PALS Vascular Access - Grand County, Colorado
21
Vascular Access Procedures © 2006 American Heart Association
Transcript of PALS Vascular Access - Grand County, Colorado

Vascular Access Procedures
© 2006 American Heart Association

© 2006 American Heart Association 2
Selection of Site and Priorities of Vascular Access
Introduction After the needs for oxygenation and ventilation have been addressed in an ill or injured child, the next management priority is vascular access. Vascular access may be established for the purposes of fluid resuscitation, administration of fluids, electrolytes, nutrition or medication, laboratory testing, and monitoring of hemodynamics. The site and priorities of vascular access depend on the provider's experience and expertise and the clinical circumstances. In performing any vascular access procedure, the provider should analyze the clinical situation, implement universal precautions, and follow sterile protocols.
During Advanced Life Support
Vascular access is vital for drug and fluid administration during advanced life support, but it may be difficult to achieve in the pediatric patient.1-5 Consider the following when evaluating vascular access options: • Rapid establishment of vascular access is more important than site
of access. • During treatment of severe shock, establish intraosseous (IO) access
if you cannot rapidly achieve venous access.5-9 When practical pursue IO and peripheral or central venous access simultaneously.
• During pediatric cardiac arrest, attempt to establish vascular access at a site that will not require interruption of compressions or ventilation.10 Immediate IO access is recommended if no other intravenous (IV) access is already in place.
• If central venous access is needed during CPR or decompensated shock, the safest site to attempt access is the femoral vein. Establishing access through the femoral vein does not require inter-ruption of CPR, and airway management is less likely to be complicated if this site is used.
• Central vascular access may be achieved via umbilical vessel catheterization in the young neonate if the umbilical vessels are still patent.
• Arterial cannulation enables direct and continuous measurement of blood pressure and access to sample blood for evaluation of oxygenation and ventilation and acid-base balance.
During attempted resuscitation if an endotracheal (ET) tube is in place but vascular access is not yet available, you may administer lipid-soluble resuscitation drugs through the ET tube.11 These drugs can be recalled using the mnemonic LEAN:

© 2006 American Heart Association 3
• Lidocaine • Epinephrine • Atropine • Naloxone Because drug absorption through the tracheobronchial tree and resulting drug levels and effects are unpredictable, administration of resuscitation drugs by any vascular or IO route is preferred to the tracheal route. Note: Intracardiac administration of drugs during closed-chest CPR is not recommended. Intracardiac injections increase the risk of coronary artery laceration, cardiac tamponade, pneumothorax, and intra-myocardial injection with resultant acute myocardial necrosis.12-14
During Nonemergent Situations
Peripheral venous cannulation is the preferred method of vascular access in most nonemergent situations. A large-bore catheter is commonly used to gain access in the proximal upper extremity. Small-bore plastic catheters allow easy and reliable venous cannulation in most infants and children.
During Postresuscita-tion
During postresuscitation a central venous catheter is the preferred method of access. It provides secure access and enables monitoring of central venous pressure. But to avoid complications and delays, only providers with significant experience and expertise should perform this procedure.
Implementa-tion of Universal Precautions
Universal precautions are infection control measures intended to reduce the exposure and transmission of blood and other body fluid pathogens between patients and healthcare workers. According to the “universal precautions” principle, blood and body fluids from all patients are considered infectious regardless of the infection risk posed by the patient. While performing vascular access procedures, be particularly careful to following safe practice standards in the handling of sharps. Do the following to implement universal precautions: • Wash hands with soap and water before and after procedures. • Use protective barriers such as gloves, gowns, masks, goggles. • Use sterile or disinfected instruments and equipment. • Use single-use disposable equipment for all injections.

© 2006 American Heart Association 4
• Discard contaminated sharps immediately in puncture-proof and liquid-proof containers as appropriate.
• Place soiled linen in leakproof biohazard bags and dispose of the bags appropriately.
• Adopt locally appropriate policies and guidelines.
Intraosseous Access
Introduction Establishing vascular access in a critically ill or injured child in shock
can be difficult, but prompt IV or IO access is essential to administer needed fluids and medications. Few providers can perform advanced access techniques such as venous cutdown or central venous access quickly and safely. A delay in establishing vascular access can be life threatening. Delays can be avoided by use of IO cannulation. IO cannulation is a relatively simple and effective method of rapidly establishing vascular access when timely fluid or drug administration is needed and other means have failed or are outside the expertise of the provider. It provides access to a noncollapsible marrow venous plexus, which serves as a rapid, safe, reliable route for administration of drugs, crystalloids, colloids, and blood during resuscitation. IO access can be performed safely in children of all ages, and it can often be achieved in 30 to 60 seconds. In certain circumstances (eg, severe shock with severe vasoconstriction or cardiac arrest), it may be the initial means of vascular access attempted. IO cannulation delivers fluid and medications to the central circulation within seconds. Do not delay establishing IO access during the resuscitation of a critically ill or injured child if no IV access is already in place.
Sites Many sites are appropriate for IO infusion. The proximal tibia, just
below the growth plate, is often used. The distal tibia just above the medial malleolus, the distal femur, and the anterior-superior iliac spine are also used.
Contraindica-tions
Contraindications to IO access include • fractures and crush injuries near the access site • conditions in which the bone is fragile, such as osteogenesis
imperfecta • previous attempts to establish access in the same bone

© 2006 American Heart Association 5
Avoid IO cannulation if infection is present in the overlying tissues.
Intraosseous Procedure
Procedure You may use the following procedure to establish intraosseous
access:
Step Action 1 • To establish access in the proximal tibia, position the leg
with slight external rotation. • Identify the tibial tuberosity just below the knee joint. The
insertion site is the flat part of the tibia, about 1 to 3 cm (about 1 finger’s width) below and medial to this bony prominence (Figure 1).
Always use universal precautions when attempting vascular access. Disinfect the overlying skin and surrounding area with an appropriate agent.
2 • The stylet should remain in place during insertion to prevent the needle from becoming clogged with bone or tissue.
• Stabilize the leg on a firm surface to facilitate needle insertion. Do not place your hand behind the leg.
Note: If a standard IO needle or bone marrow needle is not available, a large-bore standard hypodermic needle can be substituted, but the lumen may become clogged with bone or bone marrow during insertion. Short, wide-gauge spinal needles with internal stylets can be used in an emergency, but they are not the preferred needles for IO use because they bend easily. A hemostat can be used to help control the needle during insertion. Use at least an 18-gauge spinal or hypodermic needle for this purpose.
3 • Insert the needle through the skin over the anteromedial surface of the tibia in a direction perpendicular to the tibia. This directs the needle to avoid injury to the growth plate.
• Use a twisting motion with gentle but firm pressure. • Continue inserting the needle through the cortical bone
until there is a sudden release of resistance as the needle enters the marrow space. If the needle is placed correctly, it should stand easily without support.

© 2006 American Heart Association 6
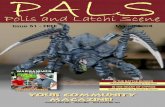
Figure 1. A, General landmarks for IO insertion in the leg of an infant. B, Locations for IO insertion in the proximal tibia and distal femur in older children. C, Location for IO insertion in the iliac crest. D, Location for IO insertion in the distal tibia. E, Technique for immobilizing the leg while twisting the IO needle into the leg of an infant.
4 • Remove the stylet and attach a syringe. • Aspiration of bone marrow contents and blood in the hub of
the needle confirms appropriate placement. Blood may be sent to the lab for study. (Note: Blood or bone marrow may not be aspirated in every case.)
• Infuse a small volume of saline and observe for swelling at the insertion site or posteriorly in the extremity opposite the insertion site. (Swelling will be observed if the needle has penetrated into and through the posterior cortical bone). Fluid should easily infuse with saline injection from the syringe.
5 There are several methods to stabilize the needle. You may place tape over the flange of the needle to provide some support and position gauze padding on both sides of the needle for additional support.
6 When connecting IV tubing, tape the tubing to the skin to avoid displacing the needle from tension placed on the tubing.
7 Volume resuscitation can be delivered via a stopcock attached to extension tubing or by infusion of fluid under pressure. When using a pressurized fluid bag, take care to avoid air embolism.

© 2006 American Heart Association 7
8 Any medication that can be administered IV can be given by the IO route, including vasoactive drug infusions such as an epinephrine drip. Follow all bolus medications with a saline flush.
After IO Insertion
After IO needle/catheter insertion keep the following points in mind: • Check the site frequently for signs of swelling and needle
displacement. • Delivery of fluids or drugs through a displaced needle may cause
severe complications, such as tissue necrosis or compartment syndrome.
• IO needles are intended for short-term use, generally less than 24 hours. Replacement with long-term vascular access is usually accomplished in the intensive care setting.

© 2006 American Heart Association 8
Central Venous Access
Introduction Central venous cannulation provides a more stable and reliable route
of venous access than peripheral venous cannulation. It is a useful option when you cannot achieve peripheral cannulation or when the child is stabilized and there is time to establish more secure vascular access. Central venous access also allows hemodynamic monitoring and sampling of central venous blood for laboratory access. Use of this route eliminates problems resulting from administration of irritating or vasoconstrictive medications. This is because there is lower risk of extravasation, and medications are diluted by high-volume central venous blood flow.
Complica-tions
Complications of central venous catheterization occur more frequently in infants and children than in adults. The most common complications are infection, thrombosis, and suppurative thrombophlebitis. The following actions may reduce the risk of complications: • Limit central venous cannulation to patients with appropriate
indications. • When possible, practice meticulous aseptic technique during
catheter insertion and maintenance. • Remove the catheter as soon as possible.3,15,16 When adherence to aseptic technique cannot be ensured (ie, when catheters are inserted during a medical emergency), replace all catheters as soon as possible and after no longer than 48 hours.17 As for all procedures, providers should perform central venous cannulation only when the potential benefits outweigh the risks. A provider experienced in the technique and knowledgeable of the unique features of central venous anatomy in infants and children should perform or directly supervise the procedure.16,18-21
Doppler Devices
Knowledge of anatomic landmarks is essential for successful and safe placement of a central venous catheter. Doppler or ultrasound devices may help you locate central vessels, and they can improve your success rate for central venous cannulation.22-27
Seldinger Technique
The Seldinger (guidewire) technique16 is especially useful for establishing central vascular access. This technique allows

© 2006 American Heart Association 9
introduction of catheters (Figure 2) into the central venous circulation after initial venous entry is achieved, using a small-gauge, thin-walled needle or an over-the-needle catheter. Once you achieve free flow of blood through the small needle or catheter, thread a flexible guidewire through the needle or catheter into the vessel. Then withdraw the needle or catheter over the guidewire while holding the guidewire in place (Figure 2). To facilitate passage of the catheter or introducing sheath, incise the skin and superficial subcutaneous tissue using a No. 11 blade; insert the blade directly over the site where the guidewire enters the skin. For most catheters you will pass a dilator over the guidewire into the vessel and then remove the dilator before you place the catheter. Finally, pass a large catheter or a catheter-introducing sheath over the guidewire into the vessel and withdraw the guidewire.
Figure 2. Seldinger technique for catheter placement. A, insert the needle into the target vessel and pass the flexible end of the guidewire into the vessel. B, Remove the needle, leaving the guidewire in place. C, Using a twisting motion, advance the catheter into the vessel. D, Remove the guidewire, and connect to an appropriate flow device or monitoring device. Modified from Schwartz AJ, Cote CJ, Jobes DR, Ellison N. Central venous catheterization in pediatrics. Scientific exhibit.
Femoral Vein Cannulation
Access to the femoral vein (Figure 3) allows access to the inferior vena cava. Providers frequently use the femoral vein for emergency vascular access because it is relatively easy to cannulate. Fewer

© 2006 American Heart Association 10
immediate complications occur when this site is used.20,28,29 Cannulation also does not require interruption of compressions or ventilations. The Seldinger technique is probably the most reliable method to access the central venous system through the femoral vein during an emergency. In general the right femoral vein is preferable for cannulation. It is easier to approach from the right side when the operator is right-handed, and the catheter is less likely to migrate into the posterior lumbar venous plexus. Such migration could lead to erosion into the subarachnoid space.30 See the “Femoral Vein Catheterization Procedure.”
External Jugular Vein Cannulation
Cannulation of the external jugular vein is relatively safe because the vein is superficial and easy to see. The major disadvantages of this site are • potential compromise of the airway by extension and rotation of the
neck to expose the vein • a low success rate for central placement of the catheter because the
angle of entry of the external jugular vein into the subclavian vein is acute.31,32
See the “External Jugular Vein Catheterization Procedure.”
Internal Jugular Vein Cannulation
Figure 3 shows the internal jugular vein in relation to the carotid artery, sternocleidomastoid muscle, and clavicle. The right internal jugular vein is preferable to the left because there is less chance of producing a pneumothorax (the dome of the right lung and pleura is lower than that on the left side) and risk of injury to the thoracic duct is eliminated. The catheter can pass in a direct route from the internal jugular vein directly through the innominate vein into the superior vena cava. Three approaches are possible for internal jugular venous cannulation: the posterior, anterior, and central (middle) routes.3,32 No one approach is clearly superior to the others.33-37 The high central route appears to be the most widely used, but the provider should choose the route based on experience. See the “Internal Jugular Vein Catheterization Procedure.”

© 2006 American Heart Association 11
Figure 3. Central veins of the thorax and neck in relation to surrounding anatomy.
Subclavian Vein Cannulation
The subclavian vein in infants and children can be cannulated through the infraclavicular route.38-40 The complication rate, however, is high when this route is used during emergencies, particularly in infants.40,41 For this reason the subclavian vein is generally not the route of choice for small children when urgent access is needed. But a skilled provider may prefer the subclavian vein. The procedure does not require immobilization of an extremity, so the catheter will not limit movement of the patient after insertion. See the “Subclavian Vein Catheterization Procedure”.
Figure 4. Femoral vein. A, Anatomy. B, Cannulation technique.

© 2006 American Heart Association 12
Femoral Venous Catheterization Procedure
Procedure You may use the following procedure for femoral venous
catheterization (Figure 4B):
Step Action 1 Restrain the leg with slight external rotation. Place a small
towel or diaper under the buttocks of the infant to flatten the inguinal area. Placing the infant in this position will make the angle of entry less acute and facilitate entry into the vein.
2 Identify the femoral artery by palpation or, if pulses are absent, by finding the midpoint between the anterior superior iliac spine and the symphysis pubis. Note that pulsations in the femoral area during chest compressions may originate from either the femoral vein or femoral artery.42 If CPR is in progress, attempt needle puncture midpoint, as the point of pulsation may be arterial or venous during CPR.
3 Use a long (1-inch to 1.5-inch) 25-gauge needle to administer local anesthetic. You may also use this needle to help locate the femoral vein. Using sterile technique, access the femoral vein using a thin-walled needle. Insert the needle one finger’s breadth below the inguinal ligament and just medial to the femoral artery. Apply gentle negative pressure to an attached 3-mL syringe and slowly advance the needle. Direct the needle parallel to the arterial pulse (generally toward the umbilicus) at a 45° angle.
4 When you observe a free flow of blood into the syringe, separate the syringe from the needle and advance a guide-wire through the needle. Remove the needle and advance the appropriate central venous catheter over the guide-wire using the Seldinger technique (described earlier).
5 Once you document free blood return and free flow of infusate, secure the catheter or catheter-introducing sheath in place with suture material. Apply a sterile, occlusive dressing.
6 Obtain an x-ray to verify that the tip of the catheter is correctly positioned.
Note: Steps 4 through 6 are common to most central venous catheterization sequences.

© 2006 American Heart Association 13
External Jugular Vein Catheterization Procedure
Procedure The external jugular vein provides another portal to the central venous circulation. Although this vein is an excellent site for venous access, it can be difficult to thread a guidewire or catheter into the central circulation because the angle of entry into the subclavian vein is acute. You may use the following procedure for external vein catheterization:
1 Restrain the child in a 30° head-down (Trendelenburg) position with the head turned away from the side to be punctured (Figure 5). Auscultate and document bilateral breath sounds before you start the procedure. The right side is preferable.
2 Using sterile technique puncture the skin slightly distal to or beside the visible external jugular vein with a 16-gauge or 18-gauge needle. This puncture will facilitate entry of the catheter through the skin.
3 Use the tip of the middle (3rd) finger of your nondominant hand to temporarily occlude the vein just above the clavicle, mimicking the effect of a tourniquet.
4 Stretch the skin over the vein just below the angle of the mandible. Allow the vein to distend fully and then use the thumb of the nondominant hand to immobilize the vein.
5 For peripheral cannulation, insert a short over-the-needle catheter into the vein and proceed as described for peripheral venous cannulation. For central venous access, insert a guidewire through the over-the-needle catheter, remove the short catheter, and insert a longer catheter-over-guidewire device as described for cannulation of the internal jugular vein.
Note: Follow steps 4 through 6 in “Femoral Venous Catheterization” to complete catheterization of the external jugular vein. Auscultate and document breath sounds. If you attempted central venous catheterization, verify on a chest x-ray that the tip of the catheter is correctly positioned at or above the junction of the superior vena cava and right atrium. Rule out pneumothorax and hemothorax.

© 2006 American Heart Association 14
Figure 5. Positioning of patient for cannulation of internal or external jugular vein.
Internal Jugular Vein Catheterization Procedure
Procedure The following technique is commonly used with the anterior, central,
and posterior routes of internal jugular vein cannulation. The right side of the neck is preferable for several reasons: • The dome of the right lung and pleura is lower than that on the left,
so the risk of pneumothorax is reduced. • The path from the right internal jugular vein to the right atrium is
more direct. • Risk of injury to the thoracic duct is eliminated. You may use the following procedure for internal jugular vein catheterization:
Step Action 1 If no cervical spine injury is present, hyperextend the
patient’s neck by placing a rolled towel transversely beneath the shoulders.
2 Restrain the child in a 30° head-down (Trendelenburg) position with the head turned slightly away from the side to be punctured (Figure 5).43 Auscultate and document bilateral breath sounds before you start the procedure.
3 Identify the sternocleidomastoid muscle and clavicle.

© 2006 American Heart Association 15
4 Use a long (1-inch to 1.5-inch) 25-gauge needle to administer local anesthetic. You may also use this needle to help locate the internal jugular vein. Use the Seldinger technique to access the internal jugular vein. If the patient is breathing spontaneously with no positive-pressure support, prevent inadvertent movement of air into the superior vena cava. To prevent this air movement, use your finger to occlude any open needles or catheters during patient inspiration and try to thread the guidewire during exhalation. If the guidewire advances into the right atrium, premature atrial contractions may occur. Advance the catheter to the junction of the superior vena cava and right atrium (determine the distance beforehand from surface landmarks).
Note: Follow steps 4 through 6 in “Femoral Venous Catheterization” to complete catheterization of the external jugular vein. Auscultate and document breath sounds. Verify on a chest x-ray that the tip of the catheter is correctly positioned at or above the junction of the superior vena cava and right atrium. Rule out pneumothorax and hemothorax.
Common Approaches
There are 3 common approaches for cannulation of the internal jugular vein (Figure 6). The provider should become familiar with 1 technique rather than randomly attempt all 3. • Anterior route. Use your index and middle (2nd and 3rd) fingers to
palpate the carotid artery medially at the anterior border of the sternocleidomastoid muscle. Introduce the needle at the midpoint of this anterior border at a 30° angle to the coronal plane. Direct the needle caudad and toward the ipsilateral nipple (Figure 6A).
• Central route. Identify a triangle formed by the 2 portions (sternoclavicular heads) of the sternocleidomastoid muscle with the clavicle at its base. Introduce the needle at the apex of this triangle at a 30° to 45° angle to the coronal plane. Direct the needle caudad and toward the ipsilateral nipple. If you do not enter the vein, withdraw the needle to just below the skin surface and redirect the needle directly caudad along the sagittal plane (ie, less lateral). Do not direct the needle medially across the sagittal plane because you will likely puncture the carotid artery (Figure 6B).
• Posterior route. Introduce the needle deep into the sternal head of the sternocleidomastoid muscle at the junction of the middle and lower thirds of the posterior margin (eg, just above the point where the external jugular vein crosses this muscle). Direct the needle toward the suprasternal notch (Figure 6C).

© 2006 American Heart Association 16
Figure 6. Technique for catheterization of internal jugular vein. A, Anterior route. B, Central route. C, Posterior route.

© 2006 American Heart Association 17
Subclavian Vein Catheterization Procedure Procedure You may use the following procedure for subclavian vein
catheterization:
Step Action 1 If no cervical spine injury is present, hyperextend the
patient’s neck and open the costoclavicular angles by placing a rolled towel directly beneath and parallel with the thoracic spine.
2 Restrain the child in a 30° head-down (Trendelenburg) position with the head turned away from the side to be punctured. Slightly flexing the neck and turning the head toward the puncture site when using the right side approach in infants may improve the likelihood of correct catheter position.44 The right side is preferable. Auscultate and document bilateral breath sounds before you start the procedure.
3 Identify the junction of the middle and medial thirds of the clavicle.
4 Use a long (1-inch to 1.5-inch) 25-gauge needle to administer local anesthetic. You may also use this needle to help locate the subclavian vein (see step 6).
5 Flush the needle, catheter, and syringe with sterile saline. 6 Using sterile technique, introduce a thin-walled needle just
under the clavicle at the junction of the middle and medial thirds of the clavicle. Slowly advance the needle while applying gentle negative pressure with an attached syringe; direct the needle toward a fingertip placed in the suprasternal notch. The syringe and needle should be parallel with the frontal plane, directed medially and slightly cephalad, beneath the clavicle toward the posterior aspect of the sternal end of the clavicle (ie, the lower end of the fingertip in the sternal notch) (Figure 7). Once you obtain a free flow of blood, indicated by backflash into the syringe, rotate the bevel to a caudad position. This position will facilitate placement of the catheter or guidewire into the superior vena cava. Carefully disconnect the syringe while stabilizing the position of the needle. Place a finger over the hub of the needle to prevent entrainment and embolism of air.
7 During a positive-pressure breath or spontaneous exhalation, insert a guidewire through the needle. Advance the guidewire into the right atrium. Entrance of the guidewire

© 2006 American Heart Association 18
into the right atrium often produces premature atrial contractions. If atrial or ventricular arrhythmias occur, withdraw the guidewire a few centimeters. Complete cannulation of the vein using the Seldinger technique.
8 Demonstrate free blood return from all ports of the catheter and, subsequently, free flow of infusate. If blood does not immediately flow back freely, the catheter may be lodged against a vessel wall or the wall of the right atrium. Slightly withdraw the catheter and repeat aspiration. (You may perform this withdrawal/aspiration sequence twice.) If you still do not observe blood return, you must assume that the catheter is not in the vessel and remove the catheter.
Note: Follow steps 5 and 6 in “Femoral Venous Catheterization” to complete catheterization of the subclavian vein. Auscultate and document breath sounds. Verify on a chest x-ray that the tip of the catheter is correctly positioned at or above the junction of the superior vena cava and right atrium. Rule out pneumothorax and hemothorax.
Figure 7. Cannulation of the subclavian vein.

© 2006 American Heart Association 19
References 1. Rosetti VA, Thompson BM, Aprahamian C, et al. Difficulty and delay in
intravascular access in pediatric arrests. Ann Emerg Med. 1984;13:406. 2. Carcillo JA, Davis AL, Zaritsky A. Role of early fluid resuscitation in
pediatric septic shock. JAMA. 1991;266(9):1242-1245. 3. Stovroff M, Teague WG. Intravenous access in infants and children.
Pediatr Clin North Am. 1998;45(6):1373-1393. 4. Lillis KA, Jaffe DM. Prehospital intravenous access in children. Ann Emerg
Med. 1992;21(12):1430-1434. 5. Glaeser PW, Losek JD, Nelson DB, et al. Pediatric intraosseous infusions:
impact on vascular access time. Am J Emerg Med. 1988;6(4):330-332. 6. Kanter RK, Zimmerman JJ, Strauss RH, et al. Pediatric emergency
intravenous access. Evaluation of a protocol. Am J Dis Child. 1986;140(2):132-134.
7. Fiser DH. Intraosseous infusion. N Engl J Med. 1990;322(22):1579-1581. 8. Banerjee S, Singhi SC, Singh S, et al. The intraosseous route is a suitable
alternative to intravenous route for fluid resuscitation in severely dehydrated children. Indian Pediatr. 1994;31(12):1511-1520.
9. Glaeser PW, Hellmich TR, Szewczuga D, et al. Five-year experience in prehospital intraosseous infusions in children and adults. Ann Emerg Med. 1993;22(7):1119-1124.
10. Redding JS, Asuncion JS, Pearson JW. Effective routes of drug administration during cardiac arrest. Anesth Analg. 1967;46(2):253-258.
11. Johnston C. Endotracheal drug delivery. Pediatr Emerg Care. 1992;8(2):94-97.
12. Davison R, Barresi V, Parker M, et al. Intracardiac injections during cardiopulmonary resuscitation: a low-risk procedure. JAMA. 1980;244(10):1110-1111.
13. Pun KK. Cardiac tamponade after intracardiac injection. Anaesth Intensive Care. 1984;12(1):66-67.
14. Vijay NK, Schoonmaker FW. Cardiopulmonary arrest and resuscitation. Am Fam Physician. 1975;12(2):85-90.
15. Maki DG, Ringer M. Evaluation of dressing regimens for prevention of infection with peripheral intravenous catheters. Gauze, a transparent polyurethane dressing, and an iodophor-transparent dressing. JAMA. 1987;258(17):2396-2403.
16. Seldinger SI. Catheter replacement of the needle in percutaneous arteriography: a new technique. Acta Radiol. 1953;39:368-376.
17. O'Grady NP, Alexander M, Dellinger EP, et al. Guidelines for the prevention of intravascular catheter-related infections. Centers for Disease Control and Prevention. MMWR Recomm Rep. 2002;51(RR-10):1-29.

© 2006 American Heart Association 20
18. Nicolson SC, Sweeney MF, Moore RA, et al. Comparison of internal and external jugular cannulation of the central circulation in the pediatric patient. Crit Care Med. 1985;13(9):747-749.
19. Cobb LM, Vinocur CD, Wagner CW, et al. The central venous anatomy in infants. Surg Gynecol Obstet. 1987;165(3):230-234.
20. Stenzel JP, Green TP, Fuhrman BP, et al. Percutaneous femoral venous catheterizations: a prospective study of complications. J Pediatr. 1989;114(3):411-415.
21. Puntis JW, Holden CE, Smallman S, et al. Staff training: a key factor in reducing intravascular catheter sepsis. Arch Dis Child. 1991;66(3):335-337.
22. Legler D, Nugent M. Doppler localization of the internal jugular vein facilitates central venous cannulation. Anesthesiology. 1984;60(5):481-482.
23. Bratton SL, Ramamoorthy C, Eck JB, et al. Teaching successful central venous cannulation in infants and children: audio Doppler versus anatomic landmarks. J Cardiothorac Vasc Anesth. 1998;12(5):523-526.
24. Mallory DL, McGee WT, Shawker TH, et al. Ultrasound guidance improves the success rate of internal jugular vein cannulation. A prospective, randomized trial. Chest. 1990;98(1):157-160.
25. Denys BG, Uretsky BF. Anatomical variations of internal jugular vein location: impact on central venous access. Crit Care Med. 1991;19(12):1516-1519.
26. Denys BG, Uretsky BF, Reddy PS. Ultrasound-assisted cannulation of the internal jugular vein. A prospective comparison to the external landmark-guided technique. Circulation. 1993;87(5):1557-1562.
27. Alderson PJ, Burrows FA, Stemp LI, et al. Use of ultrasound to evaluate internal jugular vein anatomy and to facilitate central venous cannulation in paediatric patients. Br J Anaesth. 1993;70(2):145-148.
28. Kanter RK, Gorton JM, Palmieri K, et al. Anatomy of femoral vessels in infants and guidelines for venous catheterization. Pediatrics. 1989;83(6):1020-1022.
29. Kanter RK, Zimmerman JJ, Strauss RH, et al. Central venous catheter insertion by femoral vein: safety and effectiveness for the pediatric patient. Pediatrics. 1986;77(6):842-847.
30. Lavandosky G, Gomez R, Montes J. Potentially lethal misplacement of femoral central venous catheters. Crit Care Med. 1996;24(5):893-896.
31. Taylor EA, Mowbray MJ, McLellan I. Central venous access in children via the external jugular vein. Anaesthesia. 1992;47(3):265-266.
32. Defalque RJ. Percutaneous catheterization of the internal jugular vein. Anesth Analg. 1974;53(1):116-121.
33. Rao TL, Wong AY, Salem MR. A new approach to percutaneous catheterization of the internal jugular vein. Anesthesiology. 1977;46(5):362-364.
34. Cote CJ, Jobes DR, Schwartz AJ, et al. Two approaches to cannulation of a child's internal jugular vein. Anesthesiology. 1979;50(4):371-373.

© 2006 American Heart Association 21
35. Prince SR, Sullivan RL, Hackel A. Percutaneous catheterization of the internal jugular vein in infants and children. Anesthesiology. 1976;44(2):170-174.
36. Hall DM, Geefhuysen J. Percutaneous catheterization of the internal jugular vein in infants and children. J Pediatr Surg. 1977;12(5):719-722.
37. Krausz MM, Berlatzky Y, Ayalon A, et al. Percutaneous cannulation of the internal jugular vein in infants and children. Surg Gynecol Obstet. 1979;148(4):591-594.
38. Filston HC, Grant JP. A safer system for percutaneous subclavian venous catheterization in newborn infants. J Pediatr Surg. 1979;14(5):564-570.
39. Eichelberger MR, Rous PG, Hoelzer DJ, et al. Percutaneous subclavian venous catheters in neonates and children. J Pediatr Surg. 1981;16(suppl 1)(4):547-553.
40. Venkataraman ST, Orr RA, Thompson AE. Percutaneous infraclavicular subclavian vein catheterization in critically ill infants and children. J Pediatr. 1988;113(3):480-485.
41. Groff DB, Ahmed N. Subclavian vein catheterization in the infant. J Pediatr Surg. 1974;9(2):171-174.
42. Niemann JT, Rosborough JP, Ung S, et al. Hemodynamic effects of continuous abdominal binding during cardiac arrest and resuscitation. Am J Cardiol. 1984;53(2):269-274.
43. Sulek CA, Gravenstein N, Blackshear RH, et al. Head rotation during internal jugular vein cannulation and the risk of carotid artery puncture. Anesth Analg. 1996;82(1):125-128.
44. Jung CW, Bahk JH, Kim MW, et al. Head position for facilitating the superior vena caval placement of catheters during right subclavian approach in children. Crit Care Med. 2002;30(2):297-299.