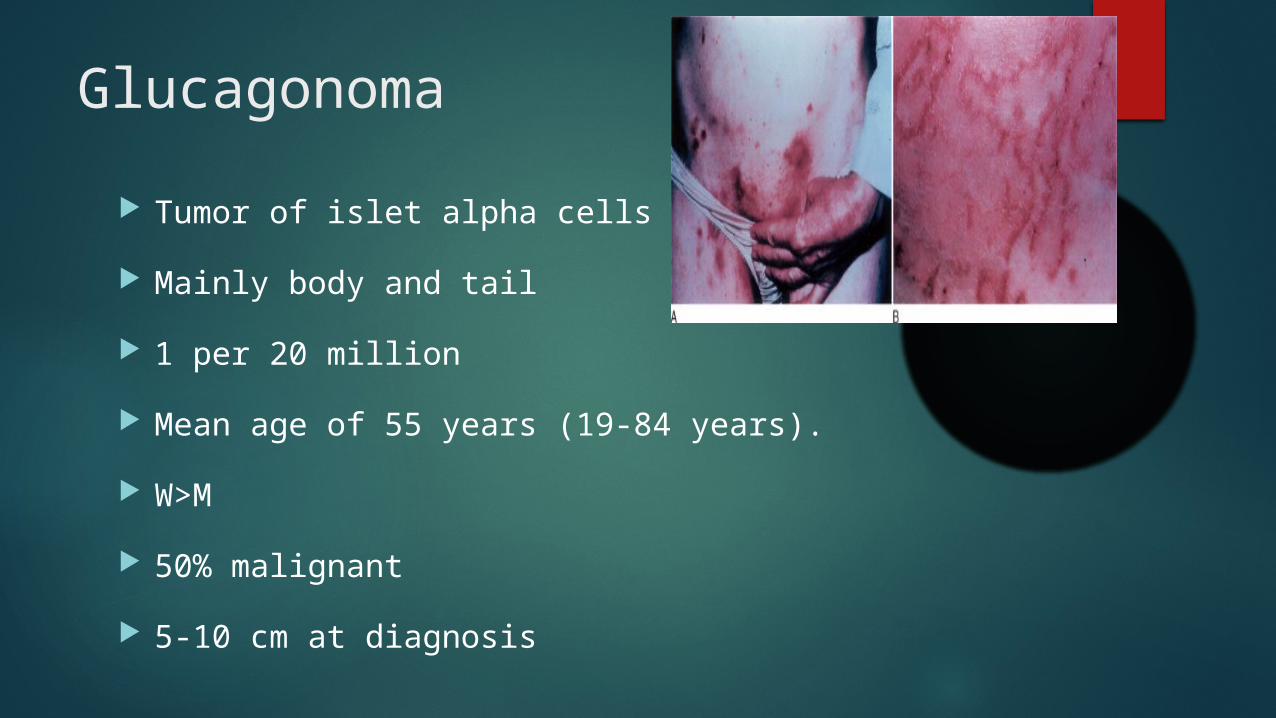
Glucagonoma Tumor of islet alpha cells Mainly body and tail 1 per 20 million Mean age of 55 years (19-84 years). W>M 50% malignant 5-10 cm at diagnosis
Migratory necrolytic erythema 2/3 cases – amino acid and trace element deficiency
4D syndrome (dermatitis, diabetes, diarrhea, DVT)
Fasting plasma glucagon >50pmol/ml: Diagnostic
Somatostatinoma Rare fewer than 100 cases in literature 70% to 90% of tumours – malignant Location – usually head Clinical findings – unpredictable
Diarrhea Gallstones – 59 % Steatorrhea Mild diabetes – 75%
Imaging and localization
CT – 71-82% sensitivity. Vascular blush is important.
MRI- can differentiate pancreatic parenchyma and small tumors.
SRS – Abundance of somatostatin receptors in pnet.
Somatostatin receptor scintigraphy (SRS)
111Indium-DTPA-octreotide (octreoscan)
frequently (>80%, except insulinomas) over-express somatostatin receptors (particularly subtypes sst 2, 5)
Sensitivity - 50-70% of primary PNETS and >90% of patients with metastatic disease.

If CT/MRI fails - EUS
EUS has a greater sensitivity for detecting tumours less than 3 cm and an overall sensitivity of 93% for tumours of all sizes.
FNA is important especially in non functioning tumours to rule out adeno carcinoma

If CT/MRI and EUS fails - Angiogram
Angiography will detect approximately 70% of insulinomas greater than 5 mm.
Usually localization difficulty may be there with insulinoma and gastrinomas, as VIPomas, glucagonomas, and somatostatinomas are usually larger and easier to localize

If all modalities fails
Blind exploration and intra operative USG
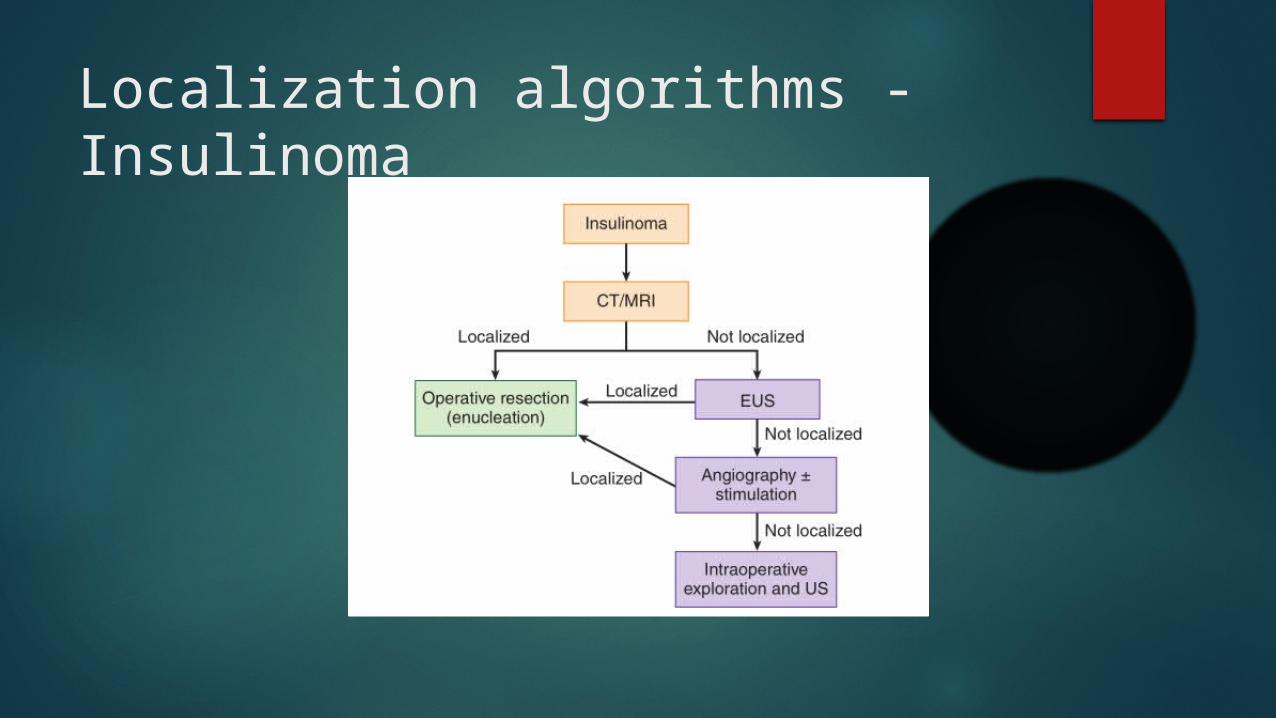
Localization algorithms - Insulinoma
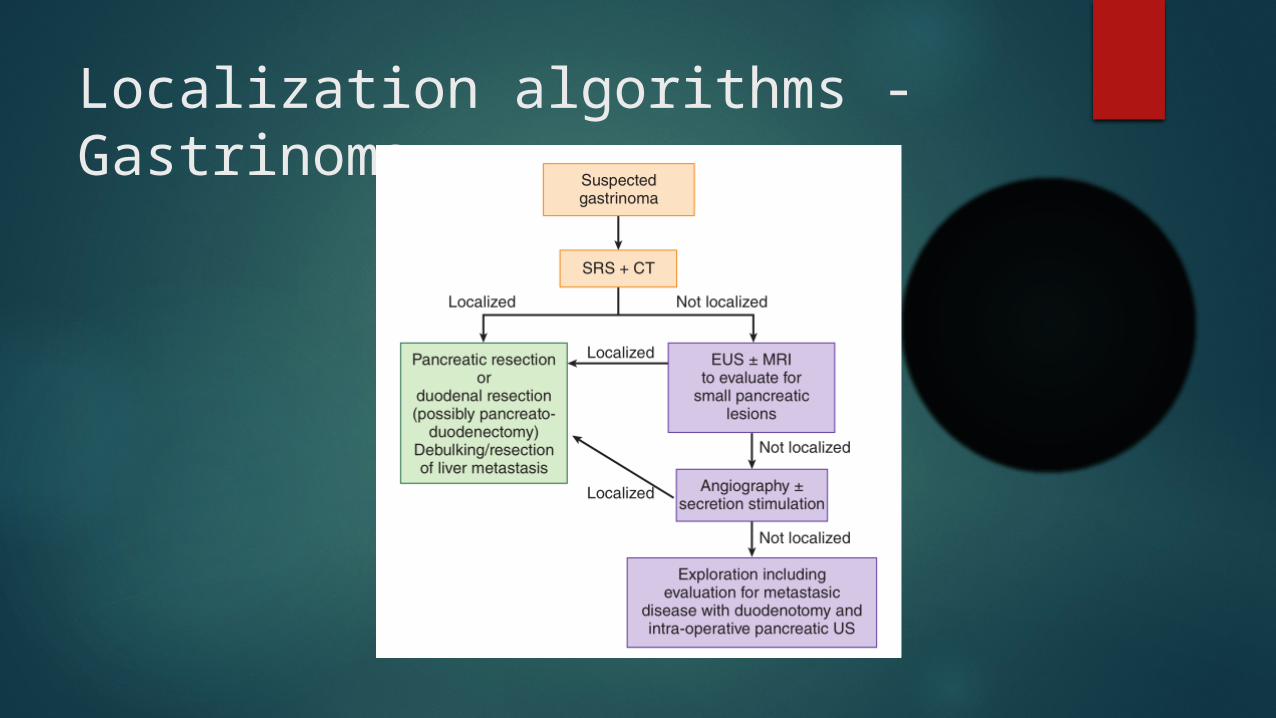
Localization algorithms - Gastrinoma
Treatment
Surgical treatment is the mainstay
Surgical management Surgical resection - the only curative
treatment for pancreatic neuroendocrine neoplasms
Management is similar for functional and non functional tumors
Insulinoma and Gastrinoma
Small, well-encapsulated tumours in the pancreas can be removed by enucleation.
Large, un-encapsulated lesions deep within the gland may require segmental resection, including distal pancreatectomy or pancreaticoduodenectomy.
VIPoma, glucagonoma, somatostatinoma, nonfunctioning pancreatic endocrine tumors
simple enucleation is inadequate and partial pancreatic resection is usually recommended.

Thank you






![Neuroendocrine Neoplasms of the Pancreas: The Pathological …€¦ · neoplasm of the pancreas, accounting for approximately 1–2% of all pancreatic neoplasms [1, 2]. The incidence](https://static.fdocuments.net/doc/165x107/5f6d4c375d58c6724b1aebea/neuroendocrine-neoplasms-of-the-pancreas-the-pathological-neoplasm-of-the-pancreas.jpg)