PANCREAS Randolph K Peterson, M.D. Department of Laboratory Medicine and Pathology Med 6724....
86
PANCREAS Randolph K Peterson, M.D. Department of Laboratory Medicine and Pathology Med 6724. Gastrointestinal/Hepatobiliary System
-
Upload
emory-chambers -
Category
Documents
-
view
222 -
download
3
Transcript of PANCREAS Randolph K Peterson, M.D. Department of Laboratory Medicine and Pathology Med 6724....
PANCREAS
Randolph K Peterson, M.D.Department of Laboratory Medicine and Pathology
Med 6724. Gastrointestinal/Hepatobiliary System

PANCREAS: GENERAL
• Surrounded by vital structures• Inaccessible• Exocrine & endocrine portions• Enzymes = precursors, inhibitors
ACUTE PANCREATITIS
There are many etiologies. The most common is believed to be transient or partial OBSTRUCTION resulting in bile reflux into the pancreatic duct system with activation of pancreatic enzymes and subsequent tissue destruction.80% of cases are associated with biliary tract disease (M;F= 1:3), or
alcoholism Post-operative due to surgical trauma Parathyroid adenoma/carcinoma (10-20% develop pancreatitis) Rarely hypercalcemia, drugs (thiazides, furosemide, estrogen)

ACUTE PANCREATITIS (2)
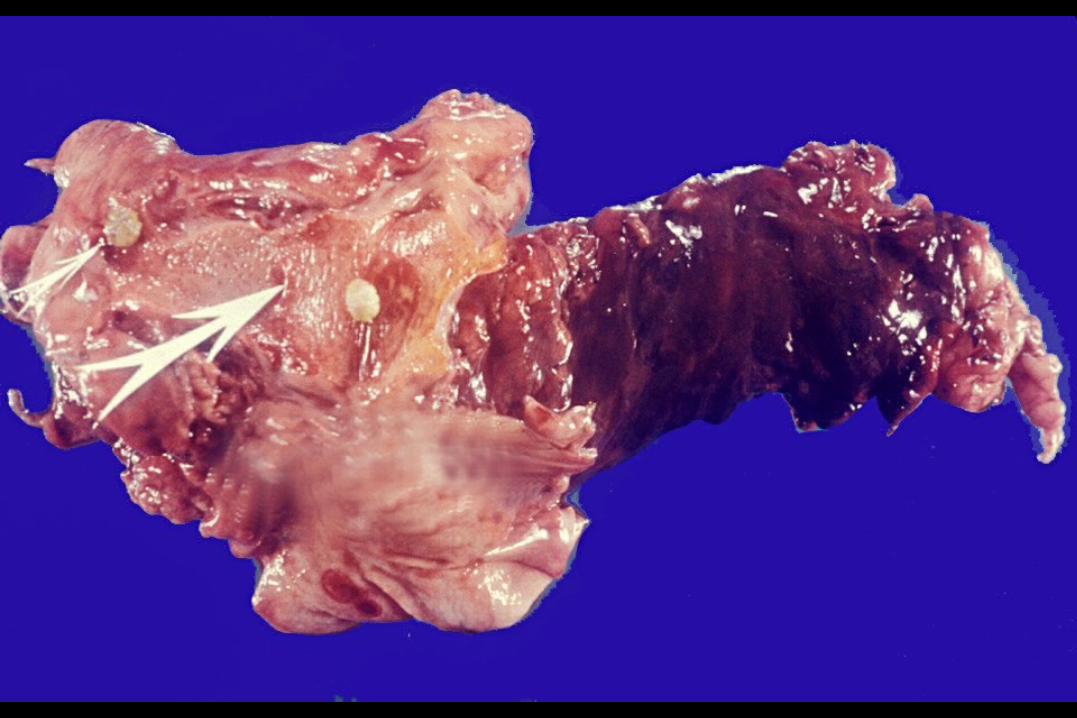
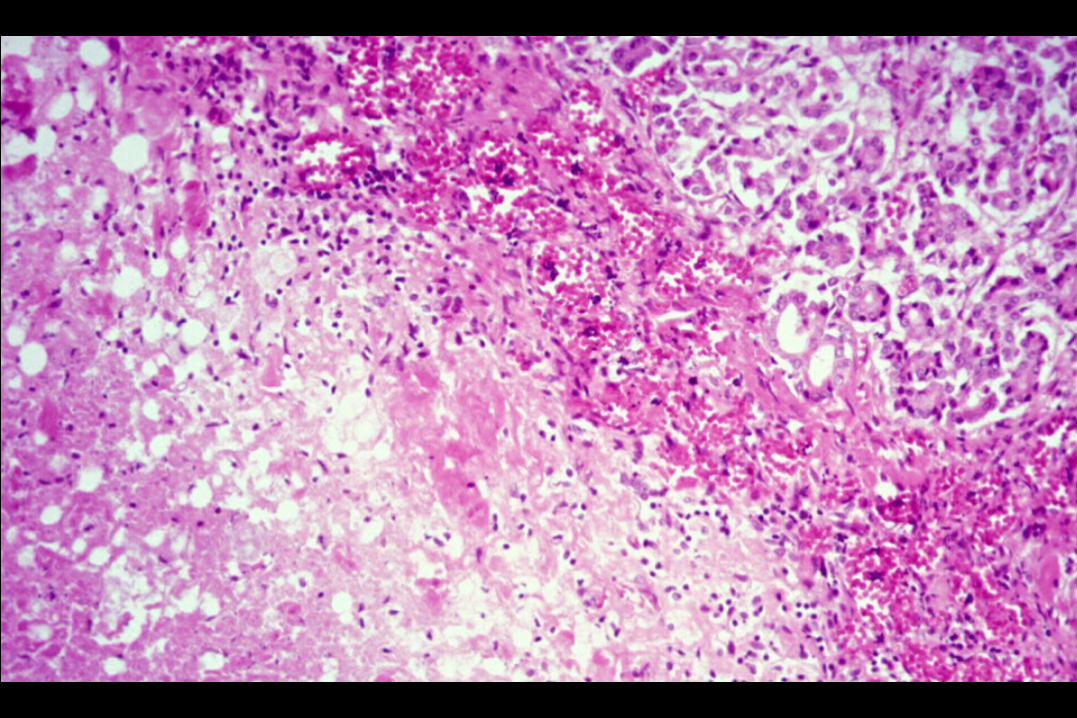
• Presents in 2 forms:– Acute pancreatitis– Acute hemorrhagic/necrotizing pancreatitis
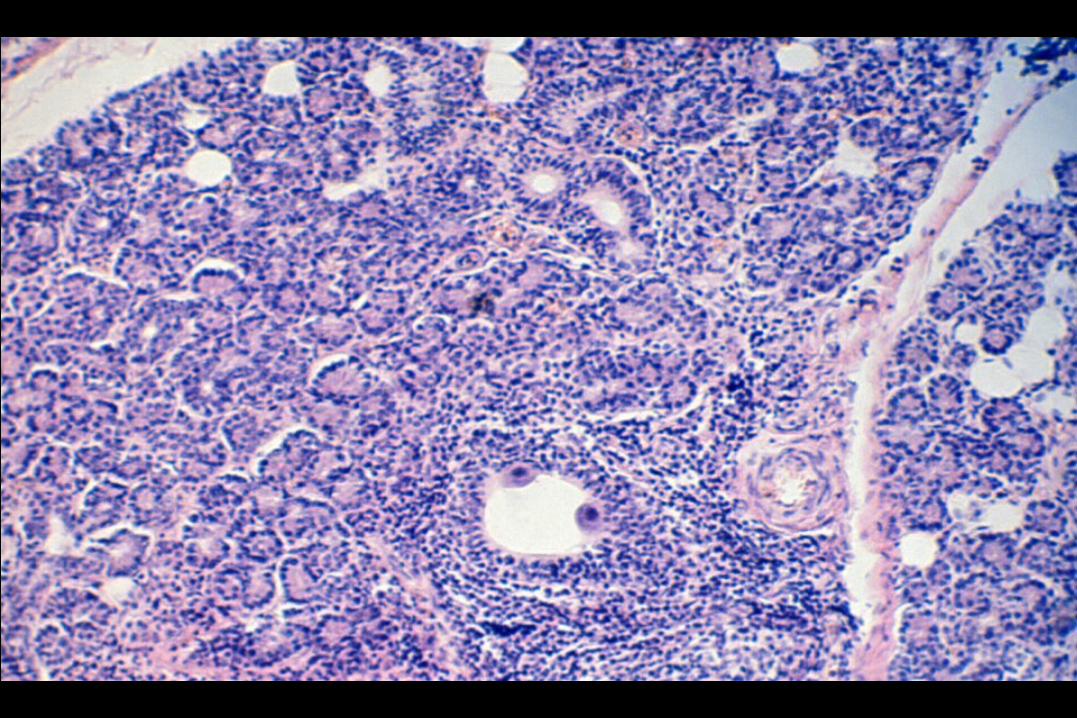
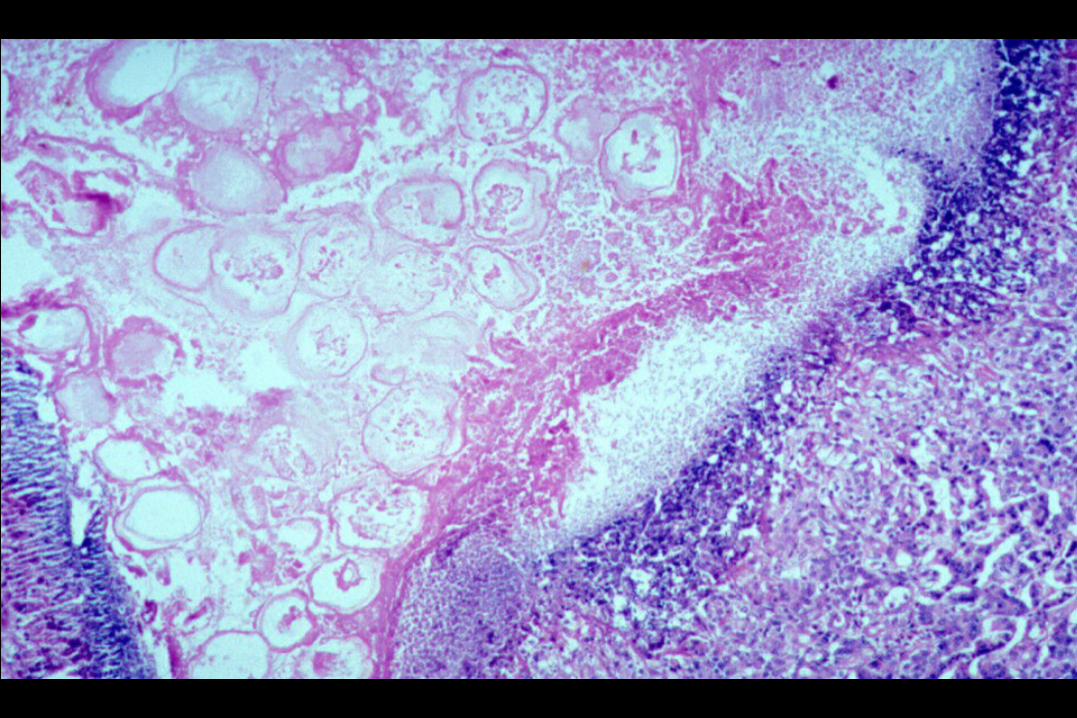
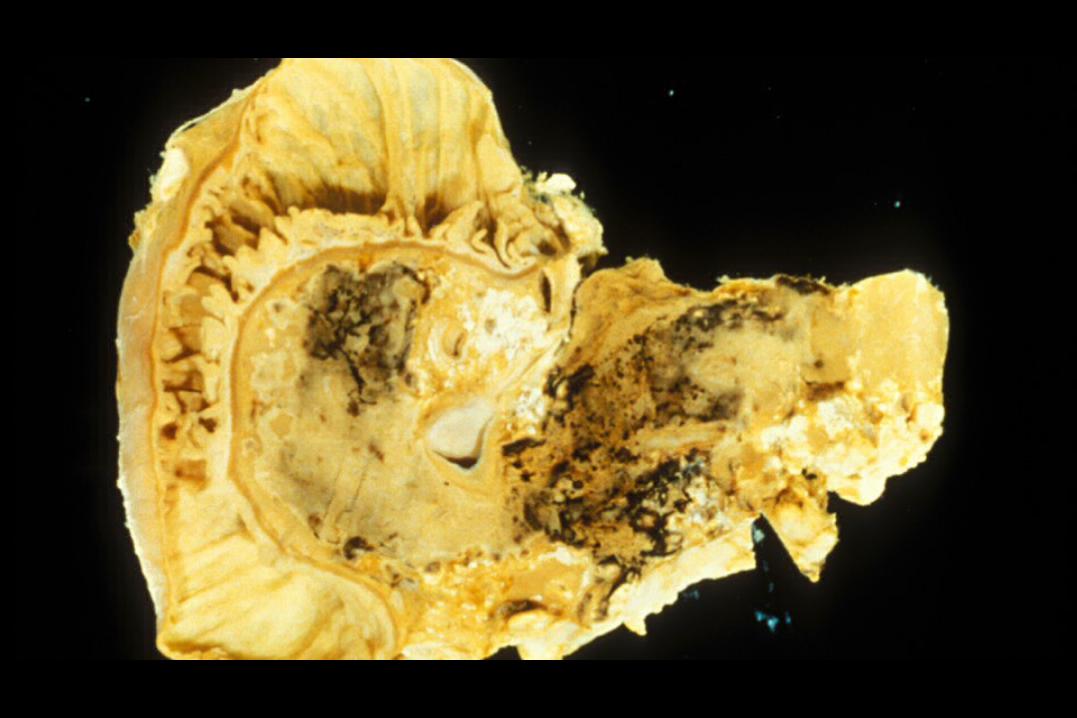
• Histologically there is ductal dilation, edema, inflammation, fibrosis, fat necrosis, and calcification.
• Large abscess formation may occur.• 20% overall mortality rate– 10-15% with non-necrosis/hemorrhage– 50% with

ACUTE PANCREATITIS: RISK FACTORS (1)
• Alcohol (75%)• Gallstones (50%)• Trauma (also cardiopulmonary bypass: 1-8%)• Pancreatic duct obstruction by tumor• Germline mutation involving trypsin (cationic trypsinogen gene
PRSS1) or of its inhibitor (serine protease inhibitor Kazal type 1: SPINK1)
• Chronic pancreatitis (?)
MOST IMPORTANT

ACUTE PANCREATITIS: RISK FACTORS (2)
• Inflammation (virus [hepatitis, mumps, CMV, coxsackie]; ulcer)
• Ischemia (atherosclerosis; cardiopulmonary bypass)
• Drugs ("The Pill," thiazide; others)
• Hyperlipoproteinemia
• Hypercalcemia
• Idiopathic (10%)

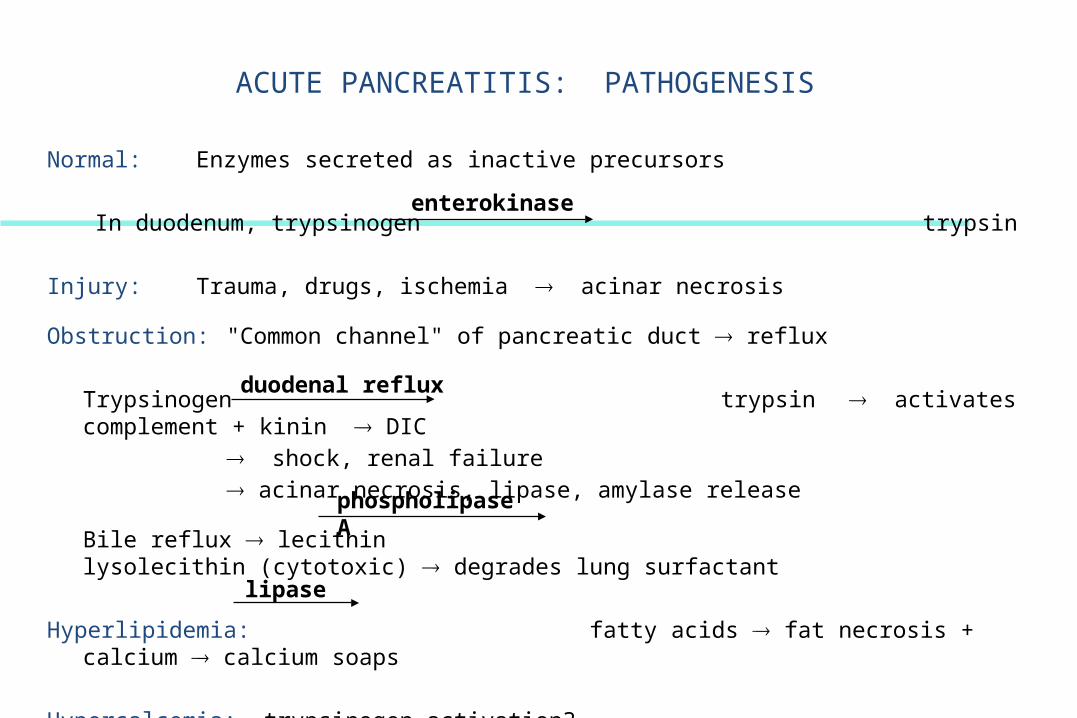
ACUTE PANCREATITIS: PATHOGENESIS
Normal: Enzymes secreted as inactive precursors
In duodenum, trypsinogen trypsin
Injury: Trauma, drugs, ischemia ® acinar necrosis
Obstruction: "Common channel" of pancreatic duct ® reflux
Trypsinogen trypsin ® activates complement + kinin ® DIC® shock, renal failure
® acinar necrosis, lipase, amylase release
Bile reflux ® lecithin lysolecithin (cytotoxic) ® degrades lung surfactant
Hyperlipidemia: fatty acids ® fat necrosis + calcium ® calcium soaps
Hypercalcemia: trypsinogen activation?
enterokinase
duodenal reflux
phospholipase A
lipase


ACUTE PANCREATITIS: PATHOGENESIS
Normal: Enzymes secreted as inactive precursors
In duodenum, trypsinogen trypsin
Injury: Trauma, drugs, ischemia ® acinar necrosis
Obstruction: "Common channel" of pancreatic duct ® reflux
Trypsinogen trypsin ® activates complement + kinin ® DIC® shock, renal failure
® acinar necrosis, lipase, amylase release
Bile reflux ® lecithin lysolecithin (cytotoxic) ® degrades lung surfactant
Hyperlipidemia: fatty acids ® fat necrosis + calcium ® calcium soaps
Hypercalcemia: trypsinogen activation?
enterokinase
duodenal reflux
phospholipase A
lipase


ACUTE PANCREATITIS: PATHOPHYSIOLOGY
• Kinin activation (kallikrien, bradykinin) by trypsin (?) vasodilatation
• Glucagon (early), insulin (late) sugar
• Lung: ARDS (shock? circulating proteases
Shock:volume down (vasoactive peptides?retroperitoneal edema?
• DIC: circulating proteases (?);Kidney function down










ACUTE PANCREATITIS: CLINICAL FEATURES
• Pain
• Fever
• Nausea, vomiting, ileus
• Jaundice
– Gallstones?
– CBD compression?
– Liver?
• Coma
• Death
ACUTE PANCREATITIS: DIAGNOSIS (1)
• Serum, urine amylase:
– 24 hrs (but also in gut obstruction)
– salivary gland
• Serum, urine lipase: 3rd day
• Triglycerides
• Calcium (±)
• Bilirubin ±
ACUTE PANCREATITIS: COMPLICATIONS
• Retroperitoneal fluid accumulation
• Shock liver, kidney, lung †
• Inflammatory pseudocyst
• Abscess (gram negative)
• Distant fat necrosis (CNS)
• ARDS (acute respiratory distress syndrome):
– Lung capillary injury by trypsin, lipase
ACUTE PANCREATITIS: Rx
• Supportive (watch fluid balance!)
• Abscess: drain , antibiotics
• Pseudocysts:
– Half resolve spontaneously
– Half drain surgically (internal? External)
• GI bleed: Rx like ulcer
• Prognosis: About 10% die
• Preventive: remove gallstones; no alcohol



CHRONIC PANCREATITIS
• Definition: chronic (or recurrent), progressive pancreatic destruction with pain, malabsorption, diabetes mellitus.
• 2 Types:– Chronic obstructive pancreatitis: narrowing or obstruction due to
stone or tumor. Less severe than below– Chronic calcifying pancreatitis: most commonly seen in alcoholics.
Damage is irregular and patchy. More severe with changes in duct epithelium with calcifying ductal “plugs”, acinar atrophy, and fibrosis.
• 30% = CFTR gene mutation (but not effects of cystic fibrosis)

CHRONIC PANCREATITIS: Complications
• Ductal dilatation with overall loss of pancreatic tissue• Acinar destruction• Islet destruction• Psuedocyst formation• Widespread “metastatic fat necrosis due to release of lipase• Avasular bone necrosis• Stetorrhea• Diabetes













CHRONIC PANCREATITIS: RISK FACTORS
• ETOH:– Chronic pancreatitis present in half of alcoholics (at autopsy)– Gallstone-induced acute pancreatitis does not lead to
chronic pancreatitis• Tropical residence• Trauma• Hyperparathyroidism• Hyperlipidemia

CHRONIC PANCREATITIS: DIAGNOSIS & Rx
• Clinical history• X-ray (calcifications). CT scan; endoscopic retrograde pancreatography• Malabsorption and/or diabetes• Absorption tests• Function tests: Administer pancreatic enzyme substrate & measure
product in urine (bentiromide or pancreatolauryl “tubeless” tests• May be difficult to exclude pancreatic carcinoma• Rx: exogenous enzymes; pancreaticojejunostomy

PANCREATIC NEOPLASMS: CARCINOMA (1)
• Clinically silent until late – >85% beyond pancreas at Dx
• Except ampulla area jaundice• Risk factors:
– Smoking– diet :fat, meat;(hyperinsulinemia?)– partial gastrectomy– male > female– >60– Black (2x)
PANCREATIC NEOPLASMS: CARCINOMA (2)
• Incidence in U.S. = 9/100,000• Mutant K-RAS genes common– others:
─CDKN2 (formerly p16)─ SMAD/DPC4 depleted in pancreatic cancer (tumor
suppressor)• Also: BRCA2 & MLH1 (latter—mismatch repair gene) • These occur in stepwise sequence beginning with in situ lesions
(pancreatic intraepithelial neoplasm (PanIN) that demonstrate telomere shortening, then as above)
PANCREATIC NEOPLASMS: Dx (1)
Clinical: weight loss, painless jaundice, back pain, palpable gallbladder, thrombophlebitis
CT scan if tumor > 2.0 cm; ultrasound (?); ERCP (endoscopic retrograde cholangiopancreatography); 85% beyond pancreas when diagnosed
Tumor markers: C19-9 (carcinoembryonic antigen) for Dx or recurrence, not screen
PANCREATIC NEOPLASMS: Dx (2)
• Biopsy:– Needle aspiration (for unresectable lesions only—Dx confirmation)– Biopsy– Mutant K-ras oncogene (PCR: polymerase chain reaction) on biopsy?
• Rare: intraductal papillary mucinous tumors– Dx: ERCP (endoscopy)
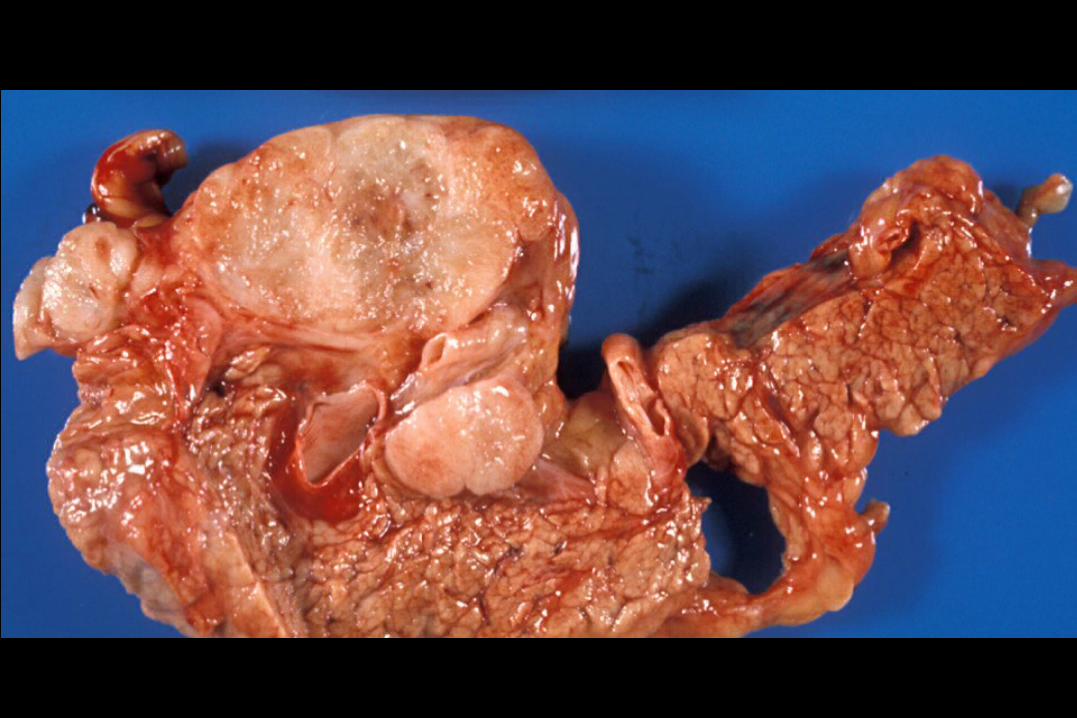
Pancratic tumors: Benign
• Microcystic Cystadenoma – Multiple small cysts lined by flat cuboidal epithelium with
abundant glycogen– Prominent vasularization, central scar
• Mucinous cystic adnoma– Young female predominance– Simple cystic spaces lined by tall mucin secreting cells.– No anaplasia or wall invasion

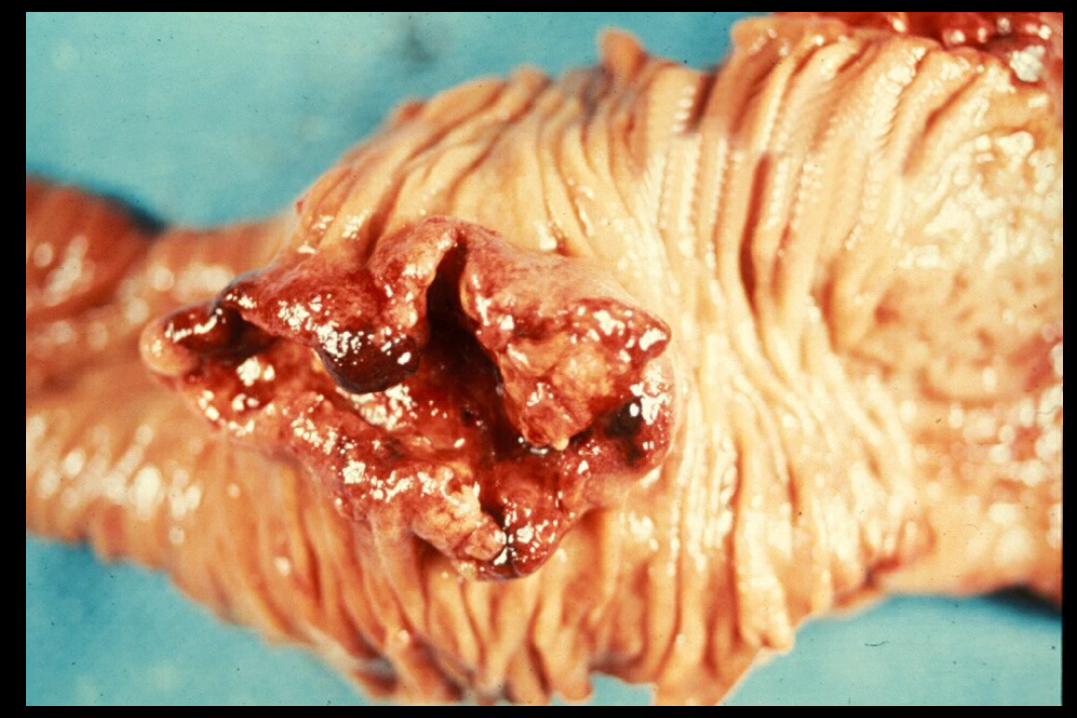
PANCREATIC CARCINOMA: PATHOLOGIC TYPES
Ductal Adenocarcinoma85% of pancratic cancers4th most common cause of ca mortality in USElderly patients, slight male pred.2/3 in head; 1/3 in tail, multiple in 20%Desmoplasia common85% beyond pancreas at dxMets to LN, liver, peritoneum, lung, adrenal, bone, skin, CNS

PANCREATIC CARCINOMA: PATHOLOGIC TYPES (2)
Papillary and solid epithelial neoplasmMost cases in young womenProbably begins as solid tunor with degeneration forming papillea
and cystic spaces.Ecellent prognosis.
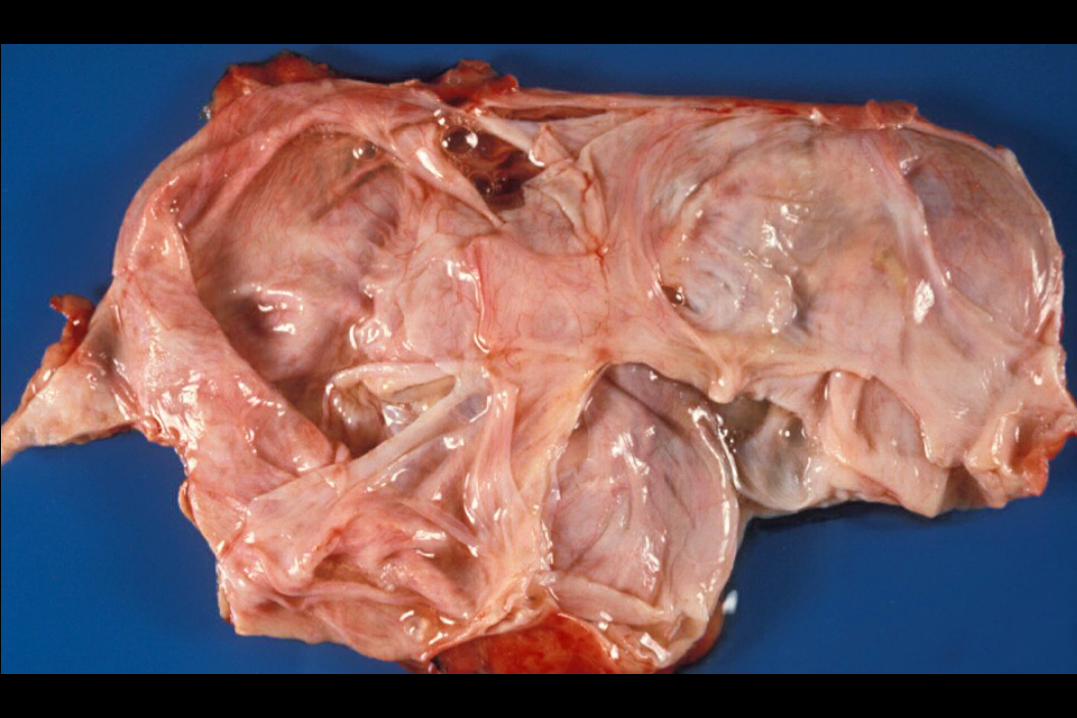
Mucinous Cystic Tumors (may be benign, see cystadenoma) Young female predominance Large encapsulated multi- or uni- locular cystic masses with tall
mucin secreating cells. Invasion of wall or presence of anaplasia indicates malignancy 5 yr survival 50%

Rarer types include:Acinar tumor: solid mass obstructing architecture of
acinar cellsAnaplastic carcinoma : poor differentiation with
extreamly poor prognosisGiant cell tumor: prognosis similair to ductal
adenocarcinoma Other considerations: tumors of the Ampula
present earlier and may have better prognosis.



PANCREATIC NEOPLASMS: CLINICAL
• Silent• Weight loss• Pain back (adjacent structure involvement)• Jaundice = CBD invasion (body and tail = late)• Nontender gallbladder (Courvoisier’s sign)• Migratory thrombophlebitis (Trousseau sign)• Pruritis• Acute pancreatitis (occasional)• Gut invasion melena


PANCREATIC NEOPLASMS: CLINICAL
• Silent• Weight loss• Pain back (adjacent structure involvement)• Jaundice = CBD invasion (body and tail = late)• Nontender gallbladder (Courvoisier’s sign)• Migratory thrombophlebitis (Trousseau sign)• Pruritis• Acute pancreatitis (occasional)• Gut invasion melena
















PANCREATIC NEOPLASMS: CLINICAL
• Silent• Weight loss• Pain back (adjacent structure involvement)• Jaundice = CBD invasion (body and tail = late)• Nontender gallbladder (Courvoisier’s sign)• Migratory thrombophlebitis (Trousseau sign)• Pruritis• Acute pancreatitis (occasional)• Gut invasion melena
PANCREATIC NEOPLASMS: Rx (1)
• Whipple resection:
– 5-20% resectable
– Of these, 20% operative mortality
– 4% five-year surgical
• Paliative bypass:
– Choledochoduodenostomy
– Gastrojejunostomy

PANCREATIC NEOPLASMS: Rx (2)
Chemotherapy: poor results RoRx: palliative (only a little) Cystadenocarcinomas of body & tail:
Sometimes Whipple or modification—better prognosis


Tumors of the Endocrine Pancreas
• Much less common than carcinoma of exocrin pancreas• Generally a monotonous proliferation of small cells.• Indication of malignancy include invasion and mets.• Malignant tumors are more likely to be functional!
– Beta tumor (insulinoma)• Most common• 90% solitary• 10% malignant
– Alpha tumor (glucogonoma)• Adult females• If functional usually malignant; not functional usually benign.
– G-cell tumor (gastrinoma)